")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Impact of Antiviral Treatment on Survival in HBV-Related Intrahepatic Cholangiocarcinoma Patients After Hepatectomy: A 14-Year Retrospective Follow-Up Study Based on the Propensity Score Matching Method
Authors Chen Z, Zhang H, Zhang L, Han G, Zhang Y, Wu J, Li X, Mu X, Wang X
Received 5 February 2025
Accepted for publication 3 June 2025
Published 11 June 2025 Volume 2025:21 Pages 869—884
DOI https://doi.org/10.2147/TCRM.S520629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Zhiqiang Chen,* Hui Zhang,* Long Zhang, Guoyong Han, Yao Zhang, Jindao Wu, Xiangcheng Li, Xiaoxin Mu, Xuehao Wang
Hepatobiliary Center, The First Affiliated Hospital of Nanjing Medical University, Key Laboratory of Liver Transplantation, Chinese Academy of Medical Sciences, NHC Key Laboratory of Hepatobiliary Cancers, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuehao Wang; Xiaoxin Mu, Hepatobiliary Center, The First Affiliated Hospital of Nanjing Medical University, Key Laboratory of Liver Transplantation, Chinese Academy of Medical Sciences, NHC Key Laboratory of Hepatobiliary Cancers, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Hepatitis B virus infection is one of the most common risk factors leading to the development of intrahepatic cholangiocarcinoma (ICC). This study aims to determine the impact of antiviral treatment (AVT) on the survival outcomes of ICC patients with hepatitis B virus infection.
Patients and Methods: This retrospective study included ICC patients who had HBV infection and underwent hepatectomy from May 2009 to June 2023 at a single medical center. Patients’ baseline characteristics were analyzed, and the 14-year follow-up data were investigated using Kaplan-Meier curves and multivariable Cox proportional hazards regression models. The propensity score matching method was performed to balance the baseline differences between the AVT group and the non-AVT group.
Results: A total of 229 patients were finally enrolled in the analysis. In the total cohort, 81 patients were classified into the AVT group and 148 patients into the non-AVT group. Kaplan-Meier curves showed that the AVT group exhibited prolonged overall survival and recurrence-free survival compared to the non-AVT group. Cox proportional hazards regression models revealed that AVT was an independent prognostic factor for both overall survival (HR 0.453, 95% CI: 0.280– 0.732) and recurrence-free survival (HR 0.659, 95% CI: 0.436– 0.997). A 1:1 nearest-neighbor matching algorithm was adopted, and 64 pairs of AVT and non-AVT patients were included in the propensity score matching cohort. Multivariable survival analyses confirmed AVT as a significant predictor for a favorable overall survival (HR 0.277, 95% CI: 0.147– 0.519), but no statistical significance for recurrence-free survival was observed between the AVT group and the non-AVT group after propensity score matching.
Conclusion: We analyzed the long-term follow-up data for ICC patients with hepatitis B virus infection who underwent hepatectomy. Notably, AVT exhibited a beneficial impact on overall survival for these postoperative ICC patients. However, our findings indicated no statistically significant effect of AVT on recurrence-free survival.
Keywords: intrahepatic cholangiocarcinoma, antiviral treatment, overall survival, recurrence-free survival, propensity score matching
Introduction
Intrahepatic cholangiocarcinoma (ICC) is the second most common type of primary liver cancer and contributes 10%–15% of the world's total liver cancer burden.1 ICC remains a fatal malignancy, and most patients are diagnosed late in the disease state. Surgical resection represents the only potential curative therapeutic option, but only 20%–30% of ICC patients present with resectable disease.2 Even after surgical resection, the survival outcomes are still dismal.3
The last two decades have witnessed a rapid increase of 120% in the incidence of ICC globally.4 Consistently, ICC-related mortality exhibits an upward trend in most countries.5 The precise reasons for this recent increase are not yet fully understood but may be associated with established predisposing factors. ICC usually arises in the setting of chronic inflammation and the resultant cholangiocyte injury. Hepatitis B virus (HBV) infection has been established as a risk factor for the development of ICC.6 The linkage between HBV infection and the development of ICC has been confirmed by abundant epidemiological data, with an odds ratio of approximately 4.5.7 Antiviral treatment (AVT) has been suggested to decrease the incidence of HBV-infected ICC.8,9 However, the impact of AVT on the survival outcomes of HBV-infected ICC patients remains largely underexplored.
Propensity score matching (PSM) stands out as a commonly used and well-established strategy to reduce confounding biases in observational studies.10 The propensity score represents the probability that a subject will receive the treatment, given their baseline covariates. PSM offers a practical approach to providing consistent estimators of causal effects.11 Multivariable Cox regression analysis is a powerful tool that is frequently used in studies of clinical outcomes. As reported in previous studies, PSM could first balance patient characteristics between different groups, followed by Cox regression to analyze survival differences.12–14
Using 14-year follow-up data from our center, this study performed PSM to balance the potential bias. We analyzed the survival data and aimed to evaluate the effects of AVT on the long-term survival outcomes of ICC patients with HBV infection.
Materials and Methods
Patients
Data for consecutive ICC patients who had HBV infection and underwent hepatectomy between May 2009 and June 2023 at the First Affiliated Hospital of Nanjing Medical University were collected. The diagnosis of ICC was histologically confirmed by two independent pathologists. The definition of HBV infection required that the patients were positive for HBV surface antigen (HBsAg) or HBV core antibody (HBcAb) as previously described.9
Exclusion criteria were: (1) received preoperative anticancer treatment, including chemotherapy, targeted therapy, immunotherapy, TACE, radiotherapy, ablation; (2) incomplete clinicopathological characteristics; (3) hepatitis C virus infection; (4) lost to follow-up within 90 days after surgery.
