")
Back to Journals » Journal of Pain Research » Volume 18
High Prevalence of Small-Fiber Neuropathy in Patients with Tarlov Cysts: Toward a More Comprehensive Clinical Understanding
Authors Hulens M , Zajonc P, Bruyninckx F , Rasschaert R , De Mulder P , Bervoets C , Dankaerts W
Received 23 January 2025
Accepted for publication 15 April 2025
Published 30 April 2025 Volume 2025:18 Pages 2241—2263
DOI https://doi.org/10.2147/JPR.S513705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Mieke Hulens,1 Peter Zajonc,2 Frans Bruyninckx,3 Ricky Rasschaert,4 Peter De Mulder,5 Chris Bervoets,6– 8 Wim Dankaerts1
1Department of Rehabilitation Sciences, Musculoskeletal Rehabilitation Research Unit, Faculty of Kinesiology and Rehabilitation Sciences, University of Leuven, Leuven, Belgium; 2Pinpoint Targeting, LLC, New York City, NY, USA; 3Department of Physical Medicine & Rehabilitation, University Hospitals of Leuven, Leuven, Belgium; 4Department of Neurosurgery, AZ Rivierenland, Bornem, Belgium; 5Department of Anesthesiology and Pain Therapy, Imelda Hospital, Bonheiden, Belgium; 6Department of Neurosciences, KU Leuven, Leuven, Belgium; 7Department of Ophthalmology, University Hospitals of Leuven, Leuven, Belgium; 8Department Adult Psychiatry, University Psychiatric Center of KU Leuven, Leuven, Belgium
Correspondence: Mieke Hulens, Department of Rehabilitation Sciences, KU Leuven, Overwegstraat 14, 3051 Sint-Joris-Weert, Leuven, Belgium, Tel +32 477 338003, Fax +32 16 329197, Email [email protected]
Purpose: To explore the prevalence of small-fiber neuropathy (SFN) and the clinical characteristics of patients with Tarlov cysts (PTCs), focusing on symptoms related to SFN and increased cerebrospinal pressure.
Patients and Methods: In this retrospective study, 126 surveys assessing symptoms in women (30– 69 years) with Tarlov cysts (TCs) ≥ 7 mm seeking treatment for chronic back, pelvic or leg pain and skin biopsy results from 75 patients assessing intraepidermal nerve fiber density (IENFD) were reviewed.
Results: IENFD < 5th percentile was documented in 80% of PTCs according to the normative reference data of Collongues et al and 72% according to the worldwide dataset of Lauria et al Questionnaires revealed high incidences of neuropathic pain (80%), allodynia (76%), pain while sitting (93%), anal sphincter (11%) and urinary sphincter (66%) problems, persistent genital arousal (27%), and restless legs (54%). Autonomic dysfunctions included early satiety (41%), bladder (93%) and bowel (88%) dysfunction, increased sweating (51%), and Raynaud’s phenomenon (45%). Other symptoms potentially associated with increased cerebrospinal fluid pressure (CSFP) were headaches (57%), fatigue (86%), cognitive issues (86%), and pulsatile tinnitus (59%).
Conclusion: This study revealed a high prevalence of SFN in PTCs (72– 80%). Although the TCs may not cause radicular pain in the corresponding dermatomes directly, individuals with TCs frequently report a range of symptoms that have previously been linked to symptomatic TCs, including bladder, bowel, sphincter, and sexual symptoms, as well as local pain. Additionally, seemingly unrelated symptoms, such as headaches, fatigue, cognitive difficulties, neuropathic pain localized in other parts of the body, and autonomic dysfunctions, are commonly reported. These symptoms may be associated with elevated CSFP within the nerve root sheath. Elevated pulsatile CSFP underlies the formation of TCs at the dorsal root ganglion and may gradually contribute to small-fiber dysfunction by irritating, compressing and damaging small nerve fibers within the dorsal root ganglion.
Plain Language Summary: Purpose: This study focused on how common small-fiber neuropathy (SFN) is in patients with Tarlov cysts (TCs) and examined their symptoms, especially those linked to SFN and increased spinal fluid pressure.
Methods: Researchers reviewed surveys from 126 women (ages 30– 69) with TCs larger than 7 mm who sought treatment for chronic back, pelvic, or leg pain. Skin biopsy results from 75 of these patients were also used to quantify small nerve fibers.
Results: A reduction in nerve fiber count per mm skin, a sign of SFN, was found in 72– 80% of patients. Common symptoms included nerve pain (80%), sensitivity to touch (76%), pain while sitting (93%), bladder problems (93%), bowel issues (88%), genital arousal (27%), and restless legs (54%). Many reported headaches (57%), fatigue (86%), memory difficulties (86%), and pulsating ear noise (59%). Other symptoms included autonomic dysfunctions (problems with the body’s automatic functions), such as sweating problems (51%), and circulation issues like Raynaud’s phenomenon (45%).
Conclusion: Most patients with TCs show signs of SFN and report various symptoms, including bladder, bowel, and sexual issues, as well as widespread nerve pain and other problems like fatigue and cognitive issues. These symptoms may be caused by increased spinal fluid pressure, which stretches the nerve coverings to form Tarlov cysts and also damages small nerves in the spinal canal. Over time, this pressure could lead to SFN.
Keywords: intracranial hypertension, neuropathic pain, meningeal cysts, dysautonomia, hEDS, PGAD
Introduction
Tarlov cysts (TCs) are dilations of the nerve root sheaths that form as a result of elevated pulsatile cerebrospinal fluid pressure (CSFP). These dilations are situated at the dorsal root ganglion (DRG), where sensory and small-fiber neurons are located. TCs are primarily situated in the sacrum, where the hydrostatic pressure adds to the pathologically increased CSFP. TCs may induce radiculopathy of the nerve root on which they are located or by compressing the nearby nerve roots. Cysts causing radiculopathy with symptoms in the corresponding dermatomes or myotomes are termed “symptomatic TCs”.1,2 In a recent meta-analysis of 13,266 subjects, the incidence of TCs in Europe was estimated to be 6%, and 1 out of 6 (16%) were symptomatic TCs.3 However, while symptomatic TCs are rare, patients with symptomatic and non-symptomatic TCs often exhibit not only radicular manifestations but also symptoms that are not directly localized at the level of the affected area but are instead felt in other, seemingly unrelated, areas. These symptoms include headaches, fatigue, neuropathic pain elsewhere and autonomic dysfunction, among others.4,5
A previous retrospective study using skin biopsy data reported small-fiber neuropathy (SFN) in 82% of a small cohort of 17 PTCs.6 Increased CSFP, the underlying mechanism for the initiation and growth of TCs, may also contribute to other bodily symptoms by irritating, compressing, and ultimately damaging sensory and small-fiber neurons and axons within the DRG of the other nerve roots.6 Increased CSFP in PTCs is able to expand nerve root sheaths and can even exert sufficient force to cause bony erosion. Consequently, this force has the strength to damage the vulnerable unmyelinated and thinly myelinated Aδ- and C-fibers.
This retrospective study had two main objectives. The first objective was to document intraepidermal nerve fiber density (IENFD) in PTCs. The second objective was to map the incidence and types of symptoms experienced by PTCs. These symptoms were categorized into two groups (however, there may be overlap among these categories):
- Symptoms that are widely recognized in the literature as being related to TCs (Table 1).
- Symptoms not conventionally linked to TCs, but with a potential common underlying pathophysiological mechanism linked to increased CSFP (Table 2) and SFN (Table 3).

Table 1 Symptoms Typically Associated with TCs

Table 2 Symptoms Associated with Increased CSFP in PTCs

Table 3 Symptoms Associated with SFN in PTCs

This classification can be used to map the symptomatic spectrum in PTCs and suggest possible underlying mechanisms, including elevated CSFP and SFN, that may contribute to the broader symptomatology in these patients.
Materials and Methods
Inclusion and Exclusion Criteria
Female patients aged 30 to 69 years who presented to the outpatient physical medicine clinic with chronic low back pain or leg pain and had MRI-documented spherical nerve root cysts measuring ≥7 mm were included. Owing to the substantial predominance of females presenting with TCs and insufficient data on male patients for statistical analysis, we limited our study to female participants. A determination of whether the visualized TCs were actually symptomatic (ie, causing radiculopathy of the corresponding nerve root) was not routinely performed, as this information is relevant mainly when planning surgery and often requires invasive techniques such as a diagnostic nerve root block.
The exclusion criteria were other nerve-compressing pathologies (spinal or neuroforaminal stenosis, or disc hernia), and past or current chemotherapy.
Questionnaires
During the clinical assessment of PTCs, comprehensive questionnaires evaluating the occurrence of symptoms associated with TCs, increased CSFP, and SFN were administered. While the surveys used in this study have not undergone prior validation, they were specifically designed for use with PTCs in the clinical setting and were based on (1) extensive review of published studies on symptoms associated with PTCs, increased CSFP, and SFN; (2) existing questionnaires, such as the International Tarlov Cyst Questionnaire, which is used to assess typical TC symptoms preoperatively (F. Feigenbaum and D. West, unpublished); the International Consultation on Incontinence Questionnaire Female Lower Urinary Tract Symptoms Modules;59 and a gastrointestinal symptoms questionnaire;60 and (3) the 10 years of clinical experience with PTCs of the first author (MH).5,18
For each question, patients could choose from the following response options: “never”, “rarely”, “sometimes”, “often”, “very often”, “always”, or “not applicable/I don’t know”. The term “sometimes” is ambiguous and lacks clarity; therefore, the answers “never”, “rarely”, and “sometimes” were coded as “no”, and “often”, “very often”, and “always” were coded as “yes” to indicate whether the patient experienced a particular symptom. For some symptoms, such as rotational vertigo, allodynia or out-of-context genital arousal, that are typically absent in healthy individuals, a response of “sometimes” was included in the incidence group.
Symptoms, such as low back pain, sweating, constipation, and fecal or urinary incontinence, may occur more frequently in menopausal or aging individuals than in younger individuals. Therefore, two age categories were compared: 30–49 years and 50–69 years.
Skin Biopsies
Skin biopsies were collected 10 cm above the malleolus externus via disposable circular 3-mm punch needles. Fixation and analysis of the samples were carried out at the Department of Pathology, University Hospitals Leuven, Belgium. The punch biopsies were fixed in 4% phosphate-buffered formaldehyde for 6–24 hours and subsequently incubated in a cryoprotective solution (10% sucrose). Cross-sections of the epidermis were cut at a thickness of 50 μm using a cryotome. Immunohistochemistry was conducted with a polyclonal rabbit antibody raised against Protein Gene Product 9.5 (PGP9.5) (1/100, DAKO, Glostrup, Denmark) via an automated immunostainer. Prior to analysis, nerve fibers associated with glands and/or blood vessels were stained to serve as internal controls. The number of nerve fibers penetrating the epithelium was quantified in three distinct cross-sections.61 The length of the epithelium was measured with ImageJ software (NIH, Bethesda, MD, USA).
