")
Back to Journals » Infection and Drug Resistance » Volume 18
Impact of Herpesvirus Detection via Metagenomic Next-Generation Sequencing in Patients with Lower Respiratory Tract Infections
Authors Zhang H, Zhang X, Zheng Y , Gu X, Fu Z, Gai W, Wang H
Received 28 June 2024
Accepted for publication 17 December 2024
Published 21 January 2025 Volume 2025:18 Pages 377—389
DOI https://doi.org/10.2147/IDR.S484768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Huihui Zhang,1,* Xiaojing Zhang,2,* Yafeng Zheng,2,* Xiao Gu,1 Zhongming Fu,1 Wei Gai,2 Huaying Wang1
1Department of Respiratory and Critical Care Medicine, The Affiliated People’s Hospital of Ningbo University, Yinzhou People’s Hospital, Ningbo, Zhejiang, 315040, People’s Republic of China; 2WillingMed Technology (Beijing) Co., Ltd, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Gai, WillingMed Technology (Beijing) Co., Ltd, No. 156 Jinghai 4th Road, Beijing Economic and Technological Development Zone, Beijing, 101103, People’s Republic of China, Email [email protected] Huaying Wang, The Affiliated People’s Hospital of Ningbo University, Yinzhou People’s Hospital, No. 251, Baizhang East Road, Ningbo, 315040, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the impact of herpesvirus detection by metagenomic next-generation sequencing (mNGS) of bronchoalveolar lavage fluid (BALF) on lower respiratory tract infections (LRTIs) patients’ lung microbiome composition and prognosis.
Patients and methods: We initially enrolled 234 hospitalized patients with LRTIs who underwent BALF mNGS between February 2022 and May 2023. The study analyzed the clinical manifestations and the pulmonary microbial composition between herpesvirus detection (HD) and non-herpesvirus detection (non-HD) group.
Results: After exclusions, a total of 201 patients were included, out of which 73 patients had herpesvirus detections (HD). The most frequently detected herpesviruses were Human herpesvirus 7 (HHV-7) (19.4%), Epstein-Barr virus (EBV) (12.4%), and cytomegalovirus (CMV) (10.4%). The HD group had a higher proportion of male patients (78.08% vs 55.04%, P = 0.001) and a greater incidence of hemoptysis and multilobar infiltrates compared non-HD group. Additionally, the HD group tended to have longer hospital stays compared to non-HD group, especially in immunosuppressed patients. Furthermore, in immunocompetent patients, there were significant differences in α diversity and β diversity between the HD group and non-HD group, but such differences were not observed in immunosuppressed patients.
Conclusion: The presence of herpesvirus in patients with non-critical LRTI is associated with longer hospital stays and alterations in the lung’s microbial composition. Additionally, the impacts of herpesvirus presence are influenced by the immune status of the patients.
Keywords: lower respiratory tract infections, herpesvirus detection, bronchoalveolar lavage fluid, microbial composition, mNGS
Introduction
Lower respiratory tract infection (LRTI) remains one of the leading causes of death worldwide.1 Despite being traditionally considered as non-pathogenic, herpesviruses are frequently found in the lungs of patients with LRTI.2,3 The mechanisms of establishment, maintenance and reactivation of herpesviruses species in different subfamilies (including Alphaherpesvirinae, Betaherpesvirinae and Gammaherpesvirinae) are different.4
Previous studies have explored the impact of herpesviruses on the prognosis and mortality of critically ill or transplanted patients. These studies identified cytomegalovirus (CMV), herpes simplex virus-1 (HSV-1) and Epstein-Barr virus (EBV) as the most commonly detected viruses in the lower respiratory tract of patients suffering from severe pneumonia, establishing a correlation between positive herpesvirus presence and increased mortality.3,5–7 In contrast, another study analyzed the incidence and clinical characteristics of human herpesvirus-7 (HHV-7), concluding that HHV-7 positivity was not an independent risk factor for mortality, suggesting that different herpesviruses may have varying impacts on patient outcomes. Moreover, the presence of herpesviruses has been shown to alter the composition of the lung microbiome in critically ill patients.3,7 Thus, it is evident that herpesvirus presence significantly affects host conditions. Understanding patients’ clinical characteristics and potential coexisting or interacting pathogens can aid clinicians in their decision-making processes. Additional analyses are warranted to evaluate the influence of positive herpesvirus on factors such as pathogen composition, and lung microbiome, etc. Moreover, the impact of herpesviruses on patients with non-critical lung infections remains poorly understood.
This study comprehensively investigated the clinical impacts of the presence of herpesvirus in patients diagnosed with LRTI. We examined clinical manifestations, clinical indicators, length of hospital stay, pathogen species and detection rates, lung microbial composition, and microbial interactions among LRTI patients with and without herpesvirus detection, aiming to establish a foundation for precise clinical diagnosis and treatment.
Methods
Study Design and Patient Population
The study exclusively enrolled patients from the Affiliated People’s Hospital of Ningbo University, Yinzhou People’s Hospital. A total of 234 hospitalized patients with suspected LRTIs between February 2022 and May 2023 were involved. The inclusion criteria were: (1) age ≥ 18 years old; (2) performed bronchoalveolar lavage fluid (BALF) metagenomic next-generation sequencing (mNGS); (3) diagnosed with LRTIs. The exclusion criteria included the following: age below 18 years, absence of BALF mNGS, missing clinical data and absence of BALF culture results (Figure 1). Patients were then categorized into two groups: the herpesvirus detected (HD) group and the non-HD group (without specific reads of herpesvirus detected). Furthermore, the patients had a clearly defined primary disease.
