")
Back to Journals » Vascular Health and Risk Management » Volume 20
Intracerebral Hemorrhage with Churg Strauss-Syndrome: Multidisciplinary Collaboration and Literature Review
Received 19 September 2024
Accepted for publication 6 December 2024
Published 14 December 2024 Volume 2024:20 Pages 567—578
DOI https://doi.org/10.2147/VHRM.S489212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Pu Bai,* Peitao Xie*
Inner Mongolia Medical University Ordos School of Clinical Medicine, Ordos, 017000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pu Bai; Peitao Xie, Ordos Center Hospital, No. 6 Sudu Street, Kangbashi District, Ordos City, 017000, People’s Republic of China, Email [email protected]; [email protected]
Objective: To explore the clinical characteristics and treatment outcomes of intracerebral hemorrhage in eosinophilic granulomatosis with polyangiitis (EGPA).
Methods and Patient Presentation: We report an 18-year-old student of EGPA complicated with intracerebral hemorrhage. The laboratory tests showed a continuous increase in eosinophils. The CT of head and chest showed cerebral hemorrhage and pulmonary infiltration.
Interventions: The patient received an intravenous infusion of methylprednisolone 1g/(kg·d) and cyclophosphamide for 3 days, followed by oral prednisone 1 mg/(kg·d).
Outcomes: At discharge, the patient’s head and chest CT showed obvious absorption of intracranial hematoma and improvement of pulmonary infiltration. We reviewed 40 previously published cases of EGPA with intracerebral hemorrhage focusing on the clinical features and treatment of intracerebral hemorrhage caused by EGPA.
Conclusion: For the cases of EGPA complicated with intracerebral hemorrhage, we should timely differentiate diagnosis and recognition. Early diagnosis with aggressive immunosuppressive therapy can help improve the prognosis of patients EGPA with intracerebral hemorrhage. When a patient is affected by EGPA, it is essential to remain vigilant for signs of Central Nervous System involvement. The treatment with glucocorticoids and cyclophosphamide is effective in managing EGPA.
Keywords: Churg Strauss-Syndrome, eosinophilic granulomatosis with polyangiitis, eosinophilia, intracerebral hemorrhage
Introduction
Churg-Strauss Syndrome (CSS) was known as Eosinophilic Granulomatosis with Polyangiitis (EGPA). The name of CSS is derived from the first case of EGPA reported by Churg and Strauss in 1951.1,2 EGPA is a disease associated with anti-Neutrophil Cytoplasmatic Antibody associated vasculitides, alongside granulomatosis with polyangiitis and microscopic polyangiitis.3 It is a rare systemic disease characterized by asthma, transient pulmonary infiltration, eosinophilia, and systemic vasculitis.4 EGPA progresses rapidly and has a variety of clinical manifestations, involving multiple organs and systems.5 The respiratory tract and lungs are the earliest and most easily involved,6 and most of the first symptoms are wheezing seizures and nasosinusitis symptoms, followed by the nervous system. Nervous system involvement is common in EGPA, especially peripheral neuropathy,7,8 which is also included in the classification criteria for EGPA. In contrast, EGPA rarely affects the central nervous system, Hemorrhagic stroke in EGPA is extremely rare.9 In patients with EGPA, most patients show with upper respiratory tract and lung involvement, such as nasosinusitis, asthma, and wandering pulmonary infiltrating shadow, and some patients may show peripheral neuropathy, skin damage, and heart involvement. Among, Eosinophilia is one of the cardinal features in EGPA.10 Recent studies have shown that the global incidence of the disease is 2.5 cases per 100,000 adults per year,11 with incidence peaking at ages 30–40 or 55–64.12 However, the pathogenesis of EGPA remains unclear, and it is currently believed to be related to environmental, genetic factors and immune disorders.10
Before 1990, the EGPA could be diagnosed when patients developed asthma, the number of eosinophils in peripheral blood exceeded 1.5×109 /L, and two organs were affected.9 This diagnosis only relies on clinical manifestations, without histopathological diagnosis, is simple and easy to use, and is widely used by clinicians. After 1990, the diagnostic criteria for EGPA mainly refer to the classification criteria proposed by the American College of Rheumatology in 1990. According to the Diagnostic criteria of the American College of Rheumatology (ACR),1 EGPA can be diagnosed when four or more of these conditions are satisfied. ACR criteria: Presence of four or more of the following: 1) eosinophilia (more than 10%), 2) asthma, 3) pulmonary infiltrates, 4) paranasal abnormalities, 5) neuropathy, and 6) extravascular eosinophilia on biopsy.13 In 2012, Chapel Hill consensus pointed out that the definition of EGPA should include eosinophilic granulomatous inflammation in tissues, necrotizing small vasculitis, blood eosinophilia, and asthma.14 With the deepening of EGPA research, more specific MIRRA classification criteria were proposed in clinical studies in 2017.15 The main criteria were: (1) history of asthma; (2) Eosinophilia (peripheral blood eosinophilia ratio > 10% or absolute value > 1.0×109 /L). Secondary criteria (meeting at least 2 criteria) were: (1) Positive biopsy: perivascular eosinophilic infiltration; (2) Neuropathy: single or multiple neuropathy; (3) pulmonary infiltration; (4) sinus lesions; (5) Cardiac color ultrasound or cardiac magnetic resonance imaging suggested cardiomyopathy; (6) glomerulonephritis; (7) Hematuria, proteinuria; (8) Alveolar hemorrhage diagnosed by alveolar lavage fluid; (9) Skin purpura; (10) Positive ANCA (MPO or PR3) test. In 2018, China “Multidisciplinary Expert Consensus on Diagnosis and Treatment of EGPA”: a. Asthma-like lesions (wheezing, cough, chest tightness and dyspnea); b. Eosinophilia (≥10% or absolute value ≥1.5*109/L); c. Multiple or single peripheral neuropathy; d. Non-fixed pulmonary infiltration; e. Sinusitis; f. Extravascular eosinophilic infiltration. The Meeting 4 or more of the 6 classification criteria can be diagnosed as EGPA. In this paper, we report a case of left frontotemporal parietal cerebral hemorrhage, and summarize and review previous reports of cerebral hemorrhage and EGPA.
