")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Immediate Treatment of Seizure Clusters: A Conceptual Roadmap to Expedited Seizure Management
Authors Wheless JW, Becker DA, Benbadis SR, Puri V, Datta P, Clarke D, Panjeti-Moore D, Carrazana E , Rabinowicz AL
Received 13 August 2024
Accepted for publication 5 November 2024
Published 22 November 2024 Volume 2024:20 Pages 2255—2265
DOI https://doi.org/10.2147/NDT.S481758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
James W Wheless,1 Danielle A Becker,2 Selim R Benbadis,3 Vinay Puri,4 Proleta Datta,5 Dave Clarke,6 Deepa Panjeti-Moore,7 Enrique Carrazana,8,9 Adrian L Rabinowicz8,10
1Le Bonheur Children’s Hospital, University of Tennessee Health Science Center, Memphis, TN, USA; 2Department of Neurology, Ohio State University Wexner Medical Center, Columbus, OH, USA; 3Comprehensive Epilepsy Program, University of South Florida & Tampa General Hospital, Tampa, FL, USA; 4Norton Children’s Neuroscience Institute, Affiliated with University of Louisville, Louisville, KY, USA; 5Department of Neurology, School of Medicine, Oregon Health & Science University, Portland, OR, USA; 6Dell Children’s Comprehensive Pediatric Epilepsy Center, University of Texas at Austin, Austin, TX, USA; 7Epilepsy Program; Neurology Consultants of Dallas, Dallas, TX, USA; 8Clinical Development and Medical Affairs, Neurelis, Inc., San Diego, CA, USA; 9Department of Family Medicine, John A. Burns School of Medicine, University of Hawaii, Honolulu, HI, USA; 10Center for Molecular Biology and Biotechnology, Charles E. Schmidt College of Science, Florida Atlantic University, Boca Raton, FL, USA
Correspondence: James W Wheless, Le Bonheur Children’s Hospital, University of Tennessee Health Science Center, 777 Washington Avenue, Suite 335, Memphis, TN, 38105, USA, Tel +1 901.287.5207, Fax +1 901.287.5325, Email [email protected]
Abstract: Some patients with epilepsy continue to have seizures despite daily treatment with antiseizure medications. This includes seizure clusters (also known as acute repetitive seizures), which are an increase in seizure frequency that is different from the usual seizure pattern for that patient. In the literature, the term “rescue” is used for pharmacologic treatment for seizure clusters, but clarity regarding timing or whether a caregiver or patient should wait until a moment of life-threatening urgency before administering the medication is lacking. Additionally, the concept of waiting 5 minutes to identify and initiate treatment of status epilepticus has been carried over to the treatment of seizure clusters, as well as the idea of waiting owing to safety concerns, without reevaluation in the context of the reported safety profiles for currently available as-needed therapies when administered as prescribed. Delaying treatment of seizure clusters may have negative outcomes, including injury, emergency room use, hospitalization, and progression to status epilepticus. Additionally, increased time for administration of benzodiazepines, the cornerstone therapies for seizure clusters, may lower the potency and effectiveness once administration takes place, because of physiologic changes. Thus, clarifying the importance of timing in the treatment terminology may be of benefit in the acute context. The term “immediate-use seizure medication” (ISM), meaning treatment that is administered as quickly as possible once a seizure cluster is recognized, may help to clarify the timing of as-needed treatment. This review examines the recognition and definitions of seizure clusters, the physiologic rationale for ISM for seizure clusters, and the effectiveness and safety of early treatment. Remaining knowledge gaps are also discussed. The findings of this review suggest that it may be time to revisit the terminology of “rescue”, which implies waiting to administer treatment for seizure clusters, as doing so is not supported by pathophysiologic, effectiveness, or safety data.
Plain Language Summary: Some people with epilepsy have seizures even if they take daily medication for their seizures. If they have more seizures than usual in a day, this may be called a seizure cluster. Drugs used to treat clusters are often said to be “rescue” medicines. But the word “rescue” may imply that the medication should only be administered when serious danger is present. Additionally, possibly because of previous instructions, people may think they have to wait to see if the seizure lasts more than 5 minutes to give the medicine, or they may be concerned about how safe the medicine will be if they give it. This older approach needs to be revisited and replaced. Waiting to give medicine could make it more likely that a person could get hurt or require a hospital or emergency room visit or their seizure condition could worsen. Waiting also may allow for changes in the body that may make a medicine less effective once it is given. Because of this, it may be better to say these medicines are for “immediate use” rather than for “rescue”. That way, the people giving the medicine know that they should give it as soon as they see the patient needs it. This paper discusses how seizure clusters are described and what can happen if someone waits to give medicine versus giving it right away. The paper shows that waiting may not be needed.
