")
Back to Journals » Journal of Pain Research » Volume 18
Global, Regional and National Burden of Low Back Pain in Adolescents Aged 10–19 years, 1990–2021: A Systematic Analysis of the Global Burden of Disease Study 2021
Authors Wang S, Zhang S, Li M, Chen S , Chen Y , Song Y, Zhang X
Received 19 March 2025
Accepted for publication 10 June 2025
Published 26 June 2025 Volume 2025:18 Pages 3171—3183
DOI https://doi.org/10.2147/JPR.S525330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor King Hei Stanley Lam
Shuang Wang,1,* Shouyao Zhang,1,* Min Li,1 Suyu Chen,1 Yiping Chen,1 Yongli Song,2 Xinghe Zhang1
1Second Clinical Medical College/Second Affiliated Hospital, Yunnan University of Chinese Medicine, Kunming, 650000, People’s Republic of China; 2School of Basic Medicine, Yunnan University of Chinese Medicine, Kunming, 650000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinghe Zhang, Second Clinical Medical College/Second Affiliated Hospital, Yunnan University of Chinese Medicine, Kunming, 650000, People’s Republic of China, Tel +86 0871 6595 4563, Email [email protected]
Objective: To comprehensively analyze the levels and trends of low back pain (LBP) prevalence, incidence, and years lived with disability (YLDs) among adolescents aged 10– 19 globally from 1990 to 2021, stratified by sex and the Socio - Demographic Index (SDI), and analyze the risk factors.
Summary of Background Data: LBP affects adolescents, but its global burden and trends among this age group need exploration.
Methods: Estimations were carried out using the Bayesian meta-regression tool, DisMod-MR(Disease Modeling Meta-Regression) 2.1. The estimated annual percentage change (EAPC) was calculated based on the linear regression patterns of age-standardized rates and calendar years to represent the temporal trends of age-standardized rates. Data analysis and visualization were performed using the R software (version 4.2.2).
Results: In 2021, global 10– 19 years old had 38,476,826 (95% UI, 29,229,615– 49,665,830) incident LBP cases, 19,234,452 (95% UI, 14,487,990– 24,798,451) prevalent cases, and 4,205,995 (95% UI, 2,713,716– 5,947,074) total YLDs. ASPR (Age-Standardized Prevalence Rate), ASIR (Age-Standardized Incidence Rate), ASYR (Age-Standardized YLDs Rate) declined. Females had higher rates. ASYR and SDI were positively correlated. Hungary, Czech Republic, Romania had high national prevalence; certain regions had big increases. Occupational risks were the only risk factor.
Conclusion: LBP still causes high distress to adolescents aged 10– 19 and seriously affects their physical and mental health. The burden of LBP remains high. It is necessary to increase the public and policymakers’ awareness of its risk factors and take preventive measures to reduce the future burden of this disease.
Keywords: low back pain, global burden of disease, years lived with disability, incidence, prevalence, adolescents
Introduction
LBP refers to pain, stiffness, or muscle tension located between the lower rib margin and the gluteal fold, which may or may not be accompanied by sciatica (pain radiating from the buttocks down the course of the sciatic nerve.1,2 It is induced by diverse factors, including poor posture, physical strain, and lifestyle habits, which contribute to the degeneration of spinal structures and the activation of inflammatory responses.3,4 LBP in adults is widely acknowledged for its substantial impact on disability, quality of life, and healthcare consumption.5–7 However, the significance of LBP in adolescents has received far less attention in both social and scientific literature. This lack of attention is concerning not only due to the considerable impact LBP has on adolescents but also because adolescent LBP is associated with the future development of disabling LBP.8–11 LBP often emerges early in adolescence, with nearly 14% of teenagers reporting LBP in the past month, and approximately 10% reporting persistent LBP.9,12 By their teenage years, girls are almost twice as likely to report persistent back pain compared to boys, and by adolescence, one-third of teenagers report experiencing back pain in the past month.8,13 Common symptoms of adolescent LBP encompass back discomfort, pain during physical activity, and in severe cases, reduced participation in school and sports activities. The recurrence of these symptoms can severely affect adolescents’ mental health, leading to anxiety, depression, and a decline in overall quality of life.14–17
The treatment methods for LBP include behavioral management, non-pharmacological treatment options, pharmacological treatment protocols, and surgery.18 As first-line treatments for LBP, exercise and physical therapy often require evaluation before implementation. The Functional Timed Single-Leg Stance Test (FTSST) is a simple, feasible, and repeatable method that can assess patients’ lower limb muscle strength, balance ability, functional status, and pain, demonstrating significant clinical guiding value.19 Meanwhile, conducting more clinical research to explore better exercise and physical therapy methods is of great significance for the treatment of LBP.A recent study has found that routine physical therapy combined with kinesiology taping yields superior outcomes compared to physical therapy alone.20
Given the global trend of increased sedentary behavior and poor posture habits among adolescents, the burden of LBP has gradually intensified over the past few decades.21 Previous studies have predominantly focused on adult populations, where LBP is closely related to age and occupational factors. However, adolescents represent a crucial developmental phase, during which they are at an elevated risk for LBP due to factors such as rapid growth spurts, heavy schoolbags, and a lack of musculoskeletal conditioning. Despite these risk factors, research on adolescent LBP remains limited, with insufficient understanding of the prevalence trends, risk factors, and long-term impacts for this age group.
The Global Burden of Disease (GBD) study offers comprehensive data on the prevalence and burden of various diseases across countries and regions, including trends in disease burden over time, stratified by factors such as age, gender, and SDI. In this study, we conducted a systematic analysis of the global, regional, and national burden of LBP among adolescents aged 10–19 years, based on GBD 2021 data from 1990 to 2021. By assessing the incidence, prevalence, and YLDs associated with adolescent LBP, this study provides novel insights into the burden of LBP across different regions and identifies key risk factors and epidemiological trends. Stratified analysis by SDI and gender also highlighted significant disparities in LBP burden, with lower-income regions experiencing greater health loss due to LBP. These findings will inform future prevention and management strategies for adolescent LBP to mitigate the risk of long-term disability.
Against this backdrop, the present study aims to address the critical gap in understanding the global burden of adolescent LBP by utilizing the most comprehensive and up-to-date GBD dataset. We seek to: Characterize the global epidemiology of adolescent LBP through incidence, prevalence, and YLDs. Identify regions and populations with disproportionately high burden to inform priority-setting in resource allocation. Evaluate the relationship between risk factors for adolescent LBP and SDI. By bridging the evidence gap in this vulnerable age group, this study aims to establish a benchmark for adolescent spinal health, advocate for age-specific preventive interventions in schools and communities, and promote cross-sectoral policies to mitigate the intergenerational transmission of LBP-related disability.