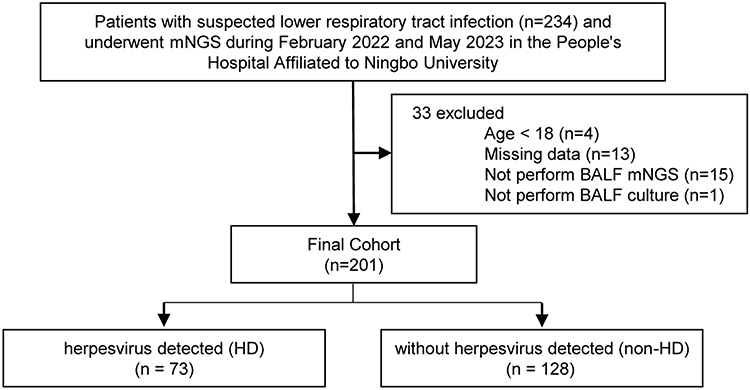 |
Figure 1 Study design. |
We collected baseline information and clinical data, including age, gender, comorbidities, symptoms, immune state, blood routine results, conventional inflammatory markers, length of hospital stay (LOHS), imaging findings, final diagnosis, and prognosis. Consensus defined immunosuppression and was determined based on meeting at least one of the following criteria:8 primary immunodeficiency disease; active malignancy; receiving anticancer chemotherapy; human immunodeficiency virus (HIV) infection; solid organ transplantation; hematopoietic stem cell transplantation; receiving corticosteroid therapy; receiving biologic immunomodulators; or receiving disease-modifying antirheumatic drugs or other immunosuppressive drugs.
Bacterial and fungal cultures were conducted on BALF samples for all the patients. Additional conventional microbiological test (CMT) results were also collected, including blood and sputum culture, 1, 3-β-D-glucan (G) test and galactomannan (GM) test for fungi, glucuronoxylomannan (GXM) test for Cryptococcus, T-spot and GeneXpert for Mycobacterium, and smear microscopy for fungi or tuberculosis. Final clinical diagnoses for the patients were made by two experienced physicians. In cases of discordant results, a senior physician provided definitive judgement.
mNGS Assay
Following standard procedures,9 BALF specimens were collected by experienced physicians and utilized for mNGS analysis. DNA was extracted using the PathoXtract® Basic Pathogen Nucleic Acid Kit (WYXM03211S, WillingMed Corp, Beijing, China), and DNA libraries were prepared with the Illumina® DNA Prep, (M) Tagmentation kit (20018705, Illumina) in accordance with the manufacturer’s protocol. High-quality libraries were sequenced on the NextSeq™ 550Dx platform using a 75 bp, single-end sequencing kit (Illumina), with a minimum of 20 million sequencing reads obtained for each sample. An external negative control (nuclease-free water) was included in each mNGS assay run to eliminate environmental and laboratory contaminants.10,11
After filtering out low-quality or undetected sequences, as well as those contaminated by splices, high-coverage repeats, and short-read-length sequences using Trimmomatic v0.40, high-quality sequencing data were obtained. The removal of human host sequences and pathogen classification was conducted with Bowtie2 v2.4.3. An RPTM (reads per ten million) value, which defined as the detected number of pathogen-specific reads per ten million, was utilized to quantify the abundance of microorganisms. To effectively identify the causative pathogen within the microbial communities, a criterion for positive mNGS results were established. An RPTM of ≥ 1 was applied as an empirical threshold for herpesvirus detection. For bacteria and fungi, positive pathogen identification required meeting a threshold of RPTM ≥ 20. Special pathogens such as Cryptococcus and Mycobacterium with an RPTM ≥ 1 was identified as positive. Normal flora of the oral cavity, the skin, or the respiratory tract, including Neisseria, coagulase-negative Staphylococci, Streptococcus infantis, Dialister invisus, and Rothia dentocariosa, were classified as part of the lung microbiome irrespective of their high reads’ numbers, as they were deemed unlikely to cause pulmonary infection.12–15
Statistical Analysis
All statistical analyses were performed using GraphPad Prism (Version 9.4.1, GraphPad Software Inc) and SPSS (version 26, IBM Corp). A Student’s t-test was utilized for continuous variables, while a chi-square test was applied to categorical variables. A significance level of P-value less than 0.05 was considered statistically significant. The alpha diversity index was calculated based on Shannon and Simpson indexes. Beta-diversity was visualized using principal coordinate analysis (PCoA). The community composition was depicted using a stacked bar plot created in R using the ggplot2 package. Species correlation was deemed statistically robust if the Spearman correlation coefficient (ρ) was > 0.6, and the Benjamini-Hochberg adjusted p-value was < 0.05. The statistical analyses were conducted by the “psych” packages in R. Network visualization was carried out using Gephi (v0.9.2). Linear discriminant analysis (LDA) effect size (LEfSe) was employed to identify significantly different species among the groups, with thresholds set at log10 LDA Score ≥ 2 and P value ≤ 0.05.
