")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Impact of Relaxation and Music Intervention on Psychological and Gastrointestinal Health in Military Recruits: A Prospective Study
Authors Liu J, Liu T, Lu H, Zhao X, Ma S, Song F, Qiao N, Cheng W, Qi X
Received 30 November 2024
Accepted for publication 13 April 2025
Published 2 May 2025 Volume 2025:21 Pages 593—608
DOI https://doi.org/10.2147/TCRM.S509551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Jun Liu,1– 3,* Tingwei Liu,3,4,* Haoxu Lu,2,* Xinyuan Zhao,3,5,* Shanshan Ma,2 Fudan Song,2 Nanhai Qiao,2 Wanshu Cheng,3 Xingshun Qi3
1School of Economics and Management, Beihang University, Beijing, People’s Republic of China; 2Military Joint Teaching and Research Office, the 32684th Troop of Chinese PLA, Shenyang, People’s Republic of China; 3Military Medical Research Group, Department of Gastroenterology, General Hospital of Northern Theater Command, Shenyang, People’s Republic of China; 4Department of Gastroenterology, Liaoning Electric Center Hospital, Shenyang, People’s Republic of China; 5Section of Medical Service, General Hospital of Northern Theater Command, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingshun Qi, Military Medical Research Group, Department of Gastroenterology, General Hospital of Northern Theater Command, No. 83 Wenhua Road, Shenyang, 110840, Liaoning Province, People’s Republic of China, Tel +86-24-28897600, Fax +86-24-28851113, Email [email protected]
Background and aims: Gastrointestinal symptoms are closely associated with psychological problems, such as anxiety and depression. This prospective before-after study aimed to explore whether progressive muscular relaxation training combined with music intervention, which is potentially beneficial for psychological conditions, can improve gastrointestinal symptoms.
Methods: A total of 623 recruits’ effective questionnaires before and after intervention were collected. They underwent progressive muscular relaxation training combined with music intervention for 4 weeks. They also completed the Self-Rating Depression Scale (SDS) and the Patient Health Questionnaire (PHQ-9) for assessment of depression, the Self-Rating Anxiety Scale (SAS) and the Generalized Anxiety Disorder-7 (GAD-7) for assessment of anxiety, the Gastrointestinal Symptom Rating Scale (GSRS) for assessment of gastrointestinal symptoms, and the Bristol Stool Form Scale (BSFS) for assessment of stool before and after interventions. Changes of psychological conditions and gastrointestinal symptoms were evaluated.
Results: The SDS (P< 0.001), PHQ-9 (P< 0.001), SAS (P< 0.001), GAD-7 (P< 0.001), and GSRS (P< 0.001) scores were significantly decreased after intervention. The proportions of regurgitation (P< 0.001), abdominal pain (P< 0.001), dyspepsia (P< 0.001), and constipation (P< 0.001) evaluated by the GSRS were significantly decreased after intervention, but not diarrhea (P=0.601). The proportions of severe (P< 0.001) and mild (P< 0.001) constipation evaluated by the BSFS decreased after intervention, but those of severe (P=0.632) and mild (P< 0.001) diarrhea evaluated by the BSFS increased.
Conclusion: Short-term progressive muscular relaxation training in combination with music intervention is potentially effective for most gastrointestinal symptoms, but not for diarrhea, in recruits.
Keywords: gastrointestinal symptom, psychology, anxiety, depression, music intervention, progressive muscular relaxation training, intervention
Introduction
Gastrointestinal symptoms, primarily abdominal pain, regurgitation, dyspepsia, diarrhea, and constipation,1,2 are common, with a prevalence of 61% (45,498/71,812) in the US general population.3 They negatively influence the quality of life and productivity and indicate the probability of functional or organic gastrointestinal diseases.4,5 It has been shown that gastrointestinal symptoms are closely associated with psychological problems, such as anxiety and depression.6–8 This association can be explained by the action of the brain-gut axis that an individual’s feelings can influence his or her gastrointestinal function, and vice versa. In addition, the gut microbiota, called the human second brain, plays a critical role in the regulation of the central nervous system.9,10 Thus, the correction of psychological problems should be clinically effective in improving gastrointestinal symptoms.
Military personnel is a special population that needs to complete high-intensity training every day and takes responsibility for war preparedness.11 Owing to high-stress conditions, they are more likely to develop various psychological and physical diseases.12,13 Recently, our group has demonstrated a significantly higher prevalence of Helicobacter pylori infection, which is closely associated with functional (ie, irritable bowel syndrome)14 and organic gastrointestinal diseases (ie, peptic ulcer and gastric cancer),15 in the military population aged 17–25 years than in the civilian population of the same age (35.6% versus 25.9%, P=0.001).16 We also found a higher score on the Symptom Checklist 90, a traditional tool for the evaluation of psychological conditions, in recruits with gastrointestinal symptoms than those without.6 Therefore, it is reasonable to infer that psychological interventions may be beneficial for the prevention of gastrointestinal symptoms. Notably, considering the peculiarity of recruits in terms of their living environment and work burden, it is necessary to develop easy-to-use approaches to adjust their psychological conditions in recruits and further improve their gastrointestinal symptoms. Apart from their advantages in reducing anxiety and stress and promoting quality of life,17–22 progressive muscular relaxation training and music therapy are very convenient to implement in real-world scenarios, because only a broadcast is required without any psychiatrist. However, until now, it remains unclear about whether progressive muscular relaxation training and music therapy can be employed for preventing from gastrointestinal symptoms in military recruits. Thus, this prospective study was conducted to address this issue.
Methods
Study Design
The protocol for this prospective before-after study was approved by the Medical Ethics Committee of the General Hospital of the Northern Theater Command. The ethical approval number is Y (2022) 162. All subjects signed their written informed consents before starting the study. This study was conducted in accordance with the principles of the Declaration of Helsinki.
We screened all new recruits who joined a troop in September 2022 for eligibility. The exclusion criteria were as follows: 1) definite diagnosis of organic disorders in the gastrointestinal system; 2) missing variables in the questionnaires; 3) suspected accuracy of questionnaires; and 4) refusal of written informed consent.
Data Collection
We collected data including age, sex, history of alcohol consumption, smoking, non-steroidal anti-inflammatory drugs, Helicobacter pylori infection, family history of gastrointestinal diseases, and questionnaires related to gastrointestinal symptoms and psychological status.
Questionnaires
We employed two scales, the Self-Rating Depression Scale (SDS)23 and the Patient Health Questionnaire (PHQ-9),24 to measure the presence and grade of depression. The SDS includes 20 items, each of which is evaluated using the Likert 4-piont scale approach, including 1 point as symptoms never or rarely develop and 4 points as symptoms always or persistently develop. The total crude score was calculated as the sum of the scores for the 20 items. The standard total score was equal to the crude total score multiplied by 1.25. A standard total score of 53–62 points is defined as mild depression, 63–72 points as moderate depression, and ≥73 points as severe depression. The PHQ-9 includes 9 items, each of which is also evaluated using the Likert 4-piont scale approach, including 0 point as symptoms never or rarely develop and 3 points as symptoms develop almost every day. The total score was calculated as the sum of the scores for the 9 items. A total score of 0–4 points is defined as no depression, 5–9 points as mild depression, 10–14 points as moderate depression, 15–19 points as severe depression, and 20–27 points as very severe depression.
