")
Back to Journals » Journal of Pain Research » Volume 18
Latent Profile Analysis of Pain Catastrophizing in Post-Operative Lung Cancer Patients
Authors Wu X , Xu T, Cai P, Shen S, Ji M, Liu Q, Wang X , Zhang M, Wang S, Gu D
Received 17 November 2024
Accepted for publication 8 March 2025
Published 1 April 2025 Volume 2025:18 Pages 1735—1745
DOI https://doi.org/10.2147/JPR.S507027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Xinyan Wu,1,2 Tao Xu,2 Ping Cai,1 Siwen Shen,1 Mengchen Ji,1 Qing Liu,3 Xiaobo Wang,2 Mingqi Zhang,2 Shiming Wang,4,* Danfeng Gu1,*
1Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China; 2Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China; 3Huadong Sanatorium, Wuxi, Jiangsu, 214122, People’s Republic of China; 4Wuxi Branch of Zhongda Hospital Southeast University, Wuxi, Jiangsu, 214122, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Danfeng Gu, Affiliated Hospital of Jiangnan University, 1000 hefeng Road, Binhu District, Wuxi, Jiangsu, People’s Republic of China, Email [email protected] Shiming Wang, Wuxi Branch of Zhongda Hospital Southeast University, No. 1128, Dacheng Road, Xishan District, Wuxi, Jiangsu, People’s Republic of China, Email [email protected]
Background: Patients with lung cancer often experience high levels of pain and recurrent pain episodes after thoracoscopic surgery, compromising their adherence to rehabilitation exercises and quality of life. Pain catastrophizing is defined as an exaggerated and negative mindset towards actual or anticipated pain and is one of the significant factors influencing pain. To date, prior investigations on pain catastrophizing have predominantly employed variable-centered approaches, focusing on broader population levels while neglecting individual specificity. Latent profile analysis represents an individual-centered data analysis method that can accurately identify distinct phenotypic subgroups and deeply analyze the characteristics of each subgroup. This enables clinicians to identify high-risk patients early and provide precision interventions to reduce pain catastrophizing and ultimately alleviate postoperative pain burden. Stratification-guided interventions play a crucial role in treating patients with pain catastrophizing, aligning with the principles of precision medicine.
Methods: 409 patients were included in this cross-sectional study. Latent profile analysis (LPA) was employed to discern distinct classes of pain catastrophizing among these patients. Chi-square tests, ANOVA, and multinomial logistic regression were conducted to analyze the factors influencing the different pain catastrophizing profiles among patients following thoracoscopic lung cancer surgery.
Results: Three distinct latent classes of pain catastrophizing were identified, Class1, labeled “Mild Pain Catastrophizing-Rumination Type”(26.2% of participants), Class2, referred to as “Moderate Pain Catastrophizing-Ruminative Exaggerative Type”(33.2%), Class3, designated as “Severe Pain Catastrophizing-Ruminative Helpless Exaggerative Type”(40.6%). Unordered multinomial logistic regression analysis indicated that factors influencing mild pain catastrophizing included fatigue, perception of social support, marital status, primary caregiver, tumor location, and clinical stage. In contrast, factors influencing moderate pain catastrophizing included fatigue, perception of social support, marital status, education level, primary caregiver, and clinical stage (P < 0.05).
Conclusion: Three distinct patterns of pain catastrophizing were identified in patients following lung cancer surgery, each exhibiting unique classification characteristics. Healthcare professionals should promptly identify individuals at high risk for pain catastrophizing and develop targeted interventions that address physiological, psychological, and social factors.
Keywords: thoracic surgery, video-assisted, pain catastrophizing, latent profile analysis
Introduction
At present, lung cancer was the most frequently diagnosed cancer, responsible for almost 2.5 million new cases, 12.4% of all cancers globally, and was also the leading cause of cancer death.1 Surgery is the preferred treatment method for early-stage lung cancer patients. Though video-assisted thoracoscopic surgery (VATS) has become increasingly popular due to minimally invasive nature, faster recovery times and fewer complications compared with thoracotomy,2 the intercostal nerves at the incision site will be inevitably damaged, which results in postoperative pain. Xiao F et al3 conducted a retrospective study involving 204 patients with early-stage lung adenocarcinoma and found that 37.3% of them suffered from acute pain following thoracoscopic surgery. Similarly, Zhang Y et al4 performed a retrospective analysis of 2,348 lung cancer patients who underwent thoracoscopic surgery and discovered that the incidence of chronic postsurgical pain (CPSP) was 43.99%. Studies have shown that patient self-reporting is the most reliable method for assessing pain.5 However, many patients may exaggerate their pain to draw attention to it from healthcare professionals and family members.6 Pain catastrophizing, as an important psychological factor affecting pain assessment, has gradually attracted attention.
Pain catastrophizing refers to an exaggerated and negative cognitive set regarding actual or anticipated pain, characterized by rumination on past painful experiences, magnification of the negative impacts of pain, and a sense of helplessness in alleviating it.7 Pain catastrophizing has several adverse effects on patients, including heightened pain perception,8 over-reliance on medication for pain relief,9 delaying postoperative recovery, and affecting psychological health, among others.9 Previous studies have indicated that the incidence of pain catastrophizing among cancer patients and lung cancer patients is 40%9 and 35.3%,10 respectively. Factors associated with pain catastrophizing include sex, age, the intensity and location of pain, loneliness, anxiety, and depression.11,12 Manning et al13 found that the severity and sensitivity of fatigue are factors affecting pain catastrophizing in patients with chronic low back pain, but their impact on pain catastrophizing in VATS postoperative patients remains to be verified. The influence of social support on pain catastrophizing has also not been conclusively determined. However, according to social cognitive theory,14 human behavior is neither entirely driven by internal forces nor entirely shaped and controlled by external environmental stimuli, but is the result of continuous interaction among the individual, environment, and behavior. Furthermore, previous research on pain catastrophizing has primarily focused on patients after joint replacement surgery,15 patients with chronic pain16 and cancer patients,17 with few studies reported on pain catastrophizing in patients after thoracoscopic surgery for lung cancer.
