")
Back to Journals » Infection and Drug Resistance » Volume 18
Hemophagocytic Lymphohistiocytosis Secondary to Melioidosis in Paediatric Patients: A Case Series
Authors Wan K, Liu Y, Chen Y, Sun S, Liang H
Received 5 December 2024
Accepted for publication 6 March 2025
Published 19 March 2025 Volume 2025:18 Pages 1561—1566
DOI https://doi.org/10.2147/IDR.S505259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Kecheng Wan,* Yingjie Liu,* Yuwen Chen, Song Sun, Hong Liang
Department of Paediatrics, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), Haikou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Liang, Department of paediatrics, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), No. 19, Xiuhua Road, Xiuying District, Haikou, Hainan Province, 570311, People’s Republic of China, Tel +86 898963399, Email [email protected]
Background: Melioidosis caused by Burkholderia pseudomallei manifests as a variety of infectious symptoms. However, hemophagocytic lymphohistiocytosis (HLH) secondary to bacteraemic melioidosis is rarely documented in the literature. We report a series of fatal cases of melioidosis combined with HLH in one Chinese family.
Case Presentation: Three cases of melioidosis with HLH were reported in a family with three children, two boys aged 4 and 6 years and a 12-year-old girl. The most common clinical presentation was fever. A blood culture confirmed B. pseudomallei, and bone marrow aspiration revealed hemophagocytosis. Despite the administration of antibiotics, glucocorticoids and other treatments, all the patients died, and their deaths were attributed to HLH.
Conclusion: Melioidosis complicating HLH is rare in occurrence, but the mortality rate is high. Clinicians should be aware of the risk of a B. pseudomallei bloodstream infection in children.
Keywords: melioidosis, Burkholderia pseudomallei, hemophagocytic lymphohistiocytosis, family
Introduction
Melioidosis is an infectious disease caused by Burkholderia pseudomallei and is found predominantly in tropical climates, especially in Southeast Asia. It has recently acquired prominence in Hainan Island, China, as an emerging pathogen.1,2 Melioidosis is typically contracted through direct contact with contaminated soil or water. It can also be transmitted via inhalation or ingestion of contaminated materials. Melioidosis can have a vast array of presentations, ranging from localised infection to disseminated infection and septic shock, which could cause death. The duration of the illness can also vary from acute infection to chronic disease, and it can even remain latent for many years.3 Melioidosis can be usually identified using blood culture and automated identification systems like VITEK and MALDI-TOF. Molecular tests are used when there is misidentification or if the patient was treated with antibiotics before blood culture.
The broad clinical presentations and diagnostic difficulties related to melioidosis limit its early detection, particularly in children.4 A confirmed diagnosis requires high levels of clinical suspicion and a number of laboratory tests, including bacterial culture, serological tests, polymerase chain reaction-based tests and, more recently, rapid specific identification technologies such as gene sequencing.5
Hemophagocytic lymphohistiocytosis (HLH) is a severe inflammatory syndrome caused by the excessive activation of macrophages and T cells.6 It is a serious and life-threatening complication that can be familial or sporadic. It can be triggered by a variety of events that disrupt the immune homeostasis and is commonly triggered by viral or bacterial infections.7 Hemophagocytic syndrome secondary to melioidosis has been reported, but research has concentrated on the adult population.8–11 Recently, we identified three cases of bacteraemic melioidosis complicated by HLH in one Chinese family.
Family Report
The Chinese family in this study had three children, two boys aged 4 and 6 years and a 12-year-old girl, and lived in Hainan Island, China.
The 4-year-old boy was admitted to hospital after experiencing fever for 3 days. At admission, the patient had tachypnoea and hypotension, with a respiratory rate of 39 beats/min and a blood pressure of 57/34 mmHg. The results of the blood tests are presented in Table 1. After the collection of blood samples for culture, the patient underwent mechanical ventilation and anti-shock therapy, as well as antibiotic therapy using imipenem and cilastatin sodium (15 mg/kg, every 6 hours). The patient was treated with an injection of 10 mg/kg of methylprednisolone intravenously. Blood cultures were positive for B. pseudomallei (Table 2). The patient continued to deteriorate despite effective antibiotic therapy and died on day 1 of admission.