We employed two scales, the Self-Rating Anxiety Scale (SAS)25 and the Generalized Anxiety Disorder-7 (GAD-7),26 to measure the presence and grade of anxiety. The SAS includes 20 items, each of which is assessed using the Likert 4-piont scale approach, including 1 point as symptoms never or rarely develop, and 4 points as symptoms always or persistently develop. The total crude score was calculated as the sum of the scores for the 20 items. The standard total score was equal to the crude total score multiplied by 1.25. A standard total score of 50–59 points is defined as mild anxiety, 60–69 points as moderate anxiety, and ≥70 points as severe anxiety. The GAD-7 includes 7 items, each of which is also assessed using the Likert 4-piont scale approach, including 0 point as symptoms never or rarely develop and 3 points as symptoms develop almost every day. The total score was calculated as the sum of the scores for the 7 items. A total score of 0–4 points is defined as no anxiety, 5–9 points as mild anxiety, 10–14 points as moderate anxiety, and 15–21 points as severe anxiety.
We used the Gastrointestinal Symptom Rating Scale (GSRS) to assess 5 types of gastrointestinal symptoms and their severity.27 The GSRS includes 3 items related to abdominal pain, 2 items related to regurgitation, 4 items related to dyspepsia, 3 items related to diarrhea, and 3 items related to constipation. The severity of each gastrointestinal symptom was evaluated using the Likert 4-piont scale approach, with 0 point as asymptomatic and 3 points as the most severe. We also employed the Bristol Stool Form Scale (BSFS) to visualize 7 types of stools by illustrating schematic graphs and descriptions of the stool.28 Specifically, types 1 and 2 refer to constipation, types 3 and 4 refer to normal stools, and types 5–7 refer to diarrhea.
Five researchers (Jun Liu, Haoxu Lu, Shanshan Ma, Fudan Song, and Nanhai Qiao) have worked in the same troop for a long time and fruitful experiences in training new recruits. In the current study, they were responsible for distributing and retrieving Chinese version questionnaires to the participants. Additionally, if a participant did not understand the contents of questionnaires, they would make detailed explanations to maximize the accuracy of responses to each questionnaire. Before intervention, these questionnaires were answered on October 14, 2022. After intervention, they were answered again on November 20, 2022.
Psychological Interventions
We conducted two types of psychological intervention, progressive muscular relaxation training and music intervention, every day. It lasted for 4 weeks from October 15, 2022 to November 11, 2002.
Progressive muscle relaxation training is a type of behavioral therapy29 in which muscles of the whole body are gradually tightened and relaxed to reduce stress and physical symptoms. It is performed before sleep at night every day and lasts for 15 minutes each time. During the period of progressive muscle relaxation training, all recruits were placed in a flat-lying position and trained in accordance with the instructions of the broadcasts.
Music therapy is a type of psychotherapy30 in which meditation music is played often. It is performed before lunch breaks every day and lasts for 15 minutes each time. When music at 30–45 decibels is played, all recruits should be placed in a flat-lying position and asked to adjust the frequency of breathing and keep them relaxed. Light music, such as Annie’s Wonderland by Bandari, was utilized in this study.
