")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Household Pharmaceutical Disposal Practices, Community Understanding, and Readiness for Medicines Take-Back in Asmara, Eritrea: A Cross-Sectional Analysis
Authors Habte HY , Bahta M , Russom N , Kibreab F , Andemariam A, Tewelde T, Russom M
Received 16 May 2024
Accepted for publication 2 November 2024
Published 11 November 2024 Volume 2024:17 Pages 2777—2788
DOI https://doi.org/10.2147/RMHP.S478511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Haiyan Qu
Heaven Yohannes Habte,1 Merhawi Bahta,1 Natnael Russom,1 Fitsum Kibreab,2 Adiam Andemariam,3 Tomas Tewelde,4 Mulugeta Russom1,5,6
1National Medicines and Food Administration, Ministry of Health, Asmara, Eritrea; 2Health Research and Resources Centre Division, Ministry of Health, Asmara, Eritrea; 3Zoba Maekel Pharmaceutical Service, Ministry of Health, Asmara, Eritrea; 4Orotta College of Medicine and Health Science, Department of Medical Science, Unit of Pharmacy, Asmara, Eritrea; 5Department of Medical Informatics, Erasmus Medical Center, Rotterdam, Netherlands; 6European Programme for Pharmacovigilance and Pharmacoepidemiology, University of Bordeaux, Bordeaux, France
Correspondence: Natnael Russom, National Medicines and Food Administration, Ministry of Health, Asmara, Eritrea, Tel +291-7602351, Email [email protected]
Introduction: Unused and/or expired pharmaceuticals stored in households are potential health and environment hazards that require safe disposal. In Eritrea, there has not been a proper household medicines disposal system and pharmaceutical wastes had been disposed of irrationally. The study was therefore conducted to assess community’s understanding and disposal practices of unused/expired medications and willingness to participate in a household medicines take-back system.
Methods: A cross-sectional study was conducted from January to February 2023 in randomly selected households of Asmara. The study participants were selected using a multi-stage-cluster sampling. Data, collected through face-to-face interview using a structured questionnaire, were double entered using CSPro version 7.3 software package and analyzed using SPSS version 26.
Results: A total of 327 participants were enrolled in the study with a predominance of female respondents (84%). The most commonly used disposal practices were throwing with household garbage (65.6%), followed by dumping under soil (38.7%) and flushing down the toilet/sink (15.2%). Around three-quarters (70.5%) of the households had unused/expired medicines stored at home during the data collection period with intention to use being the most common reason for storage (83.9%). Analgesics and anti-infectives were the most commonly stored classes of medicines, and more than half of the anti-infectives were stored for future use. The mean knowledge score of participants was 7.31/11 (95% CI: 7.09– 7.52). Moreover, participants had a satisfactory willingness to participate in a household medicines take-back system, with a mean attitude score of 16.89/20 (95% CI: 16.45– 17.29). Lack of awareness, negligence, time/health constraints, fear of accountability/stigma, accessibility and reluctance were reported as possible challenges in establishing a household medicines take-back system.
Conclusion: Unnecessary storage and improper disposal of household unused/expired medicines along with inadequate knowledge on disposal mechanisms were common in households of Asmara. Hence, public education on proper disposal as well as coordinated efforts for the establishment of safe disposal mechanisms are recommended.
Keywords: household disposal practices, expired, unused, medicines take-back, pharmaceuticals, knowledge, willingness, Asmara
Introduction
Medication consumption has increased over the past few decades.1 Substantial developments in the drug industry supplemented with enhanced access of the world population to medicines have contributed to the increase in medication consumption worldwide. This trend is expected to continue in the coming years, due to the fast-growing world population and improved access to medicines rendering medicines to be easily available and stored.2 Patients store medicines at home for various reasons, which include improvement of patient’s medical condition, adverse drug reactions, changes in dosage/regimen, medicine expiration, prescription of more drugs than required (polypharmacy), changes in prescription due to lack of therapeutic effect, poor adherence, intention for future use, patient death as well as unavailability of proper disposal mechanism.3–5 This unnecessary storage of medicines consequently bulks the size of pharmaceutical wastes to be disposed.
