")
Back to Journals » International Journal of Nanomedicine » Volume 20
Illuminating Hope for Tumors: The Progress of Light-Activated Nanomaterials in Skin Cancer
Authors Lei H, Cui H, Xia Y, Sun F, Zhang W
Received 12 November 2024
Accepted for publication 3 April 2025
Published 18 April 2025 Volume 2025:20 Pages 5081—5118
DOI https://doi.org/10.2147/IJN.S506000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. RDK Misra
Huaqing Lei,1,* Hengqing Cui,2,3,* Yu Xia,4 Fujia Sun,4 Wenjun Zhang1
1Department of Burns and Plastic Surgery, Shanghai Changzheng Hospital, Shanghai, People’s Republic of China; 2Department of Plastic and Cosmetic Surgery, Tongji Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3Institute of Aesthetic Plastic Surgery and Medicine, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 4College of Mechanical Engineering, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjun Zhang, Email [email protected] Fujia Sun, Email [email protected]
Abstract: Skin cancer is a common malignant tumor that poses significant global health and economic burdens. The main clinical types include malignant melanoma and non-melanoma. Complications such as post-surgical recurrence, wound formation, or disfigurement can severely impact the patient’s mental well-being. Traditional treatments such as surgery, chemotherapy, radiation therapy, and immunotherapy often face limitations. These challenges not only reduce the effectiveness of treatments but also negatively impact patients’ quality of life. Phototherapy, a widely used and long-standing method in dermatology, presents a promising alternative for skin cancer treatment. Light-triggered nanomaterials further enhance the potential of phototherapy by offering advantages such as improved therapeutic precision, controlled drug release, minimal invasiveness, and reduced damage to surrounding healthy tissues. This review summarizes the application of light-triggered nanomaterials in skin cancer treatment, focusing on the principles, advantages, and design strategies of photodynamic therapy (PDT), photothermal therapy (PTT), and photoacoustic therapy (PAT). In this manuscript we have an in-depth discussion on overcoming translational barriers, including strategies to enhance light penetration, mitigate toxicity, reduce production costs, and optimize delivery systems. Additionally, we discuss the challenges associated with their clinical translation, including limited light penetration in deep tissues, potential toxicity, high production costs, and the need for advanced delivery systems.
Keywords: light-triggered, nanomaterials, phototherapy, skin cancer
Graphical Abstract:

Introduction
Skin cancer is the fifth most common cancer in the world, with an estimated 1.2 million new cases diagnosed annually and over 60,000 deaths attributed to melanoma alone. Non-melanoma skin cancers contribute significantly to healthcare costs, with an annual economic burden exceeding $8 billion in the United States.1,2 Skin cancers exhibit a high rate of recurrence and malignancy in humans, with over a million cases diagnosed, particularly among people of Caucasian descent.3 To this day, the incidence and mortality rates of skin cancer continue to increase. Melanoma skin cancer (MSC) and non-melanoma skin cancer (NMSC), including basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), account for 40% of all tumors in white patients, making them the most common malignant tumors in the United States.4 Compared to white patients, the incidence of MSC and NMSC is significantly lower in Asian American and Black patients, accounting for only 1% to 4%.5 Additionally, these patients are more likely to present with more aggressive skin cancers, thicker tumors, and metastases at the initial diagnosis.6 Currently, the treatment of skin cancer mainly relies on traditional therapies such as surgery, chemotherapy, radiotherapy, and immunotherapy. Traditional treatments, including surgery, chemotherapy, radiation therapy, and immunotherapy, often face significant challenges. For instance, low drug utilization and high drug resistance result in suboptimal therapeutic outcomes, while significant cytotoxicity and skin damage lead to physical discomfort and psychological distress, ultimately lowering the patient’s quality of life. Phototherapy, with its relatively lower side effects, is emerging as a promising alternative treatment option. Phototherapy has a long history, and the use of light energy (photons) alone for disease treatment is defined as phototherapy.7 Dating back to ancient Indian, Chinese, and Egyptian civilizations document that sunlight was used to treat diseases such as psoriasis, vitiligo, and skin cancer.8 Phototherapy involves the use of specific wavelengths of light to induce biological effects. Depending on the wavelength, intensity, and duration, phototherapy can trigger the generation of reactive oxygen species (ROS), cause localized heating, or enhance acoustic imaging. These effects are harnessed for targeted tumor ablation, often with minimal damage to surrounding healthy tissues (Figure 1A). Different tumors have varying levels of infiltration into the skin tissue, ranging from superficial in squamous cell carcinoma to deeper in melanoma (Figure 1B). The effectiveness of phototherapy largely depends on the depth of light penetration, which is determined by the wavelength used. Shorter wavelengths (eg, blue light) are effective for superficial lesions but are limited in treating deeper-seated tumors due to strong scattering and absorption by skin tissues. Conversely, near-infrared (NIR) light penetrates deeper into tissues, making it suitable for treating melanoma and other tumors located in deeper skin layers. This wavelength-specific penetration allows for tailored treatment approaches depending on the cancer type and its location. The controllable nature of light exposure during treatment results in very low side effects, making tumor phototherapy a promising option for clinical applications. Since skin tumors are generally more superficial, the requirements for light penetration are less stringent compared to deeper, solid tumors. Phototherapy is primarily categorized into PDT, PTT, and PAT, or the combined treatment of PDT and PTT,9,10 each with distinct mechanisms (Figure 1C).11 In addition, other research teams have utilized vibronic-driven action to activate aminocyanines under near-infrared light, causing membrane disruption and subsequently inducing cell death.12 Local drug application minimizes toxic side effects on normal cells, while the light-stimulated response ensures precise, targeted treatment, reducing drug waste. Currently, phototherapy has been widely applied in skin-related diseases. For example, PDT has been used for almost all types of skin cancer and many benign skin conditions, particularly BCC and SCC, which are the most common indications for PDT in dermatology.13 PDT has been used clinically for over 40 years. Although PTT drugs have the potential to enhance the local light heating and ablation efficiency of tumor tissues, they have not yet been extensively tested in large-scale clinical trials. In contrast, laser ablation techniques that do not include PTT drugs have already begun to have already begun to see widely clinical applications.14
 |
Figure 1 (A) Penetration depth of light with different wavelengths in the skin. (B) The layers of the skin. (C) The mechanisms of action for the three types of phototherapy. Created in BioRender. Lei, H (2025) https://BioRender.com/j19s773. |
In this review, we provide a brief overview of skin cancer and the challenges encountered with current treatment approaches. We summarize the features of light-triggered nanoparticle (NP) and various delivery systems used in skin cancer treatment. By summarizing recent research on phototherapy for skin cancer, we highlight three commonly used phototherapy strategies. We also address the challenges faced by light-triggered NPs in transitioning from bench to bedside and discuss future research directions.
Clinical Features of Skin Cancer
The Layering of the Skin and the Classification of Skin Cancer
The skin is composed of three layers: the epidermis, the dermis, and the subcutaneous tissue. The epidermis is the outermost layer of the skin, composed of melanocytes, keratinocytes, Merkel cells, and Langerhans cells.15 Generally, skin cancer commonly occurs in the epidermis. The development of skin cancer is influenced by a combination of factors, but ultraviolet (UV) radiation from sunlight is the primary pathogenic factor for the occurrence and progression of skin cancer globally.16
Melanoma and non-melanoma skin tumors account for more than one-third of all malignant tumors, making them the most common tumor types.16 Skin cancer is classified based on the cells of origin and clinical features and can be divided into NMSC and MSC.17 NMSC includes all non-melanoma malignant tumors affecting the skin.18 In epidemiological contexts, however, NMSC specifically refers to keratinocyte carcinoma, which includes BCC, SCC, and Cutaneous T-cell lymphoma (CTCL), as these account for 99% of this group of tumors (Figure 1B).19
MSC
Melanoma is considered a multifactorial disease and has the highest mutation rate among all cancers.20 Based on the common mutation patterns in melanoma, melanoma can be categorized into four subtypes. (i) BRAF-mutant (52% present), with BRAF mutations being the largest genomic subtype of melanoma. Patients are generally younger, and this mutation often originates from skin that does not have chronic sun damage. (ii) RAS-mutant (28% present), with most NRAS mutations in melanoma associated with intermittent UV exposure. Additionally, NRAS mutations are normally associated with melanoma arising from large congenital nevi. (iii) NF1-mutant (14% present), with the NF1 subtype characterized by notably older patient age. (iv) Triple-Wild type (6% present).21
Among the different UV wavelengths, UVA (315–400 nm) and UVB (280–315 nm) are primarily responsible for causing carcinogenic skin damage. UVA penetrates deeper into the dermis than UVB but has lower genotoxicity.22 UVA, also known as long-wave UV (UVA), has strong penetrating power. It is believed to cause skin damage and ultimately lead to tumor formation, primarily through DNA damage induced by oxidative stress.23 UVB, also known as medium-wave UV (UVB), causes direct DNA damage in the form of photoproducts, including cyclobutane pyrimidine dimers (CPDs) and 6–4 photoproducts (6–4PP). These photoproducts lead to nucleotide excision repair (NER) dysregulation. Defects in NER lead to xeroderma pigmentosum, a condition that increases the risk of developing skin cancer by 2000 to 10,000 times.24
The main subtypes of melanoma are superficial spreading melanoma, nodular melanoma, lentigo maligna melanoma, and acral lentiginous melanoma. Among these, superficial spreading melanoma is the most commonly diagnosed type of melanoma, accounting for 70–80% of cases, and is most commonly found in individuals aged 30–50 years.25
Melanoma incidence varies significantly among different racial groups. Compared to individuals with darker skin, white individuals are more prone to melanoma (2.4% vs 0.1%).15,26 In most white populations, cutaneous melanoma accounts for the majority of melanoma diagnoses (>90%), while mucosal and uveal melanomas are rare (<1-5% of diagnoses, with variation by country/region).27 In populations with fair skin in North America, Northern Europe, Australia, and New Zealand, the melanoma incidence rate increases by 4–6% per year.28 Non-white patients are more likely to develop melanoma on the soles of the feet and other less sun-exposed areas. Additionally, they may present with more advanced melanoma at diagnosis and generally have worse prognosis compared to white patients. Melanoma accounts for 1.7% of all cancer diagnoses and is one of the most common cancers globally.29
Although melanoma is the least common type of skin cancer, it is the most aggressive and lethal.30 The stage at which malignant melanoma is diagnosed is crucial for patient prognosis. Approximately 90% of melanomas are diagnosed as primary tumors without any signs of metastasis, with a 10-year survival rate of 75–95% for these tumors.31 Metastatic melanoma accounts for only 10–20% of cases, with patients typically having a poorer prognosis and a median overall survival of only 6–9 months. Additionally, the high resistance characteristics of metastatic melanoma significantly limit its treatment options.7
Light-induced materials offer significant potential for melanoma treatment by leveraging their ability to generate reactive oxygen species under light exposure, selectively targeting tumor cells while sparing healthy tissue. However, several challenges must be addressed to optimize their clinical application in melanoma. The high melanin content in melanoma cells strongly absorbs visible light, which can reduce the penetration depth and efficacy of light-based therapies. Additionally, sublethal phototherapy has the potential to induce adaptive responses in melanoma cells, including increased invasiveness and progression, which necessitates careful control of therapeutic parameters to avoid unintended outcomes. Addressing these challenges through the development of advanced light sources, near-infrared-responsive materials, and precise dosimetry will be crucial for improving the safety and efficacy of light-induced therapies in melanoma.
NMSC
Compared to melanoma, NMSCs, namely BCC, SCC and CTCL, have an incidence that is 18–20 times higher. However, NMSCs typically grow slowly and have low metastatic potential, which means they rarely result in death.14 Although NMSCs do not significantly impact mortality, their incidence continues to rise with age, with recent statistics showing over 1 million cases per year.29
BCC and SCC originate from keratinocytes and are collectively referred to as keratinocyte cancers. Their development is primarily influenced by long-term exposure to UV radiation and immune suppression. BCC accounts for 80–85% of all NMSC and rarely metastasizes to other organs.32 Although BCC is rarely fatal, it can cause significant disfigurement.33 SCC accounts for 15–20% of all NMSC. It exhibits locally destructive growth and invasion into surrounding tissues, and it more frequently leads to death compared to BCC.32 Light-activated nanomaterials, particularly nanoparticles loaded with photosensitizers, have shown significant potential in CTCL treatment. Upon exposure to specific wavelengths of light, these nanomaterials selectively release reactive oxygen species, inducing oxidative stress and programmed cell death in CTCL cells.
The treatment options for NMSC depend on tumor risk stratification, patient preferences or suitability, and the availability of local services, and most NMSC can be cured through surgery and radiation therapy.34 Surgery is the gold standard treatment for invasive NMSC, with a 5-year cure rate of over 95%. Potential drawbacks of surgery include pain during and after the procedure, costs, and adverse cosmetic outcomes, especially on the face. Furthermore, treatment options have historically been limited for locally advanced, recurrent, and/or metastatic NMSC, leading to a generally poor prognosis.35
Challenges in Skin Cancer Treatment
Biological Barriers
Anticancer drugs administered through the skin typically need to pass through two biological barriers to reach the target site and exert their effects. Nanotechnology has significantly advanced phototherapy by overcoming biological barriers. For example, nanoparticles can be engineered to target tumor-specific receptors, ensuring high drug accumulation at the tumor site. Oxygen-carrying nanomaterials address hypoxic tumor microenvironments, which limit ROS generation, while light-triggered nanoparticles enable precise spatial and temporal control over drug release, minimizing off-target effects. These advancements enhance the precision and effectiveness of phototherapy while addressing limitations associated with traditional treatments.
Firstly, it is the stratum corneum (SC) barrier of the skin, and secondly, the extracellular matrix barrier of tumor cells. Studies on skin anatomy reveal that the SC is the principal barrier preventing anticancer drugs from penetrating the skin and reaching the intended target.36 The SC, the outermost layer of the epidermis, is composed of layers of dead keratinocytes. These keratinocytes represent the final product of the terminal differentiation of epidermal keratinocytes and perform the barrier function of the epidermis. Unlike most biological membranes, the lipid composition of the SC is notably distinct; it is largely devoid of phospholipids and is primarily composed of long-chain ceramides, fatty acids, and cholesterol.37 The barrier function of the SC not only protects the body from pathogen invasion but also affects the penetration and uptake efficiency of therapeutic drugs. The SC of the skin is an effective barrier that limits the penetration of most drugs, making it very difficult to pass through the skin. Beneath the SC lies the active epidermis, which extends down to the thin basal layer connecting the dermis and the epidermis.38
In the treatment of skin cancer, transdermal drug delivery using nano-carriers or microneedles is a promising strategy. This approach can bypass first-pass elimination and increase local drug concentration, leading to improved therapeutic outcomes. However, there are currently only about 20 transdermal drugs on the market,39 largely due to the restrictive nature of SC.
Another biological barrier is the dense tumor microenvironment (TME) composed of collagen, proteins, elastic fibers, and glycosaminoglycans.40 Studies on skin cancer have shown that, compared to healthy tissue, cancer cells often exhibit increased levels of keratins and lipids, and the formation of keratotic papules and erythematous plaques.38 These findings suggest that tumor microenvironment can serve as a natural biological barrier for drug delivery.
TME consists of cancer cells, various stromal cells (including fibroblasts, immune cells, endothelial cells, and bone marrow-derived immature cells), cytokines (such as TNF, VEGF, IL-1), and chemokines (such as CXCL12, CCL27, CCL21).41 Within the TME, cancer cells interact closely with the extracellular matrix, stromal cells, and immune cells, promoting chronic inflammation and immune suppression.42 The ECM of tumor cells is a dense protein network surrounding both normal and cancer cells, creating a barrier to drug delivery and severely restricting the penetration of immunosuppressants and other antitumor drugs, as well as the infiltration of immune cells into tumor sites.43
MDR
Statistics show that over 90% of deaths among cancer patients receiving traditional chemotherapy or new targeted drugs are caused by MDR.44 MDR severely limits the effectiveness of conventional chemotherapeutic drugs in the TME. Currently, MDR has become a significant factor affecting the effectiveness of cancer chemotherapy.
Initially, cancer cells develop resistance to a single anticancer drug and then gradually acquire resistance to various anticancer drugs with similar structures but different mechanisms of action, thereby expressing MDR.1 MDR is a significant barrier to effectively treating various cancers, including skin cancer, particularly melanoma.45
MDR in cancer cells during chemotherapy can rise from various mechanisms, including enhanced drug efflux, genetic factors (such as gene mutations, amplifications, and epigenetic changes), growth factors, increased DNA repair capacity, and elevated heterologous metabolism.46 The causes of MDR can be broadly categorized into two main categories: physical resistance and biological resistance.
Both intrinsic and acquired resistance leading to MDR are similar, including two main types of resistance, known as “pump” and “non-pump” resistance.47,48 Pump resistance, the key mechanism behind physical resistance, relies on active drug efflux pumps associated with the cell membrane. These efflux transporters bind to anticancer drugs as they diffuse into the membrane, forming a drug efflux system that decreases drug affinity while expelling the drugs from the cytoplasm, thereby reducing drug absorption.49
Non-pump resistance, more closely aligned with biological resistance, encompasses mechanisms such as drug inactivation and degradation, the following categories: drug inactivation and degradation, anti-apoptotic and antioxidant defenses, DNA repair, replication, and biosynthesis. These processes diminish the efficacy of anticancer drugs in inducing cell death or converting drug-induced damage into cell death.50 Additionally, tumor-initiating cells or cancer stem cells, a distinct subpopulation known for their intrinsic resistance, play a crucial role in biological resistance.51,52 These cells exhibit self-renewal capabilities and can generate heterogeneous tumor cells, expressing stem cell markers and possessing tumorigenic potential significantly greater than that of ordinary tumor cells.
NPs have emerged as a promising approach to overcome tumor MDR.53 One of the primary advantages of encapsulating drugs in NPs is their ability to circumvent resistance.54 Conventional small-molecule chemotherapeutic drugs typically diffuse through the cell membrane, making them more susceptible to binding with drug efflux transporters. However, using NPs increases the molecular weight of the drugs, enabling cellular entry via endocytosis rather than diffusion, thereby reducing physical resistance.