Keywords: benzodiazepine, early intervention, epilepsy, rescue therapy
Introduction
Epilepsy patients are primarily treated with daily antiseizure medications (ASMs) for controlling seizures; however, some patients continue to have seizures despite taking ASMs.1 Such drug-resistant patients may have a usual pattern to their seizures and also may experience a variation to that pattern, such as when the frequency of the seizures may change or severity may increase. An increase in seizure frequency within a defined time period (eg, 24 h) may be called a seizure cluster or acute repetitive seizures.1,2 In the US, seizure clusters have been designated as an orphan indication.3,4 In other geographic regions, such as the EU, regulatory bodies do not have an indication for seizure clusters but have somewhat similar classifications for prolonged acute convulsive seizures5 and epileptic and febrile convulsions.6 This review will use the available illustrative treatment timing data of seizure cluster medications approved by the US Food and Drug Administration (FDA). The prescribing information for the approved benzodiazepines, 3 diazepam formulations and 1 midazolam formulation, do not specify a delay between recognition and usage of therapies upon recognition of seizure clusters.2,7–9
When seizure clusters have occurred previously, caregivers may recognize the patient’s specific presentation as distinguishable from the patient’s other seizures.10 If untreated, such events can increase the risk of negative patient outcomes such as injury, emergency room use, hospitalization,11,12 and progression to status epilepticus,13 which is associated with morbidity and mortality.14 Recent data support prompt treatment for seizure clusters.15
Traditionally, the term “rescue” has been used to refer to pharmacologic treatment for acute management of this type of seizure (ie, seizure cluster),16–18 and drug formulations with benzodiazepines such as diazepam and midazolam have been the cornerstone for such treatment in the community.16 A 2021 publication from a group of epilepsy experts and stakeholders examined terminology associated with seizure clusters with the goal of reaching consensus for a common language.1 That publication noted that treatments used to abort seizure clusters are typically called rescue medicines/therapies and “are given at a specified time in relation to when the change in seizure frequency happens”;1 however, the specific meaning of the word “rescue” and timing of treatment administration was not discussed. Although “rescue” is widely used in this context, lack of clarification is also persistent. The reason for the treatment (to stop seizures) is addressed by this term; however, the current use of “rescue” does not clearly address when administration should occur and thus could lead to misinterpretation. For example, an observer would not wait 5 minutes when someone is drowning; he or she would act immediately to attempt a rescue. Additionally, “rescue” medication for acute asthma exacerbations (ie, with an inhaler) or anaphylaxis (ie, by epinephrine injection) may be associated with administration at moments of life-threatening urgency.
Delay in administering treatment for acute episodes such as seizure clusters may lead to ongoing and prolonged seizures with a risk of increased morbidity and mortality and potentially lower potency of benzodiazepines once administered.19 Thus, clarifying the importance of timing in the treatment terminology may be of benefit to eliminate the suggestion of waiting to administer in the acute context. With newer, easier to administer as-needed formulations now available, it may be the time for new guidance in which the adjective “rescue treatment” transitions into the more direct term “immediate-use seizure medication” (ISM), meaning treatment that is administered as quickly as possible once the patient’s stereotypic seizure cluster pattern is recognized (Figure 1). One potential timing option is for caregivers to go to get the ISM treatment and administer it if the patient is still seizing when they return.
 |
Figure 1 A proposed roadmap for treatment. Initial steps are shown in green boxes; secondary steps, if needed, shown in yellow boxes; emergency steps, if needed, shown in red boxes. |
Barriers to immediate use exist, such as timing limitations due to the route of drug administration, potentially outdated definitions of when to intervene, and excessive concerns about long-lasting adverse events. Preparation and administration for the as-needed medication with the longest FDA approval, diazepam rectal gel, requires timing for positioning and undressing the patient, as well as for undertaking several steps to complete administration.7,20 Additionally, caregivers and patients may be reluctant to use rectal administration, causing delay in administration.15 Regarding when to intervene, no clear timing has been set for seizure clusters; however, the historical use of 5 minutes to define T1 (time regarded as defining continuous seizures) for status epilepticus14,21 has been applied to fill this gap. Also, delays may have occurred because of a perception of the potential for adverse events, such as long-term somnolence or respiratory depression.
This paper examines the hypothesis that ISM may be beneficial for fast resolution of a seizure cluster and to reduce the risk of negative outcomes; thus, caregivers and patients should not wait to treat a recognized seizure cluster. This narrative review provides a roadmap for understanding the concept and importance of immediate-use treatment for seizure clusters across available therapies and is illustrated with examples from the available timing data in a noncomparative, nonexclusive manner. Comprehensive reviews and papers providing details on the available therapies for seizure clusters and their efficacy and safety can be found elsewhere.16,22–25
