")
Back to Journals » Open Access Emergency Medicine » Volume 17
Impact of Obesity on Orthopedic Injury and Fracture Patterns in Motor Vehicle Accidents
Authors Japa JP, Shats A , Zitser P , Lakhi N
Received 5 August 2024
Accepted for publication 23 April 2025
Published 17 May 2025 Volume 2025:17 Pages 185—193
DOI https://doi.org/10.2147/OAEM.S490123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Jonathan P Japa,1 Alina Shats,2 Philip Zitser,3 Nisha Lakhi4,5
1School of Medicine, New York Medical College, Valhalla, NY, USA; 2The University of Tampa, Tampa, FL, USA; 3The New York Institute of Technology, New York, NY, USA; 4New York Medical College, School of Medicine, Department of Obstetrics and Gynecology, Valhalla, NY, USA; 5Richmond University Medical Center, Department of Trauma Surgery, Staten Island, NY, USA
Correspondence: Nisha Lakhi, Richmond University Medical Center, Staten Island, NY, USA, Email [email protected]
Purpose: Obese trauma patients face a higher risk of mortality, prolonged ICU stays, and more complications than non-obese patients. However, some studies suggest that obesity might provide protective benefits in high-impact trauma situations through the “cushion effect”. This study will examine whether obesity influences fracture occurrence, injury severity, and clinical outcomes in motor vehicle accidents (MVA).
Methods: A retrospective study of 555 adult patients who presented to a Level 1 Trauma Center following a MVA from 2010– 2022. Patients with a Body Mass Index (BMI) greater than or equal to 30 kg/m2 were categorized as obese (178 patients, 32.6%), and those with a BMI less than 30 kg/m2 were classified as non-obese (377 patients, 67.4%). Incidence of bone fractures and injury severity were compared between both groups using injury severity score (ISS) and abbreviated injury scale (AIS). For variables significant on univariate analysis, binary logistic regression models were used to control age, gender, restraint use, and airbag deployment.
Results: The mean number of fractures (0.62 vs 0.46, p=0.096) and ISS (4.55 vs 4.51, p=0.703) were similar between the obese and non-obese groups. However, obese patients were more likely to experience upper extremity fractures (7.3% vs 3.4%, p=0.045) and lower extremity fractures (7.3% vs 2.7%, p =0.01), particularly fractures of the tibia/fibula (5.6% vs 1.6%, p=0.008). No significant differences were found in the incidence of head, thoracolumbar, or pelvic fractures between the two groups. After controlling for age, gender, restraint use, and airbag deployment, obesity remained an independent predictor of lower extremity fracture (aOR) 2.62 (95% CI: 1.01– 6.56), p = 0.04).
Conclusion: Obesity is an independent predictor of lower extremity fractures following a MVA. Clinicians should acknowledge potential differences in fracture occurrence and patterns between obese and non-obese patients during triage.
Keywords: motor vehicle accidents, body mass index, ISS, abbreviated injury score
Background
Obesity is an increasingly significant healthcare concern, affecting approximately 40% of adults in the U.S.1,2 Obesity tends to negatively impact multiple clinical contexts, including heart disease, diabetes, and trauma.1,3 Meta-analyses have demonstrated that obese trauma patients have an increased risk of mortality, longer ICU stays, and higher complication rates compared with non-obese patients.4 Similarly, morbidity and mortality have been found to be higher in obese patients who underwent orthopedic surgery following trauma.5 However, some studies have shown conflicting results regarding the notion that obesity might offer protection in specific trauma situations by providing a “cushion effect”.6–8 This concept was first introduced by Arbabi et al, who suggested that increased visceral adipose tissue may provide a “cushion” following blunt abdominal trauma.7 This study was the first to support an abdominal cushioning effect, finding that an “overweight” cohort (BMI 25 to 30) had a significantly decreased abdominal AIS score compared to a lean cohort (BMI <25) following a MVA.7 Similarly, Wang et al studied the effect of subcutaneous fat, measured using abdominal CT scan, on adult injury patterns in motor vehicle collisions and found that increased subcutaneous fat depth was associated with decreased injury severity to the head and abdominal regions but increased injury severity to the lower extremities8 Meanwhile, a meta-analysis investigating obesity in the setting of MVAs found no significant difference between obese and non-obese cohorts for abdominal injury, refuting the idea of a protective “cushioning effect”.6 Interestingly, all three aforementioned studies found that obesity was associated with increased lower extremity injuries.6–8
There is a plethora of data on MVA risk factors, including age, gender, and seat belt use, and their effect on clinical outcomes.9–11 For example, it has been found that the risk of injury following an MVA is higher in the young, while the risk of mortality is greater in males and the elderly.10 However, less is known about obesity as a risk factor, especially in the setting of orthopedic injury. A 2020 meta-analysis found a direct relationship between increased BMI and injury severity and mortality following an MVA; however, it did not examine orthopedic injury or fracture patterns.12 An earlier 2014 meta-analysis by Desapriya et al examined lower extremity injuries more closely and found that obese individuals had a higher risk of lower extremity and pelvic fractures following MVAs; however, fracture patterns in other body regions were not assessed.13 Given the paucity of data and conflicting findings surrounding the “cushion effect”, as well as limited knowledge with respect to orthopedic injury pattern, we aim to investigate if there is an association between obesity and orthopedic trauma severity following a MVA.