Before the study, our researchers taught all enrolled participants about how to conduct the two psychological interventions. They were also responsible for monitoring whether the two psychological interventions had been conducted. However, it should be acknowledged that no board-certified music therapist had participated in the music intervention.
Sample Size Calculation
We had not estimated the sample size before initiating this study yet. This is primarily because it is a single-arm study without any control group. Additionally, all participants were from the same troop, and thus the number of participants was fixed.
Statistical Analyses
The SPSS statistical package software was used to perform all statistical analyses. Descriptive data are expressed as mean ± standard deviation and median (range) or frequency (percentage). Paired t-tests and chi-square tests were used to compare continuous and categorical variables before and after the psychological interventions. Differences were considered statistically significant at a two-sided P-value of <0.05.
Results
Participants
In total, 623 participants’ questionnaires were included in the final analysis (Table 1). Only 15 participants had a definite history of digestive diseases.
 |
Table 1 Characteristics of Participants |
Depression by SDS
The SDS scores decreased significantly after the intervention (Table 2). The proportions of mild, moderate, and severe depression evaluated by the SDS also decreased after the intervention, but the differences in the proportions of mild and moderate depression evaluated by the SDS before and after the intervention were not statistically significant.
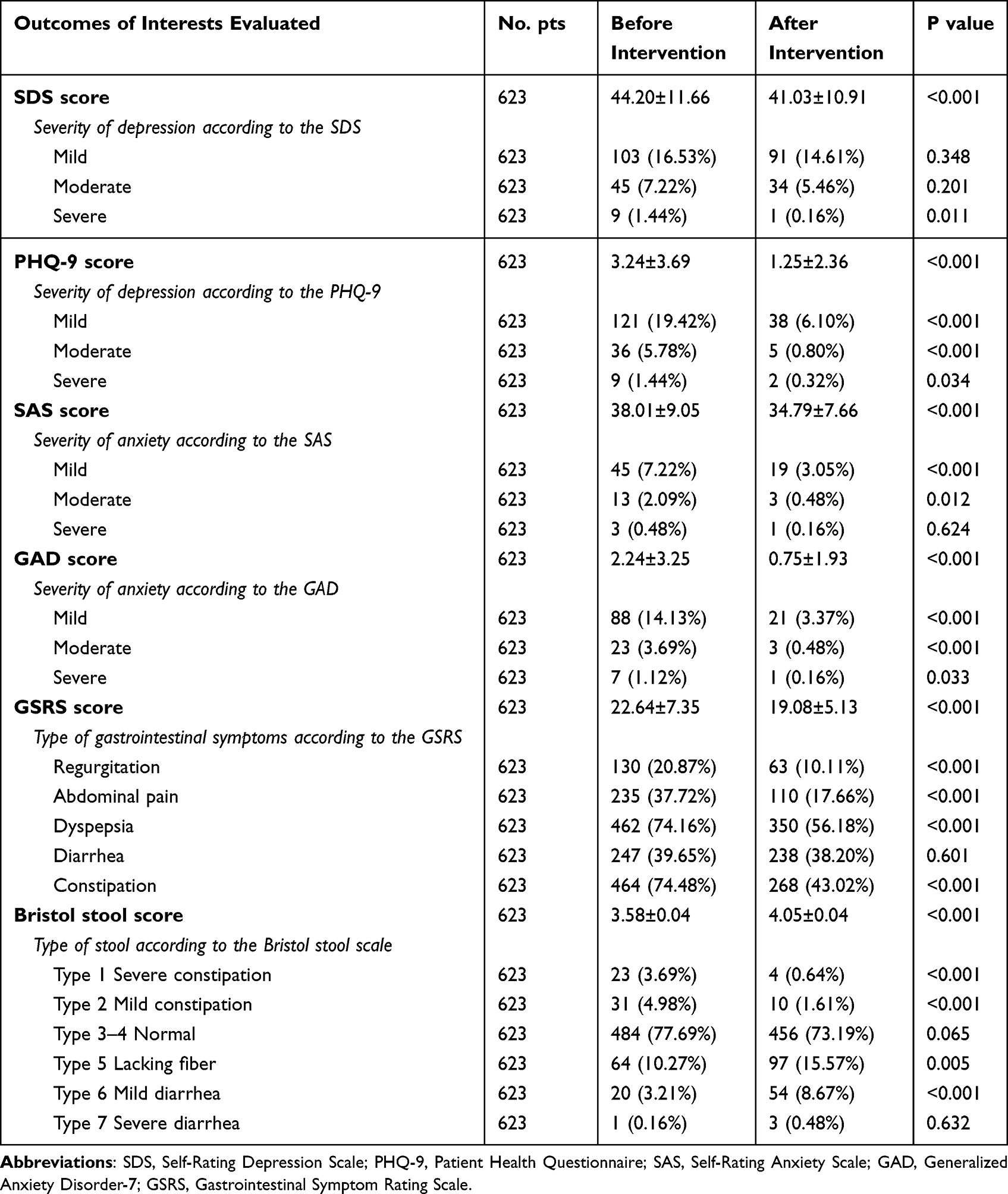 |
Table 2 Differences in Outcomes of Interests Evaluated Before and After Intervention |
In 12.23% (57/466) of the participants without depression evaluated by the SDS before the intervention, depression developed after the intervention, which was mild (n=42), moderate (n=14), and severe (n=1) (Table 3). In 56.05% (88/157) of the participants with depression evaluated using the SDS before the intervention, depression disappeared after the intervention. In 58.25% (60/103) of the participants with mild depression evaluated using the SDS before the intervention, depression disappeared after the intervention. In 80% (36/45) of the participants with moderate depression evaluated by SDS before the intervention, depression improved (n=11) or disappeared (n=25) after the intervention. In all of the 9 participants with severe depression evaluated by SDS before the intervention, depression improved (n=6) or disappeared (n=3) after the intervention.
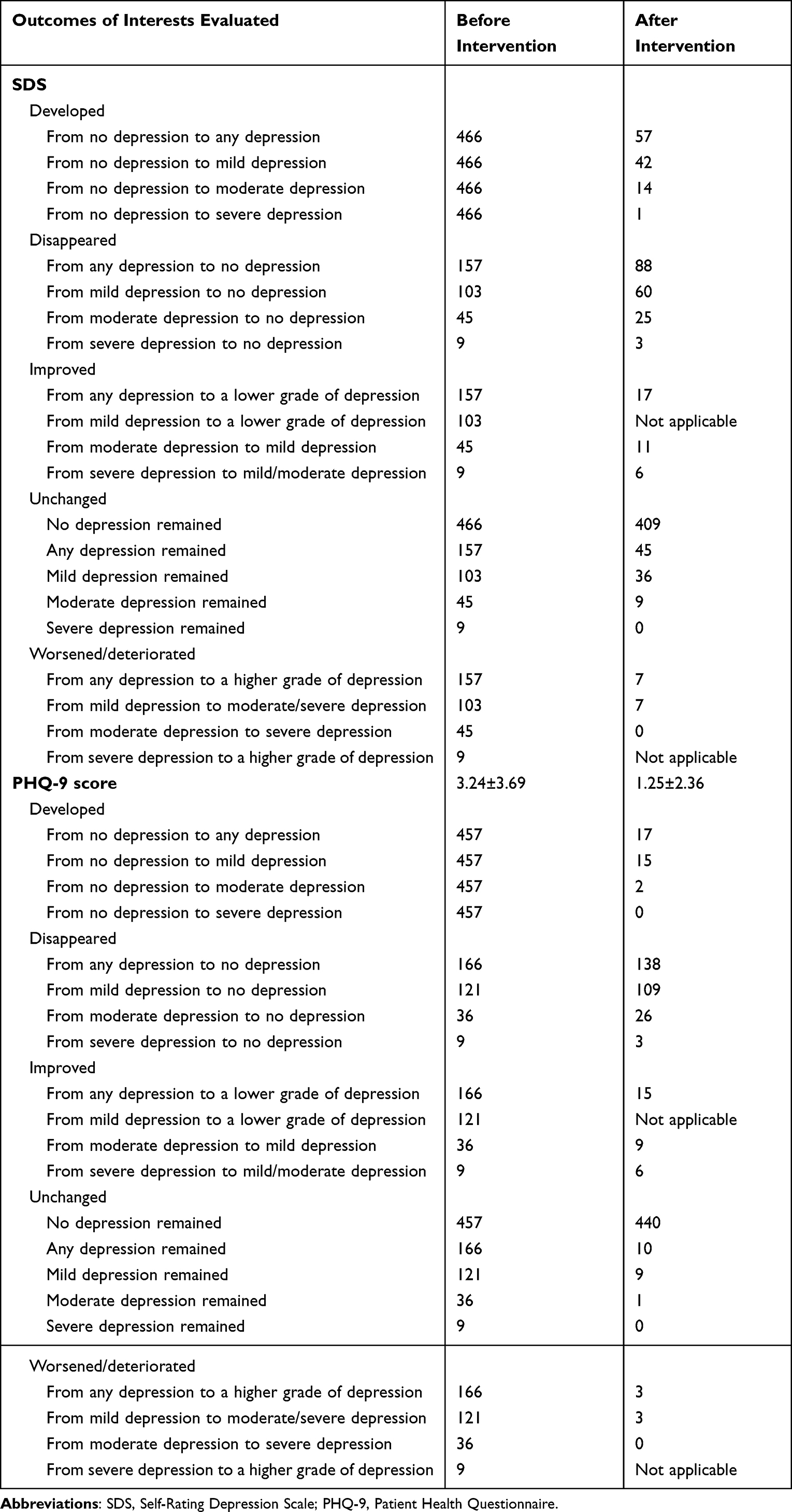 |
Table 3 Changes in Depression by SDS and PHQ-9 |
Depression by PHQ-9
The PHQ-9 score significantly decreased after the intervention (3.24±3.69 versus 1.25±2.36, P<0.001) (Table 2). The proportion of mild, moderate, and severe depression, evaluated using the PHQ-9 scale, also decreased after the intervention.
In 138 of the 166 participants with depression evaluated using the PHQ-9 before the intervention, depression disappeared after the intervention (Table 3). In 109 of the 121 participants with mild depression evaluated using the PHQ-9 before the intervention, depression disappeared after the intervention. In 35 of the 36 participants with moderate depression evaluated by the PHQ-9 before the intervention, depression improved (n=9) or disappeared (n=26) after the intervention. In all of the 9 participants with severe depression evaluated by the PHQ-9 before intervention, depression improved (n=6) or disappeared (n=3) after the intervention. In 17 of the 457 participants without depression evaluated by the PHQ-9 before the intervention, depression developed after the intervention, which was mild (n=15) and moderate (n=2).
