")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
How Does Disease Severity Affect Clinical Outcomes and Economic Burden of Patients with COPD —— A Retrospective Population-Based Cohort Study in Tianjin, China
Authors Wang L, Huang K , He X, Zhang J, Yang T , Wu J
Received 25 March 2025
Accepted for publication 10 June 2025
Published 25 June 2025 Volume 2025:20 Pages 2061—2072
DOI https://doi.org/10.2147/COPD.S524647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Lei Wang,1,2,* Ke Huang,3– 5,* Xiaoning He,1,2 Jiahui Zhang,1,2 Ting Yang,3– 5 Jing Wu1,2
1School of Pharmaceutical Science and Technology, Tianjin University, Tianjin, People’s Republic of China; 2Center for Social Science Survey and Data, Tianjin University, Tianjin, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 4National Clinical Research Center for Respiratory Diseases, Beijing, People’s Republic of China; 5Institute of Respiratory Medicine, Chinese Academy of Medical Science, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Wu, School of Pharmaceutical Science and Technology, Tianjin University, No. 92 Weijin Road, Nankai District, Tianjin, 300072, People’s Republic of China, Email [email protected] Ting Yang, Department of Pulmonary and Critical Care Medicine-Japan Friendship Hospital, No. 2, East Yinghua Road, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Introduction: Quantifying the disease burden across severity levels is essential for early intervention and effective management of chronic obstructive pulmonary disease (COPD). This study aimed to clarify the effect of severity on disease burden by comparing clinical and economic outcomes stratified by disease severity based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) in a Chinese setting.
Methods: A retrospective population-based cohort study was conducted using electronic health records of 80 hospitals (2016– 2019). Patients (≥ 40 years) diagnosed with COPD (ICD-10: J44) between 2017 and 2018 were identified and further classified into high (GOLD E) or low (GOLD A/B) exacerbation risk groups based on 12-months pre-index exacerbation history. GOLD groups A, B, and E were categorized based on exacerbation history and prior symptom burden. Clinical and economic outcomes were examined during 12-months follow-up, including incidence and time intervals between exacerbations, mortality, healthcare resource utilization, and direct medical costs.
Results: Among 6759 COPD patients (mean age 68.36 ± 11.46 years, 62.4% male), patients in group E (N=2378) showed significantly worse outcomes than group A/B (N=4381): 57% higher exacerbations risk (90.5 vs 70.5%, adjusted hazard ratio [HR]=1.57; 95% CI: 1.48– 1.67), 31% higher risk of all-cause mortality (11.6 vs 6.6%, HR=1.31; 95% CI: 1.10– 1.57), and 1.7-fold higher COPD-related total costs (Chinese yuan [CNY] 21,156 vs 12,457, adjusted difference CNY 4238) during follow-up. Notably, the incidence rates of overall exacerbation, total costs increased progressively from group A to B to E in the year following the index date.
Conclusion: Poor prognosis and high economic burden were observed among Chinese patients with COPD. Higher disease severity was associated with increased risk of exacerbation, all-cause mortality, and economic burden. These findings underscore the need for early intervention in patients with mild COPD to prevent disease progression, subsequent exacerbations, and rising economic impacts.
Keywords: chronic obstructive pulmonary disease, acute exacerbation, healthcare resource utilization, costs, disease severity
Introduction
Chronic obstructive pulmonary disease (COPD), characterized by airflow limitation, was the third leading cause of death worldwide in 2020, causing substantial and increasing economic and societal burdens.1–3 In China, the prevalence of COPD has reached 13.7% in individuals over 40 years old, accounting for nearly 100 million cases.4 Over the past decade, the credible framework recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) has been widely adopted to stratify patients into disease severity groups, A, B, C, and D, with increasing severity based on risk of exacerbation and symptoms.5 Different treatment regimens are recommended for each severity group, and patients with higher disease severity are at a greater risk of acute exacerbation, which indicates deteriorating health status and enormous disease burden. GOLD 2023 was published with a modified ABCD assessment tool.6 Groups A and B remain unchanged, and former groups C and D are merged into a single group, E (exacerbations) to highlight the clinical relevance of exacerbations. Future pharmacological treatment recommendations are implicated, and the need for practical validation of this updated framework is proposed.
Most existing studies have focused on the clinical and economic burden of overall patients with COPD or those initiating certain medications, without stratification by severity. Only a few studies have investigated the differences across severity groups, referring to earlier versions of the GOLD reports. Two studies in England found that highly symptomatic patients (groups B and D) were at greater risk of exacerbation (0.10–0.27 in groups B/D vs 0.01–0.08 in groups A/C, per person per year) and mortality (5.4–7.8% in groups B/D vs 1.9–2.8% in groups A/C, annually), results that need to be verified in other counties.7,8 Among the three studies exploring the relationship between severity and economic burden, studies in Greece and China found that total costs increased in line with disease severity (D>C>B>A),9,10 whereas inconsistent results were reported in Denmark (D>B>C>A).11 In addition, no study has simultaneously quantitatively investigated the effects of disease severity on clinical outcomes and economic burden. In particular, owing to the lack of biochemical indications and patient self-reported questionnaires, identifying different disease severity groups based on retrospective data is one of the major challenges facing real-world analysis of COPD, especially for evidence stratified by disease severity. In addition, modification of the grouping framework in GOLD 2023 has limited research conclusions on backwardness and has unquestionably raised new requirements for evidence.
In China, awareness and treatment of COPD remain inadequate, as evidenced by low diagnosis and treatment rates.12,13 COPD constitutes a major public health problem reaching an epidemic with an unacceptably low awareness rate (about 0.9%), compared with hypertension and diabetes which were included in the National Basic Public Health Services (NBPHS) project.14 Research shows that nearly 48.6% of COPD patients were prescribed inhaler regimens inconsistent with clinical guidelines three months post-hospitalization, reflecting under-prioritization of COPD management.15 Delays in diagnosis and treatment can lead to disease progression and exacerbation, which further increases the severity of the condition and the associated disease burden. Health-related quality of life is also substantially compromised in patients with COPD, and this decline becomes more pronounced as the disease progresses.16 Although China has established a public health insurance system, individuals with chronic diseases such as COPD still have substantial out-of-pocket expenses.17
Therefore, this study aimed to compare the real-world clinical outcomes, healthcare resource utilization (HRU), and cost of patients with COPD across different disease severity groups in a Chinese setting, based on GOLD 2023, to fill the evidence gap of clinical and economic outcomes across different severity groups and to provide a reference for the validation of the updated ABE framework.