Latent profile analysis (LPA) assesses an individual’s latent characteristics based on their observable responses, grouping individuals with similar traits into distinct categories. By specifically analyzing individuals within these categories, LPA examines the characteristics of different groupings within a population and the differences between them. This approach assists nursing staff in implementing targeted interventions tailored to specific groups. LPA has been widely utilized in psychological and behavioral research,18,19 and by further investigating the characteristics of different groups, it facilitates the development of precise interventions.
To our knowledge, no studies have employed LPA to explore pain catastrophizing in lung cancer patients on the third day after thoracoscopic surgery. The aim of this study was to (1) use latent profile analysis to understand subgroups of pain catastrophizing patterns in lung cancer patients 3 days following thoracoscopic surgery; (2) To analyze the heterogeneity of socio-demographic factors, disease-related factors, and socio-psychological factors across various subgroups. We anticipate that patients with high fatigue or low social support are more prone to pain catastrophizing, according to communal coping theory and existing data.20
Methods
Participants
Our cross-sectional study employed convenience sampling to recruit lung cancer patients who underwent thoracoscopic surgery at three level 3A hospitals in Wuxi between August 2023 and March 2024. Direct interviews were used to collect data.
Eligibility criteria for patients included age 18 or older; adherence to lung cancer diagnostic standards;21 completion of thoracoscopic lung resection; alertness and effective communication ability; absence of prior neoadjuvant chemotherapy or previous thoracic surgery; and consent to participate. Exclusions were implemented for individuals with alternative pain disorders or those participating in other interventional researches.
According to the regression analysis, the sample size should be 5–10 times the number of independent variables plus an extra 10% to account for attrition. Aiming for a sample size of 89–178 people with 16 independent variables, the study eventually enrolled 409 participants.
Procedure
Following defined criteria, two researchers evaluated patients on day three following surgery. Before handing over the questionnaire, they clarified the research and got permission. Those with questions got clear instructions on how to do it independently. On-site researchers rejected individuals with random or patterned answers and checked the finished surveys for completeness. Ethical approval for the study was obtained from Jiangnan University Affiliated Hospital (LS2023092), with conduct in strict adherence to Helsinki Declaration guidelines.
Measures
General Information on the Questionnaire
The questionnaire, established following a literature study and group discussions, encompassed patients’ demographic information (age, sex, education) and clinical particulars (Tumor location, Clinical stage). This study determined smoking status by inquiring about the annual amount of tobacco consumption. We initially inquire whether patients have a habit of smoking. For those who smoke, we proceed to ask about their daily consumption and use this information to calculate their annual consumption; for patients who have quit smoking, we confirm the exact time they ceased smoking and their annual consumption prior to quitting; for those who have never smoked, they are categorized as non-smokers. The approach to inquiring about alcohol consumption is identical to that of smoking. Patients were classified as smokers if they smoked ≥30 packs per year or had quit smoking for less than 15 years after previously smoking ≥30 packs. Patients were identified as drinkers if they consumed alcohol ≥ once a week in the past year.
Indicators of Class Membership
The Pain Catastrophizing Scale (PCS), translated by Yap, measures negative pain reactions with 13 items scored 0–4. It assesses magnification, helplessness, and rumination, with totals ranging 0–52. Scores ≥38 indicate significant pain catastrophizing.22 The scale demonstrates strong reliability (Cronbach’s α = 0.913).
Factors Related to Class Membership
Perception of social support: We used the Multidimensional Scale of Perceived Social Support (MSPSS), translated by Huang et al in 1996, which assesses perceived social support from family, friends, and others through 12 items scored 1–7. Total scores vary from 12 to 84, with elevated scores signifying enhanced perceived support.23 Our investigation demonstrated strong scale stability (Cronbach’s α = 0.876).
Fatigue: We used the Brief Fatigue Inventory (BFI), translated by Lin et al in 2006, to assess fatigue levels. The scale includes nine items scored 0–10, assessing general and worst levels of current and past 24h fatigue and its impact on the patient. Total scores are the mean of item scores, with values of 1–3 denoting mild exhaustion, 4–6 suggesting moderate fatigue, and 7–10 indicating severe fatigue.24 The scale demonstrated significant stability (Cronbach’s α = 0.954).
Data Analysis
Latent Profile Analysis (LPA) was performed using Mplus 8.3, employing the 13-item Pain Catastrophizing Scale (PCS) as manifest variables and assessing models ranging from 1 to 5 profiles. The evaluation of model fit was conducted using three indicators: (1) Information evaluation criteria included the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and the sample-size adjusted Bayesian Information Criterion (aBIC). Reduced values signify superior fit. Entropy (0–1 scale) quantifies categorization accuracy, with values approaching 1 indicating superior precision. (3) Likelihood ratio tests included the Lo-Mendell-Rubin (LMR) test and the Bootstrap Likelihood Ratio Test (BLRT). A substantial p-value (P < 0.05) demonstrated that the k-class model exhibited superior fit to the k-1-class model. Together, these evaluation criteria serve as references for profile decision-making. The model’s suitability was determined by considering the interpretability of the classes and the sample size of each profile.25 For data analysis to be valid, subgroups should ideally consist of more than 25 individuals or more than 1% of the profile.26,27
Descriptive statistics, univariate analysis, and multivariate analysis were performed using SPSS 24.0. Whether the data followed a normal distribution was verified using descriptive statistics. Quantitative data that followed a normal distribution were expressed as mean (standard deviation [SD] =), and comparisons between groups were performed using analysis of variance (ANOVA). Non-normally distributed quantitative data were expressed as median (interquartile range), and between-group comparisons were conducted using the Kruskal–Wallis test. Qualitative data were described using frequencies and percentages, and a chi-square test was employed for between-group comparisons.
Second, based on the results of LPA, the latent class of pain catastrophizing was used as the dependent variable, and all significantly different categorical variables in the univariate analysis were used as independent variables. Continuous numerical data and total scores from various scales were employed as covariates in an ordinal multinomial logistic regression analysis to investigate the factors influencing the latent profile classification of pain catastrophizing in lung cancer patients after surgery. All tests were two-tailed, and a value of P < 0.05 indicated statistical significance.
