")
Back to Journals » International Journal of Nanomedicine » Volume 20
Innervated Biomaterials for Improved Cutaneous Wound Healing: A Review of Recent Advancements and Future Prospects
Authors Zhang B, Zhang K, Liu Q, Zhang J, Chen W, Tang J , Wang C, Guo Z
Received 21 February 2025
Accepted for publication 7 June 2025
Published 19 June 2025 Volume 2025:20 Pages 7829—7849
DOI https://doi.org/10.2147/IJN.S524182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Anderson Oliveira Lobo
BoYang Zhang,1,* KaiYue Zhang,1,* QiuYue Liu,1 JiaLin Zhang,1 WenTao Chen,1 JieTing Tang,1 Chuang Wang,2 ZhenZhao Guo1
1School and Hospital of Stomatology, Guangdong Engineering Research Center of Oral Restoration and Reconstruction, Guangzhou Medical University, Guangzhou, 510180, People’s Republic of China; 2Foshan Stomatology Hospital, School of Medicine, Foshan University, Foshan, 528099, People’s Republic of China
*These authors contributed equally to this work
Correspondence: ZhenZhao Guo, School and Hospital of Stomatology, Guangdong Engineering Research Center of Oral Restoration and Reconstruction, Guangzhou Medical University, Guangzhou, 510180, People’s Republic of China, Email [email protected]
Abstract: Cutaneous wound healing remains a significant clinical challenge, particularly for chronic and large-scale injuries, where functional recovery—especially sensory reinnervation—is often inadequate. Recent advances highlight the pivotal role of innervation in regulating tissue repair through neuropeptide signaling, immunomodulation, and angiogenesis. Despite progress in biomaterial-based therapies, most existing solutions focus on structural repair while neglecting neural regeneration, leading to suboptimal functional outcomes. This review explores emerging biomaterial strategies that integrate neuroregenerative capabilities with wound healing properties, including electroconductive scaffolds for bioelectric stimulation, neurotrophic factor-releasing matrices, and bioengineered constructs. We critically evaluate their mechanisms in promoting axonal regrowth, macrophage polarization, and vascular network formation, while addressing challenges in long-term functional integration. This review outlines the mechanisms of wound healing, existing treatments, and the vital role of nerves in the healing process. It also highlights materials that promote skin neuralization in cutaneous wound healing, aiming to inspire further research into these materials and the underlying mechanisms involved. By bridging the gap between neural and cutaneous regeneration, this work provides a roadmap for developing next-generation wound therapies that restore both structural integrity and sensory function. Future directions emphasize the need for standardized neuroregenerative assessment criteria and clinically translatable designs.
Keywords: cutaneous wound, innervation, neuro regenerative materials
Introduction
The skin is the largest organ in the human body and performs functions such as mechanical protection, immune regulation, fluid regulation, temperature regulation, and sensing external stimuli.1,2 Treating large and chronic wounds caused by accidents or diseases on any part of the body remains a challenge. Autografts and allografts are common in clinics, but they have issues like re-traumatization, infection risk, immune rejection, and limited availability.3 Various materials have been developed to address these issues with anti-infection, inflammation modulation, and angiogenesis-promoting effects.4–7 These innovations, ranging from natural polymer-based systems to synthetic nanocomposites, have been shown to improve wound closure rates compared to traditional treatments.8–11 Nonetheless, most of these studies overlook the recovery of the sensory function of the skin. Incomplete sensory recovery, chronic neuropathic pain, and itching are frequent in healed wounds and have a significant impact on the quality of life of patients.12
Emerging evidence suggests that innervation is one of the master regulators of skin repair. Sensory neurons and Schwann cells coordinate healing through mechanisms such as neuropeptide release and neurotrophic factor signaling.13 Injury receptors regulate macrophage polarization through the IL-10/TGF-β pathway, whereas autonomic fibers regulate perfusion through VEGF-dependent angiogenesis.14,15 Critically, denervated wounds exhibited delayed healing and reduced tensile strength, confirming that nerves are active participants in tissue regeneration rather than passive bystanders.16 Therefore, to create ideal materials for treating skin wounds, we need to emphasize the role that nerves play in the healing process as well as the restoration of perceptual function after healing.
Recently, a series of materials exhibited both tissue-induction activity and neural induction activity that had been explored for innervated skin regeneration. These materials can be categorized according to functional mechanism and material type as biomaterials-enabled electrical stimulation, scaffolds as carriers of biological molecules, metal-organic frameworks, silicate-based bioceramics, and innervated engineered constructs. However, few reviews have focused on the role of materials that promote cutaneous wound regeneration through nerve action. As the important role played by nerves in wound healing is gradually being elucidated and related materials research continues to make progress, a systematic summary of the applications of innervated biomaterials in skin wound treatment is timely and necessary.
This review aims to provide an overview of current approaches for treating and repairing cutaneous wounds through material-based therapies. It highlights various materials that promote skin nerve reinnervation and enhance cutaneous wound healing by facilitating nerve regeneration. The review summarizes and discusses the latest research advancements in this field. It is hoped that this review will inspire further development of materials that support neuroregeneration in cutaneous wound healing.
Cutaneous Wound Healing
Skin wound healing is a complex process of overlapping yet coordinated cellular and molecular events that repair tissue damage and restore function through interactions among various cell types and systems (Figure 1).17 Cutaneous wound healing is conventionally divided into four overlapping stages: hemostasis, inflammation, proliferation, and dermal remodeling.18,19 The hemostasis phase involves vasoconstriction, activation of the intrinsic coagulation cascade leading to clot formation, and subsequent scab development. These processes collectively prevent hemorrhage, protect against microbial infiltration, and provide a microenvironment rich in immune cells and cytokines.20,21 The inflammatory phase typically begins within minutes to hours after injury. The key inflammatory cells include neutrophils, macrophages, and monocytes, which work together to lay the foundation for the subsequent wound-healing process.22,23 The proliferative phase involves the migration and proliferation of fibroblasts, keratinocytes, and endothelial cells alongside extracellular matrix components. Together, these processes form granulation tissue, restore the epithelial layer, and repair tissue.24,25 The remodeling phase of cutaneous wound healing, lasting weeks to years, determines wound healing quality. It involves tissue reorganization, contraction, collagen maturation, and the transition from type III to type I collagen.26,27
 |
Figure 1 Cutaneous wound healing and current treatment methods. Created in BioRender. SZ. (2025) https://BioRender.com/q5d0dl2. |
Most cutaneous wounds heal naturally without external intervention. However, deep wounds, large wounds, severe burns, and chronic wounds often require medical treatment to ensure proper healing and restore function. Deep cutaneous wounds, or those that extend into the dermis, are difficult to heal and are more likely to result in scarring. Studies suggest that this situation is related to a threshold for wound depth, which is associated with the effects of epidermal‐dermal interactions.28,29 In addition, large-area cutaneous wounds may also require medical intervention in some cases. Large-area cutaneous wounds require extensive angiogenesis and tissue repair, making complete regeneration difficult. The activation of inflammation and the enhancement of fibrosis are the main obstacles.30 Similarly, large-area cutaneous wounds are also more prone to infection, which makes wound healing more difficult. In addition, the difficulty in healing large-area burns is due not only to the risk of infection but also to an abnormal inflammatory response. Severe burns initiate an uncontrollable inflammatory process, causing excessive inflammation that hinders healing and induces a hypermetabolic state.31 Chronic cutaneous wounds constitute another type of wound that necessitates medical intervention. A chronic wound is defined as a break in the skin that lasts for a long time (>6 weeks) or recurs frequently.32 In recent years, it has become widely accepted that the presence and persistence of wound infection are the primary causes of chronic wound development.33 The microenvironment of the wound is of critical significance to the success or failure of cutaneous wound healing. Chronic wounds are frequently associated with substantial inflammatory stimuli, such as bacterial colonization, necrotic tissue, foreign bodies, and localized tissue hypoxia.34 This infection may trigger abnormal inflammation. Research indicates that excessive inflammatory responses play a key role in wound pathology. Such persistent inflammation damages tissue repeatedly, creating a cycle of chronic inflammation that drives chronic wound formation.
Large and chronic wounds, which are difficult to heal naturally, often necessitate grafts or supplementary materials to support recovery. As the gold standard for treating large areas of skin loss or chronic wounds, autologous skin grafting has a lower risk of rejection and better healing outcomes. However autologous skin grafting has drawbacks, including the need for incisions to obtain graft material, long culture times, donor site morbidity, nerve damage, and the risk of infection.35 Using dressing materials to treat chronic wounds is also a popular area of research. Traditional dressings are mainly used for early hemostasis, as well as for cleaning and drying wounds. However, the performance of traditional dressings is also less than ideal.36 Their fibers tend to adhere to granulation tissue, causing pain when the dressing is removed, disrupting newly formed tissue, and delaying healing. The inflammatory phase of wound healing is often stalled in chronic wounds. The wound should be clean, have a healthy base of granulation tissue, and be free of infection to optimize cutaneous wound healing. The choice of dressing should be such that the wound is neither too moist nor too dry, and the dressing should maintain moisture in the wound.37 Factors typically considered in the design of an ideal wound dressing include hemostatic activity to stop bleeding, prevention of microbial infection, effective absorption of wound exudate, ease of sterilization, and promotion of cutaneous wound healing. The dressing should also be gas-permeable, easy to use, biodegradable, and non-toxic.38
In addition, various modern dressings for wound repair have been developed and studied. Nowadays, the types of dressings used for wound repair include hydrogels, hydrocolloids, foams, and semipermeable films.39 The main types of these dressings are natural materials, synthetic polymer materials, biological dressings and skin substitutes, and tissue-engineered skin (TES). First, natural materials are a hot topic in skin wound healing research and clinical applications, mainly including chitosan, cellulose, collagen, and hyaluronic acid. Natural macromolecular compounds offer excellent biosafety and degradability with strong physicochemical properties that promote cell growth and differentiation, regulate the wound microenvironment, and are cost-effective for wound healing and tissue repair applications.40 In addition, studies have shown that many synthetic polymer materials and composite materials are also used in skin wound repair, such as polyvinyl alcohol, polyethylene glycol, and gelatin methacrylate acid. Moreover, biological dressings and skin substitutes are prominent research areas. Current studies focus on synthesizing and modifying biocompatible materials.41 These materials, often derived from biopolymers such as collagen and gelatin, are engineered to enhance cutaneous wound healing by leveraging the beneficial properties of these biopolymers. Another area of research for skin repair materials is the use of TES. Bioengineered artificial skin substitutes may be able to overcome graft rejection and provide local delivery of mesenchymal stem cells (MSCs) to reduce inflammation and speed up the healing process.42 In addition, these substitutes can facilitate the delivery of various biomolecules and cells to promote wound repair.43,44 Furthermore, bioactive dressings can also facilitate targeted drug delivery (such as antimicrobials, anti-inflammatories, growth factors, and other bioactive substances) to specific tissues or organs.39 In the treatment of cutaneous wounds, bioactive materials can release factors that promote skin regeneration and interact with receptors in the skin, thereby enhancing wound healing. In addition to materials such as polylactic-co-glycolic acid, polyvinylpyrrolidone, and hydrogels, nanomaterials have also gradually been applied in controlled and targeted drug delivery due to their excellent antimicrobial properties.45,46 In addition, sustained delivery of growth factors, siRNA delivery, microRNA targeting, and stem cell therapy are new potential interventions for wound healing.47 Although significant progress has been made in these areas, the current therapeutic outcomes remain suboptimal, possibly owing to the neglect of the important role of neurogenesis in cutaneous healing.
