")
Back to Journals » Psychology Research and Behavior Management » Volume 18
Intergenerational Transmission of Depressive Symptoms in Chinese Families: The Role of Mothers versus Fathers and Adolescent Perceptual Sensitivity
Authors Sun K, Zhang X, Li P, Cao C
Received 26 January 2025
Accepted for publication 10 June 2025
Published 23 June 2025 Volume 2025:18 Pages 1481—1493
DOI https://doi.org/10.2147/PRBM.S519632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Kexin Sun,1,* Xinting Zhang,2,* Ping Li,1 Cong Cao1
1School of Nursing and Rehabilitation, Shandong University, Jinan, People’s Republic of China; 2Department of Pediatrics, Qilu Hospital of Shandong University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cong Cao, School of Nursing and Rehabilitation, Shandong University, No. 44 West Wenhua Road, Jinan, Shandong Province, 250012, People’s Republic of China, Tel +86-88382268, Email [email protected]
Purpose: Depression is well-known to be transmitted across generations, whereas the focus has often been on mother-child dyads. Little is known about the role of fathers and some inherited temperaments of adolescents, especially in Chinese families. This study is the first to explore the moderated mediation transmission mechanism of depressive symptoms, in which (i) the role of fathers was compared to that of mothers, and (ii) how adolescent perceptual sensitivity worked was particularly elucidated.
Participants and Methods: A total of 738 Chinese adolescents (Mage = 12.80 ± 1.58 years; 47.2% girls) who were companied with one of their primary caregivers (mothers or fathers) were recruited, constituting two subsamples of mother-child (N = 508) versus father-child dyads (N = 230), respectively. Path models and the regions of significance approach were used to analyze the moderated mediation mechanisms.
Results: Mothers and fathers both transmitted depressive symptoms to adolescents via their rejection parenting (indirect effect = 0.14, SE = 0.02, p < 0.001). However, adolescent perceptual sensitivity moderated the second half path of this mediation pathway among mother-child dyads (b = 0.09, SE = 0.04, p = 0.011), but not among father-child dyads (b = − 0.05, SE = 0.06, p = 0.348), and worked in a manner of diathesis-stress. Adolescent sex did not moderate this transmission mechanism (χ2 = 6.52, df = 3, p = 0.089).
Conclusion: These findings suggest similarities and differences in the roles of mothers and fathers in the transmission risk of depressive symptoms in contemporary Chinese families, and highlight a diathesis-stress like moderation effect of adolescent perceptual sensitivity.
Keywords: intergenerational transmission, depressive symptoms, caregiver rejection, perceptual sensitivity, mothers versus fathers
Introduction
Depression can be transmitted across generations, especially from parents to adolescents, and the involved mechanism is an intricate process, which attracts great attention.1–3 Recent evidence proposes a moderated mediation mechanism underlying this transmission risk, ie, the mediation effect of caregiver parenting and the moderation effect of offspring’s traits (see Figure 1).4,5 Adolescent perceptual sensitivity, an individual temperament character, might function as a moderator in a vulnerable (ie, “diathesis-stress”) or plastic (ie, “differential susceptibility”) way towards environmental influences,6 whereas the role of which in this transmission pathway has rarely been investigated. Furthermore, the role of fathers in this mechanism—particularly in Chinese families—remains poorly understood.5,7 Accordingly, this study examined to address these gaps by testing this moderated mediation intergenerational transmission model of depressive symptoms, in which (i) the role of fathers was compared to that of mothers, and (ii) how adolescent perceptual sensitivity worked was particularly elucidated. A better understanding of what facilitates intergenerational transmission of depressive symptoms is needed to inform critical efforts to interrupt such transmission.
 |
Figure 1 Intergenerational transmission of depressive symptoms: A hypothetical moderated mediation model. Notes: The path coefficients of each variable are present in this Figure. The mediation effect of caregiver rejection is a × b; the direct effect from maternal or paternal depressive symptoms to adolescent depressive symptoms is c; the moderation effect of adolescent perceptual sensitivity in the direct path of this transmission model is m1; the moderation effect of adolescent perceptual sensitivity in the first and second half paths of the mediation pathway is m2 and m3, respectively. |
Intergenerational Transmission of Depressive Symptoms from Parents to Adolescents: A Moderated Mediation Model
Depressive symptoms have significant intergenerational transmission underpinnings. A great deal of research has supported the transmission pathway especially from parents to adolescents among various ethnicities or cultures.2,3 For example, adolescents with depressed mothers versus non-depressed mothers are three to four times more likely to develop a major depressive disorder by early adulthood.8 What’s more, in light of the integrative model of the transmission of risk to children of depressed mothers (integrative model), the intergenerational transmission of depressive symptoms involves an underlying moderated mediation mechanism:1 caregiver parenting are important modifiable factors proposed to underpin the intergenerational transmission pathway, and this pathway varies as a function of offspring’s traits or characteristics (eg, offspring’s temperament) (see Figure 1).
The Mediating Role of Parental Rejection
As proposed by the integrative model, caregiver parenting, especially rejection, is considered as a crucial modifiable environmental factor proposed to mediate this intricate intergenerational transmission process.9 According to the five-step, action-control model, depressive status of parents could greatly increase the likelihood that parents exhibit rejection behaviors towards their child through five specific steps, such as reducing attention to offspring’s signals and increasing negative evaluations towards offspring.10 Consistently, the parental acceptance-rejection theory holds that adolescents who perceive themselves to be rejected by parents appear to be more disposed than accepted persons to develop depressive symptoms.11 In line with these theories, the majority of extant evidence has supported this mediating effect of caregiver rejection, despite a few non-significant findings.12,13 For example, among 904 Israeli mothers and their 2- to 6-year-old children, maternal rejection was found to significantly mediate the association between maternal depressive symptoms and children’s behavioral problems.13 Notably, most of the relevant research has focused on the transmission from mothers to adolescents and the involved mediating effect of maternal rejection, whereas the role of fathers has been less investigated, especially in Chinese families.
As well established, different cultural customs and values could shape distinct parental roles in the family.14 Influenced by the traditional culture of “strict father, kind mother”, Chinese mothers are often expected to be affectionate, whereas fathers are expected to be emotional distant.15 Chinese fathers who have more depressed emotions and rejection behaviors seem to deviate less from their social expectations and may have less pronounced adverse impacts on offspring’ mental health than those mothers. Such gender socialization effect may also affect the adolescents.14 Thus, the intergenerational transmission of depression in Chinese families should take parental and adolescent sex into consideration, whereas this remains poorly understood to date.