Case Presentation
On January 13, 2021, an 18-year-old student suddenly lost consciousness at school. He was admitted to the hospital emergency department for treatment. Prior to admission, he had a persistent fever and headache for more than 10 days. On December 30, 2020 (10 days before hospitalization), he was treated at a small local clinic, where doctors treated his fever with cephalosporin antibiotics and methylprednisolone sodium succinate for injection. After treatment, his fever and headache did not ease. On 12 January 2021 (one day before admission), his headache symptoms worsened. Then, he suddenly lost consciousness, accompanied by convulsions and vomiting. He underwent a head and chest CT scan at a local hospital on the same day. Head CT showed high-density imaging of the left temporal lobe. Chest CT showed lower right pneumonia. On January 13, 2021, he was transferred to our hospital for further treatment.
In 2007, he underwent hernia surgery at a local hospital. History of allergy was not known. History of asthma, rhinitis was also not known. His parents denied that he had a history of high blood pressure, heart disease, diabetes, smoking and taking illegal drugs.
On admission, the patient had a body temperature of 36.5°C. Physical examination revealed blood pressure of 132/69 mmHg and a regular pulse rate of 56 beats/min. Chest auscultation revealed expiratory wheezes in the bilateral lower lung field. There was no palpable enlargement of systemic superficial lymph nodes. Electrocardiogram shows a normal heart rate. Neurosurgical examination: blurred consciousness, misorientation, Glasgow Coma Score: 13 (mild disturbance of consciousness). He is sensitive to light. Stretching the tongue is not biased. The muscle strength of four limbs is Ⅳ. Muscle tension is normal. And bilateral knee tendon reflex is symmetrical.
Laboratory examinations revealed a white blood cell (WBC) count of 12.31×109/L (normal range: 3.5–9.5×109 /L), a hemoglobin level of 134 g/L, and a platelet count of 65×109 /L (normal range: 125–350 ×109 /L). The neutrophil count was 10.44×109/L (normal range: 2.04–7.5×109 /L). The ratio of neutrophils was 84.70% (normal range 51–75%). The lymphocyte count and the ratio of lymphocyte were both reduced, 0.76×109/L (normal range 0.8–4.0×109/L) and 6.20% (normal range 20–50%), respectively. However, the eosinophilic granulocyte was abnormal. The count of eosinophilic granulocyte was 0.00×109/L (normal range 0.02–0.52×109/L). The creatinine level was 66 μmol/L (normal range: 53–97 μmol/L), with an increased Hypersensitive C-reactive protein (Hs-CRP) of 127.86 mg/L (≤5 mg/L). Urinalysis showed proteinuria. The patient presented with an increased aspartate aminotransferase of 42 U/L (normal range 15–40 U/L) and increasedγ-glutamyl transpeptidase (76.6 U/L) (normal range ≤73). The procalcitonin (PCT) was 0.13 ng/mL (<0.1 No bacterial infection; 0.1≤PCT<0.25 may be no bacterial infection). The coagulation indexes were all within the normal range. And the other laboratory examinations showed no abnormality.
Treatment Process
The above is the detailed process of clinical examination, treatment and diagnosis of a patient with EGPA complicated with intracerebral hemorrhage reported in this paper, as shown in Table 1. During the diagnosis and treatment of this case, the clinical pharmacist participated in the treatment and made recommendations for diagnosis and treatment. The count of eosinophilic granulocyte gradually increased from the third day of admission. Its peak reached maximum on January 22. The count of eosinophilic granulocyte was more than 10 times the normal range. Changes in eosinophilic granulocyte count and ratio during hospitalization are shown in Figure 1. The cerebrospinal fluid was detected by metagenomic next-generation sequencing (mNGS). No pathogenic microorganism infection was detected by mNGS. The MRA+MRV did not find vascular malformation (Figure 2). However, MRI revealed left inferior turbinate hypertrophy, right maxillary sinus cyst, and sphenoid sinus hypertrophy. It suggested that the patient had a history of sinusitis and allergic rhinitis. MRI and head CT showed left frontotemporal and parietal cerebral hemorrhage with soft tissue swelling in the left frontotemporal region (Figures 3 and 4), and chest CT showed shadows in the lower lobes of both lungs (Figure 5). Clinical pharmacists summarized the above results for a literature search. According to the American College of Rheumatology Criteria,1,2 EGPA was diagnosed based on clinical symptoms and laboratory findings. He was treated with methylprednisolone and cyclophosphamide and was discharged on February 9. On discharge on February 9, CT of the chest showed that shadow of lower lobe of both lungs was more absorbed than those on admission (Figure 6) and intracranial hematoma was more absorbed than those on admission (Figure 7).