Neural Repair in Cutaneous Wound Healing and Its Functions
The skin is densely innervated by the peripheral nervous system, including afferent somatosensory and efferent autonomic components. The somatosensory system, composed of neurons in the dorsal root and trigeminal ganglia whose axons form connections between peripheral tissues and the central nervous system, detects external stimuli and transmits this sensory information. The autonomic nervous system, comprising the sympathetic and parasympathetic divisions, controls involuntary physiological functions. Its serial organization involves preganglionic neurons from the central nervous system synapsing with postganglionic neurons in the sympathetic ganglia (near the spinal cord) or parasympathetic ganglia (close to target organs).35 The skin is densely populated with sensory nerves, categorized by diameter and conduction velocity into Aβ, Aδ, and C fibers, ranging from the largest and fastest to the smallest and slowest. These fibers enable the skin to perceive various sensations.48–52
The process of nerve regeneration in cutaneous wound healing involves the coordinated action of various factors and cells.53–55 Remodeling of regenerating nerve fibers and alterations in nerve fiber density have been observed during cutaneous wound healing.56 However, the underlying mechanisms of nerve regeneration remain unclear. Nerve regeneration is a crucial aspect of cutaneous wound healing and plays a pivotal role in regulating the process. During cutaneous wound healing, nerves, blood vessels, and the immune system interact in a triangular relationship. Nerves can directly regulate cutaneous wound healing by conducting electrical signals or by releasing relevant neurotransmitters, neuropeptides, and other substances. They can also influence cutaneous wound healing by modulating related blood vessels and the immune system (Figure 2).
 |
Figure 2 The role of nerves in cutaneous wound healing. Created in BioRender. SZ. (2025) https://BioRender.com/2h4o3hd. |
Nerves or Nerve-Associated Mediators Directly Regulate Cutaneous Wound Healing
Nerves are critical to the regulation of skin functions. First, the regulation of various stem cells in the skin is under the influence of nerves. Capsaicin-induced denervation hinders the expulsion of stem cell progenitors from hair follicles, which is associated with stronger epidermal activation. These may explain the prolonged healing time in denervated skin. Thus, during cutaneous wound healing, sensory innervation might contribute to the regulation of the physiological functions of hair follicle stem cells.16 Moreover, Chéré et al discovered that dorsal root ganglia and neuro mediators promote fibroblast and keratinocyte proliferation while modulating the collagen type I/type III expression ratio, shifting it toward collagen I, thereby enhancing cutaneous wound healing and restoring its original strength.57 Additionally, tissue-resident stem cells located within the skin basement membrane exhibit significant regional heterogeneity, characterized by unique anatomical structures, transcriptional profiles, and diverse markers, while sensory innervation is crucial for establishing their diverse molecular characteristics and lineage potentials.58 During acute wound healing, the release of pain mediators facilitates the initiation and progression of the inflammatory phase, while also promoting the migration of various cells and collagen production, thereby accelerating wound healing.59 These studies demonstrate that nerves play a crucial regulatory role in skin homeostasis and post-traumatic repair, with specific mechanisms related to the actions of nerve cells and associated neurotrophic factors.
Nerves and nerve-related cells can directly regulate the healing of cutaneous wounds. Neurons contribute to the regulation of collagen formation and alignment in the skin. Through interactions with fibroblasts, they influence fibroblast differentiation into myofibroblasts and modulate collagen dynamics.60 Schwann cells (SCs) are essential for myelination and nerve repair in cutaneous wounds. They promote fibroblast generation and myofibroblast differentiation via TGF-β signaling. Additionally, glial cells support repair through paracrine signaling, influencing ECM remodeling, angiogenesis, and immune cell chemotaxis, all of which are crucial for wound healing.61
Neurotransmitters, neuropeptides, neurotrophic factors, and related neuroactive substances contribute to the regulation of cutaneous wound healing. Vasoactive intestinal peptide (VIP), calcitonin gene-related peptide (CGRP), neurotrophic factors such as nerve growth factor (NGF) and brain-derived neurotrophic factor, and neurotrophins are reported to enhance fibroblast functions under in vitro conditions, in skin explants, and in vivo studies of wound healing.62 CGRP has been demonstrated to facilitate cutaneous wound healing.13 CGRP and endothelin’s receptor, Calcrl, is expressed in dermal basal layer stem cells in a nerve fiber-dependent manner, which highlights a significant interaction between neuronal components and the epidermis.63 In an innervated skin model, human CGRP significantly enhanced keratinocyte proliferation and epidermal thickness, indicating its crucial role in regulating epidermal morphogenesis, while substance P (SP) had a minimal effect.64 Additionally, CGRP promotes the production and release of mature and immature NGF in cultured human keratinocytes, indicating its role in regulating cell survival during wound healing.65 Besides CGRP, VIP and NH-2 VIP derivatives promote human keratinocyte proliferation and migration through a cAMP-dependent signaling pathway.61 NGF also plays a regulatory role in cutaneous wound healing. NGF regulates cutaneous wound healing by exerting various biological effects through its receptors, such as stimulating keratinocyte proliferation, inducing wound contraction and extracellular matrix remodeling, and accelerating wound closure.66 NGF promotes dose-dependent keratinocyte proliferation and enhances their migration at the wound margins. Additionally, keratinocytes secrete active NGF, establishing an autocrine regulatory mechanism.55 Furthermore, NGF induces myofibroblast differentiation and collagen synthesis through the NGFR-F-actin-MRTF-A signaling pathway, facilitating tissue contraction and matrix reorganization.67 Other studies indicate that the use of NGF-incorporated collagen as a localized treatment accelerates excision wound recovery.68 SP promotes neurite extension, increases vascular permeability and dilation, drives new blood vessel formation, and supports endothelial cell differentiation and growth. Moreover, it enhances the proliferation of human and murine keratinocytes through NGF release, acting through both direct and indirect mechanisms.13 SP has a significant promoting effect on skin healing.69 SP and neurokinin A have been shown to directly upregulate NGF mRNA expression and promote the secretion of bioactive NGF in human and mouse keratinocytes. Neurokinin A further amplifies NGF expression and release in both in vitro and in vivo models, contributing to the formation of a positive feedback mechanism.70 The delay in cutaneous wound closure caused by morphine is attributed to the suppression of SP and neurokinin A release at the wound site, a process associated with decreased NK-1R expression.71 Besides, SP influences collagen breakdown in wounds by enhancing matrix metalloproteinase-2 (MMP-2) function within fibroblasts, thereby participating in the process of cutaneous wound healing.72 Neurotrophin-3, a critical “epi heliotropin” in the human epidermis, functions through both paracrine and autocrine mechanisms, playing a key role in maintaining skin homeostasis and facilitating cutaneous wound healing.13 In addition, 5-hydroxytryptamine significantly contributes to promoting cutaneous wound healing. The role of neuro-related factors, however, may differ depending on wound conditions. For instance, extensive research highlights the role of SP in impaired cutaneous wound healing in diabetic individuals, whereas CGRP appears to exert no significant effect on this process.73
Sensory neurons contribute significantly to cutaneous wound healing, although their role is not indispensable, even in the absence of the immune system.69 However, innervation can make the cutaneous wound healing process optimal, improve the quality of healing, and restore more skin functions.