Pharmaceutical residues can enter the environment during production, consumption and disposal, with incorrect disposal from households being considered the second major pathway for active pharmaceuticals to enter the environment.5 Several studies have shown that most household stored pharmaceuticals are disposed of inappropriately with throwing in garbage and flushing down the toilet being common means of disposal.2,4–8 This practice is potentially health-threatening and hazardous to the environment as pharmaceutical residues can contaminate water bodies, vegetation, air and land surfaces.6,7 Additionally, improper disposal of unused and expired medications makes active pharmaceuticals be easily available and accessible leading to accidental medication poisoning, misuse and/or abuse in children and adults.3 Long-term environmental exposure to pharmaceuticals, in general, has hazardous health effects, especially on vulnerable populations, including pregnant women, newborns, and children.4
Furthermore, many developing countries lack clear guidelines on safe disposal of household unused or expired pharmaceuticals and are lagging behind in empirical studies on proper management of pharmaceutical wastes.1,4 Eritrea, like most developing countries, has not had a clear national guideline on safe disposal of pharmaceutical wastes or a standardized system for accepting and collecting household unused and expired medicines. The country has just introduced such a system following completion of data collection of this study. Additionally, public awareness of proper pharmaceutical waste disposal is unsatisfactory as evidenced by an urban population-based Knowledge, Attitude and Practice (KAP) survey conducted by Russom et al which found that over 50% of respondents considered flushing left-over antibiotics down toilets and/or disposing of in routine municipality garbage as appropriate disposal practices.9 Understanding the current household pharmaceutical waste disposal practices was hence, an important and timely exploration. This study was therefore, aimed to assess the knowledge and current disposal practices of unused and expired medicines in households of Asmara as well as household readiness to return unused and expired medicines to local community pharmacies or health facilities.
Methods
Study Design and Setting
A descriptive cross sectional study with a quantitative approach was conducted in households of Asmara. Asmara is the capital city of Eritrea, with an estimated total of 124,035 households. It comprises 13 subzones with 37 kebabi administrations.
Study Population
The source population for the study was all members of the general public aged 18 years and above residing in households of Asmara. The study population was the family heads or a household member capable of providing adequate information on behalf of the household with competent mental capacity. House members aged 18 years and above who could not provide information on behalf of the household due to mental problem or other conditions were excluded.
Sample Size and Sampling Technique
Sample Size Calculation
The sample size for this study was calculated based on the prevalence of households storing unused/expired medicines, precision level, and confidence interval. Since the proportion of households storing unused/expired medicines was unknown, it was assumed that half of the households in the study area had experienced this issue. Hence, to estimate the sample size, the parameters used were a 50% prevalence of households that stored unused treatments, a 95% confidence level, and a 7% desired precision level. The initial sample size was obtained using the Cochran formula:10

Thus, with the assumption of the estimates mentioned above, the initial sample size was 196. The sample size was adjusted for cluster sampling, and considering a 1.5 design effect, the sample size was inflated to 294 (1.5*196). The cluster size was determined to be 25; hence, the number of clusters were estimated as 12 (294/25=11.8~12). Considering a 95% response rate(r), the sample size (n) per cluster was determined as follows:

Thus, the overall sample size was calculated at 324 (12*27). Therefore, there were twelve kebabi administrations (known, in this study, as “clusters”), and 27 households/individuals were randomly selected from each cluster.
Sampling Procedure
Each kebabi administration in the 13 sub-zones of Asmara was considered a cluster, and clusters were selected using probability proportional to size of households of a kebabi. Hence, one or more than one clusters were selected from these kebabi. However, from each selected cluster, 27 households were visited or enrolled. To select clusters, all kebabi administrations were listed with their respective household sizes. Then, the cumulative frequency of kebabi administration was calculated. The cumulative frequency was divided by the number of clusters planned to be enrolled—twelve in this study. This provided a number that was considered as the interval. Afterwards, a random number was generated between one and the interval to get the random start. The cluster with a cumulative frequency of household size that included the generated number was selected as the first cluster. The interval was then added to the random start (cumulative frequency of the selected cluster) in which afterwards, the cluster that includes this number in its cumulative household size was chosen as the second cluster. The process continued until all twelve clusters were selected. Accordingly, 12 kebabi administrations (clusters) located in 11 sub-zones (Akria, Arbaete-Asmara, Edaga-Hamus, Gejeret, Geza-Banda, Godaif, Maekel-Ketema, Mai-Temenay, Paradiso, Tiravolo and Tseserat) of Asmara were selected.