From a biological resistance perspective, NPs improve drug uptake and selective intracellular accumulation in cancer cells through passive and active targeting strategies, while also minimizing toxicity to normal tissues. This approach addresses many limitations associated with conventional small-molecule chemotherapeutic drugs.55 Moreover, NPs used in phototherapy can generate reactive oxygen species (ROS) and initiate peroxide reactions, offering new opportunities for combating MDR in cancer cells.
Systemic Toxicity of Chemotherapy Drugs
The presence of drug resistance in cancer cells significantly impacts the effectiveness of chemotherapy. One common strategy to overcome drug resistance is to increase drug concentration or use multiple drugs with different mechanisms of action.50 However, high doses of anticancer drugs inevitably have adverse effects on normal tissue cells, leading to systemic toxicity.
When systemic toxicity is difficult to control, local drug administration becomes a favorable alternative. Phototherapy, which induces cytotoxic effects by generating reactive oxygen species (ROS) or heat locally, typically involves the use of photosensitizer (PS). Applying NPs in phototherapy allows for the development of a range of light-triggered NPs. Incorporating NP platforms can exploit their small size and targeting capabilities to specifically accumulate at tumor sites through enhanced permeability and targeting. Additionally, the localized action of phototherapy and its unique light stimulation patterns allow for local administration and activation of light-triggered NPs,56 thereby minimizing systemic side effects.
Skin Defects Following Tumor Excision
The rising incidence of skin cancer has spurred the development of various innovative treatment approaches. Treatment choices depend on the tumor’s location, stage, margins, and size.57 Surgery is widely regarded as the gold standard for skin cancer treatment due to its effectiveness and favorable cosmetic outcomes.58 However, surgical incisions can lead to issues such as infection and postoperative skin defects.
For larger lesions, surgery often results in significant skin defect in the affected area, which can lead to wound infection, scar formation and other complications. Research has shown that malignant skin tumors can also develop in chronic skin damage wounds and scars,59 indicating that adverse surgical incisions may increase the recurrence rate of skin cancer after surgery. Even when surgical margins appear clear in histological examination, incomplete resection of localized melanoma and other types of skin cancer may lead to recurrence due to the continued growth of residual cancer cells. Studies indicate that approximately 12% of patients experience local skin cancer recurrence after surgery because of residual cancer cells.60 Light-triggered NPs offer a promising solution for these challenges. They can selectively target and eliminate residual tumor tissue within wounds, control infection in large wounds, and promote wound healing, thereby reducing the likelihood of recurrence and improving postoperative outcomes.
Advantages of Light-Triggered NPs and Delivery Systems
Characteristics of Light-Triggered NPs
The main physicochemical characteristics of NP carriers are structure, composition, size, surface properties, porosity, charge, and aggregation behavior—play a crucial role in determining their therapeutic efficacy.61 After optimization, these properties primarily impact therapeutic outcomes by influencing the efficiency of transdermal delivery and clearance from the body.62 The development of NPs has greatly enhanced the efficiency of drug penetration through the skin. Typically, NPs that are smaller in size, non-spherical in shape, and positively charged exhibit superior skin penetration capabilities.63
Beyond these fundamental properties, certain specialized characteristics of NPs contribute to their enhanced role in phototherapy. There are common NP applications in tumor phototherapy in Table 1. However, tumors often experience hypoxia due to rapid oxygen consumption by cancer cells and insufficient blood supply, which can reduce the efficacy of PDT and increase the toxicity of PSs.64 Nanotechnology has provided innovative solutions to this challenge. NPs can be engineered as carriers for both oxygen and PSs, allowing for alternative methods of oxygen delivery. These NPs can selectively accumulate in tumors via active or passive targeting and release oxygen in situ, improving PDT outcomes in hypoxic environments.65
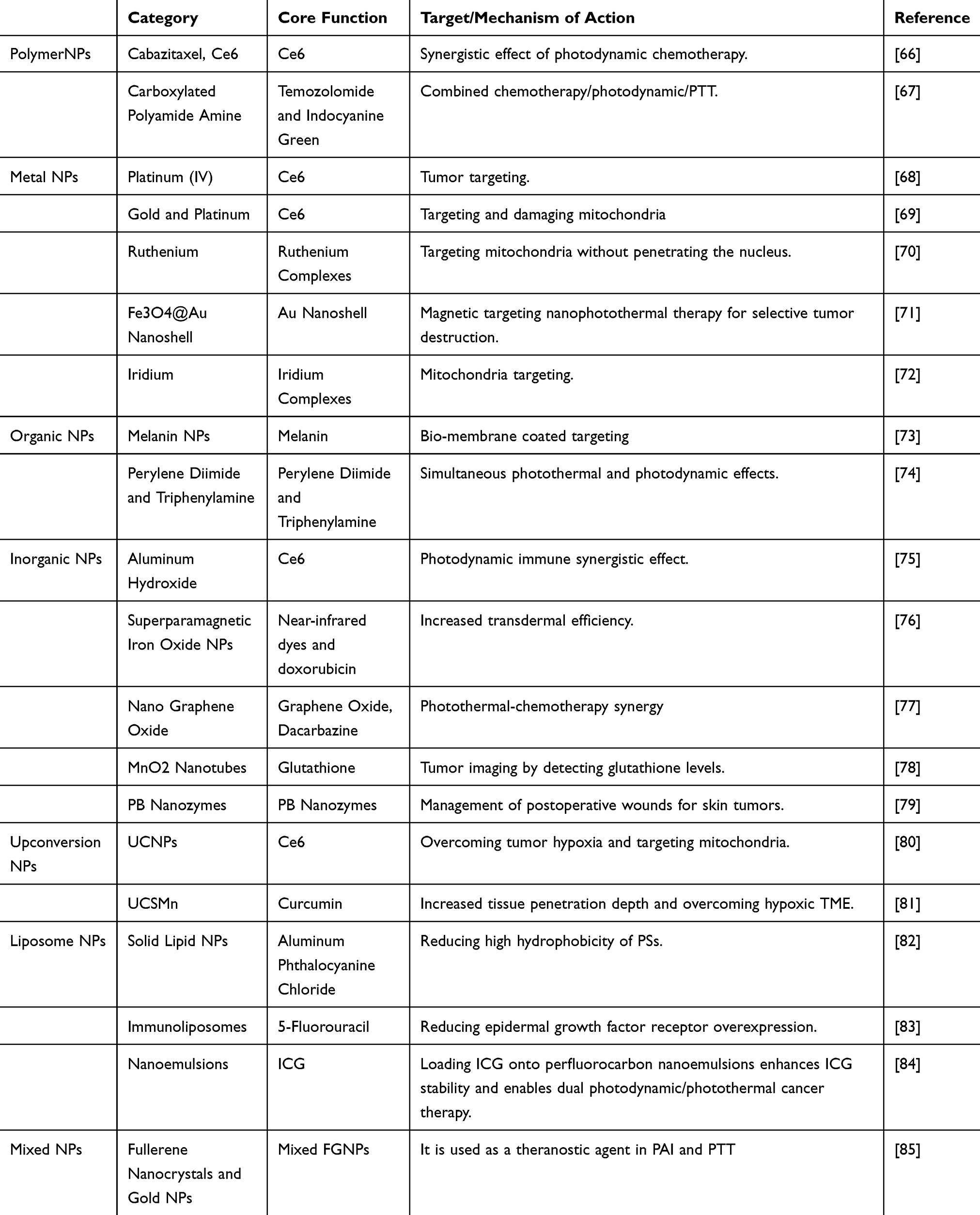 |
Table 1 Summary of NP Applications in Tumor Phototherapy |
In PTT, NPs can act as photothermal agent (PTA) to achieve the conversion of light into heat. Advances in NP-assisted hyperthermia and precise temperature control methods have enabled the application of higher therapeutic temperatures, enhancing the efficacy of PTT.86 Additionally, for larger tumors, the distribution of NPs within the tumor mass significantly influences the uniformity and effectiveness of heat distribution, ensuring more consistent therapeutic outcomes.87
Beyond their roles as drug carriers and therapeutic agents, NPs can also play a role in imaging and diagnosis. PA imaging is a technique that integrates optical imaging with therapeutic capabilities, where photoconverters within NPs serve as contrast agents. Nanomaterials enhance the quality and resolution of medical imaging, enabling more accurate tumor detection and monitoring. High-quality images facilitate better drug targeting and efficacy in nanomedicine formulations, ultimately improving treatment precision and outcomes.88
Design of Delivery Systems
Skin cancer, unlike many other malignant tumors, is typically localized and superficial tumor, making it amenable to localized treatment approaches such as phototherapy. However, effective phototherapy requires efficient transdermal drug delivery, which can be challenging. The fundamental properties of NPs—such as particle size, shape, and surface charge—are crucial in addressing these challenges by enhancing drug penetration through the skin.
A delivery system with controlled drug release ensures that drug levels remain within the therapeutic window, maximizing efficacy while minimizing side effects. Stimulus-responsive systems are often a key feature of controlled release strategies, where external physical stimuli trigger drug release. Phototherapy inherently functions as a natural stimulus-responsive system, with light acting as the external trigger for precise and localized drug release.
Phototherapy inherently includes as a natural stimulus-responsive system, where light acts as the physical trigger. Nanomedicine drug delivery systems (NDDS) are a type of nanomaterial that enhances drug stability and solubility, extends circulation time, increases uptake by target cells or tissues, and reduces enzymatic degradation, thereby improving drug safety and efficacy. NDDS can achieve controlled drug release by responding to specific stimuli, such as light, temperature, pH, ultrasound, electric potential, and magnetic fields.89
In phototherapy, nanoparticles (NPs) enable the selective release of photosensitizers (PSs) at targeted sites through light activation. Additionally, light can serve as the excitation stimulus for phototherapy, prompting NPs to release PTAs upon stimulation, thereby exerting immediate phototherapeutic effects. The integration of controlled drug delivery systems (DDS) enhances the local concentration of PTAs, minimizing waste and reducing the risk of toxic side effects from PTAs affecting normal tissues. This targeted release improves the overall efficiency of phototherapy.
While controlled drug release aids in achieving tumor selectivity for PTAs, it is not sufficient on its own to guarantee perfect targeting.Thus, enhancing the targeted delivery of PTAs becomes particularly important. Targeted therapy helps improve the bioavailability of drugs. Properly designed drugs can selectively bind to active sites and potentially mediate therapeutic effects.90 Two primary strategies are used to achieve targeted drug delivery in tumors. The first involves modifying NPs with targeting ligands such as antibodies or peptides to direct them toward tumor cells. The second strategy uses biomembrane coatings on NPs to facilitate targeted drug delivery, further enhancing treatment specificity and efficacy. The light properties of phototherapy offer an additional targeting mechanism for nanoparticles (NPs)—light-induced targeting. This capability leverages the light-activated functions of NPs. Research has shown that the light energy required for this targeting can be derived not only from external sources but also from internal bioluminescence.91 This discovery not only provides new ideas for phototargeted therapy but also has the potential to overcome the limitations of poor light penetration, further enhancing the efficacy of phototherapy.
Delivery of Light-Triggered Nanomaterials
In the treatment of skin cancer, light-triggered nanoparticles (NPs) can be delivered through two primary approaches: one using NP carriers and the other utilizing microneedles. Both methods facilitate the delivery of anticancer agents, with the activated nanoparticles playing a key role in targeting and treating cancer cells. Typically, delivered substances can be categorized into three types: drugs, genes, and NPs.
PTAs are essential substances in phototherapy. However, in most cases, PTAs are hydrophobic, and NPs serve as excellent carriers for delivering these agents. Coupling or encapsulating PTAs into NPs holds promise for addressing this issue.92 By modifying NPs to improve the water solubility of poorly soluble PTAs, a broader range of therapeutic compounds can be effectively delivered, expanding the potential for targeted treatments.93 Moreover, modified NP carriers can achieve targeted drug delivery and controlled release, maximizing the effectiveness of phototherapy.Compared to NP carriers, which enhance the lipophilicity-hydrophilicity balance of PTAs, microneedles offer a more direct approach, bypassing the need for systemic circulation and allowing for precise, localized delivery of therapeutic compounds. Microneedles can directly deliver drugs by puncturing the skin and bypassing the SC, thus improving the delivery efficiency of PTAs. Microneedles have been demonstrated to be a safe and user-friendly method for drug administration, offering an alternative to traditional subcutaneous injections. They also hold promise as a potential method for controlled release of therapeutic agents, improving patient compliance and treatment efficacy.94
The ultimate goal of various experimental cancer treatment methods is the targeted regulation of gene expression involved in cancer-related pathways, aiming to precisely control tumor growth and progression while minimizing off-target effects. For gene therapy, establishing a safe and effective gene delivery system is crucial. To achieve this goal, researchers have developed various types of gene carriers, which can be primarily classified into viral and non-viral vectors.95 Although viruses have the ability to carry exogenous genes and facilitate transfer to host cells,96 their inherent toxicity and the immune responses they provoke limit their application. NPs and microneedle-based gene delivery carriers not only circumvent the toxic effects associated with viral vectors but also offer the potential for direct gene deposition into the dermis to combat skin diseases. This localized delivery approach enhances the effectiveness of gene therapy, particularly in the treatment of skin cancer, by improving precision and reducing systemic side effects.97
In recent years, special nanoparticles (NPs), such as inorganic NPs, have gained increasing recognition due to their dual functionality. They can act not only as drug carriers but also as therapeutic agents themselves, offering a multifunctional approach to treatment that enhances both delivery efficiency and therapeutic outcomes.When employed as transport carriers, these nanoparticles (NPs) can deliver various therapeutic agents to tumor sites via active or passive targeting mechanisms. Conversely, when used as therapeutic molecules, they themselves become the therapeutic agents, directly targeting and treating tumor cells, thus offering a versatile approach in cancer therapy. Combining intrinsic therapeutic properties, drug delivery capabilities, and photothermal or photosensitive characteristics, these NPs can provide skin cancer with unique synergistic therapeutic effects.98 Delivery of NPs through nanocarriers or microneedles is also commonly used in combination therapies involving phototherapy and chemotherapy.99 In this way, NPs serving as PTAs and chemotherapy drugs enter the body simultaneously to exert their effects. While chemotherapeutic drugs can circulate throughout the body, their associated toxicity cannot be overlooked. In contrast, phototherapy offers high efficiency with minimal side effects, making it a promising alternative. Additionally, the synergistic anticancer effect of the combination of the two can significantly improve the therapeutic effect.100
Photodynamic Therapy
PDT is a technology that utilizes photodynamic effects for disease diagnosis and treatment.It is based on the local or systemic application of photosensitizing compounds, known as PSs. As a modern non-invasive therapy, photodynamic therapy (PDT) can be employed to treat not only various types and locations of cancer but also non-tumorous diseases. Its versatility and targeted approach make it a valuable tool in both oncology and dermatology.101 PDT induces cellular damage by using light of an appropriate wavelength to activate the PS. The main component is the effect of photochemical reactions on biological tissues. The initiator of these processes is light energy.38 Compared to traditional therapies, PDT has advantages such as being relatively non-invasive, having strong targeting capabilities, fewer side effects, low incidence of drug resistance, and being easy to combine with other treatments.
Principle of Photodynamic Therapy
The basis of action of PDT is the photodynamic effect, a photosensitization reaction accompanied by biological effects involving oxygen molecules.101 This destruction process is mediated by singlet oxygen (1O2) generated from the interaction between PS and oxygen under light exposure. 1O2 is considered to be the main toxic component that plays a role in PDT.
PDT can induce three main types of cell death: apoptosis, necrosis, and autophagy-related cell death.102 Due to the short half-life of 1O2 (<40 ns) and its limited diffusion distance (<20 nm),103 phototoxic responses primarily occur within the area where the PS is distributed. Therefore, the subcellular localization of the PS will fundamentally determine the extent of photodamage and influence the cellular pathways.100 In recent years, the rapid development of nanotechnology has brought significant opportunities for advancements in PDT. The use of NP-based PSs, composed of molecules with or without additional biological/photophysical functions, is a promising approach to improving PDT.104
Classification of PS
Through continuous research and development, PSs are generally classified into three generations. The comparison of three generations of PSs are summarized in Table 2. First-generation PS primarily consist of mixtures of natural porphyrins, such as hematoporphyrin and its derivatives (Photofrin I, HpD).105 Today, Photofrin II, a purified derivative of HpD, is the most commonly used PS and has been approved for clinical use. It is used in Canada for treating superficial bladder cancer and in the Netherlands and Japan for treating early-stage lung cancer and advanced esophageal cancer.106 However, as complex mixtures of several unidentified porphyrins, first-generation PS have poorly defined chemical compositions and are associated with limitations such as poor tissue penetration, lower selectivity, and higher photosensitivity, which restrict their clinical applications.107
 |
Table 2 Comparison of Three Generations of PSs |
To overcome these drawbacks, researchers have designed and developed second-generation PS. Second-generation PS are mainly categorized into three types: porphyrin-based compounds, phthalocyanine-based compounds, and conjugated quinone-based compounds.109,113 These PS have clearer chemical structures and accumulate less in skin tissues. These PS typically have strong absorption peaks at wavelengths >630 nm, allowing for deeper tissue penetration, increased production of singlet oxygen (1O2), and enhanced tumor cell killing capability, making them suitable for clinical PDT. However, their strong hydrophobicity and poor tumor selectivity hinder their widespread application.107
Third-generation PS are developed by combining PS with biologically active substances to enhance the targeting capability of PDT. With the advancement of nanotechnology, the combination of nanomaterials with PS is a hot research area. NP-based PS can enhance drug delivery of the PS either passively or actively.112 Encapsulating PS in nanocarriers modified with targeting ligands can achieve tumor specificity, increase PS accumulation at the tumor site, reduce unnecessary cytotoxicity, and improve therapeutic efficacy.
PDT Treatment Strategies
Targeting the Hypoxic Environment of Tumors
TME is the internal environment in which tumor cells grow and thrive. Interactions between tumor cells and their TME play a crucial role in influencing tumor cell survival, migration, and invasion.114 The rapid proliferation of tumor cells and increased oxygen consumption within the tumor lead to hypoxia in the TME. Hypoxia simultaneously promotes tumor invasion, metastasis, angiogenesis, and the production of MDR proteins.115 Therefore, tumor hypoxia can be considered one of the entry points for tumor therapy. Currently, PDT has proposed various treatment strategies for melanoma targeting the hypoxic TME.