The Moderating Role of Adolescent Perceptual Sensitivity
Based on the integrative model,1 the direct path and the mediating path of caregiver rejection involved in the transmission model of depression may both vary or be moderated as the function of offspring’s temperament (see Figure 1). Moreover, regarding the specific moderation pattern of temperament, there are two competing hypotheses (see Figure 2): diathesis-stress versus differential susceptibility. The traditional diathesis-stress hypothesis stipulates that individuals with certain “risk” temperament are more vulnerable than others to negative environments and thus develop poorly.16 In contrast, the differential susceptibility proposes an evolutionary perspective, such that individuals vary in their environmental plasticity — individuals with certain “plastic” temperament are not only at risk of developing poorly in adverse environments but also benefit from supportive environments and thus develop well.17
 |
Figure 2 The hypotheses of (a) diathesis-stress and (b) differential susceptibility. Notes: b = better effect or bright side effect, w = worse effect or the dark side effect. The diathesis-stress model includes only worse effect, emphasizing the dual risk of vulnerable factors and adverse environment; the differential-susceptibility model includes both better and worse effect, emphasizing the better effect in enriched environment and the worse effect in adverse environment. |
Under the fierce debate over these two hypotheses, perceptual sensitivity that reflects an ability to detect subtle changes in the environment has been argued recently for its potential as a novel “plastic” temperament maker towards environmental influences.6,18,19 Neural evidence shows that not only neuronal activity in cortex but also interaction with signals from the superior colliculus are related to changes in perceptual sensitivity.19 Meanwhile, high perceptual sensitivity individuals exhibit both high punishment and reward reactivity18 and tend to show tight link with other relatively stable plastic factors, such as respiratory sinus arrhythmia20 and orienting sensitivity.21 Therefore, theoretically, perceptual sensitivity may lie at the root of individual differences in susceptibility to the environment (ie, differential susceptibility).6 An experiment study conducted in school-aged children seems to provide preliminary support for this hypothesis. That is, Weeland et al revealed that, child perceptual sensitivity significantly interacted with positive parenting behavior in predicting children’s motor reactivity (but not affective reactivity) to both happy and angry expression in a “for better and for worse” manner.6 That is, children with high perceptual sensitivity showed not only reduced zygomaticus response to happy and angry expression under low positive parenting, but also heightened response under high positive parenting. Moreover, preliminary evidence suggests that perceptual sensitivity not only serves as a significant moderating factor but also shows association with depression transmission. For example, a study comparing 64 children with familial risk for depression and 40 low-risk children found that boys predisposed to depression may exhibit heightened perceptual sensitivity to detecting subtle sad expressions in faces.22
Nevertheless, to date, perceptual sensitivity temperament has received very little scientific attention, particularly in the key period of adolescence. This period is crucial for the transmission of depression as during which both the severity and prevalence of depression dramatically increase.23 More importantly, it should not lose sight of a novel idea that timing is a vital consideration in examining the differential susceptibility vs diathesis-stress.24,25 Preliminary evidence shows that individual plasticity to environmental influences may be more pronounced during infancy and childhood (ie, plasticity window), but not during adolescence.24,25 This plasticity window may be closely related to the plasticity period of neurobiological systems. For example, during infancy and childhood, the brain experiences rapid growth as neural connections form at remarkable speeds.26 This phase is marked by heightened environmental sensitivity that drives neuroplasticity. However, later in life, neural plasticity becomes more context-dependent, requiring specific conditions to facilitate changes. For instance, as the brain matures into adolescence, the prefrontal cortex undergoes significant reorganization, while the limbic system becomes sluggish to reward cues but vulnerable to negative emotions and signals.26 Accordingly, the extent to which perceptual sensitivity functions as a moderation in a vulnerable (ie, diathesis-stress) or plastic (ie, differential susceptibility) way towards environmental influences, especially during the key period of adolescence warrant investigation, and this will guide how we conduct preventive intervention against the transmission of depression in the families.
Current Study
The current study aimed to investigate an intergenerational transmission mechanism of depressive symptoms from both mothers and fathers to adolescents in Chinese families, where the mediation effect of caregiver rejection and the moderation effect of adolescent perceptual sensitivity were tested (see Figure 1). In particular, using a series of nested path models, the role of fathers was compared to that of mothers, and the moderation of adolescent sex was also tested in an explorative way. Adopting the regions of significance (RoS) analysis, how adolescent perceptual sensitivity worked, in a way of vulnerable (ie, diathesis-stress) or plastic (ie, differential susceptibility) was elucidated. Given controversy evidence that (i) perceptual sensitivity may be a novel, potential “plastic” temperament maker towards environmental influences and (ii) individual’s environmental plasticity may be less pronounced during adolescence, we did not infer direct hypothesis about the “plastic” or “vulnerable” role of adolescent perceptual sensitivity. In light of the Chinese culture, we hypothesized that Chinese fathers may have less pronounced adverse effects on the mental health of their offspring than those mothers.
Methods
Participants and Procedure
A total of 738 Chinese adolescents (Mage = 12.80 ± 1.58 years; 47.2% girls) who were companied with one of their primary caregivers (mothers or fathers) were recruited from four junior and senior high schools in the city of Jian, China, constituting two subsamples of mother-child (N = 508) versus father-child dyads (N = 230), respectively. Included adolescents were aged 11–18 years old, all residing in urban areas, and had no history of major physical, neurological, or pervasive developmental disorders. Included caregivers were needed to be primary caregivers of adolescents who live together with the adolescents. The median monthly household income was between ¥5000 (about $737) and ¥9999 (about $1475). The detailed characteristics of the current sample are presented in the Table 1.
