")
Back to Journals » Open Access Emergency Medicine » Volume 16
Impact of the Implementation of a Low-Complexity Emergency Care Protocol in the Patient Experience at a Level 3 Academic Institution in Colombia
Authors Devia Jaramillo G , Vargas Gallo JP, Esmeral-Zuluaga NM
Received 14 May 2024
Accepted for publication 20 November 2024
Published 18 December 2024 Volume 2024:16 Pages 329—336
DOI https://doi.org/10.2147/OAEM.S478196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
German Devia Jaramillo,1,2 Juan Pablo Vargas Gallo,1 Nathalia Maria Esmeral-Zuluaga3
1Emergency Department Hospital Universitario Fundación Santafé de Bogotá, Bogotá, Colombia; 2Grupo de Investigación Clínica, Escuela de Medicina y Ciencias de la Salud, Universidad del Rosario, Bogotá, Colombia; 3School of Medicine and Health Sciences, Universidad Del Rosario, Bogotá, Colombia
Correspondence: German Devia Jaramillo, Email [email protected]
Introduction: Emergency department overcrowding is a universal problem. It is associated not only with poor clinical outcomes but also with a decrease in patient satisfaction, especially in patients with low complexity emergencies or triage 4 and 5, who tend to have a longer waiting time.
Objective: This study aims to determine whether the implementation of a care strategy for patients with low complexity emergencies called “The special Line” in the emergency department of a third level academic institution in Colombia, has a positive impact on the level of satisfaction with the care received by the patient and the number of people who leave without being seen.
Methods: This is a retrospective analytical observational study that looks at the effect on the rate of patients who leave without being seen and the net promoter score (NPS) of the entire emergency department of establishing a protocol for the care of patients with low complexity emergencies.
Results: Of a total of 22,743 patients divided into the two comparison groups, it was found that after the implementation of the care protocol, a non-significant reduction in the median rate of patients without care from 2.35% to 1.85% was documented, as well as a significant improvement in the median value of the NPS from 44 to 53, p: 0.001.
Conclusion: The implementation of a protocol for the care of patients with low-complexity emergencies demonstrated a significant improvement in the experience of care for all users in the emergency service, additionally, indirectly influencing the leave without being seen of the entire emergency service.
Keywords: patient satisfaction, emergency department, overcrowding, patient safety
Introduction
Overcrowding in the emergency department, which is a constant problem worldwide,1 results in decreased patient satisfaction, financial losses due to patient loss, decreased patient safety, and decreased staff morale,2 overcrowding is also associated with increased medical errors.3 These results happen in all triage types of patients, even in low complexity emergencies where delay in care is related to increased mortality.4 For this reason, the ability to provide rapid, efficient, and empathetic care to this population could have an impact not only on the perception of care received but also on the effectiveness of health systems.
In the busy world of emergency medical care, patient satisfaction emerges as a key indicator of the quality of services provided.5 Patients arriving at the emergency department with problems of low complexity, ie classified as triage 4 and 5, in a 5-level classification system,6 represent a significant proportion of visits to these departments.
For the care of low complexity patients, different strategies have been described in the literature that help reduce the time of care and overcrowding in the emergency department like “Acute Medical Units” or “Rapid Assessment Zones”.7 Additionally, there are studies that show that the systematic follow-up of patients’ symptoms and opinions, that is, the use of patient-reported outcomes (PRO), improves patient-physician communication, physician awareness of symptoms, treatment, patient satisfaction, quality of life and overall survival.8
Based on the premise of the importance of measuring PRO outcomes, this study aims to determine whether the implementation of a care strategy for patients with low complexity emergencies called “The special Line” in the emergency department of a third level academic institution in Colombia has a positive impact on patient experience with the care received, in addition to reducing the left without being seen rate.
Material and Methods
Study Design
This is a retrospective analytical observational study.
Population
The study used information from the emergency department databases of the Hospital Universitario Fundación Santafé. This is a high complexity university hospital that attends approximately 60,000 adult emergencies per year of which approximately 56% are low complexity emergencies classified as triage 4 and 5.