As obesity rates continue to rise, projections indicate that nearly half of the adult population will be classified as obese by 2030.14 Therefore, it is essential to investigate the relationship between obesity and motor vehicle accident (MVA) outcomes, as obesity is a modifiable risk factor. This study aims to compare the incidence of fractures and injury patterns between obese and non-obese patients involved in MVAs. Specifically, it will explore whether obesity influences fracture incidence, injury severity, and clinical outcomes in patients involved in motor vehicle collisions. Gaining a deeper understanding of how obesity impacts MVA outcomes, alongside other known risk factors, would enable various stakeholders—including vehicle manufacturers and healthcare providers—to anticipate injury patterns and devise strategies to improve outcomes.
Methods
Patient Population
This retrospective study was conducted at Richmond University Medical Center (RUMC), a Level 1 Trauma Center in Staten Island, NY. Data were collected from the electronic medical records (EMR) of patients who presented to the trauma center between January 2010 and 31, 2022. The study was approved by the Institutional Review Board of New York Medical College School of Medicine, our affiliate medical school (Protocol Number# 21575).
The primary objective of this study was to compare fracture occurrence and body region distribution in obese and non-obese patients following a MVA. Secondary objectives were comparing injury severity and clinical outcomes among both groups. Obesity was defined as BMI ≥ 30 kg/m2, according to the National Institutes of Health (NIH) and World Health Organization (WHO) guidelines.15,16 Adult patients presenting to our Level 1 trauma center during the study period following a MVA were included. Patients younger than 18 and those with missing height/weight or BMI information were excluded from analysis.
Data Source
The analyzed data points included patient demographics (age, race, ethnicity, sex), BMI, ISS, AIS by body region, Intensive Care Unit (ICU) length of stay, hospital stay, and in-hospital mortality (death). Fractures were categorized into five body regions, each comprising bones that anatomically correspond to that region. The five regions were the Head (cranium, facial bones), Upper Extremities (humerus, radius/ulna, hand), Thoracolumbar (ribs/sternum/clavicle/scapula, spine), Pelvis (hip bone, sacrum/coccyx), and Lower Extremities (femur/patella, tibia/fibula, foot). This classification of body regions aligns with other studies examining trauma,7,13 as well as a separate study focused on fractures.11
The AIS is an injury severity scoring system that classifies each injury by body region (head, face, thorax, abdomen, spine, extremity, or pelvic girdle, and unspecified) on a 14-point scale. An AIS score greater than 3 for any region was considered a serious injury.17 The ISS is an anatomical scoring system that grades patients with multiple injuries with an overall score. To calculate this score, the highest AIS score in each body region is used. The three most severely injured body regions have their score squared and added together to produce the ISS score.17
Statistical Analysis
Statistical analysis was carried out using IBM SPSS 28.0. Data points for continuous variables were plotted to assess distribution. Univariate analyses for continuous variables were compared using a t-test if normally distributed or a Mann–Whitney U-test for non-parametric distribution. Categorical data was compared using the χ2-test or Fisher’s exact tests. A p-value of <0.05 was considered statistically significant. Risks were reported as odds ratios (OR) with 95% confidence intervals (CI). In order to determine if obesity is an independent predictor of the primary outcome (fracture occurrence), body regions that were statistically significant on univariate analysis were tested using logistic regression models controlling for age, gender, restraint use, and airbag deployment. We chose to control for these variables as they have been identified as possible confounders that could impact fracture and injury occurrence/severity independent of obesity.11,13 Variables on multivariable regression were reported as adjusted odds ratios (aOR) with a 95% confidence interval.