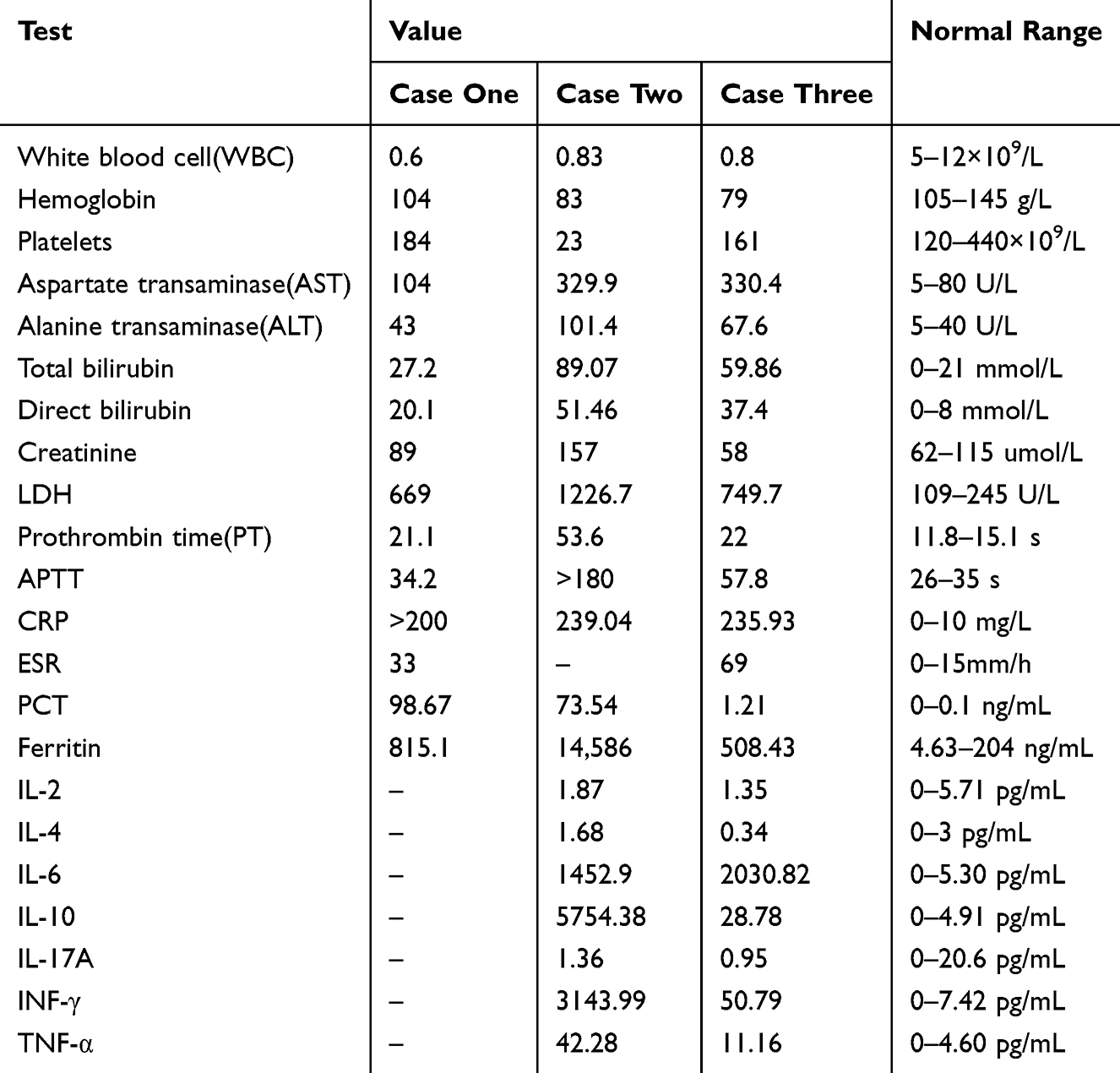 |
Table 1 Blood Investigations |
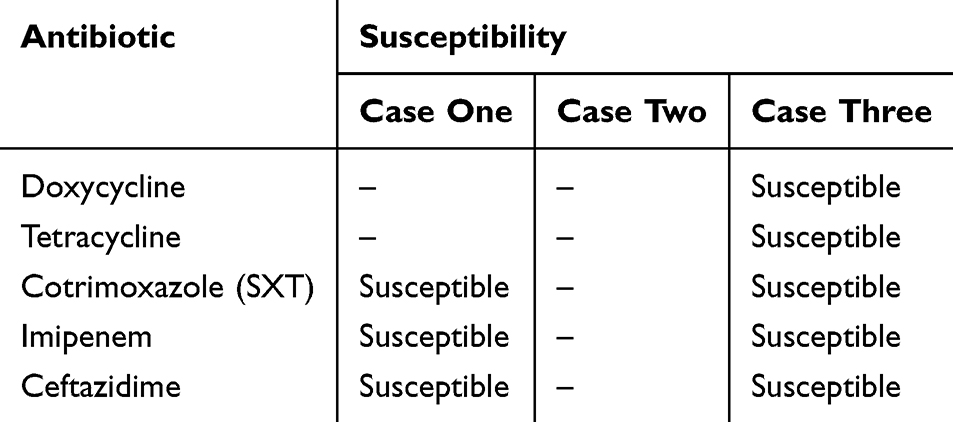 |
Table 2 Antibiotic Susceptibility Pattern for B. pseudomallei |
The daughter, a previously healthy 12-year-old, exhibited symptoms of fever for 4 days and cough for 2 days. Chest X-ray revealed extensive bilateral alveolar infiltrates in both lungs. The blood test results are presented in Table 1. Blood cultures collected on admission subsequently grew B. pseudomallei (Figure 1a and Table 2), confirming a diagnosis of melioidosis. Bone marrow aspiration revealed hemophagocytosis (Figure 1d). Therefore, the diagnosis was confirmed as septicaemic melioidosis with secondary HLH. No pathogenic variant genes were identified in a whole exome genetic test. The patient received empirical intravenous meropenem (20 mg/kg, every 6 hours) and methylprednisolone (10 mg/kg). She rapidly deteriorated and required intubation for respiratory failure. She continued to deteriorate despite ongoing antibiotic therapy and died on day 2 of admission. The cause of death was respiratory and circulatory failure caused by HLH.
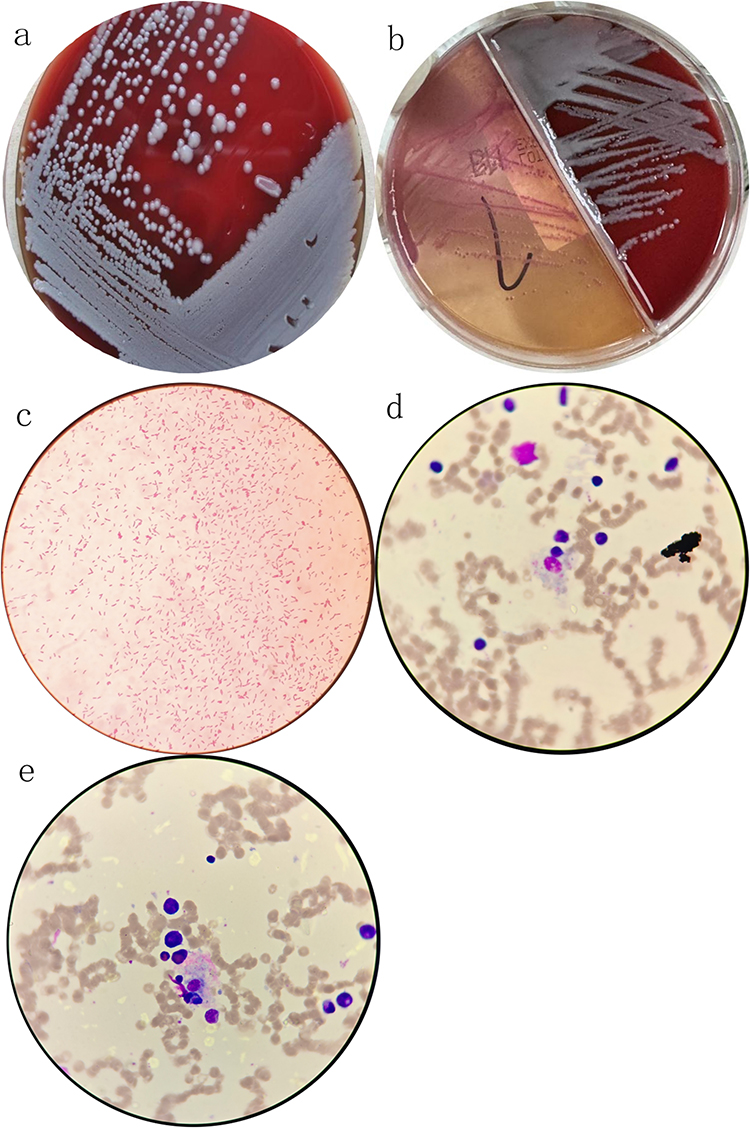 |
Figure 1 (a) Colonies of Burkholderia pseudomallei on blood agar; (b) Colonies of Burkholderia pseudomallei on MacConkey agar; (c) Gram stain of peripheral blood showing Gram-negative bacilli; (d) Bone marrow biopsy showing erythroid phagocytosis; (e) Bone marrow biopsy showing erythroid phagocytosis. |