Results
Patient Characteristics
A total of 415 questionnaires were distributed in this study, of which 6 were invalid. Ultimately, 409 useful responses were obtained, yielding a response rate of 98.5%. The total score for the fatigue scale was 4.70(standard deviation [SD] =1.58). The scores for its two dimensions were as follows: fatigue severity scored 4.88(standard deviation [SD] =1.68), and fatigue impact scored 4.61(standard deviation [SD] =1.69). The total score for the perceived social support scale was 52.54(standard deviation [SD] =8.69). The scores for the three dimensions of the scale were as follows: perceived social support from family 4.88(standard deviation [SD] =0.84), perceived social support from friends4.42(standard deviation [SD] =0.89), and perceived social support from others 3.84(standard deviation [SD] =0.86)。Further details are in Table 1.
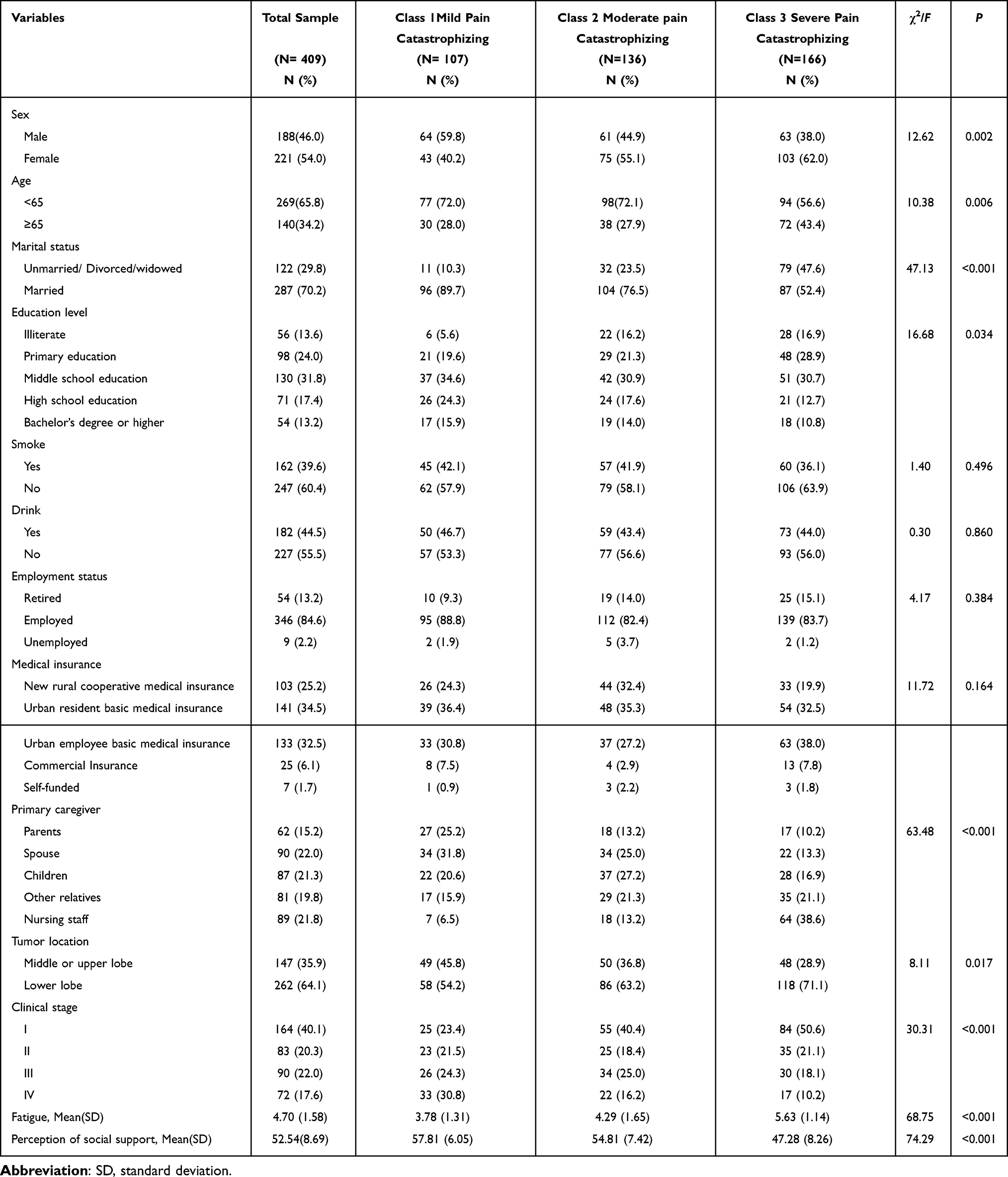 |
Table 1 General Characteristics of Post-Thoracoscopic Patients With Lung Cancer |
Results of LPA
We used AIC, BIC, aBIC, LMR (p-value), and BLRT (p-value) to identify the best of five models after performing LPA on PCS scores. Even though Models 5 and 4 had superior fit indices but had clinically uninterpretable categories below 5%, Model 3 was still selected as the best option. The results of the model fitting are shown in Table 2.