Recognition and Definition of Seizure Clusters
Currently, no consensus definition for a seizure cluster exists in the literature, and the literature is rife with multiple ways in which seizure cluster is defined.1 Recently, an expert working group recommended defining a seizure cluster as “an abnormal increase in seizure frequency compared with the individual patient’s usual seizure pattern”.26 This proposed definition does not include a specific number of seizures (eg, ≥2) and a period of time (eg, 24 h), which have been components of previous definitions. This expert group recommended treating prolonged seizures and seizure clusters as soon as they are recognized.26
Historically, for administration of diazepam rectal gel, it was shown that caregivers could be taught how to recognize the onset of acute repetitive seizures, and the stereotypic presentation was often immediately recognized.27 To recognize a seizure cluster, family members used such variables as number, type, and severity of the seizures; patient behavior changes; and time of day of the seizures.28 In 1997, diazepam rectal gel was the first ISM approved by the FDA for treatment of seizure clusters and was the only approved treatment for >20 years.16 However, due to the limitations associated with the route of administration of diazepam rectal gel, development of intranasal formulations was pursued.16
For the clinical trials of midazolam nasal spray and diazepam nasal spray, which were approved by the FDA in 2019 and 2020, respectively, definitions of seizure clusters were used that incorporated a number of seizures within a limited time interval. The Phase 3, long-term, open-label, repeat-dose safety study evaluating diazepam nasal spray enrolled patients with frequent seizure clusters; seizure timing and drug administration were recorded in a patient diary.29 The empirical definition of seizure clusters for the study was ≥2 seizures in 24 hours, which was used to assess the proportion of seizure clusters for which second doses of diazepam nasal spray were used, as a proxy for effectiveness.30
In the Acute Rescue Therapy in Epilepsy With Midazolam Intranasal Spray 1 (ARTEMIS-1) trial and an open-label extension study, seizure clusters were defined as having ≥2 seizures (focal or generalized) lasting ≥10 minutes.31 Additionally, seizure clusters had a pattern that was recognizably different from the patient’s usual seizure pattern and with another seizure occurring in <6 hours.31,32
Although oral ASMs (eg, lorazepam, clonazepam) have been prescribed off-label as acute therapy for seizure clusters in adults,33 oral administration has potential shortcomings. These include aspiration risk, inability to swallow, delayed absorption, and delayed efficacy.34–36
The current prescribing information for the FDA-approved as-needed seizure medications indicated for patients with seizure clusters does not specify the number of seizures or timing limit for seizure clusters but rather patient-specific “stereotypic presentation”.2,7–9 The FDA indication specifies acute treatment of intermittent stereotypic episodes of frequent seizures that are distinct from a patient’s usual seizure pattern.2,7–9 The FDA-approved drugs for seizure clusters in both pediatric patients and adults are rectal diazepam gel for patients aged ≥2 years,7 diazepam nasal spray for patients aged ≥6 years,2 and midazolam nasal spray for patients aged ≥12 years9 (Table 1). Recently, the FDA approved an additional medication for only a small range of pediatric patients (ie, diazepam buccal film for ages 2–5 y).8 In the EU, buccal midazolam is approved for the treatment of prolonged acute convulsive seizures, primarily in pediatric patients aged 3 months to <18 years,5 a rectal diazepam formulation in solution is approved for epileptic and febrile convulsions in patients aged ≥1 year,6 and a nasal midazolam formulation is authorized for treatment of prolonged acute convulsive seizures but is not currently marketed.37
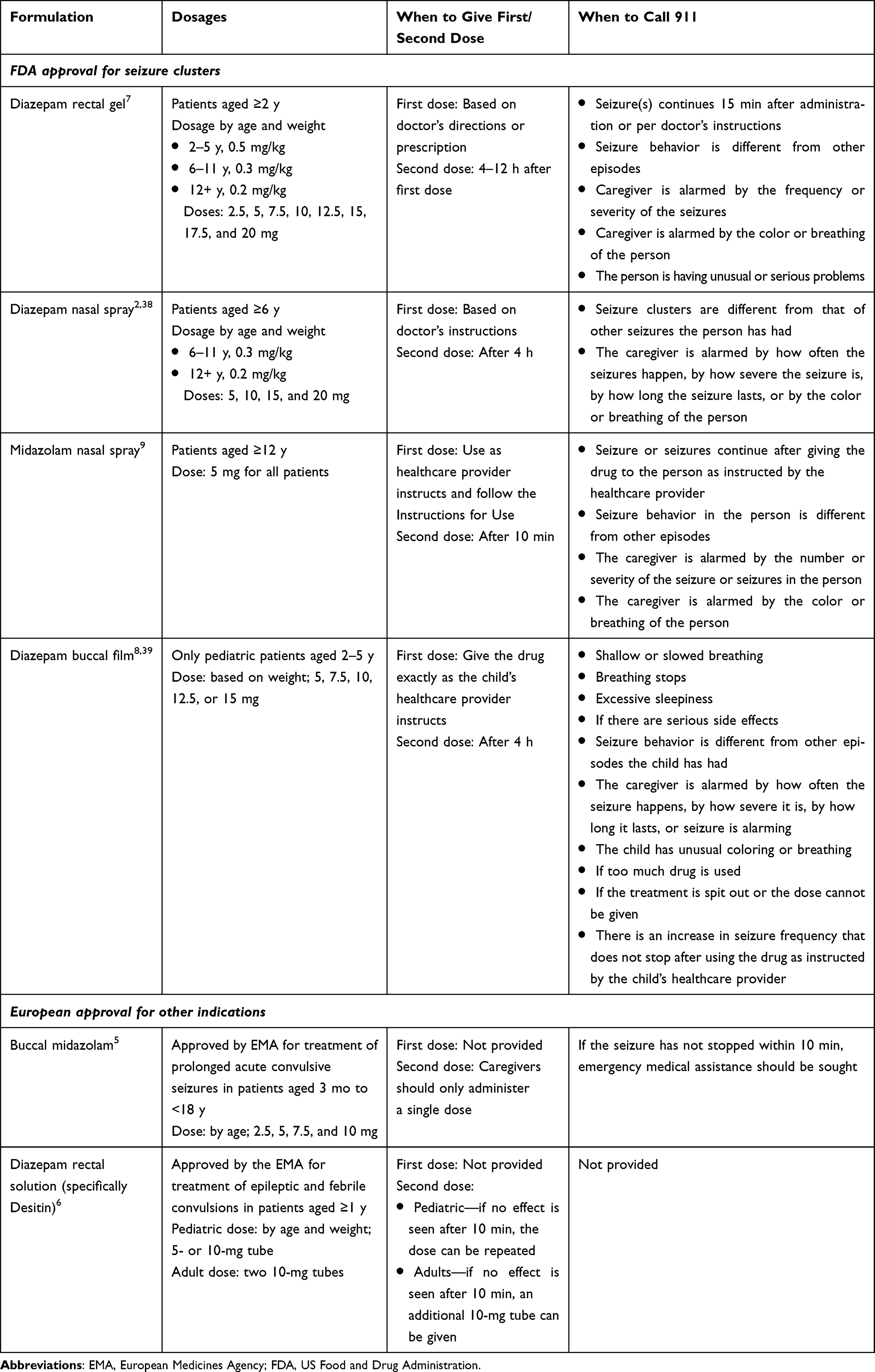 |
Table 1 Currently Approved Immediate-Use Seizure Medications |
The existence of multiple definitions of seizure clusters without a clear consensus may lead to ambiguity about when a seizure cluster is occurring and when treatment should be initiated. Thus, an acute seizure action plan developed with the patient’s physician can provide patient-specific guidance that may help with identification and clarification regarding what to do when a seizure cluster occurs.40 Such a plan should be brief and easy to use with simple wording and images. The plan should include individually customized content about what to look for in the seizures associated with a seizure cluster and when and how to treat a seizure cluster once recognized. Such a plan could be easily used by school personnel, babysitters, roommates, and coworkers, as well as traditional caregivers, family, and friends.40 In a recent study of action plan use in an adult epilepsy center, 83% of patients who reported they did not have the knowledge to recognize seizure emergencies before using the action plan reported an improvement after using the plan.41
Flexible, individualized seizure cluster definitions (rather than one all-encompassing definition) allow for customized variations in descriptions of the number of seizures and duration that define a seizure cluster for that patient, which may enhance a caregiver’s ability to recognize a seizure cluster quickly.42 A study comparing traditional definitions with a computerized algorithm using individualized patient-specific definitions (taking into account baseline seizure frequency and natural variation) found that traditional definitions were more likely to miss or misidentify seizure clusters.42 This suggests that customized definitions may be more sensitive for identifying seizure clusters.
