")
Back to Journals » Nature and Science of Sleep » Volume 17
Impact of Adenotonsillectomy on Quality of Life in Pediatric Obstructive Sleep Apnoea (OSA): Insights from the OSA-18 Questionnaire
Authors Al-Iede M , Alhelou Z, Hamdan N, Alramahi B , Algharibeh S, Qarajeh A, Ishtaieh S , Al Nsour A, AlAdwan M, Alhanbali A, Sinan RA , Khreesha L
Received 19 November 2024
Accepted for publication 9 May 2025
Published 12 June 2025 Volume 2025:17 Pages 1291—1301
DOI https://doi.org/10.2147/NSS.S506720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Valentina Alfonsi
Montaha Al-Iede,1,2 Zaina Alhelou,2 Nour Hamdan,2 Basil Alramahi,2 Shada Algharibeh,2 Ahmad Qarajeh,2 Sara Ishtaieh,2 Ahmad Al Nsour,3 Mai AlAdwan,2 Abdulrahman Alhanbali,2 Rima A Sinan,2 Lubna Khreesha3
1Division of Pediatric Pulmonology and Sleep Medicine, Department of Pediatrics, Jordan University Hospital, Amman, Jordan; 2The School of Medicine, the University of Jordan, Amman, Jordan; 3The Ear, Nose and Throat Department, The University of Jordan, Amman, Jordan
Correspondence: Montaha Al-Iede, The School of Medicine, The University of Jordan, Amman, Jordan, Email [email protected]
Purpose: Hypertrophy of the adenoids and tonsils is a common cause of obstructive sleep apnoea (OSA) in children, with adenotonsillectomy as the primary treatment. This study aimed to assess the efficacy of surgical options (adenotonsillectomy, adenoidectomy, and tonsillectomy) in managing pediatric OSA and their impact on quality of life, using the OSA-18 questionnaire.
Methods: This retrospective cohort study analyzed data from parents of 196 children who underwent adenoidectomy, tonsillectomy, or both. The OSA-18 questionnaire was administered online via Google Form to assess quality-of-life issues. Data collection occurred between November 4 and December 25, 2022. Statistical analysis included paired t-tests, ANOVA, Pearson’s correlation, and stepwise linear regression to evaluate pre- and post-surgery differences and associated factors.
Results: A significant improvement in quality of life was observed following adenotonsillectomy, with a mean reduction of 15.14 points in OSA-18 scores. The greatest improvements were noted in the domains of physical symptoms and sleep disturbance, particularly among children with severe OSA. Most participants were male (63%), with an average pre-surgery weight of 25.5 kg. Prior to surgery, 34.18% used CPAP and 56.12% nasal steroids. Post-surgery, 83.16% were hospitalized for 1– 2 days, with 4.08% requiring ICU care, and 26.53% experienced postoperative complications.
Conclusion: Surgical interventions, particularly adenotonsillectomy, significantly improved quality of life in pediatric OSA patients, with marked benefits in severe cases.
Plain Language Summary: This study assessed the effectiveness of surgical treatments for obstructive sleep apnea (OSA) in children and their impact on quality of life using OSA-18 questionnaire. OSA in children is commonly caused by enlarged adenoids and tonsils, and surgery—either removing the adenoids, tonsils, or both (adenotonsillectomy)—is the first line treatment.
Parents of 196 children who had undergone one of these surgeries were surveyed, using a questionnaire (OSA-18) to evaluate improvements in quality of life. Data was gathered online over a two-month period. Most of the children were boys, and some were using pre-surgery treatments like CPAP machines or nasal steroids to manage symptoms.
The findings showed that most children only stayed in the hospital for 1-2 days, though a few needed ICU care. Around a quarter experienced post-surgery complications, but overall, there were significant improvements in symptoms, especially among children with more severe OSA. Adenotonsillectomy, in particular, was associated with meaningful gains in physical well-being and sleep quality.