Patients with and without SFN were classified according to the quantitative normative dataset of Collongues et al,62 because this statistical model considered age and sex. In some instances, we also referred to the worldwide normative reference study from Lauria et al,63 as their dataset remains the most widely used dataset in the scientific literature. In this manuscript, the more common term “5th percentile” was used instead of the “0.05 quantile” term used by Lauria et al63 for patients whose biopsy results indicated a 95% likelihood of having SFN.
Statistics
Statistical analysis was performed in Python (Version 3.7.6, Copyright (c) 2001–2019 Python Software Foundation).
Descriptive characteristics and IENFD data are summarized as the means and standard deviations. The IENFD data for each patient were additionally plotted in Figure 1 alongside the normative data. Symptoms were summarized as a percentage. Patients who responded “I don’t know” or skipped a response were excluded from the mean and incidence calculations for that symptom.
 |
Figure 1 Biopsy results of PTCs compared to normative data. |
Medication use may cause side effects, such as sweating, constipation, or difficulty emptying the bladder. Therefore, all symptoms of patients taking tramadol, opioids, antidepressants, or antiepileptics were compared to those of patients taking no medication or medications causing less interference, such as paracetamol or supplements.
When comparing differences between two independent patient groups, a t-test was used to compare mean differences in symptom prevalence, and Fisher’s exact test was used to compare percentages of symptom incidence between groups. Significant difference levels were reported as meaningful based on a two-tailed test (p < 0.05).
Results
Descriptive statistics
Age, mean size of the largest TC in each patient, and the prevalence of SFN are detailed in Table 4. The mean age of all female PTCs was 51.3 ± 9.3 years. The mean TC size in all patients was 17.6 mm. The TC size was 2.4 mm smaller in the younger group than in the older group; however, the difference was not statistically significant.
 |
Table 4 Descriptive statistics of Patients with TCs |
In the entire cohort of PTCs, 80% of patients with skin biopsies had an IENFD below the 5th percentile value according to the quantitative normative dataset of Collongues et al62 In the younger cohort, nearly all patients (94%) were classified as having SFN, whereas the older cohort had a lower prevalence of SFN (68%).
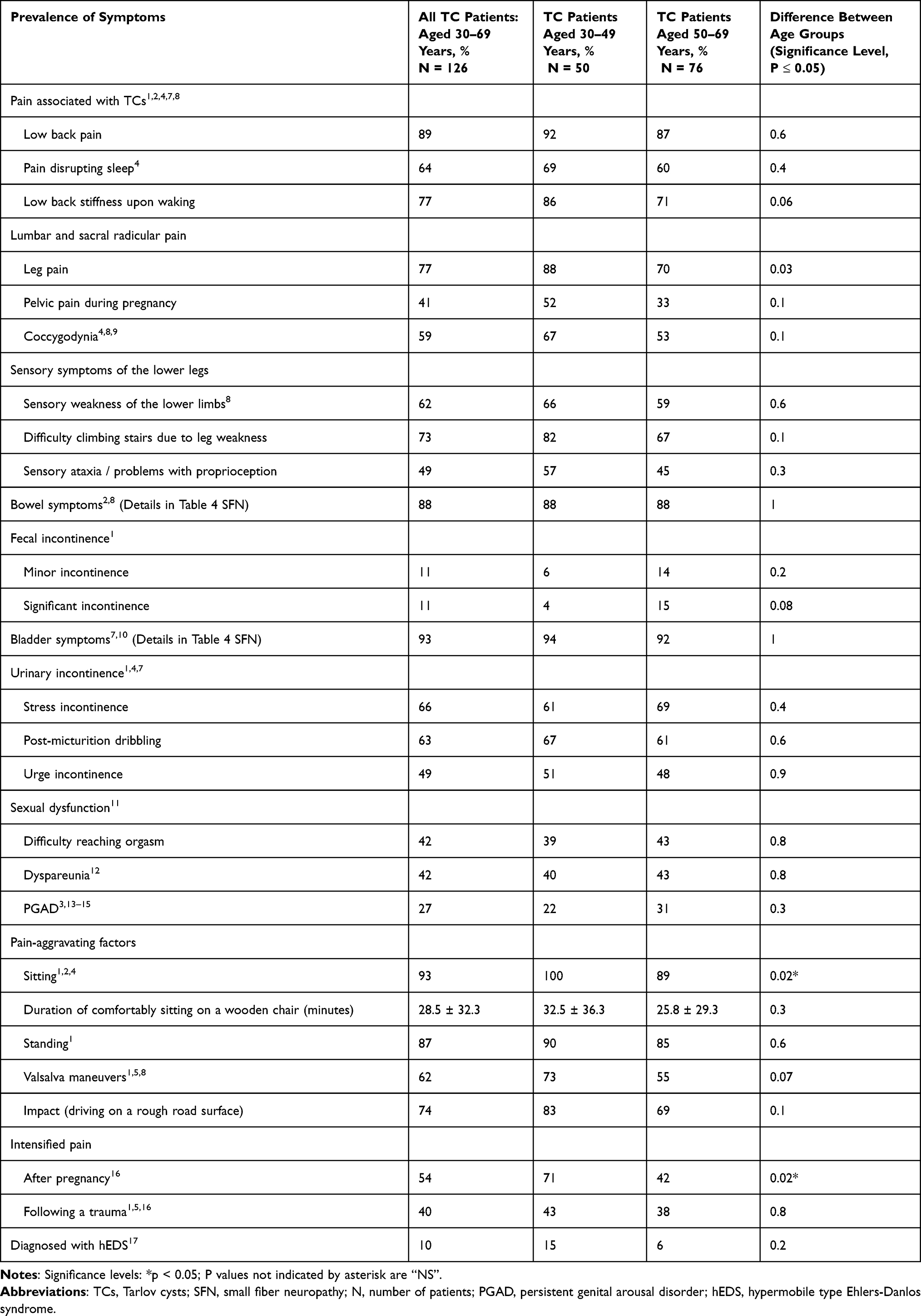
Symptoms Associated with Tarlov Cysts
The symptoms associated with symptomatic TCs have been extensively described in the literature.1,2,4,5 The incidence of these symptoms in our entire cohort of PTCs and in the two age groups is detailed in Table 1. The symptoms included low back pain (89%); leg pain (77%); difficulty sitting comfortably (93%); difficulty standing (87%); and bladder (93%), bowel (88%) and sexual dysfunctions (65%). Leg pain and sitting difficulties were reported significantly more often in the younger age group than in the older age group (p<0.05).
Pain increased with the Valsalva maneuver (62%) or with impacts such as driving on an uneven road (74%). Additionally, 10% of PTCs had a prior diagnosis of hypermobile Ehlers–Danlos syndrome (hEDS).
When patients with smaller TCs (<15 mm, N=59) were compared with those with larger TCs (≥15 mm, N=67), no relevant significant differences were observed for any of these symptoms (results not shown).
Symptoms Associated with Increased Cerebrospinal Fluid Pressure in Patients with Tarlov Cysts
Symptoms associated with increased CSFP are described elsewhere.36 The incidence of symptoms possibly associated with increased CSFP in our PTC cohort is detailed in Table 2. Overall, these symptoms were significantly more prevalent in the younger age group.
Symptoms due to overload of the (endo-)lymphatic system in the brain were highly prevalent, with episodes of rotational vertigo (64%) and aural fullness (49%) being the most frequently reported symptoms.
Increased CSFP in PTCs can cause pulsatile tinnitus (59%), fatigue (86%), headaches (57%), and cognitive dysfunction (86%). Additionally, 18% of all PTCs had been previously diagnosed with chronic fatigue syndrome (CFS). Increased sensitivity to odors (50%), light (61%), and noise (63%) was observed in PTCs.
Radicular pain unrelated to the location of the TCs but possibly associated with increased CSFP included neck pain (73%), pain between the shoulder blades (60%), and upper limb pain (50%).
Possible cranial nerve irritation due to increased CSFP was most pronounced in the accessory nerve-innervated trapezius muscles, in which patients reported painful hypertonia (71%). Similarly, hypertonia of the trigeminal nerve-innervated muscles of mastication was reported, with 67% of PTCs experiencing grinding or clenching.
Symptoms Associated with Small-Fiber Neuropathy in Patients with Tarlov Cysts
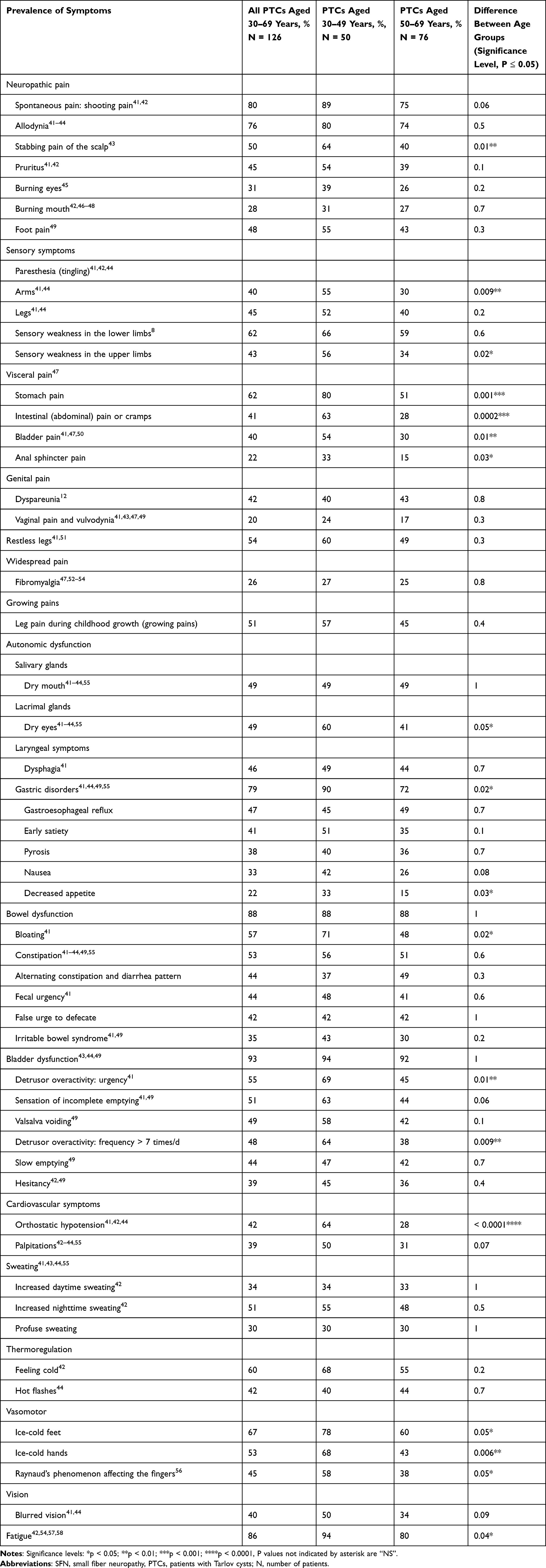
The symptoms associated with SFN are detailed in Table 3.
