")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Improved Tubeless Airway Management in JORRP Surgery: Comparative Analysis of Pre- and Post-THRIVE Implementation
Authors Lei G, Yang S, Wu L, Yin Y, Xi C, Xiao Y, Wang G
Received 4 January 2025
Accepted for publication 3 May 2025
Published 8 May 2025 Volume 2025:21 Pages 647—654
DOI https://doi.org/10.2147/TCRM.S513941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Guiyu Lei,1 Siliu Yang,2 Lili Wu,1 Yue Yin,1 Chunhua Xi,1 Yang Xiao,3 Guyan Wang1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China; 2Department of Anesthesiology, Beijing Dongcheng Maternal and Child Health Care Hospital, Beijing, 100007, People’s Republic of China; 3Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University, Key Laboratory of Otolaryngology, Head and Neck Surgery (Ministry of Education of China), Beijing, 100730, People’s Republic of China
Correspondence: Guyan Wang, Department of Anaesthesiology, Beijing Tongren Hospital, Capital Medical University, No. 1 Dongjiaominxiang, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86 13910985139, Email [email protected]
Background: Juvenile-onset recurrent respiratory papillomatosis (JORRP) is a severe pediatric condition requiring frequent surgical interventions to maintain airway patency. Managing oxygenation during tubeless anesthesia for these surgeries poses significant challenges. In 2021, our center introduced transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) as a novel method for airway management in JORRP surgeries. This study evaluated the impact of THRIVE on perioperative outcomes in pediatric JORRP surgeries.
Methods: This was a retrospective study of 122 pediatric JORRP surgical cases carried out at a tertiary center. Patients who underwent surgery prior to the implementation of THRIVE served as the control group (pre-THRIVE), while those treated after its introduction served as the intervention group (post-THRIVE), with 61 patients in each group. Perioperative data, including surgery and anesthesia parameters and extubation frequency were collected.
Results: A total of 122 patients were included. Baseline characteristics were comparable between groups. After the introduction of THRIVE, the median number of extubations significantly decreased from a median 3 in the pre-THRIVE group to 1 in the post-THRIVE group (P < 0.001). Minimum intraoperative SpO2 levels were significantly higher in the post-THRIVE group (98% vs 85%, P < 0.001). Surgery duration was reduced from 41 minutes to 35.5 minutes (P =0.003), and anesthesia duration decreased from 67 minutes to 58.5 minutes (P =0.016). No significant differences were observed in PACU stay length or complications between the groups.
Conclusion: The implementation of THRIVE in pediatric JORRP enhances intraoperative efficiency and safety. Further research is warranted to assess its long-term effect.
Keywords: THRIVE, JORRP, tubeless anesthesia, airway management, SpO2
Introduction
Juvenile-onset recurrent respiratory papillomatosis (JORRP) is a rare yet challenging pediatric condition caused by human papilloma virus infection, characterized by the recurrent growth of benign papillomas in the respiratory tract, leading to progressive airway obstruction, dysphonia, and potentially life-threatening respiration complications.1–4 Surgical removal of these papillomas remains the cornerstone of treatment, aiming to maintain airway patency and alleviate symptoms.5 However, the primary challenge in JORRP surgery is effectively managing a shared airway between the surgeon and the anesthesiologist. Achieving an unobstructed surgical field frequently necessitates tubeless airway management, placing considerable responsibility on anesthesiologists to ensure adequate oxygenation and ventilation.6,7 Pediatric patients further compound this challenge due to their higher oxygen consumption and lower functional residual capacity, making them particularly susceptible to rapid desaturation. Additionally, repeated extubation and reintubation during surgery not only disrupts the surgical process but also increase the risk of airway injury.
Traditional airway management techniques used during JORRP surgeries, such as controlled ventilation, spontaneous breathing, and intermittent apneic techniques, have been the mainstay approaches for maintaining oxygenation and ventilation.8–11 However, there is no consensus on the optimal airway strategy in shared airway management. Recently, transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) has emerged as an innovative and effective approach to airway management in pediatric patients.12–14 THRIVE delivers continuous high-flow humidified oxygen via nasal cannula, enabling apneic oxygenation, extending safe apnea durations, and enhancing surgical access without the need for frequent airway manipulations.