The 6-year-old boy presented with fever for 3 days. He was admitted to hospital on 11 September 2024. The laboratory results are presented in Table 1. Chest computed tomography revealed multiple lung infiltrates with patchy areas of consolidation. The results of the bronchoalveolar lavage fluid and blood mNGS tests revealed the presence of B. pseudomallei, and blood cultures were also positive for B. pseudomallei (Figure 1b and c, Table 2), further confirming the diagnosis of melioidosis. Bone marrow aspiration revealed hemophagocytosis (Figure 1e). Therefore, the diagnosis was confirmed as septicaemic melioidosis with secondary HLH. Hemophagocytic syndrome causes respiratory failure, low blood pressure and oliguria. Despite a series of aggressive treatments, including the antibiotic meropenem (20 mg/kg, every 6 hours), mechanical ventilation, intravenous glucocorticoids (methylprednisolone, 10 mg/kg) and continuous renal replacement therapy, the patient’s condition continued to deteriorate, and he died after 1 day of treatment.
Discussion
A review of the medical literature was performed, with few culture-confirmed cases of melioidosis complicated with HLH in adults identified.12–16 Our case series adds valuable data to the literature by documenting such cases in paediatric patients.
Burkholderia pseudomallei, a Gram-negative bacterium, is the infective pathogen of melioidosis. Melioidosis is generally thought to be epidemic in the tropical and sub-tropical zone of Southern China, with Hainan Island one of the endemic areas.17 In the present study, the patients were the children of farmers living in the endemic area, but the infection route is unknown.
Melioidosis is an infectious disease involving almost every system of the body and has complicated clinical characteristics. Melioidosis complicating HLH is rare.18 A review of the medical literature was performed, with only four culture-confirmed cases of melioidosis complicated with HLH in adults identified.