Anxiety by SAS
The SAS score significantly decreased after the intervention (38.01±9.05 versus 34.79±7.66, P<0.001) (Table 2). The proportions of mild, moderate, and severe anxiety evaluated using the SAS also decreased after the intervention.
In 51 of the 61 participants with anxiety evaluated using the SAS before the intervention, anxiety disappeared after the intervention (Table 4). In 40 of the 45 participants with mild anxiety evaluated using the SAS before the intervention, anxiety disappeared after the intervention. In all of the 13 participants with moderate anxiety evaluated by the SAS before the intervention, anxiety improved (n=4) or disappeared (n=9) after the intervention. In all of the 3 participants with severe anxiety evaluated by the SAS before the intervention, anxiety improved (n=1) or disappeared (n=2) after the intervention. In 13 of the 562 participants without anxiety evaluated by the SAS before the intervention, anxiety developed after the intervention, which was mild (n=10), moderate (n=2), and severe (n=1).
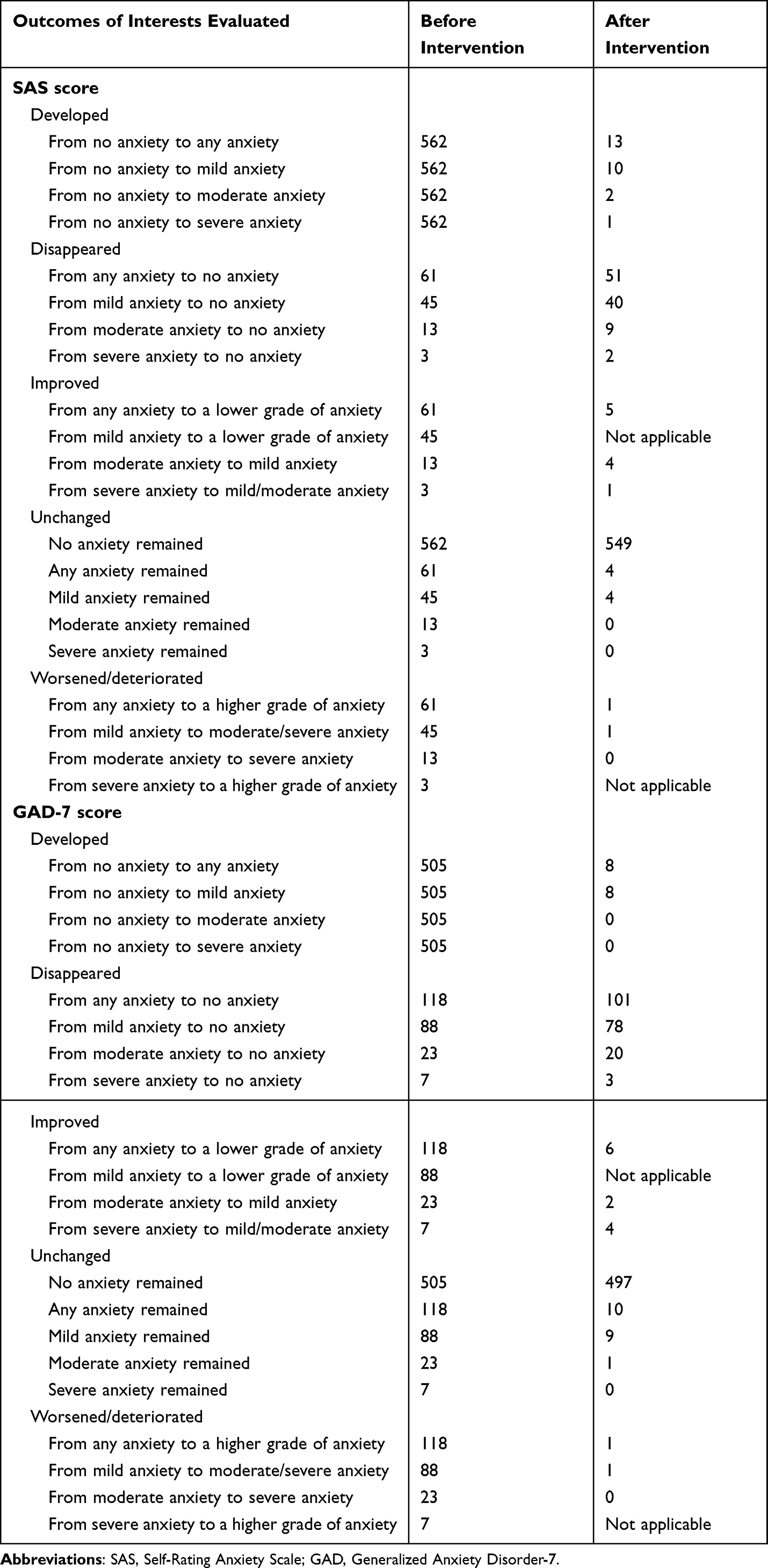 |
Table 4 Changes in Anxiety by SAS and GAD |
Anxiety by GAD-7
The GAD-7 score was significantly decreased after intervention (2.24±3.25 versus 0.75±1.93, P<0.001) (Table 2). The proportions of mild, moderate, and severe anxiety evaluated using the GAD-7 scale also decreased after the intervention.
In 101 of the 118 participants with anxiety evaluated by the GAD-7 before the intervention, anxiety disappeared after the intervention (Table 4). In 78 of the 88 participants with mild anxiety evaluated by the GAD-7 before the intervention, anxiety disappeared after the intervention. In 22 of the 23 participants with moderate anxiety evaluated by GAD-7 before the intervention, anxiety improved (n=2) or disappeared (n=20) after the intervention. In all of the 7 participants with severe anxiety evaluated by the GAD-7 before the intervention, anxiety improved (n=4) or disappeared (n=3) after the intervention. In 8 of the 505 participants without anxiety evaluated by GAD-7 before the intervention, anxiety developed after the intervention, which was mild (n=8).
Gastrointestinal Symptoms by GSRS
The GSRS score significantly decreased after the intervention (22.64±7.35 versus 19.08±5.13, P<0.001) (Table 2). The proportions of regurgitation (20.87% versus 10.11%, P<0.001), abdominal pain (37.72% versus 17.66%, P<0.001), dyspepsia (74.16% versus 56.18%, P<0.001), and constipation (74.48% versus 43.02%, P<0.001) evaluated by GSRS scale were also significantly decreased after the intervention, but the decrease in the proportion of diarrhea after the intervention (39.65% versus 38.20%, P=0.601) was not statistically significant.
Regurgitation
In 98 of the 130 participants with regurgitation evaluated by GSRS before the intervention, regurgitation disappeared after the intervention (Table 5). In 96 of the 127 participants with mild regurgitation evaluated using GSRS before the intervention, regurgitation disappeared after the intervention. In all of the 3 participants with moderate regurgitation evaluated by GSRS before the intervention, regurgitation improved (n=1) or disappeared (n=2) after the intervention. None of the participants had or developed severe regurgitation before or after intervention, respectively. In 31 of the 493 participants without regurgitation evaluated by GSRS before the intervention, regurgitation developed after the intervention, which was mild (n=31).