The approximate number of patients was anticipated by IBM SPSS. We performed an a priori power analysis. Based on data from Gilbert et al18 that evaluated altered lower extremity fracture characteristics in obese pediatric trauma patients, we estimated a small-medium effect size (w=0.02) when considering the effect of obesity on fracture occurrence. Using their data and assuming a “two-tail test” with at least 80% power and alpha=0.05, we estimate that a total of 321 patients would provide sufficient power.
Results
Patient Demographics
In the period between 01 January 2010 and 31 December 2022, a total of 555 adult patients involved in MVAs presented to the trauma center. Those with a BMI greater than or equal to 30 kg/m2 were categorized as obese (178 patients, 32.6%) and those with a BMI less than 30 kg/m2 were classified as non-obese (377 patients, 67.4%). The mean (standard deviation) BMI of the obese group compared to the non-obese groups was 34.3 (4.8) kg/m2 vs 25.6 (3.0) kg/m2, p<0.001. Both groups exhibited similarities in age, sex, and race/ethnicity (Table 1). Race distribution was similar between the obese and non-obese group (p=0.971), with a majority of patients being non-Hispanic White, followed by non-Hispanic Black (Table 1). Restraint use (76.7% vs 81.0%, p=0.263) and airbag deployment (63.6% vs 68.2%, p=0.303) were similar between both groups, respectively (Table 1).
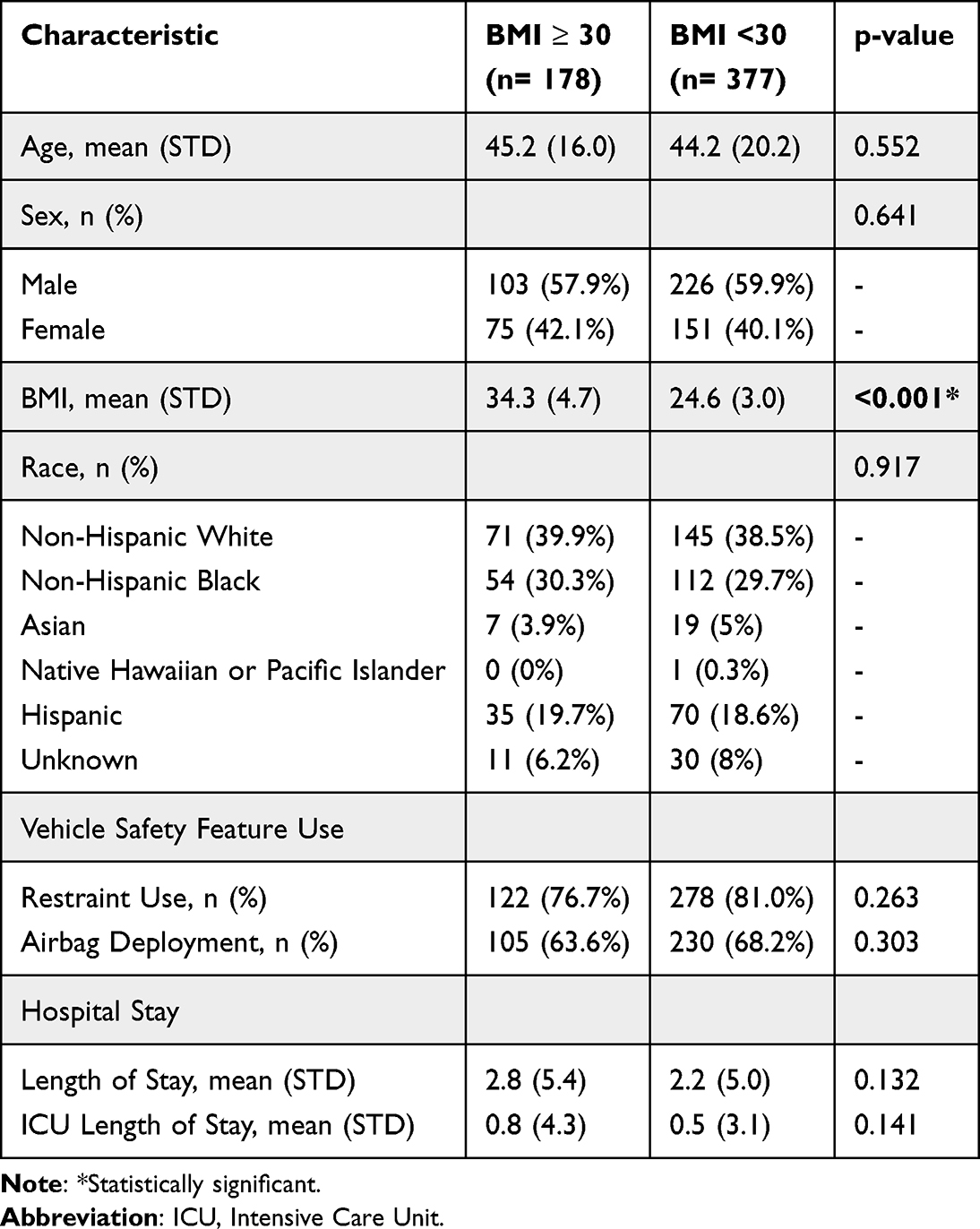 |
Table 1 Patient Demographics |
Fracture Occurrence and Location
The mean number of fractures was similar between obese and non-obese patients (0.62 (1.21) vs 0.46 (0.99), p=0.096). Open fractures occurred at a similar rate (2.2% vs 0.8%, p=0.153), respectively. With respect to location, obese patients were more likely to sustain a fracture of the upper extremity (7.3% vs 3.4%, p=0.045) and lower extremity (7.3% vs 2.7%, p =0.01) regions. Within the lower extremity region, fractures were more likely to involve the tibia/fibula (5.6% vs 1.6%, p=0.008). However, incidences of fractures involving the femur, patella, and foot were similar. For fractures involving the upper extremity, there were no specific bony locations (humerus, radius/ulna, hand) that were more likely to be fractured (Table 2). Additionally, there were no differences in head (cranium/facial bones), thoracolumbar (ribs/sternum/clavicle/scapula, spine), or pelvic (hip, sacrum/coccyx) fracture occurrence between the two groups (Table 2).
 |
Table 2 Obese and Non-Obese MVA Outcomes |
Injury Severity
Mean ISS score was similar for obese and non-obese patients (4.55 (7.46) vs 4.51 (7.20), p=0.703). Obese patients were more likely to have a severe thorax injury (Thorax AIS score ≥ 3) (46.2% vs 24.1%, p=0.044). However, severe injury in other body regions (Head, Face, Neck, Spine, Upper Extremity, Lower Extremity) was similar between both groups (Table 2).
Patient Outcomes
Mean Length of Stay (LOS) in the hospital (2.83 (5.36) days vs 2.16 (5.02), p=0.132) and mean length of ICU stay (0.75 (4.34) days vs 0.49 (3.06), p=0.141) were similar between obese and non-obese patients. None of the individuals in our study population experienced in-hospital mortality (death) during their index hospital admission.
Regression Analysis
For lower extremity fracture, binary logistic regression analysis was conducted to control for patient gender, age, use of restraint, and airbag deployment. Our model (χ2 (5, N=555) =13.41, p=0.02) outperformed the null model and demonstrated that obesity (aOR 2.62 (95% CI: 1.01–6.56), p = 0.04) retained statistical significance, indicating that it was an independent prediction of lower extremity fracture. Similarly, for tibial/fibular fractures, controlling for the same variables, our model (χ2 (5, N=555) =22.09, p<0.001) outperformed the null model (aOR 3.20 (95% CI: 1.01–9.47), p = 0.004) and demonstrated that obesity was independent predictor of a fracture involving the tibia or fibula.
