")
Back to Journals » Journal of Pain Research » Volume 18
Hippocampal Subfields Related to Cognitive Decline and Peripheral TIM-3 Levels in Elderly with Knee Osteoarthritis
Authors Zhao B, Lian X, Zeng P, Wang Y, Cai G, Chen R, Liu J, Chen L
Received 21 October 2024
Accepted for publication 12 March 2025
Published 30 March 2025 Volume 2025:18 Pages 1697—1709
DOI https://doi.org/10.2147/JPR.S496944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Baoru Zhao,1,* Xiaowen Lian,2,* Peiling Zeng,1,* Yajun Wang,1 Guiyan Cai,1 Ruilin Chen,1 Jiao Liu,1,3– 6 Lidian Chen1,4– 6
1College of Rehabilitation Medicine, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People’s Republic of China; 2Affiliated Rehabilitation Hospital, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People’s Republic of China; 3School of Traditional Chinese Medicine, Capital Medical University, Beijing, People’s Republic of China; 4National-Local Joint Engineering Research Center of Rehabilitation Medicine Technology, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People’s Republic of China; 5Traditional Chinese Medicine Rehabilitation Research Center of State Administration of Traditional Chinese Medicine, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People’s Republic of China; 6National-Local Laboratory of Orthopedics & Traumatology of Traditional Chinese Medicine and Rehabilitation (Fujian University of Traditional Chinese Medicine), Ministry of Education, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiao Liu; Lidian Chen, College of Rehabilitation Medicine, Fujian University of Traditional Chinese Medicine, 1 Qiuyang Road, Minhou Shangjie, Fuzhou, Fujian, 350122, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Knee osteoarthritis (KOA) has been linked to increased cognitive decline risk, but the specific mechanisms underlying this phenomenon remain unclear. Research suggests neuroimaging changes and chronic low-grade inflammation may play key roles as common pathways linking osteoarthritis (OA) to cognitive decline.
Patients and Methods: This cross-sectional study recruited 36 individuals diagnosed with KOA and 25 healthy controls (HCs). Cognition was assessed using the Montreal Cognitive Assessment (MoCA) and the Digit Cancellation Test (DCT). The gray matter volume of 12 hippocampal subfields and the serum TIM-3 levels were also measured.
Results: KOA patients had significantly lower MoCA scores (P < 0.01) and fewer correct responses on the DCT (P < 0.01). They also exhibited a larger volume of the right hippocampal tail (FDR-corrected P = 0.010) and a smaller volume of the right hippocampal fissure (FDR-corrected P = 0.036). Correlation analysis revealed that the volume of the right hippocampal tail was associated with the number of correct responses on the DCT (r = − 0.356, P = 0.049). Additionally, a smaller volume of the left hippocampal fissure was linked to higher serum TIM-3 levels (r = − 0.404, P = 0.030) in KOA patients.
Conclusion: The hippocampal tail and hippocampal fissure exhibited reduced volume in KOA patients, and these changes were associated with alterations in attention and serum TIM-3 levels, respectively. These findings suggest a potential link between KOA and cognitive decline through inflammation and neuroscience, offering a theoretical basis for further study. Meanwhile, serum TIM-3 and right hippocampal fissure/tail volume might be potential biomarkers for detecting cognitive decline in KOA patients. Further studies are necessary for the investigation of this possibility.
Keywords: cognitive decline, knee osteoarthritis, hippocampal subfields, TIM-3
Graphical Abstract:

Introduction
Knee osteoarthritis (KOA) is a degenerative disease and imposes a substantial burden on individuals’ daily functioning due to its high prevalence, incidence, and disability, especially in elder adults.1–3 Meta-analysis showed that OA has a higher risk of cognitive decline and dementia.4 Rapidly cognitive decline, a primary symptom of dementia, is a prognostic factor for the exacerbation of KOA symptoms.5
Neuroimaging evidence indicated that cognitive decline was associated with structural changes in the brain.6 The hippocampus, a key component of the limbic system, has been suggested as a sensitive biomarker for cognitive decline.7 This complex structure comprised multiple subfields, each performing distinct cognitive functions. For instance, the posterior hippocampus (including the hippocampal tail) served as a critical region for local detailed memories,8 while the subiculum played a significant role in spatial navigation, particularly inefficiently binding complex spatial information.9 Volume loss in the subiculum had been linked to the progression of dementia,10 and an enlarged hippocampal fissure had been observed in mild cognitive impairment, an early stage of Alzheimer’s disease.11 These findings highlighted the importance of examining all hippocampal subregions to fully understand their roles in cognitive decline.
Furthermore, neuroimaging findings have provided evidence for structural modifications occurring in the hippocampus of individuals diagnosed with KOA. Prior studies have documented a decrease in volume observed bilaterally across both hippocampus among KOA patients12–15 while also highlighting an accelerated rate of decline specifically within the hippocampal region for those affected by osteoarthritis compared to unaffected individuals.16 Nevertheless, these investigations predominantly concentrated on alterations in the global hippocampal volume, thereby leaving uncertainties regarding the precise patterns of modification within distinct subfields of the KOA-affected hippocampus and their association with cognitive decline.
Chronic low-grade inflammation has been recognized as a common pathway linking osteoarthritis (OA) and cognitive decline.17 This inflammation was not limited to knee OA but had been observed across other types of OA. OA patients, including those with knee OA, often exhibited increased synovial inflammation and elevated levels of pro-inflammatory cytokines, which could spread throughout the body via the bloodstream or lymphatic system.18 Chronic low-grade inflammation has also been identified as a hallmark of cognitive decline.19 In response to Aβ deposition, microglia, and astrocytes became activated, triggering a neuroinflammatory response that could be exacerbated by peripheral inflammation.20 Peripheral inflammation such as those associated with joint inflammation might have damaged the central nervous system through various mechanisms, including disruption of the blood-brain barrier21 and interactions with the gut-brain axis.22 The convergence of these inflammatory factors likely played a significant role in cognitive decline among OA patients.23
T-cell immunoglobulin and mucin-domain containing-3 protein (TIM-3), a transmembrane protein expressed on the surface of differentiated Th1 cells, is crucial in the release of proinflammatory cytokines.24 Higher serum levels of TIM-3 have been reported in individuals with KOA, specifically in a certain genotype.25 Elevated expression of TIM-3 has been observed in inflammatory brain tissue.26 TIM-3 can promote microglial activation and disrupt hippocampal neurogenesis.27 A negative correlation between specific proinflammatory cytokines in blood serum and cognitive function has been documented.28 We hypothesize that an association may exist between structural alterations in the hippocampal subfields and serum levels of TIM-3.