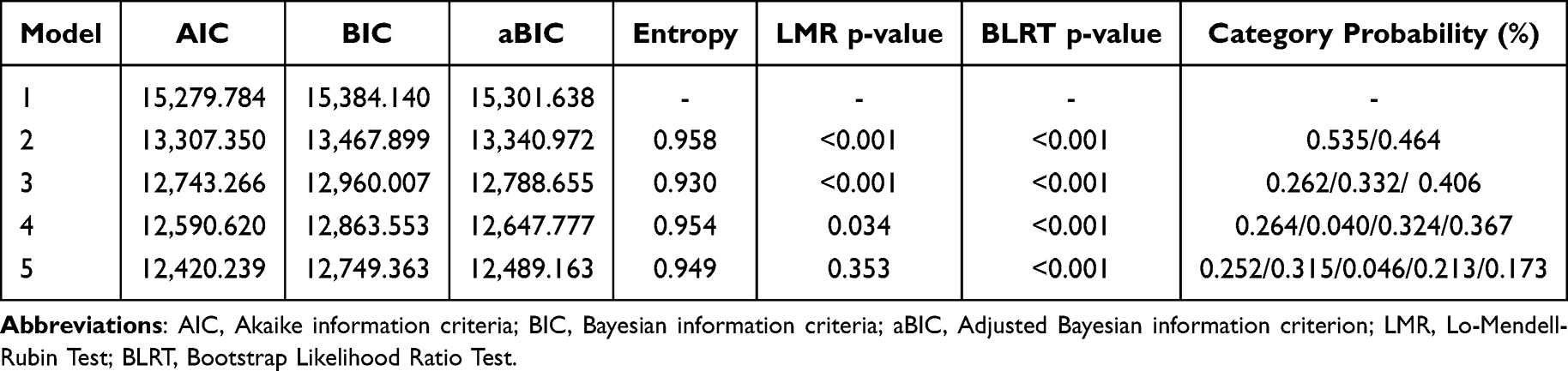 |
Table 2 Fit Indices of LPA for Post-Thoracoscopic Lung Cancer Patients |
Mean scores were used to categorize the profiles: C1 comprised 26.2% of the population, with a mean score of 16.48 (standard deviation [SD] =3.45), labeled “Mild Pain Catastrophizing - Rumination Type” because items 10 and 11 (the ruminating dimension) had higher scores. The C3 group, which made up 40.6% of the population, had the highest mean score of 38.23 (standard deviation [SD] =3.67) and was classified as “Severe Pain Catastrophizing-Ruminative Helpless Exaggerative Type” because of their significantly higher scores on items 8–10, 11 (rumination dimension), 2 (helplessness dimension), and 6 (exaggeration dimension). C2 had a mean score of 26.25 (standard deviation [SD] = 2.77), making up 33.2% of the population. With higher ratings on item 6 (exaggeration dimension) and items 8, 10, and 11 (rumination dimension), it fell between C1 and C3. Thus, it was labeled “Moderate Pain Catastrophizing-Ruminative Exaggerative Type” (Figure 1).
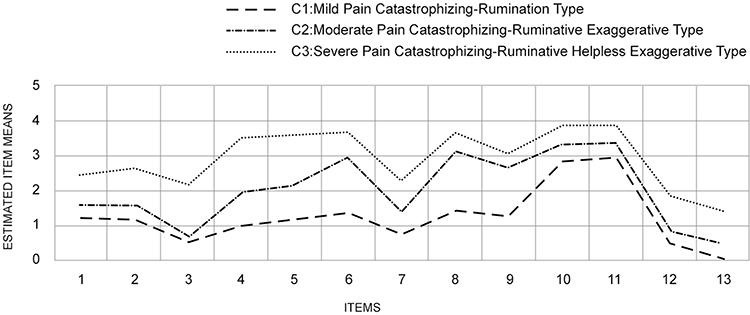 |
Figure 1 The characteristic distribution of three latent profiles of post-operative lung cancer patients. |
Multivariate Analyses Regarding Latent Withdrawal Classes
The three possible profiles of pain catastrophizing showed significant differences in most patient-related factors (Table 1). Compared to Classes 1 and 2, a much higher number of patients in Class 3 had nursing staff as their caregivers. These patients were primarily older, less educated, single, divorced, or widowed female who felt little social support and were fatigued. Class 3 patients were far more likely to have early-stage disease and lower-lobe tumor locations (p<0.05). No substantial variations were observed among the three classes regarding smoking and alcohol drinking history, employment status, and methods of medical expense payment (Table 1).
Multinomial Logistic Regression
Multinomial logistic regression was used to examine significant components from univariate analysis, exposing variations among latent classes. The comparison findings between the three latent classes are shown in Table 3. Classes 1 and 2 had six important variables, with Class 3 as the reference. For Class 1, the predictors included fatigue (odds ratio [OR]: 0.924, 95% confidence interval [CI]: 0.895–0.955; P < 0.001), perception of social support (OR: 1.178, 95% CI: 1.114–1.247; P < 0.001), status of being unmarried, divorced, or widowed (OR: 0.173, 95% CI: 0.066–0.451; P < 0.001), primary caregiver as parents (OR: 8.092, 95% CI: 2.053–31.894; P = 0.003), spouse (OR: 12.106, 95% CI: 3.525–41.568; P < 0.001), children (OR: 8.175, 95% CI: 2.329–28.698; P = 0.001), other relatives (OR: 3.588, 95% CI: 1.012–12.716; P = 0.048), localization of the tumor in the middle or upper lobe (OR: 2.718, 95% CI: 1.299–5.686; P = 0.008), and clinical stage I (OR: 0.055, 95% CI: 0.018–0.165; P < 0.001) or stage II (OR: 0.205, 95% CI: 0.062–0.675; P = 0.009). Similarly, for Class 2, the predictors comprised fatigue (OR: 0.935, 95% CI: 0.910–0.962; P < 0.001), perception of social support (OR: 1.103, 95% CI: 1.055–1.154; P < 0.001), status of being unmarried, divorced, or widowed (OR: 0.494, 95% CI: 0.255–0.957; P = 0.037), junior high school level of education (OR: 0.284, 95% CI: 0.098–0.823; P = 0.020), primary caregiver as spouse (OR: 4.119, 95% CI: 1.641–10.340; P = 0.003) or children (OR: 4.272, 95% CI: 1.762–10.357; P = 0.001), and clinical stage II (OR: 0.237, 95% CI: 0.093–0.601; P = 0.002).