Results
Patient Characteristics and Herpesvirus Distribution
A total of 234 patients were initially enrolled in this study. After excluding those who met the exclusion criteria, 201 patients were included in the final analysis. Among these patients, 73 tested positives for herpesvirus using BALF mNGS and were classified as the HD group (Supplementary Table 2). The remaining 128 patients who tested negative for herpesvirus were categorized as the non-HD group (Figure 1). Compared to the non-HD group, the HD group exhibited a notably higher proportion of male patients (78.08% vs 55.04%, P = 0.001), tumor patients (19.18% vs 9.3%, P = 0.046), and immunosuppressed patients (39.73% vs 12.50%, P < 0.0001). Additionally, a higher incidence of hemoptysis (16.44% vs 3.88%, P = 0.002), multilobar infiltrates (94.52% vs 35.66%, P < 0.0001), and significantly elevated procalcitonin (PCT) levels (0.49 vs 0.16, P = 0.008) were noted in the HD group. The most prevalent diseases observed were pneumonia, followed by tuberculosis, and bronchiectasis. Notably, the non-HD group had a slightly higher proportion of patients infected with tuberculosis compared to the HD group (20.16% vs 9.59%, P = 0.048) (Table 1).
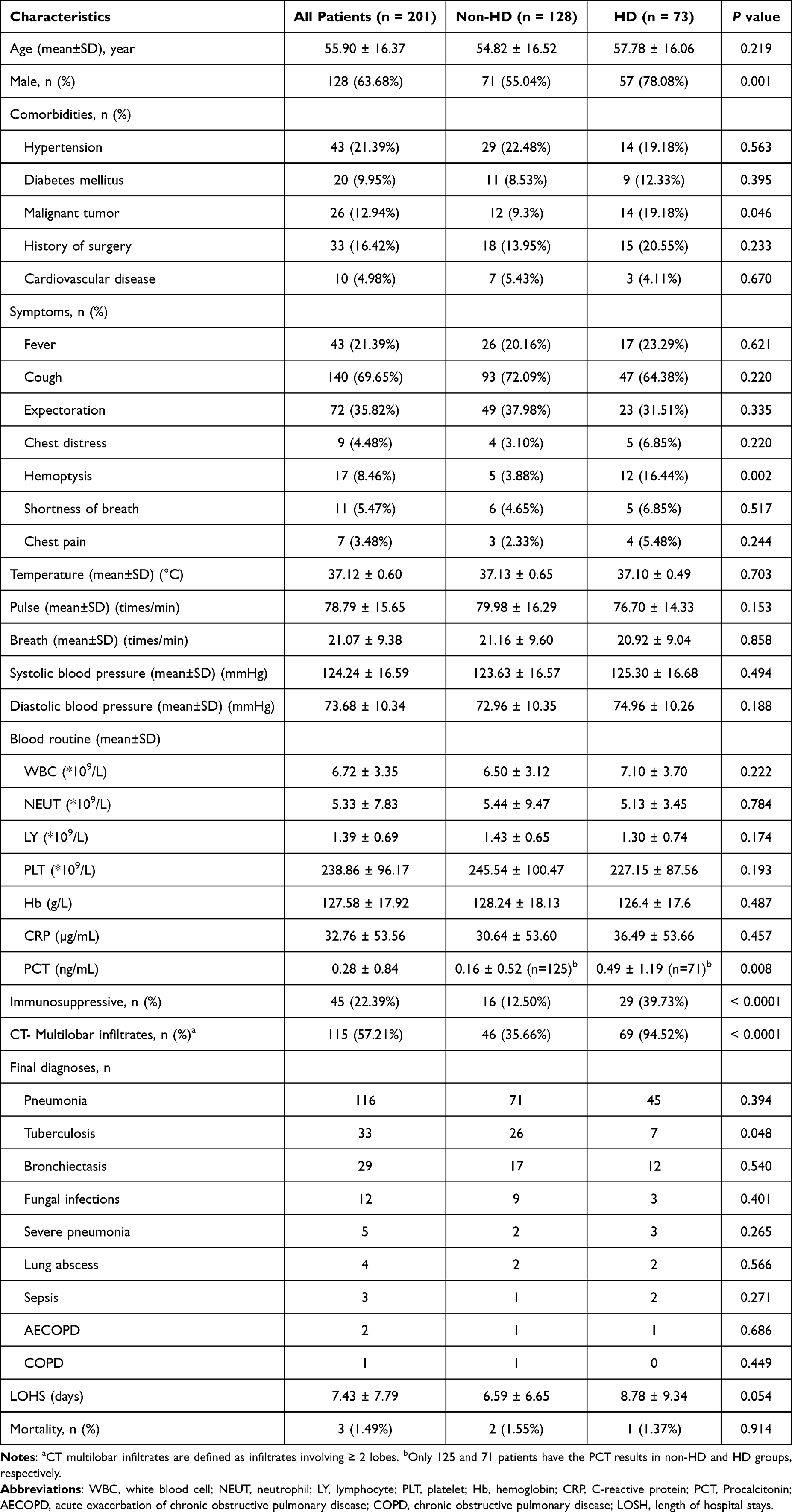 |
Table 1 Characteristics of the Patients Included in This Study |
Among the 73 patients in the HD group, a total of five types of herpesviruses were detected. The most prevalent was HHV-7, identified in 39 patients. The other herpesviruses included EBV, found in 25 patients, CMV in 21, HSV-1 in 9, and human herpes virus-6B (HHV-6B) in 5 patients. Furthermore, these viruses demonstrated a higher detected proportion in immunosuppressed patients than in immunocompetent patients (64.44% vs 28.20%, P < 0.0001), especially in cases with EBV (60.00%), HHV-6B (60.00%), and CMV (52.38%) (Figure 2A). HSV-1 was significantly more abundant compared to other herpesviruses (Figure 2B), with a significantly higher abundance observed among immunosuppressed patients compared to immunocompetent patients (P = 0.007) (Figure 2C). Two or more herpesviruses were detected in 27.40% (20/73) patients, which occurred more frequently among immunosuppressed patients (Figure 2D). Detection rates combined with other herpesviruses were highest for HHV-6B, followed by CMV, HSV-1, EBV, and HHV-7 (Figure 2E).