During treatment, a hypoxic environment can cause quenching effects in the PS, reducing the generation of cytotoxic ROS. At the same time, the oxygen consumption and microvascular damage caused by PDT can exacerbate tumor hypoxia, thereby hindering treatment efficacy.116
To address this, two strategies can be considered: ablating the tumor hypoxic environment or inhibiting the tumor’s antioxidant response.To ablate the tumor hypoxic environment and improve PDT efficacy, many strategies have been employed to alleviate hypoxia at the tumor site, including delivering oxygen to hypoxic tumors and generating oxygen within hypoxic tumors.42 For example, Liu et al117 developed an oxygen self-supplying and pH-sensitive therapeutic NP by fluorinating the PS, utilizing the hypoxic and acidic microenvironment of solid tumors. This NP not only achieved oxygen self-supply in experiments to enhance PDT efficacy but also utilized pH-dependence to increase phototoxicity and reduce PS accumulation, thereby improving the safety of the treatment. Clostridium butyricum is an anaerobic bacterium. Shi et al118 prepared d-Ala-TPApy by clicking the bacterial metabolic substrate D-alanine with aggregation-induced emission PS (TPApy) through chemical coupling. It was incubated with the oncolytic bacterium (Clostridium butyricum) to produce engineered oncolytic bacteria, which were then validated using a mouse model of malignant melanoma (Figure 2A). Under dark conditions, d-Ala-TPApy-Clos exhibited significant tumor suppression with an inhibition rate of 75.6±2%. When 3D spheroid models of cancer cells were incubated with d-Ala-TPApy-Clos under light, the tumor spheroids were almost completely suppressed, with a tumor suppression rate of 91.7±3%. This result indicates that Clostridium butyricum can penetrate the core regions of tumor spheroids and disrupt the hypoxic areas, while the PS (TPApy) can further induce apoptosis in the peripheral regions under light exposure.
 |
Figure 2 (A) Schematic illustration for the construction of dye-labeled oncolytic bacteria and melanoma eradicating mechanism by engineering bacteria under light irradiation. (a) Synthesis and preparation of metabolic labeling substrate d-Ala-TPApy. (b) Schematic illustration of d-Ala-TPApy-labeled Clostridium butyricum for malignant melanoma ablation under light irradiation. Reprinted from Shi L, Liu X, Li Y, et al. Living bacteria-based immuno-photodynamic therapy: metabolic labeling of Clostridium butyricum for eradicating malignant melanoma. Adv Sci. 2022;9:e2105807. Creative Commons.118 (B) Microscopy images after Au@MTM-HA treatment reflect the ability to generate ROS. Scale bar is 60 μm. Reprinted from Pharmacol Res. volume 158, Zhou J, Geng S, Ye W, et al. ROS-boosted photodynamic therapy against metastatic melanoma by inhibiting the activity of antioxidase and oxygen-producing nano-dopants. 104885. Copyright © 2020 Elsevier.119 (C) CLSM images of B16 cells after treatment with Ce6, PPC, and PPC@HA. Scale bar is 100 μm. (D) Ex vivo fluorescence imaging of different organs after intravenous administration. (E) Progression of mouse volume after treatment with different therapeutic agents. Reprinted from Acta Biomater. Volume 147, Huang X, Mu N, Ding Y, et al. Targeted delivery and enhanced uptake of chemo-photodynamic nanomedicine for melanoma treatment. 356–365. Copyright © 2022 Elsevier.68 (F) Inverted fluorescence microscopy images after treatment with UCNPs@G4-OH and UCNPs@G4-CTPP. Scale bar is 20 μm. (G) Schematic diagram of the synthesis of UCNPs@G4/Ce6/CAT-CTPP NPs.First, UCNPs-OA were fabricated via a high temperature pyrolysis method. G4-OH dendrimer was prepared with propargylamine as the core by repeating Michael addition reaction and amination reaction four times. Then, UCNPs@G4-OH nanoparticles were synthesized by thiol-ene and azide-acetylene two-step click grafting reactions. Next, the mitochondria-targeted molecules CTPP were covalently conjugated to UCNPs@G4-OH by the esterification reaction, achieving a multifunctional UCNPs@G4-CTPP nanoplatform. Reprinted from Biomaterials. Volume 140, Liang S, Sun C, Yang P, et al. Core-shell structured upconversion nanocrystal-dendrimer composite as a carrier for mitochondria targeting and catalase enhanced anti-cancer photodynamic therapy. 119850. Copyright © 2020 Elsevier.80 |
The hypoxic environment of tumors can limit the effectiveness of PDT. Additionally, the application of PDT in malignant melanomas is not widely promoted, partly due to the antioxidant effects of melanin, which can reduce the efficacy of PDT.120 In melanoma, antioxidant effects are present not only in the tumor tissue but also within the tumor cells. The former is due to the resistance of melanin, while the latter is caused by the tumor cells’ inherent antioxidant stress defense enzyme system.121 Therefore, targeting the inhibition of tumor cells’ antioxidant stress defense enzyme systems is another strategy to enhance PDT efficacy. Zhou et al119 developed a mesoporous TiO2 doped with MnO2 through an improved sol-gel method to create a co-doped PS, incorporating the antioxidant scavenger Au25SV9. The co-doped PS continuously generates sufficient O2, improving the source of oxygen in the tumor’s hypoxic environment. Microscopic imaging and real-time monitoring results showed that the targeted Au@MTM-HA had the strongest ROS generation capability (Figure 2B). The activity of thioredoxin reductase extracted from B16-F10 cells was measured. The results indicated that the released Au25SV9 significantly inhibited TrxR activity in a dose-dependent manner. Additionally, an increase in intracellular ROS was detected after TrxR inhibition. This demonstrates that inhibiting the intracellular antioxidant stress system can reverse the antioxidant effects in melanoma treatment, enhancing the PDT effect.
Enhancing Targeted Delivery
The reaction between PS and oxygen generates ROS, and the efficacy of PDT is closely related to the local concentration of ROS. However, the ROS generated by PDT can only migrate a very short distance (<20 nm), so the effect of PDT is limited to the immediate vicinity of the PS.122 Therefore, designing PSs with targeting capabilities can improve the efficacy of PDT. Currently, the targeting effects of DDS are mainly focused on targeting tumor cells themselves and specific organelles.
To better target tumor tissues, the surfaces of nanocarriers are often modified with targeting ligands.123 Modification with targeting ligands can enhance the delivery efficiency of nanocarriers. However, to increase the drug’s circulation time in the bloodstream, nanocarriers are typically surface-modified with negative charges, which can inhibit intracellular uptake by tumor cells. Considering that insufficient intracellular uptake by tumor cells can reduce the intracellular drug concentration, Huang et al68 developed a new type of amphiphilic charge-reversal nanomedicine, Pt(IV)-PEI-Ce6. They conjugated the prodrug (Pt derivative) and PS (Chl e6) with PEI, and then assembled it into positively charged NPs (PPC) in aqueous solution. These were further coated with HA through electronic interactions to form negatively charged PPC@HA. Compared to free Ce6, both PPC and PPC@HA enhanced the cellular uptake efficiency in B16 cells (Figure 2C). The presence of HA provides negative charges, which, to some extent, reduces cellular uptake. Thanks to HA-mediated targeted delivery and charge reversal mediated by HA degradation, PPC@HA showed improved biodistribution in tumor tissues and significantly inhibited melanoma growth. The biodistribution of PPC@HA was also superior by comparing IVIS imaging of heart, liver, spleen, lung, kidney and tumor tissues in mice receiving PPC@HA and PPC after 6 hours of intravenous administration. Thanks to HA-mediated targeted delivery and HA degradation-mediated charge reversal, the chemo-photodynamic combination therapy of PPC@HA+laser showed the most effective anti-tumor efficacy with the lowest tumor growth rate(Figure 2D and E).
Cell organelles are also ideal targeting sites, and mitochondria, as crucial regulators of cellular life activities and closely involved in various metabolic processes, are a prominent research focus. Mitochondrial dysfunction is related to oxidative stress and apoptosis. In cancer cells, mitochondrial autophagy can promote or inhibit tumorigenesis by regulating energy and oxygen supply.124 When PS is endowed with mitochondrial targeting characteristics, it can accumulate in the mitochondria of tumor cells through its targeting properties. For example, Liang et al80 designed a drug delivery system based on upconversion nanoparticles (UCNPs). They linked UCNPs to the surface of dendritic polymers and modified them with the mitochondrial-targeting molecule CTPP. Additionally, “hydrophobic and hydrophilic pockets” were constructed around the UCNPs, with hydrophobic PS (Ce6) and hydrophilic peroxidase (CTA) loaded into them (Figure 2G). After staining the cells with mitochondrial fluorescent dyes, it was observed that CTPP-modified NPs exhibited superior targeting and accumulation in the mitochondrial matrix compared to non-modified samples (Figure 2F). Study results both inside and outside the cells indicate that intracellular ROS can cause cell necrosis by damaging mitochondria and DNA.
Mitochondria are one of the organelles most susceptible to ROS damage.103 The large amounts of ROS generated during PDT lead to mitochondrial dysfunction in cancer cells, which in turn causes cellular damage. This method, which utilizes photodynamic effects to produce phototoxicity, causes oxidative damage, and blocks mitochondrial function to combat cancer, is known as mitochondrial-targeted PDT.125 Yang et al69 labeled mesoporous Au@Pt NPs with cell-targeting ligands (folic acid), mitochondrial-targeting groups (triphenylphosphine), and PS (Ce6). Successfully modified PSs endowed with mitochondrial-targeting characteristics can specifically localize to the mitochondria of tumor cells. Under the influence of abundant ROS, mitochondrial apoptosis pathways are activated, significantly enhancing the efficacy of PDT. Additionally, PDT has shown some resistance in the treatment of melanoma, significantly impacting its efficacy. Targeting mitochondria offers another potential solution. Wang et al designed a series of dinuclear ruthenium complexes in the 800–900 nm range and prepared an amphiphilic complex Ru3 with tert-butyl groups. This complex can target mitochondria without penetrating the cell nucleus, increasing its photodynamic activity and reducing its dark toxicity. It successfully inhibited melanoma tumor growth both in vitro and in vivo, avoiding the known PDT resistance in melanoma.70
Selective Cytotoxicity
The efficacy of PDT depends on the catalytic effect of light, and the toxicity of materials with photocatalytic potential can vary under light and dark conditions.126 Under dark conditions, there is a risk of “collateral damage” to normal cells, potentially causing side effects. The cell-killing effects produced under light and dark conditions are referred to as phototoxicity and dark toxicity, respectively. Selecting the appropriate PS or modifying it with nanomaterials can significantly influence its cell toxicity effects. Enhancing phototoxicity while minimizing dark toxicity is a key strategy for improving PDT efficacy and reducing adverse effects.
PS is one of the essential components of PDT; however, inherent dark toxicity in some PSs significantly limits their clinical application, which is one of the current challenges faced by PSs. In recent years, the development of metal-based PSs has garnered continued attention due to their high ROS production rates.127,128 Li et al129 developed a series of Ru(II) metallacycles (Ru1–Ru4) with low dark toxicity and high phototoxicity index based on the ruthenium receptor π-extension strategy. In in vitro anticancer activity assessments, except for Ru2, the metallacycles exhibited no activity against tumor cells under dark conditions, with Ru4 showing the lowest cytotoxicity (IC50 = 305.6 μM). Under light exposure, Ru1–Ru4 exhibited good anticancer activity against cisplatin-resistant tumor cells, maintaining high phototoxicity even under hypoxic conditions. Moreover, Ru4 has a phototoxicity index as high as 146 and exhibits good selectivity towards tumor cells. Additionally, in vivo anticancer experiments revealed that tumors treated with the Ru4 + laser group significantly extended the survival time of mice (Figure 3C) and showed no significant dark toxicity (organ damage) (Figure 3E). This indicates that designing PSs with reduced dark toxicity can enhance PDT efficiency and alleviate side effects.
 |
Figure 3 (A and B) Intracellular distribution of free or cubically encapsulated Ce6 or TPP-Mn. Reprinted from J Colloid Interface Sci. Volume 522. Bazylińska U, Kulbacka J, Schmidt J, Talmon Y, Murgia S. Polymer-free cubosomes for simultaneous bioimaging and photodynamic action of photosensitizers in melanoma skin cancer cells. 163–173. Copyright © 2018 Elsevier.130 (C) Survival time of tumor-bearing mice after different treatments. Reprinted from Li C, Tu L, Yang J, et al. Acceptor engineering of metallacycles with high phototoxicity indices for safe and effective photodynamic therapy. Chem Sci. 2023;14:2901–2909. Creative Commons.129 (D) Degradation curves of TKdC conjugates in different formulations over time under light stimulation. Reprinted from J Control Release. Volume 328. Huang L, Chen X, Bian Q, et al. Photosensitizer-stabilized self-assembling nanoparticles potentiate chemo/photodynamic efficacy of patient-derived melanoma. Copyright © 2020 Elsevier.66 (E) Histological examination of major organs in mice after Ru4 (10 μM) + laser treatment.Scale bar is 50 μm. Reprinted from Li C, Tu L, Yang J, et al. Acceptor engineering of metallacycles with high phototoxicity indices for safe and effective photodynamic therapy. Chem Sci. 2023;14:2901–2909. Creative Commons.129 (F) Tumor sections taken at 9 days after photo-ablation were immunostained against CD4 or CD8 (brown). Scale bar is 100 μm. Reprinted from J Control Release. Volume 322. Zhu Y, Xue J, Chen W, et al. Albumin-biomineralized nanoparticles to synergize phototherapy and immunotherapy against melanoma. 300–311. Copyright © 2020 Elsevier.75 (H) H&E staining of tumor sections after treatment. Scale bar is 100 μm. (I) TUNEL staining of tumor sections after treatment. Scale bar is 100 μm. Reprinted from J Control Release. Volume 328. Huang L, Chen X, Bian Q, et al. Photosensitizer-stabilized self-assembling nanoparticles potentiate chemo/photodynamic efficacy of patient-derived melanoma. Copyright © 2020 Elsevier.66 |
In addition to designing different structures of PSs to influence phototoxicity and dark toxicity, the application of NP has also introduced new possibilities for advancing PDT. There is a type of NP known as a cubic NP, which typically forms a reverse cubic double-continuous liquid crystal structure in water through self-assembly of certain lipids. Extensive research has demonstrated that these cubic NPs can be used in biomedical applications.131 Bazylińska et al130 designed a novel non-polymeric cubic double-continuous liquid crystal dispersion (cubic NP) as a carrier for PSs (Ce6 and TPP-Mn) for PDT and bioimaging of skin melanoma. Stability was achieved by incorporating phospholipids and propylene glycol. Using confocal laser scanning microscopy imaging, bioimaging studies showed that the cubic NPs can increase the cellular uptake rate. Although the absorption efficiency varied among different cell types, the PSs encapsulated within the cubic NPs showed enhanced cellular internalization and consequently stronger fluorescence signals (Figure 3A and B). In photodynamic activity assays, the cubic NP formulations demonstrated superior photodynamic properties, showing very low toxicity in the dark and causing a significant reduction in cell viability (about 90%) after irradiation. Compared to free PS, the cubic NPs provided the same photodynamic performance as a free PS at concentrations an order of magnitude higher. Therefore, this formulation can be considered to enhance the biocompatibility of target cells while boosting the PDT effect of light activation, ie, increasing phototoxicity.
Combination Therapies with PDT
Compared to traditional cancer treatment methods, PDT offers several advantages, including fewer side effects, strong targeting capabilities, low resistance rates, and relative non-invasiveness. However, traditional PDT, as a single treatment modality, is often limited by the choice of PS and may be ineffective in preventing potential tumor recurrence after treatment. Therefore, the combination of PDT with other treatment methods holds broad application prospects.
Immunotherapy achieves long-term tumor control by alleviating immune regulatory suppression or stimulating the host immune system.132 Traditional phototherapy has been found to trigger immunogenic cell death to activate anti-tumor immune responses.133 The strategy of combining phototherapy with immunotherapy is called photodynamic immunotherapy (PIT). PIT can overcome challenges such as tumor heterogeneity, tumor mutations, tumor immune editing, and escape, effectively improving anti-tumor efficacy.134
PDT induces tumor cell death through ROS, but the side effects of traditional PDT should not be underestimated. For example, the previously mentioned cytotoxicity, whether from the presence of dark toxicity or potential prolonged phototoxicity, can have adverse effects on the body. Additionally, the high recurrence rate of cancer makes the effects of phototherapy less satisfactory. PDT may enhance the immunogenicity of dead tumor cells by exposing or generating new antigens and by inducing heat shock proteins, thereby improving the efficiency of antigen cross-presentation. This provides a possibility for combining PDT with immunotherapy.135 Zhu et al75 integrated aluminum ions and PS (Ce6) into bovine serum albumin through the mineralization effect of albumin to create a novel nanoplatform (Al-BSA-Ce6 NPs). Aluminum hydroxide was used as an adjuvant to induce a sufficient immune response after PDT. The researchers hoped that by triggering a strong enough immune response, they could achieve the goal of preventing tumor recurrence or metastasis. The experiments were conducted on mice carrying B16F10 tumors with a volume of about 150 mm3. Different preparations were injected intravenously at a dose of 5 mg/kg on day 0 and irradiated for 5 minutes at a light intensity of 660 nm. Some of these mice were also injected subcutaneously with CpG around the tumors on day −1 and then again on days 1, 3 and 5. Surface markers on immune cells were stained 9 days after irradiation (Figure 3F). Flow cytometry analysis showed that Al-BSA-Ce6 NPs can induce dendritic cell maturation, with the triggered dendritic cells exhibiting higher maturity. This leads to a higher level of infiltration of CD8 and CD4 T cells into tumors and lymph nodes (Figure 3G), which can kill tumor cells. This result indicates that the novel nanocarrier system based on PIT successfully induced an effective antitumor immune response in vivo, validating the effectiveness of PIT in achieving long-term treatment after PDT.