Materials and Methods
Data Sources
Data for this study were extracted from GBD 2021 database, accessible through publicly available resources. The primary datasets utilized for this analysis can be obtained from the GBD Data Input Sources Tool (https://ghdx.healthdata.org/gbd - 2021/data - input - sources) and the GBD Results Tool (https://vizhub.healthdata.org/gbd - results/). These resources provide access to data on the incidence, prevalence, and YLDs for a wide range of diseases and risk factors across global, regional, and national levels.
In this study, we analyzed data for adolescents aged 10–19 years, covering the period from 1990 to 2021. The GBD 2021 encompasses 369 diseases and injuries, along with 87 associated risk factors.22 LBP was identified using the International Classification of Diseases (ICD-10) codes M54 - M54.9, which are specifically related to dorsopathies involving the lumbar region. The age group of 10–19 years was selected, and the data were analyzed by gender, year, and location.
Disease Modeling
The DisMod - MR 2.1, a Bayesian meta - regression tool, was employed to model the incidence, prevalence, remission, and mortality of LBP, thereby ensuring the coherence among these epidemiological parameters. This tool enables the integration of multiple data sources while accounting for known biases and generating consistent estimates across different age groups, years, and geographical locations.21 The age - standardized rates (ASRs) of LBP incidence, prevalence, and YLDs were computed based on the GBD 2021 global standard population, with the calculation method following the formula specified below: Age- standardized rate=∑Ai=1aiwi /∑Ai=1wi (where ai is the age specific rate and wi is the weight in the same age subgroup of the chosen reference standard population (in which i denotes the ith age class) and A is the upper age limit.23,24
Sdi
SDI was utilized to explore the relationship between the LBP burden and social development. SDI values, ranging from 0 to 1, represent a composite measure of income per capita, educational attainment, and total fertility rates.25 A value close to 1 signifies high socioeconomic development (eg, high income, high education levels, low fertility), often seen in developed nations. A value close to 0 indicates low socioeconomic development (eg, low income, limited education, high fertility), common in less-developed regions. Based on SDI scores, countries were categorized into five groups: high SDI, high - middle SDI, middle SDI, low - middle SDI, and low SDI. In this study, we evaluated the association between SDI levels and the age - standardized YLDs rates for LBP in 2021 across 21 GBD regions.
Attributable Risk Factors
The GBD 2021 comparative risk assessment framework was applied to assess the proportion of disability - adjusted life years (DALYs) attributable to specific risk factors, which were grouped into three categories: (1) environmental and occupational, (2) behavioral, and (3) metabolic. This study utilized the GBD comparative risk assessment framework, proposed by the GBD Risk Factor Collaborators, to evaluate the proportion of YLDs attributable to various risk factors. This comprehensive framework consists of six major steps, which are used to calculate the disease burden specific to each individual risk factor.26
YLDs and DALYs
YLDs were used as the primary metric to quantify the burden of LBP since the cause - of - death model in GBD does not directly attribute mortality to LBP. YLDs were calculated by multiplying the prevalence of each severity level by the corresponding disability weights, which are standardized measures representing the severity of health loss associated with LBP.27 DALYs were equivalent to YLDs in this study due to the non - fatal nature of LBP.
Statistical Analysis
Statistical analyses were conducted using R software (version 4.2.2). ASRs, prevalence, and YLDs per 100,000 people, along with their corresponding 95% confidence intervals (CIs), were calculated for the years 1990 to 2021. EAPC is a crucial indicator in our analysis based on GBD data. It plays a vital role in characterizing the trends of various health - related factors over time.28 The calculation of EAPC is mainly accomplished through specific statistical models. Generally, regression - based methods are used. A commonly employed approach is the join point regression model.29 In this model, EAPC is estimated by fitting the data points of the variable of interest (such as disease prevalence, incidence, or other health indicators from the GBD data set) within a specific time period. The model views the data as a function of time and aims to identify the best - fitting straight line or curve that represents the trend. Then, the slope of this line or curve in each segment (in the case of join points) is converted into an estimated annual percentage change value. For example, if the EAPC in the prevalence of a certain disease from 1990 to 2021 is 0.2%, it indicates that the number of prevalent cases of this disease increased at an annual rate of 0.2% during this period. Conversely, if the EAPC is negative, it means the number of prevalent cases of the disease decreased at an annual rate of 0.2%. All rates are reported per 100,000 population, and visualizations were created using the “ggplot2” package in R.
Results
Global Trends
In 2021, globally, there were an estimated 38,476,826 (the number of prevalent cases of musculoskeletal diseases among the global 10–19 years old population is 58,833,084) [95% CI: 29,229,615 to 49,665,830] LBP cases among people aged 10–19. Compared with 1990, the number of cases increased by 5,200,025 [95% CI: 5,009,430 to 5,645,237]. The number of incident cases was 19,234,452 (the number of incident cases of musculoskeletal diseases among the global 10–19 years old population is 22,616,875) [95% CI: 14,487,990 to 24,798,451]. Compared with 1990, there was an increase of 2,556,743 [95% CI: 1,798,139 to 3,453,406] cases. YLDs was 4,205,995 (YLD due to musculoskeletal diseases among the global 10–19 years old population is 6,279,047) [95% CI: 2,713,716 to 5,947,074]. Compared with 1990, it increased by 568,763 [95% CI: 352,242 to 840,405]. In 1990, the age - standardized incidence rate of LBP in people aged 10–19 was estimated to be 1573 [95% CI: 1110 to 2121] per 100,000 population (1.573%). By 2021, it had decreased to 1488 [95% CI: 1050 to 2007](1.488%). EAPC was - 0.21 [95% CI: - 0.23 to - 0.18]. At the same time, the age - standardized prevalence rate of LBP in this population was estimated to be 3130 [95% CI: 2279 to 4141] per 100,000 population (3.130%). By 2021, it had decreased to 2974 [95% CI: 2176 to 3928](2.974%). The EAPC was - 0.20 [95% CI: - 0.22 to - 0.18]. The age - standardized rate of YLDs per 100,000 population also decreased from 342 [95% CI: 210 to 503](0.342%) in 1990 to 325 [95% CI: 200 to 478](0.325%) in 2021. The EAPC was - 0.20 [95% CI: - 0.22 to - 0.18] (Table S1).
