")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Knowledge of, Attitudes toward, Barriers to, and Uptake Rate of Influenza Virus Vaccine among Adults Aged ≥65 Years in Jordan: A Multicenter Cross-Sectional Study
Authors Abu-Helalah M , Al-Hanaktah M , Almadani M , Asfour A , Batarseh FE, Abdelhadi NN , Al Odat BA , Sharkas SG, Alhashaika Jnr AI
Received 18 February 2025
Accepted for publication 11 June 2025
Published 26 June 2025 Volume 2025:18 Pages 2121—2137
DOI https://doi.org/10.2147/RMHP.S521918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Kyriakos Souliotis
Munir Abu-Helalah,1,2 Mohammad Al-Hanaktah,3 Mary Almadani,4 Amro Asfour,3 Fadi Essam Batarseh,5 Nadine N Abdelhadi,6 Baraa Ayed Al Odat,7 Satani G Sharkas,8 Alaa Ibraheem Alhashaika Jnr9
1Department of Family and Community Medicine, Faculty of Medicine, University of Jordan, Amman, 11942, Jordan; 2Public Health Institute, University of Jordan, Amman, 11942, Jordan; 3Faculty of Medicine, University of Jordan, Amman, 11942, Jordan; 4Jordan Hospital, Amman, 11152, Jordan; 5Ministry of Health, Amman, 11931, Jordan; 6Department of Clinical Pharmacy and Pharmacy Practice, Aqaba University of Technology, Aqaba, 11191, Jordan; 7Internal Medicine Department, Jordan University Hospital, Amman, 11942, Jordan; 8Internal Medicine Department, St. Elizabeth’s Medical Center, Boston, MA, 02118, USA; 9Specialty Hospital, Amman, 11193, Jordan
Correspondence: Munir Abu-Helalah, Email [email protected]
Purpose: Seasonal influenza significantly impacts global health, especially among high-risk groups such as the elderly. People aged ≥ 65 years have the highest morbidity and mortality due to influenza infections. Despite international recommendations, influenza vaccine-uptake rates remain low in many regions worldwide. In Jordan, data on influenza vaccine uptake in people aged ≥ 65 years is lacking. This study aimed to assess vaccination rates, knowledge, attitudes, and barriers among the elderly in Jordan.
Methods: This national cross-sectional study included 455 adults aged ≥ 65 years living at representative sites in Jordan in Amman, Irbid, Zarqa, and Karak. The study questionnaire was based on the health belief model and included data on demographics, influenza vaccination history, and knowledge of, attitudes toward, perceptions of, and barriers to influenza vaccine uptake.
Results: Only 11.4% of participants received the influenza vaccine in the 2022– 2023 season, while 30.1% had ever been vaccinated. Rural residents, higher-income groups, and those insured by private institutions demonstrated higher vaccination rates of 14% and 15.4%, respectively (P< 0.05). Barriers to being vaccinated included perceived low susceptibility (43.7%), concerns about adverse effects (52.7%), and lack of social network recommendations (38.9%). Positive predictors included trust in vaccination guidelines, higher perceived risk, and health-care provider advice (P< 0.001).
Conclusion: Influenza vaccination rates among older adults in Jordan are low compared to regional and international data. Interventions tailored to address barriers are needed to improve awareness, accessibility, and trust to reduce influenza-related morbidity and mortality.
Keywords: influenza vaccines, elderly, above 65, uptake, barriers, attitudes, Jordan
Introduction
Vaccines are considered among the most important primary prevention measures in history.1 Vaccination uptake among adults and high-risk groups is a global issue that requires much effort from stakeholders concerned at local and international levels.2 International initiatives such as the Expanded Program on Immunization and Global Alliance for Vaccines and Immunization have shown great success in the implementation and expansion of pediatric immunization programs. Nevertheless, there are challenges still facing vaccine uptake among elderly people and other high-risk groups.3
Seasonal influenza is a highly contagious acute respiratory infection caused by influenza viruses. Globally, it is a major cause of morbidity and mortality: annual estimates of severe illness can reach 5 million cases, with about 500,000 deaths worldwide.4 In high-risk groups, such as those aged ≥65 years, influenza epidemics can cause serious illness and death. People aged ≥65 years at higher risk of severe influenza clinical presentations and serious complications. This is due to age-associated decline in immunity and the presence of comorbidities.5 The US Centers for Disease Control and Prevention (CDC) reported that 50%–70% of hospitalizations and 70%–85% of influenza-related deaths occurred among people aged ≥65 years during the season of 2019–2020.6
Similarly high morbidity and mortality figures among people aged ≥65 years have been reported from the World Health Organization and European Centre for Disease Prevention and Control.7,8 According to the CDC, all people who are aged ≥6 months old are recommended to receive the seasonal influenza vaccine annually.9 Conversely, the World Health Organization and some countries have limited the recommendation to only high-risk groups, such as children aged 6 months to 5 years, those aged ≥65, the pregnant, those with chronic diseases, and health-care providers.10–12 The majority of influenza mortality occurs in people over the age of 65–70 years.13,14 Contracting influenza at this age can lead not only to death but also to severe cardiac and respiratory complications.15
Studies have revealed that the challenges facing vaccination among older adults fall into three main areas. The first is government-related, where priority is given to childhood immunization with full cost coverage, as opposed to adult vaccinations being either partially subsidized or not covered at all. This is in addition to limited surveillance of infectious diseases leading to limited vaccine effectiveness and safety data for older adults. The final area is individual-related: cost of the vaccine, low uptake rate, lack of insurance cover, limited information and awareness, and misconceptions.16
The health belief model (HBM) has been utilized to guide the assessment of physicians’ perceptions and attitudes toward influenza vaccination.17 It was developed in the 1950s based on two theories — cues to action and cognitive — for exploring different health-related behaviors. The HBM explains that the individual will take an action if he/she believes that he/she is susceptible to a disease or health problems if the occurrence of this disease will affect her or his life, if taking a preventive measure will prevent the disease or reduce its severity, and if this action does not have many barriers or limitations. The model was further reformulated to include two categories: cues to action and health motivation or self-efficacy.18,19 The HBM has been widely used to study influenza vaccine uptake among the general population and high-risk groups. It has been also used to assess reasons for people aged ≥65 years to take the influenza vaccine,20–22 reasons for health-care workers to accept influenza vaccines (or not),23,24 and in generating data for the development of intervention programs to improve influenza vaccine uptake among people aged ≥65 years.