In addition to PIT, PDT can also be combined with chemotherapy. Chemotherapy is considered one of the most common cancer treatments, but it often comes with severe toxicity issues and may lead to drug resistance. However, single PDT often fails to achieve the desired therapeutic effect.136,137 The combination of PDT and chemotherapy holds promise for improving the situation. However, chemophotodynamic therapy often involves the development of complex DDS, which increases operational difficulty and limits the clinical translation of chemophotodynamic therapy.138 Huang et al66 constructed a nanoconjugate (termed psTKdC NA) that connects the anticancer drug cabazitaxel through a ROS-activatable disulfide bond, resulting in a dimer TKdC prodrug. Ce6 generates ROS under light stimulation, which not only exerts PDT effects but also cleaves the disulfide bond to release CTX for chemotherapeutic action (Figure 3D). To evaluate the antitumor efficacy of an aggressive PDX model of human melanoma, the investigators established an aggressive in situ melanoma model of patient-derived xenografts by subcutaneously implanting tumor tissue from surgically resected inguinal lymph nodes of patients into immunocompromised Balb/c nude mice. The drug formulation was injected intravenously through the tail vein, and 12 hours after the injection, the tumor area was exposed to near-infrared light (660 nm) irradiation for 10 minutes at a laser power of 600 mW/cm2. At the end of the treatment, tumor sections were stained with hematoxylin-eosin (H&E) for histological analysis, and the results showed that the synergistic treatment of psTKdC NAs and laser irradiation was effective in inducing apoptosis and necrosis of intratumor cells.(Figure 3H). Additionally, terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling immunohistochemical staining confirmed the excellent combination of chemotherapy and photodynamic activity (Figure 3I).
In summary, PDT treatment, with its requirement for oxygen, can specifically target and ablate the hypoxic microenvironment of tumors or inhibit the antioxidant response of tumors. Enhancing the targeted delivery of PS can increase the ROS concentration at the treatment site, thereby improving the tumor cell-killing effect. As a form of phototherapy, PDT relies on light-catalyzed cellular phototoxicity. The design of light-triggered nanocarriers offers new opportunities to enhance phototoxicity and reduce dark toxicity. Additionally, combining PDT with chemotherapy and immunotherapy can achieve a synergistic effect, leveraging the strengths of each approach. Compared to traditional treatments, PDT has the advantage of being relatively non-invasive, as it generates ROS through light activation. Reasonably designing the structure of light-triggered NPs and constructing an effective delivery system can achieve targeted, safe, and combined therapeutic goals. However, although PDT is approved for clinical use, traditional therapies still dominate the treatment of skin cancer. A significant reason for this is the toxicity issues associated with PSs and the difficulties in constructing effective delivery systems. The existence of these issues significantly limits the further clinical translation of PDT. Despite this, the advantages of PDT are undeniable, and it has a broad application prospect. In the future, the development of novel PSs and the construction of light-triggered NP delivery systems may become new research directions.
Photothermal Therapy
PTT relies on selective photothermal effects to exert its therapeutic action, based on applying high temperatures locally to tissues to induce irreversible cellular damage at the target site.139 PDT relies on PS, which requires a high ROS yield, while PTT relies on materials known as PTA. Ideal PTAs should exhibit high photothermal conversion efficiency. Compared to traditional treatments like chemotherapy, radiotherapy, and surgery, PTT offers advantages such as enhanced specificity, strong tissue penetration, and ease of combination with other therapies. In the treatment of skin cancer, PTT not only targets tumors effectively but may also promote wound healing and reduce the risk of infection.
Principle of Photothermal Therapy
PTT is a promising non-invasive treatment method that involves locally irradiating the tumor with an external near-infrared laser. PTAs collect light energy through this laser and convert it into heat, releasing it in a spatially resolved manner.139 In recent years, PTT, especially NP-based PTT, has emerged as a very promising ablation therapy technique for malignant tumors.140 Currently, photothermal therapy (PTT) is a prominent research focus in cancer treatment and holds significant promise as a potential alternative to traditional therapies. While traditional PTT can cause necrosis and inflammation under light irradiation, which can hinder treatment, recent studies have demonstrated that PTT can be modulated to induce apoptosis instead. This advancement positions novel PTT as a promising approach for treating skin cancer.141
Classification of PTA
PTAs are materials with high photothermal conversion efficiency that can accumulate near tumor tissues through targeting recognition techniques and convert light energy into thermal energy under near-infrared light irradiation. In addition to killing cells through thermal energy, PTT can also exert synergistic effects when combined with other therapies to enhance treatment efficacy. Since the rise of PTT, PTA systems have undergone approximately four generations.
The first generation includes metal NPs, such as Au, Ag, and Pt, which have high photothermal conversion efficiency and imaging efficiency. However, they are expensive, relatively rare, and challenging to use in routine clinical applications.142 The second generation consists of carbon-based materials, which are more affordable compared to the first generation. Notable examples include graphene and carbon nanorods. Their advantage lies in having a larger photothermal conversion area, but they have poor absorption ability under near-infrared light.143 The third and fourth generations of PTAs are currently the focus of intense research. The third generation of PTAs consists of metal and non-metal compounds, with representative materials including CuS and ZnS. Compared to the first and second generations of PTAs, it is cost-effective and possesses high photothermal performance, but has poor targeting ability, making rapid tumor localization challenging. The fourth generation comprises organic dye materials, such as indocyanine green (ICG) and Prussian blue (PB). These materials have been extensively studied for their unique properties, including excellent biocompatibility, low toxicity, and high optical stability. ICG, in particular, has gained significant attention due to its strong near-infrared (NIR) absorption, enabling deep tissue penetration and effective photothermal conversion. Additionally, Prussian blue exhibits high photothermal efficiency and has been successfully employed in synergistic therapeutic approaches. For instance, Cui et al utilized tumor cell membrane biomimetic nanotechnology combined with PB’s anti-inflammatory and antioxidant properties to enhance its therapeutic efficacy. This approach was applied to improve outcomes in infectious wounds and radiation dermatitis, demonstrating PB’s potential in both oncological and non-oncological clinical applications. Preclinical studies have further validated the ability of these organic nanomaterials to achieve superior therapeutic outcomes while minimizing side effects, paving the way for broader clinical use.144–146
PTT Treatment Strategies
Targeted Therapy
Targeted therapy can increase the accumulation concentration of drugs within tumors. For PTT, the significance of targeted therapy lies in concentrating PTAs at the tumor site to induce a localized photothermal effect, causing cell damage while minimizing thermal damage to normal tissues.
Nanomaterials can leverage their inherent properties to exhibit targeting capabilities in response to specific physical stimuli, such as light, electricity, heat, pH, or magnetism. Pandesh et al71 synthesized Fe3O4@Au core-shell NPs, utilizing their magnetic targeting capability to accumulate in the tumor region. Fe3O4@Au core-shell NPs combined with a magnet and laser showed the greatest effect on the tumor, with an average inhibition rate of 83.5%. The average inhibition rates for the NPs group, laser group, and NPs + laser group were 6%, 26%, and 57%, respectively (Figure 4A). This result demonstrates that magnetic NPs can specifically accumulate at the tumor site under the influence of a magnet, validating the enhancement of PTT efficacy through targeting capabilities.
Biomimetic targeting strategies based on biological membrane coatings can endow NPs with certain targeting capabilities. In recent years, biomembrane-derived biomimetic nano-platforms have garnered increasing attention for promoting the application of nanomedicines in biomedical fields.147–149
 |
Figure 4 (A) Tumor inhibition rates in different treatment groups over 2 weeks. Reprinted from Pandesh S, Haghjooy Javanmard S, Shakeri-Zadeh A, Shokrani P. Targeted photothermal therapy of melanoma in C57BL/6 Mice using Fe(3)O(4)@Au core-shell nanoparticles and near-infrared laser. J Biomed Phys Eng. 2021;11:29–38. Creative Commons.71 (B) Schematic diagram of the Franz diffusion cell system with (+)T-SiDs. (C) Fluorescence images of skin sections from different treatment groups. Scale bar is 200 μm. (D and E) Temperature changes in tumors of tumor-bearing mice. (F) H&E and TUNEL staining images of tumor sections from different groups after treatment. Scale bar is 25 μm. Reprinted from Acta Biomater. Volume 130. Zhang Y, Li F, Ya S, et al. An iron oxide nanoparticle-based transdermal nanoplatform for dual-modal imaging-guided chemo-photothermal therapy of superficial tumors. 473–484. Copyright © 2021 Elsevier.76 |
In PTT for melanoma, the use of red blood cell membranes has gained considerable attention. These membranes are employed to enhance the delivery and targeting of photothermal agents, improve biocompatibility, and reduce immune recognition, thereby optimizing the therapeutic efficacy of PTT. Researchers have coated red blood cell membranes on melanin NPs, enhancing blood retention and tumor accumulation in vivo through the “enhanced permeability and retention” effect, reducing clearance by the reticuloendothelial system. This approach also leverages the NPs’ inherent photoacoustic imaging (PAI) properties and excellent photothermal conversion ability to enhance their antitumor PTT efficacy.150 To improve targeting capability, relying solely on red blood cell membranes is insufficient. Therefore, hybridization technology for biological membranes has been extensively utilized to enhance targeting precision and therapeutic effectiveness. Wang et al151 created a hybrid biomimetic membrane by fusing erythrocyte and melanoma cell membrane materials for use in the photothermal therapy of melanoma. Researchers utilized DOX-loaded hollow CuS nanoparticles, and in this study, the hybrid membrane served as a camouflage coating, forming DCuS@[RBC-B16] NPs. Under NIR irradiation, DCuS@[RBC-B16] NPs can reach 75.4°C within 10 minutes and maintain excellent photostability even after four irradiations. As nanoparticles with a biomembrane coating, they have a unique self-recognition ability for melanoma cells. Compared to A549 cells, DCuS@B16 NPs exhibit approximately 8.1 times higher average fluorescence intensity in B16-F10 cells. In in vitro anticancer performance tests under NIR irradiation, the death rate of B16-F10 cells treated with DCuS@[RBC-B16] exceeded 94.5%. In vivo experiments validated the homotypic targeting ability of these nanoparticles. After near-infrared irradiation, mice treated with DCuS@[RBC-B16] showed a tumor growth inhibition rate close to 100%. Even in the CuS@[RBC-B16] group without DOX, the tumor growth inhibition rate was as high as 86%.
Additionally, this NP platform demonstrated excellent in vivo PTT efficacy and antitumor effects. Melanin@RBC-M with a 1:1 weight ratio of red blood cell membrane to MCF-7 membrane proteins showed an increase in tumor temperature from 29.6°C to 54.0°C within 10 minutes (Figure 4D). Compared to the weak tumor suppression ability of bare melanin NPs, the 1:1 group of Melanin@RBC-M demonstrated complete tumor elimination (Figure 4E and F).
Similar to the targeting mechanism of PDT, PTT can also target organelles for precise therapy.
Considering that the effectiveness of PDT and PTT largely depends on the cellular uptake and intracellular localization of PS and PTA, Tang et al72 explored the combined effects of PDT and PTT. They designed a series of cyclometalated Ir(III) complexes with morpholine and piperazine groups as dual PSs and PTAs to combat melanoma.Further research revealed that several hydrophobic complexes precipitated upon local supersaturation. However, the amphiphilic complexes Ir3 and Ir6 did not precipitate and matched well with mitochondrial dyes. The most absorbed complex, Ir6, accounted for 95% of the total cellular uptake and was predominantly distributed in the mitochondria. This indicates the complex’s excellent mitochondrial targeting ability. Moreover, the high phototherapy index and significant photothermal response of Ir6 in melanoma cells further demonstrate the promoting effect of mitochondrial targeting on PTT.
Increasing Drug Delivery Efficiency
As a superficial tumor, transdermal drug delivery for skin cancer treatment is an attractive strategy, showing promising prospects.152,153 The choice of transdermal drug delivery carriers is a critical issue. The application of nanocarriers has addressed the need for targeted delivery and controlled release of drugs to some extent.154
Various nanocarriers have been studied for transdermal drug delivery, but their application has been limited by low stability or poor biocompatibility. Zhang et al76 designed a multifunctional nano-composite platform based on a superparamagnetic iron oxide core, named (+)T-SiDs. The positive charge on this platform enhances skin permeability and tumor cell uptake. Additionally, it includes the transdermal enhancement peptide TD and DiR. The researchers conducted an in vitro evaluation of transdermal performance (Figure 4B). The penetration efficiency of (+)T-SiDs was significantly higher than that of (+)SiDs (without TD), and the fluorescence intensity of the skin sections was also markedly stronger than the latter (Figure 4C), demonstrating higher transdermal permeability. The transdermal therapy using (+)T-SiDs also showed significant effectiveness in enhancing PTT. The investigators used intravenous (+)T-SiDs as the control group, while in the experimental group, PBS, (+)SiDs, (+)T-SiSis, and (+)T-SiDs were delivered by transdermal administration. After 24 hours of administration and 10 minutes of laser irradiation (1 W/cm2) at 808 nm, the results of infrared thermography showed that the temperatures of the tumor sites treated with (+)T-SiDs and (+)T-SiSis transdermally increased rapidly within the first 300s. However, the temperatures of the transdermally treated group increased gradually to 46°C, which was higher than that of the injected group at 43°C, and the temperatures of the injected group were higher than that of the injected group. (Figure 4D and E). Twenty-four hours after treatment, tumor sections stained for analysis showed varying degrees of cell lysis and disruption, leading to significant necrosis and apoptosis of tumor cells (Figure 4F). This demonstrates the advantage of increased transdermal efficiency in PTT.
Increased transdermal efficiency not only enhances the efficacy of PTT but can also produce a synergistic amplification effect in combination therapies involving PTT. Ho et al155 developed a nanographene oxide-hyaluronic acid conjugate (NGO-HA) for photothermal ablation therapy of MSC (Figure 5A). When the concentration of NGO-HA exceeds 250 μg/mL, NIR irradiation for 10 minutes can raise the temperature of the NGO-HA solution by approximately 40°C (Figure 5B), sufficient to induce a photothermal effect. Due to the transdermal properties of HA derivatives, NGO-HA can significantly penetrate the compromised cancerous skin barrier (Figure 5C). Additionally, HA receptors on the surface of cancer cells can further increase the transdermal efficiency of NGO-HA. Loading chemotherapeutic drugs into NGO-HA allows for the combination of transdermal chemotherapy and PTT. This demonstrates that applying nanocarriers capable of enhancing transdermal efficiency in PTT can not only improve the tumor-killing effect of PTT but also provides feasibility for combining PTT with other therapies.
 |
Figure 5 (A) Schematic diagram of NGO-HA treatment for melanoma. (B) Temperature increase curves of different concentrations of NGO-HA. (C) Confocal microscopic analysis of transdermal delivery of different drugs in tumor model mice. Scale bar is 200 μm. Arrows indicate the tumor regions. Reprinted with permission from Jung DJ, Kong WH, Sung DK, et al. Nanographene oxide-hyaluronic acid conjugate for photothermal ablation therapy of skin cancer. ACS Nano. 2014;8:260–268. Copyright © 2014 American Chemical Society. 155 (D) Schematic diagram of the synthesis of BMH hydrogels using a novel double-crosslinking process. (E) Antibacterial rate and duration of BMH hydrogels. Scale bar is 2mm. (F) Wound bed closure traces within 14 days of treatment. Reprinted from Biomaterials. Volume 260. Wang S, Zheng H, Zhou L, et al. Injectable redox and light responsive MnO(2) hybrid hydrogel for simultaneous melanoma therapy and multidrug-resistant bacteria-infected wound healing. 120314. Copyright © 2020 Elsevier.156 (G) Skin appearance images of PBVac+Light treatment and control groups. (H) Histological analysis of irradiated skin in different groups. Scale bar is 100 μm. (I) Comparison of tumor weight at the end of the study with initial weight in mice. Reprinted from Cui H, Zhang X, Zhang Z, et al. Killing three birds with one stone: tumor-membrane-decorated Prussian blue nanovaccines for synergistic management of skin tumors, radiation dermatitis and wounds. Composites Part B. 2023;264:110900. Creative Commons.79 ***P < 0.001. |
Reducing Surgical Complications
Despite the continuous development of various new treatment methods, surgical excision remains a common approach for treating skin cancer. However, wound healing and skin regeneration following traditional skin tumor surgery and chronic bacterial infection-induced wounds remain a challenge.157 The formation of chronic wounds is closely related to the presence of pathogenic bacteria in the postoperative skin defect.158 Timely application of antibiotics can reduce bacterial infection; however, the emergence of multidrug-resistant (MDR) bacteria increases the risk of chronic wounds.159 Wang et al156 developed a novel double-crosslinked BMH hydrogel (Figure 5D), which is injectable, adhesive, redox/photo-responsive, and has inherent antibacterial properties. Upon application to MDR bacteria-infected wounds, the BMH hydrogel showed significant antibacterial capability (92.6%) from the outset, compared to the control group. Furthermore, its antibacterial effect lasted longer, demonstrating a 100% antibacterial rate 14 days post-treatment (Figure 5E). In the absence of antibiotics in vivo, the experimental group effectively eradicated MDR bacterial infections. The BMH hydrogel also performed outstandingly in wound healing experiments, resulting in 75.4% wound closure by day 7, significantly higher than other groups. Additionally, the wound defects in the BMH hydrogel group almost disappeared by day 14 (Figure 5F). This study demonstrated the importance of inhibiting MDR bacterial infections for postoperative wound healing.