Regional Trends
In 2021, the three regions with the highest age - standardized prevalence rate of LBP per 100,000 people were Central Europe, with a rate of 5975 [95% CI 4379 to 7744]. High - income Asia Pacific had an age - standardized prevalence rate of 5158 [95% CI 3773 to 6774]. Australasia had an age - standardized prevalence rate of 4941 [95% CI 3644 to 6477]. In contrast, Southeast Asia had the lowest estimated age - standardized prevalence figures, with a rate of 1852 [95% CI 1323 to 2511]. East Asia had an age - standardized prevalence rate of 2075 [95% CI 1494 to 2761], and Oceania had a rate of 2088 [95% CI 1494 to 2820] (Table S1).
The age - standardized incidence rate of LBP in Central Europe was 2906 [95% CI 2079 to 3892]. Australasia had an age - standardized incidence rate of 2557 [95% CI 1784 to 3432], and High - income Asia Pacific had a rate of 2545 [95% CI 1805 to 3405]. These regions were among the top three positions. In contrast, the incidence rates were relatively low in Southeast Asia, with a rate of 959 [95% CI 655 to 1311]. Southern Sub - Saharan Africa had an incidence rate of 1044 [95% CI 722 to 1429], and East Asia had a rate of 1078 [95% CI 748 to 1473] (Table S1).
The age - standardized rate of YLDs in Central Europe was 657 [95% CI 409 to 950]. High - income Asia Pacific had a rate of 567 [95% CI 352 to 837], and Australasia had a rate of 538 [95% CI 334 to 799]. These regions were among the top three positions. In contrast, the age - standardized YLDs rates were relatively low in Southeast Asia, with a rate of 204 [95% CI 122 to 305]. Oceania had a rate of 229 [95% CI 135 to 344], and Southern Sub - Saharan Africa had a rate of 230 [95% CI 139 to 346] (Table S1).
The EAPC in age - standardized prevalence estimates from 1990 to 2019 varied among GBD regions in 2021. As can be seen from Table S1, most regions showed a downward trend. Among them, Australasia (- 0.34 (95% CI - 0.41 to - 0.26)), South Asia (- 0.29 (95% CI - 0.35 to - 0.24)), and High - income Asia Pacific (- 0.24 (95% CI - 0.26 to - 0.26)) showed a relatively high downward trend. Moreover, these regions are also among the top three in terms of the downward trends of age - standardized incidence rate and YLDs rate. However, some regions showed a slight upward trend. Tropical Latin America had the highest growth trends in age - standardized prevalence (0.20 (95% CI 0.14–0.27)), incidence rate (0.17 (95% CI 0.11–0.23)), and YLDs rate (0.21 (95% CI 0.15–0.27)) (Table S1).
It is noteworthy that from 1990 to 2021, the number of cases of illness increased significantly. The GBD regions that contributed to this growth in 2021 were different from those in 1990. Similarly, from 1990 to 2019, the number of incident cases and YLDs also increased significantly, and the contributing regions between 2019 and 1990 were also different.
National Trends
In 2021, Hungary (6662 (95% CI 5008 to 8763)), the Czech Republic (6545 (95% CI 4744 to 8694)), and Romania (6369 (95% CI 4757 to 8328)) are the countries with comparatively high age - standardized prevalence estimates. The countries with moderately low age - standardized prevalence estimates are the Republic of the Union of Myanmar (1578 (95% CI 1115 to 2171)), the Kingdom of Thailand (1631 (95% CI 1143 to 2259)), and the Republic of Maldives (1680 (95% CI 1187 to 2310)). Hungary (3141 (95% CI 2253 to 4214)), the Czech Republic (3104 (95% CI 2202 to 4176)), and Romania (3034 (95% CI 2165 to 4065)) have comparatively high age - standardized incidence rates. The Republic of the Union of Myanmar (826 (95% CI 559 to 1142)), the Kingdom of Thailand (852 (95% CI 567 to 1182)), and the Republic of Maldives (872 (95% CI 592 to 1209)) have moderately low age - standardized incidence rates. In 2021, for the three countries with high and low age - standardized prevalence estimates, their rankings in age - standardized YLDs rates are identical (Figure 1 and Table S2).
 |
Figure 1 Age-standardized prevalence (A), incidence (B), and age-standardized YLDs rate (C) of low back pain among people aged 10–19 years worldwide, by region, 2021. |
Sex Differences
In 2021, in Australasia, the gender disparity in age - standardized prevalence rate is relatively high, with a value of 4013 (95% CI 3044 to 5270). In Southern Latin America, the gender disparity in age - standardized prevalence rate is also relatively high, with a value of 3216 (95% CI 2383 to 4105). In North Africa and the Middle East, the gender disparity in age - standardized prevalence rate is relatively high as well, with a value of 3107 (95% CI 2317 to 4051). In Southern Sub - Saharan Africa, the gender disparity in age - standardized prevalence rate is relatively low, with a value of 612 (95% CI 469 to 798). In Western Sub - Saharan Africa, the gender disparity in age - standardized prevalence rate is relatively low, with a value of 623 (95% CI 451 to 833). In Central Sub - Saharan Africa, the gender disparity in age - standardized prevalence rate is relatively low, with a value of 667 (95% CI 478 to 935) (Table S3 and Figure 2).