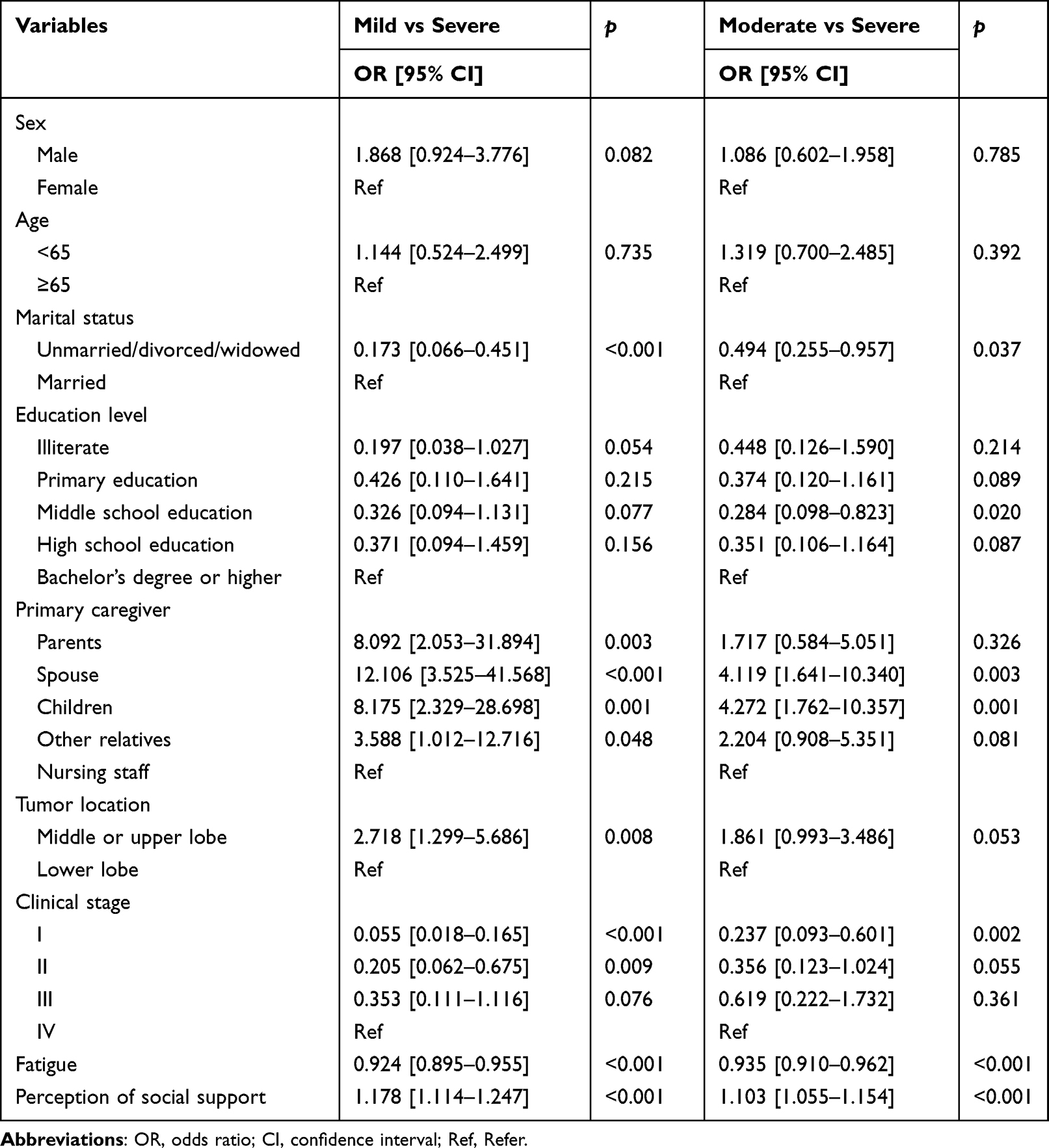 |
Table 3 Multinomial Logistic Regression for Pain Catastrophizing Profiles |
Discussion
This study employed LPA to explore subgroups of pain catastrophizing among patients after thoracoscopic surgery for lung cancer. Additionally, this study investigated the correlations between fatigue, perceived social support, and these subgroups. Three latent classes were identified based on the results of the LPA. Profile C1: “Mild Pain Catastrophizing-Rumination Type” (26.2% of patients), Patients in this category can accurately assess their pain but tend to ruminate on it excessively. The reason for this behavior is multifaceted. These patients typically have a high level of education, which leads them to evaluate pain more rationally rather than relying solely on sensory experiences. However, they also have high self-expectations and a strong motivation for achievement. They hope to quickly return to work and regain social recognition through their efforts. Yet, the impairment of work ability caused by pain triggers anxiety and a sense of frustration, leading to excessive reflection and a cycle of rumination. Profile C2: “Moderate Pain Catastrophizing-Ruminative Exaggerative Type” (33.2%% of patients), Patients in this category lack the ability to accurately assess their pain and are deeply mired in negative thoughts. The reasons for this are twofold. First, the proportion of patients with high levels of education has decreased, which has led to a decline in the overall accuracy of pain assessment. Second, the increased proportion of caregivers who are nursing aides means that patients may exaggerate their pain in order to gain attention and emotional support from their family members. Profile C3: “Severe Pain Catastrophizing-Ruminative Helpless Exaggerative Type” (40.6% of patients), Patients in this category tend to exaggerate their pain and lack coping skills and confidence in overcoming it. The reasons for this behavior are multifaceted. This group has a higher proportion of female with lower levels of education, who are more sensitive to pain and tend to have an emotional rather than rational understanding of it. They often experience information overload and have difficulty discerning relevant information, which leads to a lack of effective pain management strategies. It is recommended that healthcare professionals pay attention to the degree of pain catastrophising in post-operative lung cancer patients and identify their categories early on. For the “Mild Pain Catastrophizing-Rumination Type”, cognitive-behavioral therapy should be employed to adjust the patient’s acceptance of pain. Additionally, a progressive rehabilitation exercise program should be tailored according to the patient’s needs to help them return to work. For the “Moderate Pain Catastrophizing-Ruminative Exaggerative Type”, it is essential to enhance the patient’s cognitive understanding and management of pain, as well as improve their health literacy. Meanwhile, training should be provided to caregivers to strengthen their caregiving skills and humanistic care capabilities, encouraging them to offer empathetic and compassionate care to patients. For the “Severe Pain Catastrophizing-Ruminative Helpless Exaggerative Type”, healthcare workers should listen to the voices of patients, understand their situations with a feminine mindset, and empower patients with the experience and confidence to overcome pain through peer education. Consistent with earlier studies, moderate and mild pain catastrophizing patients had higher perception of social support and lower fatigue than severe pain catastrophizing patients.13,28 This study improves understanding of pain catastrophizing in lung cancer patients following thoracoscopic surgery and underscores the significance of LPA in identifying individuals requiring targeted therapies.