As there is such variability to the definitions of seizure clusters, the specific details of a patient’s seizure-cluster experience could be used to determine the best immediate-use treatment approach. Consideration of such patient variables as frequency of and severity of seizure clusters supports flexibility in the determination of an appropriate individualized treatment plan.
Pathophysiologic Rationale for Immediate Use
Negative pathophysiologic outcomes can occur when treatment of seizure clusters is delayed. Over time, an untreated seizure cluster will become less responsive to benzodiazepines.43 Benzodiazepines bind to gamma-aminobutyric acid (GABA) A (GABAA) receptors and increase the affinity of those receptors for GABA.44 The ability of benzodiazepines to act on receptors in cell membranes contributes to their effectiveness early in the course of a seizure episode by modulating receptor activity. However, with prolonged seizures, benzodiazepine effectiveness may decrease owing to internalization of GABAA receptors over time.45 In addition to the loss of GABAA receptors, seizures over time lead to N-Methyl-
Additionally, repeated brief seizures evoked in animal models have shown an association with GABAergic interneuron cell loss and reduction in seizure inhibition processes.46 This may contribute to self-sustaining seizures, increased neuronal excitability, and the development of intractable epilepsy.45,46
Acute seizures that continue untreated are a risk factor for injuries and a worsening condition.47,48 The long-standing theory of “seizures beget seizures” is sometimes quoted in discussions of the pathophysiology of epilepsy, suggesting that seizures affect the brain in ways that contribute to disease progression and the likelihood of future seizures; this continues to be an area of investigation that should not be generalized without being taken in the context of other factors associated with seizure-related risks.49 The repetitive and prolonged seizures associated with status epilepticus have been associated with neurologic damage to the brain that has been demonstrated in animal models,50,51 and such damage potentially may occur with shorter seizures that are not treated promptly. However, epilepsy is a condition with variations in presentation and progression among patients, so the likelihood of physiologic change should not be oversimplified.
Although it has been found that many single seizures are self-limiting and may terminate within 2 minutes of initiation,52 immediate treatment can still be beneficial. Treating immediately, once a seizure cluster is recognized, may have the potential to limit the risk of morbidity (eg, injury) and mortality and possibly post-ictal recovery time.19,48,53–55 Accidents and physical injuries may be associated with acute seizures, including head trauma, fractures, joint dislocations or sprains, and soft tissue injuries.48 Some injuries may lead to hospitalization.48
Effectiveness of Early Treatment
Prompt treatment of seizure clusters has been shown to be feasible for caregivers and patients and to lead to faster seizure termination. In a proof-of-concept study, an immediate treatment paradigm was used to assess an inhaled formulation of alprazolam, a benzodiazepine for the treatment of anxiety disorders, as a treatment to suppress epileptiform activity in patients with epilepsy and photosensitive seizures; alprazolam is being investigated as a potential acute treatment option for seizures.56 In the small group of patients previously diagnosed with epilepsy (n = 5), all doses of alprazolam (0.5, 1.0, and 2.0 mg) showed effectiveness at 2 minutes.56 Immediate use once the seizure type was identified was also included in the protocol for a phase 2b study of alprazolam for rapid seizure termination57 and the phase 3 study of midazolam nasal spray.58
In another illustrative example of timing data, early effectiveness was specifically investigated with an FDA-approved medication for seizure clusters in an exploratory post hoc analysis that was performed using timing data for treated seizure clusters of patients from the phase 3, open-label, repeat-dose safety study of diazepam nasal spray for acute treatment of seizure clusters.15 Doses were based on age and weight; if needed, second doses could be administered 4–12 hours after the initial dose, and investigators could adjust dosing if needed.29 During the study, details on seizure timing and drug administration were reported in a patient diary.29 For the post hoc analysis, mean times from the seizure prompting treatment to drug administration and from drug administration to seizure termination were calculated.15 Temporal patterns were expressed as descriptive statistics.15
The median time to administration was 2 minutes after the start of the seizure cluster, and the majority of administrations occurred in 0–5 minutes (2169/3225 [67.3%]).15 Of the doses administered within 5 minutes of the start of the seizure cluster, nearly two-thirds (65.2%) were administered ≤1 minute (Neurelis, data on file). The median time from dose to seizure termination was 3 minutes, and the mean total seizure duration was 7 minutes. For seizure clusters treated in <5 minutes, the median time to administration was 1 minute, the time from administration to termination was 2 minutes, and mean duration of seizure was 4 minutes. For seizure clusters treated in the 5–15 minutes after the start of seizure cluster, the median time to administration was 6 minutes, median time from dose to seizure termination was 7 minutes, and the mean duration of seizure was 15 minutes.15
When a sensitivity analysis removing seizure durations of 0 to 2 minutes (729/3225 [22.6%]) was performed to reduce potential confounding by seizures that may have been self-limited, the results were comparable.15 Again, the majority of administrations were in <5 minutes (1440/2495 [57.7%]) and time to seizure termination as well seizure duration were shorter with earlier intervention.15 That the results were similar shows that self-terminating seizures did not skew the results, which is supportive of the ability of caregivers to accurately identify seizure clusters.