Eligibility Criteria
Adult patients attending the Hospital Universitario Fundación Santafé seeking emergency medical care classified as triage 4 and 5 were included. The patients were assessed under the care protocol called “The special Line” between February 2018 and December 2019. Patients in pregnancy, population under 18 years of age, orthopedic emergency patients and incomplete data in medical records were excluded from the study.
Methodology
Patients treated in 2019 were the intervention group, while patients treated in 2018 were considered the comparison group, because in 2018 “The special Line” protocol did not exist. Initially, “The special Line” protocol was implemented in February between 10 am and 7 pm from Monday to Friday for patients with triage classification 4 and 5 who had specific medical insurances. Later, it was implemented 24 hours a day and 7 days a week; however, it did not continue to include only some specific insurances. For this reason, only patients who were classified in this same way during the same hours and similar health insurers during 2018 were selected as a comparison group.
Protocol “The Special Line”
The strategy called “The special Line”, is a method that combines the Fast Track strategy plus an Acute Medical Unit (AMU), designed for patients with low complexity emergencies. These patients are identified upon admission to the emergency department by the triage performed by nurses in the hospital and subsequently directed to the area designated as “The special Line”. This AMU has a group of physicians, nurses and exclusive assistants who are in charge of directing the patient in the process of medical care until their definition, in general, a specialist in emergency medicine or family medicine and a general practitioner support per shift is required. These patients have different consultation areas from more complex patients, using a designated area within the emergency room. In this space, there are two consultation rooms equipped according to national standards for low complexity emergency care. In addition, these patients are taken to diagnostic imaging by the usual physical routes for all emergency patients, and laboratory samples are processed and transported by personnel who are called by the head nurse of “The special Line”. The support staff for high complexity and low complexity emergency processes is the same. Inter-specialty consultation processes are the same as for all ED patients and hospitalization beds are the same as for other ED patients.
Definition of Terms
LWBS (leave without being seen or unmet demand): Patients who come to an emergency department (ED) and leave without being seen by a physician is the definition of LWBS.9 This is a safety concern as these patients may increase their morbidity and experience adverse events because of the lack of or delay in ED treatment.10
EDLOS (emergency department length of stay): A condition increasing resulting from overcrowding of the emergency department, EDLOS is considered to simply refer to the length of stay (LOS)(2) in the emergency department (ED).
NPS (Net promoter Score) Index: Improving patient experiences in health care is increasingly becoming a central strategic imperative and is central to overall health care performance.11 The term “patient experience” refers to “the sum of all interactions shaped by an organization’s culture that influence patients’ perceptions across the continuum of care”.12 One method for assessing patient experience is the Net Promoter Score (NPS), created in 2003,13 NPS is a popular topographic method that is used globally and has been dubbed ‘the ultimate question”.14 NPS consists of a two-part questionnaire. First, respondents are presented with a rating question: “How likely are you to recommend our business/service to a friend or colleague?” on a scale of 0 (unlikely) to 10 (very likely). This is followed by an opening free-text element, which allows respondents to provide the main reason for their rating. According to the score provided, responses are categorized into three groups: “Detractors” (scores 0–6), “Passives” (scores 7 and 8) and “Promoters” (scores 9 and 10). The overall score, known as the “Net Promoter Score”, is calculated by subtracting the percentage of Detractors from the percentage of Promoters; therefore, the NPS can range from −100 (ie, all Detractors) to +100 (ie, all Promoters).14
PRO outcomes: Patient-reported outcomes (PROs) include data reported directly by people about how they feel and function, such as symptoms, physical function, and quality of life.15
Sample Size
All patients seen at the EDs classified as triage 4 and 5 during the study period who met the inclusion criteria were included. Since this was an observational study, no sample size calculation was performed.
Measurement of Net Promoter Score
After completing the care of patients in the emergency department of the institution, patients are routinely called by telephone by an external entity to the hospital and asked the question for the evaluation of the NPS of the emergency department.
Data Analysis Plan
Differences in age, number of patients, gender and admission diagnosis were evaluated to establish comparability between groups. For quantitative variables, differences were established by calculating Student’s t-test (if the variable had normal distribution), or Wilcoxon (if it did not have normal distribution). The chi2 test was used to determine differences in categorical variables.