In Jordan, influenza infections constitute a major health and economic burden, contributing to 9% of admissions with severe acute respiratory infections according to data from the Jordanian Ministry of Health for cases aged 31 days or older.25 The influenza vaccine is not routinely administered to people aged ≥65 in Jordan. Alternatively, it can be received through a physician’s prescription or directly from community pharmacies.26 Therefore, it we decided to conduct a national cross-sectional study on uptake rate, knowledge of, barriers to, and beliefs about the influenza vaccine in people aged ≥65 years among a representative sample from Jordan for the flu season 2022–2023.
Methods
Study Design
The study used a cross-sectional design to assess knowledge of, attitudes toward, barriers to, and uptake of the influenza virus vaccine among adults aged ≥65 years in Jordan. Data were collected using a structured self-administered questionnaire in a representative sample of Jordan stratified into middle, northern, and southern regions.
Study Population and Inclusion Criteria
The study targeted Jordanian nationals aged ≥65 years who were residing permanently in the selected study areas, excluding those not living permanently in these areas and individuals with contraindications for the influenza vaccine.
Sample Size
Jordan’s population is 11,337,052, 4% of which are older than 65 years, giving an estimated number of 453,482 potential subjects. Based on a previous study from Jordan, where the uptake rate of those who had ever been vaccinated was 20%,27 a sample size of 425 subjects was required to achieve a 95% significance level with a 5% margin of error.
Statistical Analysis
SPSS version 28.0 was used to analyze the data. Frequencies and percentages are used to represent the categorical variables. Chi-squared analysis was utilized to estimate associations between all baseline characteristics, knowledge level, and vaccination status. Binary logistic regression was performed to identify predictors of vaccine uptake during the 2022–2023 season and predictors of having ever been vaccinated against influenza. The effects of particular baseline characteristics on each barrier item were investigated using stepwise regression, and the effects of all HBM variables on participants’ attitudes toward vaccination were investigated using multiple linear regression.
Sampling Technique
Multistage sampling was utilized for the Amman and Zarqa governorates, representing the central region, the Irbid governorate, representing the northern region, and the Karak governorate, representing the southern region. The sample was distributed between rural and urban areas and included subjects from different socioeconomic-class areas through a door-to-door approach. Every city included was stratified by socioeconomic class. Household members were asked if they had someone aged ≥65 years or children younger than 5 years living with them. The study included other groups, such as children younger than 5 years. Data about children younger than 5 years will be published in a separate article. Only one participant aged ≥65 years was included from each household. For children, parents were interviewed as guardians. Research coordinators were allocated to areas, then within each team, with two members visiting specific streets to avoid visiting the same household.
Data-Collection Procedure
Data collection was scheduled across different days of the week to capture a representative sample. Trained interviewers assisted the participants as needed to ensure accurate completion of the questionnaire and thank the participants for their time when they were finished. Data were collected between February and June 2023 for vaccine uptake for the season of 2022–2023. The vaccine is recommended in Jordan in October annually, but was given until early December 2022.
Study Tool
A structured questionnaire that was specifically developed for this study was utilized. The questionnaire was developed based on validated questionnaires, then translated to Arabic through a backward–forward translation process conducted by public health experts.20–22Our questionnaire included demographic data, medical and drug history, vaccine history, and socioeconomic factors. Furthermore, sections on influenza vaccine uptake and knowledge, perceived barriers, attitudes, and beliefs regarding influenza vaccination were included together with items informed by the HBM to assess factors influencing vaccine uptake. The following components of the HBM were used in the study: participants’ perceived risk of getting influenza (perceived susceptibility), their belief in the resulting consequences on them (perceived severity), the potential positive benefits of the influenza vaccine (perceived benefits), perceived barriers to the influenza vaccine, exposure to factors that prompt action (cues to action), and modifying variables (a person’s characteristics).18,19
According to the HBM, the willingness of a subject to receive the influenza vaccine depends on the following beliefs or conditions. Is he/she susceptible to influenza? Is the threat of influenza serious to his/her health? Do the benefits of taking the vaccine outweigh the barriers? Is he/she confident that they can obtain the vaccination successfully? Are there cues to action present to motivate him/her to take the vaccine?18–22The questionnaire was piloted on 30 eligible participants from the study areas to ensure clarity and relevance to the target population. Feedback was used to adjust language, length, and format as needed.
Reliability assessment based on Chronbach’s alpha showed an average score of 0.82, with results between 0.77 for perceived susceptibility to influenza infections and 0.87 for perceived barriers to vaccination. Face validity and content validity were met because all components of the HBM were included, along with assessment of the uptake rate. Items were assessed according to the HBM based on previous studies and our experience in the field. Construct validity was assessed using exploratory factor analysis, which was performed using principal-component analysis and varimax rotation. The minimum factor-loading criterion was set to 0.5. The commonality of the scale, which indicates the amount of variance in each dimension, was also assessed to ensure acceptable levels of explanation. All the items that fit with all commonalities were >0.5.
Results
Survey Participants’ Demographics, Health Conditions, and Influenza Vaccination Rates
A total of 455 participants completed the survey, with a mean age was 69.39±9.6 years. The response rate was 99%. Only five potential participants declined participation because they were not interested in completing study questionnaires. Of these, 55.4% were females and the majority (75.4%) resided in urban areas. Additionally, 47% had a school-level education and more than half (54.7%) were unemployed. The Ministry of Health provided the majority of health insurance (53.8%), while 13.2% of participants reported having no insurance coverage (Table 1).