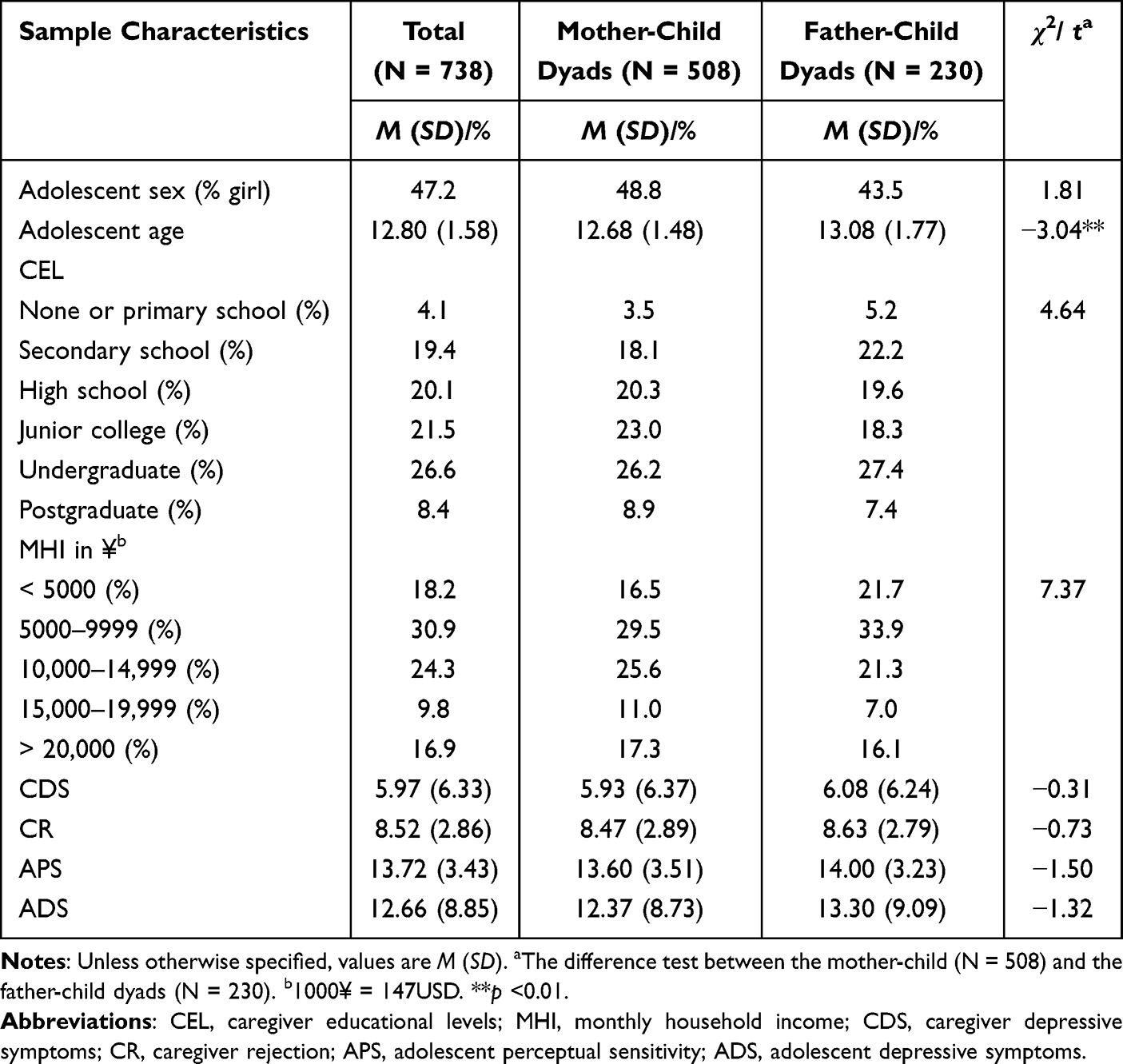 |
Table 1 Sample Characteristics |
Data collection was conducted between May and July 2023, all participants were recruited by online electronic recruitment brochures which carefully explained the purpose of the study, confidentiality principles, and potential benefits and risks to both parents and adolescents. The questionnaires for adolescents and their primary caregivers were delivered separately in sealed envelopes, filled out independently at home and forwarded to our research team. The team members further ensured the authenticity of the data collection by checking the handwriting of the responses, eliminating questionnaires with inconsistencies in the options, and those with regular responses. This study was approved by the university ethics committee, and informed consent was obtained from adolescents, their primary caregivers and school headmasters.
Measures
Caregiver Depressive Symptoms
Parents assessed depressive symptoms in the past two weeks using the Chinese version of the Beck Depression Inventory-II (BDI-II).27 The BDI-II is a widely-used self-report instrument for adults, including 21 items (eg, “I am so sad and unhappy that I can’t stand it”) which were rated on a 4-point scale ranging from 0 (no symptoms) to 3 (severe symptoms). Sum scores indicating symptom severity were calculated. In our sample, the Cronbach’s α of the BDI-II for mothers and fathers was .85 and .82, respectively.
Adolescent Depressive Symptoms
Adolescent rated their depressive symptoms in the last two weeks using the Chinese version of the Children’s Depression Inventory (CDI).28 The CDI contains 27 items, each of which is rated from 0 to 2 (eg, 0 = “I do not feel alone”; 1 = “I feel alone many times”; 2 = “I feel alone all the time”) and has shown good validity in both general and clinical child and adolescent samples worldwide.29 Sum scores indicating symptom severity were calculated. The Cronbach’s α of the CDI in mother-child and father-child dyads was excellent, achieving .90 and .91, respectively.
Caregiver Rejection
Adolescents assessed their perceptions of caregiver rejection via the rejection subscale of the widely used short form of Egna Minnen Barndoms Uppfostran (S-EMBU).30 The rejection subscale consists of six items (eg, “My parents get angry with me without letting me know the reason”) and is rated from 1 (never) to 4 (always). Sum scores were calculated, with higher scores indicating high levels of caregiver rejection perceived by adolescents. In this sample, the Cronbach’s α of rejection behaviors for mothers and fathers was .83 and .82, respectively.
Adolescent Perceptual Sensitivity
Adolescents self-reported their perceptual sensitivity using the perceptual sensitivity subscale of the Early Adolescent Temperamental Questionnaire (EATQ-R).31,32 The EATQ-R has been widely used across various adolescent samples to capture specific temperament dimensions and has good reliability.30 The perceptual sensitivity subscale included four items (eg, “I tend to notice little changes that other people do not notice”), ranging from 1 (strongly disagree) to 5 (strongly agree). Sum scores were calculated for each adolescent. The Cronbach’s α of this subscale in subsamples of mother-child and father-child dyads was both .60. Confirmatory factor analysis (CFA) supported the convergence of each item in the dimension of perceived sensitivity (χ2/df = 3.28, CFI = 0.91, TLI = 0.89, RMSEA = 0.04, SRMR = 0.04).