A descriptive analysis of the variables under study was performed, with frequency distribution for categorical variables and central tendency and dispersion measurements for continuous variables according to the type of distribution (mean and standard deviation or median and interquartile ranges (IQR) for normal or non-normal distribution, respectively) for which the normality test (Kolmogorov–Smirnov) was applied.
Subsequently, the statistical significance of the mean differences in the values of the percentage of unmet demand and the NPS score was established using Student’s t test for normally distributed variables or Wilcoxon for non-normally distributed variables. The statistical program R Version 1.4.1106 © 2009–2021 RStudio, PBC was used for the analyses. The study was not externally funded.
Results
The total number of emergencies attended in the study years was 104272, of which 11349 patients were analyzed for the intervention group and 11403 for the comparison group; however, the measurement of the NPS, as well as the unattended demand, was made for the total number of patients who attended the emergency department per year, Figure 1.
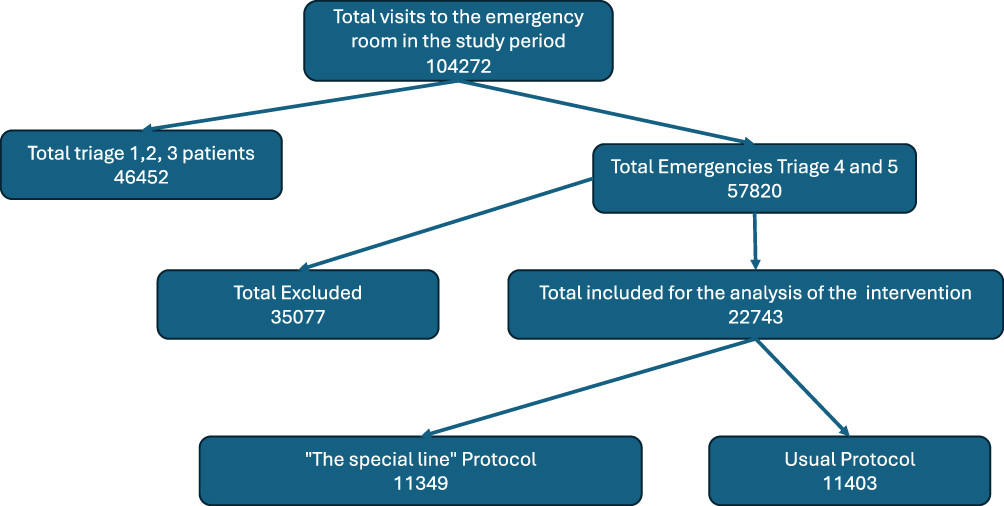 |
Figure 1 Patient selection algorithm. |
When comparing 2018 and 2019 in triage group 4 and 5, we found that in 2018 (usual care) a total of 28,781 patients were treated and in 2019 (The special line protocol) a total of 29,039 patients were treated. There was an increase of 0.8%. However, of the total number of patients with low complexity emergencies that met the inclusion criteria and were used in the analysis. Interestingly, 36.6% were included for the comparison group and 39.0% for the intervention group of the total number of patients for each group.
No difference was found when evaluating the demographic variables, which made the groups comparable. Table 1.