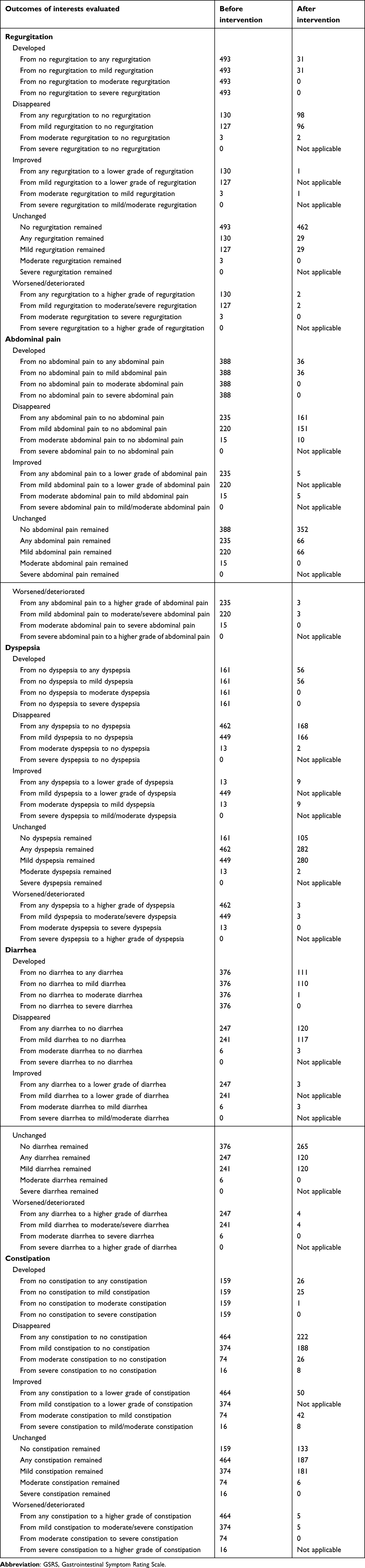 |
Table 5 Changes in Gastrointestinal Symptoms by GSRS |
Abdominal Pain
In 161 of the 235 participants with abdominal pain evaluated by the GSRS before the intervention, abdominal pain disappeared after the intervention (Table 5). In 151 of the 220 participants with mild abdominal pain evaluated by the GSRS before the intervention, abdominal pain disappeared after the intervention. In all of the 15 participants with moderate abdominal pain evaluated by the GSRS before the intervention, abdominal pain improved (n=5) or disappeared (n=10) after the intervention. None of the participants had or developed severe abdominal pain before or after the intervention, respectively. In 36 of the 388 participants without abdominal pain evaluated by GSRS before the intervention, abdominal pain developed after the intervention, which was mild (n=36).
Dyspepsia
In 168 of the 462 participants with dyspepsia evaluated by GSRS before the intervention, dyspepsia disappeared after the intervention (Table 5). In 166 of the 449 participants with mild dyspepsia evaluated by GSRS before the intervention, dyspepsia disappeared after the intervention. In 11 of the 13 participants with moderate dyspepsia evaluated by GSRS before the intervention, dyspepsia improved (n=9) or disappeared (n=2) after the intervention. None of the participants had or developed severe dyspepsia before or after intervention, respectively. In 56 of the 161 participants without dyspepsia evaluated by the GSRS before the intervention, dyspepsia developed after the intervention, which was mild (n=56).
Diarrhea
In 120 of the 247 participants with diarrhea evaluated by the GSRS before the intervention, diarrhea disappeared after the intervention (Table 5). In 117 of 241 participants with mild diarrhea evaluated using the GSRS before the intervention, diarrhea disappeared after the intervention. In all of the 6 participants with moderate diarrhea evaluated by the GSRS before the intervention, diarrhea improved (n=3) or disappeared (n=3) after the intervention. None of the participants had or developed severe diarrhea before or after the intervention, respectively. In 111 of the 376 participants without diarrhea evaluated by the GSRS before the intervention, diarrhea developed after the intervention, which was mild (n=110) and moderate (n=1).
Constipation
In 222 of the 464 participants with constipation evaluated by the GSRS before the intervention, constipation disappeared after the intervention (Table 5). In 188 of the 374 participants with mild constipation evaluated using the GSRS before the intervention, constipation disappeared after the intervention. In 68 of the 74 participants with moderate constipation evaluated by the GSRS before the intervention, constipation improved (n=42) or disappeared (n=26) after the intervention. In all of the 16 participants with severe constipation evaluated by the GSRS before the intervention, constipation improved (n=8) or disappeared (n=8) after the intervention. In 26 of the 159 participants without constipation evaluated by the GSRS before the intervention, constipation developed after the intervention, which was mild (n=25) and moderate (n=1).
Stool by Bristol Score
The proportions of severe (3.69% versus 0.64%, P<0.001) and mild (4.98% versus 1.61%, P<0.001) constipation decreased after the intervention, but those with severe (0.16% versus 0.48%, P=0.632) and mild (3.21% versus 8.67%, P<0.001) diarrhea increased after the intervention (Table 2).
In 23 participants with severe constipation evaluated by the Bristol score before the intervention, the type of stool was normalized (n=18) and changed to diarrhea (n=4) after the intervention (Table 6). In 31 participants with mild constipation evaluated by the Bristol score before the intervention, the type of stool was normalized (n=22) and changed to diarrhea (n=6) after the intervention. In one participant with severe diarrhea evaluated using the Bristol score before intervention, the type of stool remained (n=1) after the intervention. In 20 participants with mild diarrhea evaluated by the Bristol score before the intervention, the type of stool was normalized (n=6) and remained (n=14) after the intervention.
