")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Impact of Low Hand Grip Strength on Quality of Life, Utilization of Healthcare, and Mental Health in Individuals with Airflow Limitation
Authors Kim SH, Zo S , Kong SA, Cho JH , Do JG, Shin SH, Park HY
Received 7 December 2024
Accepted for publication 3 June 2025
Published 4 July 2025 Volume 2025:20 Pages 2199—2210
DOI https://doi.org/10.2147/COPD.S510974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Sang Hyuk Kim,1,2,* Sungmin Zo,3,* Sung A Kong,4 Ju hee Cho,5 Jong Geol Do,6 Sun Hye Shin,7 Hye Yun Park7
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Dongguk University Gyeongju Hospital, Dongguk University College of Medicine, Gyeongju, Republic of Korea; 2Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Republic of Korea; 3Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Republic of Korea; 4Department of Clinical Research Design and Evaluation, SAIHST, Sungkyunkwan University, Seoul, Republic of Korea; 5Center for Clinical Epidemiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; 6Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; 7Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Sun Hye Shin; Hye Yun Park, Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, Republic of Korea, Email [email protected]; [email protected]
Purpose: A higher prevalence of sarcopenia has been demonstrated in individuals with airflow limitation (AFL). However, data on the impact of sarcopenia on quality of life, utilization of healthcare, and mental health in individuals with AFL are limited.
Patients and methods: We used data from the 2014– 2019 Korea National Health and Nutrition Examination Survey (KNHANES), and participants with AFL were included. Sarcopenia was assessed using hand grip strength (HGS). The outcomes were health-related quality of life (HRQoL), utilization of healthcare, and mental health. The impact of low HGS and outcomes was assessed using multivariable logistic regression analysis.
Results: Among participants with AFL, 12.6% had low HGS and the median (interquartile range) of HGS was 22.5 (18.9– 26.1) kg for women and 37.7 (32.9– 42.6) kg for men. After adjusting for confounders, low HGS was associated with a decrease in HRQoL (usual activities: adjusted odds ratio [aOR], 1.70; 95% confidence interval [CI], 1.14– 2.54; pain/discomfort: aOR, 1.44; 95% CI, 1.02– 2.02, anxiety/depression: aOR, 1.59; 95% CI, 1.05– 2.41), and increased perceived stress (aOR, 1.77; 95% CI, 1.24– 2.53). In the subgroup analysis, the impact of low HGS on HRQoL, utilization of healthcare, and mental health was more evident in the reduced lung function and inactive physical activity groups.
Conclusion: Overall, low HGS was associated with decreased quality of life and worsening mental health in participants with AFL. Our findings underscore the importance of muscle strength for HRQoL, particularly in those with impaired lung function and sedentary lifestyles, suggesting that regular physical activity including muscle-strengthening exercises may improve HRQoL.
Plain Language Summary: People with chronic lung disease often have a higher prevalence of sarcopenia, but it is unclear how this affects their daily life and mental health. In this study, we analyzed national health data from Korea and found that among people with airflow limitation, low hand grip strength was more likely to be associated with poorer quality of life, higher stress levels, and increased use of healthcare services. These issues were more pronounced in people with reduced lung function and low physical activity. Our findings underscore the importance of muscle strength for better quality of life, particularly in those with impaired lung function and sedentary lifestyles, suggesting that regular physical activity including muscle-strengthening exercises may improve quality of life.
Keywords: chronic obstructive pulmonary disease, lung diseases, obstructive, sarcopenia, muscle strength
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of morbidity, disability, and mortality worldwide.1 The prevalence and burden of COPD are projected to increase in the coming decades as global life expectancy rises. Consequently, individuals with COPD will require lifelong management throughout their aging process. Along with the prevalent comorbidities among individuals with COPD,2,3 progressive reduction in muscle strength eventually leads to decreased exercise capacity and further physical deconditioning.4,5 Due to the complex and heterogeneous properties of the disease, the management of COPD involves not only pharmacological therapies but also interventions to improve the physical and psychological conditions of the patients.6 Accordingly, a comprehensive assessment of the overall physical status of individuals with COPD beyond standard lung function measurements is essential.
