")
Back to Journals » Clinical Interventions in Aging » Volume 19
Impact of Adverse Health Conditions on Clinical Outcomes of Older People with Atrial Fibrillation: Insights from a Prospective Cohort Study
Authors Liu JP , Zhang Y, Zhao Z , Zhang T, Na Y, Luo Y, Wan Y, Sun N, Wu C, Wang H , Yang J
Received 13 February 2024
Accepted for publication 24 July 2024
Published 6 September 2024 Volume 2024:19 Pages 1519—1528
DOI https://doi.org/10.2147/CIA.S464044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Maddalena Illario
Jun-Peng Liu,1 Yatong Zhang,2 Zinan Zhao,2 Tianqi Zhang,2 Yifan Na,2 Yao Luo,1 Yuhao Wan,1 Ning Sun,1 Cheng Wu,1 Hua Wang,1 Jiefu Yang1
1Department of Cardiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Pharmacy, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
Correspondence: Hua Wang, Department of Cardiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, No. 1, Da Hua Road, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86 13911680467, Email [email protected]
Objective: To evaluate the impact of adverse health conditions, including multimorbidity, frailty, malnutrition, cognitive impairment, and polypharmacy, on clinical outcomes in older people with atrial fibrillation (AF).
Patients and Methods: This prospective cohort study focused on patients aged 65 years and older with AF. They were admitted to the hospital between September 2018 and April 2019 and followed up for 1 year. We evaluated these participants for adverse health conditions including multimorbidity, frailty, malnutrition, cognitive impairment, and polypharmacy. The primary clinical outcome measured was a combination of all-cause mortality or rehospitalization.
Results: 197 older patients (≥ 65 years) with AF (mean age, 77.5± 7.1 years; 57.4% men) were enrolled. During 1-year follow-up, Primary endpoint events (all-cause mortality or rehospitalization) occurred in 82 patients (41.6%). Compared with the non-event group, the Charlson comorbidity index (CCI) was higher (2.5± 1.9 vs 1.7± 1.3, p=0.004), more heart failure (32.9% vs 17.4%, p=0.01) and chronic kidney disease (17.1% vs 7.0%, p=0.03), with lower systolic blood pressure (125.3± 18.3 mmHg vs 132± 17.9 mmHg, p=0.005) in the event group. On multivariate Cox regression showed that the CCI was associated with a higher odds ratio of the composite outcome of all-cause mortality and rehospitalization (HR: 1.26; 95% CI: 1.02– 1.56, p=0.03). Other adverse health conditions showed no significant association with the composite outcome of all-cause mortality and rehospitalization.
Conclusion: Among adverse health conditions in older people with AF, multimorbidity appears to be a significant determinant of adverse clinical outcomes.
Clinical Trial Registration: ChiCTR1800017204; date of registration: 07/18/2018.
Keywords: atrial fibrillation, older people, multimorbidity, prognosis
Graphical Abstract:

Introduction
Atrial fibrillation (AF) is the most common arrhythmia and a major cause of stroke, heart failure (HF), cardiovascular morbidity, and sudden death.1 Patients with AF are often older and overburdened with adverse health conditions (multimorbidity, frailty, malnutrition and cognitive impairment).2 Previous studies revealed that adverse health conditions are associated with worse clinical outcomes in older people with AF.3–6 Nevertheless, the impact on clinical outcomes, which is stronger and which is weaker, remains unclear. Therefore, in the present study, we evaluated the prognostic significance of adverse health condition, including multimorbidity, frailty, malnutrition, cognitive impairment, and polypharmacy, on clinical outcomes in older people with AF.
Methods
The data from a prospective observational cohort study on frailty in China (Trial registration: ChiCTR1800017204; date of registration: 07/18/2018). The Study recruited ≥65 years elderly inpatients who were consecutively admitted to 3 tertiary referral hospitals in Beijing, China, from September 2018 to April 2019, which approved by the Ethics Committee of Beijing Hospital (approval no. 2018BJYYEC-121-02).
Study Population
The study population included 197 consecutive ≥65 years elderly inpatients with a diagnosis of current or resolved atrial fibrillation. Baseline data collection included sociodemographics, hospitalization information, medical history, comorbidities, physical examinations, laboratory tests, echocardiographic data and medications.