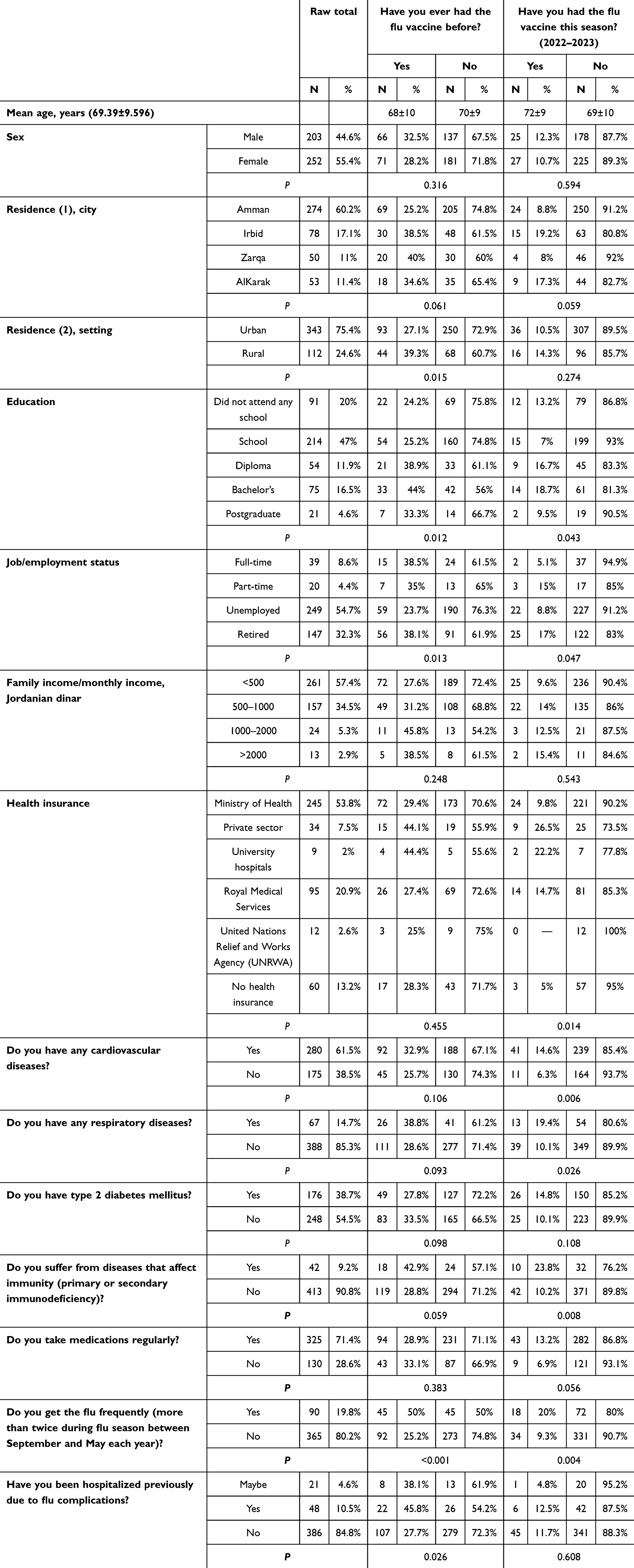 |
Table 1 Baseline characteristics and of participants by vaccination status |
In terms of disease and medication status, 61.5% of individuals reported suffering from cardiovascular diseases, followed by type II diabetes mellitus, reported in 38.7% of study subjects and chronic respiratory disorders (14.7%). Overall, 71.4% of individuals reported taking medications regularly. Among those surveyed, 19.8% reported getting the flu frequently, and 10.5% had been hospitalized due to influenza complications.
Influenza Vaccine Uptake Rate
This study revealed a low influenza vaccine uptake rate among people aged ≥65 years, with 30.1% having previously been immunized and only 11.4% having received the vaccine during the 2022–2023 season. As shown in Table 1, studying the association of sociodemographic factors revealed that individuals who lived in rural regions were more likely to have ever received a vaccination (P=0.015; 39.3% vs. 27.1% in urban areas). Additionally, having a bachelor’s degree and being currently employed or retired were substantially correlated with having ever received vaccination (P=0.012 and P=0.013, respectively) and with receiving a vaccination that season (P=0.043 and P=0.047, respectively). That season’s vaccination uptake was highest among those insured by private health insurance and by university hospitals (26.5% and 22.2%, respectively) vs. 9.8% among those having Ministry of Health insurance and 5% in subjects who had no health insurance coverage whatsoever (P=0.014). More than half the participants (57.4%) reported a low income (<500 Jordanian dinar).
Table 1 also shows the influenza vaccine uptake rate against medical history. Among individuals diagnosed with cardiovascular disease, 14.6% received the flu vaccine that season (P=0.006) while 19.4% of those with respiratory disorders and 23.8% of those with immunosuppressive conditions were vaccinated that season (P=0.026 and P=0.008, respectively). Regarding reported history of influenza infections, 19.8% reported getting flu infections frequently. Half of the participants who reported frequent flu episodes reported having been (P<0.001 and P=0.004, respectively). Moreover, 10.5% of participants reported having been hospitalized due to influenza/flu-like illness complications. This group had a statistically higher rate of ever receiving the influenza vaccine when compared to those who were not hospitalized (45.8% and 27.7%, P=0.026).
General Attitudes toward Influenza Vaccine
Interestingly, 28.8% of the participants strongly agreed or agreed with the statement “I am against flu vaccine”, with correspondingly low uptake rates of influenza vaccine. Half of the participants strongly disagreed or disagreed with this statement and had a statistically higher uptake of vaccine for that season or ever having been vaccinated when compared to the former group (2.3% vs. 20.4%, P<0.001 and 8.4% vs. 48.2%, P<0.001). Those with a neutral opinion constituted 21.5% of the participants, with an intermediate level of influenza vaccine uptake rates of 17.3% for having ever been vaccinated against influenza and 3.1% vaccinated for that season of influenza.
