")
Back to Journals » Cancer Management and Research » Volume 17
Impact of Radiation Therapy Techniques on Hippocampal Doses and Psychological Status in Patients With Nasopharyngeal Carcinoma
Authors Gai X, Huang S, Zeng J, Chen J, Liu F, Li S, Lv W, Guo F, Cai C, Hong J , Su L
Received 17 September 2024
Accepted for publication 27 December 2024
Published 16 January 2025 Volume 2025:17 Pages 83—90
DOI https://doi.org/10.2147/CMAR.S492449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Xiujuan Gai,1– 3,* Shiqi Huang,1,2,* Jiang Zeng,1,2,4 Jun Chen,1,2,4 Feng Liu,1,2,4 Shan Li,1,2,4 Wenlong Lv,1,2,4 Feibao Guo,1,2,4 Chuanshu Cai,1,2,4 Jinsheng Hong,1,2,4 Li Su1,2,4
1Department of Radiotherapy, Cancer Center, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 2Department of Radiotherapy, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical Universisty, Fuzhou, Fujian, 350212, People’s Republic of China; 3Department of Oncology, Laiyang Central Hospital of Yantai, Yantai, 265200, People’s Republic of China; 4Key Laboratory of Radiation Biology of Fujian Higher Education Institutions, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Su; Jinsheng Hong, Department of Radiotherapy, Cancer Center, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To investigate the impact of Intensity-Modulated Radiation Therapy (IMRT) and Volumetric Modulated Arc Therapy (VMAT) on hippocampal radiation dosage and psychological status in patients newly diagnosed with nasopharyngeal carcinoma (NPC).
Patients and Methods: A retrospective analysis was conducted on 269 NPC patients who received initial treatment between January 2013 and April 2022. Patients were categorized into the IMRT group and the VMAT group based on the radiotherapy technique employed. The differences in hippocampal doses for NPC patients at different stages between the two groups were analyzed. The Hospital Anxiety and Depression Scale (HADS) was used to assess patients’ anxiety and depression states. Before radiotherapy, patients with anxiety scores (HADS-A) between 0 and 10 points were included to analyze the differences in anxiety occurrence rates between IMRT and VMAT techniques. Similarly, patients with depression scores (HADS-D) between 0 and 10 points were included to analyze the differences in depression occurrence rates between the two radiotherapy techniques.
Results: In patients with T1-2 stage, those treated with IMRT had significantly higher hippocampal doses compared to those treated with VMAT. Furthermore, after radiotherapy, the occurrence rates of anxiety (HADS-A ≥ 11) and depression (HADS-D ≥ 11) in the IMRT group were 27.3% and 19.5%, respectively, while in the VMAT group, they were 9.5% and 7.4%, both showing significant statistical differences (P=0.010, P=0.035). However, there was no significant correlation between the radiotherapy technique and anxiety or depression occurrence rates in patients with T3-4 stage. Additionally, age and gender exhibited certain influences on psychological status.
Conclusion: In the absence of hippocampal protection, opting for a VMAT treatment plan over IMRT may potentially reduce the incidence of anxiety and depression. This perspective offers new insights for optimizing treatment strategies and improving quality of life.
Keywords: nasopharyngeal carcinoma, IMRT, VMAT, hippocampal doses, psychological status
Introduction
Radiation therapy (RT) is the primary treatment modality for patients newly diagnosed with nasopharyngeal carcinoma (NPC). Increasing research has revealed that psychological complications or emotional abnormalities related to treatment may occur in NPC patients after radiotherapy,1–3 with incidence significantly higher than in other head and neck malignancies.4 Among these, anxiety and depression are the most prevalent psychological disorders.5
Psychological conditions are influenced by various factors,6–9 and radiation-induced damage to the hippocampus cannot be overlooked. Animal studies have shown that the hippocampus plays a crucial role in emotional regulation, and radiation can reduce the neurogenesis of the hippocampus in rodents.10,11 Damage to hippocampal neurons is considered one of the potential mechanisms for emotional abnormalities.12–14 Our previous research also found a correlation between hippocampal radiation dose and the occurrence of anxiety.15 Therefore, the effective preservation of the hippocampus is a pressing clinical issue.
Intensity Modulated Radiation Therapy (IMRT) and Volumetric Modulated Arc Therapy (VMAT) are currently the most commonly used techniques in NPC radiotherapy. Some studies have indicated that VMAT provides superior dosimetric hippocampal protection in NPC treatment plans compared to IMRT.16,17 However, there is currently no research focused on the differential hippocampal dosimetry effects of these two radiotherapy plans on psychological status. This study aims to explore the dosimetric differences in the hippocampus between VMAT and IMRT plans when hippocampal protection is not implemented and their impact on psychological status.