This cross-sectional case-control study compared cognitive performance between individuals with knee osteoarthritis (KOA) and healthy controls (HCs). The researchers collected gray matter volume data and serum TIM-3 samples to investigate the association among hippocampal subfields, peripheral inflammation, and cognitive decline in KOA. To explore the overlapping factors of cognitive decline and inflammation, correlation analyses were conducted between TIM-3 levels and affected brain regions in KOA patients. The hypothesis was that cognitive decline in KOA was closely linked to hippocampal subfield volumes and serum TIM-3 levels.
Materials and Methods
Participants
A total of 61 participants, including 36 with KOA and 25 HCs, were recruited from local community centers in Fuzhou through the use of posters, WeChat, and phone calls. The diagnosis of KOA was made by a rheumatologist from the Affiliated Rehabilitation Hospital of Fujian University of Traditional Chinese Medicine based on the criteria established by the American College of Rheumatology.29 This study was approved by the Medical Ethics Committee at the same hospital. Informed consent was obtained from all participants before the research. The study was initiated only after the participants had signed the consent forms.
The inclusion criteria for individuals with KOA were as follows: (i) age between 40 and 70, and right-handed; (ii) diagnosis of chronic KOA in either the right or left knee based on the diagnostic criteria of the American Rheumatism Association; (iii) Kellgren-Lawrence grade 2 or 3 confirmation through X-ray;30 (iv) Body mass index (BMI) ≤30kg/m2. Individuals with KOA were excluded if they met any of the following exclusion criteria: (i) history of knee surgery within the past 6 months or intra-articular corticosteroid injection within the past 3 months; (ii) knee pain caused by rheumatic or other inflammatory diseases; (iii) presence of abnormal mental state or inability to cooperate with assessments; (iv) MRI contraindications such as dentures, porcelain teeth, and pacemakers; (v) Fasting blood sample contraindications such as bleeding disorders.
The HC control participants met any of the following inclusion criteria: (i) aged between 40 and 70 years old and right-handed; (ii) free from any pain disorders; (iii) BMI≤30kg/m2. Exclusion criteria for healthy controls were as follows: (i) presence of abnormal mental state or inability to cooperate with the assessment; (ii) MRI contraindications, such as dentures, porcelain teeth, and pacemakers.
Clinical Data Collection
We recorded demographic characteristics such as age, gender, body mass index (BMI), and years of education. The Chinese version of the Brief Pain Inventory (BPI) scale was used to measure the average pain intensity in KOA individuals over the past 24 hours.31 The BPI employed a 0 to 10 numeric scale for rating items, where 0 indicated “no pain” and 10 indicated “pain as bad as you can imagine”. Additionally, the BPI assessed the impact of pain on patients’ ability to function, using the same 0 to 10 scale, where 0 indicated “no interference” and 10 indicated “complete interference”. In our study, the BPI scores reflected the pain intensity experienced by KOA individuals over the past 24 hours.
Additionally, the Knee Injury and Osteoarthritis Outcome Score (KOOS) was used to assess various aspects of knee function in both KOA patients and HCs, with a score range from zero to one hundred. The KOOS comprised five subscales-pain, symptoms, activities of daily living (ADLs), sport and recreation function (Sport), and knee-related quality of life (Quality of life).32 For the pain subscale, higher scores indicated lower pain intensity. For the other four subscales, higher scores reflected better functioning.
Cognitive Assessments
The Montreal Cognitive Assessment (MoCA)33 was employed to assess overall cognitive function, encompassing 7 domains including visual-executive function, naming, attention, verbal fluency, abstraction, recall, and orientation. MoCA scores ranged from 0 to 30 with higher scores indicating superior cognitive function. Furthermore, the digit cancellation test (DCT) was administered to evaluate subjects’ attention,34,35 measuring both correct responses and omission and error rates.
Serum TIM-3 Levels Measurement
Fasting blood samples were collected from the antecubital veins of 36 individuals diagnosed with KOA. After clotting for 15 minutes at room temperature, serum was obtained by centrifugation at 3000×g for 10 minutes and immediately stored frozen at -80°C. Serum TIM-3 levels were quantified using an enzyme-linked immunosorbent assay following the manufacturer’s instructions (ELISA, ELISA kits: Huamei Biological Engineering Co. LTD, Wuhan, China). An ELISA reader (Bio Tek, Model ELX800, Winooski, VT, USA) was used to measure the absorbance of both TIM-3 standard and test samples.
MRI Data Acquisition
MRI data were acquired using an eight-channel phased-array head coil on a 3.0-T GE scanner (General Electric, Milwaukee, WI, USA). Participants were instructed to maintain wakefulness and immobility with their eyes closed during the scan. T1-weighted images were obtained with the following parameters: a flip angle of 15°, slice thickness of 1 mm, field of view (FOV) of 240 mm, and acquisition consisting of 160 slices.
MRI Data Processing
The T1-weighted images were processed using the FreeSurfer software (version 7.1.0, http://surfer.nmr.mgh.harvard.edu/). Hippocampal volume was extracted from the subcortical nucleus segmentation file of each subject generated by pre-processing based on Iglesias et al’s study,36 utilizing FreeSurfer software. To ensure accurate segmentation, individual subjects’ images were registered to the standard space provided by FreeSurfer. Following the hippocampus segmentation template available on the official website of FreeSurfer, each subject’s hippocampus was parcellated into 19 regions and subsequently combined into specific areas including the hippocampal tail, subiculum, cornu ammonis (CA) 1–4, hippocampal fissure, presubiculum, parasubiculum, molecular layer of dentate gyrus (GC-ML-DG), fimbria and hippocampal amygdala transition area (HATA).36 Notably, CA2 was consistently included within CA3.
Statistical Analysis
The statistical analysis was conducted using IBM SPSS Statistics software (version 25, Armonk, NY, United States). Shapiro–Wilk’s test was employed to assess the distribution of continuous variables. For normally distributed continuous variables, mean ± standard deviation (SD) was used for statistical description. For non-normally distributed continuous variables, the statistical description included the median and interquartile range (25-75th percentile). Qualitative values were presented as n (%) for the statistical description and a chi-square test was performed to compare between the two groups.
Demographic characteristics of individuals with KOA and healthy controls were compared using either the independent samples t-test (for variables with a normal distribution) or the Mann–Whitney U-test (for variables without a normal distribution).