Implications Beyond “Rescue”
Additionally, for the diazepam nasal spray safety study, the proportion of seizure clusters during which a second dose was administered within a 24-hour period was used as a proxy for effectiveness.29 Of a total of 3853 seizure clusters, second doses were administered for 485 (12.6%).29 Exposure to diazepam nasal spray was also evaluated using a population pharmacokinetic (PK) model developed with data from three Phase 1 studies (n = 126 [healthy volunteers, n = 78; patients with epilepsy, n = 48]).59 The model evaluated the effect of the dosing interval on diazepam exposure and found that dosing intervals from 1 minute to 4 hours had comparable exposures as later doses without affecting safety.59
Twenty-seven patients reported on an exit survey that they had self-administered diazepam nasal spray at least once during the safety study.54 When asked when they primarily administered diazepam nasal spray, 48% of the patients in this group responded that they did so “at the first signs that a seizure may be coming”.54 Studies of alprazolam for rapid seizure termination and diazepam buccal film also have looked at self-administration.57,60
An additional sign of effectiveness among patients in the diazepam nasal spray safety study has been the increase in interval between treated seizure clusters (SEIVAL) over time in both the overall population and specific subgroups. A post hoc analysis found that the mean duration between seizure clusters with as-needed use over a 1-year period was associated with doubling in time from the first 90-day period to the last 90-day period (day 1–day 360), a significant increase (P≤0.001 by t test).61 A consistent pattern of increasing SEIVAL over time was seen in patient age subgroups, patients with and without changes in concomitant ASMs,61 by patient sex,62 and in patients who self-administered diazepam nasal spray.63
Safety and Tolerability Profile Supports Immediate Use
There are class warnings regarding concomitant use of opioids and benzodiazepines for all of the FDA-approved therapies for adults and pediatric patients with seizure clusters.2,7–9 These approved benzodiazepines have demonstrated favorable safety profiles in clinical studies. For rectal diazepam gel and diazepam nasal spray and for midazolam nasal spray during double-blind treatment, no reports of respiratory depression were attributable to the study drugs in the respective long-term studies.29,32,64 In the test-dose phase of the midazolam nasal spray study, <1% of patients had clinically meaningful treatment-related respiratory depression,32 and there also was 1 report of respiratory failure that was possibly treatment related in the phase 3, open-label safety study of diazepam buccal film (n = 118).60
In the diazepam nasal spray long-term safety study, those patients receiving second doses ≤4 hours after the initial dose for a seizure cluster (152 of 485 second doses [31.3%]) had generally similar rates of adverse events to the overall study, with slightly higher rates of treatment-related adverse events that were related to treatment administration (eg, epistaxis and nasal discomfort [7.9% of the patients each] in the second doses in ≤4 h group vs 1.8% and 6.1%, respectively, in the overall safety population]).59
Somnolence is a common concern for treatment with benzodiazepines; however, it may be difficult to distinguish between somnolence related to medication and the patient being in a post-ictal state.64 In the open-label diazepam rectal gel study (n = 149), somnolence was the most frequently reported adverse event (17% of the patients; considered treatment related in 9%).64 In the open-label diazepam nasal spray study (n = 163), somnolence was reported in 6.7% of patients, with 1.8% of patients having treatment-related somnolence.29 In the open-label midazolam nasal spray study (n = 161), somnolence was reported in 9.3% of patients.31 A discussion between the clinician and patient on this consideration should also be balanced with information on post-treatment recovery times.
Among patients responding to a question on the diazepam nasal spray safety study exit survey about how quickly they returned to their usual selves (n = 64), 59.4% reported the time to be within an hour of their most recent administration of diazepam nasal spray.54 Among caregivers (n = 80) who administered the drug to patients in the study, 8.8% said they did so at the first sign of a seizure, while the majority said they did so during a seizure (81.4%). Of these caregivers (n = 79), 59.5% said they could return to their daily activities within an hour.54 For midazolam nasal spray, return to baseline functionality within 24 hours after treatment of a seizure cluster episode with 1 or 2 doses was seen in 97.2% (1167/1201) and 94.2% (749/795) patients, respectively, in an open-label extension trial (n = 161), with estimated return to baseline median times of 1.2 and 1.3 hours, respectively.65
Knowledge Gaps
Although the findings from this review appear to support the hypothesis that immediate treatment is beneficial for fast resolution of a seizure cluster, additional knowledge gaps will need to be addressed to further clarify this. It would be helpful to know the effect of earlier treatment on cognitive function and post-ictal recovery. Additionally, more data should be obtained on treatment across the spectrum of different lengths of seizures, the impact of consistent early treatment on outcomes, time to use of second doses, and observed change in frequency of prolonged seizures with treatment.
Conclusion
The findings of this review suggest that it may be time to reconsider the use of the term “rescue” for medication used as needed to shorten or abort seizure clusters, as this term may imply waiting to administer treatment, which is not supported by current data. The term “immediate use” may more appropriately address the guidance to treat seizure clusters when first recognized. Immediate use is consistent with the prescribing information indication for FDA-approved medications and similar to the terminology used for treating acute asthma attacks. Such treatment may help to lower the risk of morbidity and mortality associated with seizure clusters.
Acknowledgments
Medical writing support was provided by Laura J. Herold, MA, CMPP, from The Curry Rockefeller Group, LLC, a Citrus Health Group company (Chicago, Illinois) and was funded by Neurelis, Inc. (San Diego, California).
Funding
This manuscript was funded by Neurelis, Inc. (San Diego, California, USA).