The study received approval from the Ethics Committees of the First Affiliated Hospital of Nanjing Medical University (No. 2024-SRFA-893). Due to the retrospective nature of this study and without any specific intervention, the informed consent has been agreed to be waived. This study strictly kept the patients’ information confidential. The present study complied with the Declaration of Helsinki.
Data Collection
Clinicopathological characteristics of the enrolled patients were thoroughly documented, including gender, age, HBsAg, HBeAg, HBV DNA load, smoke, alcohol, hypertension, diabetes, platelet (PLT), albumin (ALB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (AKP), γ-glutamyltransferase (GGT), total bilirubin (TBIL), direct bilirubin (DBIL), prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen, CA19-9, ascites, cirrhosis, tumor encapsulation, tumor size, tumor number, satellite nodules, major hepatectomy, intraoperative blood transfusion, postoperative complications, tumor differentiation, microvascular invasion (MVI), neural invasion, T stage, N stage, TNM stage, AVT. Albumin-bilirubin grade (ALBI) was assessed with ALB and TBIL as previously reported.15 Major hepatectomy was defined as the removal of three or more Couinaud’s segments.16,17 Patients who received any of the nucleos(t)ide analogues, including entecavir, adefovir, lamivudine, telbivudine, tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF), tenofovir amibufenamide (TMF), were classified into the AVT group. Patient follow-up was carried out regularly to record the overall survival (OS) and recurrence-free survival (RFS).
Statistical Analysis
Statistical analysis was performed with R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria) and IBM SPSS software (version 27; IBM Corp., Armonk, NY, USA). Categorical variables were summarized using frequency counts with percentages and compared using Fisher’s exact test or chi-squared test as appropriate. PSM was performed to balance the baseline differences between two groups as previously reported.18,19 We included all baseline confounders in the PSM to reduce the imbalance in the AVT and non-AVT groups. A propensity score was calculated for each patient using a logistic regression model based on the following variables: gender, age, HBsAg, HBeAg, HBV DNA load, smoke, alcohol, hypertension, diabetes, PLT, albumin, ALT, AST, AKP, GGT, TBIL, DBIL, ALBI, PT, APTT, fibrinogen, CA19-9, ascites, cirrhosis, tumor encapsulation, tumor size, tumor number, satellite nodules, major hepatectomy, intraoperative blood transfusion, postoperative complications, tumor differentiation, MVI, neural invasion, T stage, N stage, TNM stage. A 1:1 nearest-neighbor matching algorithm with a caliper width of 0.2 without replacement was adopted.
Survival outcomes between the two groups were examined using the Kaplan-Meier curves and compared with the Log rank test. Only the statistically significant variables from the Log rank test were included in the multivariable Cox regression model. Cox proportional hazards regression models were adopted to determine the independent prognostic predictors and calculate their hazard ratios (HRs) and 95% confidence intervals (CIs). We checked the proportionality assumption using Schoenfeld residuals. In certain cases, the assumption was violated, we therefore interpreted the HRs as weighted averages of the time-varying HRs over the entire follow-up period, as previously reported.20–22 A two-tailed P < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 229 patients were finally included in this study. The flow diagram of patient enrollment is shown in Figure 1. Among the enrolled patients, there were 81 (35.4%) patients in the AVT group and 148 (64.6%) patients in the non-AVT group. Parameters including gender, age, HBeAg, HBV DNA load, smoke, alcohol, hypertension, diabetes, albumin, ALT, AST, AKP, TBIL, DBIL, ALBI, PT, APTT, CA19-9, ascites, tumor encapsulation, tumor number, satellite nodules, intraoperative blood transfusion, postoperative complications, tumor differentiation, MVI, T stage, and N stage were comparable between the AVT group and the non-AVT group (all P > 0.05). With regard to several characteristics including HBsAg, PLT, GGT, fibrinogen, cirrhosis, tumor size, major hepatectomy, neural invasion, and TNM stage, significant differences between the AVT group and the non-AVT group were detected. The clinicopathological features of the total cohort are demonstrated in Table 1.