In patients with malignant skin tumors, especially advanced melanoma, postoperative wound healing can be affected not only by infections but also by residual infiltrating cancer cells and secondary issues from subsequent treatments, such as radiation dermatitis, which can slow down wound recovery.160 This series of issues significantly impacts patients’ survival rates and quality of life. Although solutions exist for these issues, when these challenges occur simultaneously, they can increase the complexity of synthesis steps and costs, leading to more complex in vivo behaviors and effects, and presenting greater regulatory challenges.161
Cui et al79 developed a novel tumor cell membrane-modified PB nanozyme vaccine, PBVac, as a multifunctional nanoparticle platform for postoperative wound management and skin tumor eradication. PBVac utilizes the ROS-scavenging and anti-inflammatory capabilities of PB nanozymes to promote wound healing. Within 60 minutes, PBVac effectively scavenged superoxide radicals in a dose-dependent manner. It also significantly reduced TNF-α and IL-1β levels while upregulating the anti-inflammatory gene Arg-1. Additionally, PBVac was evaluated for its efficacy against radiation dermatitis. After PBVac + Light treatment, compared to the control group, the appearance of radiation dermatitis and scarring was alleviated, and hair growth was restored (Figure 5G). Histological analysis revealed better epithelial continuity in the PBVac + Light group (Figure 5H) and increased skin appendages, including hair follicles and blood vessels, along with enhanced collagen accumulation by day 28. In terms of antitumor activity, PBVac showed a minimal 1.5-fold increase in tumor volume compared to a 40-fold increase in the PBS and PB nanozyme groups (Figure 5I). Post-PTT, most cancer cells exhibited shrinkage and necrosis (Figure 6A). These results demonstrate PBVac’s potential in preventing cancer recurrence, managing radiation dermatitis, and aiding wound healing, emphasizing the benefits of a multifunctional nanoparticle platform.
 |
Figure 6 (A) Histological analysis of tumors at the end of the study. Scale bar is 100 μm. Reprinted from Cui H, Zhang X, Zhang Z, et al. Killing three birds with one stone: tumor-membrane-decorated Prussian blue nanovaccines for synergistic management of skin tumors, radiation dermatitis and wounds. Composites Part B. 2023;264:110900. Creative Commons.79 (B) Flowchart of the composition process for HPCT and HPCI. Reprinted from Cancer Lett. Volume 423. Tang J, Zhou H, Hou X, et al. Enhanced anti-tumor efficacy of temozolomide-loaded carboxylated poly(amido-amine) combined with photothermal/photodynamic therapy for melanoma treatment. 16–26. Copyright © 2018 Elsevier.67 (C) Fluorescence images of tumor cells with or without free CD47 treatment using nGO-COS-CD47z. Scale bar is 40 μm. (D) Comparison of tumor cell viability after treatment with free DTIC and nGO-COS-CD47/DTIC. Reprinted from Mater Sci Eng C Mater Biol Appl. Volume 123. Zhan X, Teng W, Sun K, et al. CD47-mediated DTIC-loaded chitosan oligosaccharide-grafted nGO for synergistic chemo-photothermal therapy against malignant melanoma. 112014. Copyright © 2021 Elsevier.162 (E) Schematic diagram of temperature increase at different concentrations of HPCI. (F) Comparison of temperature increase in solutions of ICG and HPCI. (G) Comparison of singlet oxygen generation between ICG and HPC. Reprinted from Cancer Lett. Volume 423. Tang J, Zhou H, Hou X, et al. Enhanced anti-tumor efficacy of temozolomide-loaded carboxylated poly(amido-amine) combined with photothermal/photodynamic therapy for melanoma treatment. 16–26. Copyright © 2018 Elsevier.67 (H) Photothermal heating curves of solutions under different treatment conditions. Reprinted from Mater Sci Eng C Mater Biol Appl. Volume 123. Zhan X, Teng W, Sun K, et al. CD47-mediated DTIC-loaded chitosan oligosaccharide-grafted nGO for synergistic chemo-photothermal therapy against malignant melanoma. 112014. Copyright © 2021 Elsevier.162 |
Combination Therapy
As previously mentioned, under the influence of nanomaterials, PTT has been endowed with targeted therapeutic capabilities, which can reduce the systemic cytotoxicity of drugs and also play a role in promoting skin wound healing. However, the sole application of PTT inevitably comes with drawbacks such as incomplete treatment and short duration of effect. The development of multifunctional NP platforms and multimodal therapies represents a future trend in the treatment of malignant tumors, offering the potential to overcome the limitations of traditional single-mode therapies and enhance anticancer efficacy.163 With their multifunctionality and optical properties, nanomaterials can enable the combination of PTT with other therapies, achieving synergistic effects.164
Immunotherapy is a viable treatment option for skin cancer, with a major milestone being the development of immune checkpoint inhibitors.165,166 However, the sole use of immunotherapy still faces the issue of low response rates. Combining PTT with immunotherapy can effectively inhibit tumor growth, extend the short-term effects of PTT, and prevent tumor recurrence.167 Zhou et al168 designed bovine serum albumin-biomimetic gold nanorods loaded with the immunoadjuvant R837 to achieve the combined application of PTT and immunotherapy. Under laser irradiation, the B16-F10 tumors treated with mPEG-GNRs@BSA/R837 showed higher TNF-α release levels compared to the non-irradiated and control groups, along with increased levels of IL-6 and IL-12. This indicates that the nanocomposite can trigger a strong immune response in vivo with the help of the immunoadjuvant. Compared to other treatment methods, mPEG-GNRs@BSA/R837-PTT has a significant advantage in inhibiting tumor growth. The PPT component based on GNRs killed some tumor cells through the photothermal effect, which represents the direct cytotoxic effect of PTT on the tumor. More importantly, the killed tumor cells can act as antigens to trigger tumor-associated immune responses, activating T cells. This immune response further enhances the antitumor effect and induces long-term immune memory against tumor recurrence. Therefore, the combination of PTT and immunotherapy not only enhances the antitumor effect but also achieves long-term prevention of recurrence. This approach holds significant potential for treating skin cancer in clinical settings.
Chemotherapy resistance is a major challenge currently faced in chemotherapy, particularly in malignant melanoma, where high metastasis rates and high chemotherapy drug resistance lead to unsatisfactory treatment outcomes.169 Additionally, the inherent properties of some chemotherapeutic drugs often limit their clinical application. For instance, dacarbazine, a first-line chemotherapeutic drug for malignant melanoma, is limited by issues such as poor solubility and toxic side effects.170 Nanomaterial-mediated PTT combined with chemotherapy holds promise for improving this situation. Zhan et al162 modified nano-graphene oxide with chitosan oligosaccharide and anti-CD47, using this composite to load dacarbazine. They constructed a multifunctional nanoplatform, nGO-COS-CD47/DTIC, to achieve active targeted drug delivery and synergistic PTT treatment. Under the influence of CD47 receptor-mediated targeting by nGO-COS, the nanocomposite material achieved a high uptake intensity in melanoma cells at a relatively low concentration (5 μg/mL) (Figure 6C). Under near-infrared light irradiation, the temperature of nGO-COS rose to 55.5°C within 10 minutes, which is more than 20°C higher than other groups. This indicates a high photothermal conversion efficiency, which is proportional to concentration and laser power intensity, making it suitable for use as a thermotherapeutic agent (Figure 6H). At the same drug concentration, the number of cancer cells killed after treatment with free DTIC was significantly lower compared to nGO-COS-CD47/DTIC (Figure 6D). The highest cell kill rate was observed in B16-F10 cells treated with 10 μg/mL nGO-COS-CD47/DTIC under near-infrared light irradiation. Adding 10 minutes of NIR light irradiation to the 10 μg/mL nGO-COS-CD47/DTIC treatment further killed approximately 97% of the cells, demonstrating the chemo-photothermal synergistic effect of nGO-COS-CD47/DTIC.
In addition to being used in combination with chemotherapy and immunotherapy, some NPs can also exhibit both near-infrared absorption and the ability to generate ROS. In this context, the construction of bimodal PTT/PDT NP platforms becomes possible.171 PTT, along with PDT, can also exert a synergistic effect. Tang et al67 utilized indocyanine green to achieve synergistic PTT/PDT based on combined optical and chemical therapies. The researchers constructed the nanoplatforms HA-PAMAM-COOH-TMZ and HA-PAMAM-COOH-ICG by loading temozolomide and indocyanine green onto HA-modified carboxylated polyamidoamine, respectively, for combined chemotherapy and PTT/PDT (Figure 6B). Under near-infrared light irradiation, as the concentration of ICG increased, the temperature of HPCI rose, reaching over 50°C at its peak (Figure 6E). Moreover, at the same concentration, the heating capacity of HPCI was similar to that of free ICG (Figure 6F), while the production of ROS was higher than that of free ICG (Figure 6G), indicating that HPCI has a good foundational capability for synergistic PTT/PDT treatment. Under near-infrared irradiation, HPCI can exert PTT/PDT effects and further promote the release of TMZ from the carrier. Compared to using each treatment alone, the combined application of HPCT and HPCI demonstrated the strongest tumor cell-killing ability. HPCI first induces cytotoxic effects and subsequently leads to the ablation of residual tumor cells by HPCT, reducing cell viability to 17.1%. This indicates that the combination of HPCT and HPCI can exert a synergistic anti-tumor effect through chemotherapy, PTT, and PDT. This finding offers new insights and potential methods for the synergistic treatment of cancers such as melanoma.
In summary, the treatment of PTT relies on the photothermal conversion of PTA, which locally releases thermal energy to induce thermal damage to tumor cells. Compared to PDT, oxygen is not a necessary component in PTT treatment, as it relies on thermal energy to exert its effects. Therefore, precision treatment is particularly important in PTT. Applying light-triggered NPs to PTT can not only enhance the targeting effect of PTAs and increase their delivery efficiency to improve PTT efficacy but also serve as an adjuvant therapy after surgery to accelerate wound healing and reduce infection. The establishment of multifunctional NP platforms provides a foundation for the combined treatment of PTT. As a superficial skin tumor, PTT treatment for skin cancer has the advantages of easily reaching the treatment site and achieving precise treatment compared to other tumors. In addition, given the widespread use of surgery in skin cancer treatment, the prospects for applying PTT in post-surgical management of skin cancer are very promising and are increasingly attracting the attention of researchers. Although the application of PTT is not fully mature and the thermal damage to cells may cause some local tissue damage, PTT remains a potentially promising treatment option in the field of skin cancer.
Photoacoustic (PA)
Phototherapy offers advantages such as being non-invasive, having high spatiotemporal selectivity, and causing fewer side effects. It holds promising potential for treating superficial tumors, including skin cancer. However, classical phototherapies, including PDT and PTT, still face challenges such as suboptimal efficacy, unavoidable thermal damage, and high rates of postoperative recurrence.172 The application of PA provides advantages for visualizing the internal structure of tumor tissues, guiding the trend toward real-time imaging and precise treatment.
Principle of Photoacoustic
Theranostics is an emerging subset of multifunctional nanomedicine compounds.173 Generally speaking, theranostics uses the same nanoformulation to provide both diagnosis and treatment, offering therapeutic effects while also enabling monitoring.174 PA is a good example of theranostics, as it can be used for PAI and PAT.
Due to the presence of light scattering, the image resolution of PAI is significantly reduced in deep biological tissues, making the development of a new imaging modality urgently needed. PAI is a non-invasive imaging modality that is highly suitable for molecular imaging of superficial cancer tissues with high resolution, and shows great promise in real-time in vivo monitoring of biological processes with deep tissue penetration and high spatial resolution.175 Compared to traditional tumor imaging methods, PAI shows good advantages in both cellular and molecular imaging of tumors.176 PAI is a hybrid imaging modality that combines optical illumination and ultrasound detection.177 Compared to the traditional ultrasound’s “sound-in, sound-out” approach, PAI uses a “light-in, sound-out” method.178
In PAI, molecules absorb light energy and convert it into heat, raising the temperature of the surrounding tissue. The resulting thermoelastic expansion generates sound waves, which are detected using ultrasound transducers.179 Since sound scattering is 1000 times less than light scattering,180 sound signals can propagate through biological tissues for a longer duration without significant attenuation. Therefore, PAI combines the high temporal and spatial resolution of ultrasound with the good contrast and multiplexing capabilities of optical imaging.178
PAT utilizes photoacoustic shock waves generated by pulsed laser-activated NPs to kill cancer cells.32 This process utilizes the photoacoustic effect. It is a novel therapeutic approach in cancer-specific ablation therapy technologies. PAI has excellent contrast, high penetration, and sensitivity, creating favorable conditions for the implementation of PAT. The mechanism of PAT has many similarities with ultrasound therapy. The primary mechanism of ultrasound therapy is based on the conversion of mechanical energy into thermal energy while simultaneously producing cavitation effects. Cavitation can produce strong physical, chemical, and biological effects through the rapid growth and collapse of bubbles. The collapse of cavitation bubbles can generate strong shock waves with amplitudes exceeding 10,000 atmospheres and very high bubble temperatures.181 Applying PA to tumor treatment can damage cells and promote drug release through the cavitation effect of PA, thereby achieving therapeutic purposes. This new therapy can compensate for the shortcomings of traditional treatments, improve treatment accuracy, and reduce damage to normal tissues.182
Applications of PA in the Diagnosis and Treatment of Skin Tumors
Differential Diagnosis of Skin Tumors
PAI can detect ultrasound signals generated by transient thermal expansion of photoabsorbers upon pulsed light irradiation.182 It forms high-resolution structural and functional vascular images through photoacoustics.183,184 These high-resolution PA vascular images provide important information about malignant tumors.185
The high sensitivity and high-resolution deep tissue optical imaging capabilities of PAI enable it to play a significant role in cancer diagnosis. To further improve the detection sensitivity and signal-to-noise ratio of PAI, Liu et al78 attempted to develop a switchable PA probe that provides on/off signal response to tumor targets. They designed a glutathione-responsive PAI based on MnO2, where glutathione reduces black MnO2 into colorless Mn²+ ions, resulting in decreased PA amplitude and signal shutdown. In the PAI validation experiments, untreated control cells showed the lowest PA amplitude, while cells incubated with MnO2 nanotubes exhibited the highest PA amplitude, which was 2.2 times higher than the control group and showed the slowest decrease in amplitude (Figure 7G). In PAI, the stability of nanomaterials is a non-negligible issue, in order to study the stability of MnO2 nanotubes in repetitive imaging, the researchers detected the PA signals of 2 mg/mL manganese dioxide nanotubes at 100, 2000, 4000, 8000 and 16000 laser pulses, respectively, and the results showed that there was no significant difference in the PA signals obtained at different laser pulses, and the this also proves the good stability of MnO2 nanotubes in PAI. (Figure 7A). The experiments also ruled out the dilution effect caused by tumor growth as a factor for the reduction in PA signal, confirming the sensitivity of MnO2 nanotubes as PA probes for PAI (Figure 7B and C). These results indicate that MnO2-based glutathione nanotubes can differentiate melanoma cells from normal cells, validating the feasibility of PAI in cancer diagnosis.
 |
Figure 7 (A) PA signals of MnO2 nanotubes under different laser pulse conditions. (B) PA images at different time points after injection. *P < 0.05 (C) Normalized PA amplitude of tumor and healthy tissues. Reprinted with permission from Liu C, Wang D, Zhan Y, et al. Switchable photoacoustic imaging of glutathione using MnO(2) nanotubes for cancer diagnosis. ACS Appl Mater Interfaces. 2018;10:44231–44239. Copyright © 2018 American Chemical Society.78 (D) Tumor growth curve. (E) Photoacoustic computed tomography (PAT) and photoacoustic microscopy (PAM) images of mouse tumors before and after intravenous injection of FA-AuNRs. Scale bar is 2 mm. (F) Representative photos of tumor-bearing mice under different treatments. Reprinted from Nanomedicine. Volume 11. Zhong J, Wen L, Yang S, Xiang L, Chen Q, Xing D. Imaging-guided high-efficient photoacoustic tumor therapy with targeting gold nanorods. 1499–1509. Copyright © 2015 Elsevier.186 (G) Comparison of PA amplitude of B16F10 cells after 18 hours of incubation with the control group. Scale bar is 1 mm. Reprinted with permission from Liu C, Wang D, Zhan Y, et al. Switchable photoacoustic imaging of glutathione using MnO(2) nanotubes for cancer diagnosis. ACS Appl Mater Interfaces. 2018;10:44231–44239. Copyright © 2018 American Chemical Society.78 (H) H&E staining images of tumor sections. Scale bar is 50 μm. Reprinted from Nanomedicine. Volume 11. Zhong J, Wen L, Yang S, Xiang L, Chen Q, Xing D. Imaging-guided high-efficient photoacoustic tumor therapy with targeting gold nanorods. 1499–1509. Copyright © 2015 Elsevier.186 |
urrently, compared to PAT, PAI is more widely applied in tumor treatment, often used for tumor imaging to guide PDT/PTT therapy. Its superior imaging performance provides a solid foundation for the diagnosis and treatment guidance of tumors.
Applications of the PA Effect in Treatment
PAT typically utilizes PA shock waves/cavitation to exert selective therapeutic effects. Its therapeutic mechanism involves converting light energy into sound energy, generating strong shock waves that mechanically damage tumor cells, leading to cell death, known as the PA effect. After these sound waves are detected by ultrasound transducers, they can be output as images, fulfilling the role of PAI.187 Therefore, the combination of PAT and PAI based on the PA effect has a theoretical foundation.
Zhong et al186 used gold nanorods with high optical absorbance and PA intensity to explore the applicable range of their PA effect. After laser pulse irradiation, the cell viability of gold nanorod-treated cells decreased by 74.4% and exhibited a concentration-dependent effect. In the validation of PA toxicity, laser irradiation alone did not show significant negative effects on cell proliferation, confirming the low cytotoxicity of PA and further indicating the safety of PAT. The researchers also conducted in vivo experiments and found that AuNRs could specifically accumulate at tumor sites, acting as contrast agents in PAI(Figure 7E). In the mouse intravenous injection PAT study, all tumors in the laser + FA-AuNRs group were damaged, and their growth rate was slower. No abnormal effects were observed in other organs of the experimental mice (Figures 7D, F, H and 8A). Further studies indicate that low-intensity laser irradiation is suitable for PAI, while high-intensity laser can induce cell death, thus performing the PAT function. This work validated the dual role of the photoacoustic effect in tumor diagnosis and treatment, achieving PAT-mediated anti-tumor effects and PAI-mediated cancer cell diagnosis.
Photoacoustic Targeted Therapy
PAT rapidly and specifically kills cancer cells based on photoacoustic shock waves, often targeting specific sites to cause cellular structural damage. For example, Zhou et al188 used unmodified single-walled carbon nanotubes to target mitochondria, exploiting the higher mitochondrial membrane potential in cancer cells compared to normal cells. This triggered mitochondrial damage, and following PAT, the release of cytochrome c led to the killing of cancer cells. Kang et al187 reported a cancer cell-targeted PAT using carbon nanotubes. They utilized folic acid-functionalized single-walled carbon nanotubes to target tumors by binding to folate receptors overexpressed on the tumor cell membrane surface.
The cell nucleus, as the center of genetic and metabolic control, plays a crucial role in cellular metabolic activities. Targeting the cell nucleus for PAT is a logical and effective strategy.