A general linear model or generalized linear model was employed to assess the differences between groups in (i) BPI, KOOS subscales, and cognitive function while controlling for age, gender, and years of education; (ii) the volume of hippocampal subfields while adjusting for age, gender, years of education, and the volume of left/right whole hippocampus. The differences in the volume of the hippocampal subfields between groups were corrected for false discovery rate (FDR) with the Benjamini-Hochberg method.
The partial correlations were conducted to examine the associations between cognitive scores and hippocampal subfield volume while controlling for age, gender, years of education, and the volume of the left/right whole hippocampus. Additionally, cognitive scores were examined concerning KOOS subscales while controlling for age, gender, and years of education. Furthermore, the association between hippocampal subfield volume and serum levels of TIM-3 was investigated while controlling for age, gender, years of education, and the volume of the left/right whole hippocampus. A significance level of P < 0.05 was used with a two-tailed test.
Results
In our study, we initially screened 76 individuals for eligibility. Of these, 15 were excluded based on the following criteria: i) MRI contraindications (n=5); ii) A history of knee surgery within the past six months or intra-articular corticosteroid injection within the preceding three months (n=3); iii) Presence of pain in regions other than the knee (n=5); iv) BMI exceeding 30 kg/m² (n=2). After applying the inclusion and exclusion criteria, a total of 61 participants were included in the final analysis: 36 with knee osteoarthritis (KOA) and 25 healthy controls (HCs). The participant selection process is summarized in Figure S1.
Demographic Characteristics
There were no significant differences observed between individuals with KOA and HCs in terms of age, gender, BMI, and years of education (Table 1). Table 2 showed that KOA patients experienced significantly higher pain intensity compared to HCs, as indicated by the pain subscale of the KOOS. The BPI scores also reflected the pain levels experienced by KOA individuals.
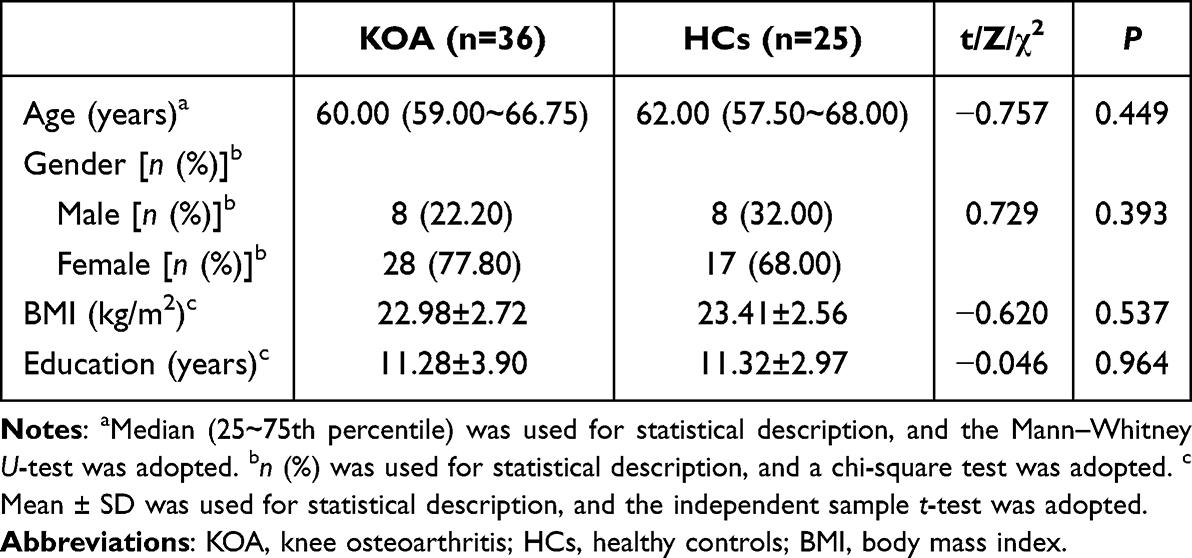 |
Table 1 Demographic Characteristics of Study Participants |
 |
Table 2 Comparisons of Clinical and Cognitive Assessments in KOA Individuals and HCs |
Comparisons of Clinical and Cognitive Assessments
The individuals with KOA demonstrated significantly poorer performance in terms of symptoms (P < 0.001), ADL(P < 0.001), sports (P < 0.001), and quality of life (P < 0.001) compared to the HCs, as presented in Table 2. Furthermore, the KOA group exhibited significantly lower scores on the MoCA test, indicating worse global cognitive function (P < 0.001). Additionally, they displayed a reduced number of correct responses in the DCT, suggesting attention decline (P < 0.001).
Comparisons of Hippocampal Subfield Volume
In the left hippocampal subfields, patients with KOA exhibited a significantly smaller volume of the hippocampal fissure compared to HCs (P = 0.044), as demonstrated in Table 3 and Figure 1A. In the right hippocampal subfields, KOA patients showed a significantly larger volume of the hippocampal tail (P = 0.003) and significantly smaller volumes of both the subiculum (P = 0.038) and hippocampal fissure (P < 0.001), as shown in Table 3 and Figure 1B. After corrected by FDR with the Benjamini-Hochberg method, significant differences were still observed in the right hippocampal tail (FDR-corrected P = 0.010) and the right hippocampal fissure (FDR-corrected P = 0.036) between KOA and HCs. No significant group differences were observed in other areas of the hippocampal subfields. To better illustrate the spatial relationships of hippocampal subfields, we included the visualization of hippocampal subfield segmentations for a single subject in Figure S2.