 |
Figure 2 Distribution and abundance of herpesvirus species in patients of the HD group. (A) Herpesvirus detections frequency. (B) Abundance distribution of herpesviruses in patients with herpesvirus detection. (C) Abundance distribution of herpesviruses in immunosuppressed and immunocompetent patients with herpesvirus detection. (D) Herpesvirus detected frequency in each patient. (E) Heatmap illustrating herpesvirus distribution. Abbreviations: HHV-7, human herpesvirus 7; EBV, Epstein-Barr virus; CMV, Cytomegalovirus; HSV-1, Herpes simplex virus-1; HHV-6B, Human herpesvirus-6B. |
The Association Between Herpesvirus and the Length of Hospital Stay of LRTI Patients
Due to the low mortality rate observed in this study, we compared the length of hospital stay (LOHS) between HD and non-HD groups to investigate the potential association between herpesviruses and the prognosis of patients with LRTI. The LOHS was found to be longer in the HD group compared to the non-HD group (8.78 ± 9.34 vs 6.59 ± 6.65), although this difference was not reach statistical significance (Table 2). Furthermore, we conducted a comparison of the LOHS between patients with specific herpesviruses detected and non-HD group (Table 2). While all patients with different kinds of herpesviruses detected tended to have extended hospital stay, only those infected with CMV showed a significant difference (Table 2). Subsequently, an analysis of the association between LOHS and immune status was performed. Across all groups, it was noted that immunosuppressed patients generally experienced longer hospital stays compared to immunocompetent patients, with the significant difference only being observed in the HD group (Table 2).
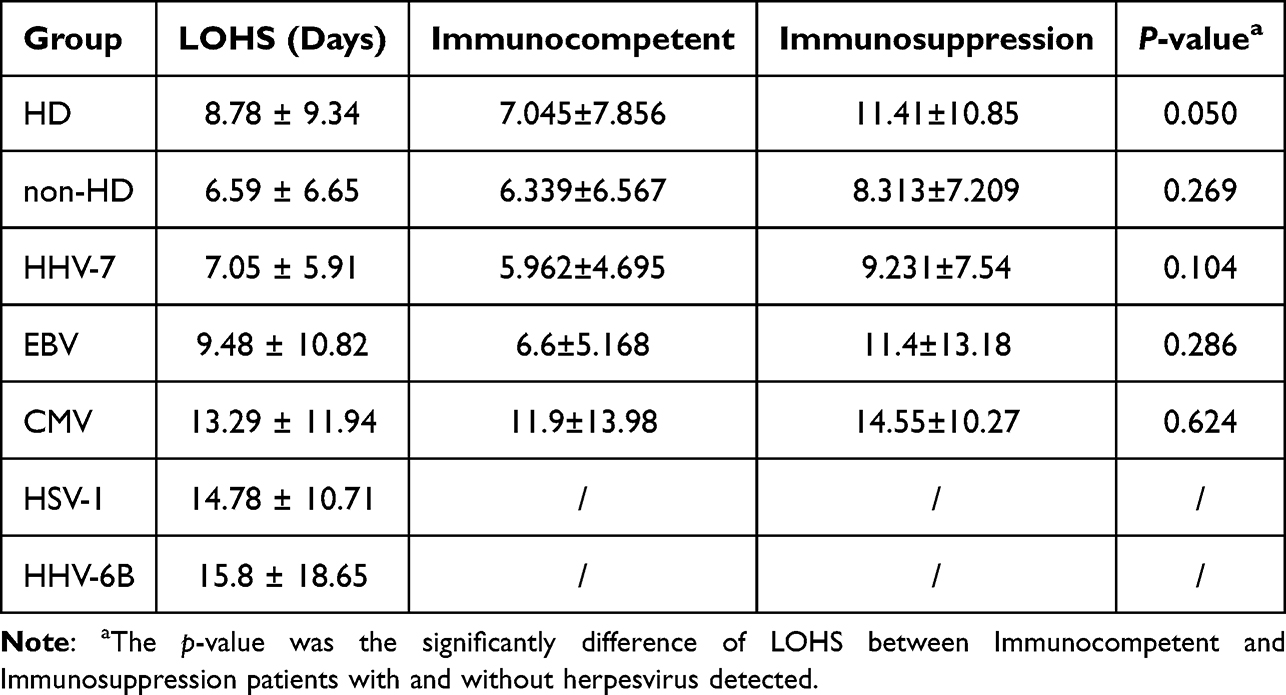 |
Table 2 The Difference of LOHS Between Patients with and without Herpesvirus Detected and the Association Between LOHS and Immune Status |
Pathogen Distribution in the HD and Non-HD Group
The pathogens detected by mNGS and CMT were list in Supplementary Table 1. Bacterial infection was the most prevalent, followed by tuberculosis infection and fungal infection in the enrolled patients (Figure 3A). In the HD group, the detection rate of gram-positive bacteria was 80.82%, with 71.88% of the non-HD group. The most common gram-positive bacteria were Corynebacterium accolens, Streptococcus pneumoniae, and Tropheryma whipplei (Figure 3B). The HD group exhibited a higher overall detection rate of gram-negative organisms when compared to the non-HD group (69.86% vs 47.66%). Among the non-HD group, the most common gram-negative bacteria were Klebsiella pneumoniae, Pseudomonas aeruginosa, and Haemophilus influenzae. Klebsiella pneumoniae was also the most detected bacteria in the HD group, with a significantly higher detection rate than the non-HD group. Special pathogens, including Mycobacterium tuberculosis complex, Chlamydia psittaci, Mycoplasma pneumoniae, and Legionella pneumophila, showed a higher detection rate in the non-HD patients (Figure 3A). Additionally, a greater detection rate of fungi was also observed in the HD group compared to the non-HD group (47.95% vs 27.34%). Moreover, the distribution of fungal species differed between the two groups, with Aspergillus fumigatus being the most common species in the non-HD group, while Candida albicans was the most common species in the HD group (Figure 3B).