Keywords: adenoids, adenotonsillectomy, OSA, OSA-18, quality of life, Tonsillectomy
Introduction
The adenoid is a group of lymphoid tissue located on the posterior wall of the nasopharynx, along with the palatine tonsils, lingual tonsils, tubal tonsils of Gerlach, and lateral pharyngeal bands from Waldeyer’s ring.1 The adenoids and tonsils can become enlarged due to inflammation, leading to medical issues such as sleep-disordered breathing (SDB).2 SDB is the most common type of sleep-disordered breathing in children, predominantly caused by adenoid and tonsillar hypertrophy, while in adults, the primary sites of upper airway obstruction are the soft palate, tongue, palatine tonsils, and lateral pharyngeal wall.3 This condition affects around 7–17% of the pediatric population, manifesting as daytime and nocturnal symptoms.1,4 The daytime symptoms include behavioral disturbances, excessive daytime tiredness, aggressivity, and hyperactivity. The nocturnal symptoms range from primary snoring and restless sleep to enuresis and obstructive sleep apnea syndrome (OSAS).5 Untreated OSAS negatively impacts the emotional, cognitive, neurological and behavioral functioning of children and their families.6,7 Obstructive sleep apnea (OSA) in children is influenced by several risk factors such as obesity, prematurity, allergic rhinitis, and asthma.8 Polysomnography (PSG) remains the gold standard for diagnosing OSA.3 However, due to its limited availability, particularly in resource-limited settings, alternative screening tools such as validated questionnaires play an essential role in clinical decision-making. Various questionnaires have been developed to assess the quality of life in children with OSA, including the obstructive sleep apnea questionnaire (OSA-18). OSA-18 stands as one of the most frequently utilized questionnaires globally and has undergone validation in numerous languages.9 This tool aids in gathering subjective information regarding the impacts on the patient`s physical, psychological, and overall well-being.
Adenotonsillectomy has become one of the most common surgeries in pediatric otolaryngology. Indications for adenotonsillectomy have been well-studied,10,11 especially when hypertrophic tonsils and/or adenoids cause upper airway obstruction and obstruction and obstructive sleep apnea syndrome (OSAS).4 While adenotonsillectomy is widely recognized for improving symptoms in pediatric OSA, few studies have explored its long-term impact on quality of life, particularly across diverse age groups. This scarcity of studies evaluating the long-term impact of surgery on children`s quality of life, as well as the lack of research examining effects across a wide age range such as ours (7 months to 16 years), underscored the importance of conducting a study that addresses these gaps. Our research aimed to assess the perceived impact on quality of life in the pediatric population before and at least 6 months after surgery treatment for OSA, utilizing the OSA-18 questionnaire.
Materials and Methods
Study Design and Data Collection
This study used a retrospective observational design to assess the perceived impact of adenoidectomy, tonsillectomy, or both on the quality of life in children with Obstructive Sleep Apnea (OSA). Patient`s medical records were reviewed to identify children who were younger than 17 years and underwent adenoidectomy, tonsillectomy, or both for OSA at Jordan University Hospital between June 2020 and December 2022. Although our search included patients from infancy up to 17 years, the youngest patient in our final sample was 7 months old. To ensure a homogeneous study population, the following exclusion criteria were applied: children with underlying medical conditions such as craniofacial anomalies, neuromuscular diseases, genetic syndromes, or comorbidities that could affect the outcomes of OSA treatment; and children with incomplete medical records or whose parents refused to participate in the study. Jordan University Hospital is considered as the biggest tertiary university hospital in Amman and serves as a crucial healthcare facility in Jordan. An electronic version of the OSA-18 questionnaire, which was adapted into the Arabic language and administered as an online survey using the Google platform. Parents of eligible children were contacted by phone to explain the study and to obtain verbal permission. Additionally, a clear written paragraph was included at the beginning of the questionnaire, explaining the study and obtaining their permission for participation. The survey was made available for two months, from December 4 to December 25, 2022. The online questionnaire encompassed 54 questions categorized into four sections. The first section consisted of a written consent form. The second section focused on demographics, including questions about the participant`s name, and age at the time of surgery, in addition to clinical information such as type of surgery undergone, family history of OSA, history of SARS-CoV-2 infection, and use of nasal steroid and antihistamine or/and nocturnal CPAP. The third section involved administering the OSA-18 questionnaire before surgery. The last section included theOSA-18 questionnaire for the postoperative period, prompting parents to recall symptoms within the first 6 months following the surgery. The OSA-18 questionnaire comprises five domains: sleep disturbances, physical symptoms, emotional symptoms, daytime functions, and caregiver concerns. Following data collection, entries were reviewed and cleaned in Microsoft Excel to ensure completeness and accuracy. Subsequently, a senior researcher conducted a thorough examination of the data before inputting it into the Statistical Package for Social Sciences (SPSS) version 23 for statistical analysis.