Methods
Data Source
Data for this retrospective cohort study were obtained from the electronic health records held by 80 secondary and tertiary hospitals in Tianjin, China. Extracted data included longitudinal views of patient-level demographics; medical records of inpatient, emergency, and outpatient services; prescriptions and procedures; and related medical and medication costs. Information about mortality was recorded separately and linked to unique de-identified codes. The Ethics Committee of Tianjin University approved the study protocol before study initiation (approval number: TJUE-2021-171).
Patient Identification
Identification of Patients with COPD
Patients with COPD were identified as those who had experienced ≥1 inpatient primary diagnoses or ≥2 outpatient diagnoses (ICD-10 codes J44, supplemented by Chinese free texts) between January 1, 2017, and December 31, 2018 (identification period). The date of the first COPD diagnosis was defined as the index date. Patients aged ≥40 years were further identified and required to have continuous medical records during the 12 months prior to (baseline period) and 12 months following the index date, with discontinuation due to death was allowed (Supplementary Figure 1). Patients without evidence of COPD (J44) or related complications, including respiratory tract infection (J00-J06, J12-J18), acute exacerbation of chronic bronchitis (J47.1), and respiratory failure (J96) during the baseline period, were excluded as incident COPD patients at the index date. The included patients were followed up until death or data cutoff (December 31, 2019), whichever came first.
Groups of Patients with Different Disease Severity
According to the combined COPD assessment recommended by GOLD and the National Guidelines for COPD Diagnosis and Treatment issued by the Chinese Thoracic Society, the included patients were first classified into low exacerbation risk (A/B) and high exacerbation risk (E) groups.5,18 Patients free of exacerbation events or who had experienced only one exacerbation event without hospital admission during the 12-month baseline period were classified into group A/B; patients with ≥1 hospitalization with a primary diagnosis of COPD or ≥2 moderate or severe exacerbations were classified into group E. Moderate exacerbation was identified with any diagnosis (primary or non-primary) of COPD or respiratory tract infection without respiratory failure, combined with the prescription of antibiotics or corticosteroids. Severe exacerbation was inferred by emergency department (ED) visits or inpatient admissions with a primary diagnosis of COPD, or outpatient or inpatient admission with any diagnosis of respiratory failure. Specifically, successive exacerbation records within a period of <14 days were merged into one episode, and the merged exacerbation was deemed severe if there was ≥1 severe exacerbation among all records within 14 days; otherwise, it was deemed moderate exacerbation.
Groups A and B were further classified. Given the unavailability of the modified British Medical Research Council Dyspnea Questionnaire (mMRC) and COPD Patient Self-Assessment Test (CAT) scores, which serve as the standard criteria for assessing highly symptomatic patients (mMRC ≥2 or CAT ≥10),5,18 several proxy indicators were explored based on clinical guidelines, published literatures and expert opinions in China to distinguish between highly or lowly symptomatic patients.5,18,19 Patients were identified as group B from group A/B if they met any one of the following alternative criteria during the baseline period: (a) ≥1 diagnosis of respiratory failure; (b) ≥4 pharmacy records for short-acting beta2-agonist (SABA) or short-acting antimuscarinic antagonist (SAMA) over a 12-month period or ≥2 pharmacy records for SABA or SAMA over a 6-month period; (c) ≥3 medical records with a COPD diagnosis over any 3 months; (d) ≥3 medical records with a dyspnea or cough diagnosis; (e) ≥1 medical record with a dyspnea or cough diagnosis and ≥1 medical record for lung function tests; and (f) treatment escalation (step-up) from a single bronchodilator to dual therapy or from dual to triple therapy. The remaining patients were classified into group A (Supplementary Figure 2).
Outcome Measures
The clinical outcomes examined included the incidence of all-cause mortality and the risk of moderate, severe, and overall COPD exacerbations during the follow-up period. The proportions of patients who experienced exacerbation (%), incidence of exacerbation events, and time intervals between exacerbations were calculated. The incidence of exacerbations was measured as the total number of exacerbations divided by the total number of follow-up years (per person per year, PPPY).
Both all-cause and COPD-related HRU and costs were assessed during the 12-month follow-up period. Visits and admissions with diagnosis of COPD and related complications were identified as COPD-related. HRU per patient was assessed using the percentage of patients who utilized inpatient services, number of admissions and outpatient visits, and annualized length of stay (LoS). Direct medical costs were estimated from the perspective of the healthcare system: payments by insurers and patients. The total costs included the costs of hospitalization and outpatient services, and cost decomposition was investigated, including the costs of medications, examinations, and treatments (eg, nursing and monitoring).
Statistical Analysis
All baseline characteristics and outcome measures were descriptively evaluated for each group. Continuous variables are reported as means and standard deviations (SD), and categorical variables are summarized as frequencies (N) and proportions (%). Statistical significance of differences between groups was assessed using the t-test, rank sum test, and analysis of variance for continuous variables, as well as the chi-square test for categorical variables. Multivariable regression models were constructed to assess the effect of disease severity (mild/severe) on clinical outcomes, HRU, and costs, including the Cox proportional hazard regression model for exacerbations and all-cause death, logistic regression model for hospitalization, negative binomial regression model for number of admissions and visits, and generalized linear model (GLM) with gamma distribution and log-link function for direct medical costs, in which the adjusted cost differences were obtained using the recycled prediction method. Controlled covariates included demographic characteristics (age, sex), the Charlson comorbidity index (CCI), baseline comorbidities (hypertension, coronary heart disease, arrhythmia, etc.), and baseline healthcare resource utilization. Statistical significance was defined as a two-sided p-value of <0.05. Post-hoc power calculations using observed parameters demonstrated >99% power to detect group differences in mortality and exacerbation rates, and 86% power for cost comparisons at α=0.05 (two-tailed). All statistical analyses were performed using STATA version 13.1 (StataCorp, Texas, USA).
Results
Group A/B vs Group E
Sample Selection and Baseline Characteristics
A total of 11,167 patients with COPD were identified between 2017 and 2018; 6759 patients were finally included (Figure 1). The mean age of included patients was 68.36±11.46 years; 62.4% were male (Table 1). The mean CCI score was estimated to be 3.15±2.51. The prevalence of comorbidities was relatively high, with coronary heart disease (72.3%) being the most common comorbidity, followed by hypertension (70.5%), and dyslipidemia (53.2%) (Supplementary Table 1). In total, 32.1% of patients experienced at least one hospitalization during the baseline period, and total costs were estimated in Chinese yuan (CNY) to be 23,925±32,158 per year. The mean number of overall exacerbations was 1.60±2.30 per patient, annually.