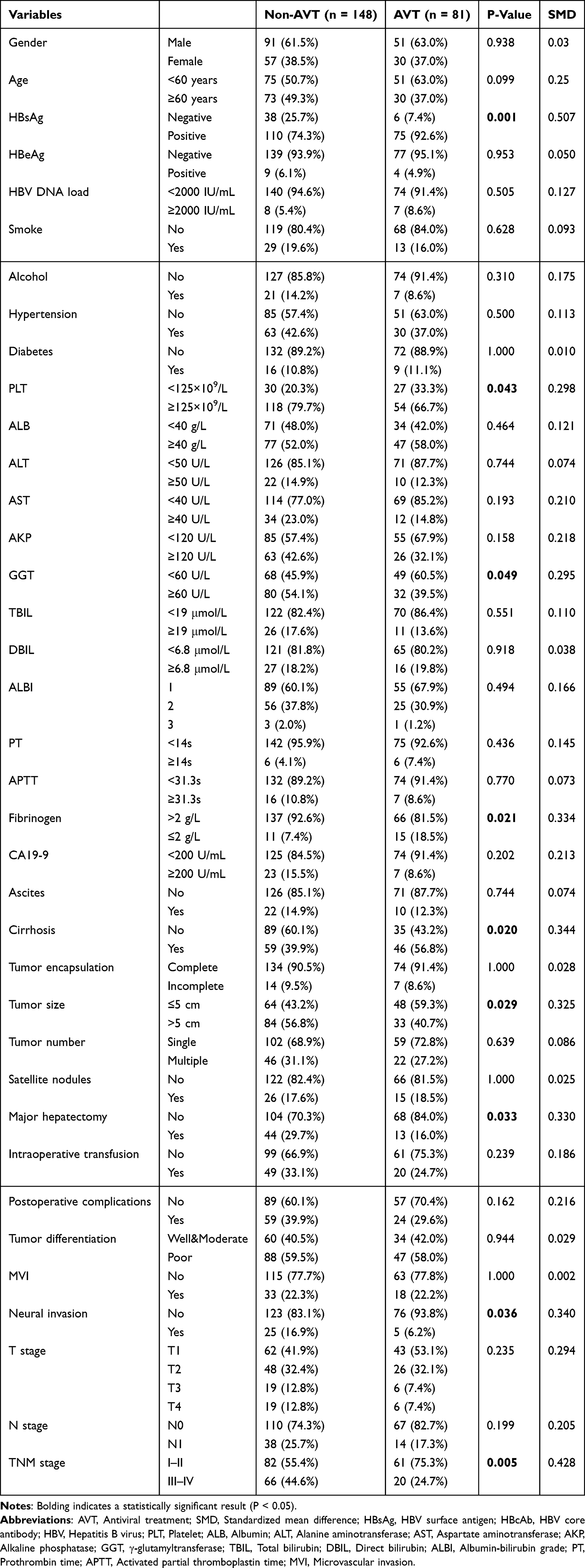 |
Table 1 Baseline Characteristics by AVT in the Total Cohort |
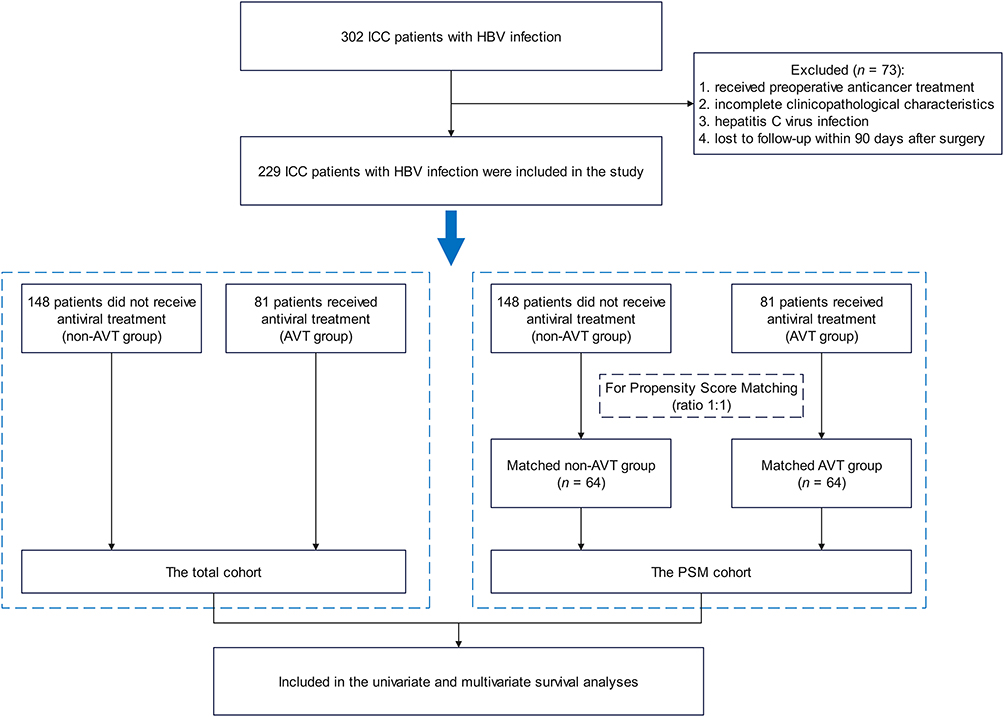 |
Figure 1 Flow diagram of this study. Abbreviations: ICC, Intrahepatic cholangiocarcinoma; HBV, Hepatitis B virus; AVT, Antiviral treatment; PSM, Propensity score matching. |
Survival Analysis in the Total Cohort
In the total cohort, the median follow-up time for OS was 38.34 months (95% CI: 24.93–51.75 months). The median OS for the AVT group was not reached, while the median OS for the non-AVT group was 19.06 months (95% CI: 12.70–25.42 months).
Median follow-up time for RFS was 27.43 months (95% CI: 16.88–37.98 months). Median RFS for the AVT group and the non-AVT group was 21.36 months (95% CI: 0–61.71 months) and 11.56 months (95% CI: 6.51–16.61 months), respectively.
The Kaplan-Meier curves of OS and RFS in the two groups are shown in Supplementary Figure 1. AVT was associated with a favorable OS (P < 0.0001) and RFS (P = 0.023). As demonstrated in Supplementary Table 1, AVT remained as an independent predictor for OS (HR 0.453, 95% CI: 0.280–0.732, P < 0.001) in the multivariable regression analysis. AVT was associated with a prolonged RFS for ICC patients in the multivariable regression analysis (HR 0.659, 95% CI: 0.436–0.997, P = 0.048).
