")
Back to Journals » Research and Reports in Tropical Medicine » Volume 15
HHV8-Associated Multicentric Castleman Disease: A Case Report on a Rare Complication of HIV in a Low-Income Setting
Authors Ground M , Veenendaal T, Chiluzi DR, Nkhonjera G, Glas AC, Glas-van Dijk L
Received 25 July 2024
Accepted for publication 10 October 2024
Published 15 October 2024 Volume 2024:15 Pages 91—97
DOI https://doi.org/10.2147/RRTM.S483426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario A. Rodríguez-Pérez
Marcus Ground,1 Thijmen Veenendaal,1 Daniel Rexie Chiluzi,1 Geoffrey Nkhonjera,2 Arie C Glas,1 Lisanne Glas-van Dijk1
1Mulanje Mission Hospital, Mulanje, Malawi; 2Oncology Department, Queen Elizabeth Central Hospital, Blantyre, Malawi
Correspondence: Marcus Ground, Email [email protected]
Abstract: We present the case of an HIV-positive man diagnosed with multicentric Castleman disease (MCD) associated with human herpesvirus 8 (HHV8) infection, complicated by renal failure. This subtype of an otherwise rare disease is a complication of HIV and HHV8 infection. The diagnosis and management of HHV8-MCD in the developing world is challenging—in part due to its rarity, but largely due to the limited access to histology and other laboratory services. Our case presented with a confusing constellation of symptoms and was diagnosed with MCD on histology. Here we discuss the epidemiology, pathogenesis, diagnosis, and treatment of HHV8-MCD in the context of HIV infection in a resource-limited setting, in the hope that greater awareness will lead to more prompt recognition.
Keywords: Castleman disease, HIV, lymphoproliferative disorders, case report, human herpesvirus 8
Introduction
Castleman disease (CD) is a group of rare lymphoproliferative disorders that vary in severity and cause. Unifocal CD is a benign condition that presents in a single lymph node, typically in the mediastinum, and is of unknown etiology.1 Multifocal CD (MCD) arises in many lymph nodes and is accompanied by a constellation of other symptoms depending on the cause. MCD can be associated with human herpesvirus 8 (HHV8, also called Kaposi sarcoma herpesvirus 8, KSHV) or arise idiopathically (iMCD). The HHV8-associated subtype is the most common form in Malawi, where levels of HIV and HHV8 in the community are high.2
Epidemiological studies of this HHV8-MCD are lacking, especially in sub-Saharan Africa, where the prevalence of HHV8 is the highest,3 and access to diagnostic pathology is often limited.2 In developed nations, where HIV rates are low, incidence of MCD is estimated to be between 1 in 5 million to 1 in 25 million person years,1 with HHV8-MCD representing less than 1% of cases.3
Incidence of HHV8-MCD appears to be increasing proportionally to antiretroviral therapy (ART) coverage, particularly highly active ART (HAART).4 This stands in stark opposition to the observed decrease in the incidence of other HIV-associated lymphoproliferative disorders such as Kaposi sarcoma5 and non-Hodgkin lymphoma,6 which reliably fall in both incidence and prevalence with the introduction of ART. A cohort study from the United Kingdom showed a dramatic increase in incidence of HHV8-MCD from 0.58 cases per 10,000 patient-years in the pre-HAART era to 8.3 in the later HAART era. In the same period, the incidence of Kaposi sarcoma fell from 520 to 63.2.4 Similar case reports demonstrate rising numbers of MCD in HIV-positive patients in both developed7 and developing nations,8 and some authors have suggested a causal link between ART coverage and the increase in incidence—namely that HHV8-MCD could be an outcome of immune reconstitution inflammatory syndrome.9