Determination of Number of Households in Each Cluster
To select the household, first, each selected cluster was divided into segments of 150–200 households (if a cluster had more than 300 households), then one segment was selected randomly. Afterwards, all households in each selected cluster were listed, and a unique number was assigned to each household (from 1 to N, where N is the population size of the segment). After that, systematic random sampling was used to select the households—the households were selected at a certain interval. The total number of households in the segment was divided by 27 (the cluster size) to get the interval. Next, one number was randomly selected between one and the interval—this was the random start (the first household). Afterwards, the interval was added to the obtained number to get the next household. The process continued until the required households were selected.
Data Collection Tools and Approach
Data were collected from January to February, 2023, through face-to-face interviews using a structured questionnaire (Supplementary file 1), after explaining the aim of the study and obtaining a written informed consent. The questionnaire was prepared by reviewing questionnaires of similar studies and was customized to reflect cases relevant to the Eritrean population. It was initially prepared in English and was translated into the local language, Tigrigna. It was then back translated to English to check the similarity between the original and translated language and approved by all co-authors.
The data collection tool covered questions that explored participants’ socio-demographic information, knowledge on disposal of unused and expired drugs, availability of unused and expired drugs, and disposal practices of these drugs. The knowledge questions were dichotomized and coded as 1 for correct responses and 0 for wrong responses. Then the score of the responses were summed up and the total knowledge score was considered as a continues variable. The household representatives were asked to provide any medication available in the household during the data collection period. Data collectors then explored the name, therapeutic category, dosage form and quantity of stored medications within households.
Pharmacy professionals who had prior experience in survey data collection were selected as data collectors to ensure data reliability. To avoid measurement and selection biases, orientation was provided to data collectors to familiarize them with the survey objectives, questionnaire, interview principles, data collection procedures, and standards of practice. To ensure the comprehensiveness, feasibility, and robustness of the data collection tool, a pre-test was conducted in unselected households of Asmara. Accordingly, necessary modifications were made in the final version of the questionnaire. The fact that the questionnaire was not self-administered also helped minimize information bias and participants were given ample time to remember previous disposal practices to minimize recall bias.
The study was reported in line with Strengthening the reporting of Observational studies in Epidemiology for Cross sectional study.11
Statistical Analysis
Data were checked for completeness and consistency, then coded, and double entered using Census and Survey processing system (CSPro, Version 7.3) software package,12 and data analysis was carried out using SPSS version 26.13 The respondents’ socio-demographic characteristics and their knowledge and disposal practice of unused/expired medicines were presented as descriptive analysis. As the study used complex cluster sampling, the sample was not self-weighted; hence a weighing variable was included during analysis to take account of the clustering effect. Thus, all results: percentages, mean and 95% confidence interval were weighted. However, the frequency or count of each variable was reported as unweighted.
Ethical Considerations
Ethical approval was obtained from the Ministry of Health Research Ethics and Protocol Review Committee (Reference number 07/11/2022). Approval was also obtained from central region administration to conduct the study in the respective kebabi administrations. Besides, a written informed consent was obtained from all study participants to ensure that participation was fully voluntary. All ethical and professional considerations were followed throughout the study to keep data strictly confidential. The identity of the participants was not revealed in the workbook, report, or any other publications, nor reported to anyone, and only aggregated and de-identified data were disseminated. This study conforms to the principles outlined in the Declaration of Helsinki.