Survival Analysis in the PSM Cohort
After balancing with PSM, none of the clinicopathological characteristics showed a statistical difference (Table 2). The balanced data after PSM is shown in a distribution figure (Figure 2). A total of 128 patients were included as the PSM cohort. The median follow-up time for OS and RFS was 42.22 months (95% CI: 30.14–54.30 months) and 36.70 months (95% CI: 25.42–47.99 months), respectively. Median OS and RFS for the AVT group were not reached, while the median OS and RFS for the non-AVT group were 22.93 months (95% CI: 15.57–30.30 months) and 33.02 months (95% CI: 1.48–64.57 months), respectively.
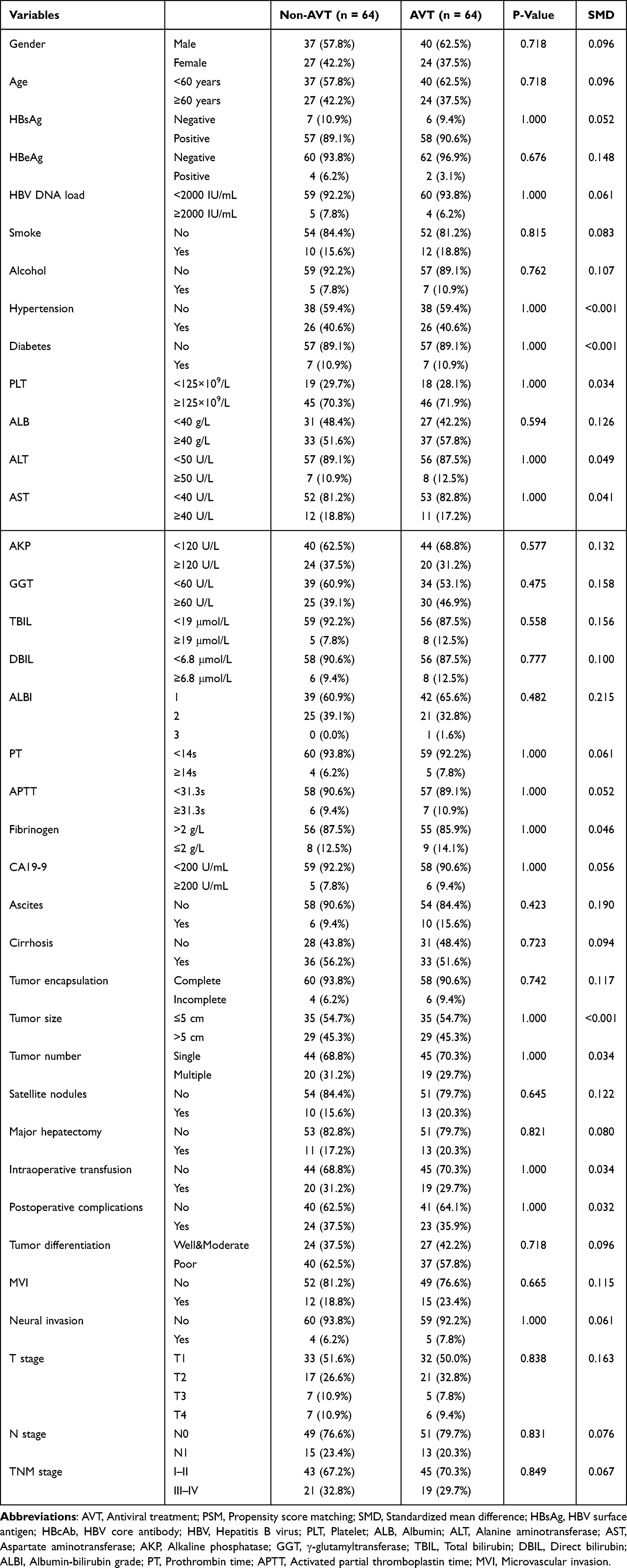 |
Table 2 Baseline Characteristics by AVT in the PSM Cohort |
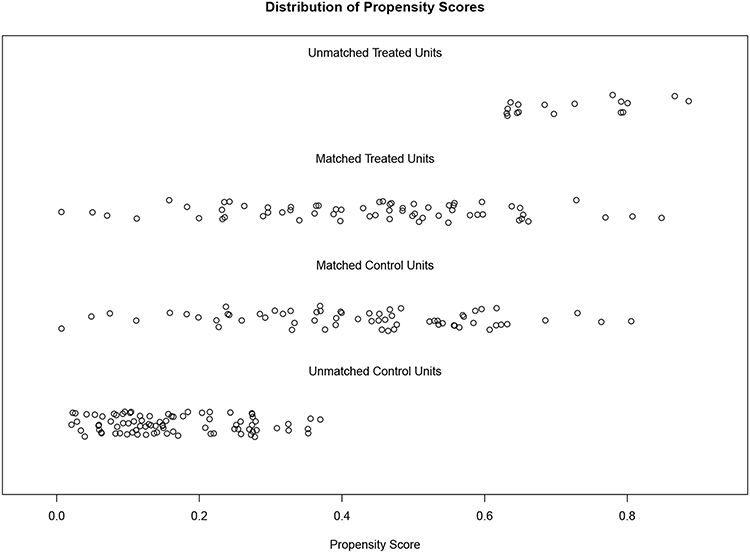 |
Figure 2 Distribution of propensity scores of the antiviral treatment group and the non- antiviral treatment group before and after propensity score matching. |
As illustrated in Figure 3A, Kaplan-Meier analysis revealed that patients in the AVT group were associated with better OS than those in the non-AVT group (P < 0.001). Multivariable analysis further confirmed that AVT was a significant predictor for a favorable OS (HR 0.277, 95% CI: 0.147–0.519, P < 0.001; Table 3). However, neither Kaplan-Meier curves nor multivariable Cox analysis indicated a statistical significance of RFS between the AVT group and the non-AVT group in the PSM cohort (Figure 3B and Table 3).