Covariates
Adolescent age, sex, caregiver educational levels, and monthly household income were considered as covariates according to previous research.4,5,7
Statistical Analyses
Five main analytical steps were conducted using SPSS 24.0 and Mplus 7.4. First, descriptive statistics of study variables were examined. Second, a series of nested path models with the Satorra-Bentler scaled chi-square difference test were established to (i) examine the moderated mediation mechanism regarding intergenerational transmission of depressive symptoms and to (ii) compare the role of fathers to that of mothers.
To be specific, in Model 1, the mediation model of “caregiver depressive symptoms → caregiver rejection → adolescent depressive symptoms” was firstly constructed in subsamples of mother-child and father-child dyads, respectively. In Model 2, regression weights in Model 1 were constrained to be equal between two subsamples. If Model 2 did not fit worse than Model 1, Model 2 would be selected, suggesting the mediation model did not vary between mother- vs father-child dyads. In Model 3, the main effect and the moderation effect of perceptual sensitivity were added and yielded the moderated mediation model (Figure 1). In Model 4, regression weights regarding perceptual sensitivity in Model 3 were constrained to be equal between two subsamples. If Model 4 did not fit worse than Model 3, Model 4 would be selected, suggesting the moderation effect of perceptual sensitivity in this transmission mechanism did not vary between mother- vs father-child dyads.
Notably, robust maximum likelihood (MLR) estimation was adopted in these nested path models, as this estimation is more sensitive to model mis-specification than Bootstrapping when variables are non-normally distributed.33 The full information maximum likelihood (FIML) was applied to handle missing data. In order to reduce multicollinearity, variables regarding the interactions were mean-centered.
Third, the simple slope analysis was used to probe the moderation effect of adolescent perceptual sensitivity. Fourth, the RoS analysis was established to test the moderation patterns of differential susceptibility vs diathesis-stress.34 As shown in Figure 2, in the current RoS analysis: (i) The RoS on X identifies the lower and upper bounds of values on the independent variable for which the moderation variable and the outcome variable are significantly associated with each other. If the lower limit of RoS is outside the ± 2SD range of the mean of the independent variable, the interaction should be interpreted as evidence for the diathesis-stress. If both limits of RoS are within ± 2SD range, the interaction will be interpreted as evidence for the differential susceptibility. (ii) The proportion of interaction (PoI) represents the proportion of worse effect on the total effect. The proportion affected (PA) represents the proportion of the population that is differentially affected by the moderation variable. The PoI and PA values that are ranged around 0.50 indicate evidence for differential susceptibility, whereas the PoI and PA values close to 1.00 provide evidence supporting the diathesis-stress. (iii) The nonlinear X2 or ZX2 term ought not to be significant to avoid the nonlinear phenomenon.
Finally, the Satorra-Bentler scaled chi-square difference test was used again to examine whether or not the moderated mediation model varied between adolescent sex.
Results
Preliminary Analyses
As shown in Table 1, no differences existed between the two subsamples on the vast majority of study variables, except that adolescents were younger in mother- vs father--child dyads (t = −3.14, p < 0.01). As shown in Table 2, caregiver depressive symptoms, caregiver rejection and adolescent depressive symptoms were all positively correlated with each other (r ≥ 0.23, p < 0.001). Older adolescents reported higher levels of depressive symptoms than younger adolescent in mother-child dyads (r = 0.17, p < 0.001). Caregiver educational levels and monthly household income were both negatively linked to caregiver and adolescent depressive symptoms (r ≤ −0.12, p < 0.05).
 |
Table 2 Descriptive Statistics and Correlations for All Study Variables |
Intergenerational Transmission of Depressive Symptoms: The Moderated Mediation Model
The results of nested moderated moderation models in mother-child and father-child dyads are shown in Supplementary Table S1 and Figure 3.
 |
Figure 3 Intergenerational transmission of depressive symptoms: The moderated mediation model. Notes: The interaction term of caregiver rejection and adolescent perceptual sensitivity was freely estimated in mother-child vs father-child dyads and represented using “/”. Values before the slash are coefficients for mother-child model; values after the slash are coefficients for father-child model. The remaining path coefficients were restricted to equality across mother- vs father-child dyads. Covariates (adolescent sex, age, paternal educational levels and monthly household income) were included in the models but not shown for ease of presentation. The standardized coefficients are presented. *p <0.05, ***p <0.001. |
The Mediation Effect of Parental Rejection
The comparison of nested Model 1 vs Model 2 showed that the constrained Model 2 did not fit worse than the unconstrained Model 1 (Δχ2 (7) = 2.58, p = 0.921), indicating that this mediation model of “caregiver depressive symptoms → caregiver rejection → adolescent depressive symptoms” did not vary between mother- vs father-child dyads.
Specifically, mothers and fathers both transmitted depressive symptoms to adolescents via their rejection parenting (indirect effect = 0.14, SE = 0.02, p < 0.001), accounting for 42% of the total effect. That is, adolescents whose caregivers had more severe depressive symptoms reported experiencing more rejection parenting (b = 0.12, SE = 0.02, p < 0.001), which in turn increased their risk of developing depressive symptoms (b = 1.15, SE = 0.10, p < 0.001). After controlling for this mediation effect, the direct (transmission) effect of caregiver depressive symptoms on adolescent depressive symptoms remained significant (b = 0.19, SE = 0.05, p < 0.001).
The Moderation Effect of Adolescent Perceptual Sensitivity
The comparison of nested Model 3 vs Model 4 showed that the constrained Model 4 fitted significantly worse than the unconstrained Model 3 (Δχ2 (5) = 12.36, p = 0.030), suggesting that at least one effect regarding the effects of adolescent perceptual sensitivity differed between mother- vs father-child dyads. By further constructing three nested models where each of the three paths regarding perceptual sensitivity was unconstrained one by one (Model 5, 6 and 7), the Model 7 was selected as the final model. That is, only the moderation effect of perceptual sensitivity on the second half of the mediation pathway (ie, “caregiver rejection × perceptual sensitivity → adolescent depressive symptoms”) differed between mother- versus father-child dyads (Model 7 versus Model 4: Δχ2 (1) = 4.58, p = 0.032). Adolescent perceptual sensitivity significantly moderated the second half path of the mediating pathway in mother-child (b = 0.09, SE = 0.04, p = 0.011), but not in father-child, dyads (b = −0.05, SE = 0.06, p = 0.348).