Materials and Methods
Participants
A retrospective study was conducted at the Department of Radiotherapy, First Affiliated Hospital of Fujian Medical University, from January 2013 to April 2022, with a total of 269 patients included. Inclusion criteria were as follows: (1) histopathological diagnosis, (2) age between 18 and 75 years, (3) Karnofsky Performance Status (KPS) score ≥70, (4) receipt of radical radiotherapy, and (5) completion of the Hospital Anxiety and Depression Scale (HADS) questionnaire.18 Exclusion criteria were: (1) a history of a second primary tumor or prior malignant tumor treatment, (2) a history of cerebrovascular disease, brain surgery, or other central nervous system disorders, (3) history of mental or psychological illness or long-term use of sedatives or anxiolytics, or recent use of such medications, and (4) treatment discontinuation or incomplete questionnaire response.
This study was approved by the Human Research Ethics Committee of the First Affiliated Hospital of Fujian Medical University (MTCA, ECFAH of FMU [2015]084–2). Given the retrospective nature of the research, informed consent was waived.19
Psychological Status Assessment
The HADS questionnaire is a widely used clinical screening tool for assessing anxiety and depression and has good reliability and validity. Patients’ psychological status was assessed using the HADS both prior to and following radiotherapy. The pre-radiotherapy questionnaire was typically administered either the day before or on the day of radiotherapy, while the post-radiotherapy assessment was usually completed on the day of the final session. The scale comprises a total of 14 items, with seven items dedicated to anxiety assessment (HADS-A) and another seven items for depression assessment (HADS-D). Each item is scored on a scale from 0 to 3, with the maximum possible scores for HADS-A and HADS-D being 21 points, respectively. Scoring within the range of 0–7 points indicates the absence of symptoms, 8–10 points signify a suspected presence, and 11–21 points indicate a definite presence.
Before radiotherapy, patients with HADS-A scores in the range of 0–10 points were included in the anxiety group (Group-A), and those with HADS-D scores in the range of 0–10 points were included in the depression group (Group-D). This categorization was done to analyze the differences in anxiety or depression incidence rates between the two radiotherapy plans.
Based on HADS-A scores post-radiotherapy, patients in Group-A were further divided into the normal group (Group-NA, HADS-A scores of 0–10 points) and the abnormal group (Group-AA, HADS-A scores of ≥11 points). Similarly, based on HADS-D scores post-radiotherapy, patients in Group-D were divided into the normal group (Group-ND, HADS-D scores of 0–10 points) and the abnormal group (Group-AD, HADS-D scores of ≥11 points).
Hippocampi Delineation
The hippocampi were re-mapped by team members. Combined with computerized tomography (CT) and magnetic resonance imaging (MRI) fusion images, bilateral hippocampi were delineated on the localization CT images. In reference to previous research protocols,20 the delineation was initially performed by a uniformly trained oncologist and then reviewed by a senior oncologist with either more than 10 years of clinical experience or a rank of associate chief physician or higher. Any discrepancies were resolved through collective discussion within the research team.
DVH Analysis of Hippocampi
Radiotherapy was planned using the RayStation treatment planning system (version 4.7, Raysearch Laboratories, Sweden), and dosimetric parameters of the hippocampi were obtained through dose volume histogram (DVH). The hippocampal doses were recalculated based on the initial radiotherapy plans.
Treatment
Radiotherapy
The tumor target area and related organs at risk were sketched on the localization CT images by the same oncologist and confirmed by another senior physician. The target area delineation followed the nasopharyngeal carcinoma target area delineation standard of our center.21 Gross tumor volume (GTV) referred to the gross tumor area visible in clinical examination or imaging examination, including nasopharyngeal and neck (plain scan or enhanced) CT, MRI, or PET-CT. GTV included primary focus (GTVnx) and metastatic regional lymph nodes (GTVnd). Clinical tumor volume (CTV) referred to the range that the tumor may invade, that was, subclinical lesions. CTV included the CTV of primary nasopharyngeal tumors, the CTV of positive lymph nodes and the lymphatic drainage area, and was divided into high-risk area (CTV1) and low-risk area (CTV2) according to the risk degree. Planning tumor volume (PTV) included the positioning error and the movement range of the target area between treatment and treatment. The external expansion of 3 mm in each direction of GTV, CTV1, and CTV2 was the corresponding PTV. The prescribed doses of PTVnx and PTVnd were 66–76Gy, 2.12–2.33Gy/fraction, 5 times a week, a total of 30–33 times. The prescribed doses of PTV1 and PTV2 were 60–62Gy and 50–56Gy, respectively. The radiation doses to the organs at risk were in accordance with Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) and Radiation Therapy Oncology Group (RTOG) 061522 and RTOG 0225.23
Due to the recalculated hippocampal doses based on the initial radiotherapy plans, the hippocampi were not spared in the planning process.