The pathogenesis of HHV8-MCD usually involves infection with both HIV and HHV8.10 Uncontrolled proliferation of HHV8 in the lymph nodes of immunocompromised people results in the transcription of a viral homologue of interleukin-6 (IL-6). This stimulates other lymphoid cells to secrete vascular endothelial growth factor (VEGF), which promotes angiogenesis and further release of IL-6, culminating in the “multicentric angiofollicular hyperplasia” of lymphoid tissue and elevated risk of malignant transformation. This IL-6 mediation is the very same mechanism behind the development of Kaposi sarcoma from the lymphatic endothelium.1
Common signs of HHV8-MCD include fever, peripheral lymphadenopathy, splenomegaly, and Kaposi sarcoma.11 Laboratory abnormalities include an elevated CRP, derangement of liver and renal function tests, and indications of autoimmune hemolytic anemia.10
The mainstay of treatment for any MCD is rituximab, usually in a 4-week regimen.12,13 However, for patients with concomitant end-organ damage or extensive Kaposi sarcoma, then the addition of a chemotherapy agent such as doxorubicin or etoposide is recommended.1,13 Prognosis for those in settings with access to rituximab is good: 5-year survival rates for patients on rituximab-only or rituximab-etoposide combination therapy approaches 90%.11,13
Case Report
Our mission hospital serves approximately 650,000 people in Mulanje and surrounding districts in Southern Malawi. The prevalence of HIV in our area is 15.6%—significantly higher than the incidence for the Southwestern region (13.3%) and higher still than the Malawian national average (8–9%). Access to free antiretroviral therapy (ART) since 2004 and good levels of adherence have effected a substantial reduction in transmission and mortality from the virus.14,15
A 45-year-old HIV-positive man presented to our hospital with a weeklong history of shortness of breath, productive cough, and fever. He was diagnosed with HIV-1 in 2010 and had been receiving efavirenz/lamivudine/tenofovir until 2019, when he was switched to tenofovir/lamivudine/dolutegravir, according to Malawi standard policy. He also had a recent background of extrapulmonary tuberculosis, diagnosed at another center by positive urine lipoarabinomannan (LAM) and pericardial effusion on ultrasound. He was on his 3rd month of tuberculosis treatment.