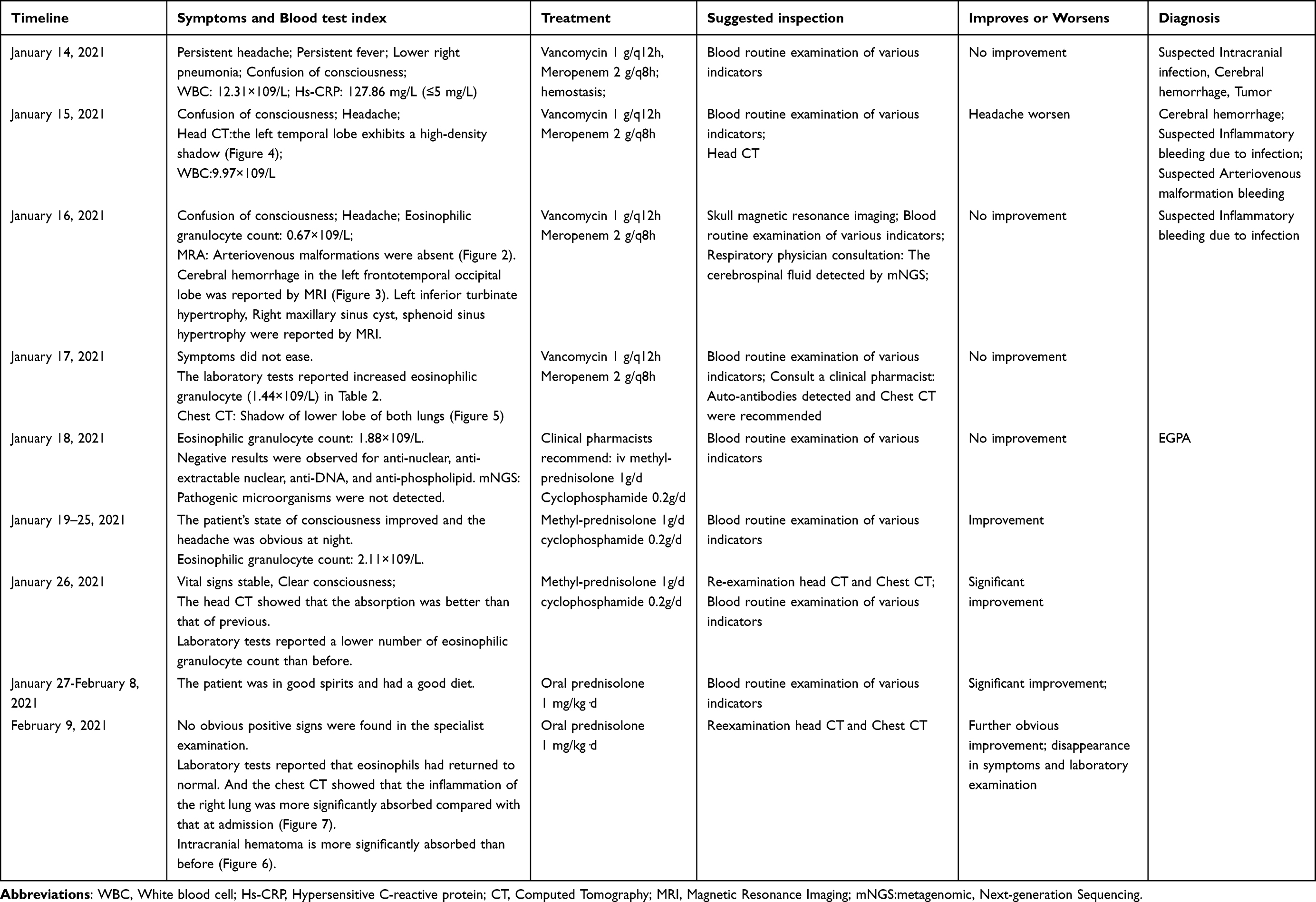 |
Table 1 The Clinical Examination, Treatment and Diagnosis Process of EGPA with Intracerebral Hemorrhage |
 |
Figure 1 The eosinophil count and ratio changed with time during hospitalization. |
 |
Figure 2 The Magnetic Resonance Angiography of the patient at admission. The MRA did not find vascular malformation at admission. |
 |
Figure 3 The Magnetic Resonance Imaging of the patient at admission. The MRI showed left frontotemporal and parietal cerebral hemorrhage. |
 |
Figure 4 The heat computerized tomography of the patient at admission. |
 |
Figure 5 The chest computerized tomography of the patient at admission. |
 |
Figure 6 The chest computerized tomography of the patient at discharge. |
 |
Figure 7 The heat computerized tomography of the patient at discharge. |
Review of the Literature
We searched the literature published in PubMed, Web of Science, and Embase databases using the MeSH terms or keywords: “Eosinophilic Granulocyte, Eosinophilia, Intracerebral Hemorrhage, Cerebral Hemorrhage, Eosinophilia with Intracerebral Hemorrhage, Churg-Strauss syndrome, Eosinophilic Granulomatosis with Polyangiitis” until October 2024. Case reports and case series of patients with the diagnoses of CSS or EGPA were eligible for inclusion. Publications were excluded if they did not meet the above criteria. As a result, 39 articles described EGPA with intracerebral hemorrhage were identified.16–54 We systematically reviewed clinical features and therapies of EGPA with intracerebral hemorrhage. Clinical information in the previous reports are summarized in Table 2, including age, sex, clinical features, Systemic involvement, and therapies.