Given that 80% of PTCs with skin biopsies were documented to have SFN, neuropathic pain was prevalent, including stabbing pain (80%) and allodynia (76%). Visceral pain included stomach (62%), abdominal (41%), and bladder pain (40%). Visceral pain was significantly more common in the younger age group.
Notably, 26% of all women with TCs were previously diagnosed with fibromyalgia.
Autonomic dysfunctions included dry eyes (49%) and dry mouth (49%), symptoms of stomach dysfunction (79%), and intestinal (88%) and bladder symptoms (93%).
Discussion
Pathologically increased CSFP is generally believed to be largely responsible for the initiation and growth of TCs by forcing CSF into the nerve root sheaths. This pressure increase may lead to CSF leakage and accumulation between the layers of the nerve root sheath, ultimately resulting in sheath dilation.1,64–66 The DRG blood–nerve interface has significantly greater permeability and interstitial leakage of fluid and nutrients than the spinal nerve does, which, under physiological conditions, is necessary to meet the higher metabolic demands of the neurons within the DRG.67,68 Consequently, CSF leakage between the endoneurium and perineurium occurs more readily at the DRG, leading to the emergence of TCs in this area.1,65,69,70 Additionally, women exhibit substantially greater vascular permeability within the DRG than men do.68 This difference may explain why the presence of TCs is notably more prevalent in women than in men. In a meta-analysis of 13,266 subjects, the prevalence of TCs worldwide was 6% in women and 3% in men.3 Approximately 16–25% of TCs are symptomatic TCs, as these cause clinically significant radicular pain or motor weakness. Approximately 75% of patients with symptomatic TCs are women.2,3,5,65,71
The prevailing assumption attributes widespread pain and various symptoms in PTCs to central sensitization triggered by a prolonged episode of initial pain. However, central sensitization or hypersensitivity in the central nociceptive system may also be induced and maintained by prolonged peripheral overstimulation or small nerve damage.72 For example, the symptoms of neuropathic pain due to postherpetic neuralgia and complex regional pain syndrome are maintained by peripheral nociceptive input.73 In PTCs (with or without confirmed SFN), this overstimulation may be prompted by prolonged irritation, compression and damage of the small nerve fibers or small-fiber neurons due to (moderately) elevated pulsatile CSFP. CSFP in PTCs, which can dilate nerve root sheaths and cause bone erosion, must be sufficient to hyperexcite or even damage frail small nerve fibers and sensory fibers in the DRG.6,11
Age, Size of Tarlov Cysts and Intraepidermal Small Fiber Density
Table 4 shows the details of the demographic characteristics. The mean age of all female PTCs was 51.3 ± 9.3 years, and the mean largest diameter of TCs in any plane (sagittal, coronal, or axial) was 17.6 ± 9.3 mm. The age and TC size of this cohort are comparable to those in the study by Baker et al,10 which included 65 women with a mean age of 53 + 12 years and a mean TC sagittal diameter of 17 mm who presented at urogynecology or neurosurgery clinics with symptoms similar to those of our cohort. In a meta-analysis, radiologic data from 13,266 PTCs were pooled, and the mean pooled sagittal diameter was 11.86 mm, which was smaller than that reported in our cohort.3
The percentage of all patients in our cohort with an IENFD below the 5th percentile for SFN according to the quantitative normative dataset of Collongues et al62 was 80%, but it was only 72% according to the worldwide normative reference study by Lauria et al63 (Figure 1).
Previously, we reported preliminary findings on SFN in a small cohort of 17 PTCs.6 In 82% of these patients, the IENFD was below the 5th percentile for age and sex based on Lauria63 reference data. Here, we present data from a significantly larger sample of 75 skin biopsies. This expanded dataset enables more robust and generalizable conclusions, while also confirming and building upon our earlier observations. Furthermore, this manuscript includes an analysis of symptom questionnaires from 126 patients treated at our clinic. These surveys were specifically designed to capture the diverse range of symptoms reported by individuals with Tarlov cysts.
We classified patients using the SFN 5th percentile reference data provided by Collongues,62 because this dataset includes age-specific data, whereas Lauria et al63 provide data by decade. Moreover, the normative data from Collongues et al62 were collected from healthy subjects in France, a neighboring country with a comparable ethnicity to that of Belgium.62 While the use of these criteria may result in a small number of false-positive biopsies compared with Lauria’s criteria, the impact on this PTCs study is believed to be minimal. Moreover, PGP9.5 staining detects skin nerves that are sufficiently intact to be identified, but it does not provide information about their functionality.41 This fact may explain the lack of correlation between IENFD and neuropathic pain reported in previous studies.74
In the younger cohort, almost all PTCs were diagnosed with SFN (97% according to Lauria and 94% according to Collongues). In contrast, in the older cohort, only 68% of patients were diagnosed with SFN via the Collongues et al62 data, and only 51% via the dataset of Lauria et al.63 The reason for this difference in SFN diagnoses, which is calibrated for age using normative data, between older and younger patients is not clear. Further research is recommended to help explain the vast differences observed between normative and a PTCs population, similar to the one in this study.
Symptoms Associated with Tarlov Cysts
Table 1 provides details on the symptoms associated with TCs. Owing to the primary location of TCs on sacral nerve roots, symptomatic TCs commonly cause symptoms such as lower back, leg, pelvic, perineal, and genital pain, as well as bladder, bowel, sphincter, and sexual dysfunctions.2,4,5
No relevant significant differences in symptom reporting were observed between patients with TCs <15 mm and those with TCs ≥15 mm, which is consistent with other studies. Baker et al10 reported no significant associations between TC size and bowel, sexual, or lumbosacral symptoms, or lower extremity weakness or numbness. The authors reported a significant association only between urinary symptoms and cyst size. Similarly, Hentzen et al11 reported that neurophysiology findings did not correlate with the number, size or location of the cysts. In another study in PTCs, neurophysiological abnormalities were found even in myotomes of non-dilated nerve roots.6,75 These results suggest that the size of the TC is not a criterion for experiencing symptoms. Instead, the pressure inside the TC is likely more important.
Among neurophysiological studies, the most common abnormalities were observed in sensory evoked potential (SEP) studies11 and anal reflex studies,6 suggesting that the sensory pathways are more susceptible to injury.
In our study, low back pain was reported in 89% of PTCs. It was not specified whether the pain was sacral or lumbar, as patients are often unable to differentiate. Most TCs are found in the sacrum given the relatively high hydrostatic CSFP in this area.64,76,77 Leg pain occurred in 77% of patients and may be caused by the involvement of sacral nerves S1 and S2 and, less frequently, due to the involvement of lumbar nerves. In a previous needle-electrode electromyography study, the L5 myotome was the most commonly affected lumbar nerve root in TC patients, even when a TC was not visible at that level.6
A distinct form of pelvic pain is pelvic girdle pain during pregnancy, which is often attributed to mechanical pelvic instability. In our cohort, 41% of PTCs reported having been diagnosed with pelvic instability during pregnancy compared to an estimated incidence of 20% in the general population during pregnancy.78 A subgroup of these PTCs with pelvic pain during pregnancy likely experienced neuropathic pelvic pain, either in isolation or in combination, with mechanical pain.
Coccygodynia is also often suspected to be a mechanical problem. However, chronic intractable coccygodynia may have a neuropathic component.79 In the general population, coccygodynia accounts for less than 1% of all non-traumatic complaints of the spine.80 The high incidence of coccygodynia (59%) in our cohort of PTCs may suggest a neuropathic component originating from radiculopathy of the nerve roots of the coccygeal plexus.
In PTCs, sensory symptoms in the lower legs included a sensation of weakness (62%), although clinical examination did not reveal any objective reduction in strength. Difficulty climbing stairs due to this feeling of weakness was reported in 73%. The term ‘sensory weakness’ is used here to describe the feeling of weakness caused by reduced sensory feedback. Weakness of the legs was reported significantly more often by younger patients than by older patients. Additionally, 49% of PTCs reported experiencing an unsteady gait (sensory ataxia). This may be attributed to the mixed etiology polyneuropathy in PTC, in which small and large sensory nerve fibers may be involved in sensory ataxia similar to that observed in diabetes mellitus.81
Bowel and bladder dysfunction are typically reported in PTCs. However, these symptoms are likely attributable primarily to autonomic dysfunction from SFN and will be discussed later in this article.
Eleven percent of PTCs reported minor fecal incontinence, and another 11% reported significant fecal incontinence. Fecal incontinence may be partly attributed to radicular sensory nerve involvement. The S2-S3-S4 anal reflex arc consists of a sensory limb and a motor limb. Electrophysiological assessment of the anal reflex arc thus incorporates sensory nerve evaluation, which is an advantage over needle‒electrode electromyography, which evaluates only motor innervation. In a study of the anal reflex in 21 PTCs, 95% showed a delayed anal reflex response unilaterally or bilaterally, and 57% of patients with a delayed anal reflex latency complained of mild to severe fecal incontinence.6 Additionally, Murphy et al7 reported sphincter tone disturbances in 29% of 213 symptomatic PTCs.
In our cohort of PTCs, the incidence of self-reported urinary stress incontinence was 66% and urge incontinence 49%. This is higher than the incidence of urinary stress incontinence (10–39%) and urge incontinence (1–7%) in the general population.10 The incidences in our cohort are also higher than those reported by Baker et al10 in women of a similar age with TCs: stress incontinence in 25% and urge incontinence in 31%. The reason for this discrepancy is unclear. It is possible that there may have been slight differences in the questions asked between the studies. The incidence of urinary incontinence was expected to increase with age; however, the rates were not significantly different between the younger and older PTCs.
In an electrophysiologic SEP study in 65 women with TCs, Hentzen et al11 reported a negative association between abnormal neurophysiology and urinary incontinence and, therefore, concluded that urinary incontinence is unlikely to be related to TC-induced nerve damage. However, electrophysiologic anal reflex studies may provide an alternative explanation. By assessing the integrity and function of the sacral nerves (S2-S4), which are involved in both anal and urinary sphincter control, a delayed anal reflex can indirectly offer information about the neural mechanisms responsible for urinary continence. The previously mentioned electrophysiological study of 21 PTCs revealed a delayed anal reflex in 95% of patients, which may suggest a neurophysiological mechanism for urinary incontinence related to TC-induced nerve sensory damage.6
Sexual dysfunction is common in PTCs.3,4,7,11–16 Difficulty reaching orgasm can be due to pelvic or leg pain during intercourse, or dyspareunia, which was reported in 42% of PTCs; however, it can also be related to genital sensory disturbances.