Validation of Parental Recall
As the majority of parents completed the OSA-18 questionnaire retrospectively, a validation step was incorporated to enhance the reliability of parental recall from pre- and post-operative symptoms. Parental reports were cross-referred with medical records. Electronic medical records were searched to verify the accuracy of parental recall of symptoms. Particular emphasis was placed during the research on clinical notes in the ENT outpatient clinics, prior to and following the surgery, to collect comprehensive information related to sleep patterns, snoring frequency, and daytime fatigue. This process aimed to gather detailed and reliable data to complement parental recall and ensure a thorough assessment of symptomatology.
The OSA-18 Quality of Life Questionnaire
The OSA-18 survey is a valid and reliable tool for measuring Quality of Life (QoL) that can discriminate between children with sleep-disordered breathing.12 It is developed as an office-based questionnaire to assess the impact of OSA on children’s health-related QOL. The survey comprises 18 items categorized under 5 domains: sleep disturbances (4 items), physical suffering (4 items), emotional distress (3 items), daytime problems (3 items), and caregiver concerns (4 items).13 Each item is rated for frequency of occurrence on a 7-point Likert scale by the caregiver, as follows; 1- none of the time, 2- hardly any of the time, 3- a little of the time, 4- some of the time, 5- a good bit of the time, 6- most of the time, and 7- all the time. OSA-18 domains yield the following scores: [A] sleep disturbances (4 items with scores between 4 and 28), [B] physical suffering (4 items with scores between 4 and 28), [C] emotional distress (3 items with scores between 3 and 21), [D] daytime problems (3 items with scores between 3 and 21), [E] parent or caretaker concern (4 items with scores between 4 and 28). The total OSA-18 score ranges from 18 (no impact on quality of life) to 126 (significant impact on quality of life). A total symptom score was calculated by summing the points from each domain to assess the impact of OSA on health-related quality of life. The impact on health-related quality of life was categorized into three groups based on Franco et al’s prior validation: minor (<60), moderate (60–80), and major (>80).12 Partial scores were also calculated for each domain by summing the items within that domain.
To ensure compliance with copyright regulations and maintain the integrity of the OSA-18 questionnaire, we obtained formal permission from its original developers to use and translate the instrument into Arabic. The questionnaire was expertly translated into Arabic in accordance with WHO guidelines. This translation process took place at a reputable translation office in Amman and was overseen by a certified translator in collaboration with a bilingual healthcare professional possessing relevant clinical and research expertise. To ensure accuracy, a rigorous back translation was conducted by English-speaking healthcare staff, verifying the precise alignment of terms with those in the original document. In addition, the face and content validity of the translated questionnaire were carefully reviewed by a panel of specialist pediatricians from Jordan University Hospital, ensuring coherence of the questions and translation. The translated Arabic version demonstrated significant construct validity and test-retest reliability, thus providing robust evidence to support its utilization in the study. In addition to the rigorous translation and validation process described previously, a separate study validating the Arabic version of the OSA-18 questionnaire has been published.14
Ethical Considerations
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and received approval from the Institutional Review Board of Jordan University Hospital (reference number: 4550/2022/67). A written informed consent form was incorporated at the beginning of the online OSA-18 questionnaire, which participants` parents reviewed and agreed to before proceeding. Confidentiality of Participants’ data was strictly maintained throughout the study. Participants were given the option to withdraw from the study at any time without the need to provide an explanation.
Statistical Analysis
Descriptive statistics were calculated using Python (version 3.9.12) within the JupyterLab environment (version 3.3.2). Nominal variables were summarized as frequencies and percentages, while continuous variables were presented as means ± standard deviations. Assuming normal distribution based on the central limit theorem, parametric tests were employed for continuous data. The primary outcome, the difference in OSA-18 scores pre- and post-surgery, was computed by subtracting the postoperative score from the preoperative score, with positive values indicating improvement. Paired t-tests were used to assess changes in OSA-18 scores and subdomain scores. Independent t-tests and one-way ANOVA were conducted to examine associations between score differences and categorical variables. Significant ANOVA results were further analyzed using Tukey’s Honest Significant Difference (HSD) test, with effect sizes estimated using Hedges’ g. Pearson’s correlation coefficient (r) assessed relationships between continuous variables. A stepwise linear regression model with forward selection was implemented to identify predictors of score differences. Variables were entered into the model based on theoretical relevance and statistical significance (entry criterion: p < 0.05).