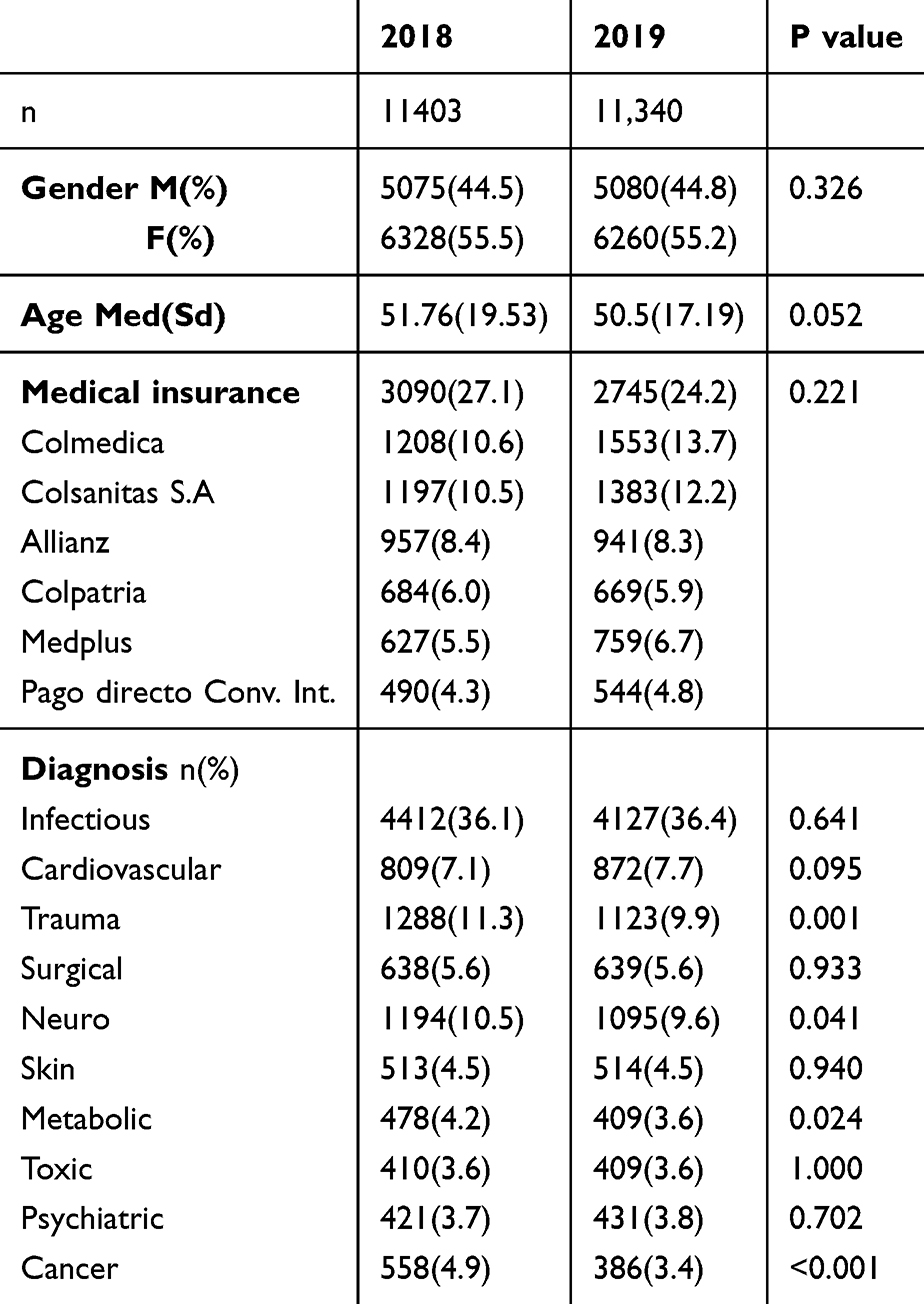 |
Table 1 Patient Characteristics |
The implementation of “The special Line” protocol during the study period resulted in a reduction in the of patients who left without being seen in all patients seen in the ED, In particular, in 2018 the total patients evaluated was 51160, median unmet demand (LWBS) 2,350 (1,900–2,900) and in 2019 total patients was 53112 median LWBS 1,850 (1,650–2,375). p value: 0.379. Figure 2.