For upper extremity fracture, our model (χ2 (5, N=555) =25.96, p<0.001) outperformed the null model. Although obesity increased the likelihood of upper extremity fracture, it fell short of statistical significance (aOR 2.33 (95% CI: 0.97–5.59, p = 0.058), indicating that other predictor variables (gender, age, restrain use, and airbag deployment) may also influence the occurrence of upper extremity fractures.
Discussion
The role of obesity in orthopedic trauma following MVAs has not been studied extensively, as most research involving obese cohorts has concentrated on other clinical outcomes after MVAs. This study analyzed the connection between obesity, fracture patterns, and injury severity in MVAs. On univariate analysis, we discovered that obese patients experienced a higher incidence of upper and lower extremity fractures compared to non-obese patients. After adjusting for gender, age, restraint use, and airbag deployment, obesity was identified as an independent predictor of lower extremity fractures.
The higher incidence of lower extremity fractures observed in the obese cohort aligns with the meta-analysis by Desapriya et al, which reported that obese individuals had a 39% increased risk of sustaining a lower extremity fracture compared to non-obese patients in the context of MVAs.13 Furthermore, the analysis revealed that obese patients experienced a 33% reduced risk of head injuries and were no more likely to suffer pelvic fractures or abdominal injuries compared to their non-obese counterparts.13 Additional studies have also indicated a reduced incidence of head injuries in obese trauma patients.14,15 For instance, in a study involving blunt trauma patients, Boulanger et al found that skull fractures and cerebral injuries, defined by intracranial traumatic lesions on CT scans, were less frequent in obese patients.15 Consistent with these findings, we observed a trend favoring reduced head injury severity between obese and non-obese groups (4.2% vs 10.9%, p=0.09). However, it did not achieve statistical significance. The reason for the lower incidence of head injury in obese patients remains unclear, but it may be associated with a reduced head-to-torso ratio.13 Future studies are necessary to enhance understanding in this area.
Kent et al utilized simulated cadaver crashes to investigate injury patterns and identified possible mechanisms for greater injury risk to the lower extremities. The study found that obese individuals, by virtue of larger mass, have greater hip excursion and less torso-forward pitch during impact, resulting in higher injury risk to the thorax but lower injury risk to the head.19 The greater hip excursion also causes an increased excursion of the lower extremities, where they are more likely to collide with the vehicle’s instrument panel.20,21 While our study did not find a difference in injury severity to the lower extremities between the two groups, we did observe a greater incidence of lower extremity fractures in the obese group, and it stands to reason that this same mechanism may be responsible. Another study examining the effect of age, BMI, and gender on outcomes of serious to fatal MVA injuries specifically described that increased hip excursion in obese individuals predisposes them to knee-thigh-hip fractures and below-the-knee injuries.19 In concordance with these observations, we found that obese individuals were more likely to have a greater incidence of tibia/fibula fractures. Several other studies have found similar associations between obesity and lower extremity injuries.21–23
Our study found a greater incidence of upper extremity fractures in obese individuals. Similarly, in a retrospective study of 13,470 occupants sampled from the US National Automotive Sampling System, Joodaki et al compared MVA injuries across different BMI categories and found that a BMI of 35–40 was associated with an increased risk of upper extremity injury.21 Furthermore, this study found radial fractures to be amongst the most common injuries in those with BMI ≥30. A study by Kent et al that conducted frontal impact sled tests using obese and non-obese human cadavers postulated some possible mechanisms to explain the upper extremity findings. The study suggested that a reduced forward pitch of the torso in obese individuals makes airbag deployment less likely.19 Additionally, the study noted a delay in seatbelt activation in obese passengers. The delay occurs because the belt must initially cause a deformation in the adipose tissue before encountering the hard, bony structures of the pelvis and chest that ultimately trigger activation.19 These mechanisms may lead to upper extremity injuries by allowing the torso to launch more forward into the vehicle’s interior.
The increased incidence of severe thoracic injury (AIS≥ 3) seen in our study may be explained by the additional forces applied by seatbelts to obese individuals during a MVA.19,20 Due to their greater mass, obese individuals will have greater kinetic energy during a crash and seatbelts will have to apply more force to decelerate the torso and individual.24 Specifically, the greater force would be applied to the lower, more complaint portion of the thorax, which may result in pulmonary contusion and rib fracture, as cited by Zhu et al.25 This may account for the greater incidence of severe thoracic injury seen in obese patients in our study. However, this did not result in a greater incidence of rib or thoracolumbar fractures.