Definition of Adverse Health Conditions/Clinical Complexity
Participants were followed up to assess the occurrence of adverse health conditions/clinical complexity including multimorbidity, frailty, malnutrition, cognitive impairment and polypharmacy. Multimorbidity were measured by the Charlson comorbidity index (CCI).7 The CCI has been validated as a reliable tool to evaluate the burden of multimorbidity, which comprised 19 diagnoses to which different weights have been assigned and summed to obtain the final calculation (Supplementary Table 1). We used the Edmonton frailty score (EFS) to assess frailty.8 EFS is a multidimensional frailty assessment tool that includes general health status, functional independence, social support, cognition, medication use, nutrition, continence and mood. Subjects with an EFS ≥8 are classified as frail (Supplementary Table 2). Malnutrition was defined according to the short form mini nutritional assessment (MNA-SF) ≤7 points (Supplementary Table 3).9 We used the mini-mental state examination (MMSE)10 and clock drawing test (CDT)11 to define cognitive impairment (Supplementary Table 4): (1) below 24 points of MMSE or (2) 24≤MMSE≤26 and incorrect CDT. Polypharmacy was defined according to the number of drugs prescribed at baseline, as the presence of ≥7 different drugs taken by a patient.12
Study End Points
The primary outcome was a composite of all-cause death or rehospitalization. All events were independently reviewed. We separately considered all-cause death or rehospitalization as independent outcomes. Clinical follow-up was routinely performed via clinical visit and/or telephone interview at 3, 6 and 12 months.
Statistical Analysis
The subjects were divided into two groups based on the occurrence of the primary endpoint. Continuous variables are presented as mean ± SD, and independent t test was performed for intergroup comparison. Non-normally distributed variables were reported as median (25th-75th percentile), and Wilcoxon rank-sum test was performed for intergroup comparison. Categorical variables are expressed as count (%), and comparisons were performed by using the Fisher exact test or chi-squared test.
Univariable and multivariable Cox proportional hazards models were developed to determine independent predictors of all-cause death or rehospitalization. We took frailty as an independent variable. We determined the covariates for the multivariable analysis based on two criteria: significant differences between groups and clinical significance. CCI, cognitive impairment, malnutrition, polypharmacy, age, sex, education, living alone, smoking, drinking, body mass index (BMI), CHA2DS2-VASc≥5, HAS-BLED≥3, heart failure, heart rate, hemoglobin, albumin, high-sensitivity C-reactive protein (hsCRP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), D-dimer, left atrial anteroposterior diameter and left ventricular ejection fraction were analyzed as dependent variables. The Cox models were tested for the proportional hazards assumption and linearity of continuous variables. We checked using the variance inflation factor ensuring that the variance inflation factor for each variable was <10. Cumulative survival curves were estimated by Kaplan-Meier methods and compared between groups using the Log rank test. All statistical tests were bilateral tests, and a P value of <0.05 was considered to indicate statistical significance. All the analyses were performed using SAS software, version 9.4 (SAS Institute Inc).
Results
Baseline Characteristics
Among the 197 patients included (Figure 1), the mean mean ± SD age was years, and 57.4% were men. 52.3% of patients were paroxysmal AF. The CHADS-VASc Score was 4.4 ± 1.6 and the HAS-BLED Score was 1.9 ± 0.7. Mean (±SD) CCI was 2.0 ± 1.6. Patients with high multimorbidity (CCI ≥4) was 34 (17.3%). There were 55 (27.9%) patients with frailty, 9 (4.6%) patients with malnutrition, 57 (28.9%) patients with cognitive impairment and 89 (45.2%) patients with polypharmacy (Figure 2).
 |
Figure 1 Selection of the study population. |
 |
Figure 2 Prevalence of adverse health conditions (multimorbidity, frailty, malnutrition, cognitive impairment, and polypharmacy). High multimorbidity = CCI ≥4. Abbreviation: CCI, Charlson comorbidity Index. |
Clinical Outcomes
188 patients completed 1-year follow-up, with a total loss rate of 4.6%. There were 6 cases of all-cause mortality (3.0%), and 80 patients experienced rehospitalization (40.6%). The primary end point event (all-cause death or rehospitalization) occurred in 82 patients (41.6%). The cohort was divided into 2 groups on the basis of the occurrence of primary endpoint events (events group and no-events group). Baseline clinical differences between the groups are shown in Table 1. Patients with an adverse event more frequently had heart failure and chronic kidney disease (CKD), had higher CCI and lower systolic blood pressure (SBP).