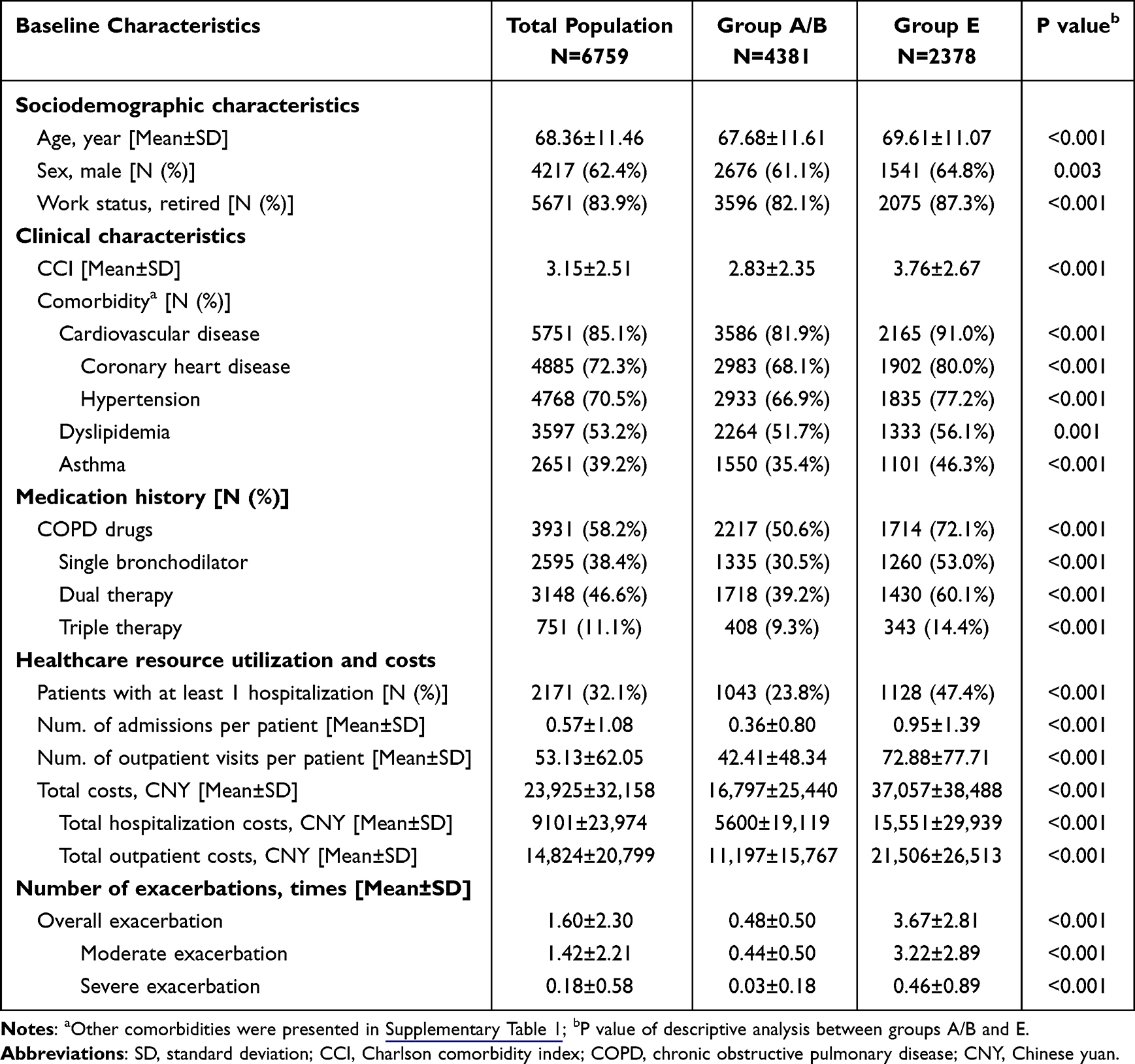 |
Table 1 Baseline Characteristics of Total Population, Group A/B and E |
 |
Figure 1 Sample selection flow chart. |
Of all patients, 64.8% (N=4381) were categorized into group A/B and 35.2% (N=2378) into group E. Compared to patients in group A/B, patients in group E were older (69.61 vs 67.68 years, p<0.001), had worse health status (CCI: 3.76 vs 2.83, p<0.001), included a higher percentage of COPD-related drug users (72.1% vs 50.6%, p<0.001), and accordingly posed a heavier economic burden (total costs: CNY 37,057 vs CNY 16,797, p<0.001) during the baseline period.
Association Between Disease Severity and Clinical Outcomes
The overall prognosis of patients with COPD was poor, with 77.6% of patients experiencing ≥1 exacerbation event and 8.4% of patients dying during the 12-month follow-up period (Table 2). Narrowing time intervals between multiple successive exacerbations were also observed in the total population.