Participants’ Knowledge of and Perspectives on Influenza and Vaccination
The knowledge part of the questionnaire on influenza and vaccination is shown in Table 2. A large proportion (43.5%) thought that influenza was moderately contagious, while almost half (48.6%) acknowledged that it could cause only minor infections, doctor’s visits, or hospitalization. Interestingly, 39.6% of all study participants believed that annual vaccination was unnecessary, while the majority (53.4%) saw that combining vaccination with abiding with the required safety precautions was the best preventive method. The vaccine’s perceived efficacy and safety received moderate mean values of 6.14±2.49 and 6.25±2.61 (Table 2).
 |
Table 2 Associations between perceived knowledge about flu, flu vaccine, and vaccination status |
In terms of perceived knowledge of influenza and influenza vaccine uptake rate, individuals who believed influenza was extremely contagious had higher vaccination rates than those who thought it not contagious: 35.2% vs. 33.3% (P=0.017) had been previously vaccinated and 13.8% vs. 11.1% (P=0.02) had been vaccinated that season. Participants who believed flu could cause hospitalization had higher vaccination rates than those who thought it only caused mild disease (25% vs. 18.8% previously, 25% vs. 5.2% that season; P<0.001). Regarding vaccine timing, individuals who knew the vaccine was provided in autumn had the highest uptake, with 45.1% having been previously vaccinated and 22.9% that season (P<0.001). Likewise, individuals who knew that the vaccine was provided in October demonstrated substantial vaccination rates (33.3% previously and 17.2% that season, P<0.001; Table 2).
Perceptions of, Barriers to, and Predictors of Influenza Vaccine Uptake
Individuals who strongly agreed or agreed with the statement that “Without the vaccine, I feel like I’m at high risk of getting the flu” had higher rates of vaccination for that season (2022–2023; 26.1%) and for having ever been vaccinated (59.2%) than those who disagreed or strongly disagreed (3.5%, P<0.001 and 13.4%, P<0.001, respectively). People who strongly agreed or agreed that they would experience severe symptoms if infected had higher rates of vaccination for that season (17.1%) and in the past (44.9%) compared to those who disagreed (5.5%, P=0.002 and 17.5%, P<0.001 respectively; Table 3).
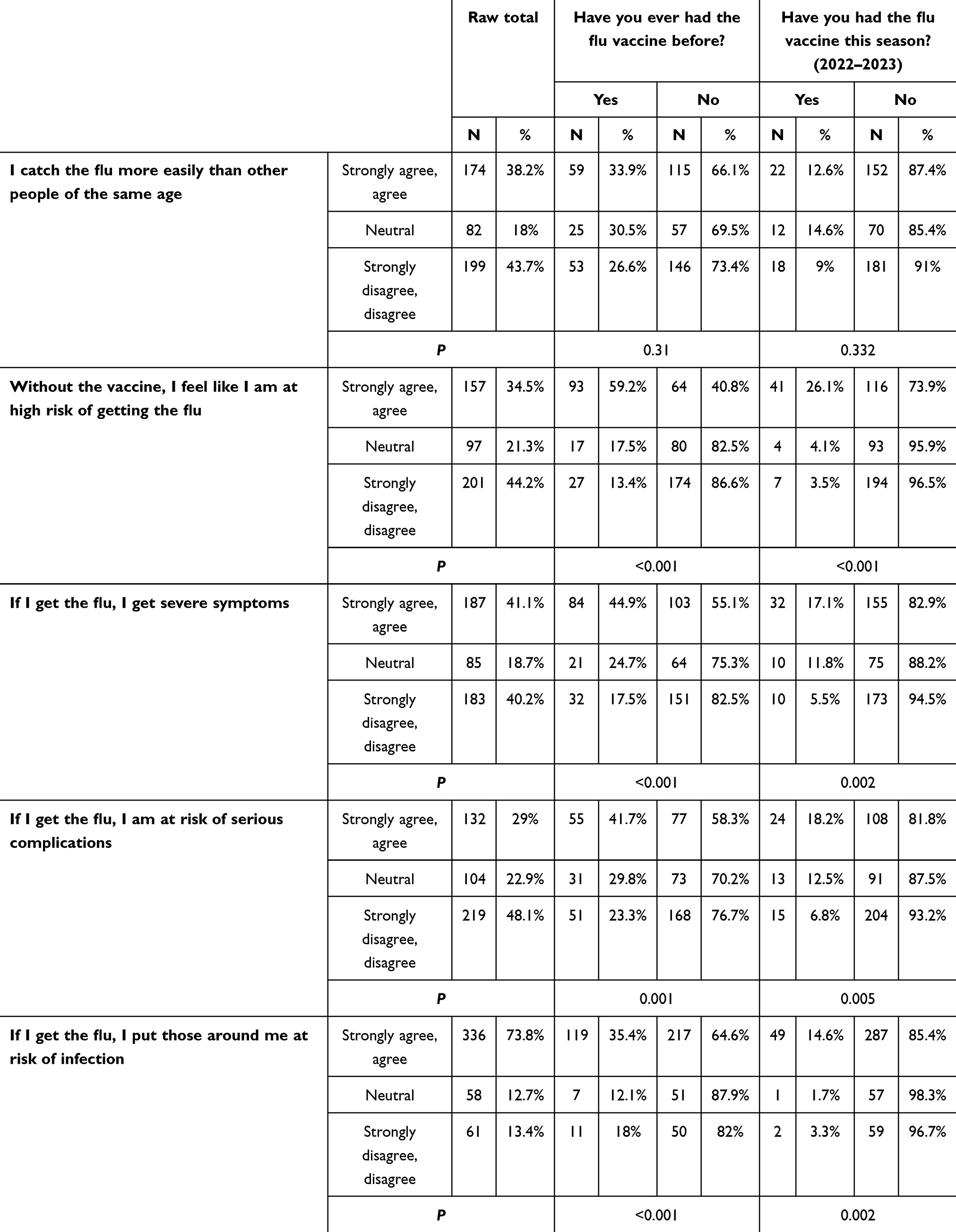 |
Table 3 Associations between perceived susceptibility and severity of influenza and vaccination status |
Around 29% of the study participants agreed or strongly agreed with the statement “If I get the flu, I am at risk of serious complications.” Uptake of the vaccine was significantly higher than those who strongly disagreed or disagreed with or were neutral on this statement for both having ever been vaccinated (41.7% vs. 23.3% vs. 29.8%, P=0.001) or having been vaccinated that season against flu (18.2% vs. 6.8% vs. 12.5%, P=0.005). Of those who agreed that they put others at risk, 14.6% had received the vaccine during that season and 35.4% had received it in the past compared to those who disagreed (3.3%, P=0.002 and 18%, P<0.001, respectively; Table 3).