Results
Our sample included 196 children who underwent adenoidectomy, tonsillectomy, or both. Surveys were completed by parents with no missing data. Of the sample, 124 (63.27%) were male. Ages ranged from 7 months to 16 years, with an average of 6.52 years (± 3.32). The average weight before surgery was 25.53 kg (±14.36), and 26.25 kg (±13.41) after, with no significant difference (p= 0.12875, CI= [−1.66, 0.21]). Table 1 summarizes demographic data and potential risk factors.
 |
Table 1 Demographic Data of the Sample in Addition to Some Possible Risk Factors |
Of the sample, 78 (39.8%) patients had a family history of OSA. Sixty-seven (34.18%) children used CPAP before surgery, and 110 (56.12%) used nasal steroids. Of those using nasal steroids, 78 (39.8%) used them for 1–3 months, 20 (10.2%) for 4–6 months, and 12 (6.12%) for over six months. Most children (163, 83.16%) were hospitalized for 1–2 days post-surgery, with 8 (4.08%) requiring ICU admission. Postoperative complications occurred in 52 (26.53%) children, as detailed in Table 2.
 |
Table 2 Complications and days of Hospitalization |
The mean OSA-18 score dropped from 61.55 ±21.33 before surgery to 46.41 ±23.23 after (p <0.001, CI [11.78, 18.5]). Table 3 shows significant differences in subsection scores pre- and post-surgery. Severe OSA-18 cases decreased from 44 (24.15%) to 24 (12.24%). Figure 1 illustrates the change in OSA-18 class, while Figure 2 compares sub-scores. There was no significant effect of family history of OSA, nasal steroid use, or CPAP use on post-surgery scores (p= 0.51, 0.12, 0.96, 0.05). Table 4 compares variables and score differences.
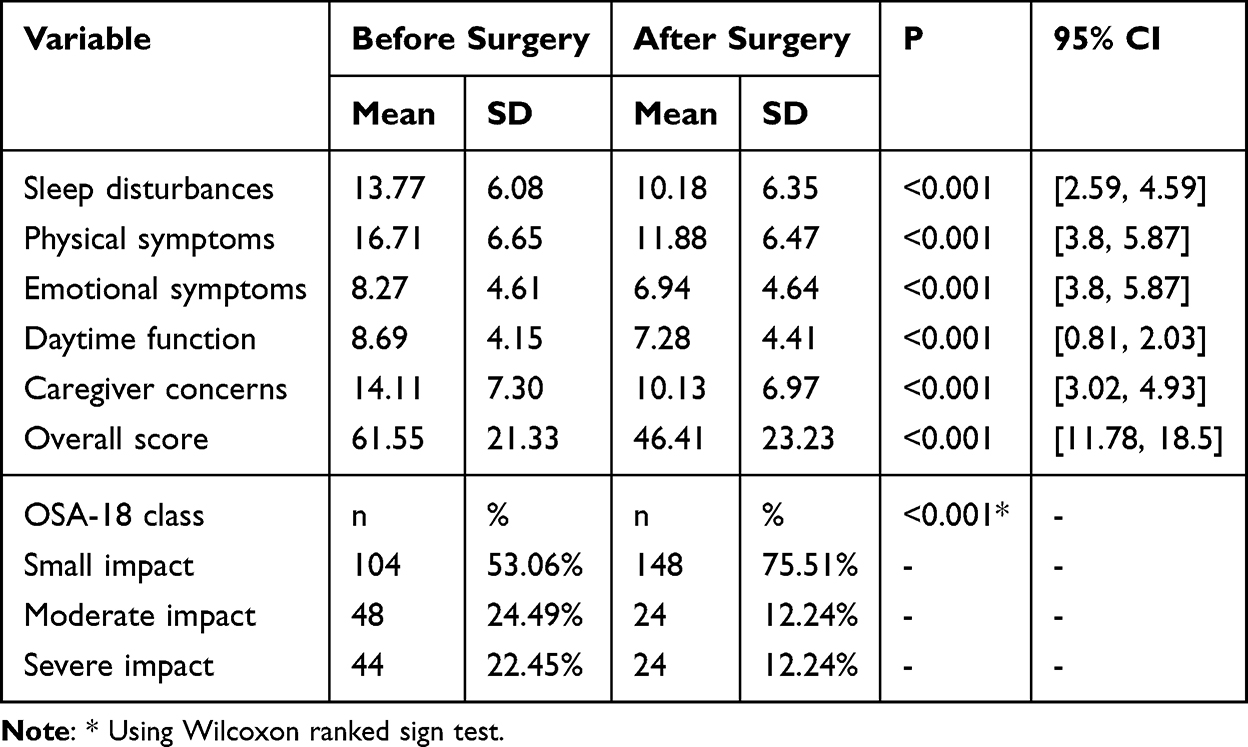 |
Table 3 OSA-18 Scores Before and After Surgery |
 |
Table 4 Interactions Between Various Variables and Score Difference |
 |
Figure 1 OSA-18 class before and after surgery. |
 |
Figure 2 OSA-18 sub-scores before and after surgery. |
Our sample had a noticeable improvement in OSA-18 scores with a mean score difference of 15.14 and a standard deviation of 23.87. Higher score category before surgery was found to be significantly associated with higher score after surgery in addition to higher score difference (p<0.001 for both). Even though age and weight before surgery were significantly correlated negatively to score before surgery (p= 0.006 and 0.035, r= −0.20 and −0.15 respectively), no significant correlation was apparent on score after surgery (p= 0.46 and 0.43 respectively) or score difference (p= 0.08 and 0.27 respectively) (Table 4).