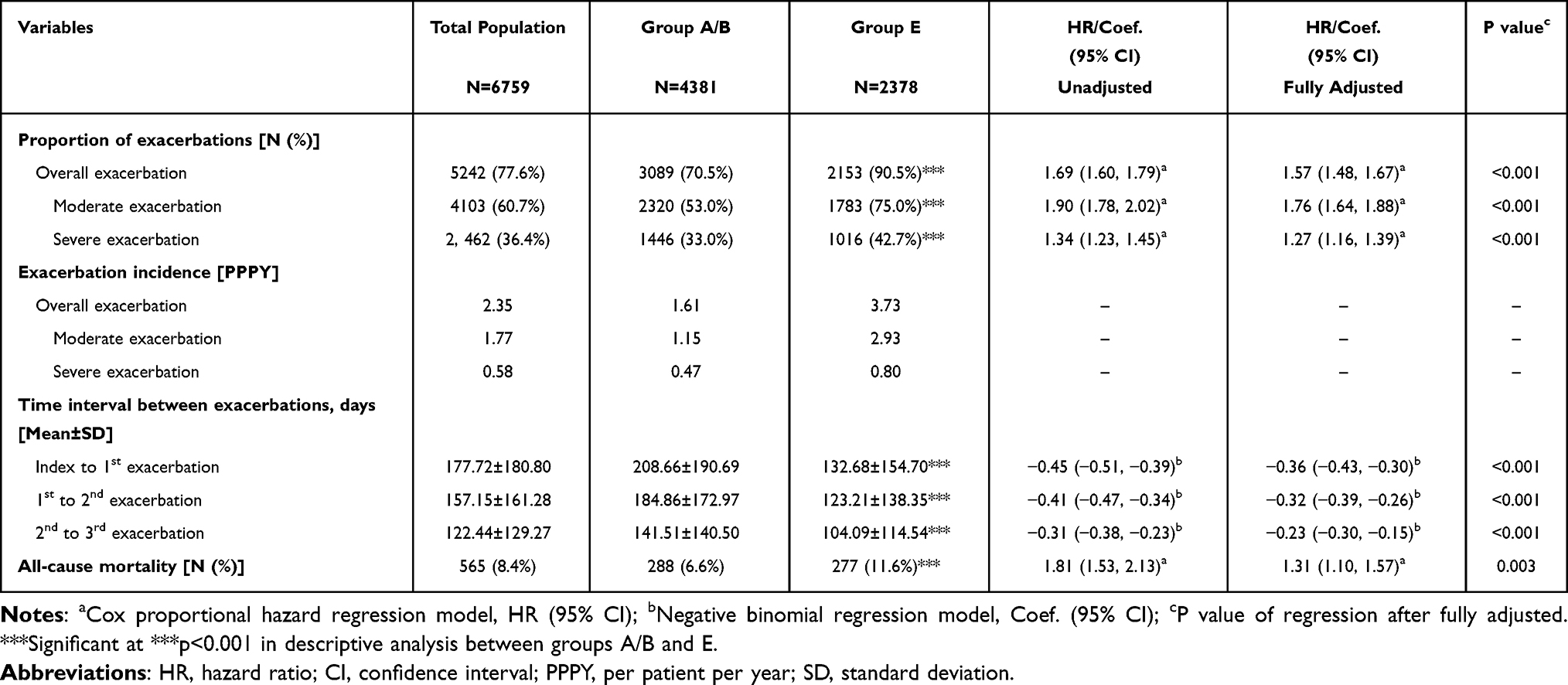 |
Table 2 Exacerbations and Mortality in the 12 months After Index of Total Population, Group A/B and E |
Compared with patients in group A/B, patients in group E had a 57% higher risk of overall exacerbation (90.5 vs 70.5%, adjusted hazard ratio [HR]=1.57; 95% CI: 1.48–1.67, p<0.001), 76% higher risk of moderate exacerbation (75.0 vs 53.0%, HR=1.76; 95% CI: 1.64–1.88, p<0.001), and 27% higher risk of severe exacerbation (42.7 vs 33.0%, HR=1.27; 95% CI: 1.16–1.39, p<0.001). The incidence rate of overall exacerbations (3.73 vs 1.61 PPPY), moderate (2.93 vs 1.15 PPPY) and severe exacerbation (0.80 vs 0.47 PPPY) were also higher in group E. Patients in group E were associated with more frequent exacerbations with shorter time intervals to next exacerbations (p<0.001) and had a higher risk of all-cause mortality (11.6 vs 6.6%, HR=1.31; 95% CI: 1.10–1.57, p=0.003) compared to group A/B.
Association Between Disease Severity and Economic Burden
Of all patients, 39.4% had at least one COPD-related hospitalization during the 12 months of follow-up, with mean number of admissions per patient estimated to be 0.72±1.22 (Table 3). Total annual COPD-related costs (CNY 15,517±CNY 31,673) accounted for approximately half (48.0%) of the total cost (CNY 32,337±41,271) among total population. 82.9% of COPD-related costs were attributed to hospitalization costs (CNY 12,857±CNY 31,367). Patients in group E were more likely to be hospitalized (46.1 vs 35.8%, adjusted difference 4.5%, p<0.001) due to COPD and had a higher number of admissions (0.96 vs 0.59, adjusted difference 0.15, p<0.001) and outpatient visits per patient (10.83 vs 6.32, adjusted difference 3.01, p<0.001) (Supplementary Figure 3). COPD-related total costs were 1.7-fold higher in group E than in group A/B (CNY 21,156 vs CNY 12,457, adjusted difference CNY 4238, p<0.001), largely driven by higher hospitalization costs (CNY 17,363 vs CNY 10,410, adjusted difference CNY 3211, P=0.006). All-cause HRU and costs were significantly higher in group E than in group A/B in the descriptive analysis, but the differences were not significant between the two groups after full adjustment, except for all-cause medication costs (Supplementary Table 2).
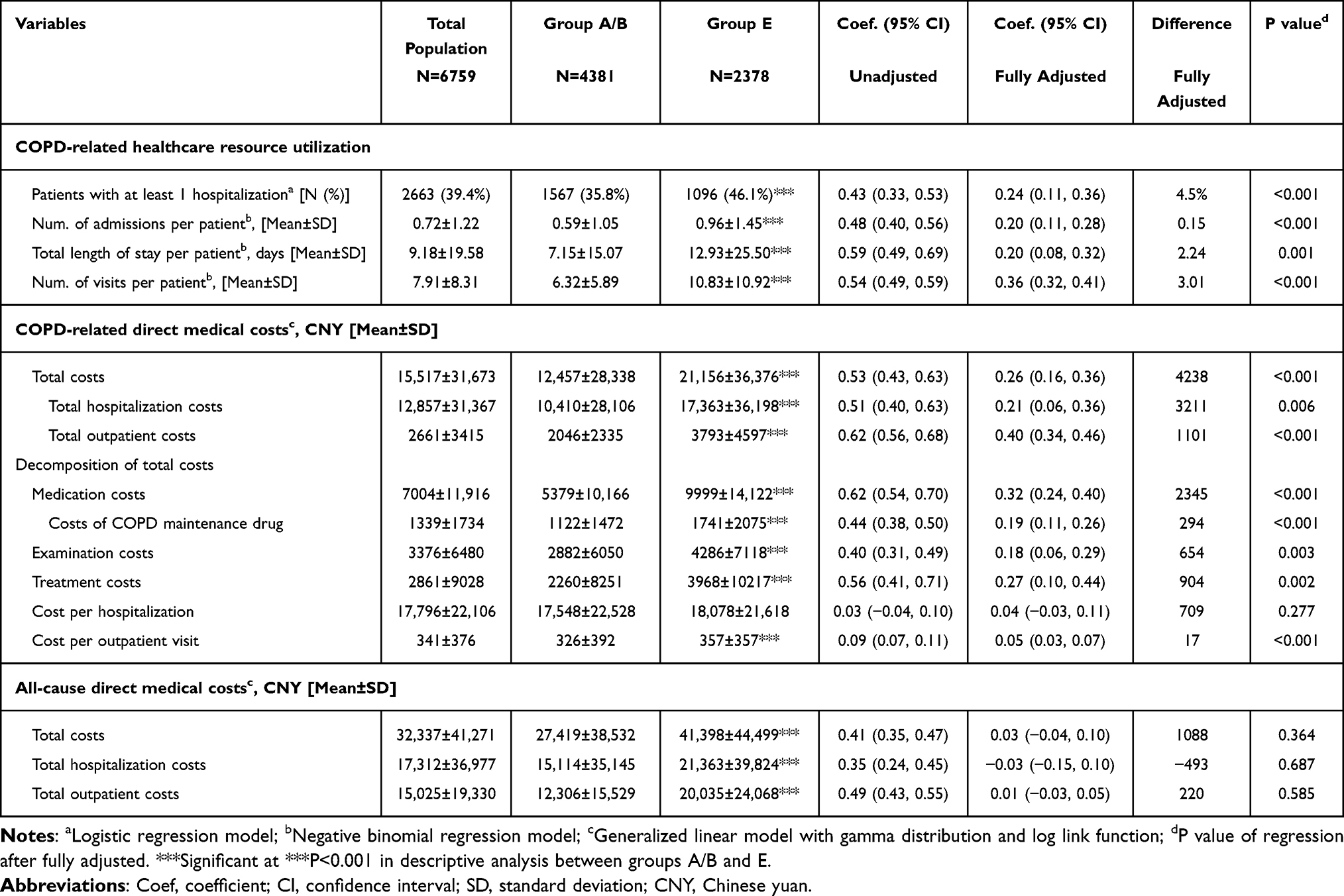 |