There is controversy surrounding obesity and its effect on abdominal injuries. Some studies found that obese patients have fewer severe abdominal injuries,7,13 while others found no differences between groups.6,12 Studies that found fewer severe injuries attribute this to the “cushion effect” which posits that greater adiposity seen in obese individuals serves as an added layer of protection and results in fewer injuries. A study by Zhu et al found a U-shaped relationship, where being overweight (25 kg/m2≤BMI<30 kg/m2) provided a protective effect, but being obese (BMI≥30 kg/m2) increased the risk of severe abdominal injury (AIS≥2). The study suggests that severe abdominal injuries are seen more often in obese individuals because the greater momentum (mass x velocity) seen at higher BMIs overrides the potential protective effect of adiposity.25 The study by Kent et al mentioned previously investigated the cushion effect directly and did not find obesity to reduce abdominal injury in cadaveric models.19 While the legitimacy of the cushioning effect remains to be clarified, another important factor to consider is body fat deposition among individuals, as different patterns of fat density (central adiposity vs peripheral adiposity) may be protective or may be associated with certain injuries. Further studies are needed in this area, as BMI alone may not be the best marker for risk stratification in this context.
Our study identified differences between obese and non-obese individuals in MVAs that can guide car manufacturers and regulatory bodies in developing vehicles and safety measures. These differences arise from the larger body habitus of obese individuals. Vehicle manufacturers could create vehicles with larger seatbelts and more spacious interiors. More spacious interiors may reduce the likelihood of an individual’s legs colliding with the interior during an MVA. Reports indicate that some obese individuals avoid using seatbelts due to poor fit or discomfort.26 Larger seatbelts could help address this issue, and in terms of car manufacturing, they are significantly easier to implement than redesigning vehicle interiors. Some car manufacturers have already implemented changes in their cars to accommodate obese individuals. For example, BMW has instituted a project called “Plump my Ride”, where they test how driving ability is affected by obesity and implemented ergonomic solutions to accommodate obese drivers.27 Additionally, governing bodies could be more involved by requiring crash testing across different BMIs. Currently, the standard crash dummy used by the US Department of Transportation represents a 50th percentile male subject (5 feet 10 inches, 171 pounds).28 Although smaller dummies are available to replicate women and children, there are fewer options available to represent obese individuals. While changes to vehicle design and testing are important, they can only go so far; managing obesity itself is crucial. Healthcare providers recognize the mortality and morbidity associated with obesity and must collaborate with patients to prevent it. Providing education to patients not only on the commonly recognized medical complications of obesity but also on the potential risks in the event of an accident is essential to the discussion and prevention of related issues of obesity.
A significant strength of this study was the inclusion of a large and diverse population of patients from a busy Level 1 Trauma Center in a metropolitan area. This enabled a more accurate representation of the general population, considering that obesity is prevalent throughout the United States. We also adjusted for gender and age in our multivariate models. Adjusting for gender may be important due to biological differences in fat distribution, with males typically exhibiting greater adiposity above the waist and females having more deposition below the waist.
The study’s limitations included its retrospective nature and the emphasis on a single center despite the diversity of its patient population. Additionally, differences between our findings and existing literature may arise from crash characteristics that were not examined in this study. These characteristics include crash severity (measured as delta V), impact direction, vehicle type and size, position in the vehicle (passenger vs driver), and weather conditions. Another important factor to consider is body fat distribution among individuals since differing patterns of fat density might provide protection or be associated with specific injuries. Incorporating these factors in future research will either confirm the associations we discovered or unveil entirely new ones.
Conclusion
Our study aimed to investigate the relationship between obesity and MVA outcomes, and we successfully identified several associations. We found that obese individuals had a higher incidence of upper and lower extremity fractures, particularly tibia and fibula fractures in the lower extremity. Additionally, we noted a greater incidence of severe thoracic injury (AIS≥3). Our findings align with prior studies and contribute to the ongoing discussion about obesity and MVAs. Future research can expand by examining specific crash parameters and uncovering new connections that automotive industry and healthcare workers can use to ensure the safety of all patients.