Nerves Promote Cutaneous Wound Healing by Neuro-Immune Regulation
Inflammation is crucial for normal cutaneous wound healing, with nerves modulating the inflammatory response to impact the healing process. Cutaneous nerve fibers engage with the immune system by releasing neurotransmitters, which bind to specific receptors on skin target cells, including mast cells, macrophages, neutrophils, and dendritic cells. These interactions affect various processes, both physiological and pathological, involving cellular behavior, immunity, and leukocyte recruitment, ultimately promoting cutaneous wound healing.74 Transient receptor potential vanilloid 1 (+) and voltage-gated sodium channel nav1.8-positive nociceptors (+) nociceptors modulate the IL-23/IL-17 pathway and regulate skin immune responses by interacting with dendritic cells.75 CGRP modulates neutrophils and macrophages via receptor activity-modifying protein 1, inhibiting recruitment, promoting cell death, enhancing phagocytosis, and polarizing macrophages for tissue repair through thrombospondin-1 release and autocrine/paracrine effects.76 SP facilitates the synthesis and release of pro-inflammatory cytokines (IL-1, IL-6, TGF-α) by keratinocytes, stimulates mast cell degranulation and TNF-α release, enhances IL-8 release from endothelial cells, and increases the production of cytokines in leukocyte subpopulations, with many effects reliant on the nitric oxide pathway, which is vital for effective cutaneous wound healing and repair.13 Acetylcholine acts as an immune modulator, inhibiting macrophages via cholinergic anti-inflammatory pathways. Several nicotinic acetylcholine receptor (nAChR) agonists have been developed to treat subcutaneous inflammation, as nAChRs on macrophages influence immune regulation and inflammatory processes, while keratinocytes produce non-neuronal acetylcholine.49 Another study demonstrates that non-peptidergic Gα-inhibiting protein interacting protein-positive skin sensory neurons regulate immunity during tissue repair by producing TAFA4, which enhances IL-10 production in dermal macrophages, supports the survival of TIM4+ macrophages, and inhibits inflammatory macrophage amplification, ultimately promoting cutaneous wound healing.15
Nerves Promote Cutaneous Wound Healing by Enhancing Angiogenesis
Angiogenesis is vital for the regeneration of new tissue in wound beds and is a key factor in the wound healing process. First, the arrangement of blood vessels is related to nerves. A study reveals that neurovascular alignment depends on the G protein-coupled receptor signaling pathway involving the neurogenic ligand Cxcl12 and its receptor Cxcr4, with genetic inactivation of this pathway disrupting neurovascular alignment and abolishing angiogenesis. In vitro experiments further demonstrate that Cxcl12 recruits blood vessels to nerves, while VEGF-A facilitates arterial differentiation.14 Another study revealed that VEGF is essential for sensory neurons or SCs to induce arterial marker expression in isolated embryonic endothelial cells. This indicates that peripheral nerves serve as a blueprint for the organotypic organization of vascular branching and arterial development in the skin through localized VEGF secretion. Neuro-related substances can also directly regulate the formation of blood vessels. For example, NGF modulates VEGF expression via the PI3K/mTOR signaling pathway in human HaCaT keratinocytes.77 NGF stimulates VEGF production through TrkA receptors in endothelial cells. It enhances endothelial cell invasion and cord formation by upregulating matrix MMP-2 and the activating protein-2 transcription factor via the PI3K/Akt pathway, thereby promoting angiogenesis.78 CGRP promotes angiogenesis and prolongs vasodilation in cutaneous wound healing, enhancing dermal endothelial cell proliferation and acting as a potent vasodilator with lasting effects across species, including humans.13 Interestingly, some neuro-related substances have a dual role in blood vessel formation, such as dopamine. This difference is likely related to the type of dopamine receptor that is activated in target cells.79 In summary, neurovascular interactions play a critical role in angiogenesis and wound healing, with nerves providing templates for vascular branching and neuro-related substances, such as VEGF, NGF, and CGRP, regulating blood vessel formation through diverse signaling pathways. These findings highlight the complex interplay between the nervous and vascular systems in tissue regeneration.
Innervated Biomaterials for Improved Cutaneous Wound Healing
Large and chronic wounds often struggle to heal on their own due to continuous inflammatory stimulation. Currently, the repair of nerves and their role in facilitating wound healing are frequently overlooked.1 However, as previously discussed, nerve repair in the skin may promote cutaneous wound healing remarkably by regulating inflammation or vascularization.80 Consequently, an increasing number of researchers are focusing on wound healing materials that can promote neurogenesis, including materials capable of generating electrical stimulation, metal-organic frameworks (MOFs), scaffolds as carriers of biological molecules, innervated engineered construct, and silicate-based bioceramics (Figure 3). Table 1 summarized representative innervated materials and their effects on cutaneous wound healing.
 |
Figure 3 Innervated biomaterials for improved cutaneous wound healing. Created in BioRender. ab, i. (2025) https://BioRender.com/vgw2cpt. |
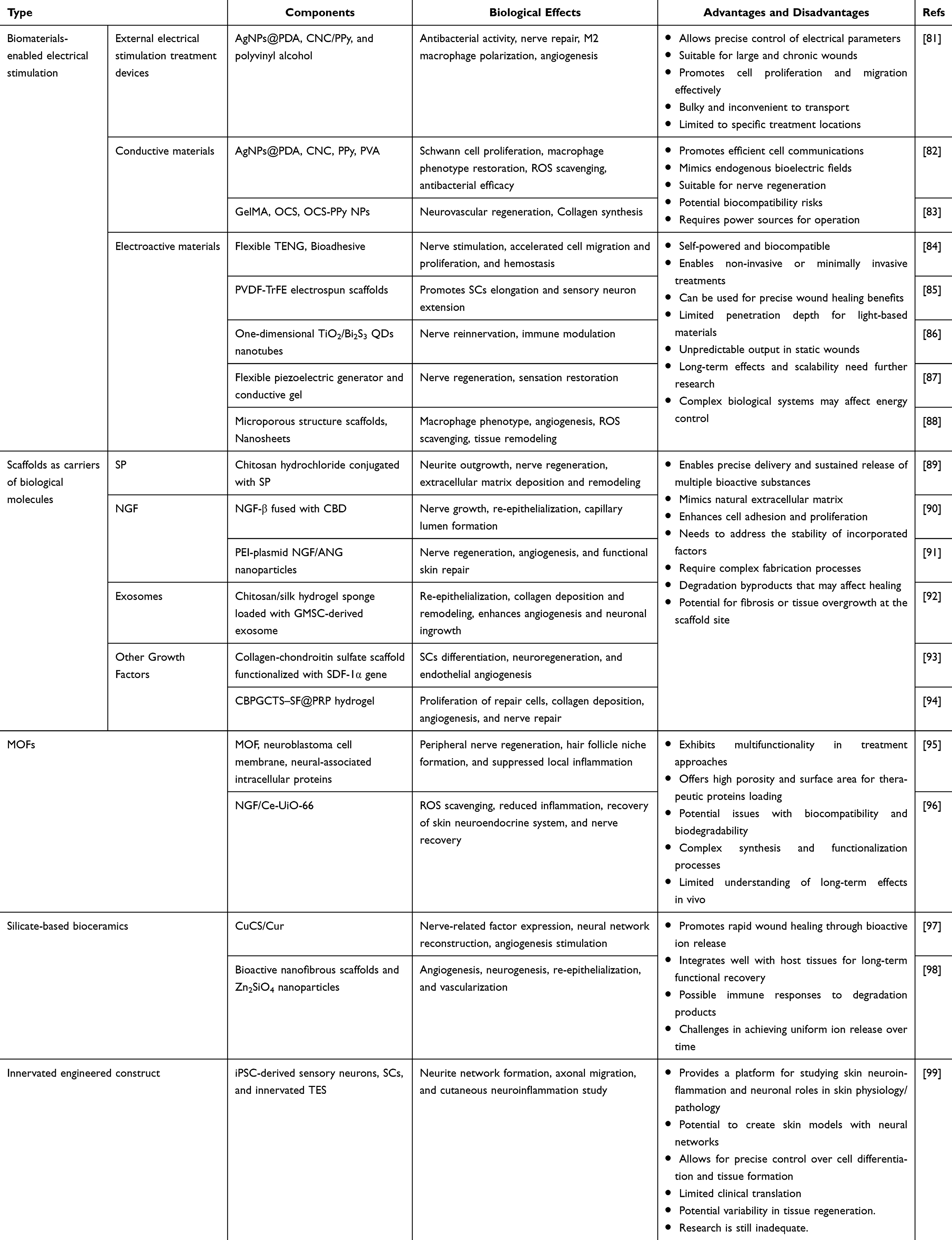 |
Table 1 A Summary of Innervated Materials and Their Effects on Cutaneous Wound Healing |
Biomaterials-Enabled Electrical Stimulation for Cutaneous Wound Healing
Biomaterials-enabled electrical stimulation is beneficial to wound healing and can stimulate neurite extension and nerve formation.100,101 There are different types of biomaterials-enabled electrical stimulation such as conductive materials and electroactive materials. A wealth of researchers have reported the use of biomaterials-enabled electrical stimulation as a potential wound-healing material in both preclinical and clinical cases, especially in large and chronic wounds.84,102,103
External Electrical Stimulation Treatment Devices
During cutaneous wound healing, researchers demonstrated that external electrical stimulation can expedite the proliferation and migration of fibroblasts, augment nerve regeneration, and thereby enhance functional restoration post-injury. A conductive hydrogel combined with external electrical stimulation was developed by Guan et al, which significantly promotes neuroregeneration in diabetic wounds.81 However, external electrical stimulation treatment devices are bulky and inconvenient to transport, limiting treatment to specific locations like hospitals.
Conductive Materials
Numerous studies have adequately demonstrated that hydrogels that can conduct electricity help cells send signals to each other more easily, which speeds up the healing of large and chronic wounds and injuries to peripheral nerves.104,105 The combination of conductive polymers with hydrogels enables the development of conductive hydrogels that possess tissue-matched conductivity and mechanical properties, making them suitable for nerve regeneration. Bi et al developed a versatile hydrogel that combines antioxidant properties, photothermal therapy, curcumin release, and electrical conductivity. This hydrogel releases curcumin that can enhance the migration and proliferation of Sc, and also facilitate myelin regeneration in diabetic wounds by regulating SOX10 and myelin-forming genes, thereby promoting the overall repair process.82 In another study, conductive hydrogels boost neuronal and vascular regeneration by elevating intracellular Ca2+ and stimulating PI3K/AKT and MEK/ERK pathways (Figure 4F and H). They accelerated full-thickness diabetic wound healing within 14 days via neuronal and vascular regeneration and collagen deposition (Figure 4G).83
 |
Figure 4 (A) Hierarchical architecture of PRG-G-C and its stimulation in endogenous stem cells based neural restoration and sensory function recovery. (B) Immunofluorescence staining of nestin expression (green fluorescence) by bone mesenchymal stem cells cultured with PBS (Blank). Scale bars indicate 10 μm. (C) for 7 days and semi-quantification of nestin-positive cells. (D) Semi-quantification of nestin and β3-tubulin expression rates in the healed skins. (E) Immunofluorescence staining of nestin (green) and β3-tubulin (red) in healed skins on day 15 post-treatment. Scale bars indicate 50 μm. Statistical significance is indicated as * p < 0.05, **p < 0.01, ***p < 0.001 Blank group. #p < 0.05, ##p < 0.05, ###p < 0.001 versus G-Exos group. & p < 0.05, && p < 0.01, &&& p < 0.001 versus PVDF group. Adapted from Biomaterials, volume: 283. Tan MH, Xu XH, Yuan TJ, et al. Self-powered smart patch promotes skin nerve regeneration and sensation restoration by delivering biological-electrical signals in program. 121413. Copyright 2022, with permission from Elsevier.87(F) Schematic illustration of the mechanism of conductive hydrogel promoting neuroregeneration. (G) Photographs of skin wounds at days 0, 3, 7, and 14 in different groups. (H) Quantitative analysis of protein expression (n = 3) (* p < 0.05, ** p < 0.01, *** p < 0.001). Adapted from Fan L, Xiao C, Guan P, et al. Extracellular matrix-based conductive interpenetrating network hydrogels with enhanced neurovascular regeneration properties for diabetic wounds repair. Adv Healthc Mater. 2022;11(1):e2101556. © 2021 Wiley-VCH GmbH.83 |
Conductive materials could mimic endogenous bioelectric fields and showed significant wound healing potential, highlighting their suitability for wound treatment. Nevertheless, the incorporation of conductive components (carbon nanotubes, polypyrrole et al) might have potential biocompatibility risks. Meanwhile, the conductive materials require power sources, which is inconvenient. To overcome these limitations, electroactive materials such as photoelectric, triboelectric, and piezoelectric materials have been engineered to facilitate electric stimulation, offering a more convenient and accessible treatment option.