 |
Table 2 Clinical Features of Previously Reported Patients with EGPA and Intracerebral Hemorrhage |
Discussion
EGPA is a rare systemic disease characterized by vascular involvement in multiple organs, such as respiratory tract, cutaneous tissue, gastrointestinal tract, cardiovascular system, paranasal sinus abnormality, arthritis/arthralgia, and peripheral nerves. The patient usually has a history of chronic asthma, long-standing rhinitis, recurrent sinusitis, nasal obstruction, and nasal polyposis. Asthma is one of the most common diseases associated with EGPA, including IgE-mediated allergic asthma, exercise-induced asthma, non-allergic asthma caused by viral upper respiratory tract infection or no obvious trigger, and cough variant asthma.55 The clinical manifestations of EGPA is characterized by asthma, peripheral eosinophilia, peripheral neuropathy and pulmonary invasion. The hallmark laboratory indicators of the disease are peripheral blood eosinophilia. The CT sinuses and CT chest are beneficial in determining sinus and respiratory involvement, respectively. ANCA was detectable in only 40% of patients, indicating vasculitis.
Granulomatosis with polyangiitis (GPA) is characterized histologically by necrotizing granulomatous inflammation in addition to vasculitis. Although the target organs of GPA and EGPA are similar, the clinical and pathological manifestations of GPA and EGPA are different, which can help to distinguish them. Both of them are easy to invade the respiratory system, but GPA often forms destructive lesions, such as nasal mucosa ulcers and pulmonary cavities. The respiratory tract involvement of EGPA is mild, which is manifested as allergic rhinitis, nasal polyps, and transient pulmonary infiltration. Skin lesions were common in patients with EGPA (70%) and GPA (13%). EGPA is prone to invade the heart, while GPA is rare. Renal failure is rare in patients with EGPA, but GPA is common. EGPA also has a better prognosis than GPA and responds well to glucocorticoids.
Hypereosinophilic syndrome has many similarities with EGPA. Both are systemic disorders with increased peripheral blood eosinophils and tissue infiltration by eosinophils. However, the peripheral blood eosinophil count of hypereosinophilic syndrome is higher than that of EGPA. Hypereosinophilic syndrome is often accompanied by diffuse central nervous system damage, hepatosplenomegaly and systemic lymphadenopathy, thromboembolism and thrombocytopenia, while EGPA is rare. Vasculitis and granulomas are rare in the hypereosinophilic syndrome. The response to glucocorticoids was also different between the two groups, and the response to hypereosinophilic syndrome was worse.
Microscopic polyarteritis (MPA) is characterized histologically by vasculitis without granulomatous inflammation.56 Common clinical manifestations include rapidly progressive pauci-immune glomerulonephritis and alveolar hemorrhage. MPA is most commonly associated with perinuclear ANCA and antibodies to myeloperoxidase.
The exact pathogenesis of EGPA remains unclear. The possible pathogenesis is that particulate matter and cytokines released by eosinophils, such as eosinophil cationic protein and major basic protein (MBP), cause vascular injury and tissue damage.1,57 In addition to eosinophil action,58 it may also be the result of interaction between B and T lymphocytes. This implies EGPA symptoms induced by autoimmunity acting on various tissues of the self.
In Table 2, we reviewed all reported cases of EGPA with ICH. A total of 39 articles reported 40 patients with EGPA complicated with cerebral hemorrhage. The patients had a mean age of 34 and shared clinical features of sinus abnormalities, asthma, elevated eosinophils, and lung involvement. Based on the literature of EGPA-related intracerebral hemorrhage, it was found that intracerebral hemorrhage was almost always preceded by prolonged asthma and atopic reactions. Twenty-five percent of these patients developed vascular structural abnormalities through MRA. The treatment is the combination of glucocorticoid and immunosuppressant.
First of all, the eosinophil count of the case reported was 2.11×109/L, which was more than 10 times the normal value. However, on admission, the eosinophil count was 0.00×109/L and less than 0.2×109/L. After the third day of admission, eosinophils continued to increase and exceeded the normal range. The possible cause for the result is that the patient had received low-dose glucocorticoids before the hospital admission. Besides, the MRI showed hypertrophy of the left inferior turbinate, right maxillary sinus cyst, and sphenoid sinus hypertrophy, which indicated a past history of allergic rhinitis and asthma. Thirdly, the cerebrospinal fluid testing contained a large Eosinophilic granulocyte infiltrate. In addition, the patient had a history of headache. Moreover, the chest CT scan showed non-fixed pulmonary infiltration. Brain magnetic resonance imaging and magnetic resonance angiography conducted showed no obvious evidence of aneurysm, artery dissection, or vascular spasm. Anti-nuclear antibody, anti-extractable nuclear antigen antibody, myeloperoxidase-ANCA, proteinase- 3-ANCA, anti-cardiolipin antibody were all normal. No pathogenic microorganisms were detected by mNGS. Therefore, according to the diagnostic criteria of ACR in 1990 and Chapel Hill consensus in 2012, the patient was comprehensively diagnosed as EGPA with following diagnostic basis: allergic rhinitis, asthma, peripheral blood eosinophilia (>10%), paranasal sinusitis, transient pulmonary infiltration and eosinophil infiltration of the cerebrospinal fluid. The ACR and the European Alliance of Associations for Rheumatology have published a new EGPA diagnostic criteria that it had a sensitivity of 85% and a specificity of 99%.59
EGPA is generally treated with medication. Prednisone 1–2 mg/(kg·d) was used for patients with mild disease. Methylprednisolone 1.0g/d (15 mg/kg) was used for 3 days, then oral prednisone 1–2 mg/(kg·d) was used for patients with rapid disease progression and vital organ involvement. In patients with major organ dysfunction (kidney damage, mononeuritis multiplex), immunosuppressive agents should be added to reduce or prevent irreversible organ damage. Immunosuppressant is mostly cyclophosphamide, generally intravenous infusion. After 6 to 12 weeks, the symptoms are relieved, the hormone should be slowly reduced, and the hormone therapy should be discontinued for one to two years. Prednisone, methylprednisolone, methotrexate, and cyclophosphamide were the most commonly prescribed drugs.