 |
Figure 3 Infection type and pathogen distribution in the HD and non-HD groups. (A) Comparison of infection type between the HD and non-HD groups. (B) Pathogen distribution for both groups. Abbreviations: TB, tuberculosis; NTM, non-tuberculous Mycobacteria. |
The distribution of pathogens in immunosuppressed and immunocompetent patients with herpesvirus detection was also analyzed. The top 4 to 5 bacterial species with the highest proportion of detections were consistent between immunocompetent and immunosuppressed patients, with gram-positive organisms predominantly Corynebacterium accolens, Streptococcus pneumoniae, Mycobacterium tuberculosis complex, Tropheryma whipplei and Staphylococcus aureus. And gram-negative organisms predominantly Klebsiella pneumoniae, Haemophilus influenzae, Escherichia coli, and Klebsiella variicola. Other bacteria detected in smaller proportions were detected only in immunocompetent or immunosuppressed patients (Supplementary Figure 1A). Significantly more fungi were detected in immunosuppressed patients than in immunocompetent patients (82.76% vs 27.27%), and the most common fungus in both groups was Candida albicans. Aspergillus fumigatus was more prevalent in immunosuppressed patients, and Cryptococcus neoformans was detected only in immunocompetent patients. In addition, two other immunocompetent patients had Aspergillus detections or positive G tests (labelled Fungi). All the other types of fungi were detected in immunosuppressed patients (Supplementary Figure 1B).
Herpesvirus Detection is Associated with the Lung Microbiome Composition
We analyzed the microbial composition of the patients’ lungs and observed that the HD group exhibited significantly higher Shannon and Simpson index compared to the non-HD group (Supplementary Figure 2A). The PCoA based on Weighted Unifrac distance revealed an overlap between samples from both the HD and non-HD group (Supplementary Figure 2B). Additionally, we examined the microbiome difference between specific HD patients and the non-HD group, including HHV-7, EBV and CMV. Among these three viruses, HHV-7 had the highest Shannon and Simpson index, followed by EBV and CMV. Only patients with HHV-7 detection showed a significantly higher α diversity than those in the non-HD group (Supplementary Figure 3A). No significantly β diversity differences were observed between patients with detections of HHV-7, EBV, and CMV when compared to non-HD group patients using PCoA analysis (Supplementary Figure 3B). As the HD group had a higher proportion of immunosuppressed patients, we divided the patients from both the HD and non-HD groups into immunosuppressed and immunocompetent subgroups to explore the relationship between respiratory tract microbiome and immune status. The findings revealed that among immunocompetent patients, the HD group exhibited higher α diversity than the non-HD group (P = 0.0004 for Shannon indexes and P = 0.0090 for Simpson indexes) (Figure 4A). Conversely, in the immunosuppressed patients, the α diversity between HD and non-HD group patients was not significantly different, and both were lower than that in immunocompetent HD patients (Figure 4A). The PCoA analysis indicated significant differences between the HD and non-HD group in immunocompetent patients (P = 0.00017), whereas there were no significant differences between the HD and non-HD group in immunosuppressed patients (P = 0.2157) (Figure 4B).
 |
Figure 4 Impact of immune status on the lung microbiome of patients with and without herpesvirus detection. (A) Measurement of alpha diversity using Shannon and Simpson indices. (B) Beta diversity analysis using PCoA. (C) Identification of the top 10 most abundant species. |
The 10 most abundant species identified in both the HD and non-HD groups were Pseudomonas aeruginosa, Mycobacterium tuberculosis, Burkholderia multivorans, Parvimonas micra, Rothia mucilaginosa, Candida albicans, Streptococcus intermedius, Staphylococcus aureus, Peptostreptococcus stomatis, and Streptococcus mitis (Supplementary Figure 2C). Seven of the top 10 species also had the highest abundance in the HHV-7, EBV and CMV detected and non-HD groups (Supplementary Figure 3C). Additionally, eight of them also appeared between immunocompetent and immunosuppressed patients with or without herpesvirus detected (Figure 4C).
Subsequently, we examined the specific interactions between herpesvirus detection and the lung microbiome. Co-occurring networks were created for both the non-HD and HD groups, comprising strong (ρ > 0.6) and significant (FDR-adjusted P < 0.05) correlations between 236 and 250 microorganism species, respectively. Notably, all correlations between species were positive. In general, the HD group demonstrated a significantly higher number of microbial interactions, as evidenced by the number of edges between the nodes, compared to the non-HD group (174 vs 93, P < 0.0001) (Supplementary Figure 4).