In a prior study conducted at our center, we evaluated the efficacy of THRIVE in JORRP surgeries through a randomized controlled trial, which demonstrated a significant improvements in oxygenation, fewer desaturation events, and short operative and anesthesia times.7 To further expand on these findings, we analyzed intraoperative airway management data by retrospectively comparing surgeries conducted before the adoption of THRIVE, which relied on traditional techniques, to those performed after its implementation. This study aims to provide a comprehensive comparison of these two approaches, offering insights into the clinical advantages of THRIVE and its role in optimizing anesthesia strategies for challenging pediatric population.
Materials and Methods
This was a retrospective study conducted at Beijing Tongren Hospital, a tertiary referral center, and approved by the institutional review board of Beijing Tongren Hospital. This study adhered to Declaration of Helsinki principles. THRIVE was introduced for airway management during JORRP surgeries by the authors in 2021. Patients aged below 12 years who underwent JORRP surgeries between January 2019 and May 2024 were included and divided into two groups based on the timing of their surgeries: the pre-THRIVE (January 2019 to November 2021) and the post-THRIVE group (June 2022 to May 2024). The time gap between these periods (November 2021 to June 2022) corresponds to the initial implementation phase of THRIVE and the conduct of a randomized controlled trial at our center. Patients treated during this phase, as well as those with a tracheostomy, were excluded from the study. Written informed consent of the parents was obtained from all patients before study commencement. A total of 61 consecutive cases were included in each group to ensure comparability. Data were extracted from the hospital’s electronic anesthesia records, including patients demographics, anesthesia and surgery durations, intraoperative vital signs and PACU parameters. The number of extubations during surgery was determined by reviewing intraoperative video recordings.
Induction of Anesthesia
Prior to anesthesia induction, a variety of endotracheal (ET) tube sizes (ranging from 2.5 to 6.0 mm), along with stylets, tracheostomy trays, cricothyroidotomy tools, and resuscitation equipment, were prepared in the operating room to ensure readiness. A laryngologist with significant expertise was present to address any complications, such as failed intubation or progression from partial to complete airway obstruction caused by muscle relaxation or papilloma prolapse during the induction process. Preoxygenation was performed, and intravenous access was secured, followed by the administration of atropine (0.015 mg/ mg, maximum 0.5 mg) to minimize secretions. Induction was initiated either by inhalation or intravenous administration methods, depending on the patient’s cooperation and the degree of airway obstruction.
For inhalation induction, 8% sevoflurane with oxygen at a flow rate of 8 L/min was used initially, then adjusted to 4%, ensuring spontaneous breathing was maintained throughout. Temporamandibular relaxation signaled readiness for intubation. In the case of intravenous induction, fentanyl (2 μg/kg) and propofol (2–3 mg/kg) were given, followed by succinylcholine (1.5–2 mg/kg) once controlled ventilation via a mask was verified as feasible. Intubation was conducted carefully, with tube size chosen based on either the glottis vera diameter seen under laryngoscopy or, when visibility was limited, on preoperative airway assessments and patient age. After successful intubation, cisatracurium (0.2 mg/kg) was administered. General anesthesia was maintained using continuous infusion of remifentanil and Propofol, with bolus adjustments applied at the anesthetist’s discretion.
Airway Management Methods
After initial debulking, tubeless anesthesia was implemented to facilitate the removal of residual papilloma fragments from the hypopharynx and trachea. Following brief hyperventilation to achieve an SpO2 of 100% and a PETCO2 of 30 to 33 mmHg, the tracheal tube was removed to optimize surgical exposure.
In the pre-THRIVE group, patients remained apneic without oxygen supplementation during the tubeless period. When SpO2 dropped to 90%, the anesthesiologist alerted the surgeon to pause the procedure. The tracheal tube was reinserted, connected to the anesthesia machine, and manual ventilation was administered to rapidly restore oxygenation. Once SpO2 stopped decreasing and began to rise, reaching 85%, mechanical ventilation was initiated with increased frequency to facilitate hyperventilation and carbon dioxide clearance. When oxygen saturation returned to 100% and PETCO2 levels decreased to 30–33mmHg, the tracheal tube was removed again, and surgery resumed. This cycle was repeated as needed until the procedure was completed.