Wang et al37 developed an efficient nuclear-targeted PAT polymer (TAT-PDMA-hCyR-NPs) for fluorescence and photoacoustic dual-modality imaging-guided PA therapy. This polymer utilizes the nuclear-targeting peptide TAT to achieve targeting. TAT-PDMA-hCyR-NPs can enter the cell nucleus and show high fluorescence within 2 hours of incubation, whereas nano-complexes without the TAT peptide cannot enter the cell nucleus. Compared to nano-complexes without the TAT peptide, TAT-PDMA-hCyR-NPs show significant killing effects under 808nm laser irradiation, achieving an 80% killing efficiency of tumor cells and demonstrating a notable photoacoustic effect. This experiment demonstrated the effectiveness of PAT in tumor treatment, and the nuclear-targeting approach provided a preliminary experimental basis for nuclear-targeted PAT research.
Photoacoustic Immunotherapy
Phototherapy has the advantages of being relatively non-invasive, having few side effects, and high selectivity, offering broad application prospects in superficial tumors. The PA effect not only converts the output sound energy into images, accurately depicting tumor areas and providing a basis for precise treatment, but it can also utilize the PA cavitation effect to destroy tumor cells, achieving a novel PAT treatment method for tumor cells. However, as a mode of phototherapy, PAT, like PDT and PTT, has limitations in its anti-cancer efficacy, particularly in controlling post-treatment recurrence and cancer cell metastasis. PDT and PTT have chosen to combine with immunotherapy to address these subsequent challenges in tumor treatment. For PAT to transition from laboratory research to clinical application, these issues are also unavoidable.
In further exploration of PA, researchers have discovered that PA can induce immunogenic cell death, which can enhance anti-tumor immune responses under certain conditions. This led to the proposal of a novel PA immunotherapy strategy. Currently, a series of NPs encoding cytosine-phosphate-guanine (CpG) have been developed to prolong antigen persistence and ultimately enhance the synergistic effect of photoimmunotherapy by improving antigen processing and presentation efficiency, significantly boosting its immunogenicity.189 He et al172 utilized polydopamine-functionalized black scales to further adsorb CpG, synthesizing a nanocomposite material called PBP@CpG, which exhibits excellent optical and immune-stimulating properties. When PBP and BP contrast agents were separately injected intravenously into tumor-bearing mice, the mice injected with PBP exhibited higher contrast in the tumor region on PAI, with a duration of up to 24 hours (Figure 8B). The photoacoustic signal intensity in these mice was stronger than in those injected with BP, indicating that PBP has stronger light absorption and higher stability, with more pronounced PAI capabilities. In terms of PAT, the killing efficiency was also the highest, with the photoacoustic cavitation effect causing the loss of cell membrane integrity and disruption of the cytoskeleton. The maximum cell apoptosis rate reached 74% (Figure 8C and D). Under the action of PBP@CpG + laser, there was a significant upregulation of CD80 and CD86, indicating increased DC maturation. A noticeable infiltration of CD8+ cells in the tumor site was observed (Figure 8E–G). Serum tests on day 7 also showed a significant increase in the release of various cytokines in the PA treatment group compared to the control group. This indicates the positive role of the immune system in the anti-tumor process and the enhancing effect of the photoacoustic cavitation on the anti-tumor immune response.
Figure 8 Continued. Figure 8 (A) Histological staining of organs in mice 25 days after treatment. Scale bar is 50 μm. Reprinted from Nanomedicine. Volume 11. Zhong J, Wen L, Yang S, Xiang L, Chen Q, Xing D. Imaging-guided high-efficient photoacoustic tumor therapy with targeting gold nanorods. 1499–1509. Copyright © 2015 Elsevier.186 (B) Fluorescence images of tumor-bearing mice at different treatment time points. (C) Photoacoustic cavitation-induced cytoskeletal disruption. Scale bar of the top half of the figure is 20 μm; Scale bar of the bottom half of the figure is 10 μm. (D) Cell death analysis using membrane-permeable V-FITC/PI double staining. (E and F) Representative flow cytometry profile of mature dendritic cells in tumor tissue and analysis of T cell infiltration. (G) Immunofluorescence images of CD8 and granzyme B after different treatments. Scale bar is 50 μm. Reprinted with permission from He J, Ouyang X, Xiao F, Liu N, Wen L. Imaging-guided photoacoustic immunotherapy based on the polydopamine-functionalized black phosphorus nanocomposites. ACS Appl Mater Interfaces. 2023;15:54322–54334. Copyright © 2023 American Chemical Society.172

In summary, PA is a phototherapy method based on theranostics, with its mechanism rooted in the PA effect. As an emerging imaging modality, PAI is highly suitable for molecular imaging of skin tumors, offering higher temporal and spatial resolution. Compared to traditional optical imaging, PAI addresses the limitations of signal attenuation and unclear resolution in pure optical imaging. The application of PAT utilizes the photoacoustic cavitation effect, where shock waves can cause damage to cells. Recent research has further explored the immunotherapeutic aspects of photoacoustics, offering new possibilities for the application of PAT. The development of PA has provided a foundation for the precise diagnosis and treatment of skin tumors. Although there are still some limitations in the selection of PA contrast agents and the application of targeting strategies, PA, particularly PAI, has been widely used in research and is gradually transitioning from the micro laboratory stage to the macro clinical practice stage.
Future Perspectives and Conclusions
This review summarizes the application of light-triggered nanomaterials in the treatment of skin cancer. Light-triggered nanomaterials represent a significant advancement in the treatment of skin cancers, offering precision, minimal invasiveness, and the ability to generate reactive oxygen species (ROS) for targeted tumor ablation. These materials have demonstrated potential in overcoming some limitations of conventional therapies, such as surgery and chemotherapy, particularly through photodynamic therapy (PDT), photothermal therapy (PTT), and photoacoustic therapy (PAT).
Despite these advancements, challenges remain, including biological barriers to delivery, limited light penetration, and the scalability and cost of nanomaterial production. The integration of advanced delivery systems, such as targeting ligands and stimuli-responsive carriers, shows promise in improving therapeutic outcomes.
By designing nano-delivery systems, the treatment options for skin cancer can be expanded (Scheme 1). Phototherapy applied to skin cancer can function through PDT, PTT, and PA (Figure 1), offering both diagnostic and therapeutic effects. Based on these different phototherapy methods, researchers have designed various treatment strategies. In phototherapy mediated by light-triggered NPs, the therapeutic effect can be enhanced by countering the TME, improving targeting capabilities and drug delivery efficiency, inducing selective cytotoxicity, or employing combination therapies. Additionally, given that surgery remains the most mainstream treatment for skin cancer, the reasonable application of phototherapy can also play a positive role in the diagnosis of skin cancer and the prevention of postoperative complications. PDT has been in clinical use for over 40 years. In contrast, the clinical translation of PTT and PA has been less extensive, partly due to the limitations in the selection of PTAs and photoacoustic contrast agents. In current clinical applications, the safety of PTAs and photoacoustic contrast agents remains a concern. The use of PSs also faces challenges related to toxicity risks. This is one of the reasons why surgical treatment remains the primary approach for skin cancer, despite PDT’s successful clinical translation in dermatology and the potential for complications with surgery. On the other hand, while the application of light-triggered NPs presents new opportunities for phototherapy, it also introduces new challenges. The convenience of nanotechnology is undeniable. By designing nano-delivery systems appropriately, it can improve drug delivery efficiency, enhance targeting capabilities, and achieve controlled drug release. However, the complexity of nano systems is a major obstacle to the application of light-triggered nanomaterials. A well-designed system can even mitigate the toxicity of photoconversion agents to some extent. Therefore, the system design based on light-triggered nanomaterials remains a hot topic in current research and holds significant development potential.
 |
Scheme 1 Three phototherapies strategies for treating skin tumors. |
In addition to the design of delivery systems, we also need to consider the potential for establishing multimodal platforms. Although dual-modal platforms, such as those combining PDT and PTT, have been proposed as joint therapies, the challenges of translating experimental results into clinical applications remain significant. Currently, multimodal platforms face issues such as disproportionate costs relative to expected outcomes and incomplete structural functionality. Therefore, developing low-cost and reliable multimodal platforms is crucial for expanding their range of applications. Reducing the cost of individual therapies is a reliable approach. Additionally, improving platform structural compatibility to achieve multifunctional effects simultaneously, enhancing therapeutic outcomes, and increasing indications is also a viable strategy (Figure 4G).
Despite significant advancements, the clinical translation of phototherapy faces several challenges. The scalability of nanomaterial production remains a major hurdle, as current manufacturing methods often result in batch-to-batch variability and lack reproducibility at a large scale. Regulatory approval processes further complicate translation, as the unique properties of nanomaterials often place them in regulatory gray areas, requiring extensive safety, efficacy, and biocompatibility data. Developing cost-effective and reproducible synthesis methods while ensuring batch-to-batch consistency is critical. Collaborative efforts between academia, industry, and regulatory bodies will be essential to address these issues. Additionally, implementing combined therapies, such as photodynamic therapy (PDT) with immunotherapy, introduces complexities, including the potential for immune-related adverse events and the need to optimize treatment protocols for timing, dosing, and sequencing. Combining phototherapy with other treatment modalities, such as immunotherapy or chemotherapy, offers promising synergistic effects but also introduces new challenges. For example, the potential for immune-related adverse events in photodynamic therapy (PDT) combined with immunotherapy must be carefully evaluated in preclinical and clinical studies. Addressing these issues through standardized guidelines, improved manufacturing techniques, and robust preclinical data will be essential to advance phototherapy toward clinical application terms of precision and localized treatment. However, it lacks the systemic immune activation and genome-wide editing capabilities of these advanced therapies. Combining phototherapy with immunotherapy or gene editing could create synergistic effects, but this also introduces complexities such as immune-related adverse events or off-target genetic modifications. Future research should prioritize the development of next-generation nanomaterials with enhanced biocompatibility, tunable properties, and multifunctional capabilities. Additionally, integrating imaging techniques such as photoacoustic imaging with phototherapy could further enhance precision and efficacy.
Currently, an increasing number of people are affected by skin cancer. Phototherapy, as a reliable non-invasive or minimally invasive treatment, offers a promising therapeutic option. It is hoped that the clinical application of light-triggered nanomaterials for skin cancer, as discussed in this article, can aid in the accurate diagnosis, precise treatment, and prevention of recurrence and complications, thereby improving the survival rate and quality of life for skin cancer patients.
Abbreviations
PDT, photodynamic therapy; PTT, photothermal therapy; PAT, photoacoustic therapy; MSC, melanoma skin cancer; NMSC, non-melanoma skin cancer; BCC, basal cell carcinoma; SCC, squamous cell carcinoma; MDR, multidrug resistance; NP, nanoparticle; UV, ultraviolet; NER, nucleotide excision repair; SC, stratum corneum; TME, tumor microenvironment; ROS, reactive oxygen species; PS, photosensitizer; PTA, photothermal agent; NDDS, nanomedicine drug delivery systems; DDS, drug delivery systems; UCNPs, upconversion nanoparticles; PIT, photodynamic immunotherapy; PB, Prussian Blue; PAI, photoacoustic imaging. PA, photoacoustic.
Acknowledgments
The figures in this article were created using BioRender.
Disclosure
The authors declare no competing interests in this work.
References
1. An S, Kim K, Moon S, et al. Indoor tanning and the risk of overall and early-onset melanoma and non-melanoma skin cancer: systematic review and meta-analysis. Cancers. 2021;13:5940. doi:10.3390/cancers13235940
2. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74:12–49. doi:10.3322/caac.21820
3. Kaur H, Kesharwani P. Advanced nanomedicine approaches applied for treatment of skin carcinoma. J Control Release. 2021;337:589–611. doi:10.1016/j.jconrel.2021.08.003
4. Dadzie OE, Jablonski NG, Mahalingam M, Dupuy A, Petit A. Skin cancer, photoprotection, and skin of color. J Am Acad Dermatol. 2014;71:586. doi:10.1016/j.jaad.2014.04.071
5. Kaufman BP, Alexis AF. Skin cancer mortality in patients with skin of color. Cutis. 2017;99:307–308.
6. Davis DS, Robinson C, Callender VD. Skin cancer in women of color: epidemiology, pathogenesis and clinical manifestations. Int J Womens Dermatol. 2021;7:127–134. doi:10.1016/j.ijwd.2021.01.017
7. Hak A, Ravasaheb Shinde V, Rengan AK. A review of advanced nanoformulations in phototherapy for cancer therapeutics. Photodiagnosis Photodyn Ther. 2021;33:102205. doi:10.1016/j.pdpdt.2021.102205
8. Ackroyd R, Kelty C, Brown N, Reed M. The history of photodetection and photodynamic therapy. Photochem Photobiol. 2001;74:656–669.
9. Tan M, Li X, Zhang H, et al. Förster resonance energy transfer nanobullet for photoacoustic imaging and amplified photothermal-photodynamic therapy of cancer. Adv Healthc Mater. 2023;12:e2202943. doi:10.1002/adhm.202202943
10. Hu J, Luo H, Qu Q, et al. Cell membrane-inspired polymeric vesicles for combined photothermal and photodynamic prostate cancer therapy. ACS Appl Mater Interfaces. 2020;12:42511–42520. doi:10.1021/acsami.0c11636
11. Hasan N, Nadaf A, Imran M, et al. Skin cancer: understanding the journey of transformation from conventional to advanced treatment approaches. mol Cancer. 2023;22:168. doi:10.1186/s12943-023-01854-3
12. Ayala-Orozco C, Galvez-Aranda D, Corona A, et al. Molecular jackhammers eradicate cancer cells by vibronic-driven action. Nat Chem. 2024;16:456–465. doi:10.1038/s41557-023-01383-y
13. Kalka K, Merk H, Mukhtar H. Photodynamic therapy in dermatology. J Am Acad Dermatol. 2000;42:389–413;quiz4–6. doi:10.1016/S0190-9622(00)90209-3
14. Li X, Lovell JF, Yoon J, Chen X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat Rev Clin Oncol. 2020;17:657–674. doi:10.1038/s41571-020-0410-2
15. Losquadro WD. Anatomy of the Skin and the Pathogenesis of Nonmelanoma Skin Cancer. Facial Plast Surg Clin North Am. 2017;25:283–289. doi:10.1016/j.fsc.2017.03.001
16. Khan NH, Mir M, Qian L, et al. Skin cancer biology and barriers to treatment: recent applications of polymeric micro/nanostructures. J Adv Res. 2022;36:223–247. doi:10.1016/j.jare.2021.06.014
17. Akhtar N, Khan RA. Liposomal systems as viable drug delivery technology for skin cancer sites with an outlook on lipid-based delivery vehicles and diagnostic imaging inputs for skin conditions’. Prog Lipid Res. 2016;64:192–230. doi:10.1016/j.plipres.2016.08.005
18. Apalla Z, Nashan D, Weller RB, Castellsagué X. Skin cancer: epidemiology, disease burden, pathophysiology, diagnosis, and therapeutic approaches. Dermatol Ther. 2017;7:5–19. doi:10.1007/s13555-016-0165-y
19. Paolino G, Donati M, Didona D, Mercuri SR, Cantisani C. Histology of non-melanoma skin cancers: an update. Biomedicines. 2017;5:5. doi:10.3390/biomedicines5010005
20. Lawrence MS, Stojanov P, Polak P, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature. 2013;499:214–218. doi:10.1038/nature12213
21. Akbani R, Akdemir K, Aksoy B. Genomic classification of cutaneous melanoma. Cell. 2015;161:1681–1696. doi:10.1016/j.cell.2015.05.044
22. Sample A, He YY. Mechanisms and prevention of UV-induced melanoma. Photodermatol Photoimmunol Photomed. 2018;34:13–24. doi:10.1111/phpp.12329
23. de Gruijl FR. Photocarcinogenesis: UVA vs. UVB radiation. Skin Pharmacol Appl Skin Physiol. 2002;15:316–320. doi:10.1159/000064535
24. Bradford PT, Goldstein AM, Tamura D, et al. Cancer and neurologic degeneration in xeroderma pigmentosum: long term follow-up characterises the role of DNA repair. J Med Genet. 2011;48:168–176. doi:10.1136/jmg.2010.083022
25. Situm M, Buljan M, Kolić M, Vučić M. Melanoma--clinical, dermatoscopical, and histopathological morphological characteristics. Acta Dermatovenerol Croat. 2014;22:1–12.
26. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1–6. doi:10.5826/dpc.0702a01
27. Long GV, Swetter SM, Menzies AM, Gershenwald JE, Scolyer RA. Cutaneous melanoma. Lancet. 2023;402:485–502. doi:10.1016/S0140-6736(23)00821-8
28. Matthews NH, Li WQ, Qureshi AA, Weinstock MA, Cho E. Epidemiology of Melanoma. In: Ward WH, Farma JM, editors. Cutaneous Melanoma: Etiology and Therapy. Brisbane (AU): Codon Publications The Authors; 2017.
29. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
30. Millet A, Martin AR, Ronco C, Rocchi S, Benhida R. Metastatic melanoma: insights into the evolution of the treatments and future challenges. Med Res Rev. 2017;37:98–148. doi:10.1002/med.21404
31. Garbe C, Amaral T, Peris K, et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: diagnostics - update 2019. Eur J Cancer. 2020;126:141–158. doi:10.1016/j.ejca.2019.11.014
32. Liu L, Chen Q, Wen L, Li C, Qin H, Xing D. Photoacoustic therapy for precise eradication of glioblastoma with a tumor site blood–brain barrier permeability upregulating nanoparticle. Adv Funct Mater. 2019;29:1808601. doi:10.1002/adfm.201808601
33. O’Driscoll L, McMorrow J, Doolan P, et al. Investigation of the molecular profile of basal cell carcinoma using whole genome microarrays. mol Cancer. 2006;5:74.
34. Samarasinghe V, Madan V. Nonmelanoma skin cancer. J Cutan Aesthet Surg. 2012;5:3–10. doi:10.4103/0974-2077.94323
35. Silk AW, Barker CA, Bhatia S, et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of nonmelanoma skin cancer. J Immunother Cancer. 2022;10:e004434. doi:10.1136/jitc-2021-004434
36. Matsui T, Amagai M. Dissecting the formation, structure and barrier function of the stratum corneum. Int Immunol. 2015;27:269–280. doi:10.1093/intimm/dxv013
37. Wang Y, Niu G, Zhai S, Zhang W, Xing D. Specific photoacoustic cavitation through nucleus targeted nanoparticles for high-efficiency tumor therapy. Nano Res. 2020;13:719–728.