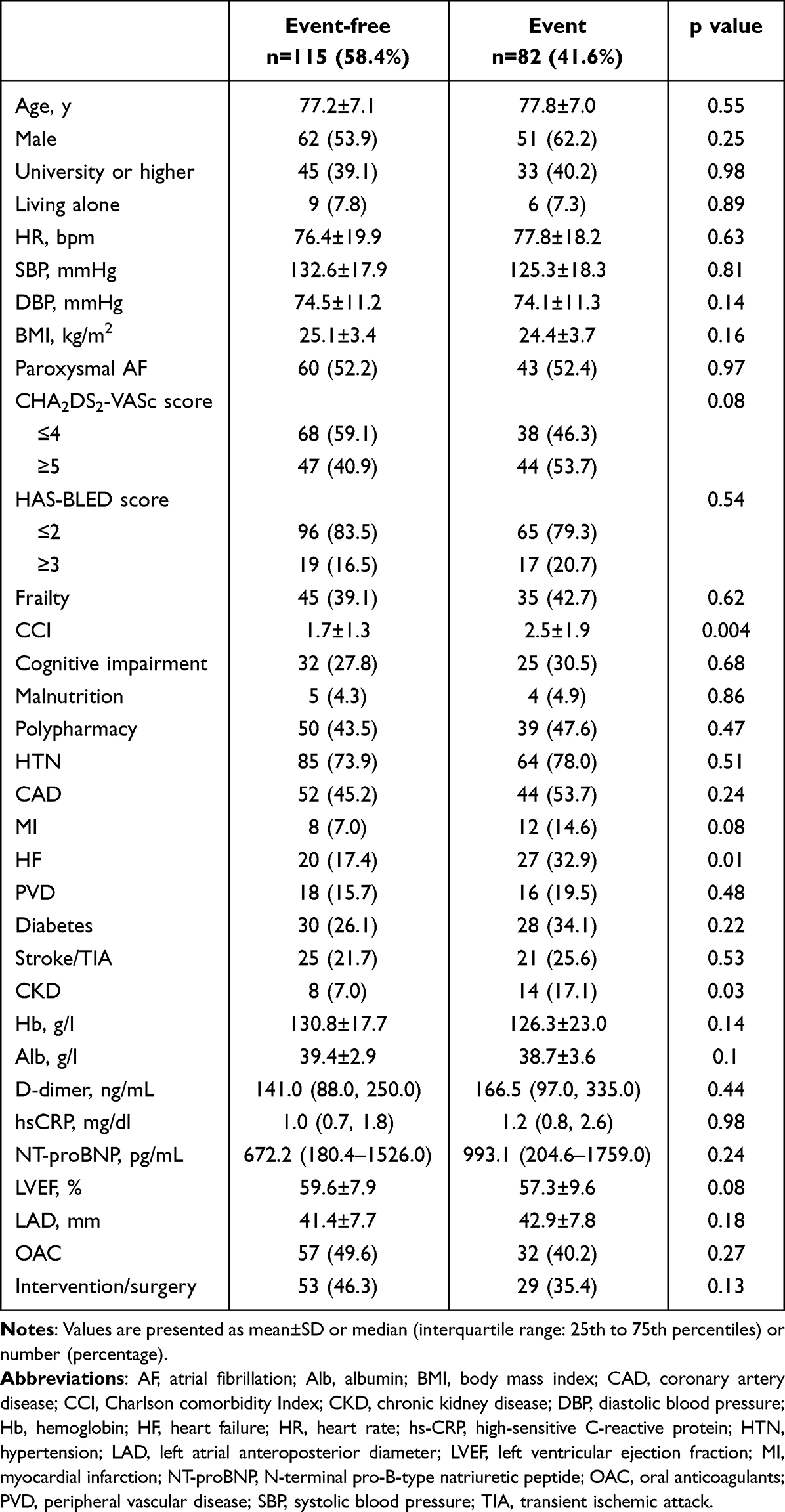 |
Table 1 Baseline Patients Characteristics |
Association Between Adverse Health Conditions and Clinical Outcomes
Cox univariable regression analysis (Table 2) showed that CCI was associated with a significantly higher risk of all-cause death or rehospitalization events (HR: 1.29; 95% CI: 1.13 to 1.47, p<0.001), and other risk factors associated with all-cause death or rehospitalization events included heart failure (HR: 1.84; 95% CI: 1.17 to 1.81, p=0.009), Log Hb (OR: 0.30; 95% CI: 0.13 to 0.69, p=0.04) and LVEF (HR: 0.98; 95% CI: 0.95 to 1.00, p=0.04). On multivariate Cox regression (Table 2) showed that the CCI was associated with a higher odds ratio of the composite outcome of all-cause mortality and rehospitalization (HR: 1.26; 95% CI: 1.02–1.56, p=0.03). Kaplan-Meier survival curve showed that the presence of high multimorbidity (CCI ≥4) had significantly lower all-cause mortality or rehospitalization survival rate (log-rank P <0.01) within 1 year (Figure 3).