Persistent genital arousal disorder (PGAD) is a condition characterized by out-of-context sexual arousal episodes.13 Out-of-context genital arousal was reported by 27% of PTCs. PGAD has been previously associated with the presence of TCs. In a recent meta-analysis of 13,266 subjects with TCs, the prevalence of PGAD was 38%.3 Feigenbaum and Boone14 identified 11 patients with PGAD in patients with symptomatic spinal meningeal cysts. Microsurgical treatment of the cysts cured or significantly reduced PGAD symptoms in 91% of the patients.
Additionally, Oaklander et al13 documented TCs in 4 out of 10 patients with PGAD and concluded that this finding strengthened the associations between TCs and sensory polyneuropathy and suggested that many cases of PGAD may be caused by unprovoked firing of small C-fibers in regional sensory neurons that contribute to sexual arousal. Similarly, Komisaruk and Goldstein82 noted that TCs induced genital radicular neuropathy can stimulate sensory nerves and produce PGAD symptoms. According to the authors, nerve compression likely represents a continuum from nerve irritation (hyperstimulation) to nerve damage (hypofunction), which can subsequently lead to nerve hypofunction and difficulty in achieving orgasm.
Pain in PTCs typically worsens with sitting (93%) and standing (87%). The ability to sit comfortably on a wooden chair was limited to an average duration of 28.5 minutes.
When changing from the lying position to the sitting position, a caudal shift in spinal CSF volume occurs. Consequently, the spinal dural sac volume increases, reducing compliance of the spinal CSF space, increasing sacral pressure and forcing CSF into the nerve root sheaths and the TCs.83 Pain in PTCs also increases during Valsalva maneuvers and following physical impacts, pregnancy, or trauma.1,4,5,16 The Valsalva maneuver increases intrathoracic and intra-abdominal pressure, leading to a sharp transient increase in CSFP in both the ventricles and lumbar spine.84 The increased CSFP during a Valsalva maneuver may apply additional transient pressure, potentially irritating the small nerve fibers in the DRG and the communicating TCs, leading to a temporary increase in pain. Moreover, in non-communicating TCs (ie, those with a valve system), during Valsalva maneuvers, CSF is forced into the TCs but cannot exit quickly. Therefore, repeated Valsalva maneuvers (coughing, lifting heavy objects) may cause longstanding increased radicular pain.
Notably, 10% of PTCs in our cohort were previously diagnosed with hypermobile Ehlers-Danlos syndrome (hEDS) according to the diagnostic criteria for hEDS of the International Consortium on Ehlers–Danlos Syndromes and Related Disorders.85 Connective tissue disorders have been linked to idiopathic intracranial hypertension (IICH), with complications such as dural ectasia and TCs being common.17,19,30 Additionally, connective tissue weakness allows the nerve root sheaths to dilate more easily in response to increased CSFP.
Symptoms Associated with Increased Cerebrospinal Fluid Pressure in Patients with Tarlov Cysts
Table 2 provides details on symptoms that are likely associated with CSFP in PTCs. The role of unrecognized moderately increased CSFP has been demonstrated in patients with other chronic pain conditions, such as widespread chronic pain,86 CFS,31,32 chronic refractory migraines,87 and hypermobility syndromes.19 The role of moderately increased CSFP has also been demonstrated in PTCs via external lumbar CSF drainage or the administration of acetazolamide, both of which temporarily relieved pain by reducing the CSFP.88–90 In the upright posture, pathologically elevated CSFP is most pronounced in the sacral spinal canal, where most TCs form.64
In the clinical assessment of PTCs in this study, diagnostic tests to confirm a diagnosis of IICH were not conducted. PTCs are thought to have a moderately increased CSFP. Therefore, papilledema is unlikely to be present. Moreover, measuring CSFP via lumbar puncture is an invasive procedure associated with potential risks. The opening pressure in PTC cases is typically less than 25 cm H2O, which does not meet the criteria for diagnosing IICH. In a retrospective study of lumbar punctures in 15 patients with TCs, the average opening pressure ranged from 11 to 32 cm H2O, with a mean of 18.5 cm H2O, which falls at the high end of the normal range.86 The cutoff values used to define IICH have been debated. Indeed, the intracranial pressure (ICP) is a continuum that lacks a clear cutoff value. Additionally, papilledema may be absent even if the ICP is greater than the cutoff value.31
Compared with the older cohort, the younger cohort often presented significantly more frequent symptoms that may be related to increased CSFP. Symptoms such as neck pain, hearing loss, or cognitive problems are expected to increase with age; however, the opposite trend was observed. This discrepancy may be because these younger patients often have a greater physical load because they have a family with children at home, work (either in sedentary or physically demanding jobs), and manage household tasks. In contrast, the older patients are more likely to be out of employment, possibly due to sick leave or retirement, and typically do not have children at home to care for. A previous retrospective study revealed that PTCs were more frequently forced to stop working or reduce their social activities than were those with chronic low back pain due to other causes.4
(Endo-)lymphatic Overload Symptoms
PTCs frequently present symptoms that are related to overload of the olfactory lymphatic pathway. Nasal congestion,18–20 rhinorrhea19,20 and sinusitis18,19,21–24 have been linked to IICH. The mechanism involves CSF drainage along the perineural spaces of the cranial nerves, most commonly the olfactory nerve. As the endothelial layer of the olfactory nerve sheath is thinner in the nasal mucosa and ethmoid sinus, CSF penetrates into the lymphatic pathways of the nasal submucosa, traveling toward the regional lymph nodes.91 When the olfactory lymphatic drainage system becomes saturated with excess CSF, the fluid may leak into the nasal mucosa, leading to mucosal swelling and nasal obstruction. Leaking of excess CSF into the paranasal and nasal cavities may cause watery rhinorrhea or sinusitis.18,19 In our cohort, 62% of patients experienced rhinitis symptoms (nasal obstruction, rhinorrhea, or both), which is a greater proportion than that reported in the general population of Belgium.92 The overall incidence of rhinitis in Belgium has been estimated at 39.2%.
Notably, 9% of PTCs had already undergone septoplasty due to persistent severe nasal obstruction.
Rotational vertigo occurred in 64% of the PTCs. Hearing loss and vertigo may result from the transmission of increased CSF pressure to the medial or inner ear via the cochlear aqueduct. Meniere’s disease and IICH share similar symptoms, such as a greater incidence of vertigo, tinnitus, aural fullness, sensorineural hearing loss, and headache.27 When lumbar punctures were performed in patients with IICH, vertigo, dizziness, fluctuating hearing loss, tinnitus, and aural fullness improved.28 Additionally, medical management with diuretics and corticosteroids is similar for both IICH and Meniere’s disease.25 This mechanism of olfactory overload may also explain the severe ear pressure experienced by 49% of PTCs during airplane flights.
Tinnitus
In our cohort of PTCs, 59% experienced pulsatile tinnitus. Among the younger cohort, the prevalence was greater (74%) than that in the older cohort (49%). Pulsatile tinnitus is a common symptom of IICH due to increased ICP acting on the blood vessels near the ear.
Fatigue
Fatigue was reported in 86% of PTCs. Among younger PTCs, 96% reported experiencing fatigue significantly more than older PTCs did (80%). Moreover, chronic fatigue syndrome was previously diagnosed in 18% of PTCs. Several researchers have proposed that a subset of chronic fatigue syndrome cases may be linked to moderately elevated CSFP.18,31,32
Headaches
In our cohort, headaches of any type were reported in 57% of PTCs. Few authors have reported headaches in symptomatic TC patients, likely because the association of headaches with TCs is unclear. Baker et al10 reported a headache incidence rate of 35% in PTCs. In our cohort, skull base pain was reported in 54% of patients, occurring significantly more frequently in younger PTCs than in older PTCs. Patients with IICH present with complaints secondary to intracranial venous congestion, including headache, skull base pain, morning and nocturnal headaches.19,30,93 A study in which CSFP was continuously monitored revealed that CSFP increased at night because of increased CSF secretion in 30% of patients,94 which may explain the morning headaches reported in 37% and nocturnal headaches reported 26% of PTCs.
Chronic migraine may be caused by unrecognized elevated CSFP.34 Migraines in PTCs (47%) were reported significantly less frequently in the older patient group (34%) than in the younger group (67%), which is consistent with the data of population-based studies on migraine that have shown an improvement in migraine after menopause. Notably, migraine has also been linked to SFN. In a prospective cohort study of 61 migraine patients, SFN was documented in 45% of the patients.33 Additionally, symptoms often associated with migraine and IICH, such as hypersensitivity to light (61%), noise (63%), or odors (50%), were highly prevalent in PTCs.
Cognitive Dysfunction
In our PTCs, brain fog (63%), difficulties with recalling names (62%), short-term memory (46%) or mental concentration (65%) were highly prevalent, especially among younger patients. There was no difference in cognitive impairment symptoms between patients taking tramadol, opioids, anti-epileptics, or antidepressants and those not taking these medications. This suggests, that the impairment is not due to aging or drug side effects. Patients with IICH may also experience cognitive impairment.30,95,96
Radicular Pain
PTCs commonly suffer from low back pain (89%) and leg pain (77%). Additionally, the incidence of neck pain (73%), arm pain (50%), upper back pain (60%), and thoracic pain (31%) was also notably high. Such symptoms may be caused by increased CSFP even in the absence of TCs on the cervical or thoracic nerve roots. Several authors have reported radicular pain in patients with IICH.97–99 Moreover, spinal nerve root sheaths of patients with IICH can be noticeably dilated,100 and signs of radiculopathy may be observed during electrophysiologic testing.101,102 Among 101 patients with IICH, 31% reported neck problems and 22% reported paresthesia. These symptoms resolved immediately following lumbar puncture.103 In another study of 165 patients with IICH, 42% reported neck pain, 53% reported back pain, and 19% reported radicular leg pain.29 In these reports, the authors suggested that radicular pain resulted from CSF filling the nerve root sheaths near the DRG under high pressure.29,97,101,103
Cranial Nerve Involvement
Some of the symptoms of PTCs may be attributed to cranial nerve involvement. The perineural spaces of cranial nerves, including the olfactory, optic, trigeminal, and auditory nerves, involve multiple lymphatic pathways of CSF drainage toward the lymph nodes.91 When ICP is chronically elevated, CSF is forced into the cranial nerve root sheaths, which may compromise the blood supply or cause mechanical pressure on the axons during their intracranial course. Increases in optic nerve sheath diameter, tortuosity, and papilledema are notable examples of this phenomenon. Although less visible on MRI than optic nerves, other cranial nerves are likely affected by the forced entry of CSF into their nerve root sheaths. Symptoms associated with cranial nerve involvement have been described in IICH patients and are prevalent in PTCs. These symptoms include a decreased sense of smell (olfactory nerves),37 diplopia (oculomotor nerve),29,39 facial pain and paresthesia (trigeminal nerve),40 sensorineural hearing loss (vestibulocochlear nerves),27,29 and swallowing difficulties,30 all of which have been reported by our PTCS at significant rates (Table 2).