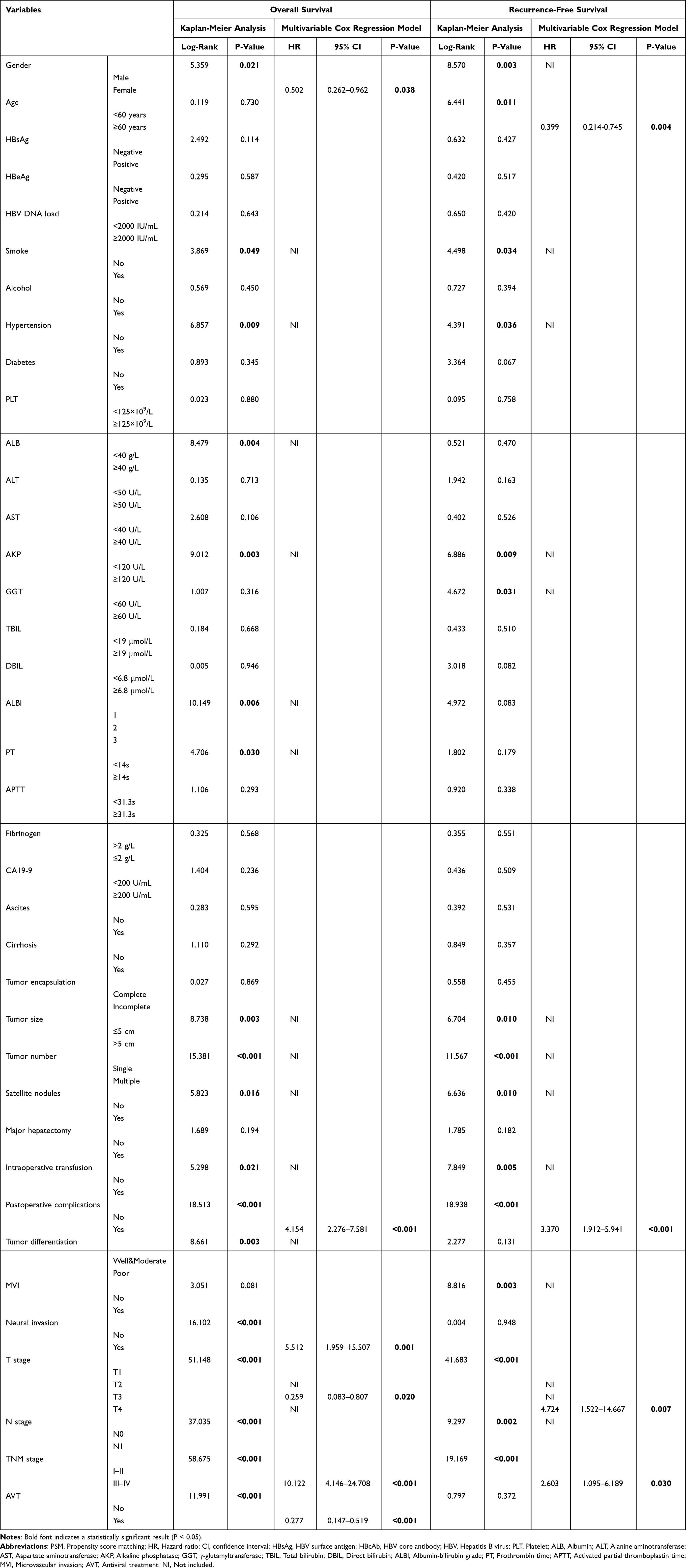 |
Table 3 Survival Analyses in the PSM Cohort |
 |
Figure 3 Kaplan-Meier curves of overall survival (A) and recurrence-free survival (B) between the AVT group and the non-AVT group in the propensity score matching cohort. Abbreviation: AVT, Antiviral treatment. |
Discussion
ICC is a heterogeneous disease with different molecular signatures, and consequently, different patient outcomes.23 Multiple risk factors have been identified for ICC, such as choledochal cysts, biliary stones, cirrhosis, viral hepatitis, and parasitic infections.24 Although it has been established that HBV infection confers an increased risk of ICC, especially in Eastern countries,24,25 the survival impact of HBV infection remains controversial. On one hand, HBV-infected ICC has shorter disease-free survival than the ICC patients without HBV infection, while the OS exhibits no significant difference between the two groups.26 On the other hand, HBV-positive ICC has a better OS than HBV-negative ICC because HBV infection could activate innate and acquired immune responses and enhance the antitumor activity.27 These results reflect the complexity of HBV in ICC pathogenesis and prognosis. Given that AVT could suppress HBV replication and alleviate liver damage, we determined to further elucidate the role of AVT in HBV-infected ICC prognosis, providing clues for improving survival of HBV-infected ICC patients.