38. Chandra J, Hasan N, Nasir N, et al. Nanotechnology-empowered strategies in treatment of skin cancer. Environ Res. 2023;235:116649. doi:10.1016/j.envres.2023.116649
39. Paudel KS, Milewski M, Swadley CL, Brogden NK, Ghosh P, Stinchcomb AL. Challenges and opportunities in dermal/transdermal delivery. Ther Deliv. 2010;1:109–131. doi:10.4155/tde.10.16
40. Borgheti-Cardoso LN, Viegas JSR, Silvestrini AVP, et al. Nanotechnology approaches in the current therapy of skin cancer. Adv Drug Deliv Rev. 2020;153:109–136. doi:10.1016/j.addr.2020.02.005
41. DeBerardinis RJ. Tumor microenvironment, metabolism, and immunotherapy. N Engl J Med. 2020;382:869–871. doi:10.1056/NEJMcibr1914890
42. Zhang M, Zhao Y, Ma H, Sun Y, Cao J. How to improve photodynamic therapy-induced antitumor immunity for cancer treatment? Theranostics. 2022;12:4629–4655. doi:10.7150/thno.72465
43. Chen Q, Liu G, Liu S, et al. Remodeling the tumor microenvironment with emerging nanotherapeutics. Trends Pharmacol Sci. 2018;39:59–74. doi:10.1016/j.tips.2017.10.009
44. Bukowski K, Kciuk M, Kontek R. Mechanisms of multidrug resistance in cancer chemotherapy. Int J mol Sci. 2020;21.
45. Kartal-Yandim M, Adan-Gokbulut A, Baran Y. Molecular mechanisms of drug resistance and its reversal in cancer. Crit Rev Biotechnol. 2016;36:716–726. doi:10.3109/07388551.2015.1015957
46. Dallavalle S, Dobričić V, Lazzarato L, et al. Improvement of conventional anti-cancer drugs as new tools against multidrug resistant tumors. Drug Resist Updat. 2020;50:100682. doi:10.1016/j.drup.2020.100682
47. Pakunlu RI, Wang Y, Saad M, Khandare JJ, Starovoytov V, Minko T. In vitro and in vivo intracellular liposomal delivery of antisense oligonucleotides and anticancer drug. J Control Release. 2006;114:153–162. doi:10.1016/j.jconrel.2006.06.010
48. Pakunlu RI, Wang Y, Tsao W, Pozharov V, Cook TJ, Minko T. Enhancement of the efficacy of chemotherapy for lung cancer by simultaneous suppression of multidrug resistance and antiapoptotic cellular defense: novel multicomponent delivery system. Cancer Res. 2004;64:6214–6224. doi:10.1158/0008-5472.CAN-04-0001
49. Loo TW, Clarke DM. Merck Frosst Award Lecture 1998. Molecular dissection of the human multidrug resistance P-glycoprotein. Biochem Cell Biol. 1999;77:11–23. doi:10.1139/o99-014
50. Minko T, Rodriguez-Rodriguez L, Pozharov V. Nanotechnology approaches for personalized treatment of multidrug resistant cancers. Adv Drug Deliv Rev. 2013;65:1880–1895. doi:10.1016/j.addr.2013.09.017
51. Bhattacharyya S, Khanduja KL. New hope in the horizon: cancer stem cells. Acta Biochim Biophys Sin. 2010;42:237–242. doi:10.1093/abbs/gmq013
52. Shah V, Taratula O, Garbuzenko OB, Taratula OR, Rodriguez-Rodriguez L, Minko T. Targeted nanomedicine for suppression of CD44 and simultaneous cell death induction in ovarian cancer: an optimal delivery of siRNA and anticancer drug. Clin Cancer Res. 2013;19:6193–6204. doi:10.1158/1078-0432.CCR-13-1536
53. Badea I. New strategies in melanoma therapy: can nanoparticles overcome chemoresistance? Nanomedicine. 2017;12:1623–1626. doi:10.2217/nnm-2017-0145
54. Kanapathipillai M, Brock A, Ingber DE. Nanoparticle targeting of anti-cancer drugs that alter intracellular signaling or influence the tumor microenvironment. Adv Drug Deliv Rev. 2014;79-80:107–118. doi:10.1016/j.addr.2014.05.005
55. Blau R, Krivitsky A, Epshtein Y, Satchi-Fainaro R. Are nanotheranostics and nanodiagnostics-guided drug delivery stepping stones towards precision medicine? Drug Resist Updat. 2016;27:39–58. doi:10.1016/j.drup.2016.06.003
56. Guo Z, Zhu AT, Fang RH, Zhang L. Recent developments in nanoparticle-based photo-immunotherapy for cancer treatment. Small Methods. 2023;7:e2300252. doi:10.1002/smtd.202300252
57. Martinez JC, Otley CC. The management of melanoma and nonmelanoma skin cancer: a review for the primary care physician. Mayo Clin Proc. 2001;76:1253–1265. doi:10.4065/76.12.1253
58. Griffin LL, Ali FR, Lear JT. Non-melanoma skin cancer. Clin Med. 2016;16:62–65. doi:10.7861/clinmedicine.16-1-62
59. Dika E, Scarfì F, Ferracin M, et al. Basal Cell Carcinoma: a Comprehensive Review. Int J mol Sci. 2020;22:21. doi:10.3390/ijms22010021
60. Gonsalves A, Tambe P, Le D, et al. Synthesis and characterization of a novel pH-responsive drug-releasing nanocomposite hydrogel for skin cancer therapy and wound healing. J Mater Chem B. 2021;9:9533–9546. doi:10.1039/d1tb01934a
61. Kettiger H, Schipanski A, Wick P, Huwyler J. Engineered nanomaterial uptake and tissue distribution: from cell to organism. Int J Nanomed. 2013;8:3255–3269. doi:10.2147/IJN.S49770
62. Savla R, Minko T. Nanoparticle design considerations for molecular imaging of apoptosis: diagnostic, prognostic, and therapeutic value. Adv Drug Deliv Rev. 2017;113:122–140. doi:10.1016/j.addr.2016.06.016
63. Barua S, Mitragotri S. Synergistic targeting of cell membrane, cytoplasm, and nucleus of cancer cells using rod-shaped nanoparticles. ACS Nano. 2013;7:9558–9570. doi:10.1021/nn403913k
64. Brown JM, Wilson WR. Exploiting tumour hypoxia in cancer treatment. Nat Rev Cancer. 2004;4:437–447. doi:10.1038/nrc1367
65. Jiang W, Delahunty IM, Xie J. Oxygenating the way for enhanced chemophototherapy. Theranostics. 2018;8:3870–3871. doi:10.7150/thno.27810
66. Huang L, Chen X, Bian Q, et al. Photosensitizer-stabilized self-assembling nanoparticles potentiate chemo/photodynamic efficacy of patient-derived melanoma. J Control Release. 2020;328:325–338. doi:10.1016/j.jconrel.2020.08.062
67. Tang J, Zhou H, Hou X, et al. Enhanced anti-tumor efficacy of temozolomide-loaded carboxylated poly(amido-amine) combined with photothermal/photodynamic therapy for melanoma treatment. Cancer Lett. 2018;423:16–26. doi:10.1016/j.canlet.2018.03.002
68. Huang X, Mu N, Ding Y, et al. Targeted delivery and enhanced uptake of chemo-photodynamic nanomedicine for melanoma treatment. Acta Biomater. 2022;147:356–365. doi:10.1016/j.actbio.2022.05.015
69. Song Y, Shi Q, Zhu C, et al. Mitochondrial-targeted multifunctional mesoporous Au@Pt nanoparticles for dual-mode photodynamic and photothermal therapy of cancers. Nanoscale. 2017;9:15813–15824. doi:10.1039/C7NR04881E
70. Wang MF, Yang R, Tang SJ, et al. In vivo realization of dual photodynamic and photothermal therapy for melanoma by mitochondria targeting dinuclear ruthenium complexes under civil infrared low-power laser. Angew Chem Int Ed Engl. 2022;61:e202208721. doi:10.1002/anie.202208721
71. Pandesh S, Haghjooy Javanmard S, Shakeri-Zadeh A, Shokrani P. Targeted photothermal therapy of melanoma in C57BL/6 Mice using Fe(3)O(4)@Au core-shell nanoparticles and near-infrared laser. J Biomed Phys Eng. 2021;11:29–38. doi:10.31661/jbpe.v0i0.736
72. Tang SJ, Li QF, Wang MF, et al. Bleeding the excited state energy to the utmost: single-molecule iridium complexes for in vivo dual photodynamic and photothermal therapy by an infrared low-power laser. Adv Healthc Mater. 2023;12:e2301227. doi:10.1002/adhm.202301227
73. Jiang Q, Liu Y, Guo R, et al. Erythrocyte-cancer hybrid membrane-camouflaged melanin nanoparticles for enhancing photothermal therapy efficacy in tumors. Biomaterials. 2019;192:292–308. doi:10.1016/j.biomaterials.2018.11.021
74. Li H, Yue L, Li L, et al. Triphenylamine-perylene diimide conjugate-based organic nanoparticles for photoacoustic imaging and cancer phototherapy. Colloids Surf B Biointerfaces. 2021;205:111841. doi:10.1016/j.colsurfb.2021.111841
75. Zhu Y, Xue J, Chen W, et al. Albumin-biomineralized nanoparticles to synergize phototherapy and immunotherapy against melanoma. J Control Release. 2020;322:300–311. doi:10.1016/j.jconrel.2020.03.045
76. Zhang Y, Li F, Ya S, et al. An iron oxide nanoparticle-based transdermal nanoplatform for dual-modal imaging-guided chemo-photothermal therapy of superficial tumors. Acta Biomater. 2021;130:473–484. doi:10.1016/j.actbio.2021.05.033
77. Salomón FF, Vega NC, Jurado JP, et al. Heteroleptic Ruthenium(II) complexes with 2,2’-bipyridines having carbonitriles as anchoring groups for ZnO surfaces: syntheses, physicochemical properties, and applications in organic solar cells. Inorg Chem. 2021;60:5660–5672. doi:10.1021/acs.inorgchem.0c03691
78. Liu C, Wang D, Zhan Y, et al. Switchable photoacoustic imaging of glutathione using MnO(2) nanotubes for cancer diagnosis. ACS Appl Mater Interfaces. 2018;10:44231–44239. doi:10.1021/acsami.8b14944
79. Cui H, Zhang X, Zhang Z, et al. Killing three birds with one stone: tumor-membrane-decorated Prussian blue nanovaccines for synergistic management of skin tumors, radiation dermatitis and wounds. Composites Part B. 2023;264:110900. doi:10.1016/j.compositesb.2023.110900
80. Liang S, Sun C, Yang P, et al. Core-shell structured upconversion nanocrystal-dendrimer composite as a carrier for mitochondria targeting and catalase enhanced anti-cancer photodynamic therapy. Biomaterials. 2020;240:119850. doi:10.1016/j.biomaterials.2020.119850
81. Chen X, Li Q, Huang Z, Lin W, Ma Y. Construction and evaluation of curcumin upconversion nanocarriers decorated with MnO(2) for tumor photodynamic therapy. Drug Deliv Transl Res. 2022;12:2678–2692. doi:10.1007/s13346-022-01118-5
82. Goto PL, Siqueira-Moura MP, Tedesco AC. Application of aluminum chloride phthalocyanine-loaded solid lipid nanoparticles for photodynamic inactivation of melanoma cells. Int J Pharm. 2017;518:228–241. doi:10.1016/j.ijpharm.2017.01.004
83. Petrilli R, Eloy JO, Saggioro FP, et al. Skin cancer treatment effectiveness is improved by iontophoresis of EGFR-targeted liposomes containing 5-FU compared with subcutaneous injection. J Control Release. 2018;283:151–162. doi:10.1016/j.jconrel.2018.05.038
84. Wang YG, Kim H, Mun S, Kim D, Choi Y. Indocyanine green-loaded perfluorocarbon nanoemulsions for bimodal (19)F-magnetic resonance/nearinfrared fluorescence imaging and subsequent phototherapy. Quant Imaging Med Surg. 2013;3:132–140. doi:10.3978/j.issn.2223-4292.2013.06.03
85. Kawasaki R, Kondo K, Miura R, et al. Theranostic agent combining fullerene nanocrystals and gold nanoparticles for photoacoustic imaging and photothermal therapy. Int J mol Sci. 2022;23:4686. doi:10.3390/ijms23094686
86. Xing R, Zou Q, Yuan C, Zhao L, Chang R, Yan X. Self-assembling endogenous biliverdin as a versatile near-infrared photothermal nanoagent for cancer theranostics. Adv Mater. 2019;31:e1900822. doi:10.1002/adma.201900822
87. Ren Y, Yan Y, Qi H. Photothermal conversion and transfer in photothermal therapy: from macroscale to nanoscale. Adv Colloid Interface Sci. 2022;308:102753. doi:10.1016/j.cis.2022.102753
88. Sridharan B, Lim HG. Advances in photoacoustic imaging aided by nano contrast agents: special focus on role of lymphatic system imaging for cancer theranostics. J Nanobiotechnology. 2023;21:437. doi:10.1186/s12951-023-02192-8
89. Jhaveri A, Deshpande P, Torchilin V. Stimuli-sensitive nanopreparations for combination cancer therapy. J Control Release. 2014;190:352–370. doi:10.1016/j.jconrel.2014.05.002
90. Liu Q, Das M, Liu Y, Huang L. Targeted drug delivery to melanoma. Adv Drug Deliv Rev. 2018;127:208–221. doi:10.1016/j.addr.2017.09.016
91. Hsu CY, Chen CW, Yu HP, Lin YF, Lai PS. Bioluminescence resonance energy transfer using luciferase-immobilized quantum dots for self-illuminated photodynamic therapy. Biomaterials. 2013;34:1204–1212. doi:10.1016/j.biomaterials.2012.08.044
92. Chatterjee DK, Fong LS, Zhang Y. Nanoparticles in photodynamic therapy: an emerging paradigm. Adv Drug Deliv Rev. 2008;60:1627–1637. doi:10.1016/j.addr.2008.08.003
93. Ding Z, Sigdel K, Yang L, et al. Nanotechnology-based drug delivery systems for enhanced diagnosis and therapy of oral cancer. J Mater Chem B. 2020;8:8781–8793. doi:10.1039/D0TB00957A
94. Simões MCF, Sousa JJS, Pais A. Skin cancer and new treatment perspectives: a review. Cancer Lett. 2015;357:8–42. doi:10.1016/j.canlet.2014.11.001
95. Luo R, Le H, Wu Q, Gong C. Nanoplatform-based in vivo gene delivery systems for cancer therapy. Small. 2024;20:e2312153. doi:10.1002/smll.202312153
96. Walther W, Stein U. Viral vectors for gene transfer: a review of their use in the treatment of human diseases. Drugs. 2000;60:249–271. doi:10.2165/00003495-200060020-00002
97. McCaffrey J, Donnelly RF, McCarthy HO. Microneedles: an innovative platform for gene delivery. Drug Deliv Transl Res. 2015;5:424–437. doi:10.1007/s13346-015-0243-1
98. Zeng L, Gowda BHJ, Ahmed MG, et al. Advancements in nanoparticle-based treatment approaches for skin cancer therapy. mol Cancer. 2023;22:10.
99. Chen MC, Lin ZW, Ling MH. Near-infrared light-activatable microneedle system for treating superficial tumors by combination of chemotherapy and photothermal therapy. ACS Nano. 2016;10:93–101.
100. Dolmans DE, Fukumura D, Jain RK. Photodynamic therapy for cancer. Nat Rev Cancer. 2003;3:380–387. doi:10.1038/nrc1071
101. Kwiatkowski S, Knap B, Przystupski D, et al. Photodynamic therapy - mechanisms, photosensitizers and combinations. Biomed Pharmacother. 2018;106:1098–1107. doi:10.1016/j.biopha.2018.07.049
102. Agostinis P, Berg K, Cengel KA, et al. Photodynamic therapy of cancer: an update. CA Cancer J Clin. 2011;61:250–281. doi:10.3322/caac.20114
103. Cheng H, Zheng RR, Fan GL, et al. Mitochondria and plasma membrane dual-targeted chimeric peptide for single-agent synergistic photodynamic therapy. Biomaterials. 2019;188:1–11. doi:10.1016/j.biomaterials.2018.10.005
104. Lim CK, Heo J, Shin S, et al. Nanophotosensitizers toward advanced photodynamic therapy of Cancer. Cancer Lett. 2013;334:176–187. doi:10.1016/j.canlet.2012.09.012
105. Yoo JO, Ha KS. New insights into the mechanisms for photodynamic therapy-induced cancer cell death. Int Rev Cell mol Biol. 2012;295:139–174.