Demographic differences in pain catastrophizing after thoracoscopic surgery were found. A higher proportion of married individuals is observed in the “Mild Pain Catastrophizing-Rumination Type” and “Moderate Pain Catastrophizing-Helpless Rumination Exaggerated Type” profiles compared to the “Severe Pain Catastrophizing-Helpless Rumination Exaggerated Type”, which aligns with the findings of Golkari S et al.29 Giardino N D et al investigated pain catastrophizing among 74 patients with chronic pain due to spinal cord injury and found a significant relationship between pain catastrophizing and spousal care behaviors. Their comparison of patients living with various cohabitating partners revealed that those living with a partner exhibited a stronger association between pain catastrophizing and pain severity than those living alone or with others.30 This suggests that spouses may mitigate the impact of other factors on pain catastrophizing and reduce its severity. Consequently, unmarried, divorced, or widowed patients should be prioritized for intervention. Healthcare providers can help alleviate pain catastrophizing through various strategies, including enhancing patients’ self-management skills and improving policy support. The findings of this study demonstrate a significant association between educational level and pain catastrophizing. Patients with a junior high school education are more likely to be classified in the “Severe Pain Catastrophizing-Helpless Rumination Exaggerated Type” category, consistent with previous research.31 According to the study, patients with different levels of education have varying understandings of their illness and treatment plans, as well as different assessments of their symptoms.32 Specifically, individuals with lower educational attainment frequently experience information overload during health education, which adversely affects their disease conceptualization and the accuracy of their assessment of somatic symptoms.33 Furthermore, patients whose primary caregivers are nursing aides also exhibit a higher likelihood of falling into the “Severe Pain Catastrophizing-Helpless Rumination Exaggerated Type” category. In the absence of family support, hospitals typically assign nursing aides to provide care, thereby compensating for the lack of familial assistance. However, nursing aides often deliver only instrumental support, failing to provide the essential emotional support needed.34 In some instances, these aides may neglect the physical care of patients, resulting in unmet physiological and psychological needs, which further exacerbates pain catastrophizing.35,36 We found that clinical variables affect pain catastrophizing latent patterns. Patients with lower lobe tumors are more likely to be categorized as “Severe Pain Catastrophizing-Helpless Rumination Exaggerated Type.” This association may be due to several factors, including older age, a higher proportion of female patients, more extensive lymphatic metastasis, and poorer prognoses typically linked to lower lobe tumors, all of which can contribute to exacerbated pain catastrophizing.37–39 Clinical stage is a critical characteristic of lung cancer, and the results of this study suggest that patients with stage I and II lung cancer are also more likely to fall into the “Severe Pain Catastrophizing-Helpless Rumination Exaggerated Type” category. Conversely, Mahlaq et al40 reported contrasting findings in their study of 230 breast cancer patients in Morocco, indicating that those with earlier TNM stages experienced greater psychological burdens. Cultural differences may significantly influence these discrepancies. In China, it is common for family members to serve as medical decision-makers on behalf of patients, primarily to protect them from the negative consequences of cancer, particularly in cases of advanced disease. This approach can significantly mitigate negative emotions in patients with advanced cancer.41 In contrast, early-stage cancer patients may endure more substantial psychological distress as they confront the challenges of their diagnosis. This increased stress can lead to heightened negative emotions and a disposition to interpret life events pessimistically, ultimately resulting in pain catastrophizing.
The regression analysis revealed that patients with high levels of perception of social support were more inclined to be categorized as “mild pain catastrophizing-rumination type” or “moderate pain catastrophizing -exaggerated rumination type”. Notably, those in the “mild pain catastrophizing-rumination type” group reported the highest levels of perception of social support, consistent with previous research findings.28 Effective management of pain catastrophizing requires not only pharmacological intervention but also substantial support from family and society. According to communal coping theory, patients may engage in pain catastrophizing as a coping mechanism; when they lack sufficient attention and support, they may exaggerate their pain to seek social assistance.42 Akbari F et al incorporated family functioning into a model of pain catastrophizing and pain-related disability, demonstrating that family dysfunction can lead to increased pain catastrophizing.43 Boothby JL et al reached divergent conclusions. They categorized partner behaviors as caring, punishing, or ignoring, and examined the relationship between pain catastrophizing and perceived partner behaviors. Their results indicated that pain catastrophizing was unrelated to perceived caring behaviors from partners but was associated with perceived punishing responses.44 This suggests that catastrophizing may not be mitigated by perceived compassion or support from others. However, the small sample size in Boothby JL et al’s study may have influenced these contradictory findings. While existing research does not definitively clarify the relationship between pain catastrophizing and social support, nor does it delineate the pathways through which different forms of social support affect pain catastrophizing, the aforementioned findings highlight the significant role that partners play in shaping patients’ experiences of pain catastrophizing. Therefore, it is essential to involve patients’ partners or primary caregivers in therapeutic interventions and provide joint treatment aimed at enhancing their communication and coping skills.
The regression analysis indicated that patients with high levels of fatigue were more likely to be classified into the category of “severe pain catastrophizing - ruminative helplessness and exaggeration” compared to the other two categories, which aligns with previous research findings.45 The intensity and sensitivity of fatigue directly impact pain catastrophizing.13 Fatigue may also indirectly impact pain catastrophizing by causing negative feelings.46 Healthcare professionals can employ mindfulness-based cancer rehabilitation training to guide patients in adopting a non-judgmental, non-demanding, and accepting attitude towards their illness. Such training can enhance patients’ self-regulation and stress management abilities, thereby alleviating fatigue. Furthermore, leveraging wearable devices to create gamified aerobic exercise programs, such as group competitions and scenario-based tracking, can enhance exercise enjoyment, promote social interaction, and improve negative emotional states, ultimately mitigating pain catastrophizing.
To our knowledge, this is the first study to investigate pain catastrophizing following thoracoscopic surgery for lung cancer using LPA, revealing its underlying patterns and determinants. This statistical method establishes a basis for developing customized interventions by reducing variability within subgroups. Additionally, the sufficient sample size enhances the reliability of our findings.