In this study, we investigated the 14-year follow-up data for ICC patients who underwent surgical treatment in our center. The potential bias of baseline variables between AVT and non-AVT groups was controlled by the PSM method. In the total cohort, the AVT group consisted of 81 patients and the non-AVT group comprised 148 patients. After PSM, 64 paired ICC patients were included in the subsequent analyses.
Kaplan-Meier curves with Log rank test and Cox proportional hazards regression models were adopted to evaluate the effects of AVT on the survival outcomes for ICC patients with HBV infection. Kaplan-Meier Log rank testing showed significant disparity in OS between the AVT group and the non-AVT group in the total cohort (P < 0.0001) and the PSM cohort (P < 0.001). As revealed by multivariable Cox proportional hazards regression models, AVT could reduce the OS of ICC patients in the total cohort (HR 0.453, 95% CI: 0.280–0.732, P < 0.001) as well as the PSM cohort (HR 0.277, 95% CI: 0.147–0.519, P < 0.001). Similarly, one retrospective study showed that AVT provides a significant benefit to ICC patients compared to patients with high HBV DNA load who are left untreated (5-year OS rate: 43% vs 20.5%, P < 0.001).9
Intriguingly, AVT improved RFS in the total cohort (Kaplan-Meier Log rank testing: P = 0.023; multivariable Cox regression model: HR 0.659, 95% CI: 0.436–0.997, P = 0.048), while no statistical significance was detected after PSM (P > 0.05). One previous study suggested that AVT is associated with a lower 5-year recurrence compared to ICC patients with high HBV DNA load (70.5% vs 86.5%, P < 0.001).9 In the present study, we performed PSM to balance the potential confounding variables and our results showed that AVT could lead to a prolonged OS but have little effect on RFS. Subgroup analyses stratified by HBV DNA load yielded no statistical differences in RFS between the AVT group and the non-AVT group both in the total cohort (HBV DNA load < 2000 IU/mL: HR 0.67, 95% CI: 0.45–1.00, P = 0.052; HBV DNA load ≥ 2000 IU/mL: HR 0.36, 95% CI: 0.06–2.06, P = 0.253) and the PSM cohort (HBV DNA load < 2000 IU/mL: HR 0.79, 95% CI: 0.47–1.35, P = 0.389; HBV DNA load ≥ 2000 IU/mL: HR 0.91, 95% CI: 0.06–15.10, P = 0.949).
HBV infection is prevalent in ICC patients in high hepatitis B endemic areas. Proteomic and single-cell transcriptomic data indicates that HBV-associated ICC is characterized with decreased cell-cell junction and increased epithelial-mesenchymal transition.28 HBV-related ICC may originate from hepatocytes, contributing to the similar clinical features of HBV-related ICC and HBV-related hepatocellular carcinoma (HCC).26 Therefore, studies on HBV-infected HCC might provide a clue to the association between AVT and RFS in HBV-infected ICC. A nationwide study showed that the recurrence rate in postoperative HCC patients is similar between the AVT group and the non-AVT group, which is further confirmed by the subsequent subgroup analyses.29 These data prompted us to hypothesize that the non-significant effect of AVT on RFS in HBV-infected ICC patients may result from the similar process of carcinogenesis between HBV-infected ICC and HBV-infected HCC. However, another study revealed that AVT is associated with decreased 6-month, 1-year, and 2-year HCC recurrence when compared with the non-AVT group.30 Nonetheless, more large-scale studies are needed to clarify the effects of AVT on RFS for HBV-infected ICC patients.
There are still several limitations in this study. First, the study was restrained by its retrospective nature. Second, the data from our single medical center was relatively limited, and multi-center data is needed to decrease the potential selection bias. Third, other potential confounding variables which might have prognostic roles were not included and adjusted. More thorough approaches to mitigating confounding variables are needed in future studies. Fourth, given the potential for a high number of determinant covariables compared to the sample size, the event-per-covariate in the multivariable Cox regression model of our study was relatively stretched. However, previous studies indicate that the rule of one covariate per ten events in Cox regression might be safely relaxed but might also be interpreted with caution.31–33
Conclusion
In the present study, we retrospectively analyzed the 14-year follow-up data on HBV-infected ICC patients. After balancing the confounding factors using the PSM method, we demonstrated that AVT independently predicted a favorable OS but it had no statistically significant effect on RFS in ICC patients who underwent hepatectomy. More large-scale studies exploring subgroup variations or determining residual confounding will be valuable to further clarify the role of AVT in RFS.
Abbreviations
ICC, Intrahepatic cholangiocarcinoma; HBV, Hepatitis B virus; AVT, Antiviral treatment; PSM, Propensity score matching; HBsAg, HBV surface antigen; HBcAb, HBV core antibody; PLT, Platelet; ALB, Albumin; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; AKP, Alkaline phosphatase; GGT, γ-glutamyltransferase; TBIL, Total bilirubin; DBIL, Direct bilirubin; PT, Prothrombin time; APTT, Activated partial thromboplastin time; MVI, Microvascular invasion; ALBI, Albumin-bilirubin grade; TDF, Tenofovir disoproxil fumarate; TAF, Tenofovir alafenamide; TMF, Tenofovir amibufenamide; OS, Overall survival; RFS, Recurrence-free survival; HR, Hazard ratio; CI, Confidence interval; HCC, Hepatocellular carcinoma; NI, Not included.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding authors upon reasonable request.