Ethics Approval
Ethical approval was obtained from the Institutional Review Board of New York Medical College School of Medicine Protocol Number# 21575. Patient data was protected, stored securely, and de-identified to protect confidentiality.
Consent to Participate
Informed consent was waived due to the retrospective nature of the research.
Funding
The authors did not receive support from any organization for the submitted work.
Disclosure
The authors report no competing or financial interests to declare relevant to this article’s content. This study complies with the Declaration of Helsinki.
References
1. Panuganti KK, Nguyen M, Kshirsagar RK. Obesity. Treasure Island, FL: StatPearls Publishing; 2023.
2. Stierman B, Afful J, Carroll MD, et al. National health and nutrition examination survey 2017–march 2020 prepandemic data files development of files and prevalence estimates for selected health outcomes. Nat Health Statistics Reports. 2021;158:10–5620.
3. Abdul WR, Cohen RV, Le Roux CW. Recent advances in the treatment of patients with obesity and chronic kidney disease. Ann Med. 2023;55(1):2203517.
4. Liu T, Chen JJ, Bai X, Zheng GS, Gao W. The effect of obesity on outcomes in trauma patients: a meta-analysis. Injury. 2013;44(9):1145–1152. doi:10.1016/j.injury.2012.10.038
5. Parratte S, Pesenti S, Argenson JNA. Obesity in orthopedics and trauma surgery. Orthop Traumatol Surg Res. 2014;100(1):S91–97. doi:10.1016/j.otsr.2013.11.003
6. Hoebee S, Ron E, Alattar Z, Kang P, VanSonnenberg E. Assessing the “cushion effect”: a systematic review and meta-analysis of the role of obesity in motor vehicle injuries and fatalities. J Intensive Care Med. 2022;37(3):293–303. doi:10.1177/0885066621989978
7. Arbabi S, Wahl WL, Hemmila MR, Kohoyda-Inglis C, Taheri PA, Wang SC. The cushion effect. J Trauma. 2003;54(6):1090–1093. doi:10.1097/01.TA.0000064449.11809.48
8. Wang SC, Bednarski B, Patel S, et al. Increased depth of subcutaneous fat is protective against abdominal injuries in motor vehicle collisions. Ann Proceedings Assoc Advancement Automotive Med. 2003;47:545–559.
9. Abaid N, Macinko J, Silver D, Porfiri M. The effect of geography and citizen behavior on motor vehicle deaths in the United States. Public Library Sci One. 2015;10(4). doi:10.1371/journal.pone.0123339
10. Karaye IM, Olokunlade T, Cevetello A, Farhadi K, Kyriacou CM. Examining the trends in motor vehicle traffic deaths in New York City, 1999-2020. J Community Health. 2023;4(48):634–639. doi:10.1007/s10900-023-01203-x
11. Almigdad A, Mustafa A, Alazaydeh S, Alshawish M, Mustafa MB, Alfukaha H. Bone fracture patterns and distributions according to trauma energy. Adv Orthopedics. 2022;2022(1):1–12. doi:10.1155/2022/8695916
12. Homaie RE, Khodadady-Hasankiadeh N, Kouchakinejad-Eramsadati L, et al. The relationship between weight indices and injuries and mortalities caused by the motor vehicle accidents: a systematic review and meta-analysis. J Injury Violence Res. 2020;12(1):85–101. doi:10.5249/jivr.v12i1.1198
13. Desapriya E, Giulia S, Subzwari S, et al. Does obesity increase the risk of injury or mortality in motor vehicle crashes? A systematic review and meta-analysis. Asia-Pacific J Public Health. 2014;26(5):447–460. doi:10.1177/1010539511430720
14. Moran SG, McGwin G, Metzger JS, Windham ST, Reiff DA, Rue LW. Injury rates among restrained drivers in motor vehicle collisions: the role of body habitus. J Trauma. 2002;52(6):1116–1120. doi:10.1097/00005373-200206000-00015
15. Boulanger BR, Milzman D, Mitchell K, Rodriguez A. Body habitus as a predictor of injury pattern after blunt trauma. J Trauma. 1992;33(2):228–232. doi:10.1097/00005373-199208000-00011
16. Ward ZJ, Bleich SN, Cradock AL, et al. Projected US state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381(25):2440–2450. doi:10.1056/NEJMsa1909301
17. Palmer CS, Gabbe BJ, Cameron PA. Defining major trauma using the 2008 abbreviated injury scale. Injury. 2016;47(1):109–115. doi:10.1016/j.injury.2015.07.003
18. World Health Organization. Obesity: preventing and managing the global epidemic: report of a WHO consultation. World Health Organization; 1997. Available from: https://iris.who.int/handle/10665/42330.