Conclusion
EGPA is rarely associated with intracerebral hemorrhage. For the cases of EGPA complicated with cerebral hemorrhage, it should be diagnosed as early as possible. The systemic symptoms of patient should be investigated after excluding other possible causes of ICH. Evaluation and recognition of EGPA and adequate intervention in the early are the key to treatment and the basis of drug therapy. Timely identification and management can reduce mortality and morbidity. EGPA is treated with corticosteroids and immunosuppressants. Corticosteroids are beneficial for controlling eosinophilia, inflammation, and symptoms of asthma. Immunosuppressive drugs deal with the autoimmune factors, which play an etiological role in the progression of the disease.
Abbreviations
MRI, Magnetic Resonance Imaging; MRA, Magnetic Resonance Angiography; CT, Computed Tomography; MRV, Magnetic Resonance Venography; EGPA, Eosinophilic Granulomatosis with Polyangiitis; SWI, Susceptibility Weighted Imaging; ACR, American College of Rheumatology; DWI, diffusion-weighted imaging; WBC, white blood cell; SI, Systemic involvement; PCT, procalcitonin; PI, Pulmonary Involvement; Hs-CRP, Hypersensitive C-reactive protein; SAH, Subarachnoid hemorrhage; CRP, C-reactive protein; ICH, Intracerebral Hemorrhage; PCT, Procalcitonin; IVH, Intraventricular Hemorrhage; EOS, Eosinophilia; PLH, Parietal Lobe Hemorrhage; mNGS, metagenomic Next-generation Sequencing; BGH, Basal ganglia Hemorrhage; IVAD, Intracranial vertebral artery dissection; PH, Putaminal Hemorrhage; ID, Immunosuppressive drugs; SD, Steroid drugs; PNS, Peripheral Nervous System; MP, Methylprednisolone; CPM, Cyclophosphamide; PSL, Prednisolone; CsA, Ciclosporin; PDS, Prednisone; BA, Bronchial asthma; PSA, Paranasal sinus abnormality; NR, Not reported; AR, Allergic rhinitis.
Ethics Approval and Consent for Publication
This case was approved by the ethics committee of Inner Mongolia Medical University Ordos School of Clinical Medicine. The case details were agreed to publish by the Ordos Central Hospital. Written and signed consent was obtained from patients to publish her clinical history.
Acknowledgments
Thanks to all the researchers involved in this study and the laboratories that provided the research platform. Also, thanks to the journal editors who were able to include and publish this study. Special thanks to the patient for granting us permission to report his illness.
Author Contributions
All authors made a significant contribution to the work reported. Pu Bai contributed to this manuscript as follows: conception, study design, execution, acquisition of data, analysis and interpretation, Funding acquisition, Writing – original draft and Writing – review & editing. Pu Bai have written the article and substantially revised the article. Peitao Xie contributed to this manuscript as follows: conception, study design, execution, acquisition of data and interpretation. All authors of manuscript have agreed to take responsibility and be accountable for the contents of the article and agreed on the journal to which the article will be submitted. All authors of manuscript have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
Funding
This work was supported by the Inner Mongolia Medical University Science and Technology Million Project [No. YKD2020KJDW(LH)063] and Inner Mongolia Health Commission Medical Health Technology Project [202201593].
Disclosure
The authors declare no conflicts of interest.
References
1. Greco A, Rizzo MI, De Virgilio A, et al. Churg-Strauss syndrome. Autoim Mun Rev. 2015;14(4):341–348. PMID: 25500434. doi:10.1016/j.autrev.2014.12.004
2. Khoury P, Grayson PC, Klion AD. Eosinophils in vasculitis: characteristics and roles in pathogenesis. Nat Rev Rheumatol. 2014;10(8):474–483. PMID: 25003763; PMCID: PMC4849122. doi:10.1038/nrrheum.2014.98
3. Geetha D, Jefferson JA. ANCA-Associated Vasculitis: core Curriculum 2020. Am J Kidney Dis. 2020;75(1):124–137. doi:10.1053/j.ajkd.2019.04.031
4. Mouthon L, Dunogue B, Guillevin L. Diagnosis and classification of eosinophilic granulomatosis with polyangiitis (formerly named Churg-Strauss syndrome). J Autoimmun. 2014;48-49:99–103. Erratum in: J Autoimmun. 2014;55:94. PMID: 24530234. doi:10.1016/j.jaut.2014.01.018
5. Medvedev I, Podzolkov VI, Ishina TI, Pisarev MV. Case report: a 64-year-old man with 10-year history of Eosinophilic Granulomatosis with Polyangiitis with Bronchiectasis and Severe Klebsiella pneumonia. Am J Case Rep. 2021;22(E929224). doi:10.12659/AJCR.929224
6. Saha B, Saha A, Cordeiro-Rudnisky F, Shkolnik B, Beegle S. Destructive Upper Airway Disease from Eosinophilic Granulomatosis with Polyangiitis (EGPA): the Very First Case. Case Rep Rheumatol. 2019;2019:6173869. PMID: 31263619; PMCID: PMC6556304. doi:10.1155/2019/6173869
7. Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, Casassus P. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine (Baltimore). 1999;78(1):26–37. PMID: 9990352. doi:10.1097/00005792-199901000-00003