In the post-THRIVE group, oxygen was continuously delivered via an OptiflowTM (Fisher & Paykel Healthcare) system at a weight-adjusted flow rate (5–15 kg, 2 L/kg/min; 15–30 kg, 35 L/min; 30–50 kg, 40 L/min; >50 kg, 50 L/min) with an FiO2 of 1.0. Due to concerns about the risk of airway fires, carbon dioxide lasers were avoided, and a microdebrider was used instead. Patients were positioned in a “sniffing” posture, and a suspended laryngoscope placed to meet surgical requirements.
All procedures were performed under suspension microlaryngoscopy using microdebriders. No CO2 lasers were used in either group. At the end of the surgery, all patients were returned to mechanical ventilated and extubated under standard monitoring. Postoperatively, all patients were transferred to the PACU and routinely received supplemental oxygen at 2L/ min via nasal cannula.
Statistical Analysis Method
Data were analyzed using SPSS software version 22.0. Categorical variables were presented as frequencies and percentage, while continuous variables were described using median and interquartile range or mean and standard variation as appropriate. Categorical variables were compared between patients in two groups using Fisher’s exact test and continuous variables were compared with Wilcoxon rank sum test. Vital signs comparisons at each time point between the groups were initially assessed with repeated measures ANOVA, followed by simple effects analysis for interactions that were statistically significant. All tests were two-sided, and a p value < 0.05 was deemed statistically significant.
Results
A total of 122 patients who underwent JORRP surgery were included in this retrospective study, with 61 patients in the control group (pre-THRIVE) and 61 patients in the THRIVE group (post-THRIVE implementation). The baseline characteristics of both groups were comparable, as shown in Table 1. The majority of patients were classified as ASA III in both groups (73.8% pre-THRIVE vs 60.7% post-THRIVE, P=0.37). The median age of disease onset was 2 years for the pre-THRIVE and 1 year for post-THRIVE group, with no significant differences (P=0.19). Both groups had a median of over 10 operations. Dyspnea grades II and III were present in approximately 60% of patients in both groups. Additionally, severe airway obstruction (> 50%) was observed in 77% of pre-THRIVE patients and 82% of post-THRIVE patients.
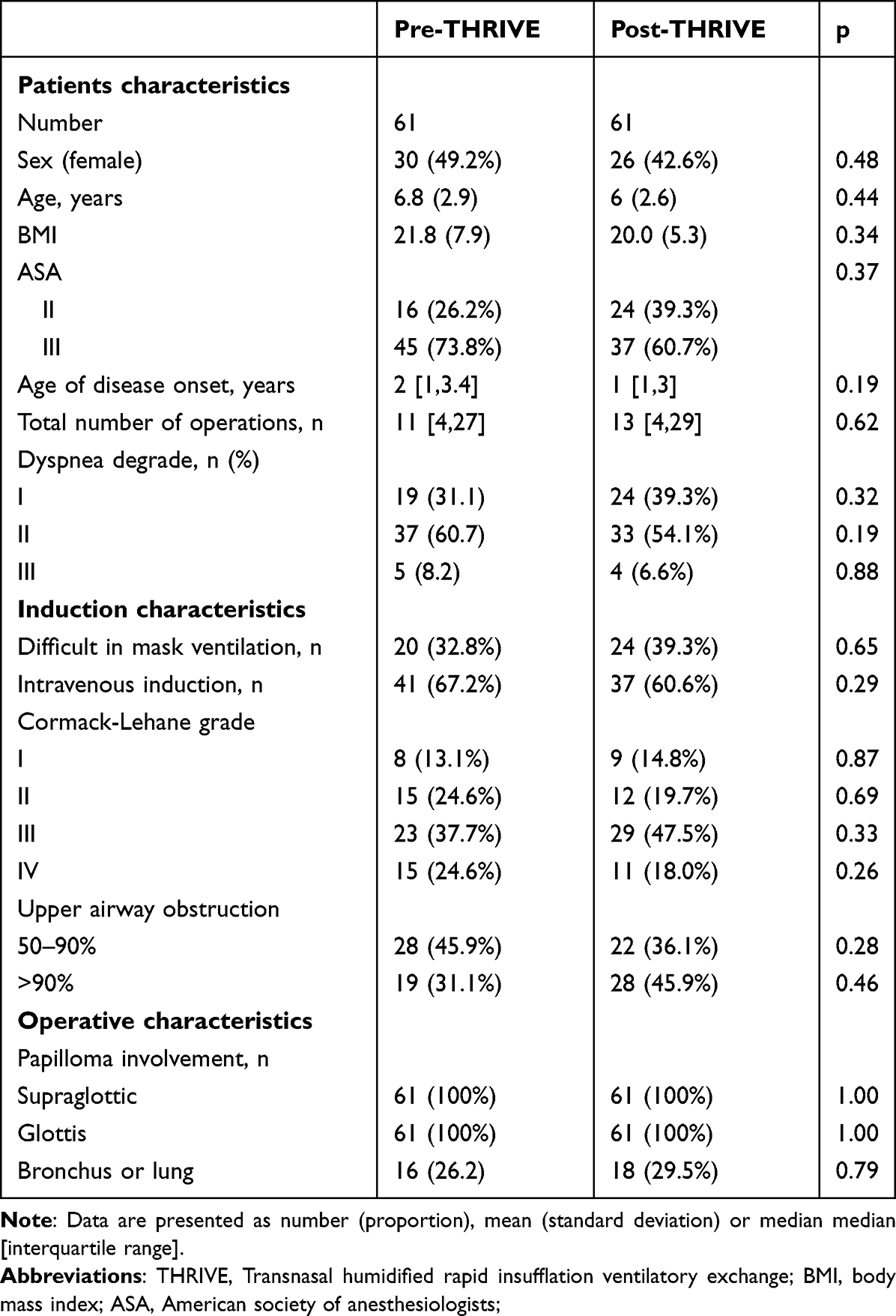 |
Table 1 Demographic Data by Pre-THRIVE vs Post- THRIVE Implementation |
Post-THRIVE implementation resulted in a significant reduction in the number of extubations, decreasing from a median of 3 to 1 (P<0.001). The THRIVE group exhibited significantly higher intraoperative minimum SpO2 levels compared to the control group (98% vs 85%, P< 0.05). The average surgery duration in the post-THRIVE group was significantly shorter compared to the pre-THRIVE group (35.5 minutes vs 41 minutes, P=0.003; Table 2), and the anesthesia duration was also significantly reduced in the post-THRIVE group than in the pre-THRIVE group (58.5 minutes vs 67 minutes, P=0.016; Table 2). The intraoperative maximum heart rate decreased slightly from 121.9 bpm in the pre-THRIVE group to 113 bpm in the post-THRIVE but without statistical significance (P=0.25). SpO2 upon arrival at PACU and the PACU stay length was similar between two groups. No significant difference between two groups in vital signs (Figure 1). Additionally, no airway complications were observed in either group.