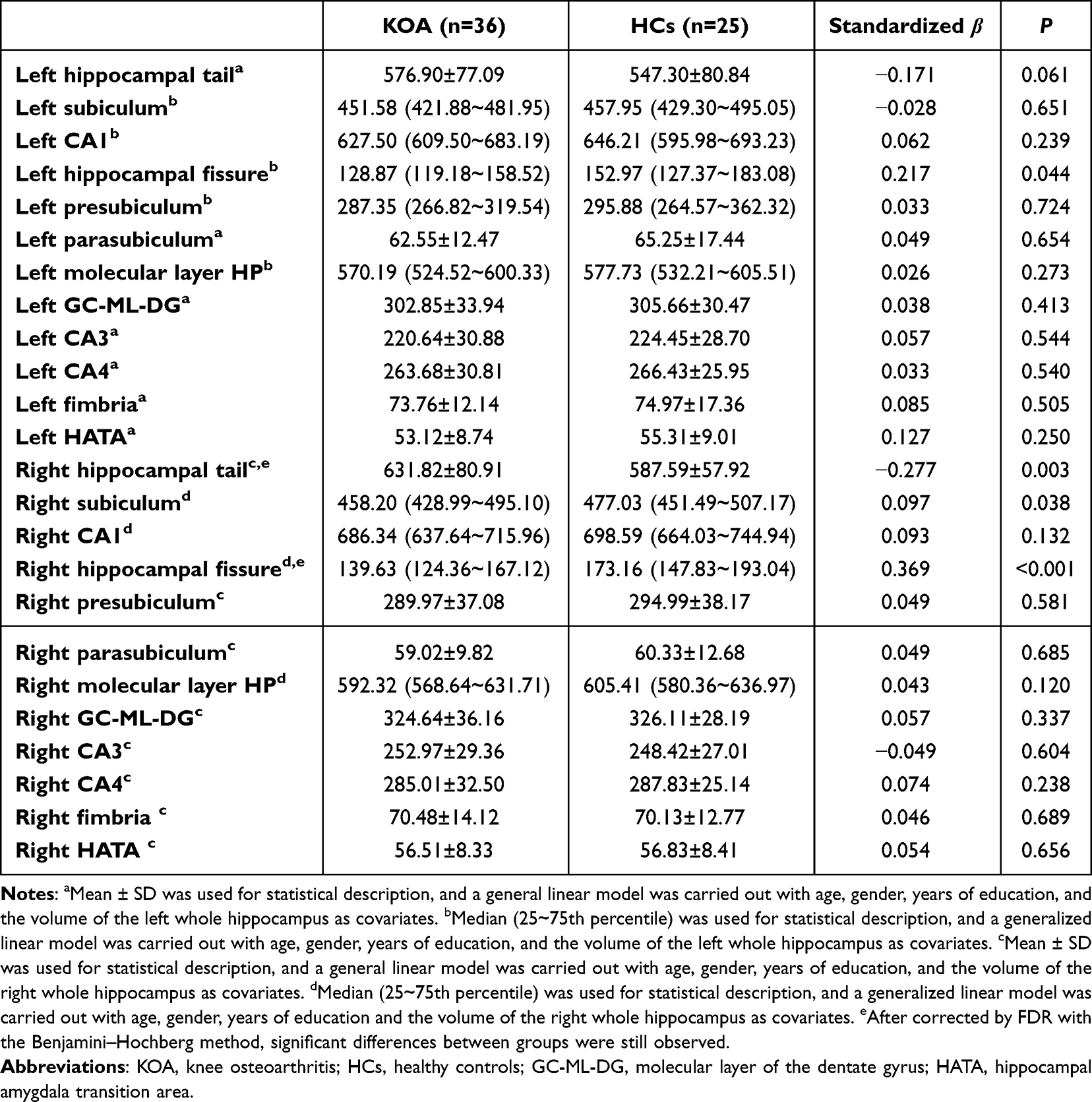 |
Table 3 Comparisons of Hippocampal Subfield Volume in KOA Individuals and HCs |
 |
Figure 1 Radar charts of the hippocampal subfield volume in KOA individuals and HCs. Abbreviations: KOA, knee osteoarthritis; HCs, healthy controls; GC-ML-DG, molecular layer of the dentate gyrus; HATA, hippocampal amygdala transition area. Notes: (A) In the left hippocampal subfields, a smaller hippocampal fissure volume was shown in KOA compared to HCs (P = 0.044). (B) In the right hippocampal subfields, a larger volume of the hippocampal tail (P = 0.003), a smaller volume of the subiculum (P = 0.038), and the hippocampal fissure (P < 0.001) were shown in KOA. The unit of volume is cubic millimeters. *P < 0.05, **P < 0.001. |
Partial Correlation Analyses
In individuals with KOA, there was a significant negative correlation between the volume of the right hippocampal tail and the number of correct responses in the DCT (r = −0.356, P = 0.049) (Figure 2A). Among HCs, the volume of the left hippocampal fissure showed a significant negative association with the MoCA scores (r = −0.554, P = 0.009) (Figure 2B), while both the volume of the right hippocampal tail (r = 0.643, P = 0.002) (Figure 2C) and right subiculum (r = 0.441, P = 0.045) (Figure 2D) exhibited significant positive associations with MoCA scores. Table S1 also showed the result of partial correlation between cognitive scores and hippocampal subfield volume.
 |
Figure 2 Partial correlations in KOA individuals and HCs. Abbreviations: DCT-Correct responses, the number of digits of correct responses on the digit cancellation test; MoCA, the Montreal Cognitive Assessment; KOOS-ADL, activities of daily living on the Knee injury and Osteoarthritis Outcome Score; TIM-3, T-cell immunoglobulin and mucin-domain containing-3 protein. Notes: (A) In KOA individuals, the volume of the right hippocampal tail was negatively correlated with the number of correct responses in DCT (r = −0.356, P = 0.049). (B) In HCs, the volume of the left hippocampal fissure was negatively associated with MoCA scores (r = −0.554, P = 0.009). (C) Also in HCs, the volume of the right hippocampal tail showed a positive correlation with MoCA scores (r = 0.643, P = 0.002). (D) The volume of the right subiculum in HCs was positively associated with MoCA scores (r = 0.441, P = 0.045). (E) In KOA individuals, KOOS-ADL scores were positively associated with MoCA scores (r = 0.444, P = 0.014). (F) In KOA, the volume of the left hippocampal fissure was negatively correlated with TIM-3 levels (r = −0.404, P = 0.030). |
The partial correlation analysis revealed a significant positive association between the scores on the KOOS subtest of ADL and MoCA scores (r = 0.444, P = 0.014) in individuals with KOA (Table S2, Figure 2E). Moreover, there was a negative correlation observed between the volume of left hippocampal fissure and TIM-3 levels (r = −0.404, P = 0.030) in KOA patients (Table S3, Figure 2F). No other significant associations were found in this study.