8. Noth I, Strek ME, Leff AR. Churg-Strauss syndrome. Lancet. 2003;361(9357):587–594. doi:10.1016/S0140-6736(03)12518-4.
9. Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome. Medicine (Baltimore). 1984;63(2):65–81. PMID: 6366453. doi:10.1097/00005792-198403000-00001
10. Furuta S, Iwamoto T, Nakajima H. Update on eosinophilic granulomatosis with polyangiitis. Allergol Int. 2019;68(4):430–436. PMID: 31266709. doi:10.1016/j.alit.2019.06.004
11. Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss Syndrome): practice Essentials, Pathophysiology, Etiology. (2022). Available from: https://emedicine.medscape.com/article/333492-overview?reg=1.
12. Gibelin A, Maldini C, Mahr A. Epidemiology and etiology of Wegener granulomatosis, microscopic polyangiitis, churg-Strauss syndrome and Goodpasture syndrome: vasculitides with frequent lung involvement. Semin Respir Crit Care Med. 2011;32(3):264–273. PMID: 21674413. doi:10.1055/s-0031-1279824
13. Ullah S, Ali M, Kyaw P, Nayeemuddin F, Sreedhar R, Gao J. P-ANCA negative eosinophilic granulomatosis with polyangiitis. Respir Med Case Rep. 2019;27:100830. doi:10.1016/j.rmcr.2019.100830
14. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1–11. PMID: 23045170. doi:10.1002/art.37715
15. Wechsler ME, Akuthota P, Jayne D, et al.; EGPA Mepolizumab Study Team. Mepolizumab or Placebo for Eosinophilic Granulomatosis with Polyangiitis. N Engl J Med. 2017;376(20):1921–1932. PMID: 28514601; PMCID: PMC5548295. doi:10.1056/NEJMoa1702079
16. Maloon A, Fritz VU, Kaplan CL.Neurological complications of systemic vasculitis. A report of 2 cases. S Afr Med J. 1985;68(8):603–605.
17. Chang Y, Kargas SA, Goates JJ, Horoupian DS. Intraventricular and subarachnoid hemorrhage resulting from necrotizing vasculitis of the choroid plexus in a patient with Churg-Strauss syndrome. PMID: 8097441. Clin Neuropathol. 1993;12(2):84–87.
18. Liou HH, Liu HM, Chiang IP, Yeh TS, Chen RC. Churg-Strauss syndrome presented as multiple intracerebral hemorrhage. Lupus. 1997;6(3):279–282. PMID: 9104737. doi:10.1177/096120339700600312
19. Muraishi K, Sugita K, Fujiwara S, Suzuki J, Izumiyama T, Okazaki T. [Allergic granulomatous angiitis with subarachnoid hemorrhage--a case report]. Japanese. PMID: 3398997. Basque No Shinkei Geka. 1988;16(5 Suppl):463–467
20. Ojeda E, Auzmendi A, Teresa Unanue M, Fathi O. Hemorragia cerebral en el síndrome de Churg-Strauss [Cerebral hemorrhage in Churg-Strauss syndrome]. Med Clin (Barc). 2001. 116(3):118–119. PMID: 11181295. Spanish. doi:10.1016/s0025-7753(01)71742-3
21. Calvo-Romero JM, Del Carmen Bonilla-Gracia M, Bureo-Dacal P. Churg-Strauss syndrome presenting as spontaneous subarachnoid haemorrhage. Clin Rheumatol. 2002;21(3):261–263. doi:10.1007/s10067-002-8293-4.
22. Tyvaert L, Devos P, Deloizy M, Belhadia A, Stekelorom T. Manifestations neurologiques périphériques et centrales révélatrices d’un syndrome de Churg et Strauss [Peripheral and central neurological manifestations in a case of Churg Strauss syndrome]. Rev Neurol (Paris). 2004. 160(1):89–92. PMID: 14978400. doi:10.1016/s0035-3787(04)70853-x. French.
23. Sakamoto S, Ohba S, Eguchi K, et al. Churg-Strauss syndrome presenting with subarachnoid hemorrhage from ruptured dissecting aneurysm of the intracranial vertebral artery. Clin Neurol Neurosurg. 2005;107(5):428–431. doi:10.1016/j.clineuro.2004.09.020.