19. Kent RW, Forman JL, Bostrom O. Is there really a cushion effect?: a biomechanical investigation of crash injury mechanisms in the obese. Obesity. 2010;18(4):749–753. doi:10.1038/oby.2009.315
20. Carter PM, Flannagan CA, Reed MP, Cunningham RM, Rupp JD. Comparing the effects of age, BMI and gender on severe injury (AIS 3+) in motor-vehicle crashes. Accid Anal Prev. 2014;72:146–160. doi:10.1016/j.aap.2014.05.024
21. Joodaki H, Gepner B, McMurry T, Kerrigan J. Comparison of injuries of belted occupants among different BMI categories in frontal crashes. Int J Obesity. 2020;44(6):1319–1329. doi:10.1038/s41366-019-0481-2
22. Ryb GE, Dischinger PC. Injury severity and outcome of overweight and obese patients after vehicular trauma: a crash injury research and engineering network (CIREN) study. J Trauma. 2008;64(2):406–411. doi:10.1097/TA.0b013e31802beff9
23. Rupp JD, Flannagan CA, Leslie AJ, Hoff CN, Reed MP, Cunningham RM. Effects of BMI on the risk and frequency of AIS 3+ injuries in motor-vehicle crashes. Obesity. 2013;21(1):E88–97. doi:10.1002/oby.20079
24. Cormier JM. The influence of body mass index on thoracic injuries in frontal impacts. Accid Anal Prev. 2008;40(2):610–615. doi:10.1016/j.aap.2007.08.016
25. Zhu S, Kim JE, Ma X, et al. BMI and risk of serious upper body injury following motor vehicle crashes: concordance of real-world and computer-simulated observations. Public Lib Sci Med. 2010;7(3). doi:10.1371/journal.pmed.1000250
26. Schlundt DG, Briggs NC, Miller ST, Arthur CM, Goldzweig IA. BMI and seatbelt use. Obesity. 2007;15(11):2541–2545. PMID: 18070742. doi:10.1038/oby.2007.303
27. Admin. Obesity crisis hits car manufacturing industry. Healthcare Digital. Bizclik Media Ltd; 2020. Available from: https://healthcare-digital.com/technology-and-ai/obesity-crisis-hits-car-manufacturing-industry.
28. National Highway Traffic Safety Administration. (n.d.). NHTSA’s crash test dummies. National Highway Traffic Safety Administration; 2023. Available from: https://www.nhtsa.gov/crash-test-dummies.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlation of Body Mass Index with Clinicopathologic Parameters in Patients with Idiopathic Membranous Nephropathy
Chen X, Chen S, Li Z, Pan X, Jia Y, Hu Z, Niu K, Liu B, Ren Q
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1897-1909
Published Date: 20 June 2022
Body Mass Index and New-Onset Atrial Fibrillation in Patients with Acute Myocardial Infarction
Liu L, Liu X, Ding X, Chen H, Li H
International Journal of General Medicine 2022, 15:5717-5728
Published Date: 21 June 2022
All Types Obesity and Physical Inactivity Associated with the Risk of Activity of Daily Living Limitations Among People with Asthma
Alhammad SA, Alwadeai KS
Journal of Multidisciplinary Healthcare 2022, 15:1573-1583
Published Date: 22 July 2022
Association Between Nutritional Knowledge, Dietary Regimen, and Excess Body Weight in Primary School Teachers
Saintila J, Calizaya-Milla YE, Calizaya-Milla SE, Elejabo-Pacheco AA, Sandoval-Valentin GA, Rodriguez-Panta SG
Journal of Multidisciplinary Healthcare 2022, 15:2331-2339
Published Date: 14 October 2022
Association of Patient Anthropometric Measurements and Dental Implant Treatment
Al-Radha ASD
Clinical, Cosmetic and Investigational Dentistry 2023, 15:51-61
Published Date: 6 April 2023