The further simple slope analysis demonstrated that for adolescents with high vs low perceptual sensitivity, maternal rejection predicted adolescent depressive symptoms in a stronger magnitude (for high perceptual sensitivity: b = 1.46, SE = 0.16, p < 0.001; for low perceptual sensitivity: b = 0.85, SE = 0.15, p < 0.001). The results of ROS analysis are shown in Table 3 and Figure 4. The estimated lower bound of RoS (−8.87, 0.46) for maternal rejection fell outside of its range (−3.47, –9.57), and meanwhile this estimated range suggests that adolescents with high vs low perceptual sensitivity were more likely to develop depressive symptoms when maternal rejection was higher than 0.46. Furthermore, the PoI (0.98) and PA (0.97) values were outside the recommended ranges for differential susceptibility model. Notably, X2, ZX2, or the set of both nonlinear terms together was not statistically significant. Taken together, these results provided support for the diathesis-stress model, adolescents with high vs low perceptual sensitivity were only more vulnerable to the adverse effects of high maternal rejection, but did not profit from relatively more positive environments (ie, low maternal rejection).
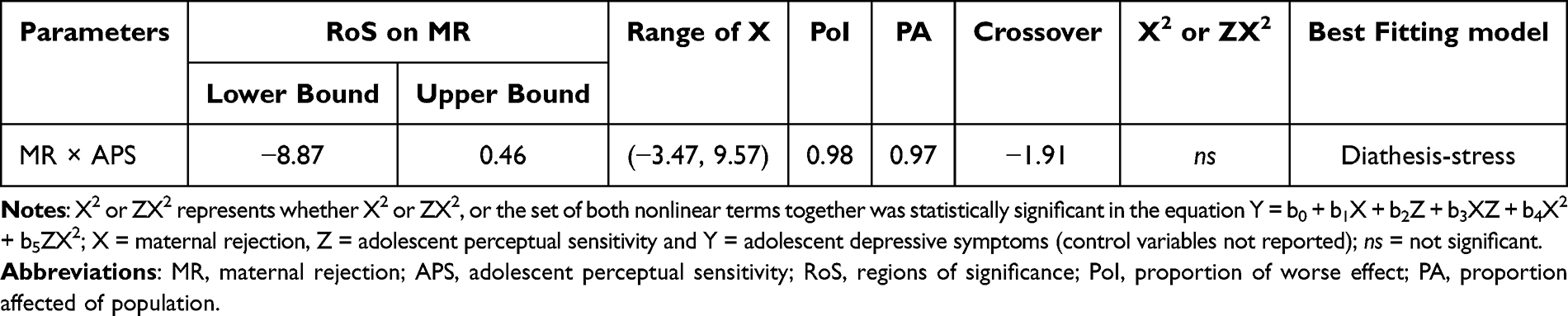 |
Table 3 The RoS for the Interaction Between Maternal Rejection and Adolescent Perceptual Sensitivity on Adolescent Depressive Symptoms |
 |
Figure 4 The moderation effect of adolescent perceptual sensitivity on the link of maternal rejection and adolescent depressive symptoms. Notes: Slopes are plotted at low and high (M ± SD) levels of adolescent perceptual sensitivity. Gray shaded area refers regions where the two lines are significantly different. |
The Moderation Effect of Adolescent Sex
The Satorra-Bentler scaled chi-square difference test did not demonstrate any significant adolescent sex differences regarding the final moderated mediation model (Model 7) (χ2 = 6.52, df = 3, p = 0.089).
Discussion
Depression is well-known to be transmitted across generations, whereas the focus has often been on mother-child dyads; little is known about the role of fathers and some inherited temperaments of adolescents in Chinese families. Targeting on a novel potential temperament “plastic” maker, the current tested a moderated mediation transmission mechanism of depressive symptoms, in which (i) the role of fathers was compared to that of mothers, and (ii) how adolescent perceptual sensitivity worked was particularly focused. Four main findings were highlighted here. First, mothers and fathers both transmitted depressive symptoms to adolescents via their rejection parenting. Second, adolescent perceptual sensitivity moderated the second half path of this mediating pathway among mother-child dyads, but not among father-child dyads. Third, this significant moderation effect of adolescent perceptual sensitivity was consistent with the diathesis-stress hypothesis rather than the differential susceptibility hypothesis. Fourth, adolescent sex did not moderate this transmission mechanism underlying depressive symptoms. These findings suggest similarities and differences in the roles of mothers and fathers in the transmission risk of depressive symptoms in contemporary Chinese families, and highlight a diathesis-stress like moderation effect of adolescent perceptual sensitivity.
Intergenerational Transmission of Depressive Symptoms: The Moderated Mediation Model
The current findings provide preliminary support for the moderated mediation mechanism in the intergenerational transmission of depressive symptoms proposed by integrative model, but only in mother-child dyads. As expected based on prior work,35 maternal rejection significantly mediated the mother-child depression transmission pathway, which was in line with the five-step, action-control model and the parental acceptance-rejection theory.10,11 Meanwhile, adolescent perceptual sensitivity was found to significantly moderate the second half path of the mediating pathway of maternal rejection and worked in a manner of diathesis-stress but not the differential susceptibility. That is, adolescents with high vs low perceptual sensitivity were more likely to develop depressive symptoms in the face of high levels of maternal rejection. Despite that recent neural and behavioral evidence suggest that perceptual sensitivity might be a novel, potential plastic temperament maker towards environmental influences,6,18,19 this finding appears support the “plastic window” effect when examining the two competing hypotheses. That is, although controversy remains in the literature,36 individual plasticity to environmental influences is more likely to be pronounced during infancy and childhood (ie, plasticity window) ―the plasticity period of neurobiological systems, but not during adolescence.24,25,37
Intringly, recent evidence regarding on brain development supports this novel “plastic window” effect. For instance, Yu et al revealed that, hippocampus development is sensitive to both adverse and protective effects of socioeconomic-related factors experienced only in childhood, but not in other periods of the development.38 Besides, adverse childhood experiences are resulted in epigenetic modifications in stress-related genes, especially in early childhood,39 which may further change cognitive and emotional adaptive strategies.40 More related, despite the mechanism remains unclear, the plastic effect towards maternal rejection of temperamental perceptual sensitivity is probably not activated during adolescence.41 High vs low perceptual sensitivity has demonstrated to make individuals more alert to surroundings and thus read and recognize mothers’ rejection signals more quickly.42 Meanwhile, excessive empathy in these adolescent as a result of better development of theory-of-mind, particularly in adolescent,6 might make them care too much about the signals and expectations of mothers and suppress their own emotions, inducing the diathesis-stress like moderation effect.