Ethic Approval
The study received approval from the Ethics Committees of the First Affiliated Hospital of Nanjing Medical University (No. 2024-SRFA-893). Due to the retrospective nature of this study and without any specific intervention, the informed consent has been agreed to be waived. This study strictly kept the patients’ information confidential. The present study complied with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank all the patients for their participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82472768, 82002556), the Natural Science Foundation of the Jiangsu Higher Education Institutions of China (24KJB320006), and the Natural Science Foundation of Jiangsu Province (BK20201083).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Moris D, Palta M, Kim C, Allen PJ, Morse MA, Lidsky ME. Advances in the treatment of intrahepatic cholangiocarcinoma: an overview of the current and future therapeutic landscape for clinicians. CA Cancer J Clin. 2023;73(2):198–222. doi:10.3322/caac.21759
3. Endo Y, Sasaki K, Moazzam Z, et al. Higher Tumor Burden Status Dictates the Impact of Surgical Margin Status on Overall Survival in Patients Undergoing Resection of Intrahepatic Cholangiocarcinoma. Ann Surg Oncol. 2023;30(4):2023–2032. doi:10.1245/s10434-022-12803-7
4. Thi Vu Q, Nishimura Y, Harada K, et al. International trends in biliary tract cancer-related mortality, 2000-2022: an observational study of the World Health Organization mortality database. Hepatology. 2024;2024:1. doi:10.1097/hep.0000000000001200
5. Florio AA, Ferlay J, Znaor A, et al. Global trends in intrahepatic and extrahepatic cholangiocarcinoma incidence from 1993 to 2012. Cancer. 2020;126(11):2666–2678. doi:10.1002/cncr.32803
6. Fwu CW, Chien YC, You SL, et al. Hepatitis B virus infection and risk of intrahepatic cholangiocarcinoma and non-Hodgkin lymphoma: a cohort study of parous women in Taiwan. Hepatology. 2011;53(4):1217–1225. doi:10.1002/hep.24150
7. Fragkou N, Sideras L, Panas P, Emmanouilides C, Sinakos E. Update on the association of hepatitis B with intrahepatic cholangiocarcinoma: is there new evidence? World J Gastroenterol. 2021;27(27):4252–4275. doi:10.3748/wjg.v27.i27.4252
8. Lee TY, Hsu YC, Yu SH, Lin JT, Wu MS, Wu CY. Effect of Nucleos(t)ide Analogue Therapy on Risk of Intrahepatic Cholangiocarcinoma in Patients With Chronic Hepatitis B. Clin Gastroenterol Hepatol. 2018;16(6):947–954.e4. doi:10.1016/j.cgh.2017.09.031
9. Lei Z, Xia Y, Si A, et al. Antiviral therapy improves survival in patients with HBV infection and intrahepatic cholangiocarcinoma undergoing liver resection. J Hepatol. 2018;68(4):655–662. doi:10.1016/j.jhep.2017.11.015
10. Chen JW, Maldonado DR, Kowalski BL, et al. Best Practice Guidelines for Propensity Score Methods in Medical Research: consideration on Theory, Implementation, and Reporting. A Review. Arthroscopy. 2022;38(2):632–642. doi:10.1016/j.arthro.2021.06.037
11. Wan F. Propensity Score Matching: should we use it in designing observational studies? BMC Med Res Methodol. 2025;25(1):25. doi:10.1186/s12874-025-02481-w
12. Ahn JC, Ng WH, Yeo YH, et al. Comparative effectiveness of immunotherapy versus lenvatinib in advanced hepatocellular carcinoma: a real-world analysis using target trial emulation. Hepatology. 2025. doi:10.1097/hep.0000000000001328
13. Guo X, Chen C, Zhao J, et al. Neoadjuvant Chemoradiotherapy vs Chemoimmunotherapy for Esophageal Squamous Cell Carcinoma. JAMA Surg. 2025;160(5):565. doi:10.1001/jamasurg.2025.0220
14. Oesterheld J, Ferguson W, Kraveka JM, et al. Eflornithine as Postimmunotherapy Maintenance in High-Risk Neuroblastoma: externally Controlled, Propensity Score-Matched Survival Outcome Comparisons. J Clin Oncol. 2024;42(1):90–102. doi:10.1200/jco.22.02875
15. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/jco.2014.57.9151
16. Yoshino O, Wang Y, McCarron F, et al. Major hepatectomy in elderly patients: possible benefit from robotic platform utilization. Surg Endosc. 2023;37(8):6228–6234. doi:10.1007/s00464-023-10062-5
17. Mai RY, Bai T, Luo XL, Wu GB. Indocyanine Green Retention Test as a Predictor of Postoperative Complications in Patients with Hepatitis B Virus-Related Hepatocellular Carcinoma. Ther Clin Risk Manag. 2022;18:761–772. doi:10.2147/tcrm.S363849
18. Xu Z, Zhao Y, Fu X, et al. Laparoscopic versus Open Inguinal Hernia Repair in Aging Patients: a Propensity Score Matching-Based Retrospective Study. Ther Clin Risk Manag. 2023;19:657–666. doi:10.2147/tcrm.S423307