The high incidences of bruxism or clenching (67%) and hypertonia or pain in the trapezius muscles (71%) are also notable in PTCs. Both symptoms have been reported in IICH patients, as well as in patients with other chronic pain conditions and CFS.18 According to our hypothesis, increased CSFP may lead to hyperexcitability of the trigeminal nerve, affecting the muscles involved in mastication,104 and the accessory nerve, impacting the upper trapezius muscle, potentially causing these symptoms.
Symptoms Associated with Small-Fiber Neuropathy in Patients with Tarlov Cysts
Table 3 provides details on neuropathic pain and autonomic dysfunctions associated with SFN in PTCs. Several of these symptoms occurred more often in the younger cohort than in the older cohort. The explanation may be twofold: first, the younger cohort likely leads a more physically demanding lifestyle than the older group does; second, nearly all younger patients were documented as having IENFD values below the 5th percentile.
SFN is caused by the damage and loss of thinly myelinated Aδ- and unmyelinated C-fibers. SFN is a debilitating condition that leads to alterations in nociceptive processing (pain), thermal sensation, and autonomic function.41 The autonomic nervous system regulates involuntary physiological processes, including blood pressure, heart rate, respiration, thermoregulation, digestion, lacrimation, urinary motility, visual focusing and sexual arousal, to maintain body homeostasis. It comprises the sympathetic, parasympathetic, and enteric nervous systems.105 The clinical symptoms of SFN are the result of conduction impairment and sensitization triggered by neural damage. Length-dependent SFN starts in the feet and progresses upward, whereas non-length-dependent SFN involves the face, scalp, mouth, trunk, and upper and lower limbs.43 The topographic pattern of non-length-dependent SFN is likely related to ganglionopathy affecting the small neurons of the DRG,42 such as in PTCs.
Potential Relationship Between Tarlov Cysts and Small-Fiber Neuropathy
The connection between TCs and SFN may involve increased endoneural CSFP in the DRG. Increased amounts of endoneural fluid distend the nerve; however, the nerve root sheath resists expansion. This resistance leads to an increase in endoneural fluid pressure, which compresses the penetrating perineurial vessels and consequently decreases blood flow to the DRG neurons and the thin or unmyelinated nerve fibers.106 Similarly, studies have shown that external mechanical compression of the DRG by disc herniation results in increased endoneural CSFP. The authors describe this phenomenon as “closed compartment syndrome in nerve roots”. According to the authors, this elevation in the CSFP may lead to a reduction in blood flow to the sensory and small-fiber neurons in the DRG, potentially serving as a mechanism underlying the occurrence of nerve root pain.107
In PTCs, the CSFP inside the endoneural space increased to the point that some of the patient’s nerve root sheaths could no longer resist expansion, leading to their dilation and the emergence of TCs. This internal pressure, which is strong enough to dilate nerve root sheaths, can also be powerful enough to erode dense bone, emphasizing that it is likely to also damage delicate small nerve fibers and neurons within the DRG, resulting in SFN. As a result of chronically elevated internal CSFP, small-fiber damage is expected to occur not only within dilated nerve roots but also within nerve root sheaths that resist that pressure and do not dilate. The increased internal pressure within both dilated and non-dilated nerve roots is likely why pain in TC patients often does not correlate with the size or location of the TCs, as noted by several authors.6,10,11,65,108,109 Similarly, Hentzen et al11 reported that SEP abnormalities and clinical sensory examination findings do not correlate with TC location. As a consequence, pain in PTCs can develop anywhere in the body in a non-length-dependent topographic pattern.49
Approximately 50% of SFN cases are idiopathic.42 The mechanism of (moderately) increased CSFP may explain a subset of these idiopathic cases of SFN. SFN in PTCs may help explain why surgery on TCs often fails to produce the expected outcomes, such as pain reduction.
Interestingly, there is a striking similarity between the process of CSF accumulation in the DRG in PTCs and glycolipid accumulation in the DRG of patients with Fabry disease, an inherited lysosomal storage disorder associated with painful neuropathy. Using magnetic resonance neurography, significantly enlarged DRGs have been documented in female patients with Fabry disease compared with those of matched healthy women. These dilations were most likely due to severe glycolipid accumulation.110
Neuropathic Pain
Common neuropathic pain symptoms in patients with SFN include shooting pain, allodynia, and paresthesia.41–44 Shooting pain was confirmed in 80% of PTCs, and allodynia was confirmed in 76% of PTCs. Paresthesia occurred not only in the legs (45%), as might be expected in PTCs, but also almost equally in the arms (40%). Additionally, 62% of patients reported a sensation of weakness in the legs, and 43% reported a sensation of weakness in the arms.
Specific types of pain associated with SFN were also reported by PTCs. They included stabbing pain on the scalp in 50% of the PTCs, pruritus in 45%, and severe burning of the eyes in 31% and mouth in 28%.41–43,45–48,111 Neuropathic pain in the feet is typically associated with length-dependent SFN49 but was also reported by 48% of PTCs, who are probably more likely to have non-length-dependent SFN.
Visceral pain and visceral hypersensitivity are mediated by small fibers.47 In our cohort of PTCs, reported visceral pain included stomach (62%) and intestinal pain (41%). These symptoms were significantly more prevalent in the younger patient cohort. Other symptoms in PTCs, including bladder pain (40%) and vulvodynia (20%), have previously been associated with SFN.41,43,47,49,50 Dyspareunia occurred in 42% of PTCs and was equally prevalent in both the younger and older groups, suggesting that dyspareunia cannot be attributed solely to declining estrogen levels and vaginal atrophy during menopause.
To our knowledge, restless leg symptoms have not been previously reported in PTCs. However, in our cohort, 54% of PTCs experienced these symptoms. Restless leg syndrome has also been linked to SFN, possibly as a form of neuropathic pain.41,51
In this study, 26% of PTCs were previously diagnosed with fibromyalgia. This association may be expected, as, similar to fibromyalgia, PTCs report unexplained widespread pain. Moreover, up to two-thirds of fibromyalgia patients have been diagnosed with SFN,112 and it has been documented that 39% of patients previously diagnosed with fibromyalgia also exhibit TCs.113
Growing pains, defined as recurrent lower limb pain during childhood, was reported in 51% of PTCs. Despite numerous cases of growing pains documented in the international literature, their exact nature and etiology remain unclear. In a retrospective study of 532 Mediterranean children aged 4–12 years, the incidence of growing pains was 25%.114 Given the high percentage of childhood leg pain in PTCs, this symptom may be neuropathic pain associated with early-stage small fiber involvement.
Autonomic Dysfunction
Autonomic dysfunction of the lacrimal glands, causing dry eyes, and salivary glands, causing dry mouth, have been reported in patients with SFN.41–44,55 In our cohort of PTCs, 49% reported one or both of these symptoms. Compared with the older age group, dry eyes were significantly more prevalent in the younger age group. Therefore, these symptoms cannot be attributed to aging alone.
There was also a high incidence of symptoms suggesting autonomic dysfunction of the gastrointestinal tract. One or more symptoms indicating gastric dysfunction were reported in 79% of PTCs. Slow gastric emptying has primarily been studied in diabetic patients with SFN.41,44,49,55 Symptoms indicating bowel dysfunction were reported by 88% of PTCs, including bloating (57%), constipation (44%), constipation alternated with diarrhea (44%), fecal urgency (44%), and false bowel movements (42%). Murphy et al7 reported bowel dysfunction in 29% of 213 patients with symptomatic TCs. As a consequence of these bowel symptoms, patients with SFN are often (mis)diagnosed with irritable bowel syndrome.41,47 In our cohort, 35% were diagnosed with irritable bowel syndrome.
Symptoms indicating bladder dysfunction were reported in 93% of PTCs. Autonomic dysfunction can play a significant role in the development of these bladder symptoms.41–44,49 Detrusor muscle contraction during voiding is mediated by the parasympathetic innervation derived from the sacral spinal cord roots (S2, S3, and S4). Our findings are consistent with those of Hentzen et al,11 who utilized the Urinary Symptom Profile questionnaire115 and reported that 93% of 65 women with TCs experienced voiding difficulties.
When our cohort was compared with the cohort of 65 female PTCs studied by Baker et al,10 the incidence of urinary urgency (54% vs 55%) and frequency (48% vs 48%) did not differ. However, urinary hesitancy was reported in 18% of the women in Baker’s cohort versus 39% in our cohort. Murphy et al7 reported bladder or urinary sphincter symptoms in 43% of 213 PTCs. The lower percentage of patients with bladder symptoms in Murphy’s cohort than in our cohort (94%) is likely because we inquired more specifically and in detail about the possible symptoms. Valsalva voiding was reported in 49% of our cohort, which is comparable to the 48% reported by Hentzen et al11 in a urodynamic study of 56 women.
Cardiovascular symptoms that may be precipitated by autonomic dysfunction were prevalent in our cohort.41–44,55 The most prevalent symptoms among the younger PTCs were orthostatic hypotension (64%) and palpitations (50%).
Thermoregulation and sweating abnormalities have been reported in patients with SFN.41–44,55 Feeling cold was reported by 60% of PTCs, and hot flashes were reported by 42%, with no statistically significant difference in the incidence between the younger and older cohorts. Similarly, profuse daytime sweating (34%) and nighttime sweating (51%) did not differ between the age groups, indicating that menopause was not the main reason for hot flashes or sweating. On the other hand, patients who chronically used tramadol, opioids, antidepressants, or antiepileptics reported significantly more sweating than those not taking these medications did (63% vs 40%, p<0.05).
Primary Raynaud’s phenomenon is characterized by pallor of the fingers in response to cold and is a common feature of systemic sclerosis. However, Raynaud’s phenomenon has also been associated with autonomic nervous system abnormalities, with both autonomic small fibers and sensory nerve fibers believed to play a role.56 This theory could explain why 45% of all PTCs reported experiencing Raynaud’s phenomenon, with significantly more in the younger age group (58%) than in the older age group (38%).
Intermittent blurred vision that could not be corrected by using lenses or glasses was confirmed in 40% of PTCs. The autonomic nervous system controls the physiological functions of the eye, including the regulation of lens accommodation.116 Blurred vision has been described in patients with SFN.41,44 There was no statistically significant difference between age groups, indicating that aging was not the main cause of these visual disturbances.