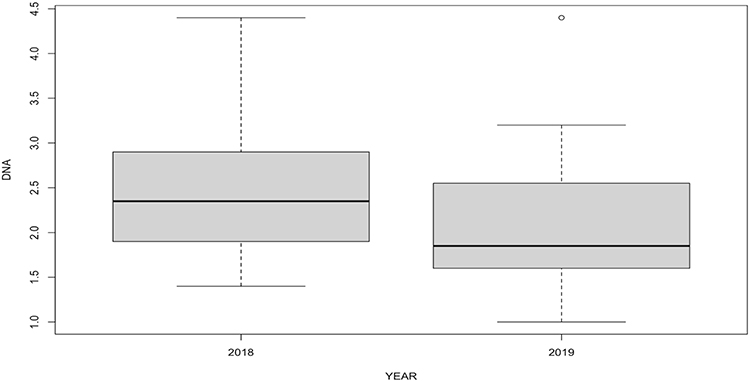 |
Figure 2 Leave without being seen. Abbreviations: DNA, unmet demand. |
Finally, when comparing the degree of patient satisfaction before and after the implementation of the “The special Line” protocol, it was possible to determine that there was a significant increase in the NPS value from 2018 to 2019. NPS year 2018, mean (Sd) 44 (7.471) vs NPS year 2019, mean (SD) 56.3 (8.906). p value: 0.001. Figure 3
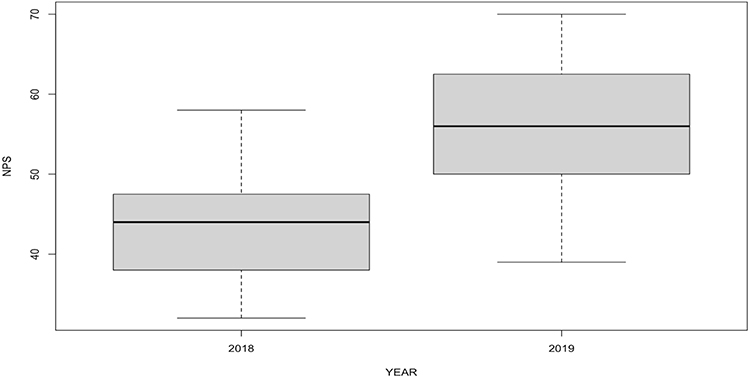 |
Figure 3 Net Promoter Score value from 2018 to 2019. |
Discussion
The objective of this study was estimate the effect on the satisfaction of patients consulting for low complexity emergencies of the implementation of a rapid care strategy called “The special Line”. This study recruited 22742 patients for analysis. It was considered that the groups were comparable in sex, age and no significant difference was found between the diagnoses of the groups. In addition the number of patients in both the intervention and observation groups were similar.
This study showed that after the implementation of “The special Line” care strategy, the satisfaction of all patients, regardless of the admission triage and not only those who consulted with low complexity emergencies, increased significantly when compared with the group of patients seen in the emergency department the previous year. The average NPS of all independent admission triage patients in the comparison year was 44, while the average NPS in the intervention year for the entire ED was 56.6. This data demonstrates the importance of patients who consult the service with low complexity emergencies, which are approximately 50% of the entire population that comes for care in the emergency department. For Latin America, Leslie et al demonstrated that the NPS is useful for determining the performance of health services.16 Although there are not many published studies that show the degree of satisfaction with interventions in emergency departments of users using the NPS, the work of Vu MT et al17 showed that with an adjustment to the program of antibiotic administration to patients with appendicitis in the emergency department, the NPS of users with this pathology increased from 26.0 to 78.3.17 Another study in the United Kingdom showed that the implementation of a rapid care unit for surgical pathologies in the emergency room not only reduced hospital mortality due to emergency laparotomy but also significantly improved the NPS of users from 64.1 to 82.2.18 These reports, added to the current study, prove that with simple modifications in emergency room processes, improvements can be achieved not only in clinical outcomes but also in PROs, which are becoming increasingly important.