Relationship Between Antibiotics Adjustments and Herpesvirus Reactivation
We also analyzed the impact of mNGS and CMT test results on antibiotic adjustment in the HD and non-HD groups. There was no clear distinction in the proportion of antibiotic adjustments performed between the HD and non-HD groups (41.10% vs 39.84%, P = 0.862), whether the adjustment was based on mNGS, or CMT, or both mNGS and CMT (Figure 5A). Additionally, we conducted an analysis to understand the effects of various herpesviruses and their antibiotic adjustments in patients with and without HHV-7, EBV, and CMV detected. Our findings show no significant differences observed between HHV-7 detected and non-detected groups (38.46% vs 40.74%, P = 0.795) (Figure 5B) as well as EBV detected and non-detected groups (28% vs 42.05%, P = 0.567) (Figure 5C). However, the percentage of patients who received antibiotic adjustments was significantly higher in the CMV detected group compared to the CMV non-detected group (66.67% vs 37.22%, P = 0.009), with the variation mostly attributable to changes guided by mNGS (38.10% vs 17.22%, P = 0.022) (Figure 5D).
 |
Figure 5 Impact of herpesvirus detected and viral species on antibiotic adjustments. Proportion of antibiotic adjustments for (A) herpesvirus detected. (B) HHV-7 detected. (C) EBV detected. (D) CMV detected. Types of antibiotic adjustments for (E) herpesvirus detected. (F) HHV-7 detected. (G) EBV detected. (H) CMV detected. |
We have conducted a further analysis of patients who received antibiotic adjustments and classified them into four categories: changing the types of antibiotics, antibiotic escalation and de-escalation, and a combination (represents simultaneous implementation of at least two adjustments, involving de-escalation, escalation, and change). The percentage of patients who received changes in the types of antibiotics was significantly higher in the non-HD group in comparison to in the HD group (90.20% vs 73.33%, P = 0.046). Nevertheless, the percentage of patients who underwent combination antibiotic adjustment was significantly greater in the HD group compared to the non-HD group (10.00% vs 0%, P = 0.021) (Figure 5E). No significant differences were found for HHV-7 (Figure 5F). The percentage for patients with changed antibiotics was significantly higher in the non-EBV group compared to the EBV group (86.49% vs 57.14%, P = 0.043) (Figure 5G). For CMV, the CMV detected group had a lower percentage of changes in antibiotics (57.14% vs 89.55%, P = 0.003) but a higher proportion of combination (21.43% vs 0%, P < 0.0001; Figure 5H). The impact of patient immunosuppression status on antibiotic adjustment in patients with detected or non-detected herpesvirus was also analyzed. The results demonstrated no significant effects (Supplementary Figure 5).
Discussion
This study comprehensively analyzed the characteristics of patients with and without herpesvirus detected, and identified that hemoptysis, multilobar infiltrates and PCT were significantly different features between the HD and non-HD patients, and variations were also found in both the distribution of pathogen and composition of the lung microbiome.
Throughout their lifetime, all humans inevitably become lifelong carriers of one or more herpesviruses.16,17 The Herpesviridae family is categorized into three groups: alpha (including HSV-1, HSV-2 and varicella zoster virus (VZV)), beta (CMV, HHV-6, HHV-7), and gamma herpesviruses (EBV and HHV-8) based on factors such as host range, genetic organization, and replication strategies.18 Despite their long-term coexistence with humans, herpesviruses have historically been considered as benign pathogens.19 In certain instances, persistent herpesvirus infection may even provide benefits to the host by providing protection against other infections and clinical conditions, such as malignancy.20–23 The degree of immunosuppression is a critical factor affecting patients’ susceptibility to herpesvirus reactivation.24,25 Among solid organ transplant recipients, the virus-positive group exhibited a higher mortality rate compared to the virus-negative group, and a notable difference in the lung microbiome was also observed between the two groups.7 In this study, the HD group included a significantly higher proportion of immunosuppressed patients compared to the non-HD group (Table 1). Additionally, among patients with herpesviruses, there was a significant difference in the alpha diversity of the lung microbiome between immunosuppressed and immunocompetent individuals. These findings suggest that the impact of herpesviruses on patients may differ depending on their immune status.
Significant disparities were noted between clinical indicators and imaging findings among individuals with and without herpesvirus detection. A higher percentage of patients in the HD group presented with hemoptysis symptoms (16.44% vs 3.88%, P = 0.002) (Table 1). Hemoptysis, the medical term for coughing up blood from the lungs or bronchial tubes, is commonly caused by bronchitis, bronchogenic carcinoma, and pneumonia in adults.26 Among the 17 patients with hemoptysis in this study, 13 were diagnosed with bronchiectasis (9 in HD group and 4 in non-HD group). The HD group exhibited a higher prevalence of multilobar infiltrates (94.52% of patients) compared to the non-HD groups (35.66% of patients) (Table 1). CT imaging is crucial for accurately assessing infection patterns and associated findings, facilitating the precise evaluation of all affected structures, and guiding diagnostic procedures such as bronchoalveolar lavage, ensuring reliable follow-up. It is essential for diagnosing various types of pulmonary infections.27 The findings suggest that herpesviruses are more likely to be detected in patients experiencing severe lung infections. PCT has been extensively studied as a biomarker of bacterial infections, aiding in the diagnosis and decision-making process for initiating or discontinuing antibiotic treatment in various conditions, including LRTI.28 A greater proportion of patients in the HD group were ultimately diagnosed with a bacterial infection (Figure 3A), which maybe the potential reason for the elevated PCT levels in the HD groups compared to the non-HD groups (Table 1). Understanding the relationship between a patient’s clinical symptoms and the disease assists clinicians in making swifter and more accurate diagnoses.