Limitations
Normative IENFD data from healthy control subjects from our anatomopathological laboratory for comparison with the data from PTCs are lacking. Therefore, we compared the IENFD of PTCs to the quantitative normative dataset by Collongues et al62 and to the data of the worldwide normative reference study by Lauria et al63 However, minor technical differences between laboratories may lead to variations in IENFD outcomes. An additional test, such as the sympathetic skin response, could serve as a complementary neurophysiological tool for assessing C-fibers and sensory pathways, both of which are affected in PTCs.117,118
Additionally, in this study, we used self-composed questionnaires that have not been previously validated. While these tools were tailored specifically for the clinical assessment of PTCs, the lack of prior validation may affect the reliability and validity of our findings. Future research should include steps to validate these instruments.
Despite the limitations, we have ensured rigor by objectively confirming the presence of TCs on the MRI and assessing IENFD. To improve the testability of our results, we suggest designing a prospective study that would allow for better patient selection, minimization of recall bias, and the inclusion of supplementary tests such as the sympathetic skin response or thermal sensory threshold testing in PTCs.
Conclusion
A high prevalence of SFN was documented in PTCs, with 80% falling below the 5th percentile as defined by Collongues et al.62 It is widely accepted that (moderately) elevated pulsatile CSFP within the nerve root sheaths contributes to TC formation at the DRG by gradually distending the nerve root sheaths. This chronically elevated pressure may also lead to small-fiber dysfunction by irritating, compressing, and ultimately damaging small fibers in the DRG, resulting in SFN. While TCs identified on MRI are often reported as incidental findings and may be asymptomatic, individuals with TCs frequently report symptoms such as headaches; fatigue; cognitive issues; widespread neuropathic pain; and dysfunctions in bladder, bowel, sphincter, sexual, and autonomic functions. These symptoms are consistent with those previously documented in PTCs, IICH patients, or SFN patients. Thus, TCs observed on MRI, regardless of whether they are symptomatic, should not be evaluated in isolation since they may be indicative of a broader systemic condition involving elevated CSFP and SFN.
Future research should focus on developing a tool capable of continuously and accurately monitoring CSFP in PTCs, allowing for the study of its effects on sensory fibers and nerve root sheaths, and enabling a more objective assessment. Currently, no such non-invasive measurement method exists.
Abbreviations
SFN, Small fiber neuropathy; PTCs, patients with Tarlov Cysts; TCs, Tarlov Cysts; IENFD, intraepidermal nerve fiber density; CSFP, cerebrospinal fluid pressure; PGP9.5, Protein Gene Product 9.5; CFS, chronic fatigue syndrome; hEDS, hypermobile Ehlers-Danlos syndrome; IICH, idiopathic intracranial hypertension; ICP, intracranial pressure.
Data Sharing Statement
The dataset has been submitted as Supplementary table 1.
Ethics Approval and Informed Consent
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of AZ Rivierenland Campus Bornem, with which RR is affiliated (reference code: 2405LA001; date of approval: May 13, 2024). Patient consent was waived due to the retrospective nature of the study, which was based on existing data. Patient data were accessed in compliance with relevant data protection and privacy regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Feigenbaum F, Henderson F. Tarlov cysts. In: Benzel E, editor. Spine Surgery. Philadelphia: Elsevier; 2012:1135–1140.
2. Murphy K, Nasralla M, Pron G, Almohaimede K, Schievink W. Management of Tarlov cysts: an uncommon but potentially serious spinal column disease-review of the literature and experience with over 1000 referrals. Neuroradiology. 2023;66(1):1–30. doi:10.1007/s00234-023-03226-6
3. Klepinowski T, Orbik W, Sagan L. Global incidence of spinal perineural Tarlov’s cysts and their morphological characteristics: a meta-analysis of 13,266 subjects. Surg Radiol Anat. 2021;43(6):855–863. doi:10.1007/s00276-020-02644-y
4. Hulens MA, Dankaerts W, Rasschaert R, et al. Can patients with symptomatic Tarlov cysts be differentiated from patients with specific low back pain based on comprehensive history taking? Acta Neurochir. 2018;160(4):839–844. doi:10.1007/s00701-018-3494-z
5. Hulens M, Rasschaert R, Bruyninckx F, et al. Symptomatic Tarlov cysts are often overlooked: ten reasons why-a narrative review. Eur Spine J. 2019;28(10):2237–2248. doi:10.1007/s00586-019-05996-1
6. Hulens M, Bruyninckx F, Thal DR, Rasschaert R, Bervoets C, Dankaerts W. Large- and small-fiber neuropathy in patients with Tarlov cysts. J Pain Res. 2022;15:193–202. doi:10.2147/JPR.S342759
7. Murphy K, Oaklander AL, Elias G, Kathuria S, Long DM. Treatment of 213 patients with symptomatic Tarlov cysts by CT-guided percutaneous injection of fibrin sealant. AJNR Am J Neuroradiol. 2015;37(2):373–379. doi:10.3174/ajnr.A4517
8. Sharma M, SirDeshpande P, Ugiliweneza B, Dietz N, Boakye M. A systematic comparative outcome analysis of surgical versus percutaneous techniques in the management of symptomatic sacral perineural (Tarlov) cysts: a meta-analysis. J Neurosurg Spine. 2019;30(5):623–634. doi:10.3171/2018.10.SPINE18952
9. Potts MB, McGrath MH, Chin CT, Garcia RM, Weinstein PR. Microsurgical fenestration and paraspinal muscle pedicle flaps for the treatment of symptomatic sacral Tarlov cysts. World Neurosurg. 2016;86:233–242. doi:10.1016/j.wneu.2015.09.055
10. Baker M, Wilson M, Wallach S. Urogenital symptoms in women with Tarlov cysts. J Obstet Gynaecol Res. 2018;44(9):1817–1823. doi:10.1111/jog.13711
11. Hentzen C, Cabrilo I, Malladi P, et al. Sacral Tarlov cysts: neurophysiology abnormalities and correlation with pelvic sensory and visceral symptoms. Eur J Neurol. 2023;30(9):2838–2848. doi:10.1111/ene.15869
12. Feigenbaum F, Parks SE, Martin MP, Ross TD, Kupanoff KM. Surgical intervention is associated with improvement in health-related quality of life outcomes in patients with symptomatic sacral Tarlov cysts: results from a prospective longitudinal cohort study. World Neurosurg. 2024;187:e189–e198. doi:10.1016/j.wneu.2024.04.065
13. Oaklander AL, Sharma S, Kessler K, Price BH. Persistent genital arousal disorder: a special sense neuropathy. Pain Rep. 2020;5(1):e801. doi:10.1097/PR9.0000000000000801
14. Feigenbaum F, Boone K. Persistent genital arousal disorder caused by spinal meningeal cysts in the sacrum: successful neurosurgical treatment. Obstet Gynecol. 2015;126(4):839–843. doi:10.1097/AOG.0000000000001060
15. Komisaruk BR, Lee HJ. Prevalence of sacral spinal (Tarlov) cysts in persistent genital arousal disorder. J Sex Med. 2012;9(8):2047–2056. doi:10.1111/j.1743-6109.2012.02765.x
16. Marino D, Carluccio MA, Di Donato I, et al. Tarlov cysts: clinical evaluation of an Italian cohort of patients. Neurol Sci. 2013;34(9):1679–1682. doi:10.1007/s10072-013-1321-0
17. Henderson FC, Austin C, Benzel E, et al. Neurological and spinal manifestations of the Ehlers–Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):195–211. doi:10.1002/ajmg.c.31549
18. Hulens M, Rasschaert R, Vansant G, Stalmans I, Bruyninckx F, Dankaerts W. The link between idiopathic intracranial hypertension, fibromyalgia, and chronic fatigue syndrome: exploration of a shared pathophysiology. J Pain Res. 2018;11:3129–3140. doi:10.2147/JPR.S186878
19. Maxwell AJ, Wardly D. The complex path to intracranial hypertension and CSF leak in those with hypermobility and dysautonomia; the theory of spiky-leaky syndrome. J MAR Pediatr. 2024;5(3):2–86.
20. Higgins JNP, Pickard JD. A paradigm for chronic fatigue syndrome: caught between idiopathic intracranial hypertension and spontaneous intracranial hypotension; caused by cranial venous outflow obstruction. Fatigue. 2021;9(3):139–147. doi:10.1080/21641846.2021.1956223
21. Masri A, Jaafar A, Noman R, Gharaibeh A, Ababneh OH. Intracranial hypertension in children: etiologies, clinical features, and outcome. J Child Neurol. 2015;30(12):1562–1568. doi:10.1177/0883073815574332
22. Keren T, Lahat E. Pseudotumor cerebri as a presenting symptom of acute sinusitis in a child. Pediatr Neurol. 1998;19(2):153–154. doi:10.1016/S0887-8994(98)00035-6
23. Garcia-Perez A, Espino M, Barrio A, et al. Pseudotumor cerebri associated with maxillary sinusitis: clinico-pathological study. Rev Neurol. 2000;31(1):45–48.
24. Matach G, Cartry G, Al Hussein H, Desrats L, Ghalayini A, Di Nolfo M. Idiopathic intracranial hypertension and sphenoid sinusitis: is there any relationship? J Fr Ophthalmol. 2007;30(Supplement 2):589.
25. Tawfik KO, Stevens SM, Mihal D, et al. Radiographic evidence of occult intracranial hypertension in patients with Ménière’s disease. Otolaryngol Head Neck Surg. 2017;157(2):260–268. doi:10.1177/0194599817699401
26. Çoban K, Aydın E, Özlüoğlu LN. Audio-vestibular findings in increased intracranial hypertension syndrome. J Int Adv Otol. 2017;13(1):100–104. doi:10.5152/iao.2016.2626
27. Pan DW, Vanstrum E, Doherty JK. Idiopathic intracranial hypertension: implications for the otolaryngologist. Otolaryngol Clin North Am. 2022;55(3):579–594. doi:10.1016/j.otc.2022.02.005
28. Ranieri A, Cavaliere M, Sicignano S, Falco P, Cautiero F, De Simone R. Endolymphatic hydrops in idiopathic intracranial hypertension: prevalence and clinical outcome after lumbar puncture. Preliminary data. Neurol Sci. 2017;38(Suppl 1):193–196. doi:10.1007/s10072-017-2895-8
29. Wall M, Kupersmith MJ, Kieburtz KD, et al. The idiopathic intracranial hypertension treatment trial clinical profile at baseline. JAMA Neurol. 2014;71(6):693–701. doi:10.1001/jamaneurol.2014.133
30. Midtlien JP, Curry BP, Chang E, Kiritsis NR, Aldridge JB, Fargen KM. Characterizing a new clinical phenotype: the co-existence of cerebral venous outflow and connective tissue disorders. Front Neurol. 2023;14:1305972. doi:10.3389/fneur.2023.1305972
31. Higgins JNP, Pickard JD, Lever AML. Chronic fatigue syndrome and idiopathic intracranial hypertension: different manifestations of the same disorder of intracranial pressure? Med Hypotheses. 2017;105:6–9. doi:10.1016/j.mehy.2017.06.014
32. Bragée B, Michos A, Drum B, Fahlgren M, Szulkin R, Bertilson BC. Signs of intracranial hypertension, hypermobility, and craniocervical obstructions in patients with myalgic encephalomyelitis/chronic fatigue syndrome. Front Neurol. 2020;11:828. doi:10.3389/fneur.2020.00828
33. Stillman M, Fouad-Tarazi F, Zhou L, et al. Autonomic dysfunction among migraineurs with and without complaints of orthostatic intolerance: evidence for small fiber nerve damage. Ann Head Med. 2021;60(1):1–16.