Discussion
This study compared cognitive function and hippocampal subfield volumes between individuals with KOA and HCs. The findings revealed that individuals with KOA exhibited significant cognitive decline, particularly in global cognitive function and attention, which was associated with impaired ADL. The study observed that KOA patients had a larger volume in the right hippocampal tail and a smaller volume in the right hippocampal fissure, after applying FDR correction. In the KOA group, we observed that a larger volume in the right hippocampal tail was linked to fewer correct responses in the digit cancellation test. However, significant correlations were observed between the volume of the right hippocampal tail/subiculum, the left hippocampal fissure, and the MoCA scores in HCs rather than in KOA. Additionally, we found a significant negative association between the serum levels of TIM-3 and the volume of the left hippocampal fissure. The results indicate that changes in certain subfields of the hippocampus and peripheral TIM-3 levels may be significant factors in the cognitive decline of individuals with KOA.
The analysis of cognitive differences between groups revealed that individuals with KOA exhibited poorer cognitive performance compared to HCs, consistent with previous research findings.37,38 Additionally, our study identified a significant decline in attention among KOA patients. Previous studies have suggested that attention decline in the elderly is associated with chronic pain,39 which is one of the most common symptoms experienced by KOA patients.40 It has been proposed that chronic pain may compete with other attention-demanding stimuli and impair top-down attentional control mechanisms, consequently leading to attention impairment.41
In our study, KOA individuals showed a smaller volume of bilateral hippocampal fissure and a larger volume of right hippocampal tail, indicating hypertrophy within the hippocampus. The hippocampal tail is part of the posterior hippocampus.42 The hippocampal fissure is a space that remains between the dentate gyrus, CA fields, and subiculum of the hippocampus.43 The increased volume of hippocampal subfields may be associated with abnormal activation of their function. A previous study confirmed that individuals with KOA exhibited higher fALFF values in the bilateral hippocampus,12 demonstrating that the hippocampus is overactivated in KOA. In addition, expansion of microglial territory and volume,44 more dendritic branching, increased spine density,45 and inflammatory edema46 may explain volume changes in hippocampal subfields at the microscopic level. Further research is warranted to elucidate the molecular mechanisms underlying these distinct changes.
Our study found a significant association between attention decline in KOA and a larger volume of the right hippocampal tail, suggesting a relationship between the right hippocampal tail and attention impairment in this population. The hippocampal tail is primarily activated during episodic memory retrieval, relying on internally focused attention rather than encoding.47,48 Additionally, it is worth noting that attentional systems tend to exhibit lateralization towards the right hemisphere,49 which aligns with our research findings.
Interestingly, our findings revealed a strong and significant positive relationship between the volume of the right hippocampal tail and MoCA scores in the HC group, as well as between the right hippocampal subiculum and MoCA scores. However, these correlations were not observed in the KOA group. Additionally, in the KOA group, the correlation between the volume of the left hippocampal fissure and MoCA scores also disappeared. These findings suggest that there may be other confounding factors at play, influencing the relationship between hippocampal subfields and cognition in KOA patients.
One possible explanation for the disappearance of these correlations in the KOA group is the presence of other factors that can impact the relationship between hippocampal subfields and cognitive function. For instance, previous studies have reported that factors such as sensitization,50 tolerance,51 and duration of pain52 are associated with changes in gray matter volume. These factors may introduce complexity and disrupt the simple linear relationship between gray matter volume and global cognition as measured by MoCA.
These findings highlight the need for further investigation to better understand the underlying mechanisms and potential confounding factors that contribute to the relationship between hippocampal subfields and cognition in the context of KOA. By elucidating these factors, we can gain a more comprehensive understanding of the complex interplay between structural brain changes and cognitive function in KOA patients.
Regarding the relationship between pain intensity and cognition in KOA patients, our study did not observe a significant association. These findings are consistent with previous research, such as the study conducted by Bell et al,53 which also reported no significant correlation between pain intensity and cognitive performance. However, it is worth noting that some studies did find a dose-dependent relationship between pain intensity and cognitive impairment, suggesting that higher levels of pain intensity may increase the risk of developing cognitive deficits.54,55 Therefore, further investigations are warranted to explore how different levels of pain intensity may influence the association between cognition and volume changes in hippocampal subfields. In KOA patients, long-term peripheral pain has been observed to lead to central sensitization, which is characterized by increased sensitivity of primary nociceptors and a disrupted balance between pain facilitation and inhibition.56 This sensitization process is characterized by the impairment of descending antinociceptive mechanisms and the enhancement of pain facilitation pathways.57 Orthopedic interventions have been clinically recognized for their efficacy in alleviating the pain abnormalities associated with this central sensitization.58
Interestingly, our study did reveal a significant relationship between global cognition and activities of daily living in KOA patients, which were influenced by the presence of KOA-related pain in various life scenarios. These findings highlight the multifaceted impact of KOA pain on cognitive function and daily functioning, underscoring the need for comprehensive management strategies that address both pain and cognitive impairments in KOA patients.
Furthermore, we observed atrophy in the right hippocampal subiculum. The subiculum, which lies beneath the dentate gyrus and the CA fields, plays a crucial role in connecting the hippocampal system and cerebral cortex.9,59 Gupta et al discovered that mice with induced osteoarthritis and dementia exhibited a reduction in neuronal count.60 Additionally, researchers have reported that a smaller volume of the subiculum is associated with an increased risk of incident dementia and suggests progression of Alzheimer’s disease based on the rate of volume loss.61,62 We propose that the atrophy observed in our study within the right hippocampal subiculum may be linked to neuronal reduction. Further investigations are necessary to validate our hypothesis.
As a prominent cytokine involved in inflammation and immune response, TIM-3 may have an impact on hippocampal plasticity. Although serum levels of HCs were not measured in our study, a previous investigation reported higher serum levels of TIM-3 in specific genotypes among individuals with KOA.25 In our current study, elevated levels of TIM-3 in KOA patients showed a significant association with reduced volume of the left hippocampal fissure (hypertrophy surrounding the left hippocampal fissure). Recent research suggests that TIM-3 could serve as a crucial link between neuroinflammation and microglia polarization, which is implicated in impaired neurogenesis within the hippocampus.63,64 We hypothesize that microglia polarization might induce the release of proinflammatory cytokines such as TIM-3,64 subsequently impacting neural precursor proliferation within the hippocampus65 in KOA. Furthermore, prior evidence has indicated that higher levels of certain proinflammatory cytokines in blood serum are associated with poorer cognition,28 suggesting a potential connection between proinflammatory cytokines and cognitive function. Large-scale studies are needed to validate this potential relationship specifically within individuals affected by KOA.