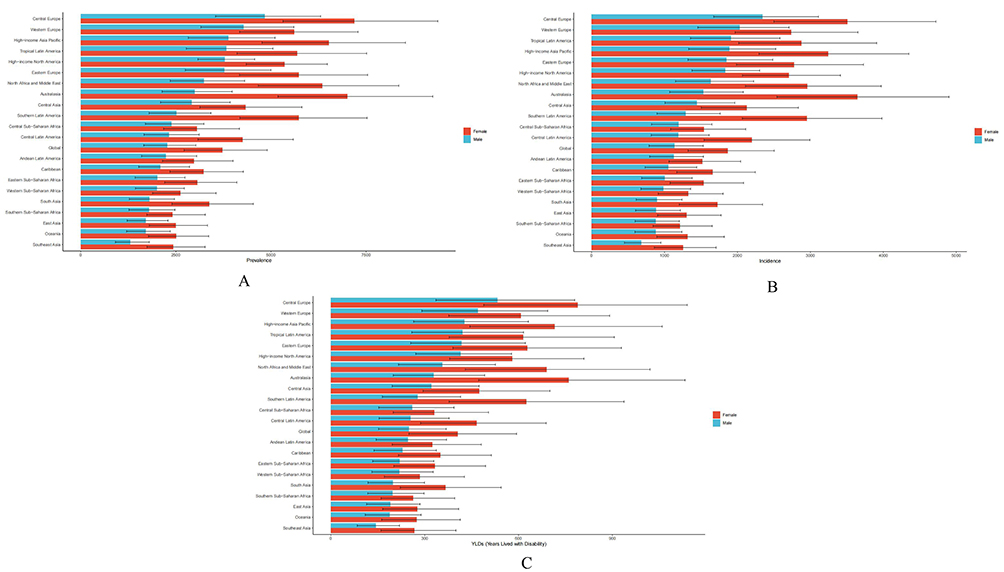 |
Figure 2 Age-standardized prevalence (A), incidence (B), and age-standardized YLDs rate (C) of low back pain by sex among people aged 10–19 years worldwide, by region, 2021. |
In 2021, in Australasia, the gender disparity in age - standardized incidence rate is relatively high, with a value of 2110 (95% CI 1471 to 2820). In Southern Latin America, the gender disparity in age - standardized incidence rate is relatively high, with a value of 1661 (95% CI 1171 to 2216). In High - income Asia Pacific, the gender disparity in age - standardized incidence rate is relatively high, with a value of 1355 (95% CI 964 to 1825). In Southern Sub - Saharan Africa, the gender disparity in age - standardized incidence rate is relatively low, with a value of 327 (95% CI 245 to 452). In Western Sub - Saharan Africa, the gender disparity in age - standardized incidence rate is relatively low, with a value of 336 (95% CI 238 to 445). In Central Sub - Saharan Africa, the gender disparity in age - standardized incidence rate is relatively low, with a value of 349 (95% CI 260 to 463) (Table S3 and Figure 2).
The regions with relatively high and low gender disparity in age - standardized YLDs rate are the same as those with a gender disparity in age - standardized prevalence rate (Table S3 and Figure 2).
Global Trends by SDI
Generally, over the past three decades, the age - standardized YLDs rate of LBP among adolescents aged 10–19 has been positively associated with SDI (Figure 3). Interestingly, at the regional level, with the increase in SDI from 1990 to 2021, the age - standardized YLDs rate of LBP in adolescents aged 10–19 globally shows a downward trend. In Central Europe, North Africa and the Middle East, Tropical Latin America, and High - income Asia Pacific, the estimated burden of LBP in adolescents aged 10–19 observed from 1990 to 2021 is higher than the expected level based on SDI. In 2021, there is also a positive association between the age - standardized YLDs rate of LBP and SDI in 204 countries and regions. In many countries and regions including Hungary, Romania, and Czechia, the age - standardized YLDs rate is higher than the expected level (Figure 4).
 |
Figure 3 Age-standardized rates of years lived with disability (YLDs) for low back pain in adolescents aged 10–19 years, calculated by sociodemographic index (SDI), for 21 Global Burden of Disease (GBD) regions, between 1990 and 2021; expected values based on SDI and disease rates for all regions are shown as the middle curve. 32 points are plotted foreach GBD region, showing the observed age-standardized YLDs rates for that region from 1990 to 2021 (generated from data provided by http://ghdx.healthdata.org/gbd-results-tool). |
 |
Figure 4 Age-standardized YLDs rates and socio-demographic index (SDI) for low back pain in adolescents aged 10–19 years in 2021 for 204 countries and territories; expected values are shown as black lines. Each point shows the age-standardized YLDs rate for a specific country or region in 2021 (generated from data provided by http://ghdx.healthdata.org/gbd-results-tool). |
Risk Factors
Among adolescents aged 10–19, occupational risks are the sole risk factor for LBP. Compared to the population aged 20 and above, two risk factors, namely high body - mass index and smoking, are not applicable. From a regional perspective, the regional attributable risk of occupational risks varies from 1.87% to 21.16%. Eastern Sub - Saharan Africa, East Asia, and Western Sub - Saharan Africa have relatively high YLDs attribution rates of 21.16%, 14.91%, and 14.86%, respectively. Eastern Europe, Central Europe, and Southern Latin America have relatively low YLDs attribution rates of 1.87%, 2.3%, and 2.74%, respectively (Tables S4, S5 and Figure 5).
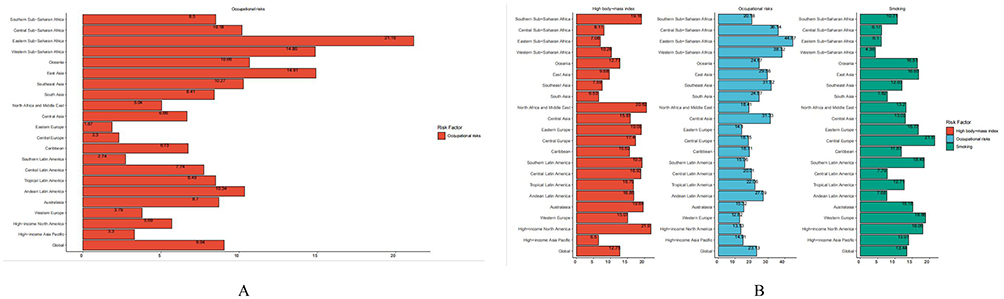 |
Figure 5 Percentage of YLDs due to risk factors in adolescents aged 10–19 (A) and 20+ years (B) in the Global Burden of Disease Study 2021. |
Discussion
In this study, we employ the publicly available modeled data and methods within the Global Burden of Disease Study 2021 (GBD Study 2021) to present the latest, comprehensive, and comparable information regarding the prevalence, incidence, and YLDs of LBP in 204 countries and territories during 1990–2021.30 This study analyzes the burden of LBP at the national level and the association between LBP burden and SDI.
In 2021, globally, there were approximately 38,476,826 prevalent cases, 19,234,452 incident cases, and 4,205,995 YLDs related to LBP among adolescents aged 10–19. Although the age - standardized prevalence, incidence, and YLDs rate of LBP in adolescents aged 10–19 decreased slightly from 1990 to 2021, the numbers of prevalent cases, incident cases, and YLDs increased substantially. Moreover, the burden of LBP in some regions is still rising, with Tropical Latin America, Eastern Europe, and High - income North America witnessing the largest increases.