 |
Table 2 Intraoperative Data by Pre-THRIVE vs Post- THRIVE |
 |
Figure 1 Perioperative vital signs before induction (T0), after induction (T1), surgery began (T2), 5 minutes after surgery started (T3), 10 minutes after surgery started (T4), 20 minutes after surgery started (T5), 30 minutes after surgery started (T6), at the end of surgery (T7), during post-anesthesia care unit (T8), 1 day post surgery (T9). (A) mean arterial pressure (MAP); (B) heart rate (HR). |
Discussion
Our study showed that after the implementation of THRIVE, anesthesia and surgery durations were significantly reduced, the maximum drop in intraoperative oxygen saturation was minimized, and the frequency of extubations decreased in pediatric JORRP surgeries. These findings demonstrated the value of this technique in improving procedural efficiency and intraoperative safety.
JORRP is a severe pediatric disease characterized by repeated growth of papillomas in the respiratory tract,2,15 necessitating frequent surgical interventions to maintain airway patency and function.3,16 The standard approach involves surgical debulking under suspension microlaryngoscopy, performed under general anesthesia, where a tubeless airway becomes essential for accessing the hypolarynx or intratracheal lumen. Various oxygenation strategies, such as spontaneous ventilation, mechanically controlled ventilation, apneic intermittent ventilation, and jet ventilation, have been utilized during suspension interventional microlaryngoscopy.10,17–19 However, each method has its limitations. A retrospective review of 1093 microlaryngoscopy procedures identified significant risks associated with jet ventilation, including laryngospasm, barotrauma and pneumothorax, making apneic intermittent ventilation a safer option.11,17 Spontaneous ventilation is increasingly preferred in pediatric shared airway surgeries, however, striking a balance between maintaining spontaneous breathing and achieving adequate anesthesia depth during such procedures remains challenging, as both insufficient and excessive anesthesia can lead to complications such as laryngospasm, bronchospasm, hypoxemia and hypercarbia. Humphreys et al proposed nasal high-flow oxygen delivery combined with spontaneous breathing as a promising alternative for tubeless airway assessment in children with abnormal airways,8 however, their method lacked continuous end-tidal CO2 monitoring, limiting its ability to detect hypercarbia. Bo et al9 reported a 10.3% failure rate for spontaneous ventilation, even though the majority of children only suffered from grade I laryngeal obstruction. In our center, which is a national tertiary care center that specializes in otolaryngology, most children with JORRP suffer grade II or III laryngeal obstruction, and apneic intermittent ventilation is commonly used during surgery. However, a definitive consensus on the most effective airway management strategy for JORRP surgeries has yet to be established.
