")
Back to Journals » Infection and Drug Resistance » Volume 18
HIV Transmission Misconceptions and Their Associated Factors Among Reproductive-Age Women in Somalia: Findings from a Nationwide Study
Authors Mohamud LA, Hassan-Kadle MA, Abdullahi HM , Ahmed AA
Received 29 December 2024
Accepted for publication 6 May 2025
Published 9 June 2025 Volume 2025:18 Pages 2929—2942
DOI https://doi.org/10.2147/IDR.S514775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Liban Ali Mohamud,1 Mohamed Abdulkadir Hassan-Kadle,2,3 Hamza Mohamed Abdullahi,4 Ahmed Ali Ahmed5
1Department of Statistics and Planning, SIMAD University, Mogadishu, Somalia; 2College of Medicine and Health Science, Abrar University, Mogadishu, Somalia; 3Center for Digestive and Liver Diseases, Waaberi Hospital, Mogadishu, Somalia; 4National HIV Program, Federal Ministry of Health, Mogadishu, Somalia; 5Somdoctor Health Services, Mogadishu, Somalia
Correspondence: Mohamed Abdulkadir Hassan-Kadle, Email [email protected]
Background: Human Immunodeficiency Virus (HIV) remains a significant public health challenge, particularly in low-resource settings, where limited knowledge contributes to its spread, especially among women facing socio-economic and educational barriers. This study examines the associations between misconceptions about HIV transmission and sociodemographic factors among Somali women. Identifying regions and groups with limited awareness will help prioritize targeted education and healthcare interventions, aligning with the National Strategic Plan (NSP).
Methods: A multivariable Bayesian logistic regression model was used to analyze data from the 2018– 2019 Somali Demographic and Health Survey (SDHS). This modeling approach was chosen for its ability to handle uncertainty and incorporate prior knowledge into the analysis. Bayesian adjusted odds ratios (BAORs) with 95% highest posterior density intervals (HPDIs) were calculated to determine significant associations between misconceptions and sociodemographic factors.
Results: The study found that 67.18% of women had misconceptions about HIV transmission. Significant factors associated with misconceptions included age, education, wealth, and internet usage. Women aged 30– 34 (BAOR = 0.94, 95% HPDI: 0.90– 0.98), 35– 39 (BAOR = 0.94, 95% HPDI: 0.90– 0.98), and 40– 44 (BAOR = 0.93, 95% HPDI: 0.89– 0.98), women with secondary education (BAOR = 0.92, 95% HPDI: 0.88– 0.95), women with higher education (BAOR = 0.84, 95% HPDI: 0.79– 0.88), women in the highest wealth quintile (BAOR = 0.90, 95% HPDI: 0.86– 0.95), and women who had never used the internet (BAOR = 1.06, 95% HPDI: 1.03– 1.09).
Conclusion: This study highlights the critical need for targeted interventions to reduce misconceptions about HIV transmission among Somali women. Policies should focus on educating younger women, promoting female education, implementing region-specific health interventions, and enhancing internet access and digital literacy, particularly in rural areas, to improve HIV knowledge and support public health efforts.
Keywords: HIV misconceptions, Somali women, digital literacy, bayesian analysis, highest posterior density interval, bayesian adjusted odds ratios, public health interventions
Introduction
The HIV remain significant global public health challenges particularly in low-income countries. HIV has infected approximately 88.4 million people since the start of the epidemic. About 42.3 million people have died of HIV since its recognition.1 As of 2023, there are about 39.9 million people living with HIV globally with more than 67% of them in sub-Saharan Africa (SSA) and its leading cause of death in AIDS related disease.2
Somalia has been struggling with the consequences of prolonged conflict since the collapse of its central government in 1991.3 This continuing instability has profoundly affected the nation’s political, social, and economic landscapes, with the healthcare sector among the most severely impacted. Systemic weaknesses in health infrastructure, compounded by limited resources, access to medical services and misinformation about HIV transmission have hindered effective responses to critical public health challenges, including misconceptions and gaps in HIV/AIDS awareness.4
Despite these challenges, Somalia reports one of the lowest HIV infection rates in Africa,5,6 a phenomenon largely attributed to its deeply rooted religious and cultural norms. The country’s strong Muslim identity and adherence to Islamic teachings play a significant role in shaping social behaviors, acting as protective factors against high-risk practices associated with HIV transmission. Additionally, the emphasis on familial and community cohesion reinforces these values, further contributing to the low prevalence of the disease.7
The first confirmed case of HIV in Somalia was identified in 1987 during a study conducted in Mogadishu. Among 287 serum samples collected from female sex workers, one tested positive for HIV antibodies—a finding first reported by Burans at the 4th International Conference on AIDS in Stockholm.8 Since then, Somalia has made strides in addressing the epidemic, including adopting the UNAIDS 90–90-90 targets to improve diagnosis, treatment, and viral suppression.9 Heterosexual transmission remains the primary mode of HIV spread, followed by perinatal transmission from mother to child.10
Since 2014, Somalia has been classified as a low-level HIV epidemic country. National prevalence rates have declined significantly, dropping from over 1% in 2013 to 0.10% in 2022. However, these rates remain geographically uneven, with prevalence among individuals aged 15–49—including women—standing at less than 0.1%.11 While progress has been made, continued efforts are needed to address regional disparities and sustain the gains achieved in HIV prevention and control.