In a multiple linear regression model using forward stepwise selection, being male, having a family history of OSA, and mild OSA-18 scores were significant negative predictors of score difference (p= 0.040, 0.033, and <0.001). Severe OSA-18 scores were a positive predictor (p=0.012). CPAP use and nasal steroids before surgery did not significantly predict score changes (p= 0.122 and 0.134). Table 5 shows the final variables in the best-fitting model.
 |
Table 5 Stepwise Linear Regression to Predict Score Difference Depending on Variables with Theoretical Significance |
Discussion
We found that adenoidectomy, tonsillectomy, or adenotonsillectomy significantly improved children’s behavior and quality of life (QoL) with obstructive sleep apnea (OSA), which is consistent with previous research.15,16 Sleep-disordered breathing (SDB) can negatively impact children’s memory and attention levels, likely due to hypoxic effects, and is associated with daytime symptoms such as irritability, aggression, and hyperactivity.17 Assessing children’s quality of life is essential for understanding how physical, emotional, and social factors impact their health and daily activities.17,18 We utilized the OSA-18 questionnaire to assess patients preoperatively and postoperatively. This validated tool is easy to implement and helps clinicians evaluate the quality of life in children with OSA. It can also enhance service quality, allow for peer comparison, and complement objective research methods.19 However, the OSA-18 is less useful as a tool to identify patients with OSA due to its lower sensitivity compared to other methods.20
In our study, the majority of patients were males, reflecting a gender distribution similar to that reported by Veena Mobarsa et al, who also found a higher proportion of males (70%).1 While Jose Junior et al observed a higher prevalence of females (56.2%) in their cohort of children aged 3 to 11 years, these demographic differences did not significantly impact the quality of life improvements observed after surgery in our cohort.16 Notably, our study included a broad age range, with participants spanning from 7 months to 16 years and a mean age of 6.52 years. This wide inclusion range offers a more comprehensive perspective on surgical outcomes across different pediatric age groups. In comparison, Juliana Caixeta et al included patients aged 3 to 13 years, and Jose Junior et al focused on those aged 2 to 11 years.5,21 This broader age spectrum enhances the generalizability of our findings regarding the impact of adenotonsillectomy on quality of life in children with OSA.
Adenoidectomy or adenotonsillectomy represent the most common surgical procedures in otorhinolaryngology, primarily performed to treat conditions such as obstructive sleep apnea, recurrent infections, and chronic airway obstruction in pediatric patients.18 In adequately selected children, these measures can enhance the quality of life and solve obstructive sleep problems. Current study revealed that the majority of patients underwent adenotonsillectomy, followed by adenoidectomy, and then tonsillectomy. This pattern was consistent with the findings of F. Escarrá and S. Vidaurreta et al, who also observed that the majority of their cohort underwent adenotonsillectomy, followed by adenoidectomy, and then tonsillectomy, mirroring our study`s results.4 It is important to note that adenotonsillectomy and adenoidectomy are preferred over tonsillectomy alone due to their lower risk of morbidity, mortality, and postoperative complications.22,23 While the definitive recommendation regarding the superiority of adenotonsillectomy over adenoidectomy has not been established, adenotonsillectomy is more commonly performed as some previous studies suggest that it carries a lower risk of residual disease.24
Our study found no significant effect of having a positive family history of OSA, using nasal steroids before surgery, or using a CPAP device before surgery on score after surgery. Previous studies have demonstrated that the use of nasal corticosteroids can reduce adenoid size and improve nasal obstruction symptoms, providing an effective alternative to surgical treatment in some mild cases.25,26 From another perspective, patients with symptoms consistent with rhinitis in a study by Juliana Caixeta et alwere treated using nasal corticosteroids and/or antihistamines, as recommended for 3 months, and were then reevaluated.5 Once they presented with full recovery, they were considered a candidate for surgery. This can be explained by the fact that Allergic Rhinitis (AR) may be a risk factor for the deterioration of long-term QOL after adenotonsillectomy. Therefore, preoperative evaluation and proper management of AR might be considered in pediatric SDB.27 In a multiple linear regression model, male gender, family history of OSA, and mild preoperative OSA-18 scores were significant negative predictors of score difference. Neither CPAP use nor nasal steroids before surgery significantly impacted score differences between pre- and postoperative evaluations. Conversely, severe OSA-18 preoperatively was a positive predictor of score difference. Similarly, M. Imanguli and S. Usual tackled the prevalence of residual OSA in patients post adenotonsillectomy, and concluded that patients with severe OSA had a higher prevalence of residual OSA than patients with moderate or mild OSA.28