Chemotherapy
According to AJCC staging criteria,24,25 patients with TNM stage I should be given radiotherapy alone, while patients with stage II–IV should be individually selected to receive chemoradiotherapy or radiotherapy alone. Neoadjuvant chemotherapy and adjuvant chemotherapy regimens were 5-Fu 500–750 mg/m2, D1-5 combined with cisplatin (DDP) 75–80 mg/m2, D1-3, q3w or paclitaxel 135–175 mg/m2, d1 combined with DDP 75–80 mg/m2, D1-3, q3w or docetaxel 75 mg/m2, d1 combined with DDP 75–80 mg/m2, D1-3, q3w. Synchronous chemotherapy regiments were DDP 40 mg/m2, qw or 80 mg/m2, q3w.
Statistical Analysis
SPSS 22.0 was used for data analysis. Quantitative data were analyzed by independent sample t test or Mann–Whitney U nonparametric test. Qualitative data were analyzed using χ2 test or Fisher’s Exact Test. Bilateral P values <0.05 were considered statistically significant.
Results
Patient Characteristics
This retrospective study included a total of 269 patients, among whom 152 were in T1-2 stage, and 117 were in T3-4 stage. Within the T1-2 stage, there were 129 patients (Group-A) for analyzing the difference in anxiety incidence between IMRT and VMAT radiotherapy techniques and 145 patients (Group-D) for analyzing the difference in depression incidence between