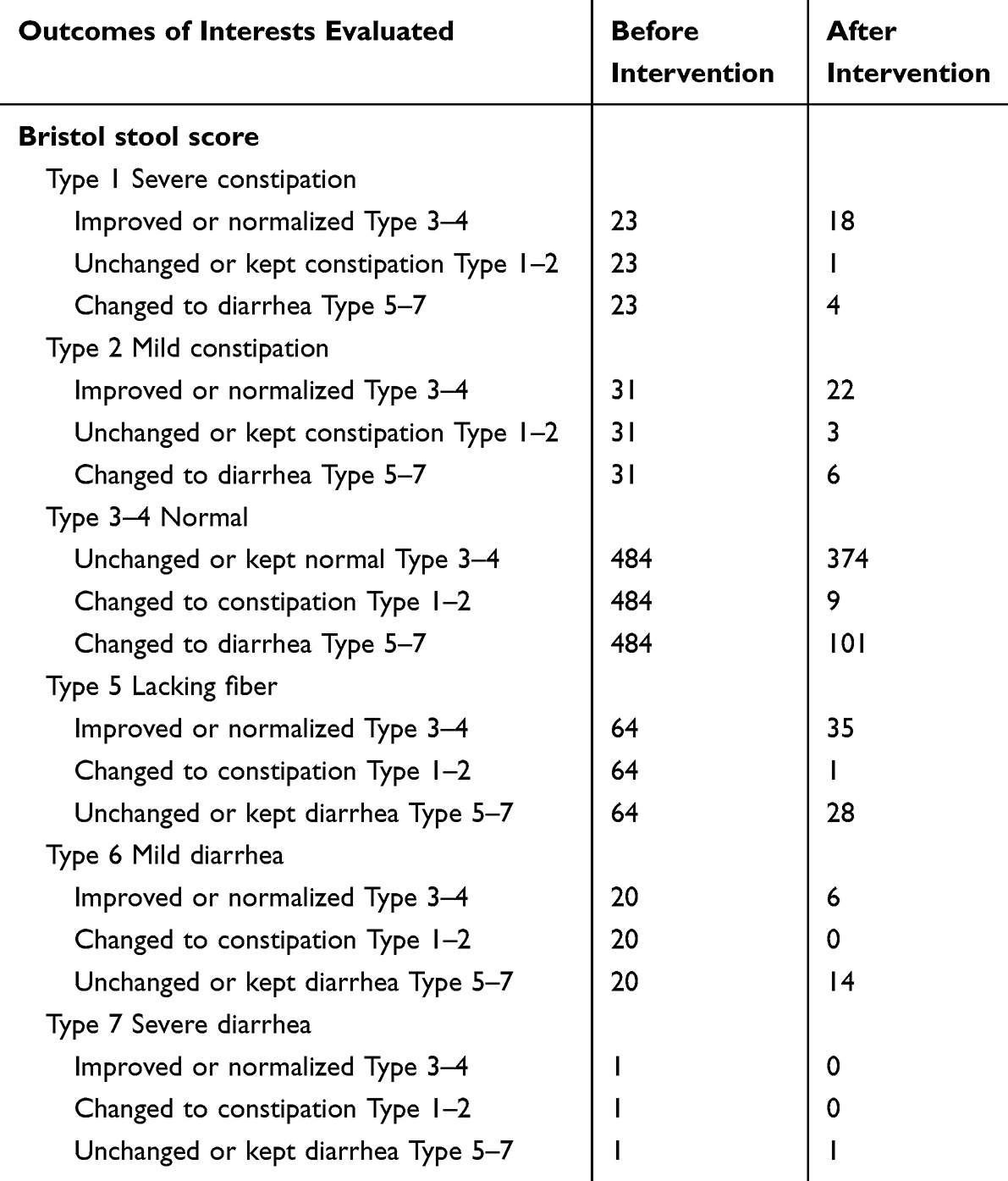 |
Table 6 Changes in Type of Stool by Bristol Stool Scale |
Discussion
Our study demonstrated a reduction in depression and anxiety after progressive muscle relaxation training combined with music intervention. Indeed, the benefits of music therapy in various clinical scenarios have been widely recognized.31–37 Similarly, numerous studies have comprehensively evaluated the effects of progressive muscular relaxation training on anxiety, depression, quality of life, quality of sleep, and other outcomes in diverse populations, including basketball athletes,38 nursing students,39,40 psychiatric patients,41,42 COVID-19 patients,43,44 patients with pulmonary resection,45 individuals with posttraumatic stress disorder,46 patients with endometriosis,18 patients who underwent coronary artery bypass graft surgery,17 and older people47 (Supplementary Table 1). However, to the best of our knowledge, the impact of their combination has never been explored in recruits, who are at high risk of developing psychological problems, yet.
Based on the currently available evidence, it seems that progressive muscular relaxation training and music intervention are beneficial for the improvement of anxiety and depression. However, the effects of progressive muscular relaxation on sleep quality remain controversial. Ziv et al compared the effects of progressive muscular relaxation and music therapy on insomnia in 15 older adults, and found that music therapy was superior to progressive muscular relaxation in sleep efficiency.47 More notably, progressive muscular relaxation may deteriorate sleep quality. Similarly, in another study by Blanaru et al including 13 individuals with posttraumatic stress disorders, music relaxation not only improved objective and subjective sleep efficiency, but also reduced depression; however, muscular relaxation was not beneficial for sleep efficiency.46 For comparison, our study was designed in which progressive muscular relaxation was performed at night. In this setting, progressive muscular relaxation might compromise the sleep quality of recruits, which is potentially harmful to gastrointestinal symptoms. Therefore, the limitations of our study design should be acknowledged. Future studies should adjust the time at which progressive muscular relaxation is performed to noon.
A major finding of our study was the decrease in the proportion of four gastrointestinal symptoms (regurgitation, abdominal pain, dyspepsia, and constipation), but not diarrhea, after the two psychological interventions. This clinical benefit in terms of gastrointestinal symptoms should be partially attributed to improvements in psychological status. First, studies by our group and others suggest an obvious interaction between psychological problems and gastrointestinal symptoms, primarily due to the brain-gut axis.6,48 Second, previous studies also indicate that various therapies, including music therapy, can improve the symptoms associated with irritable bowel syndrome, reduce the pain and anxiety, and increase the satisfaction during colonoscopy,49,50 and decrease the nausea and vomiting after chemotherapy.51,52 However, the lack of an effect on diarrhea warrants further investigation. Based on the GSRS results, 120 of the 247 participants with diarrhea before intervention did not have diarrhea after intervention, and 111 of the 238 participants with diarrhea after intervention did not have diarrhea before intervention, suggesting only a limited overlap between the two groups of participants with diarrhea before and after intervention. Similarly, based on the results of the Bristol stool scale, 10 participants with constipation and 101 with normal stool developed diarrhea. Taken together, the two interventions should be efficacious for the improvement of diarrhea to some extent, but cannot prevent its de novo occurrence. However, regardless of GSRS or Bristol stool scale, de novo diarrhea should be common in our recruits. Further studies are warranted to explore the pathogenesis of this clinical symptom, including psychological, environmental, dietary, and regional factors, and to establish novel approaches for screening, prevention, and treatment.
The absence of a control group without psychological intervention was a major limitation of our study. In the setting of a single-arm design, investigators can only compare anxiety, depression, and gastrointestinal symptoms before and after intervention, but do not adjust the effects of other factors on them. An ongoing randomized controlled trial by our group will address this issue.
Recruit adherence to the two relaxation techniques during the study period was another limitation of our study. We sent out broadcasts on time and reminded all participants to complete the progressive muscular relaxation training and music intervention. Considering that their daily schedules of training and resting were fixed, their objective adherence should be good. However, the possibility of poor subjective adherence cannot be ignored. Owing to the large number of participants included in our study, it was very difficult to monitor the participants’ completeness of these interventions in a one-to-one manner.