24. Mishra S, Das CP, Das A, Prabhakar S. Intracerebral hemorrhage in a patient with Churg-Strauss syndrome. Neurol India. 2007;55(4):416–418. PMID: 18040124. doi:10.4103/0028-3886.37102
25. Sheerin UM, Barreto J, Brown MM, Brew S, Losseff NA. Subarachnoid haemorrhage as the first clinical manifestation of Churg-Strauss syndrome. J Neurol. 2008;255(4):607–608. doi:10.1007/s00415-008-0765-2 Erratum in: J Neurol. 2008 May;255(5):783. Erratum in: J Neurol. 2008;255(5):783. PMID: 18350356. doi: 10.1007/s00415-008-0975-7
26. Nam TS, Jung HJ, Kim JT, et al. Churg-Strauss syndrome complicated with intracerebral hemorrhage[J]. J Korean Neurol Assoc. 2009;257–259.
27. Mencacci NE, Bersano A, Cinnante CM, et al. Intracerebral haemorrhage, a possible presentation in Churg-Strauss syndrome: case report and review of the literature. J Neurol Sci. 2011;301(1–2):107–111. PMID: 21094960. doi:10.1016/j.jns.2010.10.016
28. Shimizu K, Ohoba H, Shimada H, et al. A case of Churg-Strauss syndrome with subarachnoid hemorrhage and left phrenic nerve paralysis[J]. Nihon Kokyuki Gakkai Zasshi= the Journal of the Japanese Respiratory Society. 2011;49(9):642–646.
29. Halliday J, Herrick A, Leach J. Churg-Strauss, a rare cause of intracerebral haemorrhage. J Clin Neurosci. 2012;19(8):1177–1178. doi:10.1016/j.jocn.2012.01.006.
30. Go MH, Park JU, Kang JG, Lim YC. Subarachnoid and intracerebral hemorrhage in patients with Churg-Strauss syndrome: two case reports. J Cerebrovasc Endovasc Neurosurg. 2012;14(3):255–261. PMID: 23210058; PMCID: PMC3491225. doi:10.7461/jcen.2012.14.3.255
31. Menditto VG, Di Rienzo A, De Nicola M, Balzano L, Polonara S. Subarachnoid haemorrhage from PICA aneurysm rupture in a Churg-Strauss patient: a case report and a review of the literature. Clin Neurol Neurosurg. 2013;115(2):197–199. PMID: 22683043. doi:10.1016/j.clineuro.2012.04.025
32. Ito M, Kato N, Su CC, Kayama T.A case of Churg-Strauss syndrome with subarachnoid hemorrhage. Brain Nerve. 2014;66(3):283–288.
33. Taormina G, Andolina G, Banco MA, Costanza-Gaglio EJ, Bonura A, Buscemi S. An uncommon presentation of eosinophilic granulomatosis with polyangiitis: a case report. J Med Case Rep. 2014;8(1):190. PMID: 24928069; PMCID: PMC4086703. doi:10.1186/1752-1947-8-190
34. Diamanti L, Berzero G, Bini P, et al. Spinal hemorrhage in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). J Neurol. 2014;261(2):438–440. PMID: 24368404. doi:10.1007/s00415-013-7217-3
35. Sylvain L, Rondeau-Lutz M, Camille M, et al. Subarachnoid Haemorrhage in patient with Eosinophilic Granulomatosis with Polyangiitis (Churg and Strauss): a probable central nervous localisation of vasculitis[J]. Int J Brain Disord Treat. 2015;1(006). doi:10.23937/2469-5866/1510006.
36. Sharma SR, Habung H, Hussain M. Churg-Strauss syndrome in a pediatric patient presenting with recurrent hemorrhagic stroke and mitral regurgitation due to a prolapsed mitral valve. Neurol India. 2016;64(4):827–830. doi:10.4103/0028-3886.185374.
37. Ullah Z, Abideen ZU, Shoaib RF, Ahmad A, Zaman Q, Nazir R. Eosinophilic granulomatosis with polyangiitis presenting with multiple intracerebral haemorrhages - A case report. PMID: 27812073. J Pak Med Assoc. 2016;66(11):1481–1483.
38. Mattsson G, Magnusson P. Eosinophilic granulomatosis with polyangiitis: myocardial thickening reversed by corticosteroids. BMC Cardiovasc Disord. 2017;17(1):299. PMID: 29262787; PMCID: PMC5738832. doi:10.1186/s12872-017-0734-8
39. Lee MXW, Teng GG, Raju GC, Lim AYN. Catastrophic subarachnoid hemorrhage in eosinophilic granulomatosis with polyangiitis without asthma. Int J Rheum Dis. 2017;20(12):2127–2131. doi:10.1111/1756-185X.12594
40. Matsuda S, Yoshida S, Fujiki Y, et al. Eosinophilic granulomatosis with polyangiitis complicated by subarachnoid hemorrhage and coronary vasculitis: a case report and review of the literature. Rheumatol Int. 2018;38(4):689–696. PMID: 29127573. doi:10.1007/s00296-017-3875-2
41. Yamada Y, Ando S, Umeda Y, Umeda M, Oyake M, Fujita N. A case of multiple cerebral hemorrhage caused by sudden increase of eosinophil in a patient with eosinophilic granulomatosis with polyangiitis. Rinsho Shinkeigaku. 2018;58(9):565–569. [Japanese]. doi:10.5692/clinicalneurol.cn-001188
42. Hira K, Shimura H, Kamata R, et al. Multiple cerebral infarction diagnosed as Eosinophilic Granulomatosis with Polyangiitis by autopsy. BMC Neurol. 2019;19(1):288. PMID: 31729970; PMCID: PMC6857209. doi:10.1186/s12883-019-1515-z