LBP during adolescence not only affects the quality of life of patients but also imposes social and economic burdens. Firstly, in the age group of 10 to 19 years old, LBP may lead to school absenteeism and a decline in academic performance. Chronic LBP may further limit their social activities and physical exercise, thereby reducing the quality of life.15 Secondly, from an economic perspective, the direct costs associated with LBP include medical expenses such as diagnosis, treatment (including physical therapy and drug treatment), and sometimes surgical treatment. Indirect costs involve parental work absence, transportation expenses, and the cost of patient care. As one of the common types of pain, LBP accounts for a considerable proportion of direct medical costs. According to a study on the Netherlands, the annual direct medical cost of adolescent LBP is estimated to be an expenditure of 480 euros per 1,000 children.31 The long - term cost is even more significant. Chronic pain during adolescence can lead to chronic health problems in adulthood, thereby increasing medical expenses over their life cycle. For example, adolescents with chronic LBP may need continuous treatment and management in adulthood, increasing long - term medical expenditures. In the United States, the annual total cost of chronic LBP is estimated to be between 100 billion and 200 billion US dollars, and the vast majority of it is indirect cost caused by loss of work productivity.32 In general, the social and economic burden of adolescent LBP is significant, and more research is needed to reveal its comprehensive impact and develop effective prevention and intervention measures.
In the study of 21 regions globally in 2021, it was demonstrated that the age - standardized prevalence rate, incidence rate, and YLDs rate of LBP in female adolescents were all higher than those in male adolescents, and the degree of gender gap varied in different regions.
The pelvic development of females during adolescence is different from that of males, and their pelvis is usually wider.33 This structural characteristic will cause the biomechanical stress situation of the lumbar spine during human standing, walking, and movement to change.34 For example, the lumbar lordosis angle of females may be adjusted due to the wide pelvis, increasing the tension and pressure on the lower back muscles and ligaments.35 Research shows that under the same activity intensity and frequency, the load on the lumbar spine of females is more unbalanced compared to that of males, thus increasing the anatomical risk of LBP.36 Hormonal fluctuations are an important physiological characteristic of female adolescence. The levels of estrogen and progesterone show regular changes during the menstrual cycle. Estrogen plays an important regulatory role in bones and connective tissues, and its fluctuations can affect the metabolism of bone density and articular cartilage.37 During the stage of lower estrogen levels, such as the premenstrual period, the calcium loss in women’s bones may increase and the repair ability of articular cartilage may weaken.38 This makes the lumbar joints more susceptible to damage in daily activities, thereby increasing the incidence of LBP.39 During adolescence, there are certain differences in the psychological stressors faced by females and males, and females are more susceptible to some stressors. For example, society and culture have relatively high requirements for the appearance and body image of females. Adolescent females may experience negative emotions such as anxiety and depression due to dissatisfaction with their own appearance.40 At the same time, in terms of academics and social interactions, females may pay more attention to the harmony of interpersonal relationships and excellent academic performance. When facing interpersonal conflicts or academic pressure, they may bear a greater psychological burden.41 These negative emotions and psychological pressures may affect the body’s pain perception and regulatory mechanisms through the neuroendocrine system, making females more likely to perceive pain and the pain may be more severe when facing physical discomfort such as LBP, thus further affecting the development process and disability degree of LBP.42
Globally, with the improvement of SDI, economic development often brings about significant changes in lifestyle. In regions with high SDI, adolescents are more likely to engage in sedentary behaviors, such as prolonged use of electronic devices and indulgence in indoor recreational activities, and lack sufficient physical activity. For instance, in the high - income Asia Pacific region and Central Europe, with the rapid urbanization process, the daily activity patterns of adolescents have gradually shifted to static, increasing the risk of LBP. This results in the age - standardized YLDs rate remaining at a relatively high level or even exceeding the expected level at a higher SDI level.43 In addition, in regions with a high SDI, the high degree of education popularization and strict education quality requirements make adolescents face fierce academic competition. Long hours of study and poor sitting postures have become common. For example, in Eastern European countries such as Hungary, Romania, and the Czech Republic, the education system emphasizes academic achievements, and students need to spend a large amount of time at their desks, negatively affecting the spinal health of adolescents and leading to an increase in the YLDs rate of LBP, which is higher than expected.44 In regions with high SDI, issues such as high - calorie diets and insufficient physical activity are prevalent, and the obesity rate (BMI ≥ 30) can reach over 30%.45,46 Obesity not only increases the pressure on the lumbar spine through mechanical loading (for every 10kg increase in body weight, the lumbar spine load increases by 30–50kg), but also induces chronic inflammatory responses, accelerating intervertebral disc degeneration.47 In high - SDI regions, medical imaging technology has a high penetration rate, and the detection rate of asymptomatic lumbar disc herniation can reach 30%, but only 5% - 10% of these cases require intervention.48 Overdiagnosis may cause patients to experience the “disease labeling effect”, triggering anxiety and pain sensitization, which in turn prolongs the course of the disease.49 Although surgical techniques are advanced in high - SDI regions, the incidence of adjacent segment degeneration after lumbar fusion surgery can reach 20% - 40%, which may lead to secondary LBP in the long term.50 In addition, the problem of abuse of postoperative painkillers (such as opioids) is more prominent in high - SDI regions, easily forming a vicious cycle of “pain - drug dependence - functional degeneration”.51,52 Conversely, in some regions with a relatively low economic development level but a relatively fast growth in SDI, although the overall lifestyle may not have completely shifted to a sedentary one, the increase in psychological pressure may affect the body’s perception and response to pain through the neuroendocrine pathway, thereby affecting the YLDs rate of LBP and making it higher than the level expected based on SDI.53 In some regions with a lower SDI but relatively scarce educational resources, adolescents may face relatively less academic pressure, which to some extent reduces the risk factors for LBP caused by long hours of study, resulting in a YLDs rate lower than the expected level.54
In Eastern Sub - Saharan Africa, Western Sub - Saharan Africa, and East Asia, some adolescents may be engaged in relatively heavy physical labor, such as agricultural work, handicraft production, or simple industrial production. These types of labor often require long - term bending, heavy lifting, or maintaining a fixed posture, exerting greater pressure on the adolescents’ waists and increasing the possibility of LBP caused by occupational risks.55 For example, in some rural areas of Africa, adolescents may need to assist their families in heavy agricultural activities, and frequent bending actions like sowing and harvesting increase the risk of developing LBP.56 Conversely, in Eastern Europe, Central Europe, and Southern Latin America, adolescents are more concentrated in schools for education, with a relatively low proportion of participation in labor and lighter labor intensity.57 They may mainly be engaged in some light physical activities, such as part - time retail work or simple office assistant work, which exert less pressure on the waist and have relatively low occupational risks.57 In regions with a high level of education popularization, such as Central and Eastern Europe, adolescents spend most of their time receiving systematic education in schools. Vocational training is usually carried out in the later stage of the formal education system or after graduation, and vocational training focuses on skill cultivation and the imparting of labor safety knowledge.58 This enables adolescents to possess certain knowledge and skills before entering the labor market, allowing them to choose relatively safe and suitable jobs and reducing occupational risks.59 For example, vocational schools will provide students with labor safety courses related to their majors, cultivating correct working postures and labor habits and reducing the risk of LBP.60 In some regions with relatively scarce educational resources, such as some parts of Sub - Saharan Africa and East Asia, adolescents may leave school and enter the labor market earlier and lack formal vocational training. They lack the necessary skills and knowledge in work and do not understand how to prevent occupational injuries.61 Overall, the education systems in regions such as Eastern Europe are more developed compared to those in sub-Saharan Africa. Additionally, adolescent working hours are subject to clearly defined legal restrictions. These factors collectively result in significant disparities in YLDs attribution rates between these regions.