THRIVE has consistently demonstrated effectiveness in prolonging apnea duration and maintaining oxygenation across various studies.20 Humphreys et al14 reported that THRIVE doubled the expected apnea duration in children. Similarly, our prior study also observed a 5-minute increase in safe apnea time compared to conventional methods. In pediatric populations, where higher oxygen consumption and lower functional residual capacity increase the risk of desaturation, THRIVE has shown particular promise. Huang et al and Riva et al emphasized its efficacy in maintaining oxygenation during shared airway surgeries in children, significantly lowering the risk of hypoxemia.13,21 Former studies have also highlighted THRIVE’s role in minimizing severe desaturation events and hypoxemia-related complications, consistently maintaining SpO2 levels above 90% during apneic procedures.12,22,23 Consistent with these findings, our study showed that in the post-THRIVE group, the minimum SpO2 significantly improved to 98%, compared to 85% in the pre-THRIVE group. However, despite its oxygenation advantages, THRIVE dose not facilitate carbon dioxide clearance.7,21 PaCO2 levels may rise by 2.4–4.1mmHg/min during apnea, which poses a significant concern in prolonged procedures. And its efficacy may be reduced in cases with significant nasal or upper airway obstruction.24
In addition, THRIVE significantly reduced the frequency of extubations, with the median number decreasing from three in the pre-THRIVE group to just one in the post- THRIVE group. This reduction ensures smoother surgical flow and minimizes airway trauma caused by repeated intubation. Moreover, fewer extubations help mitigate the risk of downward dissemination of papillomas, a critical concern in JORRP patients, which may result from mechanical irritation caused by endotracheal tubes. Waters et al24 similarly observed that THRIVE minimized the need for rescue ventilation in 95% of cases, allowing uninterrupted surgical procedures and reducing airway manipulation. Furthermore, repeated reintubation in the pre-THRIVE group may have hindered surgical assessment and increased the risk of airway edema. This was largely avoided with uninterrupted tubeless conditions in the post-THRIVE group, highlighting a clinical advantage of the technique.
Our study also revealed that both surgery and anesthesia durations were significantly reduced in the post-THRIVE group, underscoring the efficiency introduced by this technique. This finding is particular significant for children with JORRP. Substantial evidence suggests that repeated or prolonged anesthesia exposure in early childhood may have detrimental effects on neurodevelopment.25 The US FDA has issued warnings based on preclinical and epidemiological studies, indicating that exposure to general anesthesia during critical periods of brain development- particularly under 3 years- can impair synaptogenesis and neuronal maturation.26–29 Clinical research further supports these concerns, demonstrating associations between multiple anesthesia exposures and increased risk of cognitive deficits, behavioral disturbances, and delayed neurodevelopment.30–33 This issue is particularly relevant for JORRP patients, whose median age of onset is approximately 1 years, these children often require dozens of surgical interventions throughout childhood, leading to cumulative anesthetic exposure at a time when their brains are most vulnerable. By reducing both anesthesia and surgical duration, THRIVE may help mitigate these risks by limiting the total exposure to anesthetic agents, potentially improving long-term neurodevelopmental outcomes. Although no significant difference in PACU stay was observed in our study, the post-THIRVE group exhibited a trend toward shorter stays, with a reduction of nearly 10 minutes compared to the pre-THRIVE group. However, our study did not include long-term follow-up to assess neurodevelopmental outcomes, further research with larger sample sizes and longitudinal design is warranted to evaluate the long-term benefits of THRIVE, particularly in reducing the risks associated with repeated anesthesia exposure in pediatric populations such as those with JORRP.
Our study has several limitations. First, the retrospective design inherently limits the ability to control for confounding factors. Second, while this study demonstrates significant intraoperative benefits, we did not evaluate long-term outcomes. In addition, the study was conducted at a single tertiary center with which may limit the generalizability of our findings.