Results
Demographic Characteristics of Study Participants and Households
Study respondents were primarily females (84%), unemployed (61.1%) and with secondary level of education (48.6%). The mean age of respondents in completed years and average household size were 44.28 (95% CI 42.55–46.02) and 4.43 (95% CI 4.20–4.66), respectively. About 43% of households had at least one member with chronic illness. Details of demographic characteristics of study respondents and households are presented in Table 1.
 |
Table 1 Demographic Characteristics of Study Participants and Households |
Knowledge and Attitude on Disposal of Household Unused/Expired Medications
Upon assessment of knowledge on disposal of household unused/expired medications, 60.5% of the respondents correctly answered that there is difference between disposal of household unused/expired medications and household garbage. The mean knowledge score was 7.31/11 (95% CI: 7.09–7.52; Min=0, Max=11). Similarly, 35.5 to 56.6% of the respondents answered correctly on how household unused/expired medicines should be disposed, while 46.5 to 97.3% had correct knowledge on impacts of the presence of pharmaceutical residues in the environment (Table 2).
 |
Table 2 Respondents Knowledge on How Household Unused/Expired Medicines Should Be Disposed of and the Impacts of Presence of Pharmaceutical Residues on the Environment |
A positive attitude towards participating in a household medicines take-back system was reported by majority of the respondents (82.2 to 91.2%) (Table 3). The mean attitude score was 16.89/20 (95% CI: 16.45–17.29; Min=4, Max 20).
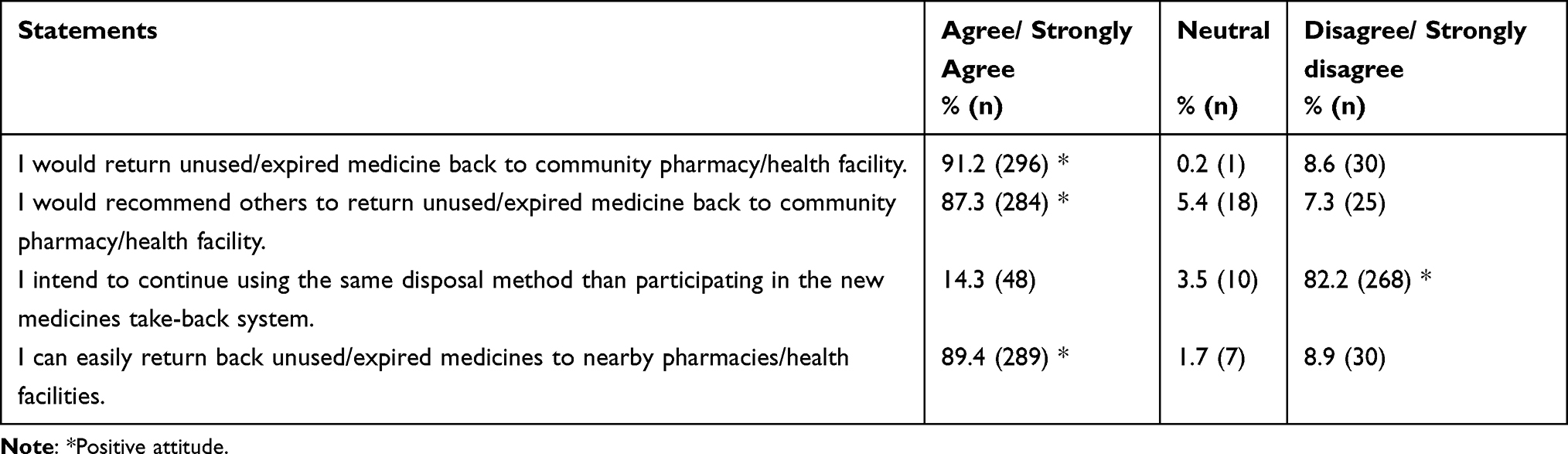 |
Table 3 Respondents’ Willingness to Return Expired/Unused Medicines Back to Local Community Pharmacies/Health Facilities |
Disposal Practices of Household Unused/Expired Medications
A sizeable proportion (84.1%, n=274) of the households reported that they had unused and/or expired medicines stored in their homes during the one-year period prior to data collection, while 70.5% (n=233) had unused and/or expired medicines during the data collection period. As shown in Figure 1, keeping for future use (90.3%) and improved medical conditions (56.7%) were the main reasons for keeping medications during the one-year period.