Table 3 COPD-Related and All-Cause HRU and Costs in the 12 months After Index of Total Population, Group A/B and E |
Comparisons Among Groups A, B, and E
Baseline Characteristics
After further identification, 39.9% (N=2697) of patients were classified into group A and 24.9% (N=1684) into group B. Baseline characteristics of patients in groups A, B, and E are presented in Supplementary Table 3. The mean age of patients was highest (69.61 years) in group E and the lowest in group A (68.19 years). More than 60% of patients in all groups were men, with the largest proportion in group E (64.8%). In groups A to E, the CCI scores increased from 2.72 to 3.76 (p<0.001), and the proportions of patients with comorbidities, HRU, and costs, as well as the number of exacerbations per patient (0.46 to 3.67 from group A to E, p<0.001) also increased accordingly with the increase in disease severity during the 12-month baseline period.
Clinical Outcomes
The proportion of patients who experienced ≥1 exacerbation event and the incidence rate of overall exacerbation in the 12 months following the index increased in line with COPD severity (E>B>A) (Table 4). The risk of moderate (75.0 vs 51.4%, HR=1.79; 95% CI: 1.66–1.94, p<0.001) or severe exacerbation events (42.7 vs 35.8%, HR=1.20; 95% CI: 1.09–1.32, p<0.001) was greater among patients in group E than in group A after full adjustment. The risk of all-cause death in the 12-month follow-up period was highest in group E (11.6%), followed by groups A (7.0%) and B (5.9%).
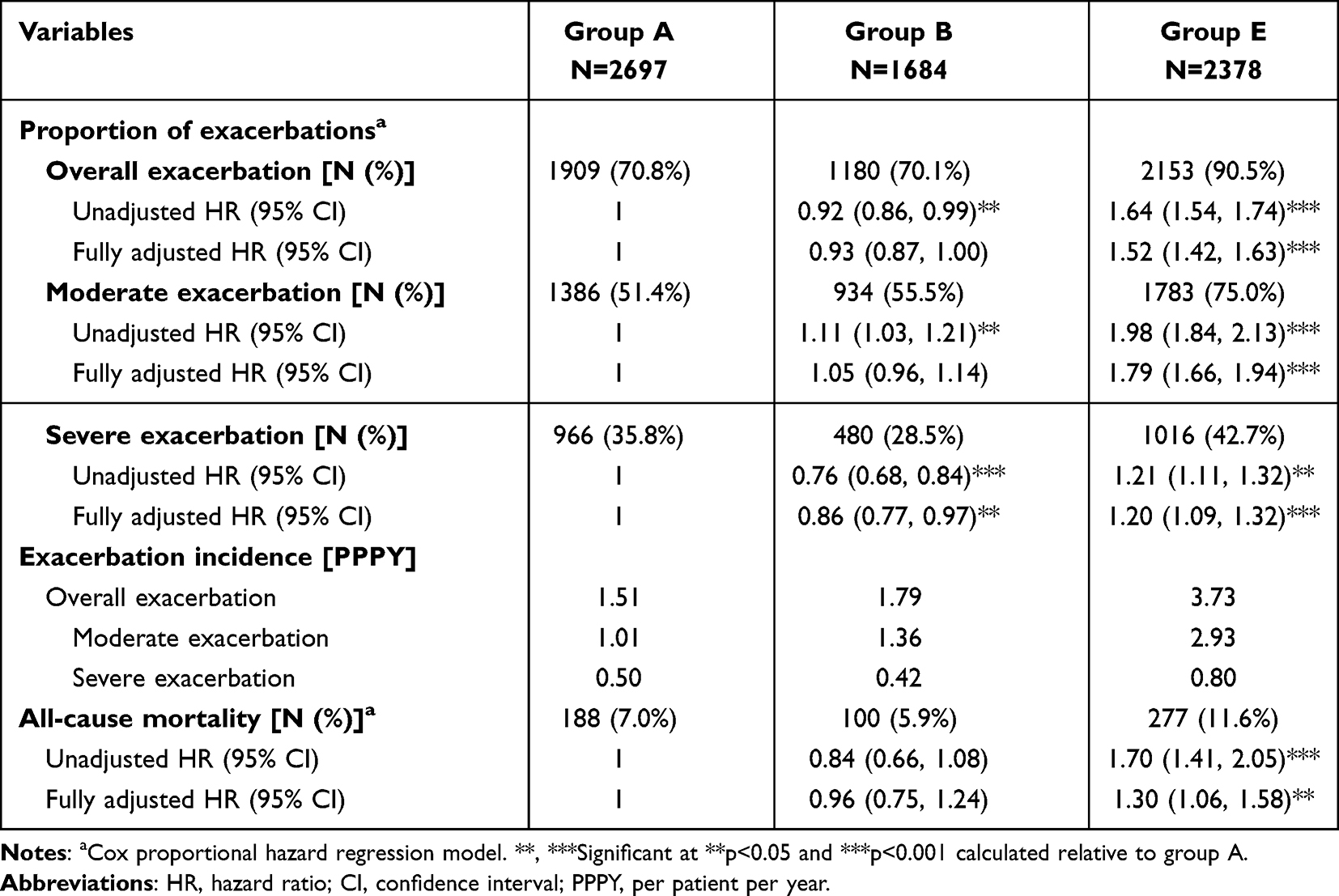 |
Table 4 Clinical Outcomes in the 12 months After Index of Group A, B, and E |
Economic Burden
The number of COPD-related admissions per patient in the 12 months following the index date was highest in group E (0.96), compared with groups A (0.63) and B (0.53) (Table 5). Patients in the higher symptomatic group experienced more COPD-related outpatient visits than those in the lower symptomatic group (8.04 in group B and 5.24 in group A). Group E was responsible for a 1.7-fold higher total COPD-related cost than Group A (CNY 21,156 vs CNY 12,310, adjusted Coef. =0.29, 95% CI: 0.17–0.40, p<0.001). In all groups, all-cause total costs (from CNY 25,767 to CNY 30,736, p<0.001) in the year following the index date increased in line with COPD severity (Supplementary Table 4).