In our study, we conducted pre- and post-operative assessments using the OSA-18 score, revealing a significant difference in average score. Juliana Caixeta et al’s study using the OSA-18 questionnaire at intervals—before, 10 days, 6 months, 12 months, and 18 months post-surgery—demonstrated consistent score improvement without increases in total or domain-specific scores. While this extended follow-up boosts reliability, long-term studies are difficult as most patients do not require further evaluation once their symptoms resolve.5 This is particularly evident in children without underlying health conditions, as the success rate of the surgery tends to be high.29 In our study, significant differences were observed across all OSA-18 domains post-surgery. This observation mirrors the findings of Veena Mobarsa et al, who noted a substantial decrease in the mean OSA-18 score accompanied by a reduction across all domains. et al concluded that caregiver concerns and physical sufferings were the domains of greatest improvement, while sleep disturbance and daytime function were the least domains to be improved.1,30 A study by Mitchell et al assessed 61 children (43 with OSA and 18 with mild SDB) using the OSA-18 survey to evaluate adenotonsillectomy outcomes.31 Both groups showed significant improvement post-surgery, with the greatest improvement in physical suffering and the least in emotional distress. Comparing these results with previous studies is difficult due to variability in parental responses, as OSA-18 is subjective and may lead to over- or under-reporting of symptoms. Additionally, there is a risk of procedural bias in the postoperative phase.
Most children were hospitalized for one to two days post-surgery, with only 4.08% requiring ICU admission. Postoperative complications occurred in 26.53% of cases, with the most common being poor eating and drinking, likely due to pain and swallowing difficulties. Bleeding and upper respiratory tract infections followed, while ICU admission for oxygen support was the least common complication. In contrast, Francisco J Schneider et al reported hemorrhage as the most prevalent postoperative complication in the initial admission, while respiratory complications being the most common in subsequent readmissions.32
Our findings underscore the effectiveness of adenotonsillectomy in improving quality of life for children with OSA, particularly in severe cases. These results can guide clinicians in surgical decision-making and postoperative care by highlighting the potential benefits of the procedure. Additionally, understanding the prevalence and nature of postoperative complications can assist healthcare providers in anticipating and managing these challenges, ultimately enhancing patient outcomes.
Limitations of the Study
Despite thorough validation efforts, the retrospective nature of the study introduces the possibility of recall bias in parental symptom reports. Additionally, the reliance on existing medical records may have led to incomplete or missing data, further highlighting a limitation commonly associated with retrospective studies. Moreover, the absence of objective diagnostic measures such as polysomnography (PSG) limits the ability to precisely correlate clinical improvements with physiological outcomes. Future prospective studies incorporating PSG are recommended to enhance diagnostic accuracy and better quality surgical efficacy in managing pediatric OSA.
Conclusion
Our study demonstrates that adenotonsillectomy improves the quality of life in children with obstructive sleep apnea (OSA), as evidenced by reductions in OSA-18 scores across all domains, particularly in physical symptoms and sleep disturbances. These improvements were most pronounced in severe cases, underscoring the procedure’s efficacy in addressing more critical presentations of pediatric OSA. By contributing data from a Middle Eastern population and utilizing a validated Arabic version of the OSA-18 questionnaire, our study adds to the global body of evidence supporting the procedure’s efficacy across diverse cultural and linguistic contexts. Our findings support the integration of adenotonsillectomy into clinical guidelines and health policies aimed at managing pediatric OSA in such environments.
While the majority of patients experienced substantial benefits, it is important to acknowledge that some encountered postoperative complications, such as poor oral intake and minor bleeding. Although these complications were generally transient and managed effectively, they may have temporarily affected recovery and parental perceptions of postoperative quality of life. Recognizing and addressing these potential challenges are crucial for comprehensive patient care and counseling.