In Victoria, Australia, a statewide community intervention aimed at changing people’s beliefs and expectations about back pain was followed by a reduction in its incidence, which was not observed in the control group.62 A unique study investigating the prevalence of back pain in Germany reported that shortly after German reunification in 1990, there were significant differences in back pain prevalence between the East and West, with lower prevalence in the East.63 Over the next 13 years, while the prevalence in the West remained high, the gap in prevalence between the East and West narrowed to nearly zero. The emergence and disappearance of these differences support the view that pain and the resulting disability are largely influenced by culture-determined health beliefs, as well as physical activity and mental health.64 In this study, the regions with the largest differences in incidence, prevalence, and YLDs (Years Lost to Disability) were Central Europe and Southeast Asia, and it is clear that there are significant cultural differences between these two regions.
From a health policy perspective, addressing the global burden of LBP in adolescents requires multi-sectoral collaboration and targeted interventions tailored to regional and socioeconomic contexts. First, preventive strategies should prioritize population-wide health education to raise awareness about LBP risk factors, such as prolonged sedentary behavior, poor posture, and unsafe lifting practices. School-based programs could integrate age-appropriate modules on spinal health, including daily warm-up exercises and ergonomic guidance, with a focus on gender-specific needs—for example, educating female adolescents about hormonal influences on pain sensitivity and stress management techniques.Second, school environment ergonomics must be systematically improved. Policies should mandate adjustable desks and chairs that accommodate adolescent growth, reduce backpack weights (eg, through digital textbook adoption), and enforce regular break times to encourage movement. In high-SDI regions with intense academic pressure, like Eastern Europe and East Asia, education systems should implement evidence-based limits on daily study hours and promote peer-led “posture champions” to reinforce healthy habits. For low-SDI regions where adolescents engage in heavy labor, occupational health protections are critical, including age-appropriate workload regulations, vocational training on safe lifting techniques, and access to protective equipment for those in agricultural or industrial roles.Third, promoting physical activity requires policy incentives to increase structured and unstructured movement. Governments should expand school-based sports programs, integrate active commuting (eg, walking or cycling to school), and collaborate with urban planners to create safe public spaces for play. In high-SDI areas with sedentary lifestyles, digital health interventions (eg, mobile apps tracking screen time and prompting movement) could complement in-person initiatives. Conversely, in regions with high physical labor burdens, policies should balance injury prevention with access to recreational activities that strengthen core muscles without exacerbating occupational strain. Lastly, health systems need enhanced capacity to diagnose and manage adolescent LBP, particularly in low-resource settings. Training primary care providers in non-pharmacological interventions (eg, physical therapy, yoga) and reducing barriers to low-cost treatments would improve outcomes. Cross-sectoral monitoring frameworks, linking education, labor, and health data, should be established to evaluate policy impacts on LBP prevalence, incidence, and YLDs over time. By embedding these strategies into national health agendas, policymakers can mitigate the lifelong social and economic toll of adolescent LBP while fostering healthier lifestyles for future generations.
Conclusion
LBP affects the health of adolescents, and the situation varies greatly in different countries and regions. Although the age-standardized prevalence, incidence, and YLDs due to LBP have not changed significantly over the past three decades, its burden remains high, especially among adolescent females who are at particularly high risk. As an important risk factor for LBP in adolescents, occupational risks should receive more extensive attention. It is strongly recommended to raise the awareness of the public and policymakers about adolescent LBP and its risk factors, and provide preventive and treatment interventions for adolescent patients with LBP to reduce the future burden of this disease.
Statement of Exemption
In accordance with Article 32(1) of the Ethical Review Measures for Life Sciences and Medical Research Involving Human Subjects (National Health Commission, Science and Education Document No. 4 [2023], issued on February 18, 2023), which stipulates that “research utilizing legally obtained publicly available data” is exempt from ethical review, this study analyzed publicly accessible data from the Global Burden of Disease Study (GBD) 2021 to investigate the burden of low back pain among adolescents aged 10–19 years from 1990 to 2021. The research did not involve the collection of individual sensitive information (eg, names, identification numbers, contact details) or biological samples, nor did it entail any interventions on individuals. Therefore, it falls within the scope of ethics review exemption and does not require approval by an Institutional Review Board (IRB).