Misconceptions about HIV/AIDS transmission remain a significant barrier to effective prevention and care, particularly in low-resource settings like Somalia. The virus is primarily spread through blood transfusions, contaminated needles, unsafe sexual intercourse, and mother-to-child transmission during childbirth or breastfeeding, as supported by studies.12
Such misunderstandings often stem from incorrect beliefs about transmission routes, fueling misinformation and stigmatization of those living with HIV. This, in turn, fosters discrimination and undermines prevention efforts, especially in developing nations like Somalia.13
According to a study conducted in Hargeisa, Somalia reported to 75%, 65%, 64% and 28% in semi nomadic population perceived that mosquito bites, sharing food, drinking contaminated water and handshaking or hugging respectively were assumed to be route of HIV/AIDS transmission.14 Moreover, according to research conducted in Somalia among the beliefs and practices of Somali citizens concerning HIV/AIDS showed that common misconception about the transmission of HIV in Somalia that it is primarily spread through adultery and other perceived immoral sexual practices.15 Furthermore, knowledge about HIV/AIDS in the Somali population has been reported as significantly insufficient, which contributes to the continuation of these misconceptions. Women of reproductive age are particularly vulnerable due to socio-cultural and economic factors, including limited education and limited healthcare services. To address this gap, our study assesses the prevalence of misconceptions regarding HIV/AIDS transmission among reproductive-age women in Somalia and identify associated risk factors.
Methods and Data
This study is cross-sectional in design and utilizes secondary data from SDHS conducted in 2018-2019 by the Ministry of Health (MOH) of the Federal Government of Somalia (FGS) and the Somali National Bureau of Statistics (NBS). This dataset is nationally representative and covers sixteen regions. However, due to security concerns, data from two regions (Lower Shabelle and Middle Juba) and two specific strata (Bay region) were excluded from the analysis16–18. For more detailed information on the sampling procedures and regional descriptions, readers are referred to the SDHS 2020 Report.
The target population for this study consisted of reproductive-aged women, defined as those aged 15 to 49 years. Initially, a comprehensive sample of 16,486 women was selected to ensure robust and representative findings. However, after a thorough data cleaning process, which excluded cases with missing or incomplete information, the final analytic sample was reduced to 8,246 women.
The outcome variable, misconceptions about HIV Transmission among reproductive-age women, was derived as a composite index based on responses from women aged 15 to 49 years in the 2018-2019 SDHS. The indicators assessed whether HIV could be transmitted through (i) mosquito bites, (ii) sharing food with a person who has AIDS, (iii) witchcraft or supernatural means. Responses were originally categorized as “No”, “Yes”, and “Don’t Know.” For analysis, they were recoded into a binary variable: women who answered “No” to all three questions were classified as having no misconceptions, while those who answered “Yes” to at least one was classified as having misconceptions. Respondents selecting “Don’t Know” were excluded to reduce ambiguity and avoid bias in the analysis, as we have a large sample that ensures sufficient statistical power without these uncertain responses. Numerous studies19,20 have utilized this methodology.
In our study, we incorporated several covariates that are commonly found in similar researches.13,19,21 The independent variables included sociodemographic factors such as age, region, residence, marital status, educational level, frequency of listening to radio, frequency of watching television, ever used internet and wealth index.
In this study, R software was used for data management and analysis. We began by generating descriptive statistics to assess the frequency and proportion of the dependent and sociodemographic variables, providing a comprehensive overview of the dataset as shown in Table 1. To explore the associations between misconceptions about HIV transmission and various sociodemographic factors, we applied multivariable Bayesian logistic regression analysis. Bayesian adjusted odds ratios (BAORs) with 95% highest posterior density interval (HPDI) were used to evaluate the strength and direction of the associations.