Data Sharing Statement
The data supporting this study`s findings are available from the corresponding author upon reasonable request.
Author Contributions
Montaha Al-Iede contributed to the conception and design of the study, methodology development, data curation, supervision, project administration, and final approval of the manuscript.
Zaina Alhelou, Nour Hamdan, Basil Alramahi, Shada Algharibeh, Ahmed Qarajeh, and Sara Ishtaieh contributed to methodology, data collection, and writing the original draft.Abdulrahman Alhanbali contributed to data curation, formal statistical analysis, and reviewing and editing the manuscript. Mai AlAdwan and Rima A Sinan contributed to data curation and writing the original draft. Ahmed Al Nsour and Lubna Khreesha contributed to data collection from the ENT department, methodology, data curation, and reviewing and editing the manuscript. All authors contributed to drafting, critically revising the article, gave final approval of the version to be published, agreed on the journal for submission, and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no competing relevant to this article to disclose.
References
1. Bamaniya H, Mobarsa V, Bhuie HS, Saxena RK. Impact of adenoidectomy or adenotonsillectomy on paediatric quality of life using obstructive sleep apnoea - 18 questionnaire. Int J Otorhinolaryngolo Head Neck Surg. 2020;6(5):955. doi:10.18203/issn.2454-5929.ijohns20201694
2. Wong HB. The problems of tonsils and adenoids. J Singapore Paediatric Soc. 1989;31(3–4):97–102.
3. Greenfeld M, Tauman R, DeRowe A, Sivan Y. Obstructive sleep apnea syndrome due to adenotonsillar hypertrophy in infants. Int J Pediatr Otorhinolaryngol. 2003;67(10):1055–1060. doi:10.1016/s0165-5876(03)00182-4
4. Escarrá F, Vidaurreta SM. Assessment of quality of life before and after an adenotonsillectomy among children with hypertrophic tonsils and/or adenoids. Archivos Argentinos De Pediatria. 2015;113(1):21–27. doi:10.5546/aap.2015.eng.21
5. Caixeta JAS, Sampaio JCS, Costa VV, et al. Long-term impact of adenotonsillectomy on the quality of life of children with sleep-disordered breathing. Int Arch Otorhinolaryngol. 2021;25(1):e123–e128. doi:10.1055/s-0040-1709195
6. Kurnatowski P, Putyński L, Łapienis M, Kowalska B. Physical and emotional disturbances in children with adenotonsillar hypertrophy. J Laryngology Otol. 2008;122(9):931–935. doi:10.1017/S0022215107001235
7. Kurnatowski P, Putyński L, Łapienis M, Kowalska B. Neurocognitive abilities in children with adenotonsillar hypertrophy. Int J Pediatric Otorhinolaryngol. 2006;70(3):419–424. doi:10.1016/J.IJPORL.2005.07.006
8. Garza N, Witmans M, Salud M, Lagera PGD, Co VA, Tablizo MA. The association between asthma and OSA in children. Children. 2022;9(10):1430. doi:10.3390/children9101430
9. Kang KT, Weng WC, Yeh TH, Lee PL, Hsu WC. Validation of the Chinese version OSA-18 quality of life questionnaire in Taiwanese children with obstructive sleep apnea. J Formosan Med Association = Taiwan Yi Zhi. 2014;113(7):454–462. doi:10.1016/j.jfma.2012.10.002
10. Kavanagh KT, Beckford NS. Adenotonsillectomy in children: indications and contraindications. Southern Med J. 1988;81(4):507–514. doi:10.1097/00007611-198804000-00023
11. Darrow DH, Siemens C. Indications for tonsillectomy and adenoidectomy. Laryngoscope. 2002;112(8 Pt 2 Suppl 100):6–10. doi:10.1002/lary.5541121404
12. Franco RA, Rosenfeld RM, Rao M. First place–resident clinical science award 1999. Quality of life for children with obstructive sleep apnea. Otolaryngol–Head Neck Surg. 2000;123(1 Pt 1):9–16. doi:10.1067/mhn.2000.105254
13. Da SVC, Leite AJM. Quality of life in children with sleep-disordered breathing: evaluation by OSA-18. Braz J Otorhinolaryngol. 2006;72(6):747–756. doi:10.1016/s1808-8694(15)31041-7
14. Al-Iede M, Alshrouf MA, Al-Ani A, et al. Validation of the Arabic version of the obstructive sleep apnea-18 quality of life questionnaire for evaluating children with sleep apnea–hypopnea syndrome. Annals Thoracic Med. 2024;19(4):266–274. doi:10.4103/atm.atm_94_24
15. Garetz SL. Behavior, cognition, and quality of life after adenotonsillectomy for pediatric sleep-disordered breathing: summary of the literature. Otolaryngol–Head Neck Surg. 2008;138(1 Suppl):S19–26. doi:10.1016/j.otohns.2007.06.738
16. Goldstein NA, Fatima M, Campbell TF, Rosenfeld RM. Child behavior and quality of life before and after tonsillectomy and adenoidectomy. Arch Otolaryngology–Head Neck Surg. 2002;128(7):770–775. doi:10.1001/archotol.128.7.770
17. Pulmonology S on OSASAA of PS on P. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002;109(4):704–712. doi:10.1542/peds.109.4.704.