34. De Simone R, Ranieri A. The role of intracranial hypertension in the chronification of migraine. Neurol Sci. 2015;36(S1):S23–S28. doi:10.1007/s10072-015-2164-7
35. Ak AK, Sarıtas AS, Batum M, Gemici YI, Karakaş B, Çelebisoy N. Cognıtıve functıons in idiopathic intracranial hypertensıon. Acta Neurol Belg. 2024;124(6):1823–1830. doi:10.1007/s13760-024-02550-9
36. Hulens M, Dankaerts W, Rasschaert R, Bruyninckx F, De Mulder P, Bervoets C. The link between empty sella syndrome, fibromyalgia, and chronic fatigue syndrome: the role of increased cerebrospinal fluid pressure. J Pain Res. 2023;16:205–219. doi:10.2147/JPR.S394321
37. Bershad EM, Urfy MZ, Calvillo E, et al. Marked olfactory impairment in idiopathic intracranial hypertension. J Neurol Neurosurg Psychiatry. 2014;85(9):959–964. doi:10.1136/jnnp-2013-307232
38. Muhlbauer Avni M, Yosha-Orpaz N, Konen O, Goldenberg-Cohen N, Straussberg R. Association of pediatric idiopathic intracranial hypertension with olfactory performance. Eur J Paediatr Neurol. 2021;30:162–169. doi:10.1016/j.ejpn.2020.09.006
39. Mallery RM, Friedman DI, Liu GT. Headache and the pseudotumor cerebri syndrome. Curr Pain Headache Rep. 2014;18(9):446. doi:10.1007/s11916-014-0446-z
40. Ali A, Santiago RB, Isidor J, et al. Debilitating trigeminal neuralgia secondary to idiopathic intracranial hypertension. Heliyon. 2023;9(9):e19756. doi:10.1016/j.heliyon.2023.e19756
41. Tseng MT, Pan CL, Hsieh ST. Overview of small fiber neuropathy. In: Hsieh ST, Anand P, Gibbons CH, Sommer C, editors. Small Fiber Neuropathy and Related Syndromes: Pain and Neurodegeneration. Singapore: Springer; 2019:3–10.
42. Gemignani F, Bellanova MF, Saccani E, Pavesi G. Non-length-dependent small fiber neuropathy: not a matter of stockings and gloves. Muscle Nerve. 2022;65(1):10–28. doi:10.1002/mus.27379
43. Devigili G, Cazzato D, Lauria G. Clinical diagnosis and management of small fiber neuropathy: an update on best practice. Expert Rev Neurother. 2020;20(9):967–980. doi:10.1080/14737175.2020.1794825
44. Galosi E, Falco P, Di Pietro G, et al. The diagnostic accuracy of the small fiber neuropathy symptoms inventory questionnaire (SFN-SIQ) for identifying pure small fiber neuropathy. J Peripher Nerv Syst. 2022;27(4):283–290. doi:10.1111/jns.12513
45. Kalangara JP, Galor A, Levitt RC, Felix ER, Alegret R, Sarantopoulos CD. Burning eye syndrome: do neuropathic pain mechanisms underlie chronic dry eye? Pain Med. 2016;17(4):746–755. doi:10.1093/pm/pnv070
46. Lauria G, Majorana A, Borgna M, et al. Trigeminal small-fiber sensory neuropathy causes burning mouth syndrome. Pain. 2005;115(3):332–337. doi:10.1016/j.pain.2005.03.028
47. Privitera R, Anand P. Visceral pain and hypersensitivity disorders. In: Hsieh ST, Anand P, Gibbons CH, Sommer C, editors. Small Fiber Neuropathy and Related Syndromes: Pain and Neurodegeneration. Singapore: Springer; 2019:131–139.
48. O’Neill F, Marshall A, Ferdousi M, Malik RA. Corneal confocal microscopy detects small-fiber neuropathy in burning mouth syndrome: a cross-sectional study. J Oral Facial Pain Headache. 2019;33(3):337–341. doi:10.11607/ofph.2338
49. Mozafarpour S, Chen A, Mogica JAP, et al. Urodynamic autonomic bladder dysfunction in women with complex chronic pelvic pain is associated with small fiber polyneuropathy. Neurourol Urodyn. 2022;41(1):482–489. doi:10.1002/nau.24858
50. Matthews CA, Deveshwar SP, Evans RJ, Badlani G, Walker SJ. Small fiber polyneuropathy as a potential therapeutic target in interstitial cystitis/bladder pain syndrome. Int Urogynecol J. 2019;30(11):1817–1820. doi:10.1007/s00192-019-04011-x
51. Gemignani F, Brindani F, Vitetta F, Marbini A. Restless legs syndrome and painful neuropathy-retrospective study. A role for nociceptive deafferentation? Pain Med. 2009;10(8):1481–1486. doi:10.1111/j.1526-4637.2009.00732.x
52. Üçeyler N, Sommer C. Fibromyalgia syndrome: a disease of the small nerve fibers? Z Rheumatol. 2015;74(6):490–492. doi:10.1007/s00393-014-1546-1
53. Oaklander AL, Herzog ZD, Downs HM, Klein MM. Objective evidence that small-fiber polyneuropathy underlies some illnesses currently labeled as fibromyalgia. Pain. 2013;154(11):2310–2316. doi:10.1016/j.pain.2013.06.001
54. Levine TD. Small fiber neuropathy: disease classification beyond pain and burning. J Cent Nerv Syst Dis. 2018;10:1179573518771703. doi:10.1177/1179573518771703
55. Johnson SA, Shouman K, Shelly S, et al. Small fiber neuropathy incidence, prevalence, longitudinal impairments, and disability. Neurology. 2021;97(22):e2236–e2247. doi:10.1212/WNL.0000000000012894
56. Lindberg L, Brinth LS, Bergmann ML, et al. Autonomic nervous system activity in primary Raynaud’s phenomenon: heart rate variability, plasma catecholamines and [123I]MIBG heart scintigraphy. Clin Physiol Funct Imaging. 2022;42(2):104–113. doi:10.1111/cpf.12737
57. Oaklander AL, Nolano M. Scientific advances in and clinical approaches to small-fiber polyneuropathy: a review. JAMA Neurol. 2019;76(10):1240–1251. doi:10.1001/jamaneurol.2019.2917
58. Basantsova NY, Starshinova AA, Dori A, Zinchenko YS, Yablonskiy PK, Shoenfeld Y. Small-fiber neuropathy definition, diagnosis, and treatment. Neurol Sci. 2019;40(7):1343–1350. doi:10.1007/s10072-019-03871-x
59. Brookes ST, Donovan JL, Wright M, Jackson S, Abrams P. A scored form of the Bristol female lower urinary tract symptoms questionnaire: data from a randomized controlled trial of surgery for women with stress incontinence. Am J Obstet Gynecol. 2004;191(1):73–82. doi:10.1016/j.ajog.2003.12.027
60. Bovenschen HJ, Janssen MJ, Van Oijen MG, Laheij RJ, Van Rossum LG, Jansen JB. Evaluation of a gastrointestinal symptoms questionnaire. Dig Dis Sci. 2006;51(9):1509–1515. doi:10.1007/s10620-006-9120-6
61. Lauria G, Cornblath DR, Johansson O, et al. EFNS guidelines on the use of skin biopsy in the diagnosis of peripheral neuropathy. Eur J Neurol. 2005;12(10):747–758. doi:10.1111/j.1468-1331.2005.01260.x
62. Collongues N, Samama B, Schmidt-Mutter C, et al. Quantitative and qualitative normative dataset for intraepidermal nerve fibers using skin biopsy. PLoS One. 2018;13(1):e0191614. doi:10.1371/journal.pone.0191614
63. Lauria G, Bakkers M, Schmitz C, et al. Intraepidermal nerve fiber density at the distal leg: a worldwide normative reference study. J Peripher Nerv Syst. 2010;15(3):202–207. doi:10.1111/j.1529-8027.2010.00271.x
64. Sun JJ, Wang ZY, Teo M, et al. Comparative outcomes of the two types of sacral extradural spinal meningeal cysts using different operation methods: a prospective clinical study. PLoS One. 2013;8(12):e83964. doi:10.1371/journal.pone.0083964
65. Paulsen RD, Call GA, Murtagh FR. Prevalence and percutaneous drainage of cysts of the sacral nerve root sheath (Tarlov cysts). Am J Neuroradiol. 1994;15(2):293–297.
66. Yang AI, Rinehart CD, McShane BJ, Hitti FL, Welch WC. Growth of lumbosacral perineural (Tarlov) cysts: a natural history analysis. Neurosurgery. 2020;86(1):88–92. doi:10.1093/neuros/nyy586
67. Weerasuriya A, Mizisin AP. The blood-nerve barrier: structure and functional significance. Methods mol Biol. 2011;686:149–173.
68. Godel T, Pham M, Heiland S, Bendszus M, Baumer P. Human dorsal-root-ganglion perfusion measured in-vivo by MRI. Neuroimage. 2016;141:81–87. doi:10.1016/j.neuroimage.2016.07.030
69. Hulens M, Dankaerts W, Rasschaert R, et al. Hydrocephalus associated with multiple Tarlov cysts. Med Hypotheses. 2019;130:109293. doi:10.1016/j.mehy.2019.109293
70. Haase J. Papilledema associated with a sacral intraspinal cyst. Surg Neurol. 1976;6(6):360–362.
71. Oaklander AL. Tarlov cysts. Neurosurg Focus. 2012;32(4):E9. doi:10.3171/2012.1.FOCUS11374
72. Chiang MC, Hsieh PC, Hsieh ST. Neuropathic pain in small fiber neuropathy. In: Hsieh ST, Anand P, Gibbons C, Sommer C, editors. Small Fiber Neuropathy and Related Syndromes: Pain and Degeneration. Singapore: Springer; 2019:153–164.