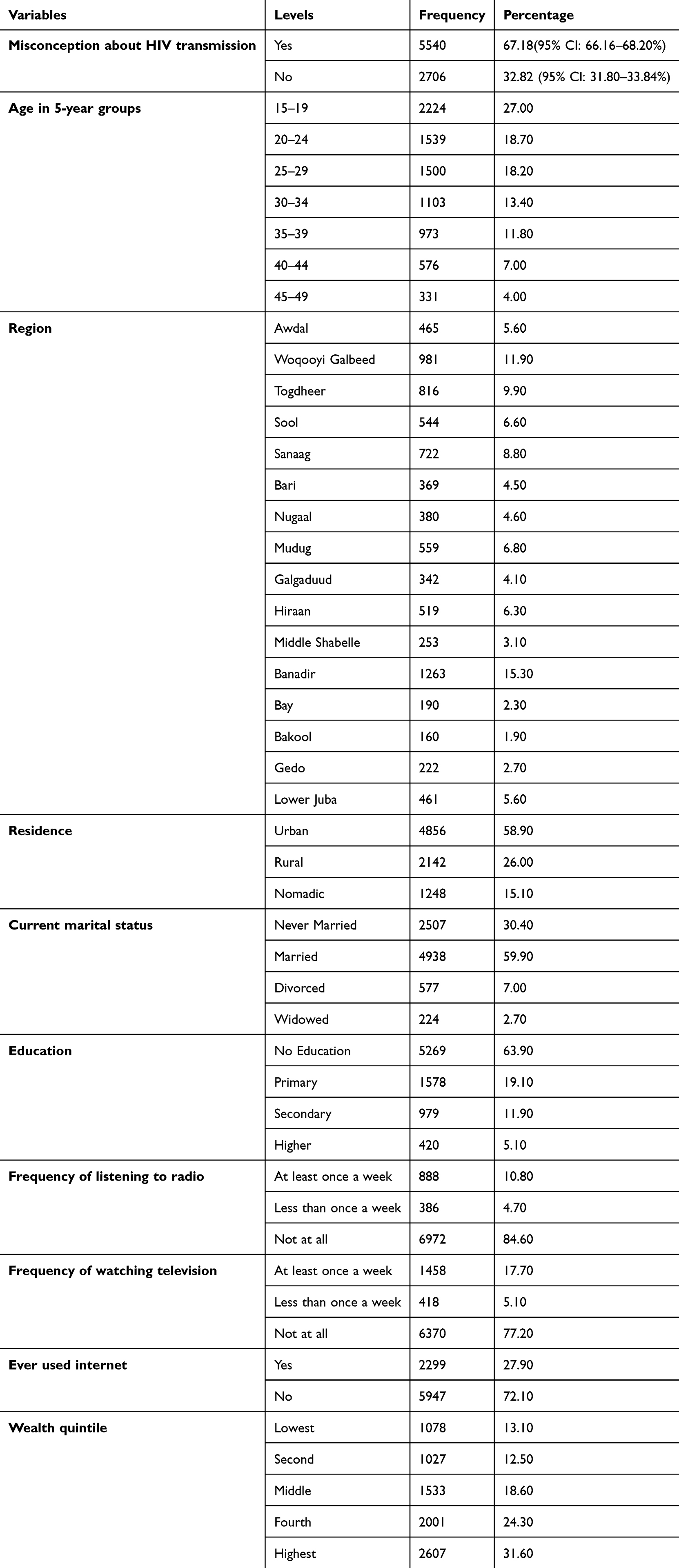 |
Table 1 Sociodemographic Profile of Participants |
Binary logistic regression is a special case of generalized linear models (GLMs) used when the response variable has two levels.22 In our study, the outcome variable, “ misconceptions about HIV transmission”, has two levels: “ no misconceptions coded as 0”, and “ having misconceptions”, coded as 1. Thus, binary logistic regression is appropriate for our study. Logistic regression uses the canonical link function,  . The frequentist logistic regression model is given below:
. The frequentist logistic regression model is given below:

where X is the vector the predictor variables and  is the vector of the regression Coefficient.
is the vector of the regression Coefficient.
Other link functions like probit and clog-log can also be used for binary data. The likelihood for the logistic regression model is:

In logistic regression, parameters are estimated using maximum likelihood estimation (MLE). Since MLE lacks a closed-form solution for β, iteratively reweighted least squares (IRWLS) is employed. IRWLS iteratively solves weighted least squares problems to approximate the MLE.
Statisticians have been debating the benefits of Bayesian and frequentist approaches to statistical inference for the past thirty years.23 Rather than preferring one approach over the other, both methods should be used when they are suitable.24 Recently, Bayesian methods have become more popular in biostatistical research due to their ability to incorporate prior information for better statistical estimation. The Bayesian approach considers parameters as random variables with their own probability distribution, whereas the frequentist approach treats them as fixed but unknown.25
In our study, we used Bayesian logistic regression to examine the relationship between predictor variables and the outcome variable. To do this, we constructed a likelihood function based on our observed sample presented in Eq.2 and then specified an appropriate prior distribution to represent our beliefs about the random and unknown parameters. By combining the prior information with the current sample data, we obtained an updated posterior distribution from which all statistical inferences were drawn. This approach allowed us to take into account both prior knowledge and current data in estimating the relationship between our variables of interest.
Bayesian inference for logistic regression requires priors on model parameters. Independent flat priors are commonly used as they allow the likelihood to dominate and fully characterize the posterior distribution. If no background knowledge is available, normal priors with a mean of zero and a very large variance are assigned to regression coefficients, ensuring minimal prior influence. These priors result in estimates driven primarily by the data, but in cases of limited data, they may lead to high uncertainty and wider credible intervals. We assume the independent random and unknown parameters; β0, β1, β2, β3, ,
,
 follows normal distribution with hyper parameters26
follows normal distribution with hyper parameters26  and
and  . Thus, we use non-informative normal priors for the regression coefficients β with mean αi and variance bi2, represented as follows:
. Thus, we use non-informative normal priors for the regression coefficients β with mean αi and variance bi2, represented as follows:

where  . The most frequently used choice of the value of hyper parameters is set mean µ is zero, and large variance σ is typically preferred to be considered as non-informative. In Bayesian Paradigm, precision
. The most frequently used choice of the value of hyper parameters is set mean µ is zero, and large variance σ is typically preferred to be considered as non-informative. In Bayesian Paradigm, precision  is adopted rather than the variance.24 In this study
is adopted rather than the variance.24 In this study  N (0,0.001). The posterior distribution is proportional to the product of the prior distribution and likelihood,
N (0,0.001). The posterior distribution is proportional to the product of the prior distribution and likelihood,  L(y/
L(y/ )
) . Therefore, from Eqs. 2 and 3, we have.