the two radiotherapy techniques. In both Group-A and Group-D, there were statistically significant differences in smoking status between the IMRT and VMAT subgroups (P=0.004 and P=0.008, respectively), as shown in Table 1. Baseline data for patients in T3-4 stage and differences in clinical characteristics between IMRT and VMAT radiotherapy techniques are presented in Table 2.
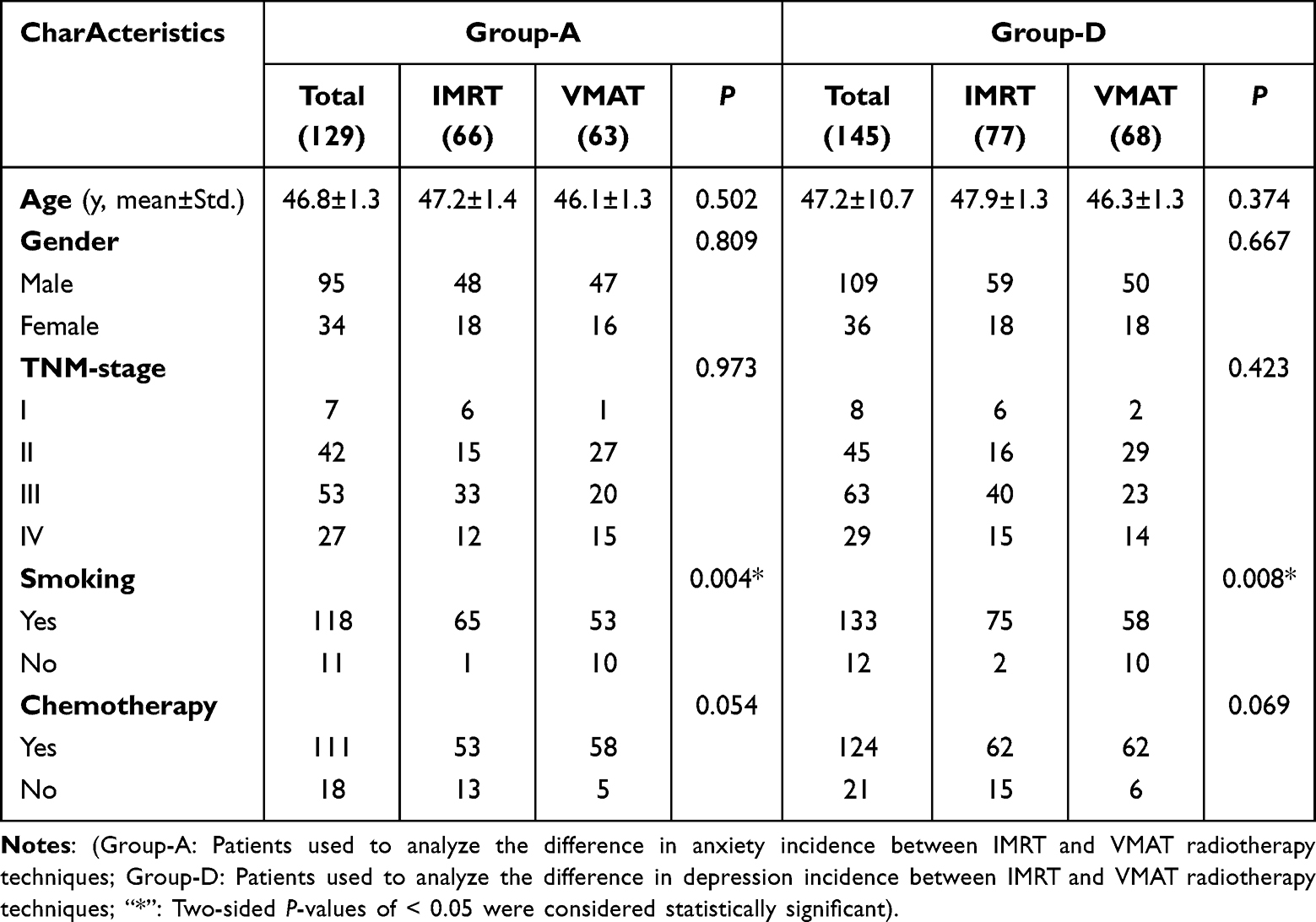 |
Table 1 Clinical Characteristic Differences Between IMRT and VMAT Radiotherapy Techniques for Patients in Group-A and Group-D of T1-2 Stage |
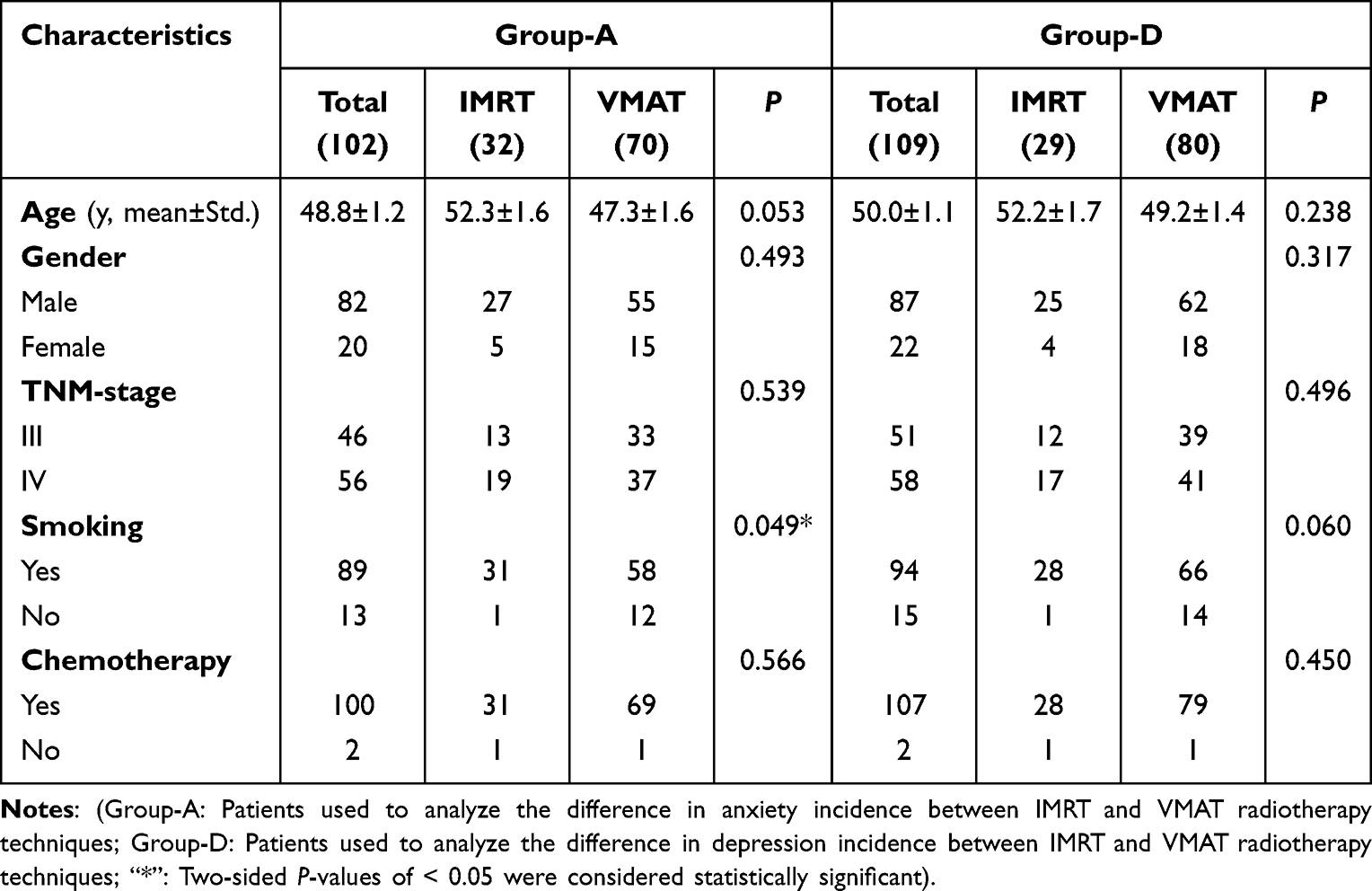 |
Table 2 Clinical Characteristic Differences Between IMRT and VMAT Radiotherapy Techniques for Patients in Group-A and Group-D of T3-4 Stage |
Comparison of Hippocampal Dosimetry
Table 3 illustrates the hippocampal dosimetry distribution and differences between IMRT and VMAT radiotherapy techniques for patients with different stages of nasopharyngeal carcinoma. The results revealed that, for T1-2 stage patients, hippocampal doses were significantly higher in those treated with IMRT compared to those treated with VMAT. However, for T3-4 stage patients, there were no statistically significant differences in hippocampal doses between the two radiotherapy techniques.