Disclosure
Dr Wheless has served as an advisor or consultant for CombiMatrix; Eisai Inc.; UCB; Jazz Pharmaceuticals; Neurelis, Inc.; Upsher-Smith Laboratories, Inc.; NobelPharma; Stoke; Praxis; and Azurity. He has served as a speaker or a member of a speakers bureau for Cyberonics, Inc.; Neurelis, Inc.; Jazz Pharmaceuticals; and SKLSI; and has received grants for clinical research from Jazz Pharmaceuticals; Neurelis, Inc.; NeuroPace, Inc.; UCB; Praxis; Stoke; LivaNova; and Azurity. Dr Becker is a consultant/speaker for Neurelis, Inc.; SK Life Science; Science; Jazz Pharmaceuticals; Neuropace, Inc.; and LivaNova and received research support from SK Life Science. Dr Benbadis is a consultant or member of an advisory board for Eisai Inc.; Jazz Pharmaceuticals; Neurelis, Inc.; SK Life Science; Sunovion; Takeda; and UCB. He is a member of the speakers bureau for Catalyst; Eisai Inc.; Jazz Pharmaceuticals; Neurelis, Inc.; SK Life Science; Sunovion; and UCB. In addition, he reports grants from Longboard, Marinus, Takeda. Dr Puri is a consultant for Eisai Inc. and a speaker and consultant for Neurelis, Inc. Dr Datta has received research support from a grant funded by LivaNova. Dr Clarke is a consultant for Neurelis, Inc. Dr Panjeti-Moore is a speaker for SK Life Science and Neurelis, Inc. Dr Carrazana is an employee of and has received stock and stock options from Neurelis, Inc. Dr Rabinowicz is an employee of and received stock options from Neurelis, Inc. The authors report no other conflicts of interest in this work.
References
1. Buchhalter J, Shafer PO, Buelow JM, et al. Preferred practices for rescue treatment of seizure clusters: a consensus-driven, multi-stakeholder approach. Epilepsy Behav. 2021;117:107836. doi:10.1016/j.yebeh.2021.107836
2. VALTOCO® (Diazepam Nasal Spray). prescribing information. https://valtoco.com/VALTOCO_Prescribing_Information.pdf.
3. US Food and Drug Administration. Orphan indications: diazepam (intranasal). Available from: https://www.accessdata.fda.gov/scripts/opdlisting/oopd/detailedIndex.cfm?cfgridkey=382512.
4. US Food and Drug Administration. Orphan drug act -- relevant excerpts. Available from: https://www.fda.gov/industry/designating-orphan-product-drugs-and-biological-products/orphan-drug-act-relevant-excerpts.
5. Buccolam Summary of Product Characteristics (Midazolam Hydrochloride Oromucosal Solution) [Summary of Product Characteristics]. Barcelona, Spain: Laboratorios Lesvi, S.L.; 2023 https://www.ema.europa.eu/en/documents/product-information/buccolam-epar-product-information_en.pdf
6. Electronic Medicines Compendium. Diazepam Desitin 5 mg rectal solution. Available from: https://www.medicines.org.uk/emc/product/2997/smpc.
7. Diastat®. C-IV (Diazepam Rectal Gel). Bridgewater, NJ: Bausch Health US, LLC; 2023. prescribing information.
8. Libervant (Diazepam Buccal Film). prescribing information https://aquestive.com/content/uploads/libervant-2-to-5-years-of-age-pi-clean-pdf.pdf
9. Nayzilam® (Midazolam Nasal Spray). prescribing information https://www.ucb-usa.com/nayzilam-prescribing-information.pdf
10. Cereghino JJ. Identification and treatment of acute repetitive seizures in children and adults. Curr Treat Options Neurol. 2007;9(4):249–255. doi:10.1007/s11940-007-0011-8
11. Penovich PE, Buelow J, Steinberg K, Sirven J, Wheless J. Burden of seizure clusters on patients with epilepsy and caregivers: survey of patient, caregiver, and clinician perspectives. Neurologist. 2017;22(6):207–214. doi:10.1097/NRL.0000000000000140
12. Haut SR. Seizure clustering. Epilepsy Behav. 2006;8(1):50–55. doi:10.1016/j.yebeh.2005.08.018
13. Haut SR, Shinnar S, Moshe SL, O’Dell C, Legatt AD. The association between seizure clustering and convulsive status epilepticus in patients with intractable complex partial seizures. Epilepsia. 1999;40(12):1832–1834. doi:10.1111/j.1528-1157.1999.tb01607.x
14. Glauser T, Shinnar S, Gloss D, et al. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults: report of the guideline committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48–61. doi:10.5698/1535-7597-16.1.48
15. Misra SN, Jarrar R, Stern JM, Becker DA, Carrazana E, Rabinowicz AL. Rapid rescue treatment with diazepam nasal spray leads to faster seizure cluster termination in epilepsy: an exploratory post hoc cohort analysis. Neurol Ther. 2024;13(1):221–231. doi:10.1007/s40120-023-00568-4
16. Cloyd J, Haut S, Carrazana E, Rabinowicz AL. Overcoming the challenges of developing an intranasal diazepam rescue therapy for the treatment of seizure clusters. Epilepsia. 2021;62(4):846–856. doi:10.1111/epi.16847