The third limitation should be that organic gastrointestinal diseases, for which psychological interventions might be hardly effective, were not sufficiently excluded from our study. However, it should be acknowledged that imaging and endoscopy, which are often required for a diagnosis of organic gastrointestinal diseases, are unavailable or neglected in most of cases. Regardless, we recommend that further diagnostic approaches should be performed if participants have persistent gastrointestinal symptoms.
Besides, according to the World Federation of Music Therapy or the American Music Therapy Association, music therapy should be administered by a board-certified or trained music therapist to accomplish individualized goals. However, no credentialed professional researcher has participated in completing music interventions in the current study.
The last limitation is that the participants’ responses may be biased. They should have recognized the purpose of our study, and thus may be inclined to answer with an improvement of psychological conditions and gastrointestinal symptoms. Additionally, considering that this study was led by military officers, it is more likely that the recruits gave positive responses after intervention. However, we have acknowledged that the participants’ responses should be honest and unbiased. Indeed, based on our daily observations, military recruits hardly denied the presence of their true discomfort.
In conclusion, a combination of progressive muscular relaxation training with music intervention should be considered in recruits to improve anxiety and depression and manage regurgitation, abdominal pain, dyspepsia, and constipation, but not diarrhea. These findings suggest the potential benefits of psychological intervention in the recruits. Thus, they may be incorporated into the routine subjects of recruits’ training. Certainly, in the future, these findings should be validated in well-designed, randomized controlled trials where no additional intervention should be designed in a control group. Additionally, the management of diarrhea in this population is an important issue that deserves further exploration.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author, XQ, upon reasonable request.
Acknowledgments
Jun Liu, Tingwei Liu, Haoxu Lu, and Xinyuan Zhao are co-first authors for this study.
Funding
This study was partially supported by grants from the “Three Elites and One Team” sponsorship program of the Joint Logistic Support Force of the Chinese People’s Liberation Army and the Independent Research Funding of General Hospital of Northern Theater Command (ZZKY2024018).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vivier H, Ross EJ, Cassisi JE. Classification of gastrointestinal symptom patterns in young adults. BMC Gastroenterol. 2020;20(1):326. doi:10.1186/s12876-020-01478-7
2. Black CJ, Drossman DA, Talley NJ, Ruddy J, Ford AC. Functional gastrointestinal disorders: advances in understanding and management. Lancet. 2020;396(10263):1664–1674. doi:10.1016/S0140-6736(20)32115-2
3. Almario CV, Ballal ML, Chey WD, Nordstrom C, Khanna D, Spiegel BMR. Burden of Gastrointestinal Symptoms in the United States: results of a Nationally Representative Survey of Over 71,000 Americans. Am J Gastroenterol. 2018;113(11):1701–1710. doi:10.1038/s41395-018-0256-8
4. Oustamanolakis P, Tack J. Dyspepsia: organic versus functional. J Clin Gastroenterol. 2012;46(3):175–190. doi:10.1097/MCG.0b013e318241b335
5. Aziz I, Simrén M. The overlap between irritable bowel syndrome and organic gastrointestinal diseases. Lancet Gastroenterol Hepatol. 2021;6(2):139–148. doi:10.1016/S2468-1253(20)30212-0
6. Liu T, Liu J, Wang C, et al. Prevalence of gastrointestinal symptoms and their association with psychological problems in youths. Ann Palliat Med. 2023;12(2):311–323. doi:10.21037/apm-22-1316
7. Ballou S, Katon J, Singh P, et al. Chronic diarrhea and constipation are more common in depressed individuals. Clin Gastroenterol Hepatol. 2019;17(13):2696–2703. doi:10.1016/j.cgh.2019.03.046
8. Aggarwal Dutta R, Ely SL, Cunningham NR. The utility of an anxiety screening measure in youth with functional abdominal pain disorders and clinical characteristics associated with presence of anxiety. Clin J Pain. 2021;37(8):616–622. doi:10.1097/AJP.0000000000000952
9. Ross EJ, Cassisi JE, Joseph D, Dunn ME, Jex S. Cross-lagged analyses between gastrointestinal symptoms, psychological distress, and disability in emerging adults. Appl Psychol Health Well Being. 2022;14(3):920–936. doi:10.1111/aphw.12358
10. Peppas S, Pansieri C, Piovani D, et al. The brain-gut axis: psychological functioning and inflammatory bowel diseases. J Clin Med. 2021;10(3):377. doi:10.3390/jcm10030377
11. Inoue C, Shawler E, Jordan CH, Moore MJ, Jackson CA. Veteran and Military Mental Health Issues. Treasure Island (FL) ineligible companies: StatPearls; 2023.
12. Jia K, An L, Wang F, et al. Aggravation of Helicobacter pylori stomach infections in stressed military recruits. J Int Med Res. 2016;44(2):367–376. doi:10.1177/0300060515593768
13. Wang C, Liu J, An Y, et al. Prevalence and risk factors of Helicobacter pylori infection in military personnel: a systematic review and meta-analysis. Indian J Pathol Microbiol. 2022;65(1):23–28. doi:10.4103/IJPM.IJPM_1084_20
14. Wang C, Yin Y, Wang L, Guo X, Liu L, Qi X. Association between Helicobacter pylori infection and irritable bowel syndrome: a systematic review and meta-analysis. Postgrad Med J. 2023;99(1169):166–175. doi:10.1136/postgradmedj-2021-141127
15. Li Y, Choi H, Leung K, Jiang F, Graham DY, Leung WK. Global prevalence of Helicobacter pylori infection between 1980 and 2022: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(6):553–564. doi:10.1016/S2468-1253(23)00070-5
16. Wang C, Liu J, Shi X, et al. Prevalence of helicobacter pylori infection in military personnel from Northeast China: a cross-sectional study. Int J Gen Med. 2021;14:1499–1505. doi:10.2147/IJGM.S308572
17. Dehdari T, Heidarnia A, Ramezankhani A, Sadeghian S, Ghofranipour F. Effects of progressive muscular relaxation training on quality of life in anxious patients after coronary artery bypass graft surgery. Indian J Med Res. 2009;129(5):603–608.
18. Zhao L, Wu H, Zhou X, Wang Q, Zhu W, Chen J. Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol. 2012;162(2):211–215. doi:10.1016/j.ejogrb.2012.02.029
19. Hassanpour-Dehkordi A, Jalali A. Effect of progressive muscle relaxation on the fatigue and quality of life among Iranian aging persons. Acta Med Iran. 2016;54(7):430–436.
20. Maratos AS, Gold C, Wang X, Crawford MJ. Music therapy for depression. Cochrane Database Syst Rev. 2008;1:Cd004517. doi:10.1002/14651858.CD004517.pub2
21. de Witte M, Pinho ADS, Stams GJ, Moonen X, Bos AER, van Hooren S. Music therapy for stress reduction: a systematic review and meta-analysis. Health Psychol Rev. 2022;16(1):134–159. doi:10.1080/17437199.2020.1846580
22. Roddis JK, Tanner M. Music therapy for depression. Res Nurs Health. 2020;43(1):134–136. doi:10.1002/nur.22006
23. Dunstan DA, Scott N. Clarification of the cut-off score for Zung’s self-rating depression scale. BMC Psychiatry. 2019;19(1):177. doi:10.1186/s12888-019-2161-0
24. Costantini L, Pasquarella C, Odone A, et al. Screening for depression in primary care with patient health questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473–483. doi:10.1016/j.jad.2020.09.131
25. Dunstan DA, Scott N. Norms for Zung’s self-rating anxiety SCALE. BMC Psychiatry. 2020;20(1):90. doi:10.1186/s12888-019-2427-6
26. [Annex 1 Generalized anxiety disorder 7]. Zhonghua Xin Xue Guan Bing Za Zhi. 2014;42:12.