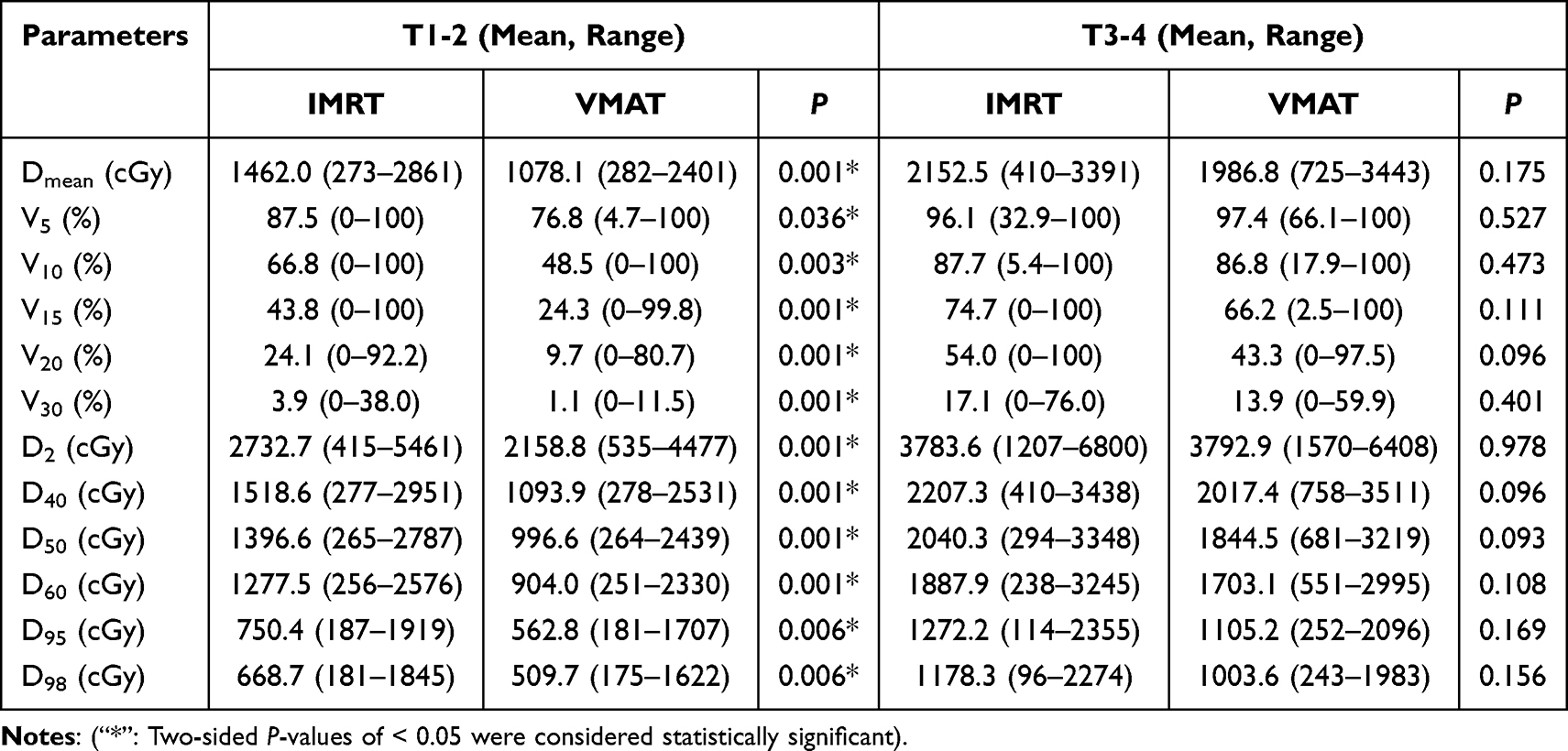 |
Table 3 Differences in Hippocampal Dosimetry Between Nasopharyngeal Carcinoma Patients at Different Stages Treated With IMRT and VMAT Techniques |
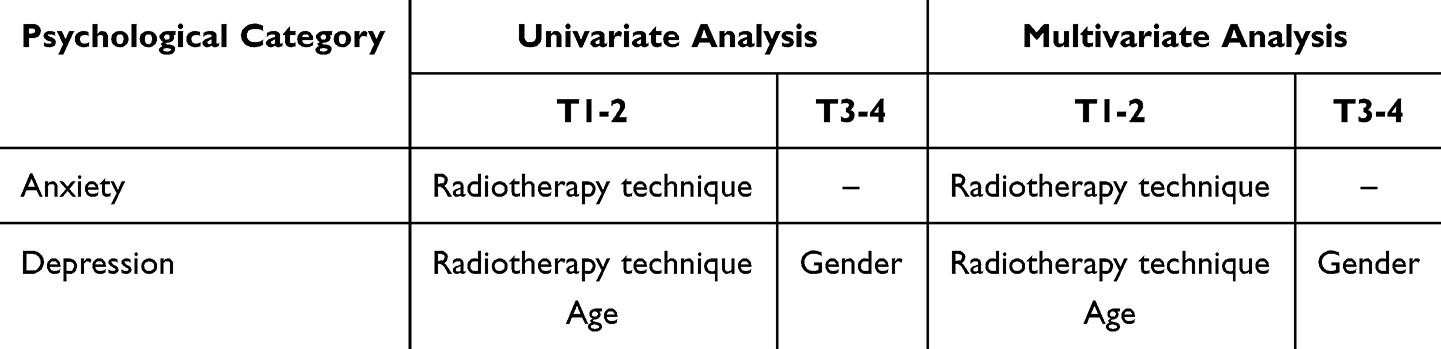 |
Table 4 Factors Influencing Anxiety and Depression Status in Nasopharyngeal Carcinoma Patients at Different Stages |
Comparison of Anxiety and Depression Incidence Rates With Different Radiotherapy Techniques
After radiotherapy, 24 cases that tested positive were assigned to Group-AA for T1-2 stage patients of Group-A, while the remaining 105 patients were in Group-NA. Among patients receiving IMRT radiotherapy, the incidence of anxiety was 27.3% (18/66), whereas in patients receiving VMAT radiotherapy, the anxiety incidence was 9.5% (6/63), showing a statistically significant difference between the two groups (P=0.010). Similarly, in Group-D, 20 patients were in the Group-AD, and the rest of the 125 patients were in Group-ND. Among those receiving IMRT, the depression incidence was 19.5% (15/77), while for patients undergoing VMAT, the depression incidence was 7.4% (5/68), indicating a significant statistical difference between the two groups (P=0.035).
For patients with T3-4 stage, both anxiety and depression incidence rates showed no statistical difference between the two radiotherapy techniques, in either the anxiety group or the depression group (P=0.128, P=0.903).
Factors Influencing Anxiety and Depression Status
A univariate analysis using the clinical characteristics and radiotherapy techniques from Table 1 for anxiety and depression status showed that, in T1-2 stage NPC patients, the anxiety status was correlated with the radiotherapy technique (r=0.228, P=0.009), while the depression status was correlated with age (r=0.196, P=0.018) and the radiotherapy technique (r=0.176, P=0.035). For classifying post-radiotherapy anxiety and depression status into two categories, the clinical characteristics and radiotherapy techniques from Table 1 were incorporated into a logistic multivariate analysis model. The results showed that, in T1-2 stage NPC patients, the different radiotherapy technique was an independent factor affecting anxiety status (P=0.022), while age and radiotherapy techniques were independent factors affecting depression status (P=0.022 and P=0.049, respectively).
Similarly, in T3-4 stage NPC patients, univariate analysis revealed that the depression status was correlated with gender (r=0.241, P=0.012). In the multivariate analysis, gender was also an independent factor affecting depression status (P=0.013). No factors related to anxiety status were identified.