19. Tang Y, Kang L, Guo M, Fan L. Intertrochanteric Fracture Surgery Patients with Diabetes Mellitus are Prone to Suffer Perioperative Neurological and Endocrine/Metabolic Complications: a Propensity-Score Matched Analysis. Ther Clin Risk Manag. 2022;18:775–783. doi:10.2147/tcrm.S366846
20. Formánek T, Potočár L, Wolfova K, et al. Deaths with COVID-19 and from all-causes following first-ever SARS-CoV-2 infection in individuals with preexisting mental disorders: a national cohort study from Czechia. PLoS Med. 2024;21(7):e1004422. doi:10.1371/journal.pmed.1004422
21. Rivera AS, Pak KJ, Mefford MT, Hechter RC. Use of Tenofovir Alafenamide Fumarate for HIV Pre-Exposure Prophylaxis and Incidence of Hypertension and Initiation of Statins. JAMA Network Open. 2023;6(9):e2332968. doi:10.1001/jamanetworkopen.2023.32968
22. Yang G, Mason AM, Wood AM, Schooling CM, Burgess S. Dose-Response Associations of Lipid Traits With Coronary Artery Disease and Mortality. JAMA Network Open. 2024;7(1):e2352572. doi:10.1001/jamanetworkopen.2023.52572
23. Zhou ZJ, Ye YH, Hu ZQ, et al. Whole-exome sequencing reveals genomic landscape of intrahepatic cholangiocarcinoma and identifies SAV1 as a potential driver. Nat Commun. 2024;15(1):9960. doi:10.1038/s41467-024-54387-8
24. Clements O, Eliahoo J, Kim JU, Taylor-Robinson SD, Khan SA. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a systematic review and meta-analysis. J Hepatol. 2020;72(1):95–103. doi:10.1016/j.jhep.2019.09.007
25. Li M, Li J, Li P, et al. Hepatitis B virus infection increases the risk of cholangiocarcinoma: a meta-analysis and systematic review. J Gastroenterol Hepatol. 2012;27(10):1561–1568. doi:10.1111/j.1440-1746.2012.07207.x
26. Song Z, Lin S, Wu X, et al. Hepatitis B virus-related intrahepatic cholangiocarcinoma originates from hepatocytes. Hepatol Int. 2023;17(5):1300–1317. doi:10.1007/s12072-023-10556-3
27. Li Z, Gao Q, Wu Y, et al. HBV infection effects prognosis and activates the immune response in intrahepatic cholangiocarcinoma. Hepatol Commun. 2024;8(1):e0360. doi:10.1097/hc9.0000000000000360
28. Shen Y, Xu S, Ye C, et al. Proteomic and single-cell landscape reveals novel pathogenic mechanisms of HBV-infected intrahepatic cholangiocarcinoma. iScience. 2023;26(2):106003. doi:10.1016/j.isci.2023.106003
29. Yun B, Ahn SH, Oh J, Yoon JH, Kim BK. Post-operative recurrence of liver cancer according to antiviral therapy for detectable hepatitis B viremia: a nationwide study. Eur J Intern Med. 2023;107:66–72. doi:10.1016/j.ejim.2022.10.026
30. Li Z, Lei Z, Xia Y, et al. Association of Preoperative Antiviral Treatment With Incidences of Microvascular Invasion and Early Tumor Recurrence in Hepatitis B Virus-Related Hepatocellular Carcinoma. JAMA Surg. 2018;153(10):e182721. doi:10.1001/jamasurg.2018.2721
31. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
32. van Smeden M, Moons KG, de Groot JA, et al. Sample size for binary logistic prediction models: beyond events per variable criteria. Stat Methods Med Res. 2019;28(8):2455–2474. doi:10.1177/0962280218784726
33. van Smeden M, de Groot JA, Moons KG, et al. No rationale for 1 variable per 10 events criterion for binary logistic regression analysis. BMC Med Res Methodol. 2016;16(1):163. doi:10.1186/s12874-016-0267-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Inflammation-Based Scores Predict Responses to PD-1 Inhibitor Treatment in Intrahepatic Cholangiocarcinoma
Yang Z, Zhang D, Zeng H, Fu Y, Hu Z, Pan Y, Chen J, Wang J, Zhang Y, Zhou Z, Xu L, Hu D, Chen M
Journal of Inflammation Research 2022, 15:5721-5731
Published Date: 6 October 2022
Clinical Significance of Fibrinogen and Platelet to Pre-Albumin Ratio in Predicting the Prognosis of Advanced Gastric Cancer
Tian H, Liu Z, Zhang Z, Zhang L, Zong Z, Liu J, Ying H, Li H
Journal of Inflammation Research 2023, 16:4373-4388
Published Date: 2 October 2023
Clinical Complete Response After Conversion Therapy for Unresectable Hepatocellular Carcinoma: Is Salvage Hepatectomy Necessary?
Wu JY, Wu JY, Liu DY, Li H, Zhuang SW, Li B, Zhou JY, Huang JY, Zhang ZB, Li SQ, Yan ML, Wang YD
Journal of Hepatocellular Carcinoma 2023, 10:2161-2171
Published Date: 5 December 2023
Surgical Strategies Affect the Long-Term Prognosis of Patients with Hepatocellular Carcinoma Adjacent to the Left Branch of the Portal Vein
Bai S, Shen X, Liu J, Lu C, Wang J, Liu L, Wang C, Wang H, Liu K, Sun Y, Xue F
Journal of Hepatocellular Carcinoma 2023, 10:2355-2366
Published Date: 27 December 2023
Negative Impact of Intra-Operative Blood Transfusion on Survival Outcomes of Hepatocellular Carcinoma Patients
Teng L, Zhao L, Shao H, Dai J, Zou H
Cancer Management and Research 2024, 16:385-393
Published Date: 25 April 2024