This work further demonstrated that with the intervention protocol, the percentage of patients leaving without being seen (LWBS) for the entire ED was reduced from 2.35% to 1.85% from 2018 to 2019, respectively. We consider this reduction relevant even though it is not statistically significant, given that it is a reduction in the percentage of patients who leave without being seen from the entire emergency service, and not only the low-complexity emergencies in which the care protocol was applied. We believe that by implementing a specific protocol for caring for patients with low-complexity emergencies, separating them from patients with more complex emergencies, the care times for all patients seen in the emergency department could be reduced, regardless of their level of complexity, compared to when all patients were seen with the usual care strategy (according to their priority according to triage), since at that time low-complexity patients waited more hours for care, positively influencing the overall care load. We believe that we did not find a significant reduction because there are other variables that we could not control in the groups of patients with greater complexities. A study conducted by nursing staff demonstrated that patients with minor injuries and illnesses who came to the ED and were directed to an expedited care line decreased the wait time to be seen from 56 to 30 minutes, with an increase in patients seen within 1 hour from 63% to 90%,19 and with a decrease in EDLOS from 57 to 34 minutes,20 even referring patients with minor traumatic injuries through these rapid care lines has shown a 30% decrease in first contact time to a physician without being at the expense of patients with more urgent needs.21
On the other hand, in addition to the reduction in waiting times and length of stay in the emergency department, its implementation has also shown a reduction in the total number of patients who leave without being seen, from 5% to 2%.22 Thus, with a structured rapid care protocol, it is possible to significantly reduce the unattended demand of emergency rooms, and on the other hand, it is possible to contribute to the reduction of overcrowding in emergency departments.
Additionally, by actively soliciting feedback from patients and involving them in the process of measuring the quality of patient care, it is important to increase the understanding of the patient’s experience in different contexts and thus ensure more effective intervention.23
Limitations
This was a study conducted in a single hospital center with specific characteristics, so care should be taken to generalize the results. Nevertheless, the findings of this study allow institutions with similar characteristics to consider establishing this type of rapid care protocols for their emergency departments.
Conclusion
The implementation of a protocol for the care of patients with low-complexity emergencies demonstrated a significant improvement in the experience of care for all users in the emergency service, additionally, indirectly influencing the leave without being seen of the entire emergency service.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted at the Hospital Universitario Fundación Santafé de Bogotá, in Colombia, and was approved by the institution’s research and ethics committee with approval number CCEI-15670-2023. This study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. The researchers did not expose the patients to biological, psychological, or social risks. Therefore, the ethics committee approved the waiver of informed consent. All research information was kept confidential in a password-protected file with access to the data limited only to the research group.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no competing interests in this work.
References
1. Bond K, Ospina M, Blitz S, et al. Frequency, Determinants and Impact of Overcrowding in Emergency Departments in Canada: a National Survey. 10(4):32–40. doi:10.12927/hcq.2007.19312
2. Di Somma S, Paladino L, Vaughan L, Lalle I, Magrini L, Magnanti M. Overcrowding in emergency department: an international issue. Intern Emerg Med. 2015;10(2):171–175. doi:10.1007/s11739-014-1154-8
3. Liu SW, Thomas SH, Gordon JA, Hamedani AG, Weissman JS. A Pilot Study Examining Undesirable Events Among Emergency Department–Boarded Patients Awaiting Inpatient Beds. Ann Emergency Med. 2009;54(3):381–385. doi:10.1016/j.annemergmed.2009.02.001
4. Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ. 342(01):d2983–d2983. doi:10.1136/bmj.d2983
5. Trout A, Magnusson AR, Hedges JR. Patient satisfaction investigations and the emergency department: what does the literature say? Acad Emerg Med. 2000;7(6):695–709. doi:10.1111/j.1553-2712.2000.tb02050.x
6. Kuriyama A, Urushidani S, Nakayama T. Five-level emergency triage systems: variation in assessment of validity. Emerg Med J. 2017;34(11):703–710. doi:10.1136/emermed-2016-206295
7. Bittencourt RJ, Stevanato ADM, CTNM B, Gottems LBD, O’Dwyer G. Interventions in overcrowding of emergency departments: an overview of systematic reviews. Rev saúde pública. 54:66.
8. Basch E, Deal AM, Dueck AC, et al. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA. 318(2):197. doi:10.1001/jama.2017.7156
9. Polevoi SK. Factors Associated with Patients Who Leave without Being Seen. Acad Emergency Med. 12(3):232–236. doi:10.1197/j.aem.2004.10.029
10. Rowe BH, Channan P, Bullard M, et al. Characteristics of Patients Who Leave Emergency Departments without Being Seen. Acad Emergency Med. 2006;13(8):848–852. doi:10.1197/j.aem.2006.01.028
11. Adams C, Walpola R, Schembri AM, Harrison R. The ultimate question? Evaluating the use of Net Promoter Score in healthcare: a systematic review. Health Expect.