Supplementary Table 1 shows a high association between vaccination status and the perceived benefits of the influenza vaccine. Of those who strongly thought that the flu vaccine would ease their worries of being ill, 49.8% had previously been vaccinated and 21.1% had received the vaccine that season compared to 11.2% who had ever been vaccinated and 0.9% for having been vaccinated that season in those who disagreed or strongly disagreed with the statement (P<0.001). Those who reported that they would benefit from the vaccine were more likely to receive it, with 19.2% having received it that season and 45.9% ever having received it compared to 4.2% and 0, respectively, for those who disagreed with the statement (P<0.001 for both). Finally, those who agreed that getting the vaccine would decrease the spread of the flu around them had higher vaccination rates than those who disagreed for both groups: having ever been vaccinated (42.3% vs. 9.5%, P<0.001) and having been vaccinated during the season of 2022–2023 (17.6% vs. 2.4%, P<0.001).
Concerns about adverse vaccine effects, disliking the vaccinations, misconceptions about the vaccine’s ability to cause influenza, lack of information, and lack of encouragement from family or peers were all major barriers to vaccination with statistically significant differences between those who reported these barriers and those who disagreed with them as barriers to their vaccine uptake. Other concerns about affordability and availability also significantly influenced vaccination rates (Table 4).
 |
Table 4 Associations between perceived barriers and vaccination status |
Health-care providers’ recommendations had a considerable impact on immunization behavior in terms of cues to action. Among individuals who strongly agreed with these recommendations, 12.5% had received the vaccine that season and 36.4% had previously received the vaccine compared to 3.7% (P<0.001) and 19.5% (P<0.001), respectively, for those who disagreed with the statements. Trust in the vaccination guidelines had a significant impact, with 39% having previously been vaccinated and 13.6% having been vaccinated that season compared to 17.2% (P<0.001) and 3.2% (P<0.001), respectively, in those who disagreed. Participants who felt well informed were more likely to have been vaccinated, 44% of whom had had previous vaccinations and 14.9% having been vaccinated that season compared to 17.3% (P<0.001) and 5.1% (P<0.001), respectively, in those who disagreed (Supplementary Table 2).
Supplementary Table 3 shows participants’ responses to other factors that may predict vaccination rates. Advice from physicians, nurses, and family members or relatives were important predictors of influenza vaccine uptake. The logistic regression analysis shown in Table 5A highlights multiple significant predictors by HBM domain of having ever been vaccinated. It emphasizes the critical factors that influence vaccination status. Monthly household income (OR 1.23, P=0.025), perceived risk without the vaccine (OR 1.63, P=0.008), trust in vaccination guidelines (OR 1.99, P<0.001), having health insurance (OR 1.52, P=0.004), and doctor’s advice (OR 2.39, P<0.001) all significantly increased the odds of being vaccinated.
 |
Table 5 Logistic regression analysis for influenza vaccine uptake |
Likewise, a number of important predictors of influenza vaccination in the current year by HBM domain are shown by the logistic regression analysis in Table 5B. Vaccination was positively correlated with health insurance status (OR 1.45, P=0.002), doctor’s advice (OR 2.30, P<0.001), perceived risk without vaccination (OR 1.52, P=0.005), and monthly family income (OR 1.26, P=0.015). Conversely, the chance of having had the vaccine that season inversely correlated with having a cardiovascular illness (OR 0.85, P=0.03).
Discussion
This study revealed low influenza vaccine uptake overall among people aged ≥65 years, where only 11.4% had received the vaccine during the 2022–2023 season and 30.1% reporting having ever been vaccinated against influenza. These figures are higher than those in a previous study from Jordan, where influenza vaccine uptake was 1.2% for the season of 2017–201828 based on a convenience sample from community pharmacies and public places. A study from Saudi Arabia revealed that 47.8% of study participants aged ≥65 years (n=496) had been vaccinated against influenza at least once. Another survey of influenza vaccine coverage in Saudi Arabia conducted in 2017 reported rates of 44.5% for having ever been vaccinated against influenza.29 Other reports of influenza vaccine coverage from the Middle East and Western countries have also shown higher rates than the figures reported in our study from Jordan.26,30 Although regional figures of influenza vaccine uptake are higher than ours, they are still lower than those reported from Europe. For example, data from the UK revealed that influenza vaccine uptake was 64% in 65- to 69-year-olds, 74% in 70- to 74-year-olds, and 80% in those aged ≥75 years.28,31 Influenza vaccination is a public health necessity in this vulnerable age group due to the increased risk of more severe consequences. Low vaccination uptake rates significantly contribute to the global burden of the disease, despite the fact that the influenza vaccine is widely accessible.32–34
Several studies have indicated that the uptake of influenza vaccination among this vulnerable group remains low worldwide, even though influenza vaccination decreases the incidence of influenza-related hospitalization and mortality.21,32–35 Regardless of the discrepancies between developed and developing countries’ vaccine uptake rates, influenza infection is still imposing high morbidity and significant mortality for people aged ≥65 years. Data from the USA for the season matching this study, 2022–2023, revealed that the mortality rate from influenza in the United States is by far the highest among those aged ≥65 years, with rates reaching around 26.6 per 100,000 population.