17. Samanta D. Rescue therapies for seizure emergencies: current and future landscape. Neurol Sci. 2021;42(10):4017–4027. doi:10.1007/s10072-021-05468-9
18. Maltseva M, Rosenow F, von Podewils F, et al. Predictors for and use of rescue medication in adults with epilepsy: a multicentre cross-sectional study from Germany. Seizure. 2024;118:58–64. doi:10.1016/j.seizure.2024.04.005
19. Almohaish S, Sandler M, Brophy GM. Time is brain: acute control of repetitive seizures and status epilepticus using alternative routes of administration of benzodiazepines. J Clin Med. 2021;10(8):1754. doi:10.3390/jcm10081754
20. Wheless JW, Gidal B, Rabinowicz AL, Carrazana E. Practical questions about rescue medications for acute treatment of seizure clusters in children and adolescents with epilepsy in the USA: expanding treatment options to address unmet needs. Paediatr Drugs. 2024;26(1):49–57. doi:10.1007/s40272-023-00601-x
21. Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus-report of the ILAE Task Force on classification of status epilepticus. Epilepsia. 2015;56(10):1515–1523. doi:10.1111/epi.13121
22. Gidal B, Detyniecki K. Rescue therapies for seizure clusters: pharmacology and target of treatments. Epilepsia. 2022;63(suppl 1):S34–S44. doi:10.1111/epi.17341
23. Becker DA, Wheless JW, Sirven J, Tatum WO, Rabinowicz AL, Carrazana E. Treatment of seizure clusters in epilepsy: a narrative review on rescue therapies. Neurol Ther. 2023;12(5):1439–1455. doi:10.1007/s40120-023-00515-3
24. Spencer DC, Sinha SR, Choi EJ, et al. Safety and efficacy of midazolam nasal spray for the treatment of intermittent bouts of increased seizure activity in the epilepsy monitoring unit: a double-blind, randomized, placebo-controlled trial. Epilepsia. 2020;61(11):2415–2425. doi:10.1111/epi.16704
25. Niraj N, Mahajan S, Prakash A, Sarma P, Medhi B. The evaluation of the efficacy and safety of midazolam nasal spray in patients with seizure clusters: a systematic review and meta-analysis. Cureus. 2023;15(1):e34064. doi:10.7759/cureus.34064
26. Pina-Garza JE, Chez M, Cloyd J, et al. Outpatient management of prolonged seizures and seizure clusters to prevent progression to a higher-level emergency: consensus recommendations of an expert working group. Epileptic Disord. 2024;26(4):484–497. doi:10.1002/epd2.20243
27. Cereghino JJ, Mitchell WG, Murphy J, Kriel RL, Rosenfeld WE, Trevathan E. Treating repetitive seizures with a rectal diazepam formulation: a randomized study. The North American Diastat Study Group. Neurology. 1998;51(5):1274–1282. doi:10.1212/wnl.51.5.1274
28. Dreifuss FE, Rosman NP, Cloyd JC, et al. A comparison of rectal diazepam gel and placebo for acute repetitive seizures. N Engl J Med. 1998;338(26):1869–1875. doi:10.1056/NEJM199806253382602
29. Wheless JW, Miller I, Hogan RE, et al. Final results from a phase 3, long-term, open-label, repeat-dose safety study of diazepam nasal spray for seizure clusters in patients with epilepsy. Epilepsia. 2021;62(10):2485–2495. doi:10.1111/epi.17041
30. Sperling MR, Wheless JW, Hogan RE, et al. Use of second doses of Valtoco® (diazepam nasal spray) across 24 hours after the initial dose for out-of-hospital seizure clusters: results from a phase 3, open-label, repeat-dose safety study. Epilepsia. 2022;63(4):836–843. doi:10.1111/epi.17177
31. Wheless JW, Meng TC, Van Ess PJ, Detyniecki K, Sequeira DJ, Pullman WE. Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters: an open-label extension trial. Epilepsia. 2019;60(9):1809–1819. doi:10.1111/epi.16300
32. Detyniecki K, Van Ess PJ, Sequeira DJ, Wheless JW, Meng TC, Pullman WE. Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters-a randomized, double-blind, placebo-controlled trial. Epilepsia. 2019;60(9):1797–1808. doi:10.1111/epi.15159
33. Chen B, Choi H, Hirsch LJ, et al. Prevalence and risk factors of seizure clusters in adult patients with epilepsy. Epilepsy Res. 2017;133:98–102. doi:10.1016/j.eplepsyres.2017.04.016
34. Gidal B, Klein P, Hirsch LJ. Seizure clusters, rescue treatments, seizure action plans: unmet needs and emerging formulations. Epilepsy Behav. 2020;112:107391. doi:10.1016/j.yebeh.2020.107391
35. Maglalang PD, Rautiola D, Siegel RA, et al. Rescue therapies for seizure emergencies: new modes of administration. Epilepsia. 2018;59(suppl 2):207–215. doi:10.1111/epi.14479
36. Tanna V, Sawarkar SP, Ravikumar P. Exploring nose to brain nano delivery for effective management of migraine. Curr Drug Deliv. 2023;20(2):144–157. doi:10.2174/1567201819666220401091632
37. European Medicines Agency. Nasolam and associated names. Available from: https://www.ema.europa.eu/en/medicines/human/referrals/nasolam-associated-names.