In conclusion, the use of transnasal humidified rapid-insufflation ventilatory exchange in pediatric JORRP surgeries reduced anesthesia and surgery durations, decreased the frequency of extubations, and minimized the maximal drop in oxygen saturation during the procedure. Further studies are warranted to evaluate its long-term effects on clinical outcomes.
Funding
This work was supported by the High Level Public Health Technical Talent Training Plan (Lingjunrencai-01-08) and Beijing Hospital Authority’s Ascent Plan (No. DFL20220203).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fortes HR, von Ranke FM, Escuissato DL, et al. Recurrent respiratory papillomatosis: a state-of-the-art review. Respir Med. 2017;126:116–121. doi:10.1016/j.rmed.2017.03.030
2. Lepine C, Leboulanger N, Badoual C. Juvenile onset recurrent respiratory papillomatosis: what do we know in 2024. Tumour Virus Res. 2024;17:200281. doi:10.1016/j.tvr.2024.200281
3. Taliercio S, Cespedes M, Born H, et al. Adult-onset recurrent respiratory papillomatosis: a review of disease pathogenesis and implications for patient counseling. JAMA Otolaryngol Head Neck Surg. 2015;141:78–83. doi:10.1001/jamaoto.2014.2826
4. Sichero L, Ferreira S, López RVM, et al. Prevalence of human papillomavirus 6 and 11 variants in recurrent respiratory papillomatosis. J Med Virol. 2021;93:3835–3840. doi:10.1002/jmv.26503
5. Yang Q, Li Y, Ma L, et al. Long-term outcomes of juvenile onset recurrent respiratory papillomatosis with pulmonary involvement. Laryngoscope. 2021;131:EE2277–E2283. doi:10.1002/lary.29376
6. Sikka K, Gupta M, Verma H, et al. Tracheo-bronchial recurrent respiratory papillomatosis: role of powered instruments in overcoming surgical challenges. Acta Otorhinolaryngol Ital. 2021;41:146–150. doi:10.14639/0392-100X-N0822
7. Lei G, Wu L, Xi C, et al. Transnasal humidified rapid insufflation ventilatory exchange augments oxygenation in children with juvenile onset recurrent respiratory papillomatosis during surgery: a prospective randomized crossover controlled trial. Anesth Analg. 2023;137:578–586. doi:10.1213/ANE.0000000000006521
8. Humphreys S, Rosen D, Housden T, et al. Nasal high-flow oxygen delivery in children with abnormal airways. Paediatr Anaesth. 2017;27:616–620. doi:10.1111/pan.13151
9. Bo L, Wang B, Shu S-Y. Anesthesia management in pediatric patients with laryngeal papillomatosis undergoing suspension laryngoscopic surgery and a review of the literature. Int J Pediatr Otorhinolaryngol. 2011;75:1442–1445. doi:10.1016/j.ijporl.2011.08.012
10. Li S-Q, Chen J-L, Fu H-B, et al. Airway management in pediatric patients undergoing suspension laryngoscopic surgery for severe laryngeal obstruction caused by papillomatosis. Paediatr Anaesth. 2010;20:1084–1091. doi:10.1111/j.1460-9592.2010.03447.x
11. Else SDN, Kovatsis PG. A narrative review of oxygenation during pediatric intubation and airway procedures. Anesth Analg. 2020;130:831–840. doi:10.1213/ANE.0000000000004403
12. Benninger MS, Zhang ES, Chen B, et al. Utility of transnasal humidified rapid insufflation ventilatory exchange for microlaryngeal surgery. Laryngoscope. 2021;131:587–591. doi:10.1002/lary.28776
13. Riva T, Pedersen TH, Seiler S, et al. Transnasal humidified rapid insufflation ventilatory exchange for oxygenation of children during apnoea: a prospective randomised controlled trial. Br J Anaesth. 2018;120:592–599. doi:10.1016/j.bja.2017.12.017
14. Humphreys S, Lee-Archer P, Reyne G, et al. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) in children: a randomized controlled trial. Br J Anaesth. 2017;118:232–238. doi:10.1093/bja/aew401
15. Ovcinnikova O, Engelbrecht K, Verma M, et al. A systematic literature review of the epidemiology, clinical, economic and humanistic burden in recurrent respiratory papillomatosis. Respir Res. 2024;25:430. doi:10.1186/s12931-024-03057-w