 |
Figure 1 Proportion of respondents by reasons for having unused and/or expired medicines during the one-year period. *Drug got lost, already expired, and replacement for initially missing drug. |
The most common ways of disposing of unused and/or expired medicines during the one-year period were throwing in household garbage (65.6%), dumping under soil (38.7%), and flushing down the toilet/sink (15.2%), while a minor proportion (1.5%) of the households returned back unused and/or expired medicines to health facility/pharmacy. In addition, a large proportion (41.4%) of households kept medications for future use (Figure 2).
 |
Figure 2 Proportion of respondents by actions taken for the unused and/or expired medicines during the one-year period. |
During the two-week data collection period, 103 types medicines categorized into 29 therapeutic categories were found in the households. This accounted for a total of 638 medicines in all households, giving a mean of 1.95 (95% CI: 1.66–2.24; Min=0, Max=19) types of medicines per household when all households were considered and a mean of 2.24 (95% CI: 2.38–3.10; Min=1, Max=19) types of medicines per household in those households, which had medicines during the data collection period. The medications were quantified as 17571 tablets and 1364 capsules (provided in strips and jars), 311 suppositories, 114 tubes, 49 bottles containing liquid preparations (the incomplete semisolid and liquid dosage forms were counted as containers without specifications), 2 canisters, 37 sachets, 7 vials, 2 cups (dosage forms which are locally compounded extemporaneously at retail pharmacies), and 53 others (unknown dosage forms). When only solid dosage forms were considered a median of 21 (IQR: 66.25) tablets/capsules/suppositories per household were found in those which had stored medicines during the data collection period.
The most frequently identified medicines during the data collection period were paracetamol (25.9%) and ibuprofen (15.1%) (Table 4), while analgesics (48.6%) and anti-infectives (11.6%) were the most frequent therapeutic categories (Table 5). Besides, out of the total medicines found in households, 7.1% were expired. The proportion of the top 20 and all individual medicines found to be stored in households of Asmara are displayed in Table 4 and Supplementary file 2, respectively.
 |
Table 4 Proportion of Top 20 Medicines Found in Households of Asmara During the Data Collection Period |
 |
Table 5 Proportion of Therapeutic Categories of Medicines Found in Households of Asmara During the Data Collection Period |
The main reason for not discarding stored medicines during the data collection period was “intention to use in the future” (83.9%) (Table 6). Similarly, from the total of 71 anti-effective medicines found in households, intention to use in the future (52.1%, n=37) and forgetting to dispose of (43.7%, n=31) were the main reasons for not discarding them.
 |
Table 6 Reasons for Not Discarding/Having Unused/Expired Medicines in Households of Asmara During the Data Collection Period (n=638) |
When study participants were asked what challenges the public would face if a new medicines take-back system was introduced, 23.2% (n=76) suggested that there would be no challenge, while 76.8% (n=251) suggested at least one challenge. The challenges that the population would possibly face as anticipated by the respondents are shown in Figure 3. Lack of awareness (49.7%) and negligence (45.2%) were the most commonly anticipated challenges.
 |
Figure 3 Anticipated challenges in establishing a household medicines take-back system (n=251). |
Discussion
Improper disposal of household unused/expired pharmaceuticals was practiced by majority of respondents with throwing in municipality garbage being the most common method of disposal followed by dumping under soil and flushing down the toilet/sink. Several other studies also reported these inappropriate disposal methods as communal practices.4,5,7,14–16 In contrast, only a very small proportion of respondents (1.5%) returned unused/expired medications to health facilities possibly because of the absence of a household medicines take-back system during the study period. This much less when compared to studies conducted in Italy (51.2%),17 Bangladesh (21%)1 and Israel (14%),2 while somehow similar to a study conducted in Saudi Arabia (5%).18 Although the exact quantity of active pharmaceutical ingredients being released to the environment due to improper disposal cannot be measured, the study suggests the possibility of presence of such in the environment, which could have detrimental effects on human/animal health and the environment.