The limitations of this study include the relative homogeneity of the sample in terms of ethnicity and nationality, which necessitates further investigation to determine the generalizability of these findings. Additionally, the cross-sectional design employed does not permit the observation of changes in pain catastrophizing over time among postoperative lung cancer patients, future research could employ longitudinal designs to fill this gap. Third, potential profile analysis as a data analysis method cannot make causal inferences about complex psychological phenomena. Future research could combine qualitative methods to gain a comprehensive understanding of the mechanisms underlying pain catastrophising. Fourth, patient self-reports may be affected by memory bias or subjectivity, which could influence the accuracy of the data. Fifth, the variables selected in this study are limited and do not cover all relevant factors, such as trauma history and illness beliefs. Future research could further explore these areas. Finally, this study did not distinguish between the types and nature of social support. Future research could continue to explore their impact on pain catastrophising in patients after thoracoscopic surgery for lung cancer.
Conclusion
This study is the first to apply Latent Profile Analysis (LPA) to examine the patterns of pain catastrophising in patients after thoracoscopic surgery for lung cancer, identifying three distinct categories:Class 1: “Mild Pain Catastrophizing-Rumination Type”, Class 2: “Moderate Pain Catastrophizing-Ruminative Exaggerative Type”, Class 3: “Severe Pain Catastrophizing-Ruminative Helpless Exaggerative Type”. Statistically significant differences were found among patients in different categories regarding marital status, education level, primary caregiver, tumour location, clinical stage, fatigue, and perception of social support. Healthcare professionals should promptly identify high-risk groups for pain catastrophising and develop targeted interventions based on physiological, psychological, and social factors.
Abbreviations
OR, odds ratio; CI, confidence interval; Ref, Refer; AIC, akaike information criteria; BIC, bayesian information criteria; aBIC, adjusted bayesian information criterion; LMR, lo-Mendell-Rubin test; BLRT, bootstrap likelihood ratio test; LPA, latent profile analysis; PCS, pain catastrophizing scale; BFI, brief fatigue inventory; MSPSS, multidimensional scale of perceived social support.
Acknowledgment
The authors acknowledge the financial support from the Jiangsu Hospital Association (grants No. JSYGY-3-2023-125).
Disclosure
The authors report no conflict of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA a Cancer J Clinicians. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Feray S, Lubach J, Joshi GP, et al. PROSPECT guidelines for video‐assisted thoracoscopic surgery: a systematic review and procedure‐specific postoperative pain management recommendations. Anaesthesia. 2021;77(3):311–325. doi:10.1111/anae.15609
3. Xiao F, Feng H, Tianzhou J, et al. Risk factors of postoperative acute pain after thoracoscopic surgery for patients with early-stage lung adenocarcinoma. J Thorac Cardiovasc Surg. 2023;39(2):5. doi:10.3760/cma.j.cn112434-20211222-00409
4. Zhang Y, Zhou R, Hou B, et al. Incidence and risk factors for chronic postsurgical pain following video-assisted thoracoscopic surgery: a retrospective study. BMC Surg. 2022;22(1):76. doi:10.1186/s12893-022-01522-1
5. Ireland KC, Lalkhen AG. Postoperative analgesia. Anaesthesia and Intensive Care Medicine. 2024;25(12):823–830. doi:10.1016/j.aicm.2024.09.005
6. Sarwar F, Crijns T, Ramtin S, et al. Patient symptom exaggeration is associated with communication effectiveness and trust. PEC Innov. 2022;1:100050. doi:10.1016/j.pecinn.2022.100050
7. Sullivan MJL, Tripp DA. Pain catastrophizing: controversies, misconceptions and future directions. J Pain. 2023;25(3):575–587. doi:10.1016/j.jpain.2023.07.004
8. Petrini L, Arendt-Nielsen L. Understanding pain catastrophizing: putting pieces together. Front Psychol. 2020;11:
9. Mercadante S, Ferrera P, Lo Cascio A, et al. Pain catastrophizing in cancer patients. Cancers. 2024;16(3):568. doi:10.3390/cancers16030568
10. Wang R, Yang L, Zhu X, et al. Current status of pain catastrophizing in patients with lung cancer pain and its analysis of influencing factors. GUANGXI MEDICAL JOURNAL. 2023;45(24):2954–2959,2971. doi:10.11675/j.issn.0253-4304.2023.24.05
11. Simic K, Savic B, Knezevic NN. Pain catastrophizing: how far have we come. Neurol Int. 2024;16(3):483–501. doi:10.3390/neurolint16030036
12. Wilson JM, Colebaugh CA, Meints SM, et al. Loneliness and pain catastrophizing among individuals with chronic pain: the mediating role of depression. JPR. 2022;15:2939–2948. doi:10.2147/jpr.s377789
13. Manning K, Kauffman BY, Rogers AH, et al. Fatigue severity and fatigue sensitivity: relations to anxiety, depression, pain catastrophizing, and pain severity among adults with severe fatigue and chronic low back pain. Behav Med. 2022;48(3):181–189. doi:10.1080/08964289.2020.1796572
14. Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–1184. doi:10.1037/0003-066x.44.9.1175
15. Hasegawa M, Tone S, Naito Y, et al. Preoperative pain catastrophizing affects pain outcome after total knee arthroplasty. J Orthop Sci. 2022;27(5):1096–1099. doi:10.1016/j.jos.2021.05.011
16. Yuan Y, Schreiber K, Flowers KM, et al. The relationship between emotion regulation and pain catastrophizing in patients with chronic pain. Pain Med. 2024;25(7):468–477. doi:10.1093/pm/pnae009
17. Arranz-Martín B, del-Castillo-Pardo-de-Vera JL, Cebrián-Carretero JL, et al. Quality of life, craniomandibular function, and psychosocial factors related to pain and movement in patients with head and neck cancer. Support Care Cancer. 2024;32(6):334. doi:10.1007/s00520-024-08518-y
18. Liu L, Chen S, Yang X, et al. Family and social class differences in sports behavior motivation among college students: an empirical study based on the latent class model. Front Psychol. 2023;14:1070862. doi:10.3389/fpsyg.2023.1070862
19. Zou W, Ding X, Wang H. Exploration of college teachers’ psychological adaptation to online teaching during the COVID-19 pandemic using potential profile analysis. PLoS One. 2022;17(12):e0278896. doi:10.1371/journal.pone.0278896
20. Lyons RF, Mickelson KD, Sullivan MJL, et al. Coping as a communal process. J Soc Pers Relatsh. 1998;15(5):579–605. doi:10.1177/0265407598155001
21. Thai AA, Solomon BJ, Sequist LV, et al. Lung cancer. Lancet. 2021;398(10299):535–554. doi:10.1016/S0140-6736(21)00312-3
22. Yap JC, Joseph L, Chen PP, et al. Validation of the Chinese pain catastrophizing scale (HK-PCS) in Patients with chronic pain. Pain Medicine. 2008;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
23. Huang L, Jiang Q, Ren W. A study of the correlation between coping styles, social support and psychosomatic symptoms in cancer patients. Chinese Mental Health Journal. 1996;10:160–161.