Hemophagocytic lymphohistiocytosis occurs in both primary and secondary forms. Primary, or genetic, HLH presents as familial HLH syndrome. The HLH-2004 diagnostic criteria19 include the following eight criteria: (1) fever ≥38.5°C; (2) splenomegaly; (3) peripheral blood cytopenia affecting at least two cell lines (hemoglobin <90 g/L, platelets <100×109/L, neutrophils <1.0×109/L); (4) hypertriglyceridemia (fasting triglycerides ≥3.0 mmol/L) and/or hypofibrinogenemia (fibrinogen ≤1.5 g/L); (5) hemophagocytosis in bone marrow, spleen, lymph nodes, or liver; (6) low or absent NK cell activity; (7) ferritin ≥500 μg/L; and (8) elevated soluble CD25 (soluble IL-2 receptor ≥2,400 U/mL). A diagnosis of HLH can be established if five out of these eight criteria are met. In our cases, all three patients presented with persistent fever >38.5°C for 3–4 days. Laboratory findings revealed significant cytopenias, with all patients showing decreased white blood cell counts (<1.0×109/L) and thrombocytopenia (<100×109/L). Ferritin levels were markedly elevated (>10,000 μg/L in all cases), far exceeding the diagnostic threshold. Hepatosplenomegaly was consistently observed in all three cases through physical examination and imaging studies. Bone marrow examination confirmed the presence of hemophagocytosis in all patients. While NK cell activity and soluble CD25 levels were not assessed due to the rapid progression of disease, the presence of five diagnostic criteria was sufficient to confirm the diagnosis of HLH in all three cases. In the present study, genetic tests on the daughter and her parents did not reveal any genes associated with primary hemophagocytic syndrome.