. Therefore, from Eqs. 2 and 3, we have.

Finding the posterior distribution from Eq.4 is highly complex. Therefore, we use the Gibbs sampler technique within the Markov Chain Monte Carlo (MCMC) simulation to approximate the posterior distribution. After running the MCMC simulation with 10000 iterations and a burn-in of 5,000 samples, the final result is 15,000 iterations with the first 5,000 samples being discarded. All statistical analyses were conducted in R (version 4.4), with MCMC output generated using the rjags package. There are a variety of statistical techniques used to evaluate the truthfulness of MCMC posterior estimates, but in this study, we will use Geweke diagnostic test and Markov Chain Monte Carlo standard error as convergence measures of MCMC result. Geweke proposed this diagnostic test for monitoring the convergence of the posterior mean of each parameter by using Z-test to compare the posterior means of sub-samples of MCMC output and concludes that this convergence measure is achieved when |Z| statistics of all posterior means variables is less than two.27,28 Additionally, the MCMC standard error of the posterior mean was used as a convergence diagnostic. If the MCMC standard error is less than 5% of its posterior standard deviation, then the posterior distribution has converged to its target distribution. To ensure accurate posterior estimates, the simulation should continue until this condition is met.28
Results
Table 1 presents the sociodemographic characteristics of participants. Regarding misconceptions about HIV transmission, 67.18% of women reported misconceptions (95% CI: 66.16–68.20%), while 32.82% demonstrated no misconceptions (95% CI: 31.80–33.84%). Regarding age distribution, most respondents were aged 15–19 years (27%), while the smallest group was 45–49 years (4%). In terms of regional representation, Banadir had the highest proportion (15.3%), whereas Bay (2.3%) and Bakool (1.9%) had the least. With respect to residence, the majority lived in urban areas (58.9%), followed by rural (26%) and nomadic (15.1%) settings. Regarding marital status and education, most participants were married (59.9%) and had no formal education (63.9%). In terms of media exposure, 84.6% did not listen to the radio weekly, and 77.2% did not watch TV weekly. Additionally, 27.9% had used the internet, while 72.1% had never accessed it. Lastly, concerning wealth distribution, 31.6% were in the highest quintile, compared to 13.1% in the lowest.
Table 2 presents the frequentist and Bayesian logistic regression analyses of factors associated with misconceptions about HIV transmission among Somali women aged 15–49 years. Since the frequentist and Bayesian results are very close, only Bayesian adjusted odds ratios (BAOR) are interpreted. A variable is considered significant if the value 1 is not included within the 95% highest posterior density interval (HPDI). The results indicate that age, region, education, wealth, and internet usage have significant associations with misconceptions about HIV transmission.
 |
Table 2 Frequentist and Bayesian Logistic Regression of the Factors Associated with Misconceptions About HIV Transmission Among Somali Women Aged 15–49 years |
Women aged 30–34 (BAOR = 0.94, 95% HPDI: 0.90–0.98), 35–39 (BAOR = 0.94, 95% HPDI: 0.90–0.98), and 40–44 (BAOR = 0.93, 95% HPDI: 0.89–0.98) exhibited lower odds of having misconceptions about HIV transmission by 6%, 6%, and 7%, respectively, compared to women aged 15–19 years. Regarding region, significant associations were found in several areas. Women in Sanaag (BAOR = 0.92, 95% HPDI: 0.87–0.97) had 8% lower odds of having misconceptions about HIV transmission compared to those in Awdal. Similarly, women in Bari (BAOR = 0.92, 95% HPDI: 0.86–0.97), Nugaal (BAOR = 0.87, 95% HPDI: 0.82–0.93), and Gedo (BAOR = 0.94, 95% HPDI: 0.87–1.01) exhibited lower odds of having misconceptions about HIV transmission by 8%, 13%, and 6%, respectively, compared to women in Awdal.
Regarding education, women with secondary education (BAOR = 0.92, 95% HPDI: 0.88–0.95) had 8% lower odds of having misconceptions about HIV transmission compared to those with no education. Similarly, women with higher education (BAOR = 0.84, 95% HPDI: 0.79–0.88) exhibited 16% lower odds of having misconceptions about HIV transmission compared to those with no education. Thus, the more educated women are, the fewer misconceptions they have about HIV transmission, and vice versa.
Furthermore, women in the fourth wealth quintile (BAOR = 0.95, 95% HPDI: 0.90–0.99) exhibited 5% lower odds of having misconceptions about HIV transmission compared to those in the lowest wealth quintile. Additionally, women in the highest wealth quintile (BAOR = 0.90, 95% HPDI: 0.86–0.95) showed 10% lower odds of having misconceptions compared to those in the lowest wealth quintile. Thus, the wealthier women are, the fewer misconceptions they have about HIV transmission, and vice versa.
Additionally, women who have never used the internet (BAOR = 1.06, 95% HPDI: 1.03–1.09) had 6% higher odds of having misconceptions about HIV transmission compared to those who have ever used the internet. Thus, the more women use the internet, the fewer misconceptions they have about HIV transmission, and vice versa.
It is important to check for convergence and representative sampling from the posterior distribution before using Bayesian logistic regression, we use MCMC Convergence Diagnostics. Table 3 shows MCMC errors for each covariate are less than 5% of their posterior standard deviation, indicating precise and converged posterior estimates. Additionally, the Geweke test results confirm convergence to stationary distributions, as all posterior mean |Z| statistics of predictors are below two.