Funding
This work is funded by Yunnan Key Laboratory of Integrated Traditional Chinese and Western Medicine for Chronic Disease in Prevention and Treatment (No.2019DG016), Yunnan Province Innovation Team of Prevention and Treatment for Brain Diseases with Acupuncture and Tuina (No.202405AS350007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vlaeyen JWS, Maher CG, Wiech K. et al. Low back pain. Nat Rev Dis Primers. 2018;4(1):52. doi:10.1038/s41572-018-0052-1
2. Urits I, Burshtein A, Sharma M, et al. Low Back Pain, a Comprehensive Review: pathophysiology, Diagnosis, and Treatment. Curr Pain Headache Rep. 2019;23(3):23. doi:10.1007/s11916-019-0757-1
3. Andersson GB. Epidemiological features of chronic low-back pain. Lancet. 1999;354(9178):581–585. doi:10.1016/S0140-6736(99)01312-4
4. Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. doi:10.1136/annrheumdis-2013-204428
5. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/S0140-6736(18)30489-6
6. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
7. Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. Lancet. 2018;391(10137):2384–2388. doi:10.1016/S0140-6736(18)30488-4
8. Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res. 2013;27(5):591–600. doi:10.1016/j.berh.2013.09.007
9. O’Sullivan K, O’Keeffe M, O’Sullivan L, O’Sullivan P, Dankaerts W. Perceptions of sitting posture among members of the community, both with and without non-specific chronic low back pain. Manual Ther. 2013;18(6):551–556. doi:10.1016/j.math.2013.05.013
10. O’Sullivan K, O’Sullivan P, O’Sullivan L, Dankaerts W. What do physiotherapists consider to be the best sitting spinal posture? Manual Ther. 2012;17(5):432–437. doi:10.1016/j.math.2012.04.007
11. Salminen JJ, Erkintalo MO, Pentti J, Oksanen A, Kormano MJ. Recurrent low back pain and early disc degeneration in the young. Spine. 1999;24(13):1316–1321. doi:10.1097/00007632-199907010-00008
12. Saarni L, Nygård C, Nummi T, Kaukiainen A, Rimpelä A. Comparing the effects of two school workstations on spine positions and mobility, and opinions on the workstations – a 2-year controlled intervention. Int J Ind Ergon. 2009;39(6):981–987. doi:10.1016/j.ergon.2009.08.006
13. Haselgrove C, Straker LM, Smith A, O’Sullivan P, Perry M, Sloan N. Perceived school bag load, duration of carriage, and method of transport to school are associated with spinal pain in adolescents: an observational study. Aust J Physiother. 2008;54(3):193–200. doi:10.1016/S0004-9514(08)70026-6
14. Dionne CE, Dunn KM, Croft PR, et al. A Consensus Approach Toward the Standardization of Back Pain Definitions for Use in Prevalence Studies. Spine. 2008;33(1):95–103. doi:10.1097/BRS.0b013e31815e7f94
15. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–747. doi:10.1016/S0140-6736(16)30970-9
16. Bejia I, Younes M, Jamila HB, et al. Prevalence and factors associated to low back pain among hospital staff. Joint Bone Spine. 2005;72(3):254–259. doi:10.1016/j.jbspin.2004.06.001
17. Goncalves TR, Mediano M, Sichieri R, Cunha DB. Is Health-related Quality of Life Decreased in Adolescents With Back Pain? Spine. 2018;43(14):E822–E829. doi:10.1097/BRS.0000000000002520
18. Knezevic NN, Candido KD, Vlaeyen J, Van ZJ, Cohen SP. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
19. Ozudogru A, Canli M, Ceylan I, Kuzu S, Alkan H, Karacay BC. Five Times Sit-to-Stand Test in people with non-specific chronic low back pain-a cross-sectional test-retest reliability study. Ir J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
20. Yildiz NT, Canlı M, Kocaman H, Alkan H. The effectiveness of kinesio taping in addition to conventional treatment in patients with chronic low back pain: a randomised controlled trial. J Health Sci Med. 2024;7(5):564–570. doi:10.32322/jhsm.1537291
21. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
22. Gu H, Yan D, Li J, Long X, Wang K. Trends and future projections of incidence rate and mortality of rheumatoid arthritis in China: a systematic analysis based on GBD 2021 data. Clin Rheumatol. 2024;43(9):2799–2806. doi:10.1007/s10067-024-07083-3
23. AJ Ferrari, DF Santomauro, A Aali, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
24. Yang K, Yang X, Jin C, et al. Global burden of type 1 diabetes in adults aged 65 years and older, 1990–2019: population based study. BMJ. 2024;385:e78432.
25. Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1160–1203.
26. Murray CJL, Aravkin AY, Zheng P, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–1249.
27. Salomon JA, Haagsma JA, Davis A, et al. Disability weights for the Global Burden of Disease 2013 study. Lancet Glob Health. 2015;3(11):e712–e723. doi:10.1016/S2214-109X(15)00069-8
28. Kyu HH, Abate D, Kh A, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922.
29. Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. doi:10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z
30. Ferreira ML, de Luca K, Haile LM, et al. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
31. van Tulder M, Furlan A, Bombardier C, Bouter L. Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. Spine. 2003;28(12):1290–1299. doi:10.1097/01.BRS.0000065484.95996.AF
32. Katz JN. Lumbar Disc Disorders and Low-Back Pain: socioeconomic Factors and Consequences. J Bone Joint Surg. 2006;88(suppl_2):21–24.
33. Bailey JF, Shefi S, Soudack M, Kramer PA, Been E. Development of Pelvic Incidence and Lumbar Lordosis in Children and Adolescents. Anat Rec. 2019;302(12):2132–2139. doi:10.1002/ar.24209
34. Hay O, Dar G, Abbas J, et al. The Lumbar Lordosis in Males and Females. Revisited PLoS One. 2015;10(8):e133685.
35. Youdas JW, Garrett TR, Harmsen S, Suman VJ, Carey JR. Lumbar lordosis and pelvic inclination of asymptomatic adults. Phys Ther. 1996;76(10):1066–1081. doi:10.1093/ptj/76.10.1066
36. Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012;221(6):537–567. doi:10.1111/j.1469-7580.2012.01564.x
37. Cheng CH, Chen LR, Chen KH. Osteoporosis Due to Hormone Imbalance: an Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover. Int J Mol Sci. 2022;23(3):1.
