")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Lean Six Sigma as a Management Tool Helps Standardize Antimicrobial Use in Hospital Settings
Authors Wang Q, Han X, Zhang X, Guo L
Received 7 December 2024
Accepted for publication 20 April 2025
Published 30 April 2025 Volume 2025:19 Pages 3539—3554
DOI https://doi.org/10.2147/DDDT.S510926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mariana Carmen Chifiriuc
Qian Wang, Xinru Han, Xiang Zhang, Lubo Guo
Department of Pharmacy, Central Hospital Affiliated to Shandong First Medical University, Jinan City, Shandong Province, 250013, People’s Republic of China
Correspondence: Lubo Guo, Department of Pharmacy, Central Hospital Affiliated to Shandong First Medical University, No. 105, Jiefang Road, Lixia District, Jinan City, Shandong Province, 250013, People’s Republic of China, Email [email protected]
Objective: This study aimed to standardize antimicrobial use in a hospital setting by implementing the Lean Six Sigma (LSS)-DMAIC model (Define, Measure, Analyze, Improve, Control), addressing the irrational use of antibacterial drugs.
Methods: A retrospective analysis was conducted using data from a single hospital’s information system in Shandong, China, covering antibacterial drug usage from January 2020 to December 2021. The LSS-DMAIC framework was applied, which involved defining problems, measuring key indicators, analyzing causes of irrational use, implementing improvement measures, and controlling outcomes. The project team comprised clinical pharmacists and healthcare professionals who evaluated antibiotic use and compliance with guidelines.
Results: In the whole hospital, the management through LSS-DMAIC led to a significant reduction in the non-standard utilization rate of antibacterial drugs from 32.5% to 11.3% (P < 0.0001), achieving the set target. The intensity of antibacterial drug use decreased to 38.82 Defined Daily Doses (DDDs), meeting national standards. Additionally, the utilization rate of antibacterial drugs has dropped from 43.61% to 40.16% (P < 0.0001), and the average cost of antibacterial drugs per inpatient significantly dropped from 1909.59 RMB (known as Renminbi, which is the legal currency of China) to 1675.20 RMB (P < 0.0001), resulting in substantial annual savings.
Conclusion: The application of the LSS-DMAIC model effectively improved the rational use of antibacterial drugs in the hospital, demonstrating its potential as a valuable management tool in healthcare settings. Continued efforts are necessary to sustain these improvements and further enhance clinician adherence to antimicrobial stewardship practices.
Keywords: lean management, six sigma, DMAIC, antibacterial use intensity, quality management
Introduction
In recent years, with the increasing variety of antibacterial drugs, the irrational use of antibacterial drugs has become more and more serious.1 With its frequent use, the problem of drug resistance has become prominent, which not only wastes medical resources but also affects the treatment of patients’ diseases and increases the difficulty of treatment.2 China is a major consumer of antibiotics. Since 2004, the Chinese government has implemented a comprehensive system for antibiotic management and antimicrobial resistance control within healthcare institutions, supported by a series of regulatory frameworks, including the “Principles for the Clinical Use of Antibiotics” and the “National Action Plan”.3 The level improvement of rational use of antibacterial drugs is the focus of hospital pharmaceutical affairs management.4
However, considerable challenges remain. Hospital administrators and healthcare professionals still lack sufficient awareness of bacterial resistance, and many medical institutions face a shortage of specialized teams, with personnel capabilities requiring further enhancement.3 Some institutions have yet to establish dedicated antimicrobial stewardship entities, and the scarcity of qualified professionals persists. Additionally, the intermittent implementation of antimicrobial management practices by hospital administrators has undermined the effectiveness and long-term sustainability of these efforts.3
With the reform of medical insurance payment method and the normalization of national centralized drug procurement, the standardization of anti-infection treatment is more urgent. National “Tenth Five-Year Plan” Health Plan 5 is clear that medical quality management should be strengthened and the medical quality control system should be improved. Lean management,6 as a scientific and standardized management method, is an effective way to improve the level of pharmaceutical management and service in hospitals and greatly promotes the establishment of a “patient-centered” pharmaceutical service management model. Lean Six Sigma (LSS) is a lean management approach designed to enhance process efficiency by minimizing defects, thereby leading to improved quality and increased customer satisfaction. LSS is successfully implemented in different industrial sectors, and now it has been widely used in the healthcare industry.7 From June 2021 to December 2021, the Lean Management DMAIC Model (Define, Measure, Analyze, Improve, Control) of LSS method was applied in our hospital.8 The LSS-DMAIC can assist healthcare organizations in managing complex tasks by offering structured frameworks to improve procedures and ensuring patient safety.6 Specifically, the LSS-DMAIC framework includes: define and analyze the problems in the management of antibacterial drug use intensity, analyze the main causes of the problems by measuring its key indicators and data, put forward improvement measures, track the improved effects and control the optimized management quality.
The successful implementation of this study will provide theoretical reference and practical guidance for the use and management of antibacterial drugs in hospitals and promote the continuous improvement and improvement of the use and management of antibacterial drugs in hospitals to a certain extent. The report is as follows:
Data and Methods
Research Object
This is a retrospective study. The information system of our hospital was used to collect the use of antibacterial drugs from the beginning of January 2020 to the beginning of December 2021. At the same time, in chronological order, the period from the beginning of January 2020 to the end of June 2021 was included before the lean management was improved, and the period from the beginning of July 2021 to the beginning of December 2021 was included after the improvement. A Gantt chart represents the timeline for different stages of the LSS-DMAIC project (Figure 1).
 |
Figure 1 A Gantt chart represents the timeline for different stages of the LSS-DMAIC project. |
The study was conducted in accordance with the Helsinki Declaration of 1964 and approved by the hospital Ethics Committee of Central Hospital Affiliated to Shandong First Medical University (No. 20241010005). Study data have been fully deidentified, and confidential information of patients has been deleted in accordance with the CIOMS/WHO International Ethical Guidelines for Health-related Research Involving Humans (2016); consequently, the study was deemed exempt from informed consent by study participants.