38. Neurelis, Inc. Valtoco Instructions for Use. San Diego, CA: Neurelis, Inc; 2022.
39. Aquestive Therapeutics. Libervant (diazepam) buccal film, C-IV medication guide and instructions for use. 2024. https://aquestive.com/content/uploads/libervant-2-to-5-years-of-age-mg-ifu-Rev-1.pdf
40. Penovich P, Glauser T, Becker D, et al. Recommendations for development of acute seizure action plans (ASAPs) from an expert panel. Epilepsy Behav. 2021;123:108264. doi:10.1016/j.yebeh.2021.108264
41. Long L, Reynolds SS, Lewis LS, Webb MA, Epley C, Maturu S. Evaluation of a seizure action plan in an adult epilepsy center. Neurol Clin Pract. 2024;14(3):e200275. doi:10.1212/CPJ.0000000000200275
42. Chiang S, Haut SR, Ferastraoaru V, et al. Individualizing the definition of seizure clusters based on temporal clustering analysis. Epilepsy Res. 2020;163:106330. doi:10.1016/j.eplepsyres.2020.106330
43. Kapur J, Long L, Dixon-Salazar T. Consequences: bench to home. Epilepsia. 2022;63(suppl 1):S14–S24. doi:10.1111/epi.17342
44. Kapur J. Prehospital treatment of status epilepticus with benzodiazepines is effective and safe. Epilepsy Curr. 2002;2(4):121–124. doi:10.1111/j.1535-7597.2002.00045.x
45. Gainza-Lein M, Fernandez IS, Ulate-Campos A, Loddenkemper T, Ostendorf AP. Timing in the treatment of status epilepticus: from basics to the clinic. Seizure. 2019;68:22–30. doi:10.1016/j.seizure.2018.05.021
46. Sayin U, Osting S, Hagen J, Rutecki P, Sutula T. Spontaneous seizures and loss of axo-axonic and axo-somatic inhibition induced by repeated brief seizures in kindled rats. J Neurosci. 2003;23(7):2759–2768. doi:10.1523/JNEUROSCI.23-07-02759.2003
47. Haut SR. Seizure clusters: characteristics and treatment. Curr Opin Neurol. 2015;28(2):143–150. doi:10.1097/WCO.0000000000000177
48. Glauser T, Becker DA, Long L, et al. Short-term impact of seizures and mitigation opportunities. Curr Neurol Neurosci Rep. 2024;24(8):303–314. doi:10.1007/s11910-024-01350-1
49. Jiruska P, Freestone D, Gnatkovsky V, Wang Y. An update on the seizures beget seizures theory. Epilepsia. 2023. doi:10.1111/epi.17721
50. Dingledine R, Varvel NH, Dudek FE. When and how do seizures kill neurons, and is cell death relevant to epileptogenesis? Adv Exp Med Biol. 2014;813:109–122. doi:10.1007/978-94-017-8914-1_9
51. Gorter JA, van Vliet EA, Lopes da Silva FH. Which insights have we gained from the kindling and post-status epilepticus models? J Neurosci Methods. 2016;260:96–108. doi:10.1016/j.jneumeth.2015.03.025
52. Meritam Larsen P, Wustenhagen S, Terney D, Gardella E, Aurlien H, Beniczky S. Duration of epileptic seizure types: a data-driven approach. Epilepsia. 2023;64(2):469–478. doi:10.1111/epi.17492
53. Detyniecki K, O’Bryan J, Choezom T, et al. Prevalence and predictors of seizure clusters: a prospective observational study of adult patients with epilepsy. Epilepsy Behav. 2018;88:349–356. doi:10.1016/j.yebeh.2018.09.035
54. Penovich P, Wheless JW, Hogan RE, et al. Examining the patient and caregiver experience with diazepam nasal spray for seizure clusters: results from an exit survey of a phase 3, open-label, repeat-dose safety study. Epilepsy Behav. 2021;121(Pt A):108013. doi:10.1016/j.yebeh.2021.108013
55. Asnis-Alibozek A, Detyniecki K. The unmet need for rapid epileptic seizure termination (REST). Epilepsy Behav Rep. 2021;15:100409. doi:10.1016/j.ebr.2020.100409
56. French JA, Wechsler R, Gelfand MA, et al. Inhaled alprazolam rapidly suppresses epileptic activity in photosensitive participants. Epilepsia. 2019;60(8):1602–1609. doi:10.1111/epi.16279
57. French J, Biton V, Dave H, et al. A randomized phase 2b efficacy study in patients with seizure episodes with a predictable pattern using Staccato(R) alprazolam for rapid seizure termination. Epilepsia. 2023;64(2):374–385. doi:10.1111/epi.17441
58. Upsher-Smith Laboratories, Inc. Clinical research protocol: a randomized, double-blind, placebo-controlled study of the safety and efficacy of intranasal midazolam (USL261) in the outpatient treatment of subjects with seizure clusters. ARTEMIS-1: Acute Rescue Therapy in Epilepsy with Midazolam Intranasal Spray-1. 2015. https://cdn.clinicaltrials.gov/large-docs/20/NCT01390220/Prot_000.pdf
59. Cascino GD, Tarquinio D, Wheless JW, et al. Lack of clinically relevant differences in safety and pharmacokinetics after second-dose administration of intranasal diazepam within 4 h for acute treatment of seizure clusters: a population analysis. Epilepsia. 2022;63(7):1714–1723. doi:10.1111/epi.17249
60. Seinfeld S, Gelfand MA, Heller AH, Buan C, Slatko G. Safety and tolerability associated with chronic intermittent use of diazepam buccal film in adult, adolescent, and pediatric patients with epilepsy. Epilepsia. 2020;61(11):2426–2434. doi:10.1111/epi.16696
61. Misra SN, Sperling MR, Rao VR, et al. Examination of the inter–seizure-cluster interval over time in pediatric patients in a phase 3, long-term, open-label, repeat-dose safety study of diazepam nasal spray for the treatment of seizure clusters [poster #42].
62. Wheless JW, Hogan RE, Davis CS, Carrazana E, Rabinowicz AL. Safety and effectiveness of diazepam nasal spray in male and female patients: post hoc analysis of data from a phase 3 safety study. Epilepsia Open. 2024;9(2):793–799. doi:10.1002/epi4.12907
63. Misra SN, Sperling MR, Rao VR, et al. Analyses of patients who self-administered diazepam nasal spray for acute treatment of seizure clusters. Epilepsy Behav Rep. 2024;25:100644. doi:10.1016/j.ebr.2024.100644
64. Mitchell WG, Conry JA, Crumrine PK, et al. An open-label study of repeated use of diazepam rectal gel (Diastat) for episodes of acute breakthrough seizures and clusters: safety, efficacy, and tolerance. North American Diastat Group Epilepsia. 1999;40(11):1610–1617. doi:10.1111/j.1528-1157.1999.tb02047.x
65. Detyniecki K, Brunnert M, Campos R, Dimova S, Wheless JW. Return to full baseline functionality after repeated intermittent use of midazolam nasal spray in patients with seizure clusters: post hoc analysis of an open-label extension trial. Epilepsy Behav. 2023;148:109483. doi:10.1016/j.yebeh.2023.109483
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.