Our study uncovered disparities in the prevalence of pathogen infection and the composition of the lung microbiome between patients with and without detected herpesvirus. Staphylococcus aureus, Streptococcus pneumoniae, Klebsiella pneumoniae and Haemophilus influenzae were the most prevalent pathogens among patients with LRTI.29,30 We observed a higher detection rate of Streptococcus pneumoniae and Klebsiella pneumoniae in patients with herpesvirus compared to those without (Figure 3B). The rates of gram-positive bacteria detection did not show a significant difference between the HD group and the non-HD group. However, the rates of gram-negative bacteria and fungi detection were higher in the HD group than in the non-HD group (Figure 3B). Moreover, patients in the HD groups, and especially for immunosuppressed HD patients, significantly higher fungi codetection rate was observed (Figure 3B and Supplementary Figure 1B).
Additionally, patients in the HD group exhibited a more diverse microbiological composition within their lungs (Figure 4 and Supplementary Figure 4). Previous reports found that individuals with severe pneumonia and transplant recipients showed variations in the lung microbiomes between the virally activated/positive and inactivated/negative groups.3,7,31 Our study also revealed that the HD group had a more complex microbiological composition within their lungs. Moreover, we observed that only in immunocompetent patients, the HD group exhibited a higher microbiome diversity than non-HD group. No significant difference in microbiome diversity was found between the HD and non-HD groups in immunosuppressed patients. Additionally, our study found differences in the microbiome’s diversity between various herpesviruses, such as HHV-7, EB and CMV. Patients with detected HHV-7 had the highest microbiome diversity, while those with CMV exhibited the lowest microbiome diversity. The absence of statistical difference may be attributed to the small sample size, and further analysis with a larger sample is necessary to confirm these findings.
Huang et al found that CMV, HSV-1 and EBV were the most common herpesvirus in the lungs of patients with severe pneumonia and the existence of viral reactivations was associated with an increased risk of mortality.3 Another study specifically assessed the prognostic implications of detecting HHV-7 in the lower respiratory tract of patients with severe pneumonia. This study concluded that HHV-7 positivity was not an independent risk factor for mortality.31 In our study, we examined the LOHS of patients detected with various herpesviruses and discovered a similar trend to previous reports, with HHV-7 associated with shortest LOHS compared to other herpesviruses such as CMV, EB, HSV-1 and HHV-6B. These findings suggest that different herpesviruses may have varying impacts on patient prognosis, with HHV-7 potentially having the least detrimental effect.
Nonetheless, this study has several limitations. Firstly, this study was retrospective, with incomplete clinical testing performed in some patients due to the clinician’s initial diagnosis. Additionally, herpesvirus serological testing was only conducted in very few patients with high suspicion of viral infection. Consequently, the aetiological support data are of a poorer quality relative to prospective studies. Furthermore, it is not possible to accurately differentiate whether herpesviruses detected by mNGS are infected, colonized or contaminated based on the available results. In addition, herpesviruses were inevitably missed due to a variety of factors, such as antibiotic use and sampling time. Secondly, the number and population of enrolled patients were not matched, which inevitably resulted in data bias. Finally, the sample size was limited and the data were from a single center, and a larger study is needed to more fully assess the impact of the presence or absence of herpesvirus on patients with LRTI.
Conclusion
Differences in symptoms, clinical indicators, LOHS, pathogen distribution, and lung microbial composition and microbial interactions were observed between LRTI patients with and without herpesvirus detection. A thorough examination of the effects of herpesvirus detection could provide valuable insights for precise clinical diagnosis and treatment.
Ethics Statement
This study was approved by the Ethics Committee of the The Affiliated People’s Hospital of Ningbo University, Yinzhou People’s Hospital (Approval NO.: 2023-Scientific research-137). Due to the retrospective nature of the study, the Ethics Committee waived the requirement for patient consents. All data were anonymized prior to analysis. In general, all data in this study were obtained in accordance with the Helsinki declaration.
Funding
The work was supported by Scientific Research Fund of Zhejiang Provincial Education Department (grant number Y202044084), Ningbo Nature Fund (grant number 2022J031), and Medical and Health Science and Technology Project of Zhejiang Province (grant number 2024KY370).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. WHO reveals leading causes of death and disability worldwide: 2000–2019. 2020. Available from: https://wwwwhoint/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019.