To summarize, the findings highlight a “diathesis-stress” like moderation effect of adolescent perceptual sensitivity in the transmission mechanism underlying depressive symptoms in the key period of adolescence. We call for more studies to focus on this rarely investigated “plastic window” effect and related neural and biological mechanisms (eg, epigenetic modifications and brain alterations) regarding on the temperamental perceptual sensitivity trait.
Intergenerational Transmission of Depressive Symptoms: The Role of Mothers versus Fathers in Chinese Families
The current findings suggest both similarities and differences in the roles of mothers and fathers in the transmission risk of depressive symptoms in contemporary Chinese families. Specifically, the mediation effect of caregiver rejection was equivalent across mother- vs father-child transmission models, whereas the moderation effect of adolescent perceptual sensitivity only occurred in mother-child dyads. Despite contrary to our expectation, the findings are not difficult to understand. The equivalent mediation effect regarding caregiver rejection might be due to that higher female employment rate and multiculturalism make Chinese fathers to shoulder more caregiving responsibilities and participate in more rearing practices than before.43–45 In these daily interaction, neither depressed fathers nor mothers are able to transmit adequate positive signals towards their children. Despite of this, the traditional role expectations of “strict father and kind mother” may still root in a significant proportion of contemporary Chinese families.44 In parent-child interactions, the mothers are often expected to be more caring, sensitive and their rearing practices are more likely to be adapted by children’s characteristics than fathers.46,47 Moreover, Chinese mothers often spend more average time with their children than fathers.48 Thus, the mothers with more rejecting signals may deviate more from their social expectations, making these perceptual sensitive adolescents more easily to perceive these “gaps”. This is probably the reason why the temperament × parenting interaction was only found in mother-child dyads. In addition, we did not capture the moderation effect of adolescent sex in these transmission mechanisms, highlighting more similar gender socialization effect in Chinese family nowadays. These preliminary findings regarding the roles of parental and adolescent sex need to be independently replicated in larger, and other ethnic samples.
Strengths, Limitations and Clinical Implications
To the best of our knowledge, this is the first study that tested such a moderated mediation mechanism underlying the intergenerational transmission of depressive symptoms, which has several strengths. First, this study advances our knowledge about the rarely-known roles of fathers in the intergenerational transmission mechanism of depressive symptoms in Chinese families. Second, this study tested the competing moderation effects (“diathesis-stress” vs “differential susceptibility”) of adolescent perceptual sensitivity in such transmission pathways for the first time. Further, the current findings emphasize the crucial timing effect of the “plastic window”. Finally, the rigorous analytic steps and methods, especially nested regression models and RoS analysis, were used to strengthen the robustness of the current findings. Several clinical implications could be drawn from the current findings. First, positive parenting skills may be useful for both depressed mothers and fathers to interrupt the transmission of depressive symptoms in families. Before that, we recommend that parental depressive symptoms should be routinely screened for and relevant health guidance and education is crucial for preventive interventions. Second, adolescents with high perceptual sensitivity may be more likely to benefit from some prevention and intervention programs (eg, mindfulness training) to reduce their excessive attention to rejection signals, especially from mothers. These findings may help establish precise preventive interventions from a perspective of “for whom” and “in which way”.
Several limitations of the current study should be carefully considered. First, this study was cross-sectional, and the causal relationships cannot be inferred and should be interpreted in caution. Nevertheless, the current moderated mediation model was theories-based (eg, considering the integrative model, parental acceptance-rejection as well as diathesis-stress/differential susceptibility theories). Future research with a longitudinal design is needed to validate this model, which could provide temporal precedence of variables and is crucial for the hypothesized causal inference. Second, mother- and father-child dyads design only allows us to examine the respective roles of mothers or fathers in the transmission mechanism of depressive symptoms. The mutual effects (eg, actor-partner interdependence effects) or the interactive effects, among fathers and mothers could be examined in future research that includes data from mother, father and child simultaneously. Besides, small sample size for the father-child subsample may raise concerns about statistical power for detecting the moderation effect in father-child dyads. We thus supplemented this corresponding analysis, which showed that the statistical power for detecting temperament × parenting interactions (R2 = 0.02 ~ 08; α = 0.05)49,50 was relatively acceptable, ranging from 79.1% to 100.0% in this subsample (N = 230; G*Power 3.1.9.7). Third, parenting behaviors that were measured by adolescent self-report may introduce potential bias. Nonetheless, adolescent development has been found to be more influenced by adolescent-perceived parenting than parenting that is rated or observed by others.51 Multi-informant methods (eg, adolescent-, parent-, and observer-report) could be used to obtain a more comprehensive picture of the role of parenting. Fourth, adolescent perceptual sensitivity assessed by only four items had a relatively low internal consistency. However, Hair et al noted that a Cronbach’s α coefficient of 0.6 demonstrates the reliability of a variable when it has fewer than six measurement items.52 Experimental methods, eg, a morphed facial expressions recognition task, are recommended to verify our findings.22 Fifth, the sample in this study was drawn from urban areas; despite that the potential effects of caregiver educational levels and monthly household income were controlled for, the generalizability of the findings in rural families requires further validation. Finally, additional mediators, eg, epigenetic modification or brain alterations, could be further explored.1,53 Larger, and/or beyond Chinese samples are needed to replicate these preliminary findings.
Conclusion
The current study provided preliminary evidence that the intergenerational transmission of depressive symptoms from parents to adolescents was a complex process within Chinese families. Mothers and fathers both transmitted depressive symptoms to adolescents via their rejection parenting. However, adolescent perceptual sensitivity moderated the second half path of this mediating pathway among mother-child dyads, but not among father-child dyads, and worked in a manner of diathesis-stress. Adolescent sex did not moderate this transmission mechanism. These findings suggest similarities and differences in the roles of mothers and fathers in the transmission risk of depressive symptoms in contemporary Chinese families, and highlight a diathesis-stress like moderation effect of adolescent perceptual sensitivity. Increasing positive parenting, and prevention and intervention for adolescents with high perceptual sensitivity would help interrupt the transmission risk of depressive symptoms. Future research needs to integrate the cultural contextualization and further consider the impact of evolving parental roles, especially evolving paternal roles, in these transmission pathways of depressive symptoms across Chinese families.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All procedures were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of School of Nursing and Rehabilitation, Shandong University. Informed consent was obtained from all individual participants and their guardians.