 |
Table 2 Univariate and Multivariate Cox Regression Analyses for the Primary Outcome of All-Cause Death or Rehospitalization |
 |
Figure 3 Kaplan-Meier Analysis of all-cause mortality or rehospitalization Events According to the presence of High Multimorbidity in patients with AF. High multimorbidity = CCI ≥4. Abbreviation: CCI, Charlson comorbidity Index. |
Discussion
In the prospective cohort study, our principal findings are as follows: (1) The adverse health conditions (multimorbidity, frailty, malnutrition, cognitive impairment and polypharmacy) are common among the older people with AF; (2) Patients with all-cause death or rehospitalization present a higher burden of multimorbidity, heart failure and CKD, and lower SBP; (3) Feature of multimorbidity is associated with a higher risk of all-cause mortality and rehospitalization, even after adjustment for main domains of adverse health conditions.
The prevalence of AF is increasing due to the aging population and epidemiological trends, posing challenges to clinical and public health systems. Older people with AF often have comorbidities such as multimorbidity, frailty, malnutrition, cognitive impairment, and polypharmacy.2 These conditions are known as adverse health conditions or geriatric syndromes.13 In recent years, there has been significant focus on the impact of adverse health conditions or geriatric syndromes in patients with AF, as they greatly influence clinical management and the risk of adverse outcomes. The presence of these chronic comorbidities is referred to as “clinical complexity”.14 A large cohort study of European AF patients demonstrated that the presence of clinical complexity features like multimorbidity, frailty, and polypharmacy is associated with lower use of oral anticoagulants (OAC), lower quality of life, and higher use of healthcare resources. Clinical complexity features are linked to a higher risk of adverse outcomes, particularly in those with a higher burden of complexity features.15
Of the five adverse health conditions in our study, multimorbidity had the strongest association with all-cause mortality and rehospitalization in older people with AF. To the best of our knowledge, our study is the first to evaluate the prognostic impact of adverse health conditions on clinical outcomes in elderly patients with AF. Interestingly, a whole population study also showed that multimorbidity had the strongest association with mortality among the three adverse health conditions (multimorbidity, frailty, and disability).13 Multimorbidity is typically defined as the presence of two or more long-term conditions, although there is no clear consensus on the specific number or nature of diseases.16 It is associated with a higher risk of mortality, reduced functional status, increased healthcare expenditure and resource utilization, and adverse outcomes in elderly patients with AF.6,17–19 For example, a study by B.D. Jani et al found that AF participants with ≥4 comorbidities had a six-fold higher risk of mortality compared to participants without any comorbid long-term health conditions.18 Proietti et al evaluated the relationship between the CCI and AF patients, showing that CCI is independently associated with an increased risk of stroke, major bleeding, and all-cause death.19 The ChiOTEAF study in elderly Chinese patients with AF confirmed that multimorbidity was an in dependent predictor of adverse clinical outcomes.6 Furthermore, multimorbidity also influences therapeutic decision-making for AF patients. Previous studies have shown that multimorbidity is inversely associated with the prescription of OAC.20,21 However, it has been demonstrated that the use of non-vitamin K antagonist oral anticoagulants (NOACs) is safe and significantly improves survival in AF patients with multimorbidity.22,23 Rhythm control therapy, including antiarrhythmic drug therapy or AF ablation, is primarily recommended to improve the quality of life in symptomatic AF patients. Similarly, multimorbidity affects the decision to pursue rhythm control therapy. It is commonly assumed that the risk of rhythm control therapy will also be higher in patients with multiple comorbidities. However, newer evidence suggests that early rhythm control therapy reduces the risk of cardiovascular death, stroke, or hospitalization for heart failure or acute coronary syndrome in patients with recently diagnosed AF and a high comorbidity burden.24 Another aspect that needs attention is the relationship between the type of multimorbidity and AF, which is usually divided into cardiometabolic comorbidity and non-cardiometabolic