On examination, he was pale, febrile at 38.1°C, tachycardic at 114 beats per minute, and hypotensive (88/56 mmHg). He had palpable lymphadenopathy in the posterior cervical region, bilaterally, measuring approximately 3x2cm and 1×1 cm. The nodes were mobile, non-tender, and rubbery. He was mildly tender in the epigastrium and had splenomegaly palpable at 8 cm below the costal margin. Laboratory abnormalities included a microcytic anemia, renal failure, hyperbilirubinemia and elevated total protein. Laboratory results are presented in Table 1. His viral load was undetectable, and his CD4 count was 219. A chest x-ray showed bilateral hilar lymphadenopathy and an obscured right cardiac border (Figure 1). An ultrasound showed hepatomegaly of 8cm, mild splenomegaly of 14.4cm, slight pericardial effusion, left-sided pleural effusion, and increased renal echogenicity. There was no free fluid in the peritoneum. A sputum smear showed no acid-fast bacilli and GeneXpert for TB was also negative. Urine LAM was not repeated because it was previously positive. The differential diagnosis for this patient was lymphoma or TB lymphadenitis, and a lymph node biopsy was performed.
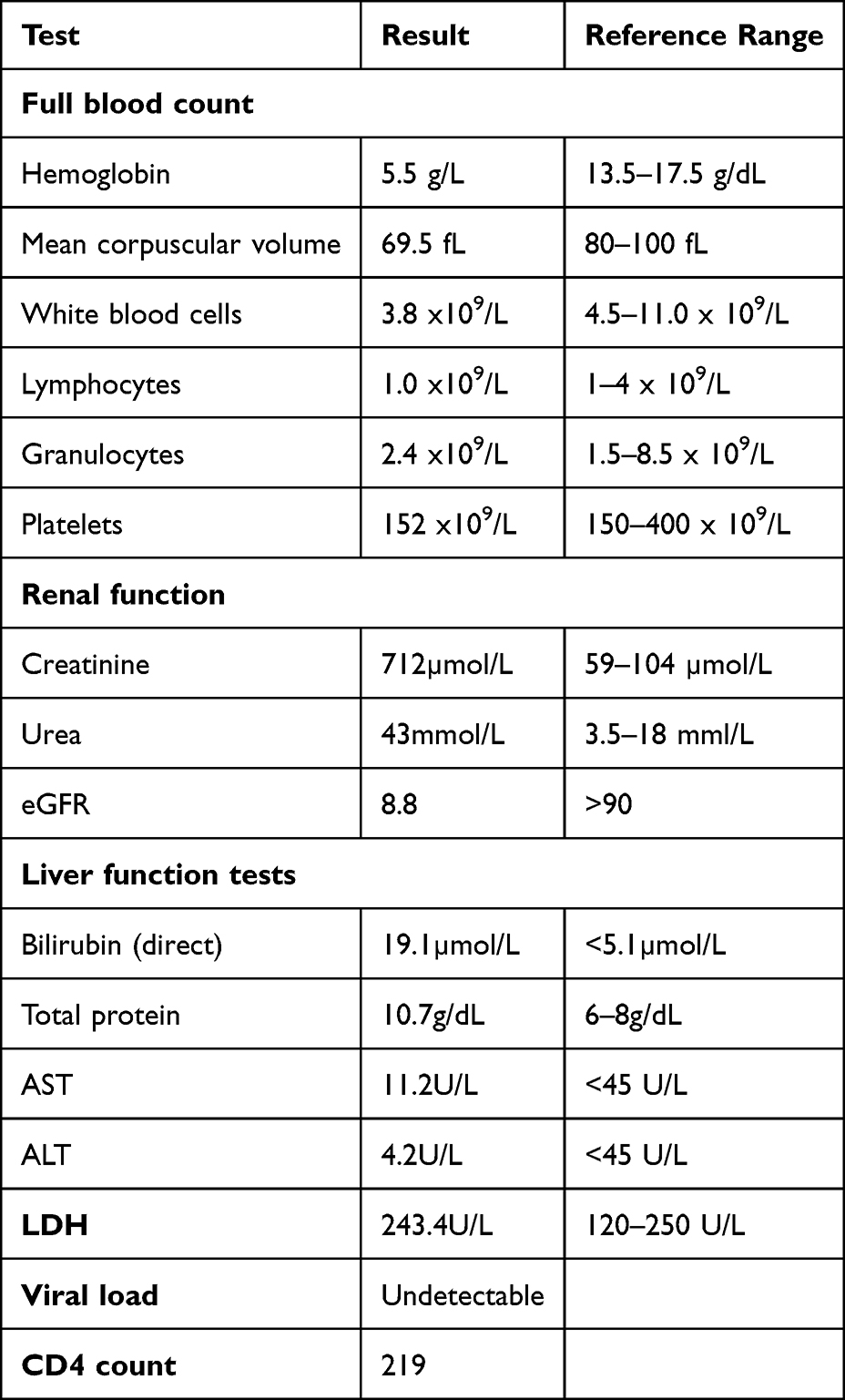 |
Table 1 Full Blood Count and Renal Function Tests at the Time of Admission |
 |
Figure 1 Chest x-ray on admission showing bilateral hilar lymphadenopathy. |
While awaiting biopsy results, the patient developed confusion and a decreasing level of consciousness. Differential diagnoses of his confusion included cryptococcal and tuberculous meningitis, acute bacterial meningitis and HIV-associated or uremic encephalopathy. A lumbar puncture was performed and ruled out bacterial, cryptococcal and tuberculous meningitis (WBC negative, RBC negative, no organisms seen on Gram stain, glucose 110mg/dL, protein negative, no cryptococci seen on Indian ink, AFB negative, cryptococcal antigen negative). Meanwhile, the patient developed an oxygen requirement and was started on 5L/min via nasal prongs. The hypoxia was likely caused by the anemia and additional kidney failure. The new confusion was ascribed to uremic encephalopathy.
Given the probability that the renal injury was related to tenofovir DF toxicity, his ART regimen was changed to abacavir/lamivudine/dolutegravir in line with local HIV treatment guidelines and over the next 17 days, the creatinine fell to 336µmol/L (eGFR 21.0). The patient received a total of 5 units of blood to address the anemia.
Biopsy results were returned as MCD—with the pathologist noting the characteristic “onion skin” appearance. His confusion and respiratory symptoms abated, and he was able to be discharged. Unfortunately, access to rituximab—the core of pharmacological therapy for MCD—is limited in Malawi. Nonetheless, the patient was referred to the oncology unit at a tertiary center where he received one cycle of cyclophosphamide, vincristine sulphate, and prednisone (CVP), and two cycles of cyclophosphamide, doxorubicin hydrochloride, vincristine sulphate, and prednisone (CHOP) at three weekly intervals. At follow-up, a left ventricular wall abnormality was noted on cardiac echo (ejection fraction 48%), and so doxorubicin was omitted from subsequent cycles. At the time of writing (5 months after index admission), the patient is doing well, and most of the involved lymph nodes have regressed.
Discussion
This case presented a diagnostic challenge; primarily due to the rarity of MCD, partly due to the confounding influence of the uremic encephalopathy on the diagnostic process, and also due to the reduced availability of diagnostic tests in our region.