Hemophagocytic lymphohistiocytosis can be triggered by conditions that disrupt immune homeostasis, such as infections, autoimmune diseases and malignancy. Viral infections are the most common triggers for HLH, such as Epstein–Barr virus, cytomegalovirus, parvovirus and herpes simplex virus.20 Herein, we report a rare bacterial infection triggering this serious complication. The three cases in this study are the first reported cases of paediatric patients that developed HLH secondary to melioidosis.
Hemophagocytic lymphohistiocytosis is a life-threatening complication that is associated with excessive immune activation and is common in children. In this study, interleukin (IL)-6, IL-10, and INF-γ in peripheral blood were significantly elevated, suggesting a cytokine storm that may have contributed to the development of hepatitis, coagulopathy, liver failure, central nervous system involvement, multi-organ failure, and other manifestations. The syndrome has a high mortality rate.21 To inhibit cytokine expression and suppress the excessive immune response, methylprednisolone at a dose of 10 mg/kg was used as an immunosuppressive agent. Unfortunately, even after vigorous rescue, our patients eventually died. The cause of death was multiple organ failure caused by HLH. HLH triggered by bacterial infections, such as melioidosis, involves dysregulation of cytokine pathways, leading to uncontrolled immune activation. This process is characterized by the overproduction of pro-inflammatory cytokines, including IL-6, IL-10, and INF-γ, which drive the pathogenesis of HLH.22 Early recognition and intervention are critical in managing these cases.
In addition to the cases documented in this study, HLH has been reported in various contexts, including as a complication of gene therapy. For instance, Galletta et al reported a case of HLH following gene replacement therapy in a child with type 1 spinal muscular atrophy.22 This highlights the diverse triggers and presentations of HLH, emphasizing the need for a comprehensive approach to diagnosis and treatment.
These cases illustrate the varied presentation of secondary HLH and highlight the importance of early diagnosis and treatment of the underlying aetiology. In summary, to the best of our knowledge, this is the first report of HLH secondary to B. pseudomallei infection in children. Hemophagocytic lymphohistiocytosis is a serious complication of melioidosis and can lead to high mortality rates. Paediatricians in endemic areas should be vigilant for signs of melioidosis and HLH, especially in children presenting with fever, hepatosplenomegaly, and cytopenia. Early diagnostic measures, such as blood cultures and bone marrow aspiration, are essential. Treatment protocols should include aggressive antimicrobial therapy, immunosuppressive agents, and supportive care to manage multi-organ failure. We recommend heightened vigilance and specific diagnostic protocols for clinicians in endemic regions to improve outcomes in these patients.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University) (Approval No. YLY [2024] 568).
Written informed consent was obtained from the legal guardians.
Consent for Publication
Written informed consent for publication was obtained from the legal guardians.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chewapreecha C, Holden MT, Vehkala M, et al. Global and regional dissemination and evolution of Burkholderia pseudomallei. Nat Microbiol. 2017;2(4):16263. doi:10.1038/nmicrobiol.2016.263
2. Wang Y, Li X, Li A, et al. The genetic diversity and evolution analysis of the Hainan melioidosis outbreak strains. Infect Genet Evol. 2024;123:105654. doi:10.1016/j.meegid.2024.105654
3. Meumann EM, Limmathurotsakul D, Dunachie SJ, et al. Burkholderia pseudomallei and melioidosis. Nat Rev Microbiol. 2024;22(3):155–169. doi:10.1038/s41579-023-00972-5
4. Jarrett O, Seng S, Fitzgerald DA. Paediatric melioidosis. Paediatr Respir Rev. 2024;50:31–37. Epub 2023 Nov 24. PMID: 38245464. doi:10.1016/j.prrv.2023.11.002.