comorbidity. Cardiovascular diseases and cardiovascular risk factors were used to define cardiometabolic conditions and included heart failure, coronary artery disease, stroke, hypertension, hyperlipidemia, and diabetes mellitus. Non-cardiometabolic conditions included arthritis, asthma, cancer, chronic kidney disease, chronic obstructive pulmonary disease, dementia, depression, and osteoporosis. Many studies, including ours, have found that the proportion of cardiometabolic comorbidity is higher in elderly AF.25,26 J’Neka S. Claxton et al further found that cardiometabolic comorbidities are more strongly associated with stroke, heart failure, and major bleeding than non-cardiometabolic comorbidities.25
In recent years, interest in the management of AF patients affected by multimorbidity has substantially increased. There is a growing trend towards an integrated or holistic approach to managing AF patients, with the Atrial Fibrillation Better Care (ABC) pathway being the most representative.27 The ABC pathway consists of three main pillars: “A“ for Avoid stroke (with Anticoagulants), “B” for Better symptom management (rate or rhythm control), and ”C” for Cardiovascular and Comorbidity risk optimization. Several studies have examined the impact of adherence/non-adherence to the ABC pathway. The first two post hoc analyses, based on clinical trials, showed that adhering to the ABC pathway is associated with a lower risk of adverse outcomes such as mortality, stroke/major bleeding/cardiovascular death, and hospitalization.28,29 The Mobile Atrial Fibrillation Application (mAFA)-II clinical trial, a prospective cluster randomized trial conducted in China, demonstrated a significant reduction in the primary outcome when using the ABC pathway intervention through a mHealth App compared to usual care.30 A review of twelve studies on the ABC pathway consistently showed a statistically significant reduction in the risk of stroke, myocardial infarction, and mortality among patients who adhered to the pathway.31 Another meta-analysis also found that patients treated according to the ABC pathway showed a lower risk of all-cause death, cardiovascular death, stroke and major bleeding, with moderate heterogeneity.32 Additionally, an analysis of the ESC-EHRA EURObservational Research Programme (EORP) Atrial Fibrillation General Long-Term Registry data demonstrated that an ABC-adherent approach reduced the risk of major outcomes in clinically complex AF patients.14 In addition, as an important part of the ABC pathway, the integrated care of AF patients has received more and more attention in recent years. The integrated care intervention consisted of (1) quarterly AF check-ups by trained nurses in primary care, also focusing on possibly interfering comorbidities, (2) monitoring of anticoagulation therapy in primary care, and finally (3) easy-access availability of consultations from cardiologists and anticoagulation clinics. Clinical study has confirmed that integrated care can reduce the risk of all-cause death, cardiovascular death, etc.33 Moreover, the higher the risk and the more complications the patient has, the greater the benefit from comprehensive care.34,35
However, implementing the ABC pathway in clinical practice poses challenges. A European study found that fewer than one-third of AF patients demonstrated complete adherence to the ABC pathway.14 Barriers to referring AF patients to specialist services for comorbidities include a lack of integrated care models, organizational/institutional issues, and patient adherence problems.36 To address these challenges, it is necessary to establish clinical workshops where cardiologists and nurses can collaborate with other specialists to achieve patient-centered multidisciplinary management. It is also important to involve empowered patients, families, and caregivers. In line with this approach, the Horizon 2020 research program launched EHRA-PATHS,37 “Addressing multimorbidity in elderly atrial fibrillation patients through interdisciplinary, tailored, patient-centered care pathways”, to implement and validate this approach. Meanwhile, the “Atrial fibrillation integrated approach in frail, multimorbid, and polymedicated older people” (AFFIRMO) Programme has been funded by the European Union through the Horizon 2020 research programme.38 The AFFIRMO Programme will offer novel evidence on specific care models for the general multimorbid AF population. This will aid in improving clinical management and reducing the risks of major clinical adverse outcomes in a rapidly growing and significant patient group.