During the data collection period, majority of the households had unused and/or expired medicines stored at home. This finding is similar to a study conducted in India (69%).19 It is, however, higher than that of Ethiopia (52.4%)20 and Jordan (58.1%)21 and lower than studies conducted in Afghanistan, Tanzania, Indonesia and Pakistan in which 95.3%, 96%, 95.5% and 87% of respondents had unused medication stored at home, respectively.5,22–24 Analgesics and anti-infectives were the most commonly stored classes of drugs, while expired medicines and prescription drugs were also present in significant proportions. Consistent to the current study, studies published elsewhere reported analgesics23,25,26 and both antibiotics and antipyretics/analgesics4,19,27,28 as the most common types of therapeutic categories stored in households. The main reason for storing such significant amount of unused/expired medicines during the data collection period was the intention to use in the future. This finding is noteworthy as it indicates a propensity towards self-medication, given the high proportion of medicines kept for this purpose. However, the excessive storage of these medications not only increases the volume of drugs for disposal but also poses risks such as accidental poisoning, drug misuse, or abuse. Interestingly, the prevalent reason for storing medication for future use differs from other studies, where improved medical conditions or self-discontinuation were more commonly cited.22,29–31 Particularly concerning is the fact that over half of the stored anti-infectives were earmarked for future use, a practice that could exacerbate antimicrobial resistance issues. Antimicrobial resistance is not confined to borders and the finding of this study in this regard has an effect, which goes beyond local metropolitan.
While respondents demonstrated above average awareness on the environmental impact of pharmaceutical residues, there existed a significant misconception concerning proper disposal practices. This paradox suggests a disconnect between understanding the environmental repercussions of pharmaceutical residues and knowing how to appropriately dispose them. These findings underscore the necessity for educational initiatives focusing on correct disposal methods, pathways of pharmaceutical entry into the environment, and the environmental consequences of pharmaceutical residues. The respondents’ misconception regarding the link between improper household pharmaceutical waste disposal and antimicrobial resistance aligns with a broader urban study in Eritrea, indicating a general disregard for the appropriate disposal of antibiotics.9 Addressing this concerning trend calls for immediate awareness campaigns, including bolstering ongoing annual antimicrobial resistance awareness efforts that need to be conducted in a one-health approach.
Respondents’ willingness to participate in a household medicines take-back system, consistent with the findings of a study from Nepal,32 was impressive. This strong attitude is explained by the respondents’ readiness, where about a quarter anticipated no challenge to participate in such a system while the remaining considered lack of awareness, negligence, time/health constraints, fear of accountability/stigma, accessibility and reluctance as possible challenges that could face a newly established household medicines take-back system.
The study's key findings reflect the following programmatic, policy, and public health implications and recommendations: Primarily, improper disposal of unused/expired medicines is likely to escalate the burden of antimicrobial resistance as several antibiotics were reported as inappropriately disposed to the environment. Besides, unnecessary storage and inappropriate disposal of unused/expired medicines could expose the community to accidental poisoning. Yet, the perceived impact is likely to be continued unless a suitable household medicines take-back system is established in Eritrea. Secondly, taking the reported willingness of the respondents, establishment of a household medicines take-back system could be successfully implemented in Asmara city. To ensure successful implementation, policy makers and relevant stakeholders are recommended to maximize community awareness-raising campaigns on safe medicine waste disposal and establish an easy and accessible medicines take-back system.
Limitations
As the results were self-reported, information or recall bias could have been introduced and results could have been over or underestimated. The reliability and validity of the scales for knowledge on disposal of pharmaceutical wastes and willingness to participate in medicines take-back system were also not statistically verified. Additionally, household members who could provide accurate information in place of the household were purposively selected. Although this enabled the most reliable data to be obtained regarding household disposal practices, it meant that only knowledge of the respondents was measured, and therefore does not represent the knowledge score of the household.