Acknowledgments
We are grateful to all the students, parents and teachers who participated or contributed to the current study, as well as undergraduate and graduate research assistants who helped with data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Humanity and Social Science Foundation of Ministry of Education of China (24C10422012), Natural Science Foundation of Shandong Province (ZR2023MC118), National Natural Science Foundation of China (31800936), and Future Plan of Young Scholars in Shandong University (21330089964217) to CC.
Disclosure
All authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Goodman SH, Gotlib IH. Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission. Psychol Rev. 1999;106(3):458–490. doi:10.1037/0033-295x.106.3.458
2. Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, Heyward D. Maternal depression and child psychopathology: a meta-analytic review. Clin Child Fam Psychol Rev. 2011;14(1):1–27. doi:10.1007/s10567-010-0080-1
3. Sweeney S, MacBeth A. The effects of paternal depression on child and adolescent outcomes: a systematic review. J Affect Disord. 2016;205:44–59. doi:10.1016/j.jad.2016.05.073
4. Hentges RF, Graham SA, Plamondon A, Tough S, Madigan S. Bidirectional associations between maternal depression, hostile parenting, and early child emotional problems: findings from the all our families cohort. J Affect Disord. 2021;287:397–404. doi:10.1016/j.jad.2021.03.056
5. Yang Y, Chen L, Ji LQ, Zhang W. The intergenerational transmission of maternal depression: the mediating role of mother-adolescent relationship and the moderating role of adolescents’ negative affectivity. Psychol Develop Educ. 2017;33(3):368–377. doi:10.16187/j.cnki.issn1001-4918.2017.03.15
6. Weeland J, Van den Akker A, Slagt M, Putnam S. Perception is key? Does perceptual sensitivity and parenting behavior predict children’s reactivity to others’ emotions? J Exp Child Psychol. 2017;163:53–68. doi:10.1016/j.jecp.2017.06.012
7. Dix T, Yan N. Mothers’ depressive symptoms and infant negative emotionality in the prediction of child adjustment at age 3: testing the maternal reactivity and child vulnerability hypotheses. Dev Psychopathol. 2014;26(1):111–124. doi:10.1017/S0954579413000898
8. Gibb BE, Grassia M, Stone LB, Uhrlass DJ, McGeary JE. Brooding rumination and risk for depressive disorders in children of depressed mothers. J Abnorm Child Psychol. 2012;40(2):317–326. doi:10.1007/s10802-011-9554-y
9. Whitbeck LB, Hoyt DR, Simons RL, et al. Intergenerational continuity of parental rejection and depressed affect. J Pers Soc Psychol. 1992;63(6):1036–1045. doi:10.1037//0022-3514.63.6.1036
10. Dix T, Meunier LN. Depressive symptoms and parenting competence: an analysis of 13 regulatory processes. Dev Rev. 2009;29(1):45–68. doi:10.1016/j.dr.2008.11.002
11. Rohner RP, Khaleque A, Cournoyer DE. Parental acceptance-rejection: theory, methods, cross-cultural evidence, and implications. Ethos. 2005;33(3):299–334. doi:10.1525/eth.2005.33.3.299
12. Goodman SH, Simon HFM, Shamblaw AL, Kim CY. Parenting as a mediator of associations between depression in mothers and children’s functioning: a systematic review and meta-analysis. Clin Child Fam Psychol Rev. 2020;23(4):427–460. doi:10.1007/s10567-020-00322-4
13. Schiff M, Pat-Horenczyk R, Ziv Y, Brom D. Multiple traumas, maternal depression, mother-child relationship, social support, and young children’s behavioral problems. J Interpers Violence. 2021;36(1–2):892–914. doi:10.1177/0886260517725738
14. Lansford JE. Annual research review: cross-cultural similarities and differences in parenting. J Child Psychol Psychiatr. 2022;63(4):466–479. doi:10.1111/jcpp.13539
15. Feng Y, Whiteman SD, Xu S, Li L, Jin S, French DC. Chinese adolescents’ relationships with mothers, fathers, and siblings: associations with youth’s internalising and externalising problems. J Relationships Res. 2019;10:e15. doi:10.1017/jrr.2019.11
16. Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: implications for the depressive disorders. Psychol Bull. 1991;110(3):406–425. doi:10.1037/0033-2909.110.3.406
17. Bakermans-Kranenburg MJ, van IJzendoorn MH. The hidden efficacy of interventions: gene×environment experiments from a differential susceptibility perspective. Annu Rev Psychol. 2015;66(1):381–409. doi:10.1146/annurev-psych-010814-015407
18. Bolders AC, Tops M, Band GPH, Stallen PJM. Perceptual sensitivity and response to strong stimuli are related. Front Psychol. 2017;8:1642. doi:10.3389/fpsyg.2017.01642
19. Lovejoy LP, Krauzlis RJ. Changes in perceptual sensitivity related to spatial cues depends on subcortical activity. Proc Natl Acad Sci U S A. 2017;114(23):6122–6126. doi:10.1073/pnas.1609711114
20. Conradt E, Measelle J, Ablow JC. Poverty, problem behavior, and promise: differential susceptibility among infants reared in poverty. Psychol Sci. 2013;24(3):235–242. doi:10.1177/0956797612457381
21. Evans DE, Rothbart MK. Developing a model for adult temperament. J Res Pers. 2007;41(4):868–888. doi:10.1016/j.jrp.2006.11.002
22. Lopez-Duran NL, Kuhlman KR, George C, Kovacs M. Facial emotion expression recognition by children at familial risk for depression: high-risk boys are oversensitive to sadness. J Child Psychol Psychiatr. 2013;54(5):565–574. doi:10.1111/jcpp.12005
23. Juul EML, Hjemdal O, Aune T. Prevalence of depressive symptoms among older children and young adolescents: a longitudinal population-based study. Scand J Child Adolesc Psychiatr Psychol. 2021;9:64–72. doi:10.21307/sjcapp-2021-008
24. Rioux C, Castellanos-Ryan N, Parent S, Séguin JR. The interaction between temperament and the family environment in adolescent substance use and externalizing behaviors: support for diathesis-stress or differential susceptibility? Dev Rev. 2016;40:117–150. doi:10.1016/j.dr.2016.03.003
25. Slagt M, Dubas JS, Deković M, van Aken MA. Differences in sensitivity to parenting depending on child temperament: a meta-analysis. Psychol Bull. 2016;142(10):1068–1110. doi:10.1037/bul0000061
26. Marzola P, Melzer T, Pavesi E, Gil-Mohapel J, Brocardo PS. Exploring the role of neuroplasticity in development, aging, and neurodegeneration. Brain Sci. 2023;13(12):1610. doi:10.3390/brainsci13121610
27. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. Psychological Corporation; 1996.