The diagnostic challenge in this case first required the elimination of non-lymphoproliferative disorders from the differential, such as TB lymphadenitis. Given our patient was known to have extrapulmonary TB, the normal “rule out” diagnostics (such as urine LAM) were unlikely to be useful. The clue may lie in the pattern of lymphadenopathy: TB lymphadenitis is more likely to present unilaterally (often a single node),16 while HHV8-MCD and the other HIV-associated lymphoproliferative disorders are more often present bilaterally, involving multiple nodes.17
The second challenge was determining which lymphoproliferative disorder was responsible for the presentation, considering the HIV status of the patient, his viral load, and CD4 count. The diagnosis of any MCD in an HIV-positive individual should be performed alongside the exclusion of other lymphoproliferative disorders, such as Hodgkin and non-Hodgkin lymphoma (NHL), which can present very similarly. Incidence of NHL incidence rises proportionately to increasing viral load, and fall proportionally with increasing CD4 count,6 while the effect of viral load and CD4 count on the incidence of Hodgkin lymphoma appears weaker.18 Interestingly, HHV8-MCD incidence increases with CD4 count and falls with viral load4—perhaps serving as a clue in the diagnosis of our case, whose CD4 count was 219 and his viral load was undetectable.
To distinguish definitively between these HIV-associated lymphoproliferative disorders, an excisional lymph node biopsy was required. Histopathologically, HHV8-MCD is of the “plasma cell type” of Castleman disease, in which the lymph node germinal center displays hyperplasticity, and the mantle zone shows concentric rings of small plasmacytes, giving an “onion skin” appearance.1,13 In addition, immunohistochemistry staining of the lymph node for HHV8’s latency-associated nuclear antigen (LANA) protein will be positive.
Traditionally, diagnosis of HHV8-MCD required fulfilment of one of two diagnostic criteria: the first devised by the National Cancer Institute (NCI) in 2004,19 and the second by the French Agence Nationale de Recherche sur le SIDA (ANRS) in 200712 (see Table 2, where asterisks have been placed next to each criterion that our patient met).
 |
Table 2 A Comparison of the Diagnostic Criteria for HHV8-MCD (Adapted from20). Criteria Met by Our Patient are Denoted with * |
Reliance on laboratory values such as CRP to form a diagnosis may prove difficult in low-income settings such as ours. Our case met the clinical and laboratory criteria of the NCI, and both clinical criteria of the ANRS, but failed to meet either criteria in totality, as we are unable to measure CRP at our hospital. Bower et al applied the two diagnostic criteria to a case series of 75 patients with HIV-associated MCD and found the specificity of the NCI and ANRS criteria to be 92% and 81%, respectively. The authors suggest that rather than relying on the “cumbersome” criteria, a simple triad of ‘histopathological findings, detectable plasma HHV-8, and B symptoms’ is adequate.20 Furthermore, while CRP is sensitive,21 it has been shown by small case series to be non-specific for HHV8-MCD.22,23 HHV-8 serological testing appears to be available in our region, albeit in a research capacity;24 to our knowledge HHV-8 testing is not used clinically. Serological testing may be precluded by cost and access to polymerase chain reaction (PCR) infrastructure. Instead, researchers in resource-limited settings have found that the addition of HHV8’s LANA to the immunohistochemical staining panel for biopsies of lesions suspicious for Kaposi sarcoma (a related HHV-8 associated pathology) is a cost-effective measure.25 Both HHV8 serology and LANA staining are highly sensitive but have the drawback of poor specificity in regions where HHV8 prevalence is high.26 Our case suggests that expanded use of either HHV-8 serological testing or LANA immunohistochemical staining may be warranted in regions like ours.
Histopathology may present a challenge in resource-limited settings such as Sub-Saharan Africa. While access to these services in our region—Malawi—is present, turnaround times are often slow,27 and the expertise is centered around more common cancers,28 rather than rarer diagnoses such as MCD. One recent study sought to improve histopathological diagnosis of lymphoproliferative disorders; Montgomery et al set up a targeted pathology laboratory in Lilongwe, staffed by Malawian pathologists, and using a small number of readily available immunohistochemical stains demonstrated excellent diagnostic concordance (>95%) with independent analysis in a high income setting (United States).29 This research demonstrates that low-income countries such as Malawi can cheaply and effectively utilize histopathology for rapid diagnosis of lymphoproliferative disorders such as MCD. Our case further supports this notion—the histopathological diagnosis was made within 2 weeks of presentation to our hospital.
Ideally, this patient would have received rituximab. In areas such as ours, where access to rituximab is limited, prognosis is poor. In a small Malawian case series published by Gopal et al, all 6 patients with MCD had died within 6 months of diagnosis.30 These patients were either untreated or received systemic chemotherapy.