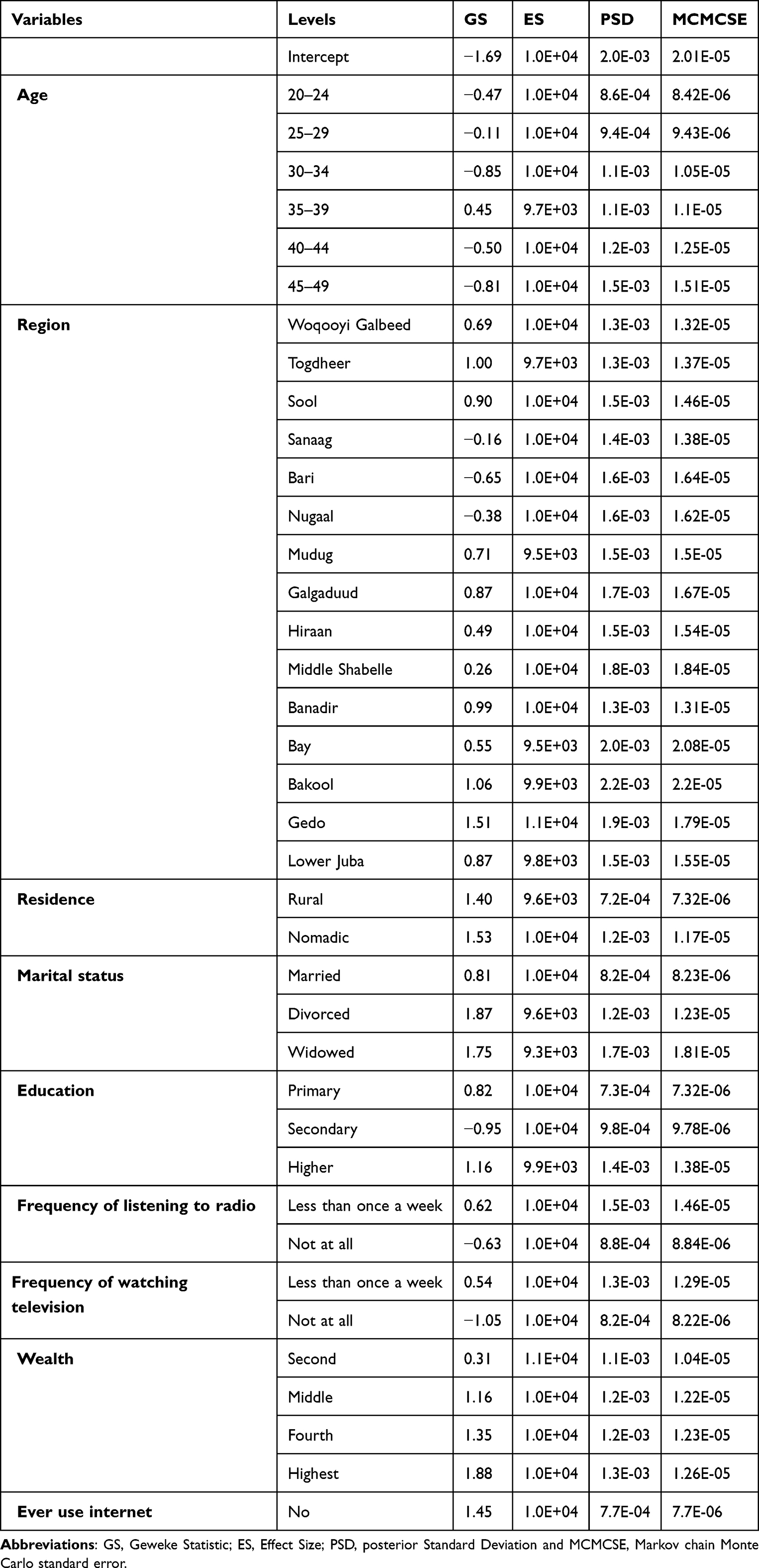 |
Table 3 Diagnostics of MCMC Results |
Discussion
This study investigates the relationship between misconceptions about HIV transmission and sociodemographic factors among Somali women aged 15–49 years. The analysis highlights age, education, region, internet usage, and wealth as significant predictors of misconceptions about HIV transmission.
This study found that 67.18% of women reported misconceptions about HIV transmission, while only 32.82% of women demonstrated an accurate knowledge. These findings highlight a significant public health concern, as misconceptions about HIV transmission can delay effective prevention strategies.
When compared with findings from other countries, the proportion of women harboring misconceptions in this study is markedly higher than that reported in Ethiopia (27%)20 and South Africa (48%),29 but slightly lower than the figure from Bangladesh (71.7%).30 These discrepancies may reflect differences in public health education campaigns, cultural contexts, access to accurate information, and the general literacy level across populations. For instance, South Africa and Ethiopia have implemented extensive national HIV education programs over the past decade, which may have contributed to better public knowledge. In contrast, Bangladesh’s high rate of misconception might be attributed to limited health education, lack of media access, poverty, illiteracy, and low education that strongly linked to poor HIV knowledge and persistent myths. In contrast, Somalia faces challenges such as limited healthcare infrastructure, lower literacy rates, and restricted access to health education due to sociopolitical instability and cultural beliefs.