24. Lin CC, Chang AP, Chen ML, et al. Validation of the Taiwanese version of the brief fatigue inventory. J Pain Symptom Manage. 2006;32(1):52–59. doi:10.1016/j.jpainsymman.2005.12.019
25. Kavčič T, Avsec A, Zager Kocjan G. Coping profiles and their association with psychological functioning: a latent profile analysis of coping strategies during the COVID-19 pandemic. Personality and Individual Differences. 2022;185:111287. doi:10.1016/j.paid.2021.111287
26. Berlin KS, Williams NA, Parra GR. An Introduction to latent variable mixture modeling (Part 1): overview and cross-sectional latent class and latent profile analyses. Journal of Pediatric Psychology. 2014;39(2):174–187. doi:10.1093/jpepsy/jst084
27. Lubke G, Neale MC. Distinguishing between latent classes and continuous factors: resolution by maximum likelihood? Multivariate Behavioral Research. 2006;41(4):499–532. doi:10.1207/s15327906mbr4104_4
28. Yousefi Afrashteh M, Abbasi M, Abbasi M. The relationship between meaning of life, perceived social support, spiritual well-being and pain catastrophizing with quality of life in migraine patients: the mediating role of pain self-efficacy. BMC Psychol. 2023;11(1):17. doi:10.1186/s40359-023-01053-1
29. Golkari S, Teunis T, Ring D, et al. Changes in depression, health anxiety, and pain catastrophizing between enrollment and 1 month after a radius fracture. Psychosomatics. 2015;56(6):652–657. doi:10.1016/j.psym.2015.03.008
30. Giardino ND, Jensen MP, Turner JA, et al. Social environment moderates the association between catastrophizing and pain among persons with a spinal cord injury. PAIN. 2003;106(1):19–25. doi:10.1016/s0304-3959(03)00226-4
31. Aily JB, de Almeida AC, Ramírez PC, et al. Lower education is an associated factor with the combination of pain catastrophizing and kinesiophobia in patients with knee osteoarthritis? Clin Rheumatol. 2020;40(6):2361–2367. doi:10.1007/s10067-020-05518-1
32. Kaomba L, Mulwafu W. Assessing informed consent in surgical patients at queen Elizabeth central hospital in Blantyre, Malawi: a cross-sectional study. Malawi Medical Journal. 2025;36(4):249–254. doi:10.4314/mmj.v36i4.3
33. Ding Y, Han J, Yang F. Analysis of status quo and influencing factors of information overload in patients with atrial fibrillation. CHINESE NURSING RESEARCH. 2023;37(2):355–358. doi:10.12102/j.issn.1009-6493.2023.02.034
34. Sun L. A Study on the Latent Profile Analysis and Factors Influencing Neglect of Elderly Caregivers. Shandong: Shandong University; 2023.
35. Ayoubian A, Habibi M, Yazdian P, et al. Survey of nursery errors in healthcare centers, Isfahan, Iran. Global Journal of Health Science. 2015;8(3):43. doi:10.5539/gjhs.v8n3p43
36. Lu Q, Uysal A, Teo I. Need satisfaction and catastrophizing: explaining the relationship among emotional ambivalence, pain, and depressive symptoms. J Health Psychol. 2011;16(5):819–827. doi:10.1177/1359105310392092
37. Booker SQ, Sibille KT, Terry EL, et al. Psychological predictors of perceived age and chronic pain impact in individuals with and without knee osteoarthritis. Clin J Pain. 2020;36(8):569–577. doi:10.1097/ajp.0000000000000842
38. Kuo WK, Chen PJ, Wu MH, et al. Tumor location is an independent prognostic factor in completely resected pathological stage I non-small cell lung cancer: a multicenter retrospective study. Cancers. 2024;16(9):1710. doi:10.3390/cancers16091710
39. Lhl L, Brown VAV, Mol S, et al. Sex differences in pain catastrophizing and its relation to the transition from acute pain to chronic pain. BMC Anesthesiol. 2024;24(1):127. doi:10.1186/s12871-024-02496-8
40. Mahlaq S, Lahlou L, Rammouz I, et al. Factors associated with psychological burden of breast cancer in women in Morocco: cross-sectional study. BMC Women’s Health. 2023;23(1):1–10. doi:10.1186/s12905-023-02769-3
41. Chittem M, Norman P, Harris P. primary family caregivers’ reasons for disclosing versus not disclosing a cancer diagnosis in India. Cancer Nurs. 2020;43(2):126–133. doi:10.1097/NCC.0000000000000669
42. Sullivan MJL. The communal coping model of pain catastrophising: clinical and research implications. Canadian Psychology. 2012;53(1):32–41. doi:10.1037/a0026726
43. Akbari F, Dehghani M, Khatibi A, Vervoort T. Incorporating family function into chronic pain disability: the role of catastrophizing. Pain Res Manag. 2016;2016:6838596. doi:10.1155/2016/6838596
44. Boothby JL, Thorn BE, Overduin LY, et al. Catastrophizing and perceived partner responses to pain. PAIN. 2004;109(3):500–506. doi:10.1016/j.pain.2004.02.030
45. Falling CL, Siegel CA, Salwen-Deremer JK. Inflammatory bowel disease and pain interference: a conceptual model for the role of insomnia, fatigue, and pain catastrophizing. Crohns Colitis 360. 2022;4(3):otac028. doi:10.1093/crocol/otac028
46. Gong Y, Wang Y, Wu W, et al. Study on relationship between pain resilience and pain catastrophizing in elderly patients with chronic musculo-skeletal pain. Geriatr Health Care. 2023;29(1):111–116. doi:10.3969/j.issn.1008-8296.2023.01.025
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.