12. Bell SK, Dong J, Ngo L, McGaffigan P, Thomas EJ, Bourgeois F. Diagnostic error experiences of patients and families with limited English-language health literacy or disadvantaged socioeconomic position in a cross-sectional US population-based survey. BMJ Qual Saf.
13. Hamilton DF, Lane JV, Gaston P, et al. Assessing treatment outcomes using a single question: the Net Promoter Score. Bone Joint J. 2014;96(5):622–628.
14. Krol MW, de Boer D, Delnoij DM, JJDJM R. The Net Promoter Score - an asset to patient experience surveys? Health Expect. 18(6):3099–3109. doi:10.1111/hex.12297
15. Basch E, Barbera L, Kerrigan CL, Velikova G. Implementation of Patient-Reported Outcomes in Routine Medical Care. Am Soc Clin Oncol Educat Book. 122–134.
16. Leslie HH, Lee HY, Blouin B, Kruk ME, García PJ. Evaluating patient-reported outcome measures in Peru: a cross-sectional study of satisfaction and net promoter score using the 2016 EnSuSalud survey. BMJ Qual Saf. 2022;31(8):599–608. doi:10.1136/bmjqs-2021-014095
17. Vu MT, Schwartz H, Straube S, et al. Compass for antibiotic stewardship: using a digital tool to improve guideline adherence and drive clinician behaviour for appendicitis treatment in the emergency department. Emerg Med J. 40: 847–853. doi:10.1136/emermed-2022-213015
18. Navarro A, Hardy E, Oakley B, Mohamed E, Welch N, Parsons S. The front-line general surgery consultant as a new model of emergency care. Annals. 99(7):550–554. doi:10.1308/rcsann.2017.0081
19. Rogers T, Ross N, Spooner D. Evaluation of a ‘see and treat’ pilot study introduced to an emergency department. Accident and Emergency Nursing. 2004;12(1):24–27. doi:10.1016/j.aaen.2003.08.005
20. Fernandes CM, Christenson JM, Price A. Continuous quality improvement reduces length of stay for fast-track patients in an emergency department. Acad Emerg Med. 1996;3(3):258–263.
21. Cooke MW. The effect of a separate stream for minor injuries on accident and emergency department waiting times. Emer Med J. 19(1):28–30. doi:10.1136/emj.19.1.28
22. Darrab AA, Fan J, Fernandes CMB, et al. How does fast track affect quality of care in the emergency department? Eur J Emerg Med. 2006;13(1):32–35. doi:10.1097/00063110-200602000-00008
23. Al-Abri R, Al-Balushi A. Patient satisfaction survey as a tool towards quality improvement. Oman Med J. 2014;29(1):3–7. doi:10.5001/omj.2014.02
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between the Emergency Department Length of Stay and in-Hospital Mortality: A Retrospective Cohort Study
Habib H, Sudaryo MK
Open Access Emergency Medicine 2023, 15:313-323
Published Date: 13 September 2023
Impact of Target Management Card on Patient Safety in the Emergency Department: A Mixed Methods Study
Chen L, Yang H, Cui S, Ye D
Risk Management and Healthcare Policy 2023, 16:1905-1914
Published Date: 18 September 2023
Perceived Causes and Effects of Overcrowding Among Nurses in the Emergency Departments of Tertiary Hospitals: A Multicenter Study
Guerrero JG, Alqarni AS, Cordero RP, Aljarrah I, Almahaid MA
Risk Management and Healthcare Policy 2024, 17:973-982
Published Date: 20 April 2024
Correlation Between Emergency Department Crowding and Adverse Occurrences in an Academic Hospital: A Retrospective Cohort Study
Alassaf W, Albrahim R, Abukhaled JK, Aldhaif M, Mohammed MA, Al Baiz A, Aljahany M
Risk Management and Healthcare Policy 2025, 18:561-568
Published Date: 19 February 2025
An Updated Scoping Review of Factors Associated with Length of Stay in Emergency Department
Kurhayati K, Emaliyawati E, Trisyani Y
Journal of Multidisciplinary Healthcare 2025, 18:3191-3203
Published Date: 4 June 2025