Sarcopenia is a progressive and generalized skeletal muscle disorder that is recognized as an independent condition.7 It is a clinical syndrome with multiple contributing factors, such as physical inactivity, malnutrition, and chronic diseases, including COPD.8 Sarcopenia is observed more frequently in individuals with COPD than in age-matched controls.9 Sarcopenia is associated with reduced functional performance, exercise capacity, and quality of life in individuals with COPD.8 Given the heterogeneity of symptoms and pathophysiological features among individuals with COPD, the loss of muscle strength in individuals with COPD may differ despite a similar degree of airflow obstruction. However, limited data is available on the impact of sarcopenia on quality of life, utilization of healthcare, and mental health among individuals with COPD of similar severity.
Korea has a nationally representative database that contains HGS, pre-bronchodilator lung function measurement, and questionnaires evaluating quality of life, utilization of healthcare, and mental health. Sarcopenia is closely associated with reduced handgrip strength (HGS), which is a widely recommended tool to assess sarcopenia.10 Airflow limitation (AFL), defined by spirometry as reduced forced expiratory volume in 1s (FEV₁)/forced vital capacity (FVC) ratio, is a hallmark diagnostic criterion for COPD and reflects impaired respiratory function, making it an appropriate representative measure for assessing an association between sarcopenia and COPD-related health outcomes.11 Therefore, our objective was to assess the impact of low HGS on health-related quality of life (HRQoL), utilization of healthcare, and mental health in individuals with AFL.
Methods
Study Population
The Korea National Health and Nutrition Examination Survey (KNHANES) is a nationwide government-administered survey. Participants were included using a multistage stratified probability sampling method. Several studies have been conducted on COPD and AFL using data from this survey.12–15 We used KNHANES data from 2014 to 2019. In the KNHANES, lung function measurements were performed only in participants aged ≥40 years. AFL was defined as pre-bronchodilator FEV1/FVC <0.7.
For 6 years, a total of 46,171 participants were included in this study. Of the 46,171 participants, 19,377 aged <40 years and 9,625 with missing baseline measurements were excluded. Among the remaining 17,169 adults aged >40 years, 14,777 participants without AFL were excluded. Finally, a total of 2,392 participants were included in the analysis (Figure 1).
 |
Figure 1 Flow chart of the study population. Abbreviations: KNHANES, Korea National Health and Nutrition Examination Survey; HGS, hand grip strength. |
Hand Grip Strength
The HGS was measured using a digital grip strength dynamometer (TKK 5401; Takei Scientific Instruments Co., Ltd., Tokyo, Japan). The maximum HGS was measured in kilogram (kg) on both left and right arms, three times each. The highest value among the six measurements was used to define the HGS. Low HGS was determined using Asian criteria from the Asian Working Group for Sarcopenia.16 The cut-off values for low HGS were 28 kg for men and 18 kg for women. Normal HGS was defined as HGS values above the cut-off for low HGS.
Quality of Life, Utilization of Healthcare, and Mental Health
The outcomes assessed were HRQoL, utilization of healthcare, and mental health. We used the EQ-5D to assess HRQoL, which consists of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.17 The decrease in HRQoL was defined when the participant responded that he/she had a problem in each dimension. Hospital admission was used to investigate healthcare utilization, defined as any hospitalization in the last year. Among mental health items, perceived stress was assessed using a questionnaire.