The results of this study reveal several important associations between sociodemographic factors and misconceptions about HIV transmission: Women aged 30–34, 35–39, and 40–44 exhibited lower odds of having misconceptions about HIV transmission by 6%, 6%, and 7%, respectively, compared to women aged 15–19 years. This finding demonstrates an inverse relationship between age and misconceptions about HIV transmission. Older women are less likely to harbor misconceptions than younger women. This aligns with studies conducted in in sub-Saharan Africa,31 Uganda,32 Gambia,33 and Nigeria,34 which similarly found that older women tend to have a better knowledge of HIV compared to younger women. The observed disparity may be attributed to several factors. First, older women have had more cumulative exposure to HIV-related information through life experiences, including repeated interactions with healthcare systems, antenatal care visits, or community health campaigns. Second, they may have greater access to social networks and peer discussions that reinforce accurate HIV knowledge. Third, older women are more likely to have encountered HIV education programs, which have been implemented over the years, whereas younger women may not yet have had the same level of exposure. Additionally, older women’s maturity and decision-making autonomy may enable them to seek out and retain health information more effectively than adolescents. These findings imply that policymakers and health practitioners should consider age-specific variations when designing interventions to address misconceptions about HIV transmission among reproductive-age women in Somalia. Tailored strategies targeting younger women—such as school-based health education, youth-friendly HIV awareness campaigns, and digital outreach through social media—may help bridge knowledge gaps and promote accurate understanding of HIV transmission.
This study also found that women with secondary and higher education were 8% and 16% less likely, respectively, to have misconceptions about HIV transmission compared to those with no formal education. This demonstrates a negative relationship between education level and misconceptions about HIV transmission—the more educated women are, the less likely they are to harbor misconceptions. Similar findings have been reported in Botswana,35 Malawi13 and Ethiopia,19 where higher educational attainment was consistently associated with improved HIV knowledge. Beyond mere access to information, education enhances critical health literacy, enabling women to evaluate and interpret HIV-related messages more effectively. Formal schooling often teach basic health education, which provides structured learning about disease transmission and prevention. Educated individuals also tend to use healthcare services more, seek out credible sources of information through medical professionals and literature. (i.e., medical professionals, scientific literature), and resist harmful myths spread in their communities. Higher education levels also correlate with greater exposure to workplace or media-based health campaigns, reinforcing accurate HIV knowledge over time. Therefore, strategies targeting individuals without formal education must be tailored appropriately, as a “one-size-fits-all” approach to HIV education is unlikely to effectively address misconceptions about transmission and prevention.
Furthermore, Women in the fourth wealth quintile and those in the highest wealth quintile were 5% and 10% less likely, respectively, to have misconceptions compared to women in the lowest wealth quintile. This indicates that wealthier women are less likely to hold misconceptions about HIV transmission. Studies in Malawi,13 Ethiopia20 and Ghana21 have similarly observed that economic status influences health literacy, with wealthier individuals more likely to access healthcare services, resources, and educational opportunities, all of which can promote accurate understanding of HIV transmission. The association between wealth and reduced misconceptions may be explained by several mechanisms. First, higher economic status often grants women better access to formal education, which enhances their ability to critically assess health information. Second, wealthier households are more likely to afford healthcare services, including HIV counselling and testing, which provide accurate information on transmission modes. Additionally, financial stability may increase exposure to media and public health campaigns that disseminate evidence-based HIV knowledge. Conversely, women in lower wealth quintiles may face structural barriers—such as limited schooling, reliance on informal health information sources, or competing survival priorities—that perpetuate misconceptions. Addressing these disparities requires targeted interventions, such as community-based health education and subsidized healthcare access, to ensure equitable HIV knowledge across socioeconomic groups.
Additionally, Women who had never used the internet had 6% higher odds of having misconceptions about HIV transmission compared to those who had used the internet. This demonstrates that internet usage is inversely related to misconceptions about HIV transmission—the more women use the internet, the fewer misconceptions they have. This is consistent with findings from Ethiopia,19 Nigeria36 and Gambia33, where internet access has been linked to improved HIV knowledge and reduced stigma. Internet access has a substantial role in seeking and providing health information for various population groups including women, participate in online awareness campaigns, and engage with educational content.37 This finding highlights the importance of using social media and internet platforms to disseminate accurate HIV-related health information and address misconceptions effectively.
However, it is important to acknowledge the limitations of internet accessibility, particularly in rural areas of Somalia, where infrastructure challenges, low literacy rates, and socioeconomic barriers restrict widespread internet use. In these regions, women may have limited or no access to digital devices, reliable electricity, or affordable data services, which hinders their ability to benefit from online health information. Consequently, relying solely on internet-based interventions may exclude vulnerable populations who are already at higher risk of HIV misinformation. To address this gap, complementary strategies—such as community-based education, radio broadcasts, and mobile health outreach programs—should be implemented alongside digital campaigns to ensure equitable access to accurate HIV knowledge across all demographics.