Conclusion
Improper disposal of unused/expired household pharmaceuticals was a common practice in households of Asmara, which could possibly be explained by the limited knowledge on disposal mechanisms although the overall knowledge score was satisfactory. To minimize the risks related to unused/expired household medicines, massive public awareness-raising campaigns, establishment of medicines take-back system and multi-sectorial coordination mechanism as well as easy access to collection bins are highly recommended.
Data Sharing Statement
The complete dataset used in this study can be obtained from the corresponding author upon reasonable request.
Acknowledgment
The authors would like to thank the Eritrean Pharmaceutical Association (ERIPA) and administration of the Central Region for their cooperation throughout the study. The authors also convey their sincere gratitude to the data collectors and study respondents for their willingness to participate in the study.
Author Contributions
All authors made a significant contribution to the project, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was funded by the Eritrean Pharmaceutical Association (ERIPA).
Disclosure
The authors report no conflict of interest.
References
1. Begum MM, Rivu SF, Hasan MMA, et al. Disposal practices of unused and leftover medicines in the households of Dhaka metropolis. Pharmacy. 2021;9(2):103. doi:10.3390/pharmacy9020103
2. Barnett-Itzhaki Z, Berman T, Grotto I, Schwartzberg E. Household medical waste disposal policy in Israel. Israel j Health Policy Res. 2016;5:1–8. doi:10.1186/s13584-016-0108-1
3. Kusturica MP, Tomas A, Tomic Z, et al. Analysis of expired medications in Serbian households. Slovenian J Public Health. 2016;55(3):195–201. doi:10.1515/sjph-2016-0025
4. Ayele Y, Mamu M. Assessment of knowledge, attitude and practice towards disposal of unused and expired pharmaceuticals among community in Harar city, Eastern Ethiopia. J Pharmaceutical Policy Pract. 2018;11(1):27. doi:10.1186/s40545-018-0155-9
5. Bashaar M, Thawani V, Hassali MA, Saleem F. Disposal practices of unused and expired pharmaceuticals among general public in Kabul. BMC Public Health. 2017;17:1–8. doi:10.1186/s12889-016-3954-4
6. Magagula BK, Rampedi IT, Yessoufou K. Household pharmaceutical waste management practices in the Johannesburg Area, South Africa. Int J Environ Res Public Health. 2022;19(12):7484. doi:10.3390/ijerph19127484
7. Adedeji-Adenola H, Adesina A, Obon M, Onedo T, Okafor GU, Longe M. Knowledge, perception and practice of pharmaceutical waste disposal among the public in Lagos State, Nigeria. Pan Afr Med J. 2022;42(1). doi:10.11604/pamj.2022.42.106.34529
8. Michael I, Ogbonna B, Sunday N, Anetoh M, Matthew O. Assessment of disposal practices of expired and unused medications among community pharmacies in Anambra State southeast Nigeria: a mixed study design. J Pharmaceutical Policy Pract. 2019;12:1–10. doi:10.1186/s40545-019-0174-1
9. Russom M, Bahta M, Debesai M, et al. Knowledge, attitude and practice of antibiotics and their determinants in Eritrea: an urban population-based survey. BMJ open. 2021;11(9):e046432. doi:10.1136/bmjopen-2020-046432
10. Cochran W Cochran_1977_Sampling Techniques. pdf. 1977.
11. Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int j Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
12. U.S. Census Bureau, ICF International, and Serpro SA 2019. Census and survey processing system for windows, version 7.3.1.
13. IBM Corp. IBM SPSS Statistics for Windows VA. NY: IBM Corp; 2019.
14. Tong AY, Peake BM, Braund R. Disposal practices for unused medications around the world. Environment International. 2011;37(1):292–298. doi:10.1016/j.envint.2010.10.002
15. Azmi Hassali M, Shakeel SJP. Unused and expired medications disposal practices among the general public in Selangor. Malaysia. 2020;8(4):196.