Electroactive Materials
Firstly, triboelectric nanogenerators are recognized for their biocompatibility, miniaturization, and ability to produce stable electrical outputs, making them ideal for energy harvesting medical healthcare. Qian et al designed a bioadhesive triboelectric nanogenerator that possesses the potential to be utilized not only in wound treatment but also for nerve regeneration.84
Secondly, low-intensity pulsed ultrasound-based electrical stimulation, a non-invasive approach, offers precise wound healing benefits. In the study by Westphal et al, ultrasound was used to enhance SC elongation and sensory neuron extension in skin-tissue engineering.85 In another study, Wang et al employed ultrasound to rapidly eliminate 94.2% of Staphylococcus aureus and utilized piezoelectric microfibers to promote wound healing and promote nerve vascularization.103 Besides, a recent study demonstrated that low-frequency ultrasound-driven MXene/PVDF films can enhance axonal regeneration and promote M2 macrophage polarization in diabetic wounds, accelerating healing and restoring sensory function through neuro-immune regulation.106
Subsequently, the photoelectric effect is utilized to precisely treat wounds and promote nerve repair by adjusting the intensity and frequency of light to act on specific areas.107,108 Qiao et al proposed one-dimensional TiO2/Bi2S3 QDs nanotubes with high photoelectric properties excited by visible red light.86 This photoelectric therapy offers an advantageous electrophysiological milieu conducive to neuronal differentiation and axon growth. In the TBCHA+L phototherapy group, a significant expression of β-3 tubulin and α-smooth muscle actin markers was observed on day 14, indicative of nerve fiber regeneration and the re-establishment of the epithelial neural network.
In addition, Tan et al developed a self-powered patch using a flexible piezoelectric generator and conductive gel (Figure 4A), which can foster skin repair and nerve regeneration by delivering biological-electrical signals in the program.87 This advancement was attributed to the synergistic interplay between neuro-directed glial cell-derived exosomes and electrical stimulation (Figure 4B and C). The combination of these elements fostered an environment conducive to the substantial promotion of MSC differentiation towards a neuronal lineage and the generation of new neurons (Figure 4D and E).
Finally, leveraging intrinsic bioelectric fields offers a self-sustaining approach for chronic wound management. Liu et al developed an MXene-integrated decellularized scaffold that established a neuro-immunoregulatory microenvironment through endogenous ion flow.88 It achieving 96.9% diabetic wound closure within 14 days via macrophage reprogramming, ROS clearance, and angiogenesis activation. This endogenous electrotherapy bypasses the need for external devices while facilitating neural-immune crosstalk, presenting strong translational potential for electrosensitive tissue regeneration through autonomous bioenergy utilization.
These innovative biomaterials and therapeutic approaches leverage physical stimuli like triboelectricity, ultrasound, photoelectric effects, piezoelectricity, and intrinsic bioelectric fields to enhance wound healing and nerve regeneration. Key features include biocompatibility, precise electrical signal generation or delivery, and sometimes self-powering capabilities, enabling non-invasive or minimally invasive treatments. But visible/NlR light cannot reach deep wounds, which might have limited photoelectric effect. Charge generation depends on unpredictable wound movement, which might resulted in unreliable output in static wounds. Furthermore, these methods promote tissue repair by influencing cell behavior, further research is necessary to fully understand long-term effects, improve scalability and cost-effectiveness, and achieve precise energy control within complex biological systems.
Scaffolds as Carriers of Biological Molecules
Bioactive molecules such as neurotrophins, and growth factors within the neural tissue exert their effects through complex signaling pathways, which in turn enhances the nutritive supply and repair processes at the wound site.80,109 However, due to the transient half-life of these molecules, many studies have employed scaffolds to deliver these factors effectively.110,111 Scaffolds provide not only structural reinforcement at the wound site but also serve as vehicles for sustained delivery of growth factors and cytokines, thus creating a conducive atmosphere for tissue regeneration. Neurotransmitters, neuropeptides, neurotrophic factors, and other neuro-related substances that could play regulatory roles in cutaneous wound healing were fabricated into scaffolds to achieve enhanced cutaneous wound healing.
Substance P (SP)
Accumulating evidence has supported that SP stands as a prominent neuropeptide among those secreted by nerve fibers in reaction to damage, which accelerates wound healing by regulating the inflammatory phase.112 Whereas the application of SP is significantly hindered by its low stability and susceptibility to oxidative degradation during manufacturing, transit, and preservation processes. Therefore, the incorporation of SP into scaffold materials, such as hydrogels, can enhance their bioavailability.111,113 A multifunctional SP-conjugated chitosan hydrochloride hydrogel was designed by Li et al and used for the loading and release of SP.89 In vivo, the material significantly enhances vascularization, extracellular matrix deposition and remodeling, and nerve regeneration, thus facilitating effective healing of full-thickness skin defects. Moreover, the hydrogel formulated with 10−5 M SP facilitated 98% wound closure within 16 days, whereas the comparator sample failed to achieve complete re-epithelialization during the same period.114
Nerve Growth Factor (NGF)
NGF plays a crucial role in the differentiation, regeneration, and repair of both the central and peripheral nervous systems. Consequently, numerous researchers have developed materials loaded with NGF, aiming to facilitate neural repair and regeneration. Furthermore, researchers have discovered that NGF may accelerate wound healing by promoting angiogenesis, stimulating keratinocyte proliferation, and enhancing neuroregeneration.115
So far, several works have been done about the application of NGF for angiogenesis to the wound. Keykhaee et al have fabricated a multifunctional hydrogel combining alginate, gum arabic, and specially designed mesoporous silica nanoparticles loaded with NGF, forming SiNGF.116 The hydrogel, AG-Car/SiNGF, sustains NGF release over 21 days, ideal for diabetic wound healing. Histological results show it improves re-epithelialization, collagen deposition, and neovascularization, with enhanced TGF-β expression and nerve neurofilament. This composite system holds promise for treating large and chronic wounds. Furthermore, with peripheral nerve growth, scaffolds impregnated with collagen-binding human NGF-beta effectively expedite ulcer repair.90 Recent advancements in NGF-based therapies demonstrate enhanced neurovascular regeneration through biomaterial innovation. Yang et al developed a dual-gene activated dermal scaffold delivering NGF/ANG via PEI-chimeric plasmid nanoparticles in PLGA/collagen-chitosan scaffolds. This system achieved 3.9× greater nerve density and complete wound healing within 10 days by synergistically upregulating β3-tubulin/PGP9.5 neural markers and CD31/α-SMA vascular markers. Notably, it restored physiological sensory thresholds through Piezo2-mediated mechanotransduction, outperforming single-factor systems by addressing neurovascular interdependence - a critical advancement for functional tissue regeneration.91
Exosomes
Exosomes secreted by cells are vesicles with a variety of functions. Research has shown that somatic stem cells can promote wound healing and skin regeneration by facilitating the proliferation and migration of epithelial cells, enhancing angiogenesis, and aiding in neural repair.117–121
In the study of Shi et al, they extract exosomes originating from gingival mesenchymal stem cells (GMSCs) and incorporate these GMSC-derived exosomes into the hydrogel for the purpose of administering them directly to wounds.92 In diabetic rats, GMSCs embedded within the hydrogel secrete NGF, thereby enhancing neuronal growth and regeneration, and increasing neural density. Simultaneously, GMSCs foster angiogenesis and collagen regeneration, collectively contributing to accelerated chronic and large wound healing.
Other Growth Factors
Among growth factors, VEGF plays a pivotal role in promoting angiogenesis and is one of the extensively studied stimulatory factors in the wound healing process.122 Recent research underscores the importance of considering the angiogenic potential of nervous system cells, such as Schwann cells (SCs).93 By genetically activating SCs on scaffolds with stromal cell-derived factor-1α (SDF-1α), SCs overexpressing SDF-1α subsequently produce higher levels of VEGF, enhancing endothelial angiogenesis and promoting a repair phenotype in SCs. These findings suggest that neuronal system cells can facilitate comprehensive vascular formation and regeneration through the expression of angiogenic factor genes, thereby accelerating the healing of large and slow-healing wounds.
Besides, platelet-rich plasma hydrogel (PRP gel), made from fibrin glue mixed with PRP and thrombin/calcium, treats diabetic wounds. Extracted from whole blood, it contains platelets and bioactive molecules like exosomes, NGF, and Platelet-derived growth factor, aiding wound healing.123–125 Due to PRP gel’s instability and rapid degradation, its efficacy in treating chronic diabetic wounds was limited. Therefore, Qian et al developed a self-healing, injectable hydrogel (CBPGCTS-SF@PRP) combining chitosan, silk fibroin, and PRP. This hydrogel protects PRP from degradation, enabling sustained release and enhancing MSC chemotaxis.94 It accelerated collagen deposition, angiogenesis, and nerve regeneration in skin defect rat models, enhancing wound healing.
Metal-Organic Frameworks (MOFs)
MOFs have emerged as promising tools in promoting wound healing through their versatility.126,127 In the context of deep burns, a neuro-inspired biomimetic microreactor, termed Neuro-MOF, has been designed to emulate the outer membrane of neuroblastoma cells that enables immune evasion, as well as neural-related intracellular proteins.95 This microreactor, mounted on a MOF and coated with a membrane of neuroblastoma cells, effectively triggers the release of therapeutic proteins upon near-infrared light excitation. These proteins help compensate for enduring skin neurological damage, initiating peripheral nerve regeneration and hair follicle niche formation. In mouse models, Neuro-MOF demonstrated significant functional skin regeneration effects, especially in the restoration of sensation and hair follicle neogenesis, highlighting its potential in large and chronic wound therapy targeting sensory nerves.