2. Saade A, Moratelli G, Azoulay E, Darmon M. Herpesvirus reactivation during severe COVID-19 and high rate of immune defect. Infect Dis Now. 2021;51(8):676–679. doi:10.1016/j.idnow.2021.07.005
3. Huang L, Zhang X, Pang L, et al. Viral reactivation in the lungs of patients with severe pneumonia is associated with increased mortality, a multicenter, retrospective study. J Med Virol. 2023;95(1):e28337. doi:10.1002/jmv.28337
4. Lieberman PM. Epigenetics and genetics of viral latency. Cell Host Microbe. 2016;19(5):619–628. doi:10.1016/j.chom.2016.04.008
5. Gatto I, Biagioni E, Coloretti I, et al. Cytomegalovirus blood reactivation in COVID-19 critically ill patients: risk factors and impact on mortality. Intensive Care Med. 2022;48(6):706–713. doi:10.1007/s00134-022-06716-y
6. Simonnet A, Engelmann I, Moreau AS, et al. High incidence of Epstein-Barr virus, cytomegalovirus, and human-herpes virus-6 reactivations in critically ill patients with COVID-19. Infect Dis Now. 2021;51(3):296–299. doi:10.1016/j.idnow.2021.01.005
7. Pan L, Wu F, Cai Q, et al. Whole genome profiling of lung microbiome in solid organ transplant recipients reveals virus involved microecology may worsen prognosis. Front Cell Infect Microbiol. 2022;12:863399. doi:10.3389/fcimb.2022.863399
8. Ramirez JA, Musher DM, Evans SE, et al. Treatment of community-acquired pneumonia in immunocompromised adults: a consensus statement regarding initial strategies. Chest. 2020;158(5):1896–1911. doi:10.1016/j.chest.2020.05.598
9. Meyer KC, Raghu G, Baughman RP, et al. An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. 2012;185(9):1004–1014. doi:10.1164/rccm.201202-0320ST
10. Blauwkamp TA, Thair S, Rosen MJ, et al. Analytical and clinical validation of a microbial cell-free DNA sequencing test for infectious disease. Nat Microbiol. 2019;4(4):663–674. doi:10.1038/s41564-018-0349-6
11. Chen H, Zheng Y, Zhang X, et al. Clinical evaluation of cell-free and cellular metagenomic next-generation sequencing of infected body fluids. J Adv Res. 2023. doi:10.1016/j.jare.2023.02.018
12. Chen H, Yin Y, Gao H, et al. Clinical utility of in-house metagenomic next-generation sequencing for the diagnosis of lower respiratory tract infections and analysis of the host immune response. Clin Infect Dis. 2020;71(Suppl 4):S416–S426. doi:10.1093/cid/ciaa1516
13. Tan Y, Chen Z, Zeng Z, et al. Microbiomes detected by bronchoalveolar lavage fluid metagenomic next-generation sequencing among HIV-infected and uninfected patients with pulmonary infection. Microbiol Spectr. 2023;11(4):e0000523. doi:10.1128/spectrum.00005-23
14. Shi Y, Peng JM, Qin HY, Du B. Metagenomic next-generation sequencing: a promising tool for diagnosis and treatment of suspected pneumonia in rheumatic patients with acute respiratory failure: retrospective cohort study. Front Cell Infect Microbiol. 2022;12:941930. doi:10.3389/fcimb.2022.941930
15. Xie G, Zhao B, Wang X, et al. Exploring the clinical utility of metagenomic next-generation sequencing in the diagnosis of pulmonary infection. Infect Dis Ther. 2021;10(3):1419–1435. doi:10.1007/s40121-021-00476-w
16. Virgin HW, Wherry EJ, Ahmed R. Redefining chronic viral infection. Cell. 2009;138(1):30–50. doi:10.1016/j.cell.2009.06.036
17. Boshoff C, Weiss RA. Epidemiology and pathogenesis of Kaposi’s sarcoma-associated herpesvirus. Philos Trans R Soc Lond B Biol Sci. 2001;356(1408):517–534. doi:10.1098/rstb.2000.0778
18. Whitley RJ. Herpesviruses. In: Baron S, editor. Medical Microbiology.
19. Parrish CR, Holmes EC, Morens DM, et al. Cross-species virus transmission and the emergence of new epidemic diseases. Microbiol Mol Biol Rev. 2008;72(3):457–470. doi:10.1128/MMBR.00004-08
20. Barton ES, White DW, Cathelyn JS, et al. Herpesvirus latency confers symbiotic protection from bacterial infection. Nature. 2007;447(7142):326–329. doi:10.1038/nature05762
21. White DW, Suzanne Beard R, Barton ES. Immune modulation during latent herpesvirus infection. Immunol Rev. 2012;245(1):189–208. doi:10.1111/j.1600-065X.2011.01074.x
22. Furman D, Jojic V, Sharma S, et al. Cytomegalovirus infection enhances the immune response to influenza. Sci Transl Med. 2015;7(281):281ra43. doi:10.1126/scitranslmed.aaa2293
23. Litjens NHR, van der Wagen L, Kuball J, Kwekkeboom J. Potential beneficial effects of cytomegalovirus infection after transplantation. Front Immunol. 2018;9:389. doi:10.3389/fimmu.2018.00389
24. Libert N, Bigaillon C, Chargari C, et al. Epstein-Barr virus reactivation in critically ill immunocompetent patients. Biomed J. 2015;38(1):70–76. doi:10.4103/2319-4170.132905
25. Bailey ES, Zemke JN, Choi JY, Gray GC. A mini-review of adverse lung transplant outcomes associated with respiratory viruses. Front Immunol. 2019;10:2861. doi:10.3389/fimmu.2019.02861
26. Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005;72(7):1253–1260.
27. Walker CM, Abbott GF, Greene RE, Shepard JA, Vummidi D, Digumarthy SR. Imaging pulmonary infection: classic signs and patterns. AJR Am J Roentgenol. 2014;202(3):479–492. doi:10.2214/AJR.13.11463
28. Creamer AW, Kent AE, Albur M. Procalcitonin in respiratory disease: use as a biomarker for diagnosis and guiding antibiotic therapy. Breathe. 2019;15(4):296–304. doi:10.1183/20734735.0258-2019
29. Duan N, Du J, Huang C, Li H. Microbial distribution and antibiotic susceptibility of lower respiratory tract infections patients from pediatric ward, adult respiratory ward, and respiratory intensive care unit. Front Microbiol. 2020;11:1480. doi:10.3389/fmicb.2020.01480
30. Diao Z, Han D, Zhang R, Li J. Metagenomics next-generation sequencing tests take the stage in the diagnosis of lower respiratory tract infections. J Adv Res. 2022;38:201–212. doi:10.1016/j.jare.2021.09.012
31. Xu J, Zhong L, Shao H, et al. Incidence and clinical features of HHV-7 detection in lower respiratory tract in patients with severe pneumonia: a multicenter, retrospective study. Crit Care. 2023;27(1):248. doi:10.1186/s13054-023-04530-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.