Adjustment for Covariates
Body mass index (BMI) was calculated by dividing weight (kg) by the square of height (m2). BMI (kg/m²) was categorized as follows: normal weight (18.5 to <24.9), underweight (<18.5), and overweight/obesity (≥25) according to the classifications of the Korean Society for the Study of Obesity.18 Income was defined as low, intermediate, or high corresponding to the lowest, second to third, and highest quartiles of monthly income, respectively. Pulmonary function was assessed using a spirometer (Vyntus Spiro; Care Fusion, SanDiego, CA, USA) or a dry rolling seal spirometer (model 2130; SensorMedics Corporation, Yorba Linda, CA, USA) according to the American Thoracic Society/European Respiratory Society guidelines.19 Since KNHANES does not include post-bronchodilator spirometry, pre-bronchodilator values were used. Predicted FVC and FEV₁ were calculated using the Korean reference equations.20 The Korean formula for the predicted values was used to calculate the predicted FVC and FEV1. Respiratory symptoms (chronic cough and sputum production), physical limitations, and comorbidities were assessed using self-questionnaires.13 Physical activity was assessed using the Global Physical Activity Questionnaire (GPAQ) and presented as metabolic equivalent of task (MET) minutes per week.21
Statistical Analyses
Data are expressed as weighted percentages (standard errors). Differences between participants based on the presence of low HGS were assessed using Pearson’s chi-square test. Multivariate logistic regression analysis was used to assess the impact of low HGS on HRQoL, utilization of healthcare, and mental health. In the adjustment, age, sex, categorized BMI, smoking status, income, education, respiratory symptoms, FEV1%predicted, and comorbidities (a history of pulmonary tuberculosis, asthma, hypertension, and diabetes mellitus) were included. A subgroup analysis was performed for clinically significant variables–lung function (FEV1%predicted) and physical activity (METS-min/week)–in management of individuals with AFL. The cut-off for FEV1 and physical activity was determined as 80%predicted and 600 METS-min/week according to the severity grade of AFL and physical activity level recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and World Health Organization (WHO).22,23
We performed a post-hoc analysis among individuals with low HGS to examine whether activity physical activity could reduce the burden of HRQoL, utilization of healthcare, and mental health. We used the “survey” package of R to adjust the sampling weights, and those adjustments were used in all analyses. Data for participants in the single primary survey unit were centered on the grand mean instead of the stratum mean. A two-sided p-value of <0.05 was considered statistically significant. All analyses were performed with R version 4.1.2 (R Core Team 2021; R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
The baseline characteristics of the study population are presented in Table 1. The weighted mean age was 64.9 years; 73.9% were men and 67.6% were ever smokers. Of the total individuals, 12.6% had a low HGS. Individuals with low HGS were older (72.9 years vs 63.7 years, p < 0.001), and the proportion of men (56.7% vs 76.4%, p < 0.001) and college graduates (5.4% vs 22.6%, p < 0.001) was lower compared to those with normal HGS. Furthermore, individuals with low HGS were more likely to be underweight (4.4% vs 1.7%, p < 0.001), never smokers (43.7% vs 30.8%, p < 0.001), and have lower income (32.8% vs 25.1%, p < 0.001), more respiratory symptoms (18.8% vs 9.9%, p < 0.001), and limited physical activity (< MET-min/week: 69.5% vs 54.1%, p < 0.001) than those with normal HGS.
 |
Table 1 Baseline Characteristics of the Study Population |
Regarding comorbidities, the proportions of asthma (13.3% vs 6.5%, p = 0.002), hypertension (61.8% vs 46.0%, p < 0.001), and diabetes mellitus (24.2% vs 18.4%, p = 0.031) were higher in individuals with low HGS than in those with normal HGS. However, the proportion of a history of pulmonary tuberculosis did not differ between individuals with low HGS and those with normal HGS (9.7% vs 9.9%, p = 0.928). Regarding lung function, FVC (82.4%predicted vs 89.1%predicted, p < 0.001), FEV1 (73.8%predicted vs 77.5%predicted, p < 0.001), and FEV1/FVC (62.0% vs 63.9%, p < 0.001) were significantly lower in individuals with low HGS than in those with normal HGS. However, the magnitude of these differences was small and may not be clinically relevant.
Impact of HGS on HRQoL
Overall, participants with low HGS showed a decreased quality of life compared to those with normal HGS (Table 2). In the multivariable model, individuals with low HGS showed a significantly higher risk of decreased HRQoL in self-care (adjusted odds ratio [aOR], 1.70; 95% CI, 1.03–2.83) usual activities (aOR, 1.70; 95% CI, 1.14–2.54), pain/discomfort (aOR, 1.44; 95% CI, 1.02–2.02), and anxiety/depression (aOR, 1.57; 95% CI, 1.03–2.39) than those with normal HGS.