Moreover, MOFs have also shown efficacy in treating diabetic ulcers, where peripheral neuropathy and extreme ROS due to diabetes hinder wound healing.96 A nanoscale MOF loaded with nerve growth factor (NGF/Ce-UiO-66 or NGF/CU) has been created to address this issue. The Ce-UiO-66 component acts as an oxidation Inhibitor, scavenging ROS and reducing inflammation, while NGF aids in nerve regeneration in the skin. Experiments confirmed the efficacy of NGF/CU in promoting diabetic ulcers healing in vivo and in vitro. RNA sequencing analysis further showed that NGF/CU improves wound healing by suppressing the NF-κB signaling route and restoring the neuroendocrine system of the skin.
In conclusion, MOFs exhibit neuro-inspired potential in wound healing through targeted delivery of therapeutic proteins and antioxidants, enhancing nerve regeneration and reducing inflammation.128 These findings open new avenues for the treatment of burns and diabetic ulcers, offering promising strategies for neural regulation in wound management.
Silicate-Based Bioceramics
Silicate-based bioceramics represent a promising category of materials for wound dressings, owing to their ability to expedite wound healing processes through the modulation of endothelial cells, dermal fibroblasts, macrophages, and epidermal cells. Notably, silicate-based bioceramics can undergo further functional enhancement through specific structural designs or the incorporation of functional components.129–131
Zhang et al developed a wound dressing, created through electrospinning, comprised of calcium silicate enriched with copper and Cur, referred to as CuCS/Cur.97 The Cu2+-Cur chelate exhibited exceptional neuro-inductive properties, facilitating the transformation of neuronal cells derived from hair follicles into fully functional neural networks. Furthermore, the Cu2+-Cur chelate demonstrated remarkable angiogenic potential and provided abundant nutrition for wound regeneration, hair follicle regeneration, and neural regeneration.
In another research, the treatment of severe burn injuries, was addressed through the use of Zn2SiO4 nanoparticles-incorporated bioactive nanofibrous scaffolds.98 The Zn2SiO4 nanoparticles, synthesized via a facile hydrothermal way and incorporated into the scaffolds, exhibited excellent angiogenic and neurogenic activities in vitro. Results further demonstrated that these scaffolds, through Zn2SiO4 nanoparticles releasing bioactive Zn and Si ions, promoted wound healing with skin regeneration, nerve repair, and vascularization in vivo.
Innervated Engineered Construct
Engineered construct is composed of an artificial extracellular matrix as a scaffold, and cells are mounted on it. Through the incorporation of cytokines and stem cells, tissue-engineered skin(TES) facilitates optimal tissue repair and regeneration of full-thickness wounds. Studies showed that in vitro, SCs significantly enhance sensory neuronal outgrowth in 3D dermal models, doubling that of controls. SCs spontaneously co-localize with neuronal outgrowth and form myelin sheaths, observed via transmission electron microscopy. In vivo, reconstructed skin enriched with SCs, transplanted onto nude mice, increased neuronal migration by 1.8-fold and 1.7-fold at 60 and 90 days, respectively. These SC-enriched reconstructed skin samples exhibited similar current perception thresholds for large myelinated Aβ sensory fibers to normal skin, unlike controls. This suggests that SCs in engineered skin enhance neuronal migration, promote myelination, and restore neural function in vivo.132
To further investigate, researchers developed neuronal TES models initially using murine sensory neurons. To create fully human TES, they differentiated induced pluripotent stem cells (iPSCs) from human skin fibroblasts. After 19 days, differentiated sensory neurons expressed markers like BRN3A and β3-tubulin, and responded to stimuli by releasing neuropeptides. SCs, essential for neuronal function, were also differentiated from human iPSCs. In TES models with additional month-long culture, iPSC-derived neurons formed neuronal networks spanning the entire TES to the epidermis, only when combined with mouse or iPSC-derived SCs. This human TES model is significant for studying skin neuroinflammation.99
In conclusion, by utilizing SCs and iPSC-derived neurons, researchers can create skin models with neural networks, crucial for studying skin neuroinflammation and neuronal roles in skin physiology/pathology. With further research, neuronal TES could emerge as a novel treatment for large and chronic wound healing.
Conclusions and Future Prospects
Innervated biomaterials serve as an effective method capable of improving cutaneous wound healing.111,128 This review briefly demonstrates the course of cutaneous wound healing and the materials commonly applied for cutaneous wound healing in medical practice. By emphasizing the function of nerve repair in wound healing, it highlights the potential role of innervated materials in wound healing. This review summarizes the design of innervated wound healing biomaterials by researchers in the areas of electrical stimulation, biomolecule delivery, MOFs, silicate-based bioceramics, and engineered constructs.
Despite promising preclinical results in select innervated biomaterial systems for accelerating cutaneous wound repair, significant translational barriers persist, including unresolved biocompatibility concerns, inconsistent neuromodulatory efficacy, and limited mechanistic understanding of neuro-immuno-regenerative crosstalk, which collectively underscore the imperative for systematic multidisciplinary investigations to advance these technologies toward clinical viability. Future research can be conducted in the following aspects:
1. The development of cutaneous wound healing materials with desirable therapeutic effects requires an in-depth understanding of several important issues. Current research mainly centers on materials that can simultaneously promote neurogenesis and wound healing. However, there is insufficient evidence to show how these materials facilitate the wound-healing process through neuronal pathways. It is important to gain a deeper understanding of the specific mechanisms by which nerves promote cutaneous wound healing. Therefore, future studies are required to provide more detailed proof of how innervated biomaterials accelerate wound healing. Meanwhile, although regeneration of cutaneous sensory nerves is essential to restore sensory function, regeneration of tactile and pain nerves also contributes to enhancing the quality of patients’ lives. The precise mechanism by which tactile and pain nerves contribute to the improvement of wound healing remains unknown.
2. While innervated biomaterials hold promise for enhancing cutaneous wound healing by mimicking neural-electrical microenvironments, their biosafety remains a critical concern. Current biocompatibility evaluations often focus on short-term in vitro cytocompatibility and basic inflammatory responses in vivo. However, comprehensive assessment of their long-term biosafety in physiological environments is still lacking. Beyond localized inflammation and histological analysis of major organs, the fate, distribution, and degradation behavior of these materials—particularly conductive or piezoelectric components (eg, polymers or ceramics used to enable neural interfacing)—must be rigorously evaluated. For instance, piezoelectric additives or electroactive polymers, though beneficial for electrical stimulation, may raise concerns about chronic toxicity, bioaccumulation, or adverse immune reactions if degradation products persist in tissues. Advanced characterization tools, such as high-throughput screening and real-time biodistribution tracking, could provide multidimensional insights into systemic biosafety. Additionally, the interplay between material properties (eg, stiffness, electrical cues) and neural tissue remodeling requires careful optimization to avoid unintended neurotoxicity or dysregulated regeneration. Addressing these challenges will bridge the gap between innovative design and clinical translation, ensuring that innervated biomaterials achieve both therapeutic efficacy and long-term safety in wound healing applications.
3. Despite their potential to revolutionize cutaneous wound healing, innervated biomaterials face significant barriers in clinical translation. A primary challenge lies in the complex synthesis and scalability of components (eg, piezoelectric ceramics or conductive polymers) often integrated into these systems. Developing low-cost, eco-friendly synthesis strategies to ensure reproducible physicochemical properties is critical for regulatory approval and commercialization. From a translational perspective, most studies on innervated biomaterials are confined to small animal models (mice, rats), which fail to replicate human anatomical complexity, biomechanical stresses, or chronic wound healing dynamics. Transitioning to large-animal preclinical trials (eg, porcine models) is essential to validate safety, dosing, and functional efficacy under clinically relevant conditions, including surgical implantation and long-term biosafety monitoring.
In conclusion, innervated biomaterials represent a transformative frontier in cutaneous wound healing, offering unprecedented potential to restore both structural integrity and sensory function by bridging neural regeneration with tissue repair. While innervated biomaterial systems have demonstrated remarkable preclinical success in enhancing neuro-integrated healing, critical challenges persist in elucidating mechanistic neuro-immuno-regenerative crosstalk, ensuring long-term biosafety, and achieving scalable clinical translation. Future efforts must prioritize mechanistic exploration, eco-friendly synthesis, and rigorous preclinical evaluation in large-animal models to address regulatory and translational barriers. By uniting materials science, neurobiology, and clinical expertise, this emerging field can unlock innovative therapies that not only accelerate wound closure but also restore sensory fidelity, ultimately improving patient outcomes. We envision that this review will inspire collaborative advancements, driving innervated biomaterials from conceptual innovation to clinical reality in regenerative medicine.
Abbreviations
TES, Tissue-engineered skin; MSCs, Mesenchymal stem cells; SCs, Schwann cells; VIP, Vasoactive intestinal peptide; NGF, Nerve growth factor; CGRP, Calcitonin gene-related peptide; SP, Substance P; MMP-2, Metalloproteinase-2; nAChR, Micotinic acetylcholine receptor; MOFs, Metal-organic frameworks; Cur, Curcumin; GMSCs, Mesenchymal stem cells; SDF-1α, Stromal cell-derived factor-1α; PRP gel, Platelet-rich plasma hydrogel; iPSCs, Induced pluripotent stem cells.