This case highlights the challenges faced by patients and carers concerning complications associated with advanced HIV in Malawi. With increasing ART coverage, clinicians in Sub-Saharan Africa can expect to see increasing numbers of patients with HHV8-MCD. However, this case demonstrates that effective diagnosis is possible in low-income setting: the definitive diagnosis in our case required only histological analysis of a lymph node biopsy and was made within two weeks of presentation. We suggest that clinicians working in settings like ours need not despair at a lack of available blood tests, as our case demonstrates that a diagnosis can be made without conforming to the established diagnostic criteria. We advocate for further work to be undertaken to improve access to diagnosis and treatment for rare HIV complications that are common in low-income countries.
Data Sharing Statement
All data related to the case is presented in the manuscript.
Ethical Approval
Ethical approval was not required for this case report.
Consent to Publish
Consent to publish was gained from the patient, in writing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Carbone A, Borok M, Damania B, et al. Castleman disease. Nat Rev Dis Primer. 2021;7(1). doi:10.1038/s41572-021-00317-7
2. Gopal S, Fedoriw Y, Montgomery ND, et al. Multicentric Castleman’s disease in Malawi. Lancet. 2014;384(9948):1158. doi:10.1016/S0140-6736(14)61366-0
3. Simpson D. Epidemiology of Castleman Disease. Hematol Oncol Clin North Am. 2018;32(1):1–10. doi:10.1016/j.hoc.2017.09.001
4. Powles T, Stebbing J, Bazeos A, et al. The role of immune suppression and HHV-8 in the increasing incidence of HIV-associated multicentric Castleman’s disease. Ann Oncol. 2009;20(4):775–779. doi:10.1093/annonc/mdn697
5. Liu Z, Fang Q, Zuo J, Minhas V, Wood C, Zhang T. The world‐wide incidence of Kaposi’s sarcoma in the
6. Bohlius J, Schmidlin K, Costagliola D, et al. Incidence and risk factors of HIV-related non-Hodgkin’s lymphoma in the era of combination antiretroviral therapy: a European multicohort study. Antivir Ther. 2009;14(8):1065–1074. doi:10.3851/IMP1462
7. Katchanov J, Zimmermann U, Branding G, Arastéh K, Müller M. HIV-associated multicentric Castleman’s disease after initiation of antiretroviral therapy: experience of a European centre. Infection. 2014;42(4):791–793. doi:10.1007/s15010-014-0605-5
8. Mmusi LM Castleman’s disease at Chris Hani Baragwanath Academic Hospital - a retrospective study. University of Witwatersrand; 2018. Available from: https://wiredspace.wits.ac.za/server/api/core/bitstreams/e4ef28af-be3c-438f-8ea3-a940a1e9c53a/content.
9. Tarrant TK,ed..Rare Rheumatic Diseases of Immunologic Dysregulation.Springer International Publishing;2019. doi:10.1007/978-3-319-99139-9
10. Dispenzieri A. Castleman disease. Cancer Treat Res. 2008;142:293–330. doi:10.1007/978-0-387-73744-7_13
11. Bower M, Newsom-Davis T, Naresh K, et al. Clinical features and outcome in HIV-associated multicentric Castleman’s disease. J Clin Oncol. 2011;29(18):2481–2486. doi:10.1200/JCO.2010.34.1909
12. Gérard L, Bérezné A, Galicier L, et al. Prospective study of rituximab in chemotherapy-dependent human immunodeficiency virus associated multicentric Castleman’s disease: ANRS 117 CastlemaB Trial. J Clin Oncol off J Am Soc Clin Oncol. 2007;25(22):3350–3356. doi:10.1200/JCO.2007.10.6732
13. Dispenzieri A, Fajgenbaum DC. Overview of Castleman disease. Blood. 2020;135(16):1353–1364. doi:10.1182/BLOOD.2019000931
14. Wolock TM, Flaxman S, Chimpandule T, et al. Subnational HIV incidence trends in Malawi: large, heterogeneous declines across space. medRxiv. 2023;4:2023. doi:10.1101/2023.02.02.23285334
15. Ministry of Health (MOH), Malawi. The Malawi Population-Based HIV Impact Assessment 2020–2021. Malawi: Ministry of Health (MOH); 2022. https://phia.icap.columbia.edu/wp-content/uploads/2022/12/241122_Mphia_Foreword.pdf.