Maintaining awareness of cognitive decline in KOA patients had significant practical implications. For instance, health education plays a pivotal role in the conservative management of elderly patients with KOA or hip OA.58 However, cognitive decline in these patients might weaken the efficacy of rehabilitation. Therefore, future rehabilitation plans for elderly patients with OA should have incorporated cognitive support strategies to enhance overall treatment outcomes.
Notably, a limitation of this study was that it did not account for the impact of lifestyle differences on OA patients. Increased physical activity has been shown to reduce inflammation and oxidative damage,66 whereas sleep fragmentation and intermittent hypoxia may exacerbate inflammation and lead to cognitive dysfunction.67 However, evidence linking lifestyle to OA was inconsistent. Although some studies suggest that sleep disturbances may be associated with OA, further evidence is needed.68 In addition, associations between physical activity and molecular biomarkers might be weak or absent.69 Therefore, future studies should investigate the specific effects of lifestyle factors on cognitive function, hippocampal subregion volume, and inflammatory factors in patients with OA. This research might help clarify the complex relationships among these variables and provide a more comprehensive understanding of how lifestyle influences OA.
The present study has certain limitations. First, the inadequate sample size included in this study may lead to unstable research findings. Second, our cross-sectional design precludes longitudinal observation of hippocampal subfield progression in KOA. Future investigations should involve large-scale, multi-center, and longitudinal studies to explore both structural and functional changes occurring within hippocampal subfields during KOA progression. Additionally, examining correlations between these changes and cognition as well as serum biomarkers would be beneficial.
Conclusion
In summary, our study has yielded compelling evidence of cognitive decline and the volume of hippocampal subfields among patients with KOA. The hippocampal tail and hippocampal fissure exhibited reduced volume in KOA patients, and these changes were associated with alterations in attention and serum TIM-3 levels, respectively. This finding offers a theoretical basis for understanding cognitive decline in KOA. Further research is warranted to elucidate the potential role of TIM-3 in driving changes within different hippocampal subfields. Meanwhile, serum TIM-3 and right hippocampal fissure/tail volume might be potential biomarkers for detecting cognitive decline in KOA patients. Further studies are necessary for the investigation of this possibility.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Medical Ethics Committee at the Affiliated Rehabilitation Hospital of Fujian University of Traditional Chinese Medicine. Written informed consent has been obtained from the patients to publish this paper.
Acknowledgment
We thank the Second Affiliated Hospital of Fujian University of Traditional Chinese Medicine and the Affiliated Rehabilitation Hospital of Fujian University of Traditional Chinese Medicine for their assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Fujian Collaborative Innovation Center for Rehabilitation Technology, Traditional Chinese Medicine Rehabilitation Research Center of State Administration of Traditional Chinese Medicine, and National-Local Joint Engineering Research Center of Rehabilitation Medicine Technology [China, grant number X2012001-Collaboration and X2021001-Collaboration].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Q, Wang S, Lin J, Zhang Y. The burden for knee osteoarthritis among Chinese elderly: estimates from a nationally representative study. Osteoarthritis Cartilage. 2018;26(12):1636–1642. doi:10.1016/J.JOCA.2018.07.019
2. Chen H, Wu J, Wang Z, et al. Trends and patterns of knee osteoarthritis in China: a longitudinal study of 17.7 Million adults from 2008 to 2017. Int J Environ Res Public Health. 2021;18(16):8864. doi:10.3390/ijerph18168864
3. Collaborators GO. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/s2665-9913(23)00163-7
4. Guo R, Ou YN, Hu HY, Ma YH, Tan L, Yu JT. The association between osteoarthritis with risk of dementia and cognitive impairment: a meta-analysis and systematic review. J Alzheimers Dis. 2022;89(4):1159–1172. doi:10.3233/jad-220568
5. van Dijk GM, Veenhof C, Spreeuwenberg P, et al. Prognosis of limitations in activities in osteoarthritis of the hip or knee: a 3-year cohort study. Arch Phys Med Rehabil. 2010;91(1):58–66. doi:10.1016/J.APMR.2009.08.147
6. Wang X, Huang W, Su L, et al. Neuroimaging advances regarding subjective cognitive decline in preclinical Alzheimer’s disease. Mol Neurodegener. 2020;15(1):55. doi:10.1186/s13024-020-00395-3
7. Mak E, Gabel S, Mirette H, et al. Structural neuroimaging in preclinical dementia: from microstructural deficits and grey matter atrophy to macroscale connectomic changes. Ageing Res Rev. 2017;35:250–264. doi:10.1016/j.arr.2016.10.001
8. Sekeres MJ, Winocur G, Moscovitch M. The hippocampus and related neocortical structures in memory transformation. Neurosci Lett. 2018;680:39–53. doi:10.1016/j.neulet.2018.05.006
9. Matsumoto N, Kitanishi T, Mizuseki K. The subiculum: unique hippocampal hub and more. Neurosci Res. 2019;143:1–12. doi:10.1016/j.neures.2018.08.002
10. Izzo J, Andreassen OA, Westlye LT, van der Meer D. The association between hippocampal subfield volumes in mild cognitive impairment and conversion to Alzheimer’s disease. Brain Res. 2020;1728:146591. doi:10.1016/j.brainres.2019.146591
11. Wang N, Zhang L, Yang H, Luo X, Fan G. Do multiple system atrophy and Parkinson’s disease show distinct patterns of volumetric alterations across hippocampal subfields? An exploratory study. Eur Radiol. 2019;29(9):4948–4956. doi:10.1007/s00330-019-06043-9
12. Guo H, Wang Y, Qiu L, et al. Structural and functional abnormalities in knee osteoarthritis pain revealed with multimodal magnetic resonance imaging. Front Hum Neurosci. 2021;15:783355. doi:10.3389/fnhum.2021.783355