Our study has some limitations. Firstly, while being a multicenter study, the sample size is relatively small, and the participants are limited to inpatients in tertiary hospitals. Secondly, While we used a multivariate Cox regression model to adjust for potential confounders, residual or unknown confounding factors might still be present. For instance, re-hospitalizations probably constituted a significant portion of the events. If these rehospitalizations are weighed similarly to other events, the results could be skewed due to their higher frequency. Additionally, the lack of association for other health conditions, such as frailty, could be attributed to limited statistical power to detect differences. It is also important to note that frailty and multimorbidity often coexist, which could further complicate the analysis. Thirdly, the follow-up period for this study was only one year, and further studies with larger sample sizes and longer follow-up periods are necessary.
Conclusion
Among adverse health conditions in older adults with atrial fibrillation (AF), multimorbidity appears to be a significant determinant of adverse clinical outcomes. Evidence suggests that multimorbidity may be an independent predictor of such outcomes. Therefore, it is advisable to consider an integrated approach that emphasizes the holistic management of comorbidities in older adults with AF.
Abbreviations
AF, Atrial fibrillation; BMI, Body mass index; CCI, Charlson comorbidity index; CDT, Clock drawing test; CGA-FI, Comprehensive geriatric assessment-frailty index; hsCRP, High sensitivity C-reactive protein; LAD, Left atrial diameter; LVEF, Left ventricular ejection fraction; MMSE, Mini-mental state examination; NT-proBNP, N-terminal pro-brain natriuretic peptide.
Data Sharing Statement
Raw data are available upon reasonable request with the corresponding author.
Ethics Approval and Consent to Participate
The trial was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, and the research protocol was approved by the Ethics Committee of Beijing Hospital (ID number: 2018BJYYEC-121-02). Written informed consent was obtained from the patients or their legal representatives.
Acknowledgments
The authors thank the study coordinators for their efforts in collecting clinical data and ensuring the accuracy and completeness of the data.
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project has received funding from National High Level Hospital Clinical Research Funding (BJ-2023-162).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schnabel RB, Yin X, Gona P, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham heart study: a cohort study. Lancet. 2015;386(9989):154–162. doi:10.1016/S0140-6736(14)61774-8
2. Wu J, Nadarajah R, Nakao YM, et al. Temporal trends and patterns in atrial fibrillation incidence: a population-based study of 3.4 million individuals. Lancet Reg Health-Eu. 2022;17:100386.
3. Gallagher C, Nyfort-Hansen K, Rowett D, et al. Polypharmacy and health outcomes in atrial fibrillation: a systematic review and meta-analysis. Open Heart. 2020;7(1):e1257. doi:10.1136/openhrt-2020-001257
4. Proietti M, Romiti GF, Raparelli V, et al. Frailty prevalence and impact on outcomes in patients with atrial fibrillation: a systematic review and meta-analysis of 1,187,000 patients. Ageing Res Rev. 2022;79:101652. doi:10.1016/j.arr.2022.101652
5. Liu J, Chai K, Zhu W, et al. Implication of different frailty criteria in older people with atrial fibrillation: a prospective cohort study. Bmc Geriatr. 2023;23(1):604. doi:10.1186/s12877-023-04330-1
6. Kotalczyk A, Guo Y, Wang Y, Lip G, Botc O. Impact of multimorbidity and polypharmacy on clinical outcomes of elderly Chinese patients with atrial fibrillation. J Clin Med. 2022;11(5):1370. doi:10.3390/jcm11051370
7. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
8. Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton frail scale. Age Ageing. 2006;35(5):526–529. doi:10.1093/ageing/afl041
9. Rubenstein LZ, Harker JO, Salva A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A-Biol. 2001;56(6):M366–72. doi:10.1093/gerona/56.6.M366