28. Kovacs M. Manual for the Children’s Depression Inventory. Multi-Heath Systems; 1992.
29. Liu Z, Li J, Wang Y, Miao N, Zhong J. Structural verification and measurement invariance of Chinese version of children’s depression inventory. Chin J Clin Psychol. 2019. doi:10.16128/j.cnki.1005-3611.2019.06.019
30. Li Z, Wang L, Zhang L. Exploratory and confirmatory factor analysis of a short-form of the EMBU among Chinese adolescents. Psychol Rep. 2012;110(1):263–275. doi:10.2466/02.08.09.21.PR0.110.1.263-275
31. Capaldi DM, Rothbart MK. Development and validation of an early adolescent temperament measure. J Early Adolesc. 1992;12(2):153–173. doi:10.1177/0272431692012002002
32. Zhang J, Shen L, Gao N, Yan C. The revision and application of the revision of the early adolescent temperament questionnaire. Chin Mental Health J. 2008;22(6):439–443. doi:10.3724/SP.J.1041.2008.00418
33. Finney SJ, DiStefano C. Non-Normal and Categorical Data in Structural Equation Modeling: Structural Equation Modeling: A second Course. Information Age Publishin; 2006.
34. Roisman GI, Newman DA, Fraley RC, Haltigan JD, Groh AM, Haydon KC. Distinguishing differential susceptibility from diathesis-stress: recommendations for evaluating interaction effects. Dev Psychopathol. 2012;24(2):389–409. doi:10.1017/S0954579412000065
35. Israel ES, Gibb BE. A transactional mediation model of risk for the intergenerational transmission of depression: the role of maternal criticism. Dev Psychopathol. 2024;36(1):92–100. doi:10.1017/S0954579422000992
36. Leighton C, Botto A, Silva JR, Jiménez JP, Luyten P. Vulnerability or sensitivity to the environment? Methodological issues, trends, and recommendations in gene-environment interactions research in human behavior. Front Psychiatry. 2017;8:106. doi:10.3389/fpsyt.2017.00106
37. Lionetti F, Spinelli M, Moscardino U, et al. The interplay between parenting and environmental sensitivity in the prediction of children’s externalizing and internalizing behaviors during COVID-19. Dev Psychopathol. 2023;35(3):1390–1403. doi:10.1017/S0954579421001309
38. Eves R, Nearchou F, Wolke D, Pluess M, Lemola S. Interactions between infant characteristics and parenting factors rarely replicate across cohorts and developmental domains. J Child Psychol Psychiatr. 2025. doi:10.1111/jcpp.14149
39. Yu Q, Daugherty AM, Anderson DM, et al. Socioeconomic status and hippocampal volume in children and young adults. Dev Sci. 2018;21(3):e12561. doi:10.1111/desc.12561
40. Lussier AA, Smith BJ, Fisher JD, et al. DNA methylation mediates the link between adversity and depressive symptoms. Nat Mental Health. 2024;2(12):1476–1485. doi:10.1038/s44220-024-00345-8
41. Xu Y, Yang S, Cao C. Glucocorticoid receptor gene (NR3C1) methylation, childhood maltreatment, multilevel reward responsiveness and depressive and anxiety symptoms: a neuroimaging epigenetic study. Neuroimage. 2025;306:121003. doi:10.1016/j.neuroimage.2025.121003
42. Lionetti F, Aron A, Aron EN, Burns GL, Jagiellowicz J, Pluess M. Dandelions, tulips and orchids: evidence for the existence of low-sensitive, medium-sensitive and high-sensitive individuals. Transl Psychiatry. 2018;8(1):24. doi:10.1038/s41398-017-0090-6
43. Gölcük M, Berument SK. The relationship between negative parenting and child and maternal temperament. Curr Psychol. 2021;40(7):3596–3608. doi:10.1007/s12144-019-00307-9
44. Dou D, Shek DTL, Kwok KHR. Perceived paternal and maternal parenting attributes among Chinese adolescents: a meta-analysis. Int J Environ Res Public Health. 2020;17(23):8741. doi:10.3390/ijerph17238741
45. Li X. Fathers’ involvement in Chinese societies: increasing presence, uneven progress. Child Dev Perspect. 2020;14(3):150–156. doi:10.1111/cdep.12375
46. Cerniglia L, Cimino S, Ballarotto G. Mother-child and father-child interaction with their 24-month-old children during feeding, considering paternal involvement and the child’s temperament in a community sample. Infant Ment Health J. 2014;35(5):473–481. doi:10.1002/imhj.21466
47. Hallers-Haalboom ET, Mesman J, Groeneveld MG, et al. Mothers, fathers, sons and daughters: parental sensitivity in families with two children. J Fam Psychol. 2014;28(2):138–147. doi:10.1037/a0036004
48. Li D, Guo X. The effect of the time parents spend with children on children’s well-being. Front Psychol. 2023;14:1096128. doi:10.3389/fpsyg.2023.1096128
49. Danzig AP, Dyson MW, Olino TM, Laptook RS, Klein DN. Positive parenting interacts with child temperament and negative parenting to predict children’s socially appropriate behavior. J Soc Clin Psychol. 2015;34(5):411–435. doi:10.1521/jscp.2015.34.5.411
50. Karreman A, de Haas S, van Tuijl C, van Aken MA, Deković M. Relations among temperament, parenting and problem behavior in young children. Infant Behav Dev. 2010;33(1):39–49. doi:10.1016/j.infbeh.2009.10.008
51. Cao C, Rijlaarsdam J. Childhood parenting and adolescent internalizing and externalizing symptoms: moderation by multilocus hypothalamic-pituitary-adrenal axis-related genetic variation. Dev Psychopathol. 2023;35(2):524–536. doi:10.1017/S0954579421001620
52. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis: A Global Perspective. Englewood Cliffs, NJ: Prentice Hall; 2010.
53. Chen Y, Cheung S, Huang CC. Intimate partner violence during pregnancy: effects of maternal depression symptoms and parenting on teen depression symptoms. J Interpers Violence. 2022;37(9–10):NP7034–NP7056. doi:10.1177/0886260520967754
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.