13. Mao CP, Bai ZL, Zhang XN, Zhang QJ, Zhang L. Abnormal subcortical brain morphology in patients with knee osteoarthritis: a cross-sectional study. Front Aging Neurosci. 2016;8:3. doi:10.3389/FNAGI.2016.00003/PDF
14. Baliki MN, Schnitzer TJ, Bauer WR, Apkarian AV. Brain morphological signatures for chronic pain. PLoS One. 2011;6(10):e26010. doi:10.1371/journal.pone.0026010
15. Salazar-Méndez J, Cuyul-Vásquez I, Viscay-Sanhueza N, et al. Structural and functional brain changes in people with knee osteoarthritis: a scoping review. PeerJ. 2023;11:e16003. doi:10.7717/peerj.16003
16. Li X, Tong Q, Gao J, Liu C, Initiative AsDN, Liu Y. Osteoarthritis was associated with a faster decline in hippocampal volumes in cognitively normal older people. Front Aging Neurosci. 2020;12:190. doi:10.3389/fnagi.2020.00190
17. Umoh IO, Dos Reis HJ, de Oliveira ACP. Molecular mechanisms linking osteoarthritis and Alzheimer’s disease: shared pathways, mechanisms and breakthrough prospects. Int J mol Sci. 2024;25(5):3044. doi:10.3390/ijms25053044
18. Sanchez-Lopez E, Coras R, Torres A, Lane NE, Guma M. Synovial inflammation in osteoarthritis progression. Nat Rev Rheumatol. 2022;18(5):258–275. doi:10.1038/s41584-022-00749-9
19. Gaikwad S, Senapati S, Haque MA, Kayed R. Senescence, brain inflammation, and oligomeric tau drive cognitive decline in Alzheimer’s disease: evidence from clinical and preclinical studies. Alzheimers Dement. 2024;20(1):709–727. doi:10.1002/alz.13490
20. Veitch DP, Weiner MW, Miller M, et al. The Alzheimer’s disease neuroimaging initiative in the era of Alzheimer’s disease treatment: a review of ADNI studies from 2021 to 2022. Alzheimers Dement. 2024;20(1):652–694. doi:10.1002/alz.13449
21. Culibrk RA, Hahn MS. The role of chronic inflammatory bone and joint disorders in the pathogenesis and progression of Alzheimer’s disease. Front Aging Neurosci. 2020;12:583884. doi:10.3389/fnagi.2020.583884
22. Gonzalez-Alvarez ME, Sanchez-Romero EA, Turroni S, Fernandez-Carnero J, Villafañe JH. Correlation between the altered gut microbiome and lifestyle interventions in chronic widespread pain patients: a systematic review. Medicina. 2023;59(2):256. doi:10.3390/medicina59020256
23. Al-Khazraji BK, Appleton CT, Beier F, Birmingham TB, Shoemaker JK. Osteoarthritis, cerebrovascular dysfunction and the common denominator of inflammation: a narrative review. Osteoarthritis Cartilage. 2018;26(4):462–470. doi:10.1016/j.joca.2018.01.011
24. Monney L, Sabatos CA, Gaglia JL, et al. Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease. Nature. 2002;415(6871):536–541. doi:10.1038/415536A
25. Chen J, Sun G, Chen F, Fang Y, Gates MH, Yang S. T-cell immunoglobulin domain and mucin domain 3 polymorphism affects cytokine expression in different cells and is associated with increased susceptibility to knee osteoarthritis. Gene. 2015;566(1):32–36. doi:10.1016/J.GENE.2015.04.024
26. Yu A, Zhang X, Li M, et al. Tim-3 enhances brain inflammation by promoting M1 macrophage polarization following intracerebral hemorrhage in mice. Int Immunopharmacol. 2017;53:143–148. doi:10.1016/j.intimp.2017.10.023
27. Chesnokova V, Pechnick RN, Wawrowsky K. Chronic peripheral inflammation, hippocampal neurogenesis, and behavior. Brain Behav Immun. 2016;58:1–8. doi:10.1016/j.bbi.2016.01.017
28. Stebbins RC, Edwards JK, Plassman BL, et al. Immune function, cortisol, and cognitive decline & dementia in an aging latino population. Psychoneuroendocrinology. 2021;133:105414. doi:10.1016/j.psyneuen.2021.105414
29. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum. 1986;29(8):1039–1049. doi:10.1002/art.1780290816
30. Holzer N, Salvo D, Marijnissen ACA, et al. Radiographic evaluation of posttraumatic osteoarthritis of the ankle: the Kellgren–Lawrence scale is reliable and correlates with clinical symptoms. Osteoarthritis Cartilage. 2015;23(3):363–369. doi:10.1016/j.joca.2014.11.010
31. Wang XS, Mendoza TR, Gao S, Cleeland CS. The Chinese version of the brief pain inventory (BPI-C): its development and use in a study of cancer pain. Pain. 1996;67(2):407–416. doi:10.1016/0304-3959(96)03147-8
32. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)—development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28(2):88–96. doi:10.2519/jospt.1998.28.2.88
33. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
34. Hatta T, Yoshizaki K, Ito Y, Mase M, Kabasawa H. Reliability and validity of the digit cancellation test: a brief screen of attention. Psychologia. 2012;55(4):246–256. doi:10.2117/psysoc.2012.246
35. Sala SD, Laiacona M, Spinnler H, Ubezio C. A cancellation test: its reliability in assessing attentional deficits in Alzheimer’s disease. Psychol Med. 1992;22(4):885–901. doi:10.1017/S0033291700038460
36. Iglesias JE, Augustinack JC, Nguyen K, et al. A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: application to adaptive segmentation of in vivo MRI. Neuroimage. 2015;115:117–137. doi:10.1016/j.neuroimage.2015.04.042
37. Kazim MA, Strahl A, Moritz S, Arlt S, Niemeier A. Chronic pain in osteoarthritis of the Hip is associated with selective cognitive impairment. Arch Orthop Trauma Surg. 2022;143:2189–2197. doi:10.1007/s00402-022-04445-x
38. Weber A, Mak SH, Berenbaum F, et al. Association between osteoarthritis and increased risk of dementia: a systemic review and meta-analysis. Medicine. 2019;98(10):e14355. doi:10.1097/MD.0000000000014355
39. van der Leeuw G, Leveille SG, Dong Z, et al. Chronic pain and attention in older community-dwelling adults. J Am Geriatr Soc. 2018;66(7):1318–1324. doi:10.1111/jgs.15413
40. Sharma L. Osteoarthritis of the Knee. N Engl J Med. 2021;384(1):51–59. doi:10.1056/NEJMcp1903768
41. Moriarty O, McGuire BE, Finn DP. The effect of pain on cognitive function: a review of clinical and preclinical research. Prog Neurobiol. 2011;93(3):385–404. doi:10.1016/j.pneurobio.2011.01.002
42. Bronen RA, Cheung G. Relationship of hippocampus and amygdala to coronal MRI landmarks. Magn Reson Imaging. 1991;9(3):449–457. doi:10.1016/0730-725x(91)90434-n
43. Kier EL, Kim JH, Fulbright RK, Bronen RA. Embryology of the human fetal hippocampus: MR imaging, anatomy, and histology. Am J Neuroradiol. 1997;18(3):525–532.