16. Agarwal AK, Sethi A, Sethi D, Malhotra V, Singal S. Tubercular cervical adenitis: clinicopathologic analysis of 180 cases. J Otolaryngol. 2009;38(5):521–525.
17. Storck K, Brandstetter M, Keller U, Knopf A. Clinical presentation and characteristics of lymphoma in the head and neck region. Head Face Med. 2019;15(1):1. doi:10.1186/s13005-018-0186-0
18. Fagundes RBC, Delgado de Mederios LG, Barros de Souza AT, et al. Impact of the HIV infection in Hodgkin lymphoma individuals: a protocol for systematic review and meta analysis. Medicine. 2022;101(39):e30765. doi:10.1097/MD.0000000000030765
19. Robert Cronin Yung Peng, Rose Khavari ND. Recent advances in Kaposi sarcoma herpesvirus-associated multicentric Castleman disease. Physiol Behav. 2017;176(3):139–148. doi:10.1097/CCO.0b013e328355e0f3
20. Bower M, Pria AD, Coyle C, Nelson M, Naresh K. Diagnostic criteria schemes for multicentric Castleman disease in 75 cases. J Acquir Immune Defic Syndr. 2014;65(2):2013–2015. doi:10.1097/QAI.0b013e3182a8338f
21. Fajgenbaum DC, Uldrick TS, Bagg A, et al. International, evidence-based consensus diagnostic criteria for HHV-8–negative/idiopathic multicentric Castleman disease. Blood. 2017;129(12):1646–1657. doi:10.1182/blood-2016-10-746933
22. Pribyl K, Vakayil V, Farooqi N, et al. Castleman disease: a single-center case series. Int J Surg Case Rep. 2021;80:105650. doi:10.1016/j.ijscr.2021.105650
23. Hu C, Zou Y, Pan J, et al. Analysis of clinical characteristics, pathological changes and changes of interleukin-6 (IL-6) and C-Reactive Protein (CRP) in children with Castleman’s disease. Med Sci Monit Int Med J Exp Clin Res. 2020;26:e924783–1–e924783–6. doi:10.12659/MSM.924783
24. Desantis SM, Pau Pong C, Archibald LK, et al. Demographic and immune correlates of human herpesvirus 8 seropositivity in Malawi, Africa. Int J Infect Dis. 2002;6(4):266–271. doi:10.1016/S1201-9712(02)90159-1
25. Speicher DJ, Wanzala P, D’Lima M, et al. Diagnostic challenges of oral and cutaneous Kaposi’s sarcoma in resource-constrained settings. J Oral Pathol Med. 2015;44(10):842–849. doi:10.1111/jop.12315
26. Mwakigonja AR, Pyakurel P, Kokhaei P, et al. Human herpesvirus-8 (HHV-8) sero-detection and HIV association in Kaposi’s sarcoma (KS), non-KS tumors and non-neoplastic conditions. Infect Agent Cancer. 2008;3(1):10. doi:10.1186/1750-9378-3-10
27. Masamba LPL, Mtonga PE, Kalilani Phiri L, Bychkovsky BL. Cancer pathology turnaround time at Queen Elizabeth Central Hospital, the largest referral center in Malawi for oncology patients. J Glob Oncol. 2017;3(6):734–739. doi:10.1200/JGO.2015.000257
28. Kachimanga C. Evaluating the use of pathology in improving diagnosis in rural Malawi. Malawi Med J. 2018;30(3):162. doi:10.4314/mmj.v30i3.6
29. Montgomery ND, Liomba NG, Kampani C, et al. Accurate real-time diagnosis of lymphoproliferative disorders in Malawi through clinicopathologic teleconferences: a model for pathology services in Sub-Saharan Africa. Am J Clin Pathol. 2016;146(4):423–430. doi:10.1093/ajcp/aqw118
30. Gopal S, Liomba NG, Montgomery ND, et al. Characteristics and survival for HIV-associated multicentric Castleman disease in Malawi. J Int AIDS Soc. 2015;18(1):1–6. doi:10.7448/IAS.18.1.20122
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
HIV-Associated Mycobacterium Avium Complex, Oral Candida, and SARS-CoV-2 Co-Infection: A Rare Case Report
Ding X, Ma X, Xu Y, Xu L
Infection and Drug Resistance 2022, 15:7037-7042
Published Date: 2 December 2022
Optimizing Type 2 Diabetes Management in a Medically Complex Patient: A Case Report of a Patient with Type 2 Diabetes and HIV
Kabakambira JD, Kong JM
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2401-2406
Published Date: 11 August 2023