27. Revicki DA, Wood M, Wiklund I, Crawley J. Reliability and validity of the gastrointestinal symptom rating scale in patients with gastroesophageal reflux disease. Qual Life Res. 1998;7(1):75–83. doi:10.1023/A:1008841022998
28. Blake MR, Raker JM, Whelan K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2016;44(7):693–703. doi:10.1111/apt.13746
29. Molassiotis A. A pilot study of the use of progressive muscle relaxation training in the management of post-chemotherapy nausea and vomiting. Eur J Cancer Care. 2000;9(4):230–234. doi:10.1046/j.1365-2354.2000.00220.x
30. Kemper KJ, Danhauer SC. Music as therapy. South Med J. 2005;98(3):282–288. doi:10.1097/01.SMJ.0000154773.11986.39
31. Applewhite B, Cankaya Z, Heiderscheit A, Himmerich H. A systematic review of scientific studies on the effects of music in people with or at risk for autism spectrum disorder. Int J Environ Res Public Health. 2022;19(9):5150. doi:10.3390/ijerph19095150
32. Geretsegger M, Fusar-Poli L, Elefant C, Mössler KA, Vitale G, Gold C. Music therapy for autistic people. Cochrane Database Syst Rev. 2022;5(5):Cd004381. doi:10.1002/14651858.CD004381.pub4
33. Bradt J, Dileo C, Myers-Coffman K, Biondo J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev. 2021;10(10):Cd006911. doi:10.1002/14651858.CD006911.pub4
34. Erkkilä J, Punkanen M, Fachner J, et al. Individual music therapy for depression: randomised controlled trial. Br J Psychiatry. 2011;199(2):132–139. doi:10.1192/bjp.bp.110.085431
35. Erkkilä J, Brabant O, Hartmann M, et al. Music therapy for depression enhanced with listening homework and slow paced breathing: a randomised controlled trial. Front Psychol. 2021;12:613821. doi:10.3389/fpsyg.2021.613821
36. Aalbers S, Fusar-Poli L, Freeman RE, et al. Music therapy for depression. Cochrane Database Syst Rev. 2017;11(11):Cd004517. doi:10.1002/14651858.CD004517.pub3
37. Bieleninik L, Geretsegger M, Mossler K, et al. Effects of improvisational music therapy vs enhanced standard care on symptom severity among children with autism spectrum disorder: the TIME-A randomized clinical trial. JAMA. 2017;318(6):525–535. doi:10.1001/jama.2017.9478
38. Battaglini MP, Pessôa Filho DM, Calais SL, et al. Analysis of progressive muscle relaxation on psychophysiological variables in basketball athletes. Int J Environ Res Public Health. 2022;19(24):17065. doi:10.3390/ijerph192417065
39. Toqan D, Ayed A, Joudallah H, et al. Effect of progressive muscle relaxation exercise on anxiety reduction among nursing students during their initial clinical training: a quasi-experimental study. Inquiry. 2022;59:469580221097425. doi:10.1177/00469580221097425
40. Gallego-Gómez JI, Balanza S, Leal-Llopis J, et al. Effectiveness of music therapy and progressive muscle relaxation in reducing stress before exams and improving academic performance in Nursing students: a randomized trial. Nurse Educ Today. 2020;84:104217. doi:10.1016/j.nedt.2019.104217
41. Içel S, Başoğul C. Effects of progressive muscle relaxation training with music therapy on sleep and anger of patients at community mental health center. Complement Ther Clin Pract. 2021;43:101338. doi:10.1016/j.ctcp.2021.101338
42. Vancampfort D, Correll CU, Scheewe TW, et al. Progressive muscle relaxation in persons with schizophrenia: a systematic review of randomized controlled trials. Clin Rehabil. 2013;27(4):291–298. doi:10.1177/0269215512455531
43. Liu K, Chen Y, Wu D, Lin R, Wang Z, Pan L. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complement Ther Clin Pract. 2020;39:101132. doi:10.1016/j.ctcp.2020.101132
44. Xiao CX, Lin YJ, Lin RQ, Liu AN, Zhong GQ, Lan CF. Effects of progressive muscle relaxation training on negative emotions and sleep quality in COVID-19 patients: a clinical observational study. Medicine. 2020;99(47):e23185. doi:10.1097/MD.0000000000023185
45. Aksu NT, Erdogan A, Ozgur N. Effects of progressive muscle relaxation training on sleep and quality of life in patients with pulmonary resection. Sleep Breath. 2018;22(3):695–702. doi:10.1007/s11325-017-1614-2
46. Blanaru M, Bloch B, Vadas L, et al. The effects of music relaxation and muscle relaxation techniques on sleep quality and emotional measures among individuals with posttraumatic stress disorder. Ment Illn. 2012;4(2):e13. doi:10.4081/mi.2012.e13
47. Ziv N, Rotem T, Arnon Z, Haimov I. The effect of music relaxation versus progressive muscular relaxation on insomnia in older people and their relationship to personality traits. J Music Ther. 2008;45(3):360–380. doi:10.1093/jmt/45.3.360
48. Warreman EB, Nooteboom LA, Terry MB, et al. Psychological, behavioural and biological factors associated with gastrointestinal symptoms in autistic adults and adults with autistic traits. Autism. 2023;27(7):2173–2186. doi:10.1177/13623613231155324
49. Ko SY, Leung DY, Wong EM. Effects of easy listening music intervention on satisfaction, anxiety, and pain in patients undergoing colonoscopy: a pilot randomized controlled trial. Clin Interv Aging. 2019;14:977–986. doi:10.2147/CIA.S207191
50. Spagnuolo R, Corea A, Blumetti M, et al. Effects of listening to music in digestive endoscopy: a prospective intervention study led by nursing. J Adv Nurs. 2020;76(11):2993–3002. doi:10.1111/jan.14516
51. Dadkhah B, Anisi E, Mozaffari N, Amani F, Pourghasemian M. Effect of music therapy with periorbital massage on chemotherapy-induced nausea and vomiting in gastrointestinal cancer: a randomized controlled trail. J Caring Sci. 2019;8(3):165–171. doi:10.15171/jcs.2019.024
52. Zhong FP, Zhong J, Zhong MY. Effect of music therapy on chemotherapy-induced nausea and vomiting in gastrointestinal cancer: a systematic review and meta-analysis. World J Gastrointest Surg. 2023;15(3):471–479. doi:10.4240/wjgs.v15.i3.471
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.