Individuals living in rural regions were more likely to have ever received a vaccination than those in urban areas. Interestingly, the reported influenza uptake patterns differ from those reported in the literature for other high-risk groups, such as children, where reported vaccine uptake rates in urban areas are statistically much higher than those in rural areas.36,37 Our study also showed that residents of the capital were less likely to receive the influenza vaccine when compared to residents of other cities in the north or the south of Jordan. This might be justified by the fact that health-care centers are less busy in rural areas outside the capital, enabling physicians to allocate more time to discuss the influenza vaccine and other preventive measures with elderly subjects. This is consistent with a study from Spain that showed that rural residents, particularly in small rural counties (80.8%), were more dependent upon clinical settings than urban residents (69.1%) for influenza vaccinations. In adjusted analyzes, living in a large or small rural county remained significantly related to increased odds of being vaccinated in a clinical setting (OR 1.17, 95% CI 1.06–1.29 and OR 1.45, 95% CI 1.24–1.69, respectively).38–41
However, the low overall rates for this high-risk group of people aged ≥65 years revealed that they face multiple barriers to vaccine access and delivery. Their lower overall rate of preventive services receipt13,14 may be due to insufficient services, fewer traditional health-care settings, higher rates of poverty and uninsured people, and longer distances to sources of care, particularly in rural areas.14
Education level and employment status were also substantially correlated with vaccination uptake: individuals with a bachelor’s degree had higher vaccination rates. Only school education or not having attended school showed lower vaccine uptake rates. This differs from the findings of a large study investigating the barriers to county-level seasonal influenza vaccinations by United States Medicare beneficiaries during the influenza season.35 The study aimed to quantify flu vaccination rates at the county level among Medicare-eligible individuals aged ≥65 years. The proportions of individuals with a college degree or higher, those with weak English proficiency, and those residing in multi-unit housing and single-parent households were significantly and favorably correlated with higher influenza vaccination uptake.35 Similarly, educational attainment was reported to be among the most significant characteristics positively influencing influenza vaccination uptake rates in Hungarian adults aged ≥65.32
Half of the study participants who reported frequent flu episodes were significantly more likely to having previously been vaccinated. A recent study from Saudi Arabia revealed that awareness of the severity of influenza infections was one of the key predictors of influenza vaccine uptake.42 Similarly, a recent study on attitudes and perceptions among individuals in Singapore toward influenza vaccination uptake indicated that the motivation for vaccination by individuals aged ≥65 was primarily derived from previous positive vaccination experiences.21
Lack of perceived susceptibility was a key barrier to influenza vaccine uptake in our study. The abovementioned study from Singapore revealed that one of the reported barriers to influenza vaccine uptake was the belief that the influenza virus causes a minor infection and that annual vaccinations are unnecessary.21 The reported misconceptions mirrored those reported in the literature previously, including the belief that vaccines were only necessary before travel.21,43,44 In addition, similarly to previous studies, most elderly individuals, particularly those who did not take the influenza vaccine, neither believed in the efficacy of influenza vaccines nor perceived influenza infection as a potentially serious disease.45
Concerns about potential adverse events of the vaccine were among the major barriers to vaccination. This is consistent with previous studies indicating that adverse events are frequently reported as reasons for not receiving the vaccine.21,32–36 This is also consistent with a recent regional study from Saudi Arabia, where fear of influenza vaccine side effects was the key barrier for influenza vaccine uptake.42 Furthermore, concerns about affordability and availability also significantly influenced vaccination rates. This could be further investigated to strategically guide policies to implement universal health coverage.
Health-care providers’ recommendations impacted immunization behavior considerably. This was one key finding where study participants who felt well informed by health-care providers about the influenza vaccine were more likely to be vaccinated. Previous studies also underscored the role of physicians’, nurses’, and family members’ or relatives’ advice as important predictors of influenza vaccine uptake21,36,37,43,44,46–48 A nationwide cross-sectional survey of UK general practices to increase influenza vaccination rates in primary care reported that uptake rates were positively influenced by the availability of a primary staff member for planning the flu campaign and producing a written report of practice performance.43 These strategies enhanced the vaccination rates in patients aged ≥65 years. Significantly improved flu vaccination rates were independently linked to clear health-care leadership, effective communication regarding performance, and the methodologies employed to identify and contact eligible patients.43 In addition, recent clinical trials revealed that health literacy and health education methodologies positively affected influenza vaccination uptake among individuals aged ≥65 years.46–48 It is evident that health-care personnel and family members are significant influencers in the decision-making process of older adults and should be actively pursued in future health-promotion initiatives.
This study has several areas of strength, firstly covering one of the important areas of need in Jordan and developing countries, influenza vaccination at age of risk of influenza complications, selection of a large and representative sample, utilizing face-to-face interviews to ensure completeness of the data, and finally using a comprehensive survey based on the HBM. On the other hand, depending on self-reporting for uptake rates may constitute a limitation in the study, and reported history of admissions due to influenza infections was not investigated further through medical notes of the study participants either.
Conclusion
This study revealed a low uptake rate of influenza vaccine among people aged ≥65 years in Jordan. In order to reduce morbidity and mortality from influenza infections among this high-risk group, it is essential to ensure high annual influenza vaccine coverage rates in Jordan. This study also provided a comprehensive understanding of perceptions of, attitudes toward, cues to action, and barriers to influenza vaccine uptake among the elderly in Jordan. Actions and interventions should be tailored to leverage predictors of influenza vaccine uptake, such as providing free vaccines for low-income groups, active involvement of physicians in the promotion of the influenza vaccine by advising patients, and increasing awareness about influenza burden for groups undermining vaccination uptake rates. Similarly, health-promotion programs can utilize such data. The findings of this study can be considered baseline data for future interventions to improve uptake rates among this vulnerable group in Jordan and conduct comparisons. Primary health-care services need to play a role in reaching people aged ≥65 years for vaccine promotion and improving influenza vaccine uptake.
Abbreviations
CDC, Centers for Disease Control and Prevention; HBM, health belief model.
Data Sharing
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The original project was approved by the Institutional Review Committee (IRC) for the Ministry of Health Ethics Committee (MOH/REC/2022/328, October 26, 2022). Written informed consent was obtained from the participants who were eligible to participate in this study. Prior to signing the consent form, all participants were provided with relevant information about this study. Participants without a written study consent were not enrolled. As per regulations of the IRB committee, for illiterate participants, verbal consent was obtained in the presence of a literate family member, who also signed the consent form on their behalf.
Acknowledgments
We thank the management of Al-Bashir Hospital, Amman; Princess Rahma Hospital for Pediatrics, Irbid; Princess Basma Hospital, Irbid; Princess Badiya Hospital for Obstetrics and Gynecology, Irbid; Zarqa Governmental Hospital; Karak Governmental Hospital; Amman Comprehensive Healthcare Center; and the comprehensive health centers in Zarqa, Karak, and Irbid for their great support.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention (CDC). Ten great public health achievements--worldwide, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011;60(24):814–818.