Acknowledgments
This work was supported by the National Natural Science Foundation of China [Grant Nos. 31900946] and Guangdong Basic and Applied Basic Research Foundation [Grant Nos. 2022A1515110181] and University-Industry Collaborative Education Program [Grant Nos. 230805309315401] and Science and Technology Planning Projects of Guangzhou City [Grant Nos. 202201020203]. Graphical Abstract was created in BioRender. SZ. (2025) https ://BioRender.com/pk.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weng T, Wu P, Zhang W, et al. Regeneration of skin appendages and nerves: current status and further challenges. J Transl Med. 2020;18(1):53. doi:10.1186/s12967-020-02248-5
2. Sun BK, Siprashvili Z, Khavari PA. Advances in skin grafting and treatment of cutaneous wounds. Science. 2014;346(6212):941–945. doi:10.1126/science.1253836
3. Greenhalgh DG. Management of burns. N Engl J Med. 2019;380(24):2349–2359. doi:10.1056/NEJMra1807442
4. Zhao Y, Yi B, Hu J, et al. Double cross-linked biomimetic hyaluronic acid-based hydrogels with thermo-stimulated self-contraction and tissue adhesiveness for accelerating post-wound closure and wound healing. Adv Funct Mater. 2023;33(26):2300710. doi:10.1002/adfm.202300710
5. Shang S, Zhuang K, Chen J, Zhang M, Jiang S, Li W. A bioactive composite hydrogel dressing that promotes healing of both acute and chronic diabetic skin wounds. Bioact Mater. 2024;34:298–310. doi:10.1016/j.bioactmat.2023.12.026
6. Cheng S, Wang H, Pan X, et al. Dendritic hydrogels with robust inherent antibacterial properties for promoting bacteria-infected wound healing. ACS Appl Mater Interfaces. 2022;14(9):11144–11155. doi:10.1021/acsami.1c25014
7. Qi X, Xiang Y, Li Y, et al. An ATP-activated spatiotemporally controlled hydrogel prodrug system for treating multidrug-resistant bacteria-infected pressure ulcers. Bioact Mater. 2025;45:301–321. doi:10.1016/j.bioactmat.2024.11.029
8. Xie H, Wang Z, Wang R, Chen Q, Yu A, Self-Healing LA. Injectable hydrogel dressing for monitoring and therapy of diabetic wound. Adv Funct Mater. 2024;34(36):2401209. doi:10.1002/adfm.202401209
9. He L, Xing S, Zhang W, et al. Multifunctional dynamic chitosan-guar gum nanocomposite hydrogels in infection and diabetic wound healing. Carbohydr Polym. 2025;354:123316. doi:10.1016/j.carbpol.2025.123316
10. Khan NU, Chengfeng X, Jiang MQ, et al. Obstructed vein delivery of ceftriaxone via poly (vinyl-pyrrolidone)-iodine-chitosan nanofibers for the management of diabetic foot infections and burn wounds. Int J Biol Macromol. 2024;277:134166. doi:10.1016/j.ijbiomac.2024.134166
11. Song J, Razzaq A, Khan NU, Iqbal H, Ni J. Chitosan/poly (3-hydroxy butyric acid-co-3-hydroxy valeric acid) electrospun nanofibers with cephradine for superficial incisional skin wound infection management. Int J Biol Macromol. 2023;250:126229. doi:10.1016/j.ijbiomac.2023.126229
12. Saffari TM, Schüttenhelm BN, Van Neck Johan W, Holstege JC. Nerve reinnervation and itch behavior in a rat burn wound model. Wound Repair Regen. 2018;26(1):16–26. doi:10.1111/wrr.12620
13. Chéret J, Lebonvallet N, Carré J, Misery L, Le Gall‐Ianotto C. Role of neuropeptides, neurotrophins, and neurohormones in skin wound healing. Wound Repair Regen. 2013;21(6):772–788. doi:10.1111/wrr.12101
14. Li W, Kohara H, Uchida Y, et al. Peripheral nerve-derived CXCL12 and VEGF-A regulate the patterning of arterial vessel branching in developing limb skin. Dev Cell. 2013;24(4):359–371. doi:10.1016/j.devcel.2013.01.009
15. Hoeffel G, Debroas G, Roger A, et al. Sensory neuron-derived TAFA4 promotes macrophage tissue repair functions. Nature. 2021;594(7861):94–99. doi:10.1038/s41586-021-03563-7
16. Martínez-Martínez E, Galván-Hernández CI, Toscano-Márquez B, Gutiérrez-Ospina G. Modulatory role of sensory innervation on hair follicle stem cell progeny during wound healing of the rat skin. PLoS One. 2012;7(5):e36421. doi:10.1371/journal.pone.0036421
17. Geer DJ, Swartz DD, Andreadis ST. In vivo model of wound healing based on transplanted tissue-engineered skin. Tissue Eng. 2004;10(7–8):1006–1017. doi:10.1089/ten.2004.10.1006
18. Broughton G, Janis JE, Attinger CE. Wound healing: an overview. Plast Reconstr Surg. 2006;117(SUPPLEMENT):1e–S–32e–S. doi:10.1097/01.prs.0000222562.60260.f9
19. Baron JM, Glatz M, Proksch E. Optimal support of wound healing: new insights. Dermatology. 2020;236(6):593–600. doi:10.1159/000505291
20. Wang PH, Huang BS, Horng HC, Yeh CC, Chen YJ. Wound healing. J Chin Med Assoc. 2018;81(2):94–101. doi:10.1016/j.jcma.2017.11.002
21. Wilkinson HN, Hardman MJ. Wound healing: cellular mechanisms and pathological outcomes. Open Biol. 2020;10(9):200223. doi:10.1098/rsob.200223
22. Chen L, DiPietro LA. Toll-like receptor function in acute wounds. Adv Wound Care. 2017;6(10):344–355. doi:10.1089/wound.2017.0734
23. Koh TJ, DiPietro LA. Inflammation and wound healing: the role of the macrophage. Expert Rev Mol Med. 2011;13:e23. doi:10.1017/S1462399411001943
24. Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. 2008;453(7193):314–321. doi:10.1038/nature07039
25. Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA. Myofibroblasts and mechano-regulation of connective tissue remodelling. Nat Rev Mol Cell Biol. 2002;3(5):349–363. doi:10.1038/nrm809
26. Talbott HE, Mascharak S, Griffin M, Wan DC, Longaker MT. Wound healing, fibroblast heterogeneity, and fibrosis. Cell Stem Cell. 2022;29(8):1161–1180. doi:10.1016/j.stem.2022.07.006
27. Witte MB, Barbul A. General principles of wound healing. Surg Clin North Am. 1997;77(3):509–528. doi:10.1016/S0039-6109(05)70566-1
28. Wang Y, Guerrero‐Juarez CF, Qiu Y, et al. A multiscale hybrid mathematical model of epidermal‐dermal interactions during skin wound healing. Exp Dermatol. 2019;28(4):493–502. doi:10.1111/exd.13909
29. Dunkin CSJ, Pleat JM, Gillespie PH, Tyler MPH, Roberts AHN, McGrouther DA. Scarring occurs at a critical depth of skin injury: precise measurement in a graduated dermal scratch in human volunteers. Plast Reconstr Surg. 2007;119(6):1722–1732. doi:10.1097/01.prs.0000258829.07399.f0
30. Reinke JM, Sorg H. Wound repair and regeneration. Eur Surg Res. 2012;49(1):35–43. doi:10.1159/000339613
31. Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primer. 2020;6(1):11. doi:10.1038/s41572-020-0145-5
32. Fonder MA, Lazarus GS, Cowan DA, Aronson-Cook B, Kohli AR, Mamelak AJ. Treating the chronic wound: a practical approach to the care of nonhealing wounds and wound care dressings. J Am Acad Dermatol. 2008;58(2):185–206. doi:10.1016/j.jaad.2007.08.048
33. Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017;34(3):599–610. doi:10.1007/s12325-017-0478-y
34. Greaves NS, Iqbal SA, Baguneid M, Bayat A. The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regeneration. 2013;21(2):194–210. doi:10.1111/wrr.12029
35. Ständer S, Schmelz M. Skin Innervation. J Invest Dermatol. 2024;144(8):1716–1723. doi:10.1016/j.jid.2023.10.047
36. Nguyen HM, Ngoc Le TT, Nguyen AT, Thien Le HN, Pham TT. Biomedical materials for wound dressing: recent advances and applications. RSC Adv. 2023;13(8):5509–5528. doi:10.1039/d2ra07673j
37. Powers JG, Higham C, Broussard K, Phillips TJ. Wound healing and treating wounds. J Am Acad Dermatol. 2016;74(4):607–625. doi:10.1016/j.jaad.2015.08.070
38. Chittleborough CR, Grant JF, Phillips PJ, Taylor AW. The increasing prevalence of diabetes in South Australia: the relationship with population ageing and obesity. Public Health. 2007;121(2):92–99. doi:10.1016/j.puhe.2006.09.017
39. Lagoa T, Queiroga MC, Martins L. An overview of wound dressing materials. Pharmaceuticals. 2024;17(9):1110. doi:10.3390/ph17091110
40. Yang Y, Li B, Wang M, Pan S, Wang Y, Gu J. Effect of natural polymer materials on skin healing based on internal wound microenvironment: a review. Front Chem. 2023;11:1257915. doi:10.3389/fchem.2023.1257915
41. Sheikholeslam M, Wright MEE, Jeschke MG, Amini‐Nik S. Biomaterials for skin substitutes. Adv Healthc Mater. 2018;7(5):1700897. doi:10.1002/adhm.201700897
42. Przekora A. A concise review on tissue engineered artificial skin grafts for chronic wound treatment: can we reconstruct functional skin tissue in vitro? Cells. 2020;9(7):1622. doi:10.3390/cells9071622
43. Kalirajan C, Palanisamy T. Bioengineered hybrid collagen scaffold tethered with silver‐catechin nanocomposite modulates angiogenesis and TGF‐ β toward scarless healing in chronic deep second degree infected burns. Adv Healthc Mater. 2020;9(12):2000247. doi:10.1002/adhm.202000247
44. Zhao H, Li Z, Wang Y, et al. Bioengineered MSC-derived exosomes in skin wound repair and regeneration. Front Cell Dev Biol. 2023;11:1029671. doi:10.3389/fcell.2023.1029671
45. Kalashnikova I, Das S, Seal S. Nanomaterials for wound healing: scope and advancement. Nanomed. 2015;10(16):2593–2612. doi:10.2217/nnm.15.82
46. Wang W, Lu KJ, Yu CH, Huang QL, Du YZ. Nano-drug delivery systems in wound treatment and skin regeneration. J Nanobiotechnology. 2019;17(1):82. doi:10.1186/s12951-019-0514-y
47. Dreifke MB, Jayasuriya AA, Jayasuriya AC. Current wound healing procedures and potential care. Mater Sci Eng C. 2015;48:651–662. doi:10.1016/j.msec.2014.12.068