The results are presented in Table 4.
Discussion
Radiation therapy is widely employed as the primary treatment modality for newly diagnosed NPC patients in clinical practice. However, an increasing body of research has highlighted the potential for therapy-related psychological disorders following radiotherapy, especially in NPC patients, where the incidence of psychological disorders is significantly higher than in other head and neck malignancies.4 Anxiety and depression, being the most common psychological disorders, profoundly impact the quality of life and treatment outcomes for patients.2,5 Hence, understanding the factors influencing psychological status, especially those related to radiotherapy planning, holds significant importance for optimizing treatment strategies and improving patient prognosis.
This study conducted a retrospective analysis of 269 patients with newly diagnosed NPC to explore the impact of IMRT and VMAT radiotherapy techniques, in the absence of hippocampal protection planning, on hippocampal dosimetry and patient psychological status. The study revealed that, for T1-2 stage patients, those treated with IMRT had significantly higher hippocampal doses than those treated with VMAT, and patients receiving IMRT also had significantly higher rates of anxiety and depression. However, in T3-4 stage patients, no significant correlation was observed between radiotherapy technique and the incidence of anxiety or depression. This study analyzed the same patient cohort as a previous publication,15 sharing some tables, methodology, and substantial portions of the paper, but it also includes patients in stage T3-4, focusing on different aspects. Previous research has already demonstrated a correlation between hippocampal radiation and anxiety. However, current guidelines do not designate the hippocampus as an organ at risk in nasopharyngeal carcinoma radiotherapy. Importantly, VMAT and IMRT differ in their delivery of radiation to organs at risk in this context. This study primarily explores scenarios where hippocampal dose is not specifically considered, aiming to assess whether VMAT and IMRT influence the risk of anxiety and depression. As such, we believe this paper holds significant clinical relevance. And for T1-2 stage NPC patients, the choice of an appropriate radiotherapy technique may help mitigate the risk of anxiety and depression.