10. Folstein MF, Folstein SE, McHugh PR. ”Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198.
11. Yang L, Yan J, Jin X, et al. Screening for dementia in older adults: comparison of mini-mental state examination, mini-cog, clock drawing test and AD8. PLoS One. 2016;11(12):e168949. doi:10.1371/journal.pone.0168949
12. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. Bmc Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
13. Dugravot A, Fayosse A, Dumurgier J, et al. Social inequalities in multimorbidity, frailty, disability, and transitions to mortality: a 24-year follow-up of the Whitehall II cohort study. Lancet Public Health. 2020;5(1):e42–50. doi:10.1016/S2468-2667(19)30226-9
14. Romiti GF, Proietti M, Vitolo M, et al. Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational research programme in AF general long-term registry. Bmc Med. 2022;20(1):326. doi:10.1186/s12916-022-02526-7
15. Proietti M, Romiti GF, Corica B, et al. Features of clinical complexity in European patients with atrial fibrillation: a report from a European observational prospective AF registry. Curr Prob Cardiology. 2023;48(8):101752. doi:10.1016/j.cpcardiol.2023.101752
16. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
17. Chamberlain AM, Alonso A, Gersh BJ, et al. Multimorbidity and the risk of hospitalization and death in atrial fibrillation: a population-based study. Am Heart J. 2017;185:74–84. doi:10.1016/j.ahj.2016.11.008
18. Jani BD, Nicholl BI, McQueenie R, et al. Multimorbidity and co-morbidity in atrial fibrillation and effects on survival: findings from UK Biobank cohort. Europace. 2018;20(FI_3):f329–36. doi:10.1093/europace/eux322
19. Proietti M, Esteve-Pastor MA, Rivera-Caravaca JM, et al. Relationship between multimorbidity and outcomes in atrial fibrillation. Exp Gerontol. 2021;153:111482. doi:10.1016/j.exger.2021.111482
20. Proietti M, Marzona I, Vannini T, et al. Long-term relationship between atrial fibrillation, multimorbidity and oral anticoagulant drug use. Mayo Clin Proc. 2019;94(12):2427–2436. doi:10.1016/j.mayocp.2019.06.012
21. Dalgaard F, Xu H, Matsouaka RA, et al. Management of atrial fibrillation in older patients by morbidity burden: insights from get with the guidelines-atrial fibrillation. J Am Heart Assoc. 2020;9(23):e17024. doi:10.1161/JAHA.120.017024
22. Alexander KP, Brouwer MA, Mulder H, et al. Outcomes of apixaban versus warfarin in patients with atrial fibrillation and multi-morbidity: insights from the ARISTOTLE trial. AM HEART J. 2019;208:123–131. doi:10.1016/j.ahj.2018.09.017
23. Nicolau AM, Corbalan R, Nicolau JC, et al. Efficacy and safety of edoxaban compared with warfarin according to the burden of diseases in patients with atrial fibrillation: insights from the ENGAGE AF-TIMI 48 trial. Eur Heart J-Card Pha. 2020;6(3):167–175.