106. Konan YN, Gurny R, Allémann E. State of the art in the delivery of photosensitizers for photodynamic therapy. J Photochem Photobiol B. 2002;66:89–106. doi:10.1016/S1011-1344(01)00267-6
107. Zhang Y, Wang B, Zhao R, Zhang Q, Kong X. Multifunctional nanoparticles as photosensitizer delivery carriers for enhanced photodynamic cancer therapy. Mater Sci Eng C Mater Biol Appl. 2020;115:111099. doi:10.1016/j.msec.2020.111099
108. Dougherty TJ. Photosensitizers: therapy and detection of malignant tumors. Photochem Photobiol. 1987;45:879–889. doi:10.1111/j.1751-1097.1987.tb07898.x
109. Park JM, Hong KI, Lee H, Jang WD. Bioinspired applications of porphyrin derivatives. Acc Chem Res. 2021;54:2249–2260. doi:10.1021/acs.accounts.1c00114
110. Zhang Y, Lovell JF. Recent applications of phthalocyanines and naphthalocyanines for imaging and therapy. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2017;9. doi:10.1002/wnan.1420
111. Singh J, Hussain Y, Luqman S, Meena A. Purpurin: a natural anthraquinone with multifaceted pharmacological activities. Phytother Res. 2021;35:2418–2428. doi:10.1002/ptr.6965
112. Mokwena MG, Kruger CA, Ivan MT, Heidi A. A review of nanoparticle photosensitizer drug delivery uptake systems for photodynamic treatment of lung cancer. Photodiagnosis Photodyn Ther. 2018;22:147–154. doi:10.1016/j.pdpdt.2018.03.006
113. Lo PC, Rodríguez-Morgade MS, Pandey RK, Ng DKP, Torres T, Dumoulin F. The unique features and promises of phthalocyanines as advanced photosensitisers for photodynamic therapy of cancer. Chem Soc Rev. 2020;49:1041–1056. doi:10.1039/c9cs00129h
114. Whiteside TL. The tumor microenvironment and its role in promoting tumor growth. Oncogene. 2008;27:5904–5912. doi:10.1038/onc.2008.271
115. Sharma A, Arambula JF, Koo S, et al. Hypoxia-targeted drug delivery. Chem Soc Rev. 2019;48:771–813. doi:10.1039/c8cs00304a
116. Lu B, Wang L, Tang H, Cao D. Recent advances in type I organic photosensitizers for efficient photodynamic therapy for overcoming tumor hypoxia. J Mater Chem B. 2023;11:4600–4618. doi:10.1039/D3TB00545C
117. Liu Z, Xue Y, Wu M, Yang G, Lan M, Zhang W. Sensitization of hypoxic tumor to photodynamic therapy via oxygen self-supply of fluorinated photosensitizers. Biomacromolecules. 2019;20:4563–4573. doi:10.1021/acs.biomac.9b01368
118. Shi L, Liu X, Li Y, et al. Living bacteria-based immuno-photodynamic therapy: metabolic labeling of Clostridium butyricum for eradicating malignant melanoma. Adv Sci. 2022;9:e2105807. doi:10.1002/advs.202105807
119. Zhou J, Geng S, Ye W, et al. ROS-boosted photodynamic therapy against metastatic melanoma by inhibiting the activity of antioxidase and oxygen-producing nano-dopants. Pharmacol Res. 2020;158:104885. doi:10.1016/j.phrs.2020.104885
120. Mroz P, Huang YY, Szokalska A, et al. Stable synthetic bacteriochlorins overcome the resistance of melanoma to photodynamic therapy. FASEB J. 2010;24:3160–3170. doi:10.1096/fj.09-152587
121. Urig S, Becker K. On the potential of thioredoxin reductase inhibitors for cancer therapy. Semin Cancer Biol. 2006;16:452–465. doi:10.1016/j.semcancer.2006.09.004
122. Liu Y, Liu Y, Bu W, et al. Hypoxia induced by upconversion-based photodynamic therapy: towards highly effective synergistic bioreductive therapy in tumors. Angew Chem Int Ed Engl. 2015;54:8105–8109. doi:10.1002/anie.201500478
123. Huang J, Li Y, Orza A, et al. Magnetic nanoparticle facilitated drug delivery for cancer therapy with targeted and image-guided approaches. Adv Funct Mater. 2016;26:3818–3836. doi:10.1002/adfm.201504185
124. Kadkhoda J, Tarighatnia A, Nader ND, Aghanejad A. Targeting mitochondria in cancer therapy: insight into photodynamic and photothermal therapies. Life Sci. 2022;307:120898. doi:10.1016/j.lfs.2022.120898
125. Li X, Zhao Y, Zhang T, Xing D. Mitochondria-specific agents for photodynamic cancer therapy: a key determinant to boost the efficacy. Adv Healthc Mater. 2021;10:e2001240. doi:10.1002/adhm.202001240
126. Friehs E, AlSalka Y, Jonczyk R, et al. Toxicity, phototoxicity and biocidal activity of nanoparticles employed in photocatalysis. J Photochem Photobiol C. 2016;29:1–28.
127. Qin Y, Chen LJ, Dong F, et al. Light-controlled generation of singlet oxygen within a discrete dual-stage metallacycle for cancer therapy. J Am Chem Soc. 2019;141:8943–8950. doi:10.1021/jacs.9b02726
128. Wang H, Liu CH, Wang K, et al. Assembling pentatopic terpyridine ligands with three types of coordination moieties into a giant supramolecular hexagonal prism: synthesis, self-assembly, characterization, and antimicrobial study. J Am Chem Soc. 2019;141:16108–16116. doi:10.1021/jacs.9b08484
129. Li C, Tu L, Yang J, et al. Acceptor engineering of metallacycles with high phototoxicity indices for safe and effective photodynamic therapy. Chem Sci. 2023;14:2901–2909. doi:10.1039/D2SC06936A
130. Bazylińska U, Kulbacka J, Schmidt J, Talmon Y, Murgia S. Polymer-free cubosomes for simultaneous bioimaging and photodynamic action of photosensitizers in melanoma skin cancer cells. J Colloid Interface Sci. 2018;522:163–173. doi:10.1016/j.jcis.2018.03.063
131. Monduzzi M, Lampis S, Murgia S, Salis A. From self-assembly fundamental knowledge to nanomedicine developments. Adv Colloid Interface Sci. 2014;205:48–67. doi:10.1016/j.cis.2013.10.009
132. Vanneman M, Dranoff G. Combining immunotherapy and targeted therapies in cancer treatment. Nat Rev Cancer. 2012;12:237–251. doi:10.1038/nrc3237
133. Zhang JY, Gao WD, Lin JY, et al. Nanotechnology-based photo-immunotherapy: a new hope for inhibition of melanoma growth and metastasis. J Drug Target. 2023;31:555–568. doi:10.1080/1061186X.2023.2216402
134. Wang M, Rao J, Wang M, et al. Cancer photo-immunotherapy: from bench to bedside. Theranostics. 2021;11:2218–2231. doi:10.7150/thno.53056
135. Castano AP, Mroz P, Hamblin MR. Photodynamic therapy and anti-tumour immunity. Nat Rev Cancer. 2006;6:535–545. doi:10.1038/nrc1894
136. Cong Z, Zhang L, Ma SQ, Lam KS, Yang FF, Liao YH. Size-transformable hyaluronan stacked self-assembling peptide nanoparticles for improved transcellular tumor penetration and photo-chemo combination therapy. ACS Nano. 2020;14:1958–1970. doi:10.1021/acsnano.9b08434
137. Gotwals P, Cameron S, Cipolletta D, et al. Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer. 2017;17:286–301. doi:10.1038/nrc.2017.17
138. Ioannidis JPA, Kim BYS, Trounson A. How to design preclinical studies in nanomedicine and cell therapy to maximize the prospects of clinical translation. Nat Biomed Eng. 2018;2:797–809. doi:10.1038/s41551-018-0314-y
139. Moschetta M, Trevisani M, Castagnola V, Bramini M. Chapter 19 - nanotechnology-based approaches in glioblastoma treatment: how can the dual blood-brain/tumor barriers be overcome? In: Vitorino C, Balaña C, Cabral C, editors. New Insights Into Glioblastoma. Academic Press; 2023:435–475.
140. Vankayala R, Hwang KC. Near-infrared-light-activatable nanomaterial-mediated phototheranostic nanomedicines: an emerging paradigm for cancer treatment. Adv Mater. 2018;30:e1706320. doi:10.1002/adma.201706320
141. Melamed JR, Edelstein RS, Day ES. Elucidating the fundamental mechanisms of cell death triggered by photothermal therapy. ACS Nano. 2015;9:6–11. doi:10.1021/acsnano.5b00021
142. Hou YJ, Yang XX, Liu RQ, et al. Pathological mechanism of photodynamic therapy and photothermal therapy based on nanoparticles. Int J Nanomed. 2020;15:6827–6838. doi:10.2147/IJN.S269321
143. Gazzi A, Fusco L, Khan A, et al. Photodynamic therapy based on graphene and MXene in cancer theranostics. Front Bioeng Biotechnol. 2019;7:295. doi:10.3389/fbioe.2019.00295
144. Curcio A, Silva AKA, Cabana S, et al. Iron Oxide nanoflowers @ CuS hybrids for cancer tri-therapy: interplay of photothermal therapy, magnetic hyperthermia and photodynamic therapy. Theranostics. 2019;9:1288–1302. doi:10.7150/thno.30238
145. Liang S, Deng X, Chang Y, et al. Intelligent hollow Pt-CuS Janus Architecture for Synergistic Catalysis-Enhanced Sonodynamic and Photothermal Cancer Therapy. Nano Lett. 2019;19:4134–4145. doi:10.1021/acs.nanolett.9b01595
146. Song X, Gong H, Liu T, et al. J-aggregates of organic dye molecules complexed with iron oxide nanoparticles for imaging-guided photothermal therapy under 915-nm light. Small. 2014;10:4362–4370. doi:10.1002/smll.201401025
147. Fang RH, Kroll AV, Gao W, Zhang L. Cell membrane coating nanotechnology. Adv Mater. 2018;30:e1706759. doi:10.1002/adma.201706759
148. Hu Q, Sun W, Qian C, Wang C, Bomba HN, Gu Z. Anticancer platelet-mimicking nanovehicles. Adv Mater. 2015;27:7043–7050. doi:10.1002/adma.201503323
149. Sun H, Su J, Meng Q, et al. Cancer-cell-biomimetic nanoparticles for targeted therapy of homotypic tumors. Adv Mater. 2016;28:9581–9588. doi:10.1002/adma.201602173
150. Jiang Q, Luo Z, Men Y, et al. Red blood cell membrane-camouflaged melanin nanoparticles for enhanced photothermal therapy. Biomaterials. 2017;143:29–45. doi:10.1016/j.biomaterials.2017.07.027
151. Wang D, Dong H, Li M, et al. Erythrocyte-cancer hybrid membrane camouflaged hollow copper sulfide nanoparticles for prolonged circulation life and homotypic-targeting photothermal/chemotherapy of melanoma. ACS Nano. 2018;12:5241–5252. doi:10.1021/acsnano.7b08355
152. Li D, Hu D, Xu H, et al. Progress and perspective of microneedle system for anti-cancer drug delivery. Biomaterials. 2021;264:120410. doi:10.1016/j.biomaterials.2020.120410
153. Peng LH, Wang MZ, Chu Y, et al. Engineering bacterial outer membrane vesicles as transdermal nanoplatforms for photo-TRAIL-programmed therapy against melanoma. Sci Adv. 2020;6:eaba2735. doi:10.1126/sciadv.aba2735
154. Shi J, Kantoff PW, Wooster R, Farokhzad OC. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17:20–37. doi:10.1038/nrc.2016.108
155. Jung HS, Kong WH, Sung DK, et al. Nanographene oxide-hyaluronic acid conjugate for photothermal ablation therapy of skin cancer. ACS Nano. 2014;8:260–268. doi:10.1021/nn405383a
156. Wang S, Zheng H, Zhou L, et al. Injectable redox and light responsive MnO(2) hybrid hydrogel for simultaneous melanoma therapy and multidrug-resistant bacteria-infected wound healing. Biomaterials. 2020;260:120314. doi:10.1016/j.biomaterials.2020.120314
157. Xi Y, Ge J, Wang M, et al. Bioactive anti-inflammatory, antibacterial, antioxidative silicon-based nanofibrous dressing enables cutaneous tumor photothermo-chemo therapy and infection-induced wound healing. ACS Nano. 2020;14:2904–2916. doi:10.1021/acsnano.9b07173
158. Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 2014;6:265sr6. doi:10.1126/scitranslmed.3009337
159. Hao Y, Dong Z, Chen M, et al. Near-infrared light and glucose dual-responsive cascading hydroxyl radical generation for in situ gelation and effective breast cancer treatment. Biomaterials. 2020;228:119568. doi:10.1016/j.biomaterials.2019.119568
160. Manna B, Cooper JS. Radiation-Induced Skin Ulcer. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC; 2024.
161. Cheng Z, Al Zaki A, Hui JZ, Muzykantov VR, Tsourkas A. Multifunctional nanoparticles: cost versus benefit of adding targeting and imaging capabilities. Science. 2012;338:903–910. doi:10.1126/science.1226338
162. Zhan X, Teng W, Sun K, et al. CD47-mediated DTIC-loaded chitosan oligosaccharide-grafted nGO for synergistic chemo-photothermal therapy against malignant melanoma. Mater Sci Eng C Mater Biol Appl. 2021;123:112014. doi:10.1016/j.msec.2021.112014
163. Xu W, Qian J, Hou G, et al. PEGylated hydrazided gold nanorods for pH-triggered chemo/photodynamic/photothermal triple therapy of breast cancer. Acta Biomater. 2018;82:171–183. doi:10.1016/j.actbio.2018.10.019
164. Duan X, Chan C, Guo N, Han W, Weichselbaum RR, Lin W. Photodynamic therapy mediated by nontoxic core-shell nanoparticles synergizes with immune checkpoint blockade to elicit antitumor immunity and antimetastatic effect on breast cancer. J Am Chem Soc. 2016;138:16686–16695. doi:10.1021/jacs.6b09538
165. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252–264. doi:10.1038/nrc3239
166. Sharma P, Allison JP. The future of immune checkpoint therapy. Science. 2015;348:56–61. doi:10.1126/science.aaa8172
167. Zhou F, Wu S, Song S, Chen WR, Resasco DE, Xing D. Antitumor immunologically modified carbon nanotubes for photothermal therapy. Biomaterials. 2012;33:3235–3242. doi:10.1016/j.biomaterials.2011.12.029
168. Zhou B, Song J, Wang M, et al. BSA-bioinspired gold nanorods loaded with immunoadjuvant for the treatment of melanoma by combined photothermal therapy and immunotherapy. Nanoscale. 2018;10:21640–21647. doi:10.1039/C8NR05323E
169. Bombelli FB, Webster CA, Moncrieff M, Sherwood V. The scope of nanoparticle therapies for future metastatic melanoma treatment. Lancet Oncol. 2014;15:e22–32. doi:10.1016/S1470-2045(13)70333-4
170. Ugurel S, Paschen A, Becker JC. Dacarbazine in melanoma: from a chemotherapeutic drug to an immunomodulating agent. J Invest Dermatol. 2013;133:289–292. doi:10.1038/jid.2012.341
171. Jiang BP, Zhang L, Guo XL, et al. Poly(N-phenylglycine)-based nanoparticles as highly effective and targeted near-infrared photothermal therapy/photodynamic therapeutic agents for malignant melanoma. Small. 2017;13. doi:10.1002/smll.201602496
172. He J, Ouyang X, Xiao F, Liu N, Wen L. Imaging-guided photoacoustic immunotherapy based on the polydopamine-functionalized black phosphorus nanocomposites. ACS Appl Mater Interfaces. 2023;15:54322–54334. doi:10.1021/acsami.3c13998
173. Liong M, Lu J, Kovochich M, et al. Multifunctional inorganic nanoparticles for imaging, targeting, and drug delivery. ACS Nano. 2008;2:889–896. doi:10.1021/nn800072t
174. Wicki A, Witzigmann D, Balasubramanian V, Huwyler J. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release. 2015;200:138–157. doi:10.1016/j.jconrel.2014.12.030
175. Zhu H, Xie C, Chen P, Pu K. Organic nanotheranostics for photoacoustic imaging-guided phototherapy. Curr Med Chem. 2019;26:1389–1405.
176. Rich LJ, Seshadri M. Photoacoustic imaging of vascular hemodynamics: validation with blood oxygenation level-dependent MR imaging. Radiology. 2015;275:110–118. doi:10.1148/radiol.14140654
177. Ntziachristos V, Razansky D. Molecular imaging by means of multispectral optoacoustic tomography (MSOT). Chem Rev. 2010;110:2783–2794. doi:10.1021/cr9002566
178. Lemaster JE, Jokerst JV. What is new in nanoparticle-based photoacoustic imaging? Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2017;9. doi:10.1002/wnan.1404
179. Attia ABE, Balasundaram G, Moothanchery M, et al. A review of clinical photoacoustic imaging: current and future trends. Photoacoustics. 2019;16:100144. doi:10.1016/j.pacs.2019.100144
180. Wang LV, Hu S. Photoacoustic tomography: in vivo imaging from organelles to organs. Science. 2012;335:1458–1462. doi:10.1126/science.1216210
181. Wang Z, Zhan M, Hu X. Pulsed laser excited photoacoustic effect for disease diagnosis and therapy. Chemistry. 2022;28:e202200042. doi:10.1002/chem.202200042
182. Jeon S, Choi W, Park B, Kim C. A deep learning-based model that reduces speed of sound aberrations for improved in vivo photoacoustic imaging. IEEE Trans Image Process. 2021;30:8773–8784. doi:10.1109/TIP.2021.3120053
183. Kim J, Kim JY, Jeon S, Baik JW, Cho SH, Kim C. Super-resolution localization photoacoustic microscopy using intrinsic red blood cells as contrast absorbers. Light Sci Appl. 2019;8:103. doi:10.1038/s41377-019-0220-4
184. Wang LV, Yao J. A practical guide to photoacoustic tomography in the life sciences. Nat Methods. 2016;13:627–638. doi:10.1038/nmeth.3925
185. Haedicke K, Agemy L, Omar M, et al. High-resolution optoacoustic imaging of tissue responses to vascular-targeted therapies. Nat Biomed Eng. 2020;4:286–297. doi:10.1038/s41551-020-0527-8
186. Zhong J, Wen L, Yang S, Xiang L, Chen Q, Xing D. Imaging-guided high-efficient photoacoustic tumor therapy with targeting gold nanorods. Nanomedicine. 2015;11:1499–1509. doi:10.1016/j.nano.2015.04.002
187. Kang B, Yu D, Dai Y, Chang S, Chen D, Ding Y. Cancer-cell targeting and photoacoustic therapy using carbon nanotubes as “bomb” agents. Small. 2009;5:1292–1301. doi:10.1002/smll.200801820
188. Zhou F, Wu S, Yuan Y, Chen WR, Xing D. Mitochondria-targeting photoacoustic therapy using single-walled carbon nanotubes. Small. 2012;8:1543–1550. doi:10.1002/smll.201101892
189. Hu L, Cao Z, Ma L, et al. The potentiated checkpoint blockade immunotherapy by ROS-responsive nanocarrier-mediated cascade chemo-photodynamic therapy. Biomaterials. 2019;223:119469. doi:10.1016/j.biomaterials.2019.119469
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.