48. Blais M, Parenteau-Bareil R, Cadau S, Berthod F. Concise review: tissue-engineered skin and nerve regeneration in burn treatment. Stem Cells Transl Med. 2013;2(7):545–551. doi:10.5966/sctm.2012-0181
49. Vidal yucha SE, Tamamoto KA, Kaplan DL. The importance of the neuro‐immuno‐cutaneous system on human skin equivalent design. Cell Prolif. 2019;52(6):e12677. doi:10.1111/cpr.12677
50. Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009;139(2):267–284. doi:10.1016/j.cell.2009.09.028
51. Zhang S, Sumpter TL, Kaplan DH. Neuron‒mast cell cross-talk in the skin. J Invest Dermatol. 2022;142(3):841–848. doi:10.1016/j.jid.2021.10.006
52. Abraira VE, Ginty DD. The sensory neurons of touch. Neuron. 2013;79(4):618–639. doi:10.1016/j.neuron.2013.07.051
53. de S Aarão TL, de Sousa JR, Falcão ASC, Falcão LFM, Quaresma JAS. Nerve growth factor and pathogenesis of leprosy: review and update. Front Immunol. 2018;9:939. doi:10.3389/fimmu.2018.00939
54. Cattin AL, Burden JJ, Van Emmenis L, et al. Macrophage-induced blood vessels guide Schwann cell-mediated regeneration of peripheral nerves. Cell. 2015;162(5):1127–1139. doi:10.1016/j.cell.2015.07.021
55. G El Baassiri M, Dosh L, Haidar H, et al. Nerve growth factor and burn wound healing: update of molecular interactions with skin cells. Burns J Int Soc Burn Inj. 2023;49(5):989–1002. doi:10.1016/j.burns.2022.11.001
56. Girard D, Laverdet B, Buhé V, et al. Biotechnological management of skin burn injuries: challenges and perspectives in wound healing and sensory recovery. Tissue Eng Part B Rev. 2017;23(1):59–82. doi:10.1089/ten.teb.2016.0195
57. Chéret J, Lebonvallet N, Buhé V, Carre JL, Misery L, Le Gall-Ianotto C. Influence of sensory neuropeptides on human cutaneous wound healing process. J Dermatol Sci. 2014;74(3):193–203. doi:10.1016/j.jdermsci.2014.02.001
58. Garrison SR, Dietrich A, Stucky CL. TRPC1 contributes to light-touch sensation and mechanical responses in low-threshold cutaneous sensory neurons. J Neurophysiol. 2012;107(3):913–922. doi:10.1152/jn.00658.2011
59. Widgerow AD, Kalaria S. Pain mediators and wound healing—Establishing the connection. Burns. 2012;38(7):951–959. doi:10.1016/j.burns.2012.05.024
60. Fujiwara T, Kubo T, Kanazawa S, et al. Direct contact of fibroblasts with neuronal processes promotes differentiation to myofibroblasts and induces contraction of collagen matrix in vitro. Wound Repair Regen. 2013;21(4):588–594. doi:10.1111/wrr.12059
61. Parfejevs V, Debbache J, Shakhova O, et al. Injury-activated glial cells promote wound healing of the adult skin in mice. Nat Commun. 2018;9(1):236. doi:10.1038/s41467-017-01488-2
62. Lebonvallet N, Laverdet B, Misery L, Desmoulière A, Girard D. New insights into the roles of myofibroblasts and innervation during skin healing and innovative therapies to improve scar innervation. Exp Dermatol. 2018;27(9):950–958. doi:10.1111/exd.13681
63. Gong Y, Wei JP, Wang TH, Zhong HB, Liao XH. Calcitonin gene-related peptide receptor Calcrl is enriched in hair follicles stem cells and differentially expressed in interfollicular epidermis in murine skin. NeuroReport. 2020;31(11):814–818. doi:10.1097/WNR.0000000000001497
64. Roggenkamp D, Köpnick S, Stäb F, Wenck H, Schmelz M, Neufang G. Epidermal nerve fibers modulate keratinocyte growth via neuropeptide signaling in an innervated skin model. J Invest Dermatol. 2013;133(6):1620–1628. doi:10.1038/jid.2012.464
65. Dallos A, Kiss M, Polyánka H, Dobozy A, Kemény L, Husz S. Effects of the neuropeptides substance P, calcitonin gene-related peptide, vasoactive intestinal polypeptide and galanin on the production of nerve growth factor and inflammatory cytokines in cultured human keratinocytes. Neuropeptides. 2006;40(4):251–263. doi:10.1016/j.npep.2006.06.002
66. Liu Z, Wu H, Huang S. Role of NGF and its receptors in wound healing (Review). Exp Ther Med. 2021;21(6):599. doi:10.3892/etm.2021.10031
67. Ashrafi M, Baguneid M, Bayat A. The role of neuromediators and innervation in cutaneous wound healing. Acta Derm Venereol. 2016;96(5):587–594. doi:10.2340/00015555-2321
68. Nithya M, Suguna L, Rose C. The effect of nerve growth factor on the early responses during the process of wound healing. Biochim Biophys Acta Gen Subj. 2003;1620(1–3):25–31. doi:10.1016/S0304-4165(02)00501-9
69. Blais M, Mottier L, Germain MA, Bellenfant S, Cadau S, Berthod F. Sensory neurons accelerate skin reepithelialization via substance P in an innervated tissue-engineered wound healing model. Tissue Eng Part A. 2014;20(15–16):2180–2188. doi:10.1089/ten.tea.2013.0535
70. Burbach GJ, Kim KH, Zivony AS, et al. The neurosensory tachykinins substance P and neurokinin a directly induce keratinocyte nerve growth factor. J Invest Dermatol. 2001;117(5):1075–1082. doi:10.1046/j.0022-202x.2001.01498.x
71. Rook JM, Hasan W, McCarson KE. Morphine-induced early delays in wound closure: involvement of sensory neuropeptides and modification of neurokinin receptor expression. Biochem Pharmacol. 2009;77(11):1747–1755. doi:10.1016/j.bcp.2009.03.003
72. Hecker-Kia A, Kolkenbrock H, Orgel D, Zimmermann B, Sparmann M, Ulbrich N. Substance P induces the secretion of gelatinase a from human synovial fibroblasts. Clin Chem Lab Med. 1997;35(9). doi:10.1515/cclm.1997.35.9.655
73. Relationship between cutaneous glycometabolic disorders and cutaneous neuropathy in diabetic rats.
74. Steinhoff M, Ständer S, Seeliger S, Ansel JC, Schmelz M, Luger T. Modern aspects of cutaneous neurogenic inflammation. Arch Dermatol. 2003;139(11). doi:10.1001/archderm.139.11.1479
75. Riol-Blanco L, Ordovas-Montanes J, Perro M, et al. Nociceptive sensory neurons drive interleukin-23-mediated psoriasiform skin inflammation. Nature. 2014;510(7503):157–161. doi:10.1038/nature13199
76. Lu YZ, Nayer B, Singh SK, et al. CGRP sensory neurons promote tissue healing via neutrophils and macrophages. Nature. 2024;628(8008):604–611. doi:10.1038/s41586-024-07237-y
77. Zhang J, Ma WY. Nerve growth factor regulates the expression of vascular endothelial growth factor in human HaCaT keratinocytes via PI3K/mTOR pathway. Genet Mol Res. 2014;13(4):9324–9335. doi:10.4238/2014.January.24.14
78. Park MJ, Kwak HJ, Lee HC, et al. Nerve growth factor induces endothelial cell invasion and cord formation by promoting matrix metalloproteinase-2 expression through the phosphatidylinositol 3-Kinase/Akt signaling pathway and AP-2 transcription factor. J Biol Chem. 2007;282(42):30485–30496. doi:10.1074/jbc.M701081200
79. Vaughn A, Davis M, Sivamani R, Isseroff R. A concise review of the conflicting roles of dopamine-1 versus dopamine-2 receptors in wound healing. Molecules. 2017;23(1):50. doi:10.3390/molecules23010050
80. Kiya K, Kubo T. Neurovascular interactions in skin wound healing. Neurochem Int. 2019;125:144–150. doi:10.1016/j.neuint.2019.02.014
81. Guan L, Ou X, Wang Z, et al. Electrical stimulation-based conductive hydrogel for immunoregulation, neuroregeneration and rapid angiogenesis in diabetic wound repair. Sci China Mater. 2023;66(3):1237–1248. doi:10.1007/s40843-022-2242-y
82. Bi S, He C, Zhou Y, Liu R, Chen C. Versatile conductive hydrogel orchestrating neuro–immune microenvironment for rapid diabetic wound healing through peripheral nerve regeneration. Biomaterials. 2025;314:122841. doi:10.1016/j.biomaterials.2024.122841
83. Fan L, Xiao C, Guan P, et al. Extracellular matrix-based conductive interpenetrating network hydrogels with enhanced neurovascular regeneration properties for diabetic wounds repair. Adv Healthc Mater. 2022;11(1):e2101556. doi:10.1002/adhm.202101556
84. Meng X, Xiao X, Jeon S, et al. An ultrasound-driven bioadhesive triboelectric nanogenerator for instant wound sealing and electrically accelerated healing in emergencies. Adv Mater Deerfield Beach Fla. 2023;35(12):e2209054. doi:10.1002/adma.202209054
85. Westphal JA, Bryan AE, Krutko M, Esfandiari L, Schutte SC, Harris GM. Innervation of an ultrasound-mediated PVDF-TrFE scaffold for skin-tissue engineering. Biomim Basel Switz. 2023;9(1):2. doi:10.3390/biomimetics9010002
86. Qiao Z, Ding J, Yang M, et al. Red-light-excited TiO2/Bi2S3 heterojunction nanotubes and photoelectric hydrogels mediate epidermal-neural network reconstruction in deep burns. Acta Biomater. 2024;184:114–126. doi:10.1016/j.actbio.2024.06.028
87. Tan MH, Xu XH, Yuan TJ, et al. Self-powered smart patch promotes skin nerve regeneration and sensation restoration by delivering biological-electrical signals in program. Biomaterials. 2022;283:121413. doi:10.1016/j.biomaterials.2022.121413
88. Liu Z, Wang T, Zhao J, et al. Endogenous electric field-driven neuro-immuno-regulatory scaffold for effective diabetic wound healing. Bioact Mater. 2025;47:266–282. doi:10.1016/j.bioactmat.2025.01.024
89. Li H, Li M, Liu P, et al. A multifunctional substance P-conjugated chitosan hydrochloride hydrogel accelerates full-thickness wound healing by enhancing synchronized vascularization, extracellular matrix deposition, and nerve regeneration. Biomater Sci. 2021;9(11):4199–4210. doi:10.1039/d1bm00357g