43. Southam C, Hahn C. Intracerebral and Spinal Subarachnoid Hemorrhage in Eosinophilic Polyangiitis. Can J Neurol Sci. 2019;46(4):475–476. PMID: 31179954. doi:10.1017/cjn.2019.63
44. Mrackova J, Holeckova I, Rohan V, et al.Eosinophilic granulomatosis with polyangiitis-an uncommon cause of intracerebral and subarachnoid hemorrhage: a case report[C]//international journal of stroke 1 olivers yard, 55 city road, london ec1y 1sp england sage pubications ltd 2020 vol. 151_ suppl 670
45. Lázaro Romero A, Carilla Sanromán A, Horna Cañete L, Serrano Ponz M. Spontaneous spinal epidural haematoma and nonaneurysmal subarachnoid haemorrhage in a patient with eosinophilic granulomatosis with polyangiitis. Neurologia. 2021;36(9):723–725. PMID: 34261616. doi:10.1016/j.nrleng.2020.12.002
46. Burtson KM, Bishop J. Prevasculitic Eosinophilic Granulomatosis With Polyangiitis. Cureus. 2021;13(4):e14649. PMID: 34055509; PMCID: PMC8144070. doi:10.7759/cureus.14649
47. Frikha F, Ellouz E, Damak C, Hentati Y, Mekki S, Bahloul Z. Intracerebral hemorrhage revealing eosinophilic granulomatosis with polyangiitis (EGPA): a case report. Rev Neurol (Paris). 2022;178(6):631–633. PMID: 34920894. doi:10.1016/j.neurol.2021.10.009
48. Mino T, Sakaguchi H, Hasegawa I, et al. Multiple cerebral infarctions accompanied by subcortical and subarachnoid hemorrhaging in bilateral border zone areas in a patient with Eosinophilic Granulomatosis with Polyangiitis. Intern Med. 2022;61(6):891–895. PMID: 34483211; PMCID: PMC8987242. doi:10.2169/internalmedicine.7999-21
49. Mutoh T, Shirai T, Sato H, Fujii H, Ishii T, Harigae H. Multi-targeted therapy for refractory eosinophilic granulomatosis with polyangiitis characterized by intracerebral hemorrhage and cardiomyopathy: a case-based review. Rheumatol Int. 2022;42(11):2069–2076. PMID: 34287685. doi:10.1007/s00296-021-04950-z
50. Guerra M, Marado D, Fortuna J. Acute paraplegia in a patient with eosinophilic granulomatosis and polyangiitis with 20 years of evolution: case report. Acta Biomed. 2023;94(6):e2023243. doi:10.23750/abm.v95i1.14209
51. Mahmood K, Butt NI, Ashfaq F, Aftab S. Eosinophilic Granulomatosis with (EGPA): a case report with atypical presentation. Pak J Med Sci. 2023;39(1):307–309. PMID: 36694733; PMCID: PMC9842979. doi:10.12669/pjms.39.1.6436
52. Satake Y, Sakai S, Takao T, Saeki T. A case of subarachnoid haemorrhage associated with MPO-ANCA-positive eosinophilic granulomatosis with polyangiitis, successfully treated with glucocorticoid, cyclophosphamide, and mepolizumab. Mod Rheumatol Case Rep. 2024;8(2):310–313. PMID: 38109745. doi:10.1093/mrcr/rxad071
53. Nie N, Liu L, Bai C, et al. Eosinophilic granulomatous polyangiitis with central nervous system involvement in children: a case report and literature review. Front Immunol. 2024;15:1406424. PMID: 38812515; PMCID: PMC11133702 doi:10.3389/fimmu.2024.1406424
54. Li G, Liu XR, Yang LJ. Multiple intracerebral hemorrhages secondary to eosinophilic granulomatosis with polyangiitis: a case report and literature review. Kaohsiung J Med Sci. 2024;40(10):949–950. PMID: 39158219. doi:10.1002/kjm2.12882
55. Li Y, Chen Z, Zhu S, et al. Negative anti-neutrophil cytoplasmic antibodies and eosinophilic granulomatosis with polyangiitis accompanied by cough variant asthma: a case report. Ann Palliat Med. 2021;10(10):11209–11215. PMID: 34763478. doi:10.21037/apm-21-2236
56. Chung SA, Langford CA, Maz M, et al. American college of rheumatology/vasculitis foundation guideline for the management of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheumatol. 2021;73(8):1366–1383. PMID: 34235894. doi:10.1002/art.41773
57. Chen KR, Pittelkow MR, Su D, Gleich J, Newman W, Leiferman KM. Recurrent cutaneous necrotizing eosinophilic vasculitis. A novel eosinophil-mediated syndrome. Arch Dermatol. 1994;130(9):1159–1166. [PMID: 7522002]. doi:10.1001/archderm.1994.01690090083012
58. Kataoka H, Tomita T, Kondo M, Mukai M. Presence of purpura is related to active inflammation in association with IL-5 in eosinophilic granulomatosis with polyangiitis. Rheumatol Int. 2021;41(2):449–454. doi:10.1007/s00296-020-04672-8
59. Robson JC, Grayson PC, Ponte C, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Arthritis Rheumatol. 2022;74(3):393–399. doi:10.1002/art.41986
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Chronic Atopic Dermatitis with Eosinophilia Improved by Daesiho-Tang: A Case Report

Park MC, Lee JH, Seong EJ, Lee DS, Jo EH
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2561-2572
Published Date: 20 September 2023