 |
Table 2 Impact of Hand Grip Strength on HRQoL in individuals with Airflow Limitation |
In the stratified analysis based on FEV1, low HGS was associated with decreased HRQoL in usual activities (aOR, 1.74; 95% CI, 1.08–2.79) among those with FEV1 <80%predicted. In individuals with FEV1 ≥80%predicted, low HGS was associated with a decreased HRQoL in self-care (aOR, 2.49; 95% CI, 1.11–5.60). In individuals with physical activity level <600 MET-min/week, low HGS was associated with a decreased HRQoL in self-care (aOR, 1.87; 95% CI, 1.05–3.31), usual activities (aOR, 1.90; 95% CI, 1.18–3.07), pain/discomfort (aOR, 1.59; 95% CI, 1.05–2.41), and anxiety/depression (aOR, 1.76; 95% CI, 1.05–2.94). However, in individuals with a physical activity level ≥600 MET-min/week, low HGS did not show a significant association with a decrease in HRQoL after full adjustment.
Impact of HGS on Mental Health and Healthcare Utilization
Table 3 shows the effect of HGS on mental health and healthcare utilization. In the multivariable model, individuals with low HGS had increased odds of perceived stress (aOR, 1.77; 95% CI, 1.24–2.53) compared to those with normal HGS. Among individuals with FEV1 ≥80%predicted, low HGS did not increase the odds of perceived stress. However, in individuals with FEV1 <80%predicted, low HGS was associated with a higher probability of perceived stress (aOR, 1.95; 95% CI, 1.26–3.03). Stratified analysis based on physical activity showed that low HGS was related to increased perceived stress regardless of activity level (aOR, 1.94; 95% CI, 1.03–3.65 for ≥600 MET-min/week and aOR, 1.66; 95% CI, 1.08–2.57 for <600 MET-min/week).
 |
Table 3 Impact of Hand Grip Strength on Mental Health and Healthcare Utilization in individualswith Airflow Limitation |
Regarding utilization of healthcare, hospital admission was not associated with low HGS. Among individuals with FEV1 ≥80%predicted, low HGS did not increase the odds of hospital admission. However, in participants with FEV1 <80%predicted, low HGS was associated with higher odds of hospital admission (aOR, 1.64; 95% CI, 1.03–2.61). Stratified analysis based on physical activity showed that low HGS was not associated with utilization of healthcare in individuals with <600 MET-min/week or ≥600 MET-min/week.
Impact of Physical Activity on HRQoL, Mental Health, and Healthcare Utilization Among Individuals with AFL and Low HGS
Among individuals with AFL and low HGS, engaging in active physical activity was significantly associated with better HRQoL in the domains of self-care (aOR, 0.38; 95% CI, 0.15–0.98) and usual activities (aOR, 0.45; 95% CI, 0.22–0.92), compared to those who were not physically active (Table 4). However, physical activity did not significantly affect mental health or healthcare utilization in individuals with AFL and low HGS (Table 5).
 |
Table 4 Impact of Physical Activity on HRQoL in individuals with Airflow Limitation and Low HGS |
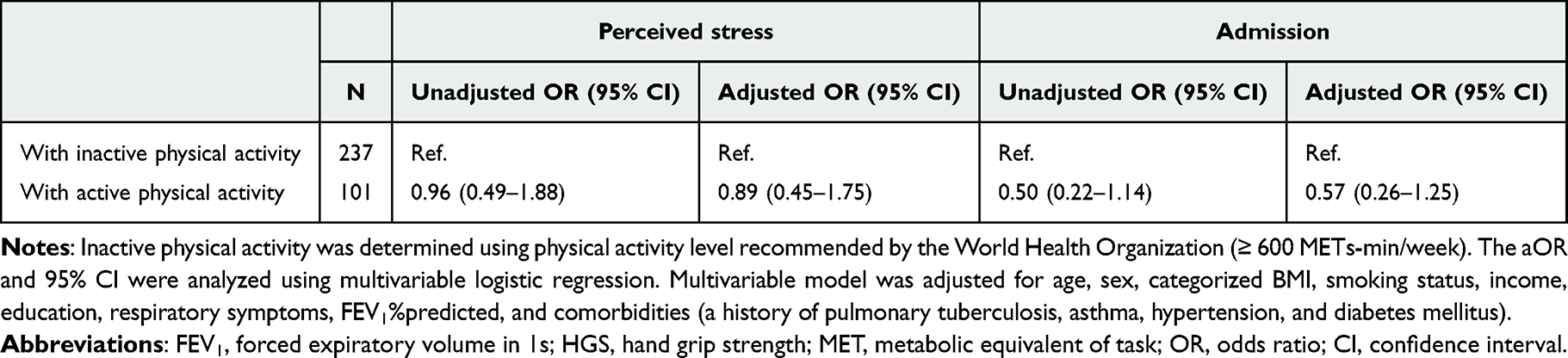 |
Table 5 Impact of Physical Activity on Mental Health and Healthcare Utilization in individuals with Airflow Limitation and Low HGS |
Discussion
In this study, we found that 12.6% of individuals with AFL in Korea exhibited low HGS. Low HGS was associated with decreased HRQoL and increased perceived stress. These associations were more evident in individuals with reduced lung function and inactive physical activity, underscoring the combined importance of lung function and muscle strength. Furthermore, engaging in physical activity was significantly associated with better HRQoL in the domains of self-care and usual activities, compared to those who were not physically active among individuals with AFL and low HGS. Furthermore, in individuals with AFL and reduced HGS, participation in regular physical activity was significantly linked to improved HRQoL, particularly in self-care and usual activity domains, compared to those who remained physically inactive.