90. Sun W, Lin H, Chen B, et al. Collagen scaffolds loaded with collagen-binding NGF-beta accelerate ulcer healing. J Biomed Mater Res A. 2010;92(3):887–895. doi:10.1002/jbm.a.32445
91. Yang M, He F, Cai C, et al. Nerve growth factor/angiogenin gene activated dermal bioscaffold for nerve repair in cutaneous wound healing. NANO Res. 2025;18(3):94907193. doi:10.26599/NR.2025.94907193
92. Shi Q, Qian Z, Liu D, et al. GMSC-derived exosomes combined with a Chitosan/Silk hydrogel sponge accelerates wound healing in a diabetic rat skin defect model. Front Physiol. 2017;8:904. doi:10.3389/fphys.2017.00904
93. Laiva AL, O’Brien FJ, Keogh MB. SDF-1α gene-activated collagen scaffold drives functional differentiation of human Schwann cells for wound healing applications. Biotechnol Bioeng. 2021;118(2):725–736. doi:10.1002/bit.27601
94. Qian Z, Wang H, Bai Y, et al. Improving chronic diabetic wound healing through an injectable and self-healing hydrogel with platelet-rich plasma release. ACS Appl Mater Interfaces. 2020;12(50):55659–55674. doi:10.1021/acsami.0c17142
95. Zhao Q, Wang J, Qu S, et al. Neuro-inspired biomimetic microreactor for sensory recovery and hair follicle neogenesis under skin burns. ACS Nano. 2023;17(22):23115–23131. doi:10.1021/acsnano.3c09107
96. Ji X, Zhou J, Zhou Z, et al. Recovering skin-nerve interaction by nanoscale metal-organic framework for diabetic ulcers healing. Bioact Mater. 2024;42:112–123. doi:10.1016/j.bioactmat.2024.08.024
97. Zhang Z, Chang D, Zeng Z, et al. CuCS/Cur composite wound dressings promote neuralized skin regeneration by rebuilding the nerve cell “factory” in deep skin burns. Mater Today Bio. 2024;26. doi:10.1016/j.mtbio.2024.101075
98. Zhang H, Ma W, Ma H, Qin C, Chen J, Wu C. Spindle-like zinc silicate nanoparticles accelerating innervated and vascularized skin burn wound healing. Adv Healthc Mater. 2022;11(10). doi:10.1002/adhm.202102359
99. Muller Q, Beaudet MJ, De Serres-Bérard T, Bellenfant S, Flacher V, Berthod F. Development of an innervated tissue-engineered skin with human sensory neurons and Schwann cells differentiated from iPS cells. Acta Biomater. 2018;82:93–101. doi:10.1016/j.actbio.2018.10.011
100. Qian Y, Cheng Y, Song J, et al. Mechano-informed biomimetic polymer scaffolds by incorporating self-powered zinc oxide nanogenerators enhance motor recovery and neural function. Small Weinh Bergstr Ger. 2020;16(32):e2000796. doi:10.1002/smll.202000796
101. Qian Y, Xu Y, Yan Z, et al. Boron nitride nanosheets functionalized channel scaffold favors microenvironment rebalance cocktail therapy for piezocatalytic neuronal repair. Nano Energy. 2021;83:105779. doi:10.1016/j.nanoen.2021.105779
102. Fan W, Yang X, Hu X, Huang R, Shi H, Liu G. A novel conductive microtubule hydrogel for electrical stimulation of chronic wounds based on biological electrical wires. J Nanobiotechnology. 2024;22(1):258. doi:10.1186/s12951-024-02524-2
103. Wang X, Sun K, Wang C, et al. Ultrasound-responsive microfibers promoted infected wound healing with neuro-vascularization by segmented sonodynamic therapy and electrical stimulation. Biomaterials. 2025;313:122803. doi:10.1016/j.biomaterials.2024.122803
104. Luo Y, Fan L, Liu C, et al. An injectable, self-healing, electroconductive extracellular matrix-based hydrogel for enhancing tissue repair after traumatic spinal cord injury. Bioact Mater. 2022;7:98–111. doi:10.1016/j.bioactmat.2021.05.039
105. Yu R, Zhang H, Guo B. Conductive biomaterials as bioactive wound dressing for wound healing and skin tissue engineering. Nano-Micro Lett. 2021;14(1):1. doi:10.1007/s40820-021-00751-y
106. Yu C, Hu Y, Zhang X, et al. Low-frequency ultrasound-driven piezoelectric films repair neuro-immune circuits in diabetic wound healing. Chem Eng J. 2025;511:162045. doi:10.1016/j.cej.2025.162045
107. Karatum O, Gwak MJ, Hyun J, et al. Optical neuromodulation at all scales: from nanomaterials to wireless optoelectronics and integrated systems. Chem Soc Rev. 2023;52(10):3326–3352. doi:10.1039/D2CS01020H
108. Fu J, Liu X, Tan L, et al. Photoelectric-responsive extracellular matrix for bone engineering. ACS Nano. 2019;13(11):13581–13594. doi:10.1021/acsnano.9b08115
109. Hao L, Zou Z, Tian H, et al. Novel roles of perivascular nerves on neovascularization. Neurol Sci. 2015;36(3):353–360. doi:10.1007/s10072-014-2016-x
110. Wang X, Wu J, Wang M, et al. Substance P&dimethyloxallyl glycine-loaded carboxymethyl chitosan/gelatin hydrogel for wound healing. J Biomed Mater Res A. 2023;111(3):404–414. doi:10.1002/jbm.a.37475
111. Kim DJ, Jang JH, Jang SS, Lee J. A novel substance P-based hydrogel for increased wound healing efficiency. Mol. 2018;23(9):2215. doi:10.3390/molecules23092215
112. Redkiewicz P. The Regenerative Potential of Substance P. Int J Mol Sci. 2022;23(2):750. doi:10.3390/ijms23020750
113. Diekmann O, Tschesche H. Degradation of kinins, angiotensins and substance P by polymorphonuclear matrix metalloproteinases MMP 8 and MMP 9. Braz J Med Biol Res Rev Bras Pesqui Medicas E Biol. 1994;27(8):1865–1876.
114. Serres-Bérard TD, Becher TB, Braga CB, Ornelas C, Berthod F. Neuropeptide substance P released from a nonswellable laponite-based hydrogel enhances wound healing in a tissue-engineered skin in vitro. ACS Appl Polym Mater. 2020. doi:10.1021/acsapm.0c01034
115. Tuveri M, Generini S, Matucci-Cerinic M, Aloe L. NGF, a useful tool in the treatment of chronic vasculitic ulcers in rheumatoid arthritis. Lancet. 2000;356(9243):1739–1740. doi:10.1016/S0140-6736(00)03212-8
116. Keykhaee M, Rahimifard M, Najafi A, et al. Alginate/gum arabic-based biomimetic hydrogel enriched with immobilized nerve growth factor and carnosine improves diabetic wound regeneration. Carbohydr Polym. 2023;321:121179. doi:10.1016/j.carbpol.2023.121179
117. Zhang J, Guan J, Niu X, et al. Exosomes released from human induced pluripotent stem cells-derived MSCs facilitate cutaneous wound healing by promoting collagen synthesis and angiogenesis. J Transl Med. 2015;13(1):49. doi:10.1186/s12967-015-0417-0
118. Zhu Z, Zhang X, Hao H, et al. Exosomes derived from umbilical cord mesenchymal stem cells treat cutaneous nerve damage and promote wound healing. Front Cell Neurosci. 2022;16:913009. doi:10.3389/fncel.2022.913009
119. Xiong Y, Lin Z, Bu P, et al. A Whole-course-repair system based on neurogenesis-angiogenesis crosstalk and macrophage reprogramming promotes diabetic wound healing. Adv Mater. 2023;35(19):2212300. doi:10.1002/adma.202212300
120. Rani S, Ritter T. The exosome - a naturally secreted nanoparticle and its application to wound healing. Adv Mater. 2016;28(27):5542–5552. doi:10.1002/adma.201504009
121. Kourembanas S. Exosomes: vehicles of intercellular signaling, biomarkers, and vectors of cell therapy. Annu Rev Physiol. 2015;77(Volume 77, 2015):13–27. doi:10.1146/annurev-physiol-021014-071641
122. Johnson KE, Wilgus TA. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv Wound Care. 2014;3(10):647–661. doi:10.1089/wound.2013.0517
123. Picard F, Hersant B, Bosc R, Meningaud JP. The growing evidence for the use of platelet-rich plasma on diabetic chronic wounds: a review and a proposal for a new standard care. Wound Repair Regen. 2015;23(5):638–643. doi:10.1111/wrr.12317
124. Deng W, Boey J, Chen B, et al. Platelet-rich plasma, bilayered acellular matrix grafting and negative pressure wound therapy in diabetic foot infection. J Wound Care. 2016;25(7):393–397. doi:10.12968/jowc.2016.25.7.393
125. Mehta S, Watson JT. Platelet rich concentrate: basic science and current clinical applications. J Orthop Trauma. 2008;22(6):432. doi:10.1097/BOT.0b013e31817e793f
126. Xiong Y, Feng Q, Lu L, et al. Metal–organic frameworks and their composites for chronic wound healing: from bench to bedside. Adv Mater. 2024;36(2):2302587. doi:10.1002/adma.202302587
127. Bigham A, Islami N, Khosravi A, Zarepour A, Iravani S, Zarrabi A. MOFs and MOF-based composites as next-generation materials for wound healing and dressings. Small. 2024;20(30):2311903. doi:10.1002/smll.202311903
128. Yuan T, Tan M, Xu Y, et al. All-in-one smart dressing for simultaneous angiogenesis and neural regeneration. J Nanobiotechnology. 2023;21(1):38. doi:10.1186/s12951-023-01787-5
129. Zhang Z, Dai Q, Zhang Y, et al. Design of a multifunctional biomaterial inspired by ancient Chinese medicine for hair regeneration in burned skin. ACS Appl Mater Interfaces. 2020;12(11):12489–12499. doi:10.1021/acsami.9b22769
130. Zhang Z, Li W, Liu Y, et al. Design of a biofluid-absorbing bioactive sandwich-structured Zn–Si bioceramic composite wound dressing for hair follicle regeneration and skin burn wound healing. Bioact Mater. 2020;6(7):1910–1920. doi:10.1016/j.bioactmat.2020.12.006
131. Fan C, Xu Q, Hao R, et al. Multi-functional wound dressings based on silicate bioactive materials. Biomaterials. 2022;287:121652. doi:10.1016/j.biomaterials.2022.121652
132. Blais M, Grenier M, Berthod F. Improvement of nerve regeneration in tissue-engineered skin enriched with Schwann cells. J Invest Dermatol. 2009;129(12):2895–2900. doi:10.1038/jid.2009.159
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.