This study has both strengths and limitations. A key strength is its use of nationally representative data from the SDHS 2018–19, providing valuable insights into misconceptions about HIV among reproductive-aged women in Somalia. However, several limitations should be considered when interpreting the findings. First, the exclusion of the Lower Shabelle, Middle Juba regions, and two strata of the Bay region due to security concerns may limit the generalizability of the results, as these areas may have distinct sociodemographic or HIV-related knowledge patterns that differ from the included regions. Second, reliance on self-reported data introduces potential biases, such as social desirability or recall bias, which may affect the accuracy of responses regarding HIV knowledge and misconceptions. Additionally, the absence of HIV status data prevents an assessment of how misconceptions relate to actual HIV prevalence. Finally, as a cross-sectional study, causality cannot be established for the observed associations. Despite these limitations, the study is pioneering in exploring the impact of various sociodemographic factors on misconceptions about HIV among reproductive-aged women in Somalia. The use of national SDHS data and a substantial sample size enhances the reliability of the findings. However, future research could further deepen understanding by: (1) investigating the underlying cultural and educational drivers of these misconceptions, (2) examining the role of media and community engagement in shaping HIV knowledge, and (3) assessing the effectiveness of targeted interventions in correcting misinformation. Such studies would help translate these findings into actionable public health strategies.
Conclusion
The Bayesian logistic regression analysis identified key factors influencing HIV transmission misconceptions among Somali women aged 15–49 years. Younger women, those with lower education levels, and individuals from low-income backgrounds exhibited higher misconceptions. Regional disparities were evident, with women in Sanaag, Bari, Nugaal, and Gedo having lower odds of misconceptions compared to those in Awdal.
To strengthen HIV prevention efforts, policies should focus on health education for young and less-educated women, region-specific awareness programs, and expanding digital literacy and internet access—especially in rural areas. Integrating HIV education into national curricula can further reduce stigma and misconceptions. Future research should explore barriers to HIV awareness, including digital health campaigns and socio-cultural influences on misinformation.
Data Sharing Statement
The study utilizes secondary data from the SDHS 2018–19, a publicly available dataset that can be requested from the Somali National Bureau of Statistics (SNBS) at this link (https://microdata.nbs.gov.so/index.php/catalog/50).
Ethical Considerations
This study was approved by the ethical committee of Abrar University, Somalia (Approval number AUEC11224). It was conducted in accordance with the principles and guidelines outlined in the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Latest global and regional HIV statistics on the status of the AIDS epidemic. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf.
2. Moyo E, Moyo P, Murewanhema G, Mhango M, Chitungo I, Dzinamarira T. Key populations and Sub-Saharan Africa’s HIV response. Front Public Health. 2023;11:1079990. doi:10.3389/FPUBH.2023.1079990
3. Menkhaus K. Governance without government in Somalia: spoilers, State building, and the politics of coping. Int Secur. 2007;31(3):74–106. doi:10.1162/isec.2007.31.3.74
4. Ahmed AY, Nor FA, Ahmed MY, Osman MM. Universal health coverage in Somalia: charting the path to equitable healthcare financing and governance. Health N Hav. 2023;15(11):1298–1317. doi:10.4236/health.2023.1511085
5. UNAIDS. (2023). Country factsheets: Somalia. UNAIDS.
6. Mohamud LA, Aslam M. Level and factors associated with comprehensive knowledge about HIV among currently married women in Somalia: a nationwide cross-sectional study. HIV/AIDS Res Palliative Care. 2024;16:485–494. doi:10.2147/HIV.S491513
7. Hasnain M. Cultural approach to HIV/AIDS harm reduction in Muslim countries. Harm Reduct J. 2005;2(1):23. doi:10.1186/1477-7517-2-23
8. Ahmed HJ, Omar K, Adan SY, Guled AM, Grillner L, Bygdeman S. Syphilis and human immunodeficiency virus seroconversion during a 6-month follow-up of female prostitutes in Mogadishu, Somalia. Int J STD AIDS. 1991;2(2):119–123. doi:10.1177/095646249100200209
9. 90-90-90: an ambitious treatment target to help end the AIDS epidemic. Available from: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf.
10. Somali HIV Epidemic and response. Available from: https://www.unaids.org/sites/default/files/country/documents/SOM_narrative_report_2014.pdf.
11. Integrated hiv and sexually transmitted infections (STIs) bio-behavioral survey (IBBS) amongst key populations In Somalia - Wasaaradda Caafimaadka Soomaaliya. Available from: https://moh.gov.so/so/pdfs/integrated-hiv-and-sexually-transmitted-infections-stis-bio-behavioral-survey-ibbs-amongst-key-populations-in-somalia/.
12. Mondal MNI, Hoque N, Chowdhury MRK, Hossain MS. Factors associated with misconceptions about HIV transmission among ever-married women in Bangladesh. Jpn J Infect Dis. 2015;68(1):13–19. doi:10.7883/YOKEN.JJID.2013.323
13. Sano Y, Antabe R, Atuoye KN, et al. Persistent misconceptions about HIV transmission among males and females in Malawi. BMC Int Health Hum Rights. 2016;16(1):1–10. doi:10.1186/S12914-016-0089-8/TABLES/4
14. Abdi IA, Ereg D, Ali M, Rahlenbeck SI. Knowledge and attitudes about AIDS/HIV in a semi-nomadic population in Somaliland. J Community Health. 2013;38(2):246–249. doi:10.1007/S10900-012-9606-4
15. Beliefs and practices of Somali citizens concerning HIV/AIDS. Available from: https://www.africasvoices.org/wp-content/uploads/2020/09/UNICEF-Somalia-HIV_AIDS-report-March-2017-Google-Docs.pdf.