HGS is a valuable tool for assessing muscle strength due to its simplicity, cost-effectiveness, and well-established role in predicting negative patient outcomes.24,25 Given these notable merits of HGS, the KNHANES incorporates HGS, reporting an average of 39.5 ± 9.3 kg for men and 24.4 ± 5.3 kg for women.26 Meanwhile, the overall prevalence of sarcopenia was reported to be 13.1% in the elderly Korean population.27 Although only individuals with AFL were included in this study, the prevalence of low HGS was comparable at 12.6%. Consistent with this result, another study using KNHANES data did not report significant differences in HGS between individuals with and without AFL.28 A potential explanation for this could be our recruitment method, which focused on individuals with AFL from the general population. Both our study and a previous study observed an average FEV1 value of approximately 80%predicted, indicating that most participants might have had mild disease. However, the inclusion of individuals under 65 years of age in our study allowed us to infer that low HGS may be more prevalent in this specific population with AFL.
Our study showed that low HGS was associated with a decrease in HRQoL in individuals with AFL. Previous studies have already demonstrated negative correlations between HGS and HRQoL in individuals at risk of AFL, including asthma and COPD.15,29,30 Our subgroup analysis found that individuals with reduced lung function and low HGS had a decrease in HRQoL across more items than those with preserved lung function. In further analyses stratified by physical activity level, low HGS was significantly associated with decreased HRQoL in individuals with inactive physical activity. These results suggest that the combination of reduced lung function or inactive physical activity, with low HGS not only decreases quality of life, but may also have a compounded negative effect on it, which can be explained by the vicious circle of dyspnea inactivity.31,32
Moreover, low HGS was associated with increased perceived stress in individuals with AFL, which was more evident in those with reduced lung function.33,34 Mental disorders and exacerbation–the major leading cause of hospitalization–are common features of chronic respiratory diseases, including asthma, COPD, interstitial lung diseases, and bronchiectasis.35–37 Our findings highlight the additional detrimental impact of sarcopenia on clinical outcomes in individuals with chronic respiratory diseases and reduced lung function. Notably, we also found that active engagement in physical activity was associated with better HRQoL, especially in the domains of self-care and usual activities, among individuals with AFL and low HGS, suggesting that maintaining regular physical activity may support better HRQoL in this population. These findings could extend to populations with AFL due to various respiratory diseases such as asthma and TB destroyed lung.38,39 Conversely, our data showed no significant differences across most HRQoL domains—including mobility, usual activities, pain/discomfort, anxiety/depression, perceived stress, and hospitalization—between individuals with normal and low HGS when FEV₁ was ≥ 80% predicted or when physical activity levels were high. This lack of perceived impairment of HRQoL may partially explain why individuals with AFL but better lung function may delay or be less likely to initiate pulmonary rehabilitation.