2. Palache A, Oriol-Mathieu V, Abelin A, Music T. Influenza vaccine supply task force (IFPMA IVS). Seasonal influenza vaccine dose distribution in 157 countries (2004-2011). Vaccine. 2014;32(48):6369–6376. doi:10.1016/j.vaccine.2014.07.012
3. Greenwood B. The contribution of vaccination to global health: past, present and future. Philos Trans R Soc Lond B Biol Sci. 2014;369(1645):20130433. doi:10.1098/rstb.2013.0433
4. Influenza (Seasonal). Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-seasonal.
5. Krammer F, Smith GJD, Fouchier RAM, et al. Influenza. Nat Rev Dis Primers. 2018;4(1):3. doi:10.1038/s41572-018-0002-y
6. CDC. Flu and people 65 years and older. influenza (Flu). 2025. Available from: https://www.cdc.gov/flu/highrisk/65over.htm.
7. Influenza (seasonal). Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-seasonal.
8. Factsheet about seasonal influenza. 2017. Available from: https://www.ecdc.europa.eu/en/seasonal-influenza/facts/factsheet.
9. Grohskopf LA, Sokolow LZ, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices-United States, 2018-19 influenza season. MMWR Recommendations Reports. 2018;67(3):1–20. doi:10.15585/MMWR.RR6703A1
10. Kanitz EE, Wu LA, Giambi C, et al. Variation in adult vaccination policies across Europe: an overview from VENICE network on vaccine recommendations, funding and coverage. Vaccine. 2012;30(35):5222–5228. doi:10.1016/j.vaccine.2012.06.012
11. Costantino C, Vitale F. Influenza vaccination in high-risk groups: a revision of existing guidelines and rationale for an evidence-based preventive strategy. J Prev Med Hyg. 2016;57(1):E13–18.
12. Ortiz JR, Perut M, Dumolard L, et al. A global review of national influenza immunization policies: analysis of the 2014 WHO/UNICEF joint reporting form on immunization. Vaccine. 2016;34(45):5400–5405. doi:10.1016/j.vaccine.2016.07.045
13. Thompson WW, Weintraub E, Dhankhar P, et al. Estimates of US influenza-associated deaths made using four different methods. Influenza Other Respir Viruses. 2009;3(1):37–49. doi:10.1111/j.1750-2659.2009.00073.x
14. Troeger CE, Blacker BF, Khalil IA; GBD 2017 Influenza Collaborators. Mortality, morbidity, and hospitalisations due to influenza lower respiratory tract infections, 2017: an analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2019;7(1):69–89. doi:10.1016/S2213-2600(18)30496-X
15. Ciabattini A, Nardini C, Santoro F, Garagnani P, Franceschi C, Medaglini D. Vaccination in the elderly: the challenge of immune changes with aging. Semin Immunol. 2018;40:83–94. doi:10.1016/j.smim.2018.10.010
16. Woodward M, Ramasubramanian V, Kamarulzaman A, et al. Addressing unmet needs in vaccination for older adults in the Asia pacific: insights from the COVID-19 pandemic. Clin Interv Aging. 2023;18:869–880. doi:10.2147/CIA.S406601
17. Silva SB, de O Souza F, de S Pinho P, Santos DV. Health belief model in studies of influenza vaccination among health care workers. Rev Bras Med Trab. 2023;21(2):e2022839. doi:10.47626/1679-4435-2022-839
18. Rosenstock IM. The health belief model and preventive health behavior. Health Educat Monograph. 1974;2(4):354–386. doi:10.1177/109019817400200405
19. Rosenstock IM, Strecher VJ, Becker MH, DiClemente R, Peterson J. Preventing AIDS: Theories and Methods of Behavioral Interventions. US: Springer US; 1994.
20. Ang LW, Cutter J, James L, Goh KT. Factors associated with influenza vaccine uptake in older adults living in the community in Singapore. Epidemiol Infect. 2017;145(4):775–786. doi:10.1017/S0950268816002491
21. Teo LM, Smith HE, Lwin MO, Tang WE. Attitudes and perception of influenza vaccines among older people in Singapore: a qualitative study. Vaccine. 2019;37(44):6665–6672. doi:10.1016/j.vaccine.2019.09.037
22. Panchapakesan C, Sheldenkar A, Cayabyab YM, Ng JS, Lu J, Lwin MO. A comparison between the predictors of vaccine uptake intentions for influenza and dengue. Int J Environ Res Public Health. 2018;15(12):2694. doi:10.3390/ijerph15122694
23. Ballestas T, McEvoy SP, Doyle J. SMAHS healthcare worker influenza vaccination working party. co-ordinated approach to healthcare worker influenza vaccination in an area health service. J Hosp Infect. 2009;73(3):203–209. doi:10.1016/j.jhin.2009.07.028
24. Corace KM, Srigley JA, Hargadon DP, et al. Using behavior change frameworks to improve healthcare worker influenza vaccination rates: a systematic review. Vaccine. 2016;34(28):3235–3242. doi:10.1016/j.vaccine.2016.04.071
25. Tinoco YO, Osman TS, Ampuero JS, et al. Respiratory disease surveillance in the Middle East and Latin America during the COVID-19 pandemic, 2020–2022. Emerg Infect Dis. 2024;30(14). doi:10.3201/eid3014.240303
26. Assaf AM, Hammad EA, Haddadin RN. Influenza vaccination coverage rates, knowledge, attitudes, and beliefs in Jordan: a comprehensive study. Viral Immunol. 2016;29(9):516–525. doi:10.1089/vim.2015.0135