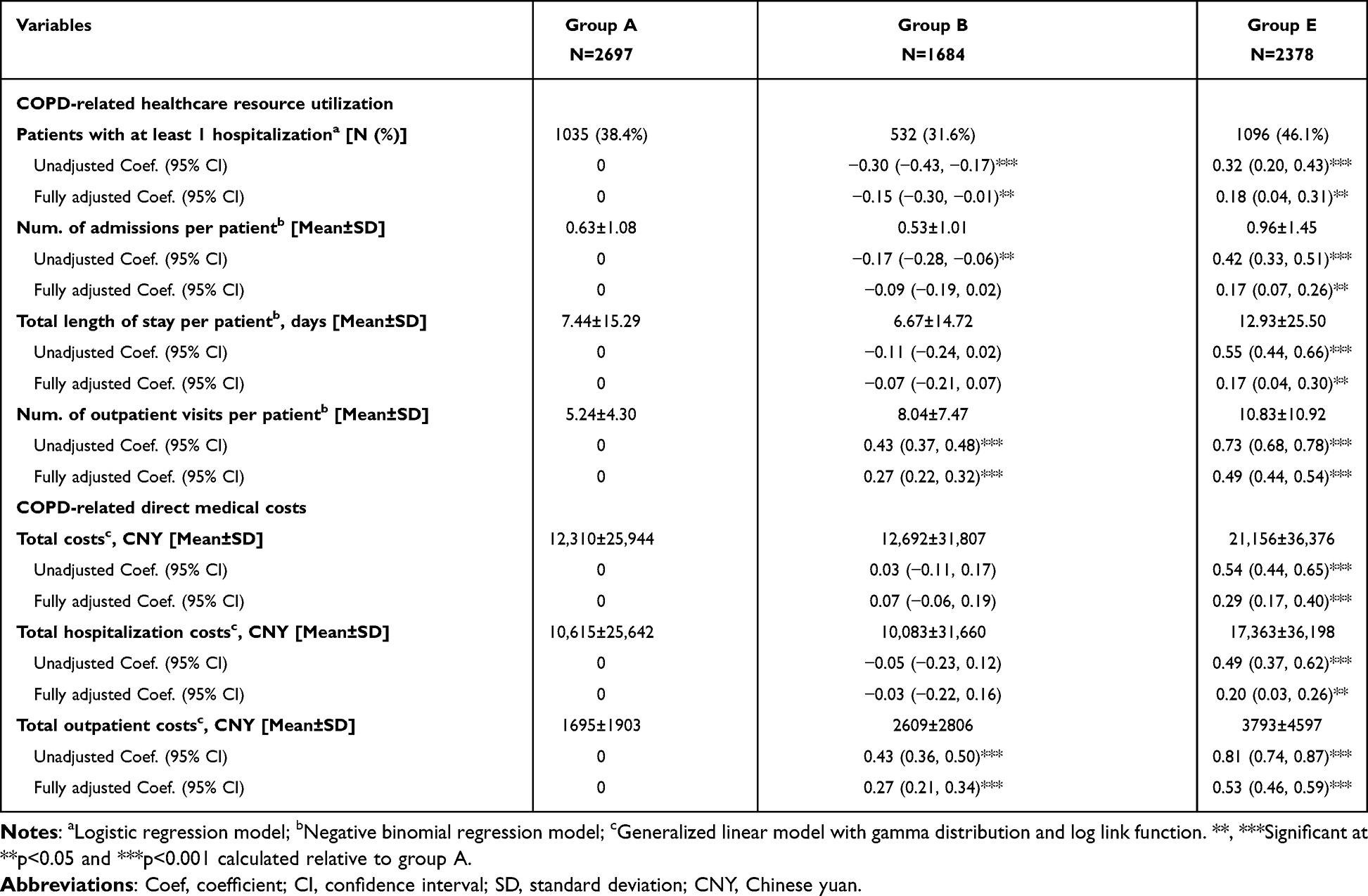 |
Table 5 COPD-Related HRU and Costs in the 12 months After Index of Group A, B, and E |
Discussion
This retrospective population-based cohort study provided precise insights into the clinical outcomes and economic burden posed by COPD stratified by disease severity in Tianjin, China. Our results highlight the poor prognosis of and high economic burden among Chinese patients with COPD, and patients with higher disease severity (group E) were associated with 57% higher risk of exacerbation and 31% higher risk of all-cause mortality than group A/B, with a 1.7-fold increase in total direct medical costs between the two groups. The results across the GOLD 2023 disease severity groups further demonstrated that clinical outcomes and economic burden increased in line with increases in disease severity.
According to this study, the clinical prognosis of patients with COPD in China was poorer than that in Europe and North America, as indicated by almost twice the proportion of patients experiencing exacerbation events within a 12-month period (77.6 vs 34.7%-48.1%) and a higher exacerbation rate (2.35 vs 1.01 PPPY).20,21 The management of COPD was insufficient and was further revealed by cost decomposition. First, in contrast to studies on other similar chronic diseases, such as diabetes (66.2%),22 COPD-related costs were less prominent in total costs (accounting for 48.0%), which indicated that patients with other comorbidities did not pay enough attention to the management of COPD. Unoptimistic routine care and prevention also showed that COPD-related costs were mostly driven by hospitalization, compared with a previous Danish study (82.9 vs 53.7%),11 while outpatient visits were not as regular as expected (7.91 times per patient annually).