In modern radiotherapy, IMRT and VMAT techniques are widely used due to their precise dose distribution and organ-sparing effects. The results of this study are consistent with previous research, showing that VMAT is superior to IMRT in hippocampal protection.16,17 Additionally, a previous study has already compared IMRT and VMAT, emphasizing the importance of considering variations in tumor location and patient anatomy, which can lead to different dosimetric outcomes.26 To mitigate the impact of these differences, we stratified the sample into T1-2 and T3-4 stages, thereby reducing the influence of tumor location on radiation dose to some extent. Notably, this study is the first to explore the impact of differential hippocampal dosimetry on psychological status in different radiotherapy plans, and it suggests that in T1-2 stage NPC patients, the dosimetric advantages of VMAT also appear to have a positive impact on patient psychological status. This result offers a new perspective on considering the influence of psychological status when planning treatments.
Furthermore, this study found differences in post-radiotherapy depression status among patients of different ages and genders. In T1-2 stage patients, changes in post-radiotherapy depression status were correlated with age. Prior research has also indicated age as an independent factor influencing NPC radiotherapy patients,3 and our study further revealed that age was an independent factor affecting depression status only in T1-2 stage NPC patients. In T3-4 stage patients, gender played an independent role in the occurrence of depression. Previous research has likewise identified gender as a factor influencing the psychological status of NPC radiotherapy patients,9 and our study further found that gender specifically impacted changes in depression status, with little influence on anxiety status. This result suggests that individual differences such as age and gender may also have associations with the occurrence of psychological disorders, emphasizing the need for clinical attention.
The study also has several limitations. First, it lacks long-term follow-up data to evaluate trends in psychological status and does not explore specific biological mechanisms. Additionally, this study only establishes correlation, not causation, between psychological status changes and radiotherapy techniques. Although our previous study found that higher doses to the hippocampi are likely associated with an increased incidence of anxiety,15 other factors, such as hippocampal sparing leading to higher doses in neighboring brain regions, may also contribute to post-radiation psychological status changes. Furthermore, in our study, we focused on directly comparing anxiety and depression levels between patients treated with VMAT and IMRT, aiming to isolate the effects of the radiotherapy techniques themselves. While we recognize that factors such as education level and treatment-related side effects (eg, dry mouth, sore throat, and hearing loss) can influence psychological states,3 the retrospective nature of this study limited our ability to fully account for these variables. Currently, a prospective study is underway to further investigate these factors.
Conclusions
In summary, this study holds clinical significance for the choice of radiotherapy treatment techniques and the management of psychological status in newly diagnosed NPC patients. In the absence of hippocampal protection, selecting a VMAT treatment plan over IMRT may potentially reduce the incidence of anxiety and depression. These results underscore the importance of considering both physical and psychological factors when tailoring treatment plans. Future research will focus on developing more personalized and effective radiotherapy strategies to further improve the quality of life and long-term prognosis for NPC patients.
Funding
This study was supported by the Leading Project Foundation of Science and Technology, Fujian Province (No.2023Y0017); and CIFST - Abbott Foundation of Food Nutrition and Safety (Grant Number: 2020-12) and Joint Funds for the Innovation of Science and Technology, Fujian Province (Grant Number: 2023Y9109).
Disclosure
The study complies with the Declaration of Helsinki.
The anonymized data from the First Affiliated Hospital of Fujian Medical University is not publicly available.
The authors report no conflicts of interest in this work.
References
1. Djan R, Penington A. A systematic review of questionnaires to measure the impact of appearance on quality of life for head and neck cancer patients. J Plast Reconstr Aesthet Surg. 2013;66(5):647–659. doi:10.1016/j.bjps.2013.01.007
2. McDowell LJ, Rock K, Xu W, et al. Long-term late toxicity, quality of life, and emotional distress in patients with nasopharyngeal carcinoma treated with intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2018;102(2):340–352. doi:10.1016/j.ijrobp.2018.05.060
3. Wang C, Chen J, Su L, et al. The psychological status in patients with nasopharyngeal carcinoma during radiotherapy. Eur Arch Otorhinolaryngol. 2022;279(2):1035–1042. doi:10.1007/s00405-021-06892-5
4. Björklund M, Anneli S, Agneta B. Living with head and neck cancer: a profile of captivity. J Nurs Healthcare Chronic Illness. 2010;2(1):22–31. doi:10.1111/j.1752-9824.2010.01042.x
5. Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ. 2018;2018:361k1415.