16. Qian ZJ, Peñaranda D, Valdez TA, et al. Recurrent respiratory papillomatosis in the post-human papillomavirus vaccination era. JAMA Pediatr. 2024;178(12):1372–1373. doi:10.1001/jamapediatrics.2024.4422
17. Jaquet Y, Monnier P, Van Melle G, et al. Complications of different ventilation strategies in endoscopic laryngeal surgery: a 10-year review. Anesthesiology. 2006;104:52–59. doi:10.1097/00000542-200601000-00010
18. Bradley J, Lee GS, Peyton J. Anesthesia for shared airway surgery in children. Paediatr Anaesth. 2020;30:288–295. doi:10.1111/pan.13815
19. Miller AG, Bartle RM, Rehder KJ. High-frequency jet ventilation in neonatal and pediatric subjects: a narrative review. Respir Care. 2021;66:845–856. doi:10.4187/respcare.08691
20. Humphreys S, von Ungern-Sternberg BS, Taverner F, et al. High-flow nasal oxygen for children’s airway surgery to reduce hypoxaemic events: a randomised controlled trial. Lancet Respir Med. 2024;12(7):535–543. doi:10.1016/S2213-2600(24)00115-2
21. Huang L, Dharmawardana N, Badenoch A, et al. A review of the use of transnasal humidified rapid insufflation ventilatory exchange for patients undergoing surgery in the shared airway setting. J Anesth. 2020;34:134–143. doi:10.1007/s00540-019-02697-3
22. Mir F, Patel A, Iqbal R, et al. A randomised controlled trial comparing transnasal humidified rapid insufflation ventilatory exchange (THRIVE) pre-oxygenation with facemask pre-oxygenation in patients undergoing rapid sequence induction of anaesthesia. Anaesthesia. 2017;72:439–443. doi:10.1111/anae.13799
23. Khan NC, Vukkadala N, Saxena A, et al. Safety and utility of transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) for laser laryngeal surgery. Otolaryngol Head Neck Surg. 2023;169:598–605. doi:10.1002/ohn.324
24. Waters E, Kellner M, Milligan P, et al. The use of transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) in one hundred and five upper airway endoscopies. A case series. Clin Otolaryngol. 2019;44:1115–1119. doi:10.1111/coa.13408
25. Hays SR, Deshpande JK.Newly postulated neurodevelopmental risks of pediatric anesthesia: theories that could rock our world. J Urol. 2013;189:1222–1228. doi:10.1016/j.juro.2012.11.090
26. O’Leary JD. Human studies of anesthesia-related neurotoxicity in children: a narrative review of recent additions to the clinical literature. Clin Perinatol. 2019;46:637–645. doi:10.1016/j.clp.2019.08.001
27. Davidson AJ, Sun LS. Clinical evidence for any effect of anesthesia on the developing brain. Anesthesiology. 2018;128:840–853. doi:10.1097/ALN.0000000000001972
28. Jevtovic-Todorovic V. Exposure of developing brain to general anesthesia: what is the animal evidence? Anesthesiology. 2018;128:832–839. doi:10.1097/ALN.0000000000002047
29. Rappaport B, Mellon RD, Simone A, et al. Defining safe use of anesthesia in children. N Engl J Med. 2011;364:1387–1390. doi:10.1056/NEJMp1102155
30. Walkden GJ, Gill H, Davies NM, et al. Early childhood general anesthesia and neurodevelopmental outcomes in the Avon longitudinal study of parents and children birth cohort. Anesthesiology. 2020;133:1007–1020. doi:10.1097/ALN.0000000000003522
31. Xiao A, Feng Y, Yu S, et al. General anesthesia in children and long-term neurodevelopmental deficits: a systematic review. Front Mol Neurosci. 2022;15:972025. doi:10.3389/fnmol.2022.972025
32. Useinovic N, Jevtovic-Todorovic V. Controversies in anesthesia-induced developmental neurotoxicity. Best Pract Res Clin Anaesthesiol. 2023;37:28–39. doi:10.1016/j.bpa.2023.03.004
33. Salaün J-P, Chagnot A, Cachia A, et al. Consequences of general anesthesia in infancy on behavior and brain structure. Anesth Analg. 2023;136:240–250. doi:10.1213/ANE.0000000000006233
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.