16. Toe J, Orok E, Erah P, Pharmacy S. Assessment of knowledge and disposal practices of unused and expired household medicines in a community in Liberia. Exploratory Research in Clinical and Social pharmacy. 2023;12:100369. doi:10.1016/j.rcsop.2023.100369
17. Kamal KM, Chiumente M, Nakagawa S, Giannetti V, Marlin T. Disposal practices for unused and expired medications: pilot data from three cities in three countries. GMS Health Innov Technol. 2022;16. doi:10.3205/hta000133
18. Abdullah SAM, Ibrahim T, Alharbi H, Sciences B. Drug consumers behaviors toward the disposal of unused and expired medicines in Qassim Province/Saudi Arabia. J Pharmaceutical Biomed Sci. 2018;8(01).
19. Vaseem A. A study on awareness and disposal practices of unused and expired medicines by consumers. 2020.
20. Kahsay H, Ahmedin M, Kebede B, Gebrezihar K, Araya H, Tesfay D. Assessment of knowledge, attitude, and disposal practice of unused and expired pharmaceuticals in community of Adigrat City, Northern Ethiopia. J Environ Public Health. 2020;2020:1–11. doi:10.1155/2020/6725423
21. Naser AY, Amara N, Dagash A, Naddaf A. Medications disposal and medications storage in Jordan: a cross‐sectional study. Int J Clin Pract. 2021;75(3):e13822. doi:10.1111/ijcp.13822
22. Marwa KJ, Mcharo G, Mwita S, Katabalo D, Ruganuza D, Kapesa A. Disposal practices of expired and unused medications among households in Mwanza, Tanzania. PLoS One. 2021;16(2):e0246418. doi:10.1371/journal.pone.0246418
23. Insani WN, Qonita NA, Jannah SS, et al. Improper disposal practice of unused and expired pharmaceutical products in Indonesian households. Heliyon. 2020;6(7):e04551. doi:10.1016/j.heliyon.2020.e04551
24. Shoaib M, Raziq A, Iqbal Q, et al. Disposal practices of unused and expired pharmaceuticals among the general public in Quetta city. Pakistan. 2022;17(5):e0268200.
25. Sonowal S, Desai C, Kapadia JD, Desai MK. A survey of knowledge, attitude, and practice of consumers at a tertiary care hospital regarding the disposal of unused medicines. J Basic Clin Pharma. 2016;8(1):4. doi:10.4103/0976-0105.195079
26. Köksoy SJBPH. Unused, expired pharmaceuticals and their disposal practices among the general public in Burdur-Türkiye: a cross-sectional study. BMC Public Health. 2024;24(1):1303.
27. Hassan EWE, Al Taisan AA, Abualhommos AKJSPJ. Knowledge and practices concerning the storage and disposal of home medications among people in the eastern region of Saudi Arabia: a cross-sectional study. Saudi Pharmaceutical Journal: SPJ: the Official Publication of the Saudi Pharmaceutical Society. 2022;30(2):172–179. doi:10.1016/j.jsps.2021.12.010
28. Aluko OO, Imbianozor G, Jideama C, et al. The perception and disposal practices of unused and expired medicines by households in an urban municipality, southwest Nigeria: a comparative cross-sectional study. Waste Management (New York, N.Y.). 2022;140:121–132. doi:10.1016/j.wasman.2022.01.022
29. Gidey MT, Birhanu AH, Tsadik AG, Welie AG, Assefa BT. Knowledge, attitude, and practice of unused and expired medication disposal among patients visiting Ayder Comprehensive Specialized Hospital. Biomed Res Int. 2020;2020:1–7. doi:10.1155/2020/9538127
30. Ong SC, Ooi GS, Shafie AA, Hassali MA. Knowledge, attitude and disposing practice of unused and expired medicines among the general public in Malaysia. J Pharm Health Serv Res. 2020;11(2):141–148. doi:10.1111/jphs.12333
31. Braund R, Peake BM, Shieffelbien L. Disposal practices for unused medications in New Zealand. Environment International. 2009;35(6):952–955. doi:10.1016/j.envint.2009.04.003
32. Sapkota B, Giri A, Bhatta B, et al. Implementation of medicine take-back concept at community level in Nepal: a pilot study. Journal of Public Health (Oxford, England). 2022;44(3):575–585. doi:10.1093/pubmed/fdab134
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.