6. Lee PW, Kwan TT, Kwong DL, et al. A prospective study of the impact of nasopharyngeal cancer and radiotherapy on the psychosocial condition of Chinese patients. Cancer. 2007;109(7):1344–1354. doi:10.1002/cncr.22539
7. Arnold SD, Forman LM, Brigidi BD, et al. Evaluation and characterization of generalized anxiety and depression in patients with primary brain tumors. Neuro Oncol. 2008;10(2):171–181. doi:10.1215/15228517-2007-057
8. Rooney AG, Carson A, Grant R. Depression in cerebral glioma patients: a systematic review of observational studies. J Natl Cancer Inst. 2011;103(1):61–76. doi:10.1093/jnci/djq458
9. Tibbs MD, Huynh-Le MP, Reyes A, et al. Longitudinal analysis of depression and anxiety symptoms as independent predictors of neurocognitive function in primary brain tumor patients. Int J Radiat Oncol Biol Phys. 2020;108(5):1229–1239. doi:10.1016/j.ijrobp.2020.07.002
10. Pereira Dias G, Hollywood R, Bevilaqua MC, et al. Consequences of cancer treatments on adult hippocampal neurogenesis: implications for cognitive function and depressive symptoms. Neuro Oncol. 2014;16(4):476–492. doi:10.1093/neuonc/not321
11. Snyder JS, Soumier A, Brewer M, Pickel J, Cameron HA. Adult hippocampal neurogenesis buffers stress responses and depressive behaviour. Nature. 2011;476(7361):458–461. doi:10.1038/nature10287
12. Wong-Goodrich SJ, Pfau ML, Flores CT, et al. Voluntary running prevents progressive memory decline and increases adult hippocampal neurogenesis and growth factor expression after whole-brain irradiation. Cancer Res. 2010;70(22):9329–9338. doi:10.1158/0008-5472.CAN-10-1854
13. Raber J, Rola R, LeFevour A, et al. Radiation-induced cognitive impairments are associated with changes in indicators of hippocampal neurogenesis. Radiat Res. 2004;162(1):39–47. doi:10.1667/RR3206
14. Son Y, Yang M, Kim JS, et al. Hippocampal dysfunction during the chronic phase following a single exposure to cranial irradiation. Exp Neurol. 2014;254:134–144. doi:10.1016/j.expneurol.2014.01.018
15. Gai X, Su L, Huang S, et al. Correlation between hippocampal radiation doses and psychological condition for patients with stage T1-2 nasopharyngeal carcinoma. Radiother Oncol. 2023;7(189):109942. doi:10.1016/j.radonc.2023.109942
16. Gu W, Li Q, Xi D, et al. The hippocampus sparing volume modulated arc therapy does not influence plan quality on locally advanced nasopharyngeal carcinoma patients. Sci Rep. 2017;7(1):3443. doi:10.1038/s41598-017-03517-y
17. Soydemir GP, Bilici N, Tiken EE, et al. Hippocampal sparing for brain tumor radiotherapy: a retrospective study comparing intensity-modulated radiotherapy and volumetric-modulated arc therapy. J Cancer Res Ther. 2021;17(1):99–105. doi:10.4103/jcrt.JCRT_32_19
18. Zigmond A-S, Snaith R-P. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
19. CIOMS. International Ethical Guidelines for Health-Related Research Involving Humans. CIOMS; Geneva:2016. Available from: is https://cioms.ch/publications/product/international-ethical-guidelines-for-health-related-research-involving-humans
20. Ghia A, Tomé WA, Thomas S, et al. Distribution of brain metastases in relation to the hippocampus: implications for neurocognitive functional preservation. Int J Radiat Oncol Biol Phys. 2007;68(4):971–977. doi:10.1016/j.ijrobp.2007.02.016
21. Hong JS, Hua YJ, Su L, et al. Modified-nutrition index is a significant prognostic factor for the overall survival of the nasopharyngeal carcinoma patients who undergo intensity-modulated radiotherapy. Nutr Cancer. 2017;69(7):1011–1018. doi:10.1080/01635581.2017.1359311
22. Lee NY, Zhang Q, Pfister DG, et al. Addition of bevacizumab to standard chemoradiation for locoregionally advanced nasopharyngeal carcinoma (RTOG 0615): a Phase 2 multi-institutional trial. Lancet Oncol. 2012;13(2):172–180. doi:10.1016/S1470-2045(11)70303-5
23. Chen A, Lee N, Yang C, et al. Comparison of intensity-modulated radiotherapy using helical tomotherapy and segmental multileaf collimator-based techniques for nasopharyngeal carcinoma: dosimetric analysis incorporating quality assurance guidelines from RTOG 0225. Technol Cancer Res Treat. 2010;9(3):291–298. doi:10.1177/153303461000900308
24. Edge SB, Compton CC. The American joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
25. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
26. Nguyen K, Cummings D, Lanza VC, et al. A dosimetric comparative study: volumetric modulated arc therapy vs intensity-modulated radiation therapy in the treatment of nasal cavity carcinomas. Med Dosim. 2013;38(3):225–232. doi:10.1016/j.meddos.2013.01.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.