27. World bank open data. Available from: https://data.worldbank.org.
28. Ababneh M, Jaber M, Rababa’h A, Ababneh F. Seasonal influenza vaccination among older adults in Jordan: prevalence, knowledge, and attitudes. Hum Vaccin Immunother. 2020;16(9):2252–2256. doi:10.1080/21645515.2020.1718438
29. Alqahtani AS, Althobaity HM, Al Aboud D, Abdel-Moneim AS. Knowledge and attitudes of Saudi populations regarding seasonal influenza vaccination. J Infect Public Health. 2017;10(6):897–900. doi:10.1016/j.jiph.2017.03.011
30. Alqahtani AS, Bondagji DM, Alshehari AA, et al. Vaccinations against respiratory infections in Arabian Gulf countries: barriers and motivators. World J Clin Cases. 2017;5(6):212–221. doi:10.12998/wjcc.v5.i6.212
31. Pebody RG, Warburton F, Andrews N, et al. Uptake and effectiveness of influenza vaccine in those aged 65 years and older in the United Kingdom, influenza seasons 2010/11 to 2016/17. Euro Surveill. 2018;23(39):1800092. doi:10.2807/1560-7917.ES.2018.23.39.1800092
32. Szőllősi GJ, Minh NC, Santoso CMA, Zsuga J, Nagy AC, Kardos L. An exploratory assessment of factors with which influenza vaccine uptake is associated in Hungarian adults 65 years old and older: findings from European health interview surveys. Int J Environ Res Public Health. 2022;19(12):7545. doi:10.3390/ijerph19127545
33. Abu-Rish EY, Elayeh ER, Mousa LA, Butanji YK, Albsoul-Younes AM. Knowledge, awareness and practices towards seasonal influenza and its vaccine: implications for future vaccination campaigns in Jordan. Fam Pract. 2016;33(6):690–697. doi:10.1093/fampra/cmw086
34. Barry MA, Aljammaz KI, Alrashed AA. Knowledge, attitude, and barriers influencing seasonal influenza vaccination uptake. Can J Infect Dis Med Microbiol. 2020;2020:7653745. doi:10.1155/2020/7653745
35. Cho BH, O’Halloran A, Pike J. Investigation of barriers to county-level seasonal influenza vaccine uptake among medicare beneficiaries in the United States - 2018-2019 seasonal influenza season. Vaccine. 2023;14:100326. doi:10.1016/j.jvacx.2023.100326
36. Zakhour R, Tamim H, Faytrouni F, Khoury J, Makki M, Charafeddine L. Knowledge, attitude and practice of influenza vaccination among Lebanese parents: a cross-sectional survey from a developing country. PLoS One. 2021;16(10):e0258258. doi:10.1371/journal.pone.0258258
37. Ahmed WS, Halboup AM, Alshargabi A, Al-Mohamadi A, Al-Ashbat YK, Al-Jamei S. Attitudes, motivators, and barriers toward influenza vaccination for children: a study from a conflict-ridden country. Confl Health. 2024;18(1):26. doi:10.1186/s13031-024-00590-9
38. Peña-Rey I, Pérez-Farinós N, Sarría-Santamera A. Factors associated with influenza vaccination among elderly Spanish women. Public Health. 2004;118(8):582–587. doi:10.1016/j.puhe.2004.04.010
39. Fiore AE, Uyeki TM, Broder K, et al. Prevention and control of influenza with vaccines: recommendations of the advisory committee on immunization practices (ACIP), 2010. MMWR Recomm Rep. 2010;59(RR–8):1–62.
40. Centers for Disease Control and Prevention (CDC). State-specific influenza vaccination coverage among adults aged > or =18 years--United States, 2003-04 and 2005-06 influenza seasons. MMWR Morb Mortal Wkly Rep. 2007;56(37):953–959.
41. Bennett KJ, Pumkam C, Probst JC. Rural-urban differences in the location of influenza vaccine administration. Vaccine. 2011;29(35):5970–5977. doi:10.1016/j.vaccine.2011.06.038
42. Gosadi IM, Zogel B, Alfaifi S, et al. Assessment of influenza vaccine uptake according to the presence of a chronic disease. Vaccines. 2023;11(5):938. doi:10.3390/vaccines11050938
43. Dexter LJ, Teare MD, Dexter M, Siriwardena AN, Read RC. Strategies to increase influenza vaccination rates: outcomes of a nationwide cross-sectional survey of UK general practice. BMJ Open. 2012;2(3):e000851. doi:10.1136/bmjopen-2011-000851
44. Lau L, Lau Y, Lau YH. Prevalence and correlates of influenza vaccination among non-institutionalized elderly people: an exploratory cross-sectional survey. Int J Nurs Stud. 2009;46(6):768–777. doi:10.1016/j.ijnurstu.2008.12.006
45. Santos AJ, Kislaya I, Machado A, Nunes B. Beliefs and attitudes towards the influenza vaccine in high-risk individuals. Epidemiol Infect. 2017;145(9):1786–1796. doi:10.1017/S0950268817000814
46. Hu PL, Koh EYL, Tay JSH, Chan VXB, Goh SSM, Wang SZ. Assessing the impact of educational methods on influenza vaccine uptake and patient knowledge and attitudes: a randomised controlled trial. Singapore Med J. 2023;64(2):98–104. doi:10.11622/smedj.2021222
47. Siena LM, Isonne C, Sciurti A, et al. The association of health literacy with intention to vaccinate and vaccination status: a systematic review. Vaccines. 2022;10(11):1832. doi:10.3390/vaccines10111832
48. Johansen ND, Vaduganathan M, Bhatt AS, et al. Nationwide utilization of Danish government electronic letter system for increasing inFLUenza vaccine uptake (NUDGE-FLU): study protocol for a nationwide randomized implementation trial. Am Heart J. 2023;260:58–71. doi:10.1016/j.ahj.2023.02.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Middle-Aged and Elderly Population Towards Ultrasound Screening for Strokes
Wang W, Peng Y, Tang K, Zheng Z, He L, Yang S
Journal of Multidisciplinary Healthcare 2024, 17:147-157
Published Date: 9 January 2024
Identification of Facilitators and Barriers to Functional Ability in Elderly Stroke Patients: A Descriptive Qualitative Study
Zhang W, Ma R, Tao X, Wang A
Journal of Multidisciplinary Healthcare 2025, 18:1007-1019
Published Date: 21 February 2025