5. Currie BJ. Melioidosis and Burkholderia pseudomallei: progress in epidemiology, diagnosis, treatment and vaccination. Curr Opin Infect Dis. 2022;35(6):517–523. doi:10.1097/QCO.0000000000000869
6. Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: an update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. 2020;34(4):101515. doi:10.1016/j.berh.2020.101515
7. Liu L, Cui Y, Zhou Q, et al. Hemophagocytic lymphohistiocytosis during pregnancy: a review of the literature in epidemiology, pathogenesis, diagnosis and treatment. Orphanet J Rare Dis. 2021;16(1):281. doi:10.1186/s13023-021-01790-9
8. Beig J, Read K, Welch D, et al. Melioidosis with possible Haemophagocytic lymphohistiocytosis. N Z Med J. 2017;130(1456):76–79.
9. Smith S, Munas AM, Hanson J. Hemophagocytic lymphohistiocytosis complicating melioidosis. Am J Trop Med Hyg. 2018;99(3):557–558. doi:10.4269/ajtmh.18-0331
10. Devi S, Dash A, Dey A, et al. Hemophagocytic lymphohistiocytosis complicating septicemic melioidosis: a case report. J Infect Chemother. 2024;31(1):102423. Epub ahead of print. doi:10.1016/j.jiac.2024.05.003.
11. Bojanapati K, Gohil R, Siddem C, et al. Whitmore’s disease: a case report of melioidosis triggering Hemophagocytic lymphohistiocytosis. Cureus. 2024;16(8):e65948. doi:10.7759/cureus.65948
12. Tan G, Liu Y, Wang J, et al. Clinical characteristics and outcomes of melioidosis in children: a 10-year retrospective study from southern China. J Infect Public Health. 2023;16(2):286–292. doi:10.1016/j.jiph.2022.12.022
13. Kumar N, Chaudhary D, Kandel R, et al. Pediatric Hemophagocytic lymphohistiocytosis secondary to bacterial infections: a systematic review. Pediatr Blood Cancer. 2023;70(12):e30448. doi:10.1002/pbc.30448
14. Chen Y, Feng W, Li B, et al. Emergence and molecular characterization of melioidosis in children from Hainan, China: a retrospective study. Front Cell Infect Microbiol. 2023;13:1172161. doi:10.3389/fcimb.2023.1172161
15. Wang H, Wu Y, Xu X, et al. Infection-associated hemophagocytic lymphohistiocytosis in children: clinical features and treatment outcomes of 85 cases from a single center. Pediatr Hematol Oncol. 2023;40(8):943–955. doi:10.1080/08880018.2023.2206643
16. Lin H, Li M, Chen L, et al. Clinical and molecular epidemiology of melioidosis in children from Hainan Province, China, 2019–2023. Emerg Microbes Infect. 2024;13(1):2289891. doi:10.1080/22221751.2024.2289891
17. Zheng X, Xia Q, Xia L, et al. Endemic melioidosis in Southern China: past and present. Trop Med Infect Dis. 2019;4(1):39. doi:10.3390/tropicalmed4010039
18. Chakravorty A, Heath CH. Melioidosis: an updated review. Aust J Gen Pract. 2019;48(5):327–332. doi:10.31128/AJGP-04-18-4558
19. Henter JI, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.21039
20. Xu XJ, Wang HS, Ju XL, et al. Clinical presentation and outcome of pediatric patients with hemophagocytic lymphohistiocytosis in China: a retrospective multicenter study. Pediatr Blood Cancer. 2017;64(4):e26264. doi:10.1002/pbc.26264
21. Canna SW, Marsh RA. Pediatric hemophagocytic lymphohistiocytosis. Blood. 2020;135(16):1332–1343. doi:10.1182/blood.2019000936
22. Galletta F, Cucinotta U, Marseglia L, et al. Hemophagocytic lymphohistiocytosis following gene replacement therapy in a child with type 1 spinal muscular atrophy. J Clin Pharm Ther. 2022;47(9):1478–1481. doi:10.1111/jcpt.13733
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.