Our study has several limitations. First, the absence of post-bronchodilator spirometry results indicates that individuals with AFL may represent heterogeneous disease entities rather than classical COPD.40 However, recent proposals have advocated for broadening the definition of COPD to encompass a range of underlying causes, aiming to support earlier detection. In this context, most individuals with AFL could be classified as having COPD under a unified umbrella term.41 Nevertheless, the possibility of subject misclassification should be considered. Second, lung function was assessed only once, which may have introduced measurement errors. Third, the use of survey data based on self-administered questionnaires may have introduced recall bias. Fourth, this study was conducted in a single nation and ethnic group, which necessitates caution when generalizing the findings to other populations.
In conclusion, low HGS was associated with reduced quality of life and worsened mental health in individuals with AFL. These associations were more evident in individuals with reduced lung function and low levels of physical activity. Moreover, participation in regular physical activity was significantly associated with better HRQoL, particularly in the domains of self-care and usual activities in individuals with AFL and reduced HGS. Our findings highlight the critical role of muscle strength in maintaining HRQoL, especially in individuals with impaired lung function and sedentary lifestyles, and suggest that engaging in regular physical activity including muscle-strengthening exercises may offer meaningful improvements of HRQoL.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; KNHANES, Korea National Health and Nutrition Examination Survey; AFL, Airflow Limitation; HGS, Handgrip Strength; HRQoL, Health-Related Quality of Life; aOR, Adjusted Odds Ratio; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; BMI, Body Mass Index; GPAQ, Global Physical Activity Questionnaire; MET, Metabolic Equivalent of Task; GOLD, Global Initiative for Chronic Obstructive Lung Disease; WHO, World Health Organization.
Ethics Approval Declaration
The KNHANES 2014–2019 was conducted following the Declaration of Helsinki. The Institutional Review Board (IRB) of the Korea Disease Control and Prevention Agency (KDCA) approved the study (IRB: 2013-12EXP-03-5C, 2018-01-03-P-A, and 2018-01-03-C-A). Also, this study protocol was approved by the Institutional Review Board of Korea University Anam Hospital (No. 2024AN0383). Written informed consent was obtained from all participants, and anonymized data were provided.
Acknowledgments
This study is part of a Master’s thesis by Dr. Sang Hyuk Kim at the Department of Internal Medicine, Sungkyunkwan University, Republic of Korea.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT)(RS-2023-00279988). This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health Welfare, Republic of Korea (grant number: HR21C0885).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Venkatesan P. GOLD report: 2022 update. Lancet Respir Med. 2022;10(2):e20. doi:10.1016/s2213-2600(21)00561-0
2. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
3. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
4. Machado FVC, Spruit MA, Coenjaerds M, Pitta F, Reynaert NL, Franssen FME. Longitudinal changes in total and regional body composition in patients with chronic obstructive pulmonary disease. Respirology. 2021;26(9):851–860. doi:10.1111/resp.14100
5. Maltais F, Decramer M, Casaburi R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(9):e15–62. doi:10.1164/rccm.201402-0373ST
6. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
7. Santilli V, Bernetti A, Mangone M, Paoloni M. Clinical definition of sarcopenia. Clin Cases Miner Bone Metab. 2014;11(3):177–180. doi:10.1007/s00223-013-9758-y