18. Stewart MG. Pediatric outcomes research: development of an outcomes instrument for tonsil and adenoid disease. Laryngoscope. 2000;110(3 III):12–15. doi:10.1097/00005537-200003002-00004
19. Ishman SL, Tawfik KO, Smith DF, et al. Screening for pediatric obstructive sleep apnea before ambulatory surgery. J Clin Sleep Med. 2015;11(7):751–755. doi:10.5664/jcsm.4852
20. Ishman SL, Yang CJ, Cohen AP, et al. Is the OSA-18 predictive of obstructive sleep apnea: comparison to polysomnography. Laryngoscope. 2015;125(6):1491–1495. doi:10.1002/lary.25098
21. de L JJM, da SVC, de FMR. Long term results in the life quality of children with obstructive sleep disorders submitted to adenoidectomy/adenotonsillectomy. Braz J Otorhinolaryngol. 2008;74(5):718–724. doi:10.1016/S1808-8694(15)31382-3
22. Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):e714–55. doi:10.1542/peds.2012-1672
23. Kirkham EM, Baldassari CM. Mortality after pediatric tonsillectomy-does the “D” word have a place in tonsillectomy discussions? JAMA Otolaryngol– Head Neck Surg. 2022;148(8):717–718. doi:10.1001/jamaoto.2022.1803
24. Domany KA, Dana E, Tauman R, et al. Adenoidectomy for obstructive sleep apnea in children. J Clin Sleep Med. 2016;12(9):1285–1291. doi:10.5664/jcsm.6134
25. Demirhan H, Aksoy F, Ozturan O, Yildirim YS, Veyseller B. Medical treatment of adenoid hypertrophy with “fluticasone propionate nasal drops”. Int J Pediatric Otorhinolaryngol. 2010;74(7):773–776. doi:10.1016/j.ijporl.2010.03.051
26. Demain JG, Goetz DW. Pediatric adenoidal hypertrophy and nasal airway obstruction: reduction with aqueous nasal beclomethasone. Pediatrics. 1995;95(3):355–364. doi:10.1542/peds.95.3.355
27. Kim DK, Han DH. Impact of allergic rhinitis on quality of life after adenotonsillectomy for pediatric sleep-disordered breathing. Int Forum Allergy Rhinol. 2015;5(8):741–746. doi:10.1002/alr.21529
28. Imanguli M, Ulualp SO. Risk factors for residual obstructive sleep apnea after adenotonsillectomy in children. Laryngoscope. 2016;126(11):2624–2629. doi:10.1002/lary.25979
29. Brietzke SE, Gallagher D. The effectiveness of tonsillectomy and adenoidectomy in the treatment of pediatric obstructive sleep apnea/hypopnea syndrome: a meta-analysis. Otolaryngol–Head Neck Surg. 2006;134(6):979–984. doi:10.1016/j.otohns.2006.02.033
30. Sarmah U, Mandal S, Roy M. Quality of life and behavioural assessment in post-adenotonsillectomy cases of paediatric age group. Ind J Otolaryngol Head Neck Surg. 2019;71(Suppl 1):221–229. doi:10.1007/s12070-018-01569-8
31. Mitchell RB, Kelly J. Quality of life after adenotonsillectomy for SDB in children. Otolaryngol–Head Neck Surg. 2005;133(4):569–572. doi:10.1016/j.otohns.2005.05.040
32. Schneuer FJ, Bell KJ, Dalton C, Elshaug A, Nassar N. Adenotonsillectomy and adenoidectomy in children: the impact of timing of surgery and post-operative outcomes. J Paediatr Child Health. 2022;58(9):1608–1615. doi:10.1111/jpc.16052
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.