16. Mohamud LA, Hassan AM, Nasir JA. Determinants of HIV/Aids knowledge among females in Somalia: findings from 2018 to 2019 SDHS data. HIV/AIDS Res Palliative Care. 2023;15:435–444. doi:10.2147/HIV.S414290
17. Mohamud LA, Nasir JA. Role of proximate determinants on the fertility rate among currently married women in Somalia via bongaart’s model: findings from 2018-19 SDHS data. Sci Rep. 2024.
18. Mohamud LA. Understanding the Fertility Transition in Somalia Through Proximate Determinants of Fertility. GC University Lahore; 2023.
19. Seid A, Ahmed M. What are the determinants of misconception about HIV transmission among ever-married women in Ethiopia? HIV/AIDS Res Palliative Care. 2020;12:441–448. doi:10.2147/HIV.S274650
20. Yimer A, Kebede Kassaw AA, Surur S, Mussa E. Prevalence of misconception about HIV/AIDS transmission and associated factors among reproductive age women in Ethiopia: a nationwide study. BMC Infect Dis. 2024;24(1):1–7. doi:10.1186/s12879-023-08884-8
21. Amo-Adjei J, Kumi-Kyereme A. Myths and misconceptions about tuberculosis transmission in Ghana. BMC Int Health Hum Rights. 2013;13(1). doi:10.1186/1472-698X-13-38
22. Hastie TJ, Pregibon D. Generalized linear models. Statistical Models in S. 2017;195–247. doi:10.1201/9780203738535
23. Little RJ. Calibrated Bayes: a Bayes/frequentist roadmap. Ame Statistician. 2006;60(3):213–223. doi:10.1198/000313006X117837
24. Hamra G, MacLehose R, Richardson D. Markov chain monte carlo: an introduction for epidemiologists. Int J Epidemiol. 2013;42(2):627–634. doi:10.1093/ije/dyt043
25. Kerkering JC. Subjective And Objective Bayesian Statistics: Principles, Models, And Applications. 2003;45. doi:10.1198/tech.2003.s175
26. Vrugt JA. Markov chain Monte Carlo simulation using the DREAM software package: theory, concepts, and MATLAB implementation. Environ Modell Software. 2016;75:273–316. doi:10.1016/j.envsoft.2015.08.013
27. Geweke J. Evaluating the accuracy of sampling-based approaches to the calculation of posterior moments. Bayesian Stat. 1992;4:1–31.
28. Workie MS, Lakew AM. Bayesian count regression analysis for determinants of antenatal care service visits among pregnant women in Amhara regional state, Ethiopia. J Big Data. 2018;5(1). doi:10.1186/s40537-018-0117-8
29. Rauf W, Hitchcock S, Rauf A, Becker PJ. Knowledge of and misconceptions about the spread and prevention of HIV infection among older urban women attending the Tshwane District hospital, South Africa. S Afr Family Pract. 2010;52(2):142–148. doi:10.1080/20786204.2010.10873957
30. Bhowmik J, Biswas RK. Knowledge about HIV/AIDS and its transmission and misconception among Women in Bangladesh. Int J Health Policy Manag. 2022. doi:10.34172/ijhpm.2022.6321
31. Teshale AB, Yeshaw Y, Alem AZ, et al. Comprehensive knowledge about HIV/AIDS and associated factors among women of reproductive age in sub-Saharan Africa: a multilevel analysis using the most recent demographic and health survey of each country. BMC Infect Dis. 2022;22(1):1–10. doi:10.1186/S12879-022-07124-9/TABLES/5
32. Ankunda D, Asiimwe JB. Determinants of comprehensive knowledge of HIV/AIDS among women of the reproductive age (15-49) in Uganda. Int J Community Med Public Health. 2017;4(10):3530–3535. doi:10.18203/2394-6040.IJCMPH20174215
33. Tsegaw M, Mulat B, Shitu K, Barrow A. Comprehensive HIV knowledge and associated factors among reproductive-age women: analysis of the Gambia Demographic and health survey 2019/2020. Health Res Policy Syst. 2024;22(1):1–9. doi:10.1186/S12961-024-01128-4/TABLES/2
34. Oginni AB, Adebajo SB, Ahonsi BA. Trends and determinants of comprehensive knowledge of HIV among adolescents and young adults in Nigeria: 2003 - 2013. Afr J Reprod Health. 2017;21(2):26–34. doi:10.29063/AJRH2017/V21I2.4
35. Letamo G. Misconceptions about HIV prevention and transmission in Botswana. Afr J AIDS Res. 2007;6(2):193–198. doi:10.2989/16085900709490414
36. Iyamu I, Oladele EA, Eboreime E, Karim ME. Is regular access to internet services associated with comprehensive correct HIV/AIDS knowledge among people aged 15–49 years in Nigeria? Findings from the 2018 demographic health survey. J Consum Health Internet. 2021;25(3):242–260. doi:10.1080/15398285.2021.1943634
37. Pandey SK, Hart JJ, Tiwary S. Women’s health and the internet: understanding emerging trends and implications. Soc Sci Med. 2003;56(1):179–191. doi:10.1016/S0277-9536(02)00019-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.