73. Baron R, Hans G, Dickenson AH. Peripheral input and its importance for central sensitization. Ann Neurol. 2013;74(5):630–636. doi:10.1002/ana.24017
74. Lauria G, Faber CG, Cornblath DR. Skin biopsy and small fibre neuropathies: facts and thoughts 30 years later. J Neurol Neurosurg Psychiatry. 2022;93(9):915–918. doi:10.1136/jnnp-2021-327742
75. Hulens M, Bruyninckx F, Dankaerts W, Vansant G, De Mulder PA. Electromyographic abnormalities associated with symptomatic sacral Tarlov cysts. Pain Pract. 2016;16(5):E81–E88. doi:10.1111/papr.12441
76. Smith DT. Cystic formations associated with human spinal nerve roots. J Neurosurg. 1961;18(5):654. doi:10.3171/jns.1961.18.5.0654
77. Voyadzis JM, Bhargava P, Henderson FC. Tarlov cysts: a study of 10 cases with review of the literature. J Neurosurg. 2001;95(1):25–32. doi:10.3171/spi.2001.95.1.0025
78. Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008;17(6):794–819. doi:10.1007/s00586-008-0602-4
79. Sencan S, Kenis-Coskun O, Demir FGU, Cuce I, Ercalık T, Gunduz OH. Ganglion Impar block improves neuropathic pain in coccygodynia: a preliminary report. Neurol Neurochir Pol. 2018;52(5):612–617. doi:10.1016/j.pjnns.2018.08.006
80. Nathan ST, Fisher BE, Roberts CS. Coccydynia: a review of pathoanatomy, aetiology, treatment and outcome. J Bone Joint Surg Br. 2010;92(12):1622–1627. doi:10.1302/0301-620X.92B12.25486
81. Gomatos EL, Dulebohn SC, Rehman A. Sensory neuropathy. In: StatPearls. Treasure Island, FL: StatPearls Publishing LLC.; 2024.
82. Komisaruk BR, Goldstein I. Persistent genital arousal disorder: current conceptualizations and etiologic mechanisms. Curr Sex Health Rep. 2017;9(4):177–182. doi:10.1007/s11930-017-0122-5
83. Gehlen M, Kurtcuoglu V, Daners MS. Is posture-related craniospinal compliance shift caused by jugular vein collapse? A theoretical analysis. Fluids Barriers CNS. 2017;14(1):5. doi:10.1186/s12987-017-0053-6
84. Wostyn P, Audenaert K, De Deyn PP. The Valsalva maneuver and Alzheimer’s disease: is there a link? Curr Alzheimer Res. 2009;6(1):59–68. doi:10.2174/156720509787313943
85. Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8–26. doi:10.1002/ajmg.c.31552
86. Hulens M, Rasschaert R, Dankaerts W, Stalmans I, Vansant G, Bruyninckx F. Spinal fluid evacuation may provide temporary relief for patients with unexplained widespread pain and fibromyalgia. Med Hypotheses. 2018;118:55–58. doi:10.1016/j.mehy.2018.06.017
87. De Simone R, Ranieri A. Commentary: idiopathic intracranial hypertension without papilledema (IIHWOP) in chronic refractory headache. Front Neurol. 2019;10:39. doi:10.3389/fneur.2019.00039
88. Bartels RH, Van Overbeeke JJ. Lumbar cerebrospinal fluid drainage for symptomatic sacral nerve root cysts: an adjuvant diagnostic procedure and/or alternative treatment? Technical case report. Neurosurgery. 1997;40(4):861–864. doi:10.1097/00006123-199704000-00044
89. Takemori T, Kakutani K, Maeno K, Akisue T, Kurosaka M, Nishida K. Symptomatic perineural cyst: report of two cases treated with cyst-subarachnoid shunts. Eur Spine J. 2014;23:S267–S270.
90. Rodrigues T, Rodrigues M, Suriano I, Zymberg S. Idiopathic intracranial hypertension associated with symptomatic perineural cysts: presentation of two cases. World Neurosurg. 2018;119:17–19. doi:10.1016/j.wneu.2018.07.198
91. Chen L, Elias G, Yostos MP, Stimec B, Fasel J, Murphy K. Pathways of cerebrospinal fluid outflow: a deeper understanding of resorption. Neuroradiology. 2015;57(2):139–147. doi:10.1007/s00234-014-1461-9
92. Bachert C, Van Cauwenberge P, Olbrecht J, Van Schoor J. Prevalence, classification and perception of allergic and nonallergic rhinitis in Belgium. Allergy. 2006;61(6):693–698. doi:10.1111/j.1398-9995.2006.01054.x
93. Bono F, Curcio M, Rapisarda L, et al. Cerebrospinal fluid pressure-related features in chronic headache: a prospective study and potential diagnostic implications. Front Neurol. 2018;9:1090. doi:10.3389/fneur.2018.01090
94. Steffensen AB, Edelbo BL, Barbuskaite D, et al. Nocturnal increase in cerebrospinal fluid secretion as a circadian regulator of intracranial pressure. Fluids Barriers CNS. 2023;20(1):49. doi:10.1186/s12987-023-00451-2
95. Yri HM, Fagerlund B, Forchhammer HB, Jensen RH. Cognitive function in idiopathic intracranial hypertension: a prospective case-control study. BMJ Open. 2014;4(4):e004376. doi:10.1136/bmjopen-2013-004376
96. Zur D, Naftaliev E, Kesler A. Evidence of multidomain mild cognitive impairment in idiopathic intracranial hypertension. J Neuroophthalmol. 2015;35(1):26–30. doi:10.1097/WNO.0000000000000199
97. Moosa A, Joy MA, Kumar A. Extensive radiculopathy: another false localising sign in intracranial hypertension. J Neurol Neurosurg Psychiatry. 2004;75(7):1080–1081.
98. Groves MD, McCutcheon IE, Ginsberg LE, Kyritsis AP. Radicular pain can be a symptom of elevated intracranial pressure. Neurology. 1999;52(5):1093–1095. doi:10.1212/WNL.52.5.1093
99. Santinelli R, Tolone C, Toraldo R, Canino G, De Simone A, D’Avanzo M. Familial idiopathic intracranial hypertension with spinal and radicular pain. Arch Neurol. 1998;55(6):854–856. doi:10.1001/archneur.55.6.854
100. Bortoluzzi M, Di Lauro L, Marini G. Benign intracranial hypertension with spinal and radicular pain. Case Report J Neurosurg. 1982;57(6):833–836.
101. Kincaid O, Rowin J. Intracranial hypertension causing polyradiculopathy and late or absent F-waves. J Neurol Neurosurg Psychiatry. 2006;77(12):1384–1386. doi:10.1136/jnnp.2006.092387
102. Obeid T, Awada A, Mousali Y, Nusair M, Muhayawi S, Memish S. Extensive radiculopathy: a manifestation of intracranial hypertension. Eur J Neurol. 2000;7(5):549–553. doi:10.1046/j.1468-1331.2000.t01-1-00099.x
103. Round R, Keane JR. The minor symptoms of increased intracranial pressure: 101 patients with benign intracranial hypertension. Neurology. 1988;38(9):1461–1464. doi:10.1212/WNL.38.9.1461
104. Arsava EM, Uluc K, Nurlu G, Kansu T. Electrophysiological evidence of trigeminal neuropathy in pseudotumor cerebri. J Neurol. 2002;249(11):1601–1602. doi:10.1007/s00415-002-0866-2
105. Sánchez-Manso JC, Gujarathi R, Varacallo M. Autonomic dysfunction. In: StatPearls. Treasure Island, FL: StatPearls Publishing LLC.; 2024.
106. Myers RR, Murakami H, Powell HC. Reduced nerve blood flow in edematous neuropathies: a biomechanical mechanism. Microvasc Res. 1986;32(2):145–151. doi:10.1016/0026-2862(86)90050-6
107. Rydevik BL, Myers RR, Powell HC. Pressure increase in the dorsal root ganglion following mechanical compression. Closed compartment syndrome in nerve roots. Spine. 1989;14(6):574–576. doi:10.1097/00007632-198906000-00004
108. Lim VM, Khanna R, Kalinkin O, Castellanos ME, Hibner M. Evaluating the discordant relationship between Tarlov cysts and symptoms of pudendal neuralgia. Am J Obstet Gynecol. 2019;222(1):70.e1–e6. doi:10.1016/j.ajog.2019.07.021
109. Naderi S. Surgical approaches in symptomatic Tarlov cysts. World Neurosurg. 2016;86:20–21. doi:10.1016/j.wneu.2015.10.044
110. Godel T, Köhn A, Muschol N, et al. Dorsal root ganglia in vivo morphometry and perfusion in female patients with Fabry disease. J Neurol. 2018;265(11):2723–2729. doi:10.1007/s00415-018-9053-y
111. Brenaut E, Marcorelles P, Genestet S, Ménard D, Misery L. Pruritus: an underrecognized symptom of small-fiber neuropathies. J Am Acad Dermatol. 2015;72(2):328–332. doi:10.1016/j.jaad.2014.10.034
112. Sommer C, Üçeyler N. Small fiber pathology in pain syndromes. In: Hsieh ST, Anand P, Gibbons CH, Sommer C, editors. Small Fiber Neuropathy and Related Syndromes: Pain and Neurodegeneration Singapore. Springer; 2019:121–130.
113. Hulens M, Bruyninckx F, Dankaerts W, et al. High prevalence of perineural cysts in patients with fibromyalgia and chronic fatigue syndrome. Pain Med. 2021;22(4):883–890. doi:10.1093/pm/pnaa410
114. Kaspiris A, Zafiropoulou C. Growing pains in children: epidemiological analysis in a Mediterranean population. Jt Bone Spine. 2009;76(5):486–490. doi:10.1016/j.jbspin.2009.09.001
115. Haab F, Richard F, Amarenco G, et al. Comprehensive evaluation of bladder and urethral dysfunction symptoms: development and psychometric validation of the urinary symptom profile (USP) questionnaire. Urology. 2008;71(4):646–656. doi:10.1016/j.urology.2007.11.100
116. Ashwini DL, Raju TR. Autonomic nervous system and control of visual function. Ann Neurosci. 2023;30(3):151–153. doi:10.1177/09727531231176119
117. Fernández-Cuadros ME, Martín-Martín LM, Albaladejo-Florín MJ, et al. Sensitivity of the sympathetic skin response and scintigraphy in the diagnosis of complex regional pain syndrome. Rehabilitation. 2023;58(1):100807.
118. Fernández Cuadros ME, Martín-Martín LM, Albaladejo-Florín MJ, et al. Overactive bladder, lack of habituation, and central sensitisation: the sympathetic skin response as a possible diagnostic marker and neuromodulation as a treatment. Neurol Perspect. 2023;3(1):100112. doi:10.1016/j.neurop.2023.100112
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.