24. Rillig A, Borof K, Breithardt G, et al. Early rhythm control in patients with atrial fibrillation and high comorbidity burden. Circulation. 2022;146(11):836–847. doi:10.1161/CIRCULATIONAHA.122.060274
25. Claxton JS, Chamberlain AM, Lutsey PL, et al. Association of multimorbidity with cardiovascular endpoints and treatment effectiveness in patients 75 years and older with atrial fibrillation. Am J Med. 2020;133(10):e554–67. doi:10.1016/j.amjmed.2020.03.038
26. Lu Z, Nlapto N, Tilly MJ, et al. Burden of cardiometabolic disorders and lifetime risk of new-onset atrial fibrillation among men and women: the Rotterdam study. Eur J Prev Cardiol. 2024;31:1141–1149. doi:10.1093/eurjpc/zwae045
27. Lip G. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. 2017;14(11):627–628. doi:10.1038/nrcardio.2017.153
28. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip G. Improved outcomes by integrated care of anticoagulated patients with atrial fibrillation using the simple ABC (Atrial Fibrillation Better Care) Pathway. Am J Med. 2018;131(11):1359–1366. doi:10.1016/j.amjmed.2018.06.012
29. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip G. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc. 2020;9(10):e14932. doi:10.1161/JAHA.119.014932
30. Yao Y, Guo Y, Lip G. The effects of implementing a mobile health-technology supported pathway on atrial fibrillation-related adverse events among patients with multimorbidity: the mAFA-II randomized clinical trial. JAMA Network Open. 2021;4(12):e2140071. doi:10.1001/jamanetworkopen.2021.40071
31. Stevens D, Harrison SL, Kolamunnage-Dona R, Lip G, Lane DA. The atrial fibrillation better care pathway for managing atrial fibrillation: a review. Europace. 2021;23(10):1511–1527. doi:10.1093/europace/euab092
32. Romiti GF, Pastori D, Rivera-Caravaca JM, et al. Adherence to the ‘atrial fibrillation better care’ pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemostasis. 2022;122(3):406–414. doi:10.1055/a-1515-9630
33. van den Dries CJ, van Doorn S, Rutten FH, et al. Integrated management of atrial fibrillation in primary care: results of the ALL-IN cluster randomized trial. Eur Heart J. 2020;41(30):2836–2844. doi:10.1093/eurheartj/ehaa055
34. Trinks-Roerdink EM, Geersing GJ, van den Dries CJ, et al. Integrated care in patients with atrial fibrillation- A predictive heterogeneous treatment effect analysis of the ALL-IN trial. PLoS One. 2023;18(10):e292586. doi:10.1371/journal.pone.0292586
35. Proietti M, Vitolo M, Lip G. Integrated care and outcomes in patients with atrial fibrillation and comorbidities. Eur J Clin Invest. 2021;51(6):e13498. doi:10.1111/eci.13498
36. Lee G, Baker E, Collins R, Merino JL, Desteghe L, Heidbuchel H. The challenge of managing multimorbid atrial fibrillation: a pan-European European Heart Rhythm Association (EHRA) member survey of current management practices and clinical priorities. Europace. 2022;24(12):2004–2014. doi:10.1093/europace/euac136
37. Heidbuchel H, Van Gelder IC, Desteghe L. ESC and EHRA lead a path towards integrated care for multimorbid atrial fibrillation patients: the Horizon 2020 EHRA-PATHS project. Eur Heart J. 2022;43(15):1450–1452. doi:10.1093/eurheartj/ehab672
38. Johnsen SP, Proietti M, Maggioni AP, Lip G. A multinational European network to implement integrated care in elderly multimorbid atrial fibrillation patients: the AFFIRMO Consortium. Eur Heart J. 2022;43(31):2916–2918. doi:10.1093/eurheartj/ehac265
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disease Progression and Age as Factors Underlying Multimorbidity in Patients with COPD: Results from COSYCONET
Alter P, Kahnert K, Trudzinski FC, Bals R, Watz H, Speicher T, Söhler S, Andreas S, Welte T, Rabe KF, Wouters EFM, Sassmann-Schweda A, Wirtz H, Ficker JH, Vogelmeier CF, Jörres RA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1703-1713
Published Date: 29 July 2022
Independent and Joint Association of Statin Therapy with Adverse Outcomes in Heart Failure Patients with Atrial Fibrillation Treated with Cardiac Resynchronization Therapy

Yu Y, Ding L, Deng Y, Huang H, Cheng S, Cai C, Gu M, Chen X, Ning X, Niu H, Hua W
Journal of Inflammation Research 2022, 15:6645-6656
Published Date: 9 December 2022
Prognosis of Older Adult Patients Suffering from Atrial Fibrillation and Hypokalemia
Wang XD, Wang Y, Liu J, Yao JW, Zhang J, Zhang YN
Clinical Interventions in Aging 2023, 18:1363-1371
Published Date: 17 August 2023
Bilirubin Elevation During Hospitalization Post Radiofrequency Catheter Ablation of Persistent Atrial Fibrillation: Variation Trend, Related Factors, and Relevance to 1-Year Recurrence
Shao JM, Shen B, Zhou ZX, D'Angelo L, James SM, Lin JF, Zheng C
Clinical Interventions in Aging 2024, 19:817-825
Published Date: 13 May 2024