8. Jones SE, Maddocks M, Kon SS, et al. Sarcopenia in COPD: prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax. 2015;70(3):213–218. doi:10.1136/thoraxjnl-2014-206440
9. Benz E, Trajanoska K, Lahousse L, et al. Sarcopenia in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2019;28(154):190049. doi:10.1183/16000617.0049-2019
10. Vaishya R, Misra A, Vaish A, Ursino N, D’Ambrosi R. Hand grip strength as a proposed new vital sign of health: a narrative review of evidences. J Health Popul Nutr. 2024;43(1):7. doi:10.1186/s41043-024-00500-y
11. Kim SH, Han MK. Challenges and the Future of Pulmonary Function Testing in COPD: toward Earlier Diagnosis of COPD. Tuberc Respir Dis. 2025 88 3 413–418. doi:10.4046/trd.2025.0009
12. Kim SH, Lee H, Kim Y, et al. Recent Prevalence of and Factors Associated With Chronic Obstructive Pulmonary Disease in a Rapidly Aging Society: Korea National Health and Nutrition Examination Survey 2015-2019. J Korean Med Sci. 2023;38(14):e108. doi:10.3346/jkms.2023.38.e108
13. Lee H, Shin SH, Gu S, et al. Racial differences in comorbidity profile among patients with chronic obstructive pulmonary disease. BMC Med. 2018;16(1):178. doi:10.1186/s12916-018-1159-7
14. Kim T, Choi H, Seo JI, et al. Prevalence, Trend, and Risk Factors for Early Chronic Obstructive Pulmonary Disease: an Analysis of the Nationwide Population-Based Survey from 2010 to 2019 in South Korea. COPD. 2023;20(1):153–161. doi:10.1080/15412555.2023.2192789
15. Lee SH, Kim SJ, Han Y, Ryu YJ, Lee JH, JH C. Hand grip strength and chronic obstructive pulmonary disease in Korea: an analysis in KNHANES VI. Int J Chron Obstruct Pulmon Dis. 2017;12:2313–2321. doi:10.2147/copd.S142621
16. Jung JW, Park SY, Kim H. An Analysis on Distribution of Handgrip Strength and Associated Factors in Korean Adults. Korean J Clin Pharm. 2021;31(3):231–236. doi:10.24304/kjcp.2021.31.3.231
17. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
18. Kim KK, Haam JH, Kim BT, et al. Evaluation and Treatment of Obesity and Its Comorbidities: 2022 Update of Clinical Practice Guidelines for Obesity by the Korean Society for the Study of Obesity. J Obes Metab Syndr. 2023;32(1):1–24. doi:10.7570/jomes23016
19. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
20. Choi JK, Paek D, Lee JO. Normal predictive values of spirometry in Korean population. Tuberculosis Respiratory Dis. 2005;58(3):230–242.
21. Cleland CL, Hunter RF, Kee F, Cupples ME, Sallis JF, Tully MA. Validity of the global physical activity questionnaire (GPAQ) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health. 2014;14:1255. doi:10.1186/1471-2458-14-1255
22. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report. 2023. Available from: http://goldcopd.org/2023-gold-report-2.
23. World Health Organization. Global recommendations on physical activity for health. Available from: https://www.who.int/publications/i/item/9789241599979.
24. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
25. Ibrahim K, May C, Patel HP, Baxter M, Sayer AA, Roberts H. A feasibility study of implementing grip strength measurement into routine hospital practice (GRImP): study protocol. Pilot Feasibility Stud. 2016;2(1):27. doi:10.1186/s40814-016-0067-x
26. YL L, BH L, SY L. Handgrip Strength in the Korean Population: normative Data and Cutoff Values. Ann Geriatr Med Res. 2019;23(4):183–189. doi:10.4235/agmr.19.0042
27. Choo YJ, Chang MC. Prevalence of Sarcopenia Among the Elderly in Korea: a Meta-Analysis. J Prev Med Public Health. 2021;54(2):96–102. doi:10.3961/jpmph.21.046
28. Kim S, Yoon HK, Rhee CK, Jung HW, Lee H, Jo YS. Hand Grip Strength and Likelihood of Moderate-to-Severe Airflow Limitation in the General Population. Int J Chron Obstruct Pulmon Dis. 2022;17:1237–1245. doi:10.2147/copd.S364351