38. Gordon CM, Nelson LM. Amenorrhea and bone health in adolescents and young women. Curr Opin Obstet Gynecol. 2003;15(5):377–384. doi:10.1097/00001703-200310000-00005
39. Sowers MR, Jannausch M, McConnell D, et al. Hormone Predictors of Bone Mineral Density Changes during the Menopausal Transition. J Clin Endocrinol Metab. 2006;91(4):1261–1267. doi:10.1210/jc.2005-1836
40. Gu Q, Zhao X, Lin L, Teo WP, Liu L, Yuan S. Effects of open-skill and closed-skill exercise on subthreshold depression in female adolescents: a randomized controlled trial. Int J Clin Health Psychol. 2024;24(4):100512. doi:10.1016/j.ijchp.2024.100512
41. Gao W, Ping S, Liu X. Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J Affect Disord. 2020;263:292–300. doi:10.1016/j.jad.2019.11.121
42. Stice E, Hayward C, Cameron RP, Killen JD, Taylor CB. Body-image and eating disturbances predict onset of depression among female adolescents: a longitudinal study. J Abnorm Psychol. 2000;109(3):438–444. doi:10.1037/0021-843X.109.3.438
43. Lucherini M, Hill S, Smith K. Potential for non-combustible nicotine products to reduce socioeconomic inequalities in smoking: a systematic review and synthesis of best available evidence. BMC Public Health. 2019;19(1):1469. doi:10.1186/s12889-019-7836-4
44. Luthar SS. The culture of affluence: psychological costs of material wealth. Child Dev. 2003;74(6):1581–1593. doi:10.1046/j.1467-8624.2003.00625.x
45. Shepard TY, Weil KM, Sharp TA, et al. Occasional physical inactivity combined with a high-fat diet may be important in the development and maintenance of obesity in human subjects. Am J Clin Nutr. 2001;73(4):703–708. doi:10.1093/ajcn/73.4.703
46. Ward ZJ, Long MW, Resch SC, et al. Redrawing the US Obesity Landscape: bias-Corrected Estimates of State-Specific Adult Obesity Prevalence. PLoS One. 2016;11(3):e150735. doi:10.1371/journal.pone.0150735
47. Pryce R, Kriellaars D. Central adiposity and mechanical, perceptual and physiological loading during long duration, repetitive lifting. Clin Biomech. 2018;60:170–176. doi:10.1016/j.clinbiomech.2018.10.011
48. Xiang Q, Wu Z, Zhao Y, et al. Cellular and molecular mechanisms underlying obesity in degenerative spine and joint diseases. Bone Res. 2024;12(1):71. doi:10.1038/s41413-024-00388-8
49. Wang Y, Xu Y, Tian G, Dai G. Pediatric lumbar disc herniation: a report of two cases and review of the literature. Eur J Med Res. 2022;27(1):82. doi:10.1186/s40001-022-00696-x
50. Linder R, Horenkamp-Sonntag D, Engel S, Schneider U, Verheyen F. Quality Assurance using routine data: overdiagnosis by radiological imaging for back pain. Dtsch Med Wochenschr. 2016;141(10):e96–e103. doi:10.1055/s-0042-101467
51. Cannizzaro D, Anania CD, Safa A, et al. Lumbar adjacent segment degeneration after spinal fusion surgery: a systematic review and meta-analysis. J Neurosurg Sci. 2023;67(6):740–749. doi:10.23736/S0390-5616.22.05891-X
52. Coquet J, Zammit A, Hajouji OE, et al. Changes in postoperative opioid prescribing across three diverse healthcare systems, 2010–2020. Front Digit Health. 2022;4:995497. doi:10.3389/fdgth.2022.995497
53. Chen Y, Zhong Y, Wang M, et al. Global trends and differences in the burden of alcohol use disorders attributable to childhood sexual abuse by sex, age, and socio-demographic index: findings from the Global Burden of Disease Study. Child Abuse Negl. 2019;153:106818.
54. Williams N. Education, gender, and migration in the context of social change. Soc Sci Res. 2009;38(4):883–896. doi:10.1016/j.ssresearch.2009.04.005
55. Hauser RA, Matias D, Woznica D, Rawlings B, Woldin BA. Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: a review. J Back Musculoskelet Rehabil. 2022;35(4):701–712. doi:10.3233/BMR-210097
56. Louw QA, Morris LD, Grimmer-Somers K. The prevalence of low back pain in Africa: a systematic review. BMC Musculoskelet Disord. 2007;8(1):105. doi:10.1186/1471-2474-8-105
57. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–257. doi:10.1016/S0140-6736(12)60646-1
58. Milmeister P, Rastoder M, Houssemand C. Mechanisms of Participation in Vocational Education and Training in Europe. Front Psychol. 2022;13:842307. doi:10.3389/fpsyg.2022.842307
59. Young M, Rischitelli DG. Occupational risks and risk perception among Hispanic adolescents. McGill J Med. 2006;9(1):49–53.
60. Mathew M, Doppalapudi R, Ravi J. A quantitative study on the impact of educational modules on the awareness of postural ergonomics among the dental clinical trainees of Jouf University: a North Saudi Arabian Cohort. Heliyon. 2024;10(1):e24090. doi:10.1016/j.heliyon.2024.e24090
61. Aboagye RG, Mireku DO, Nsiah JJ, et al. Prevalence and psychosocial factors associated with serious injuries among in-school adolescents in eight sub-Saharan African countries. BMC Public Health. 2022;22(1):853. doi:10.1186/s12889-022-13198-6
62. Buchbinder R, Jolley D, Wyatt M. Population based intervention to change back pain beliefs and disability: three part evaluation. BMJ. 2001;322(7301):1516–1520. doi:10.1136/bmj.322.7301.1516
63. Raspe H, Hueppe A, Neuhauser H. Back pain, a communicable disease? Int J Epidemiol. 2008;37(1):69–74. doi:10.1093/ije/dym220
64. Coggon D, Ntani G, Palmer KT, et al. The CUPID (Cultural and Psychosocial Influences on Disability) study: methods of data collection and characteristics of study sample. PLoS One. 2012;7(7):e39820. doi:10.1371/journal.pone.0039820
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Characteristics of Chronic Viral Hepatitis in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019
Ashimkhanova A, Syssoyev D, Gusmanov A, Yesmembetov K, Yespotayeva A, Abbay A, Nurpeissova A, Sarria-Santamera A, Gaipov A
Infection and Drug Resistance 2022, 15:3333-3346
Published Date: 27 June 2022
Prevalence of Primary Dysmenorrhea, Its Intensity and Associated Factors Among Female Students at High Schools of Wolaita Zone, Southern Ethiopia: Cross-Sectional Study Design
Mammo M, Alemayehu M, Ambaw G
International Journal of Women's Health 2022, 14:1569-1577
Published Date: 9 November 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Association of Triglyceride Glucose Index with Prevalence and Incidence of Diabetic Retinopathy in a Singaporean Population
Neelam K, Aung KCY, Ang K, Tavintharan S, Sum CF, Lim SC
Clinical Ophthalmology 2023, 17:445-454
Published Date: 2 February 2023
Use of Linked Nordic Registries for Population Studies in Hematologic Cancers: The Case of Multiple Myeloma
Abildgaard N, Freilich J, Anttila P, Bent-Ennakhil N, Ma Y, Lassenius M, Ørstavik S, Toppila I, Waage A, Turesson I, Hansson M
Clinical Epidemiology 2023, 15:987-999
Published Date: 18 September 2023