Our analyses indicated that a higher disease severity was associated with a higher risk of exacerbations and mortality. To our knowledge, this is the first study to classify patients with COPD into three different severity groups according to the latest GOLD 2023 guidelines. Previous studies divided patients into four groups, A, B, C, and D, and exacerbation trends in two British studies were inconsistent with disease severity (D>B>C>A) – at least four times lower exacerbation risks in each group compared with our study. This was possibly due to population heterogeneity in different countries and the prospective design, which also highlights the poorer prognosis of patients in China and the importance of COPD management.7,8 In addition, our study innovatively estimated the difference between groups A/B and E, and revealed that baseline exacerbation risk could predict the follow-up clinical outcomes of patients. Furthermore, few studies have explored the time intervals between exacerbations in different severity groups, and our findings are significant in suggesting that patients with higher disease severity should pay more attention to preventing the recurrence of exacerbations.
In general, COPD-related HRU increased in line with the severity indicated by our study, which is consistent with findings in the UK.8 In terms of costs, our study verified the increasing trends in COPD-related costs from mild to severe severity in previous studies in Greece and China,9,10 with the cost difference almost twice as high as the previous Chinese study. This may be because it only included patients in a stable condition or different annual cost estimations (inferred by three-month follow-up costs) may be another reason; they may contain significant errors considering the natural progression of COPD.10
As one of the four major chronic diseases in China as well as internationally, COPD is given far less attention than cardiovascular diseases, cancer, and diabetes, which leads to insufficient diagnosis and treatment, poor prognosis, and high disease severity. Relative to COPD, remarkable improvements in public awareness and clinical management have been achieved for two other major chronic diseases, hypertension and diabetes. One important explanation for this situation is that hypertension and diabetes were included in the NBPHS project launched by the Chinese government in 2009 with the aim of improving health service continuity and regional equality.23 The current NBPHS is dedicated to disease management at an early age and now covers 12 services following major adjustments from 2009 to 2024, which provide disease screening, diagnosis and regular treatment for residents at primary healthcare institutions. The evidence gap for COPD was one of the major barriers to inclusion in the NBPHS, which was partially filled by the present study. This research also emphasizes the necessity of including COPD in the NBPHS in China to ensure early management to prevent disease progression and decrease the economic burden for patients and the healthcare system.
The major strength of this study is the innovative division of patients into groups according to disease severity based on GOLD 2023 (from A to E), which may provide valuable evidence supporting the modified grouping framework and corresponding management recommendations. We also performed the analysis based on the previous framework (not reported). The small percentage of patients classified into group C and the minor differences between groups C and D may also validate the efficiency and feasibility of the current merged framework. To distinguish between patients with high and low symptom burden, we performed explorations to simulate proxy indicators for CAT/mMRC scores, based on guidelines, published literature, and clinical opinions. This identification algorithm may provide a reference for future studies using similar data sources. Furthermore, differences in the distribution of disease severity existed between the current study and published literature, with group A/B accounting for a relatively higher proportion in our study than in previous studies (64.8 vs 33.4–85.5%).8,11,19,24,25 This may be partly explained by the use of proxy indicators to measure symptom burden, which could underestimate the proportion of group B patients. The different distributions may also be explained by insufficient awareness and diagnosis of COPD in China and different epidemiological distributions in different countries, which indicates the importance of localized management of COPD.
Our study had some limitations. First, early stage patients may not seek medical advice if they are asymptomatic or their symptoms are tolerable and thus remain undiagnosed, leading to underestimation of COPD diagnosis based on ICD-10 codes and Chinese words. In addition, owing to the lack of CAT or mMRC scores in the database, there may be an underestimation in the proportion of group B (high symptom burden) patients based on proxy indicators in this study, although clinical expert opinions were considered. While sensitivity analysis would be valuable, our anonymized database precludes patient-level verification. However, one validation study showed moderate agreement between claims-based data and clinical measures in COPD severity.26 Future studies incorporating both electronic health record (EHR) data and patient-reported outcomes are needed to refine these classification approaches. Lastly, the generalizability of our results is limited to the entire Chinese population. Clinical practice, related costs, and medical policies may be heterogeneous across urban and rural residents, as well as across various regions in China. Although our research findings represent the situation in urban tertiary care settings, significant disparities exist in rural areas. Specifically, the accessibility of spirometry in rural regions is notably lower than that in urban centers, which restricts the generalizability of our results to China’s rural population.4 Further studies based on multi-region populations are also warranted.
Conclusions
Poor prognosis and high economic burden were observed among Chinese patients with COPD, and a higher disease severity was associated with a higher risk of exacerbation, all-cause mortality, and economic burden. Paying more attention to patients with milder disease severity (early stage) can improve the quality of care for COPD patients in primary healthcare institutions. To prevent mild COPD from progressing to severe stages, public health departments should expand community-based screening programs, particularly for high-risk populations using digital monitoring tools. Meanwhile, healthcare authorities need to strengthen training for primary care physicians on early diagnosis and GOLD guideline adherence. Additionally, policymakers could consider subsidizing essential COPD medications to improve treatment accessibility. These steps would collectively mitigate disease progression and reduce its economic burden.
Abbreviations
COPD, Chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HRU, Healthcare resource utilization; GDP, Gross domestic product; ED, Emergency department; mMRC, Modified British Medical Research Council Dyspnea Questionnaire; CAT, COPD assessment test; SABA, Short-acting beta2-agonist; SAMA, Short-acting anti-muscarinic antagonist; PPPY, Per person per year; LoS, length of stay; SD, Standard deviation; GLM, generalized linear model; CCI, Charlson comorbidity index; CNY, Chinese yuan; HR, Hazard ratio; NBPHS, National Basic Public Health Services; EHR, Electronic health record.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available because of legal restrictions in China regarding the privacy of individual patient data from hospitals. However, some datasets are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Our study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Tianjin University (approval number: TJUE-2021-171). This retrospective study used de-identified data, and the requirement for consent to participate was waived by the Ethics Committee of Tianjin University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Natural Science Foundation of Tianjin, China (no. 21JCQNJC00660). The funder played no role in the study design, data collection, data analysis, or reporting.
Disclosure
The abstract of this paper was presented at the ISPOR Europe 2022 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Value in Health: https://doi.org/10.1016/j.jval.2022.09.2244. The authors declare that they have no competing interests.
References
1. Naghavi M, Abajobir AA, Abbafati C. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
2. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. Merino M, Villoro R, Hidalgo-Vega Á, Carmona C. Social economic costs of COPD in Extremadura (Spain): an observational study. Int J Chron Obstruct Pulmon Dis. 2018;13:2501–2514. doi:10.2147/COPD.S167357
4. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China pulmonary health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
5. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis m, and prevention of chronic obstructive pulmonary disease (2020 REPORT). Available from: https://goldcopd.org/goldreports/.
6. Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis management, and prevention of chronic obstructive pulmonary disease (2023 REPORT). Available from: https://goldcopd.org/.
7. Plutinsky M, Brat K, Svoboda M, Zatloukal J, Popelkova P, Koblizek V. Prognostic accuracy of three COPD classification systems in relation to long-term mortality of COPD patients: a prospective multicenter study. Lung. 2019;197(2):173–179. doi:10.1007/s00408-019-00196-6
8. Sansbury LB, Rothnie KJ, Bains C, Compton C, Anley G, Ismaila AS. Healthcare, medication utilization and outcomes of patients with COPD by GOLD classification in England. Int J Chron Obstruct Pulmon Dis. 2021;16:2591–2604. doi:10.2147/COPD.S318969
9. Stafyla E, Geitona M, Kerenidi T, Economou A, Daniil Z, Gourgoulianis KI. The annual direct costs of stable COPD in Greece. Int J Chron Obstruct Pulmon Dis. 2018;13:309–315. doi:10.2147/COPD.S148051
10. Li J, Feng R, Cui Y, Liu S, Zeng Z, Wang X. Analysis on the affordability and economic risk for using medicine to treat patients with chronic obstructive pulmonary disease in Tier 3 hospitals in China. Chinese Health Economics. 2015;34:66–68.
11. Løkke A, Lange P, Lykkegaard J, et al. Economic burden of COPD by disease severity - a nationwide cohort study in Denmark. Int J Chron Obstruct Pulmon Dis. 2021;16:603–613. doi:10.2147/COPD.S295388
12. Lyu X, Cong S, Fan J, et al. Analyses of the rate of spirometry examination and its related factors in chronic obstructive pulmonary disease patients aged 40 years or older in China, 2014-2015. Chin J Epidemiol. 2020;41:678–684.
13. Chen R, Gao Y, Wang H, Shang H, Xuan J. Association between adherence to maintenance medication in patients with COPD and acute exacerbation occurrence and cost in China: a retrospective cohort database study. Int J Chron Obstruct Pulmon Dis. 2020;15:963–971. doi:10.2147/COPD.S234349
14. Xu G, Fan G, Niu W. COPD awareness and treatment in China. Lancet Respir Med. 2018;6(8):e38. doi:10.1016/S2213-2600(18)30200-5
15. Baldomero AK, Kunisaki KM, Wendt CH, et al. Guideline-discordant inhaler regimens after COPD hospitalization: associations with rurality, drive time to care, and fragmented care - a United States cohort study. Lancet Reg Health Am. 2023;26:100597. doi:10.1016/j.lana.2023.100597
16. Kharbanda S, Anand R. Health-related quality of life in patients with chronic obstructive pulmonary disease: a hospital-based study. Indian J Med Res. 2021;153(4):459–464. doi:10.4103/ijmr.IJMR_1812_18
17. Yi B. An overview of the Chinese healthcare system. Hepatobiliary Surg Nutr. 2021;10(1):93–95. doi:10.21037/hbsn-2021-3
18. Chinese Thoracic Society. The guideline for the diagnosis and treatment of chronic obstructive pulmonary disease (2021 revision). Chinese J Tuberculosis Respiratory Dis. 2021;44:170–205.
19. Palli SR, Zhou S, Shaikh A, Willey VJ. Effect of compliance with GOLD treatment recommendations on COPD health care resource utilization, cost, and exacerbations among patients with COPD on maintenance therapy. J Manag Care Spec Pharm. 2021;27(5):625–637. doi:10.18553/jmcp.2021.20390
20. Fox C, Pace W, Brandt E, et al. Variation in demographic and clinical characteristics of patients with COPD receiving care in US primary care: data from the advancing the patient EXperience (APEX) in COPD registry. Pragmat Obs Res. 2022;13:17–31. doi:10.2147/POR.S342736
21. Sansbury LB, Lipson DA, Bains C, Anley GA, Rothnie KJ, Ismaila AS. Disease burden and healthcare utilization among patients with chronic obstructive pulmonary disease (COPD) in England. Int J Chron Obstruct Pulmon Dis. 2022;17:415–426. doi:10.2147/COPD.S336158
22. Mody R, Huang Q, Yu M, et al. Clinical and economic outcomes among injection-naïve patients with type 2 diabetes initiating dulaglutide compared with basal insulin in a US real-world setting: the DISPEL Study. BMJ Open Diabetes Res Care. 2019;7(1):e000884. doi:10.1136/bmjdrc-2019-000884
23. Zhao P, Diao Y, You L, Wu S, Yang L, Liu Y. The influence of basic public health service project on maternal health services: an interrupted time series study. BMC Public Health. 2019;19(1):824. doi:10.1186/s12889-019-7207-1
24. Ghosh S, Anderson WH, Putcha N, et al. Alignment of inhaled chronic obstructive pulmonary disease therapies with published strategies. Analysis of the global initiative for chronic obstructive lung disease recommendations in SPIROMICS. Ann Am Thorac Soc. 2019;16(2):200–208. doi:10.1513/AnnalsATS.201804-283OC
25. Yang T, Cai B, Cao B, et al. Severity distribution and treatment of chronic obstructive pulmonary disease in China: baseline results of an observational study. Respir Res. 2022;23(1):106. doi:10.1186/s12931-022-02021-w
26. Macaulay D, Sun SX, Sorg RA, et al. Development and validation of a claims-based prediction model for COPD severity. Respir Med. 2013;107(10):1568–1577. doi:10.1016/j.rmed.2013.05.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Prediction Model to Identify Acute Exacerbation of COPD and Its Severity for COPD Management in China (DETECT Study): A Multicenter, Observational, Cross-Sectional Study
Yin Y, Xu J, Cai S, Chen Y, Chen Y, Li M, Zhang Z, Kang J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2093-2106
Published Date: 5 September 2022
The Influence of Influenza Virus Infections in Patients with Chronic Obstructive Pulmonary Disease
Liao KM, Chen YJ, Shen CW, Ou SK, Chen CY
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2253-2261
Published Date: 14 September 2022
Analyses of Factors Associated with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Review
Qian Y, Cai C, Sun M, Lv D, Zhao Y
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2707-2723
Published Date: 24 November 2023
The Relationship of Fractional Exhaled Nitric Oxide in Patients with AECOPD
Xu X, Zhou L, Tong Z
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:3037-3046
Published Date: 21 December 2023
Glucocorticoid Use in Patients Hospitalized with Chronic Obstructive Pulmonary Disease Exacerbations
Yu S, Li S, Zhang J, Fang Q
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:431-438
Published Date: 12 February 2024