29. Chen L, Liu X, Wang Q, et al. Better pulmonary function is associated with greater handgrip strength in a healthy Chinese Han population. BMC Pulm Med. 2020;20(1):114. doi:10.1186/s12890-020-1155-5
30. Lima TRL, Almeida VP, Ferreira AS, Guimarães FS, Lopes AJ. Handgrip Strength and Pulmonary Disease in the Elderly: what is the Link? Aging Dis. 2019;10(5):1109–1129. doi:10.14336/ad.2018.1226
31. Ramon MA, Riet GT, Carsin A-E, et al. The dyspnoea–inactivity vicious circle in COPD: development and external validation of a conceptual model. Eur Respir J. 2018;52(3):1800079. doi:10.1183/13993003.00079-2018
32. Cooper CB. Exercise in chronic pulmonary disease: limitations and rehabilitation. Med Sci Sports Exerc. 2001;33(7 Suppl):S643–646. doi:10.1097/00005768-200107001-00001
33. Kaczorowska A, Kozieł S, Ignasiak Z. Hand grip strength and quality of life among adults aged 50-90 years from South West Poland. Sci Rep. 2025;15(1):882. doi:10.1038/s41598-024-84923-x
34. Marques LP, Confortin SC, Ono LM, Barbosa AR, d’Orsi E. Quality of life associated with handgrip strength and sarcopenia: epiFloripa Aging Study. Arch Gerontol Geriatr. 2019;81:234–239. doi:10.1016/j.archger.2018.12.015
35. Kim BG, Han K, Jung JH, et al. Risk of Suicide in Individuals with Idiopathic Pulmonary Fibrosis: a Nationwide Cohort Study. Am J Respir Crit Care Med. 2024;210(4):524–527. doi:10.1164/rccm.202404-0767RL
36. Kim SH, Lee H, Jung JH, et al. Asthma Increases Long-Term Risk of Death by Suicide: a Nationwide Population-Based Cohort Study. J Allergy Clin Immunol Pract. 2025;13(3):559–567.e553. doi:10.1016/j.jaip.2024.11.013
37. Roca M, Verduri A, Corbetta L, Clini E, Fabbri LM, Beghé B. Mechanisms of acute exacerbation of respiratory symptoms in chronic obstructive pulmonary disease. Eur J Clin Invest. 2013;43(5):510–521. doi:10.1111/eci.12064
38. Huang S, Vasquez MM, Halonen M, Martinez FD, Guerra S. Asthma, airflow limitation and mortality risk in the general population. Eur Respir J. 2015;45(2):338–346. doi:10.1183/09031936.00108514
39. Kim CJ, Yoon HK, Park MJ, et al. Inhaled indacaterol for the treatment of COPD patients with destroyed lung by tuberculosis and moderate-to-severe airflow limitation: results from the randomized INFINITY study. Int J Chron Obstruct Pulmon Dis. 2017;12:1589–1596. doi:10.2147/copd.S128750
40. Kim SH, Moon JY, Min KH, Lee H. Proposed Etiotypes for Chronic Obstructive Pulmonary Disease: controversial Issues. Tuberc Respir Dis. 2024;87(3):221–233. doi:10.4046/trd.2023.0194
41. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission. Lancet. 2022;400(10356):921–972. doi:10.1016/s0140-6736(22)01273-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Derivatives of Reactive Oxygen Metabolites are Associated with Severity of Chronic Obstructive Pulmonary Disease and Affected by a p53 Gene Polymorphism
Yamamura K, Nojiri M, Nishiki K, Kato R, Shinomiya S, Takahara Y, Oikawa T, Ishizaki T, Toga H, Mizuno S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1589-1600
Published Date: 13 July 2022
TT3, a More Practical Indicator for Evaluating the Relationship Between Sarcopenia and Thyroid Hormone in the Euthyroid Elderly Compared with FT3

Chen J, Wei L, Zhu X, Xu W, Zou Y, Qi X, Fang J, Wang X, Shi X, Sheng Y, Ding G, Ouyang X, Duan Y
Clinical Interventions in Aging 2023, 18:1285-1293
Published Date: 4 August 2023
An Indian Consensus on Sarcopenia: Epidemiology, Etiology, Clinical Impact, Screening, and Therapeutic Approaches
Kalra S, Shaikh IA, Shende S, Kapoor N, Unnikrishnan A, Sharma O, Tiwaskar MH, Vora A, Verma SK, Kantroo V, Mehta P, Lovesley D, Sivakumar N, Kukreja BB, Kulkarni K, Deora A
International Journal of General Medicine 2025, 18:1731-1745
Published Date: 26 March 2025