44. Hisaoka-Nakashima K, Ohata K, Yoshimoto N, et al. High-mobility group box 1-mediated hippocampal microglial activation induces cognitive impairment in mice with neuropathic pain. Exp Neurol. 2022;355:114146. doi:10.1016/j.expneurol.2022.114146
45. Metz AE, Yau HJ, Centeno MV, Apkarian AV, Martina M. Morphological and functional reorganization of rat medial prefrontal cortex in neuropathic pain. Proc Natl Acad Sci U S A. 2009;106(7):2423–2428. doi:10.1073/pnas.0809897106
46. Pomares FB, Funck T, Feier NA, et al. Histological underpinnings of grey matter changes in fibromyalgia investigated using multimodal brain imaging. J Neurosci. 2017;37(5):1090–1101. doi:10.1523/JNEUROSCI.2619-16.2016
47. Grady CL. Meta-analytic and functional connectivity evidence from functional magnetic resonance imaging for an anterior to posterior gradient of function along the hippocampal axis. Hippocampus. 2020;30(5):456–471. doi:10.1002/hipo.23164
48. Kim H. Encoding and retrieval along the long axis of the hippocampus and their relationships with dorsal attention and default mode networks: the HERNET model. Hippocampus. 2015;25(4):500–510. doi:10.1002/hipo.22387
49. Bartolomeo P, Seidel Malkinson T. Hemispheric lateralization of attention processes in the human brain. Curr Opin Psychol. 2019;29:90–96. doi:10.1016/J.COPSYC.2018.12.023
50. Pedersini P, Gobbo M, Bishop MD, Arendt-Nielsen L, Villafañe JH. Functional and structural neuroplastic changes related to sensitization proxies in patients with osteoarthritis: a systematic review. Pain Med. 2022;23(3):488–498. doi:10.1093/pm/pnab301
51. Melum TA, Vangberg TR, Johnsen LH, et al. Gray matter volume and pain tolerance in a general population: the Tromsø study. Pain. 2023;164(8):1750–1758. doi:10.1097/j.pain.0000000000002871
52. Tang Y, Ren C, Wang M, et al. Altered gray matter volume and functional connectivity in patients with herpes zoster and postherpetic neuralgia. Brain Res. 2021;1769:147608. doi:10.1016/j.brainres.2021.147608
53. Bell T, Franz CE, Kremen WS. Persistence of pain and cognitive impairment in older adults. J Am Geriatr Soc. 2022;70(2):449–458. doi:10.1111/jgs.17542
54. Smith L, López Sánchez GF, Shin JI, et al. Pain and mild cognitive impairment among adults aged 50 years and above residing in low- and middle-income countries. Aging Clin Exp Res. 2023;35(7):1513–1520. doi:10.1007/s40520-023-02434-7
55. van der Leeuw G, Ayers E, Leveille SG, Blankenstein AH, van der Horst HE, Verghese J. The effect of pain on major cognitive impairment in older adults. J Pain. 2018;19(12):1435–1444. doi:10.1016/j.jpain.2018.06.009
56. Nijs J, Lahousse A, Kapreli E, et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J Clin Med. 2021;10(15):3203. doi:10.3390/jcm10153203
57. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–s15. doi:10.1016/j.pain.2010.09.030
58. Martínez-Pozas O, Sánchez-Romero EA, Beltran-Alacreu H, et al. Effects of orthopedic manual therapy on pain sensitization in patients with chronic musculoskeletal pain: an umbrella review with meta-meta-analysis. Am J Phys Med Rehabil. 2023;102(10):879–885. doi:10.1097/phm.0000000000002239
59. Aggleton JP, Christiansen K. The subiculum: the heart of the extended hippocampal system. Prog Brain Res. 2015;219:65–82. doi:10.1016/bs.pbr.2015.03.003
60. Gupta DP, Lee Y, Choe Y, Kim K, Song GJ, Hwang S. Knee osteoarthritis accelerates amyloid beta deposition and neurodegeneration in a mouse model of Alzheimer’s disease. Mol Brain. 2023;16(1):1. doi:10.1186/s13041-022-00986-9
61. Evans TE, Adams HHH, Licher S, et al. Subregional volumes of the hippocampus in relation to cognitive function and risk of dementia. Neuroimage. 2018;178:129–135. doi:10.1016/J.NEUROIMAGE.2018.05.041
62. Zeng Q, Li K, Luo X, et al. Distinct atrophy pattern of hippocampal subfields in patients with progressive and stable mild cognitive impairment: a longitudinal MRI study. J Alzheimers Dis. 2021;79(1):237–247. doi:10.3233/JAD-200775
63. Chen ZQ, Yu H, Li HY, et al. Negative regulation of glial Tim-3 inhibits the secretion of inflammatory factors and modulates microglia to antiinflammatory phenotype after experimental intracerebral hemorrhage in rats. CNS Neurosci Ther. 2019;25(6):674–684. doi:10.1111/CNS.13100
64. Kohman RA, Rhodes JS. Neurogenesis, inflammation and behavior. Brain Behav Immun. 2013;27:22–32. doi:10.1016/j.bbi.2012.09.003
65. Fujioka H, Akema T. Lipopolysaccharide acutely inhibits proliferation of neural precursor cells in the dentate gyrus in adult rats. Brain Res. 2010;1352:35–42. doi:10.1016/J.BRAINRES.2010.07.032
66. El Assar M, Álvarez-bustos A, Sosa P, Angulo J, Rodríguez-Mañas L. Effect of physical activity/exercise on oxidative stress and inflammation in muscle and vascular aging. Int J Mol Sci. 2022;23(15):8713. doi:10.3390/ijms23158713
67. Liu X, Ma Y, Ouyang R, et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J Neuroinflammation. 2020;17(1):229. doi:10.1186/s12974-020-01905-2
68. Sánchez Romero EA, Martínez-Pozas O, García-González M, et al. Association between sleep disorders and sleep quality in patients with temporomandibular joint osteoarthritis: a systematic review. Biomedicines. 2022;10(9):2143. doi:10.3390/biomedicines10092143
69. Östlind E, Eek F, Stigmar K, Sant’Anna A, Ekvall Hansson E, Struglics A. Associations between physical activity, self-reported joint function, and molecular biomarkers in working age individuals with hip and/or knee osteoarthritis. Clin Med Insights Arthritis Musculoskelet Disord. 2022;15:11795441221081063. doi:10.1177/11795441221081063
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.