Methods
Problem Definition (Define)
(1) Problem description
The Defined Daily Dose (DDD) value is a standard value established by the World Health Organization (WHO) and represents the standard daily dose. The reference dose of each antibiotic is based on WHO’s DDD of antimicrobial agents (https://atcddd.fhi.no/atc_ddd_index/). The formula to calculate DDD is as follows:

This formula allows healthcare professionals to determine the number of daily doses of a specific drug based on its actual consumption in milligrams divided by its defined daily dose value. The DDD value serves as a benchmark for evaluating the intensity of drug use in a hospital or healthcare setting.
The information system of our hospital has embedded the rational application module of antibiotics, one of which is the use intensity of antibiotics. HIS (hospital information system) of our hospital can collect the number of inpatients and the number of days of hospitalization of each patient according to clinical departments, and the statistical cycle can be based on day, month, quarter and year. The total drug usage is the accumulation of single dose, frequency and total course of antibacterial drugs used in the corresponding time period. Through the conversion of the actual cost of antibiotics generated by patients, the HIS system excluded the antibiotics used for external use and skin test, and provided the intensity of antibiotic use in each department and the whole hospital, that is, the DDDs of antibiotics consumed per 100 inpatients per day. Finally, the daily doses of the same drug in different time periods or different hospitals were compared to evaluate the consistency and rationality of the data. The use intensity of antimicrobial agents is one of the core indicators of performance evaluation of national tertiary public hospitals, which requires that the use intensity of antimicrobial agents for inpatients in tertiary general hospitals should not exceed 40 DDDs.9,10 In 2020, the use intensity of antibacterial drugs in our hospital was 41.34 DDDs, which was 1.34 different from the target value. Focus on the core of the problem-the rational use of antibacterial drugs, sort out the use process of antibacterial drugs (Figure 2), and determine the rationality of drug use from the evaluation of use indications, pathogenic inspection, empirical treatment, curative effect evaluation, scheme adjustment to re-evaluation and determination of course of treatment.
 |
Figure 2 Flowchart of Antibiotic Use in Inpatients. |
The project team identified the problems to be solved, defined the problem as reducing the irrational utilization rate of antibacterial drugs (Y), and identified the project measurement index: 
Irrational use of antibacterial drugs means non-standardized therapeutic application and perioperative preventive drug use, including unindicated use, non-standardized drug selection, non-standardized drug timing, prolonged course of treatment, unreasonable combination application. Among them, the irrational use of special use grade antibacterial drugs in addition to the above cases also included no dynamic assessment of etiology during treatment, no expert consultation of special use grade antibiotics, and the use of special use grade antibiotics. The definition and standards of special use grade antibacterial drugs refer to the Ministry of Health of the People’s Republic of China Decree No. 84 “Measures for the Administration of Clinical Application of Antibacterial Drugs” (https://www.gov.cn/flfg/2012-05/08/content_2132174.htm). The special use grade antibacterial drugs are antibiotics that have one of the following situations: antibiotics that have obvious or serious adverse reactions and should not be used at will; it is necessary to strictly control the use of antibacterial drugs to avoid the rapid production of resistant bacteria; antibiotics with few clinical data on efficacy and safety; and expensive antimicrobial drugs. The list of the special use grade antibacterial drugs refer to the Classification of clinical application of antibiotics in Shandong Province (http://wsjkw.shandong.gov.cn/zwgk/fdzdgknr/gfxwj/202104/t20210430_3592980.html).
(2) Set up a project team
Notice of the General Office of the National Health and Wellness Commission on Continuous Management of Clinical Application of Antibacterials in 202011 (Guo Wei Ban Yi Fa [2020] No.8)proposed: In order to thoroughly implement the Opinions on Strengthening Pharmaceutical Affairs Management in Medical Institutions to Promote Rational Drug Use and the National Action Plan for Curbing Bacterial Resistance (2016–2020) and continuously improve the level of rational use of antibacterial drugs, all medical institutions should continuously improve their understanding of the importance of clinical application management of antibacterial drugs, clarify the responsible departments and persons, and earnestly implement management responsibilities. Therefore, under the advocacy of the hospital director, under the guidance of lean management experts, and with the support of the director in charge, the medical department and the performance office, the project team set up a team with the director of the pharmaceutical department as the team leader, the deputy director as the deputy team leader and all clinical pharmacists as the team members (Figure 3).
 |
Figure 3 Project Team Composition and Task Assignment. |
(3) Quantitative objectives
According to the baseline review data of antibacterial drugs from January to June, 2021, the non-standard utilization rate of antibacterial drugs was 32.5%. Combined with the actual project, the initial target value was set to reduce the non-standard utilization rate of antibacterial drugs by half, and the limit target was reduced to 0. And make a reasonable implementation time plan, the project lasted for 6 months, which is consistent with the plan.
Data Measurement (Measure)
(1) Find the potential cause of the problem.
Hold a project team meeting, brainstorm, and adopt a causal system diagram (Reasons of system diagram, RCA), to find the potential cause of the problem.
The irrational use of antibacterial drugs is divided into two aspects: preventive use and therapeutic use during perioperative period, and further divided into drug use indications, drug selection, usage and dosage, course of treatment, etc, and the potential reasons leading to irrationality in all aspects are found by using the cause tree diagram analysis (Figure 4). Finally, nine data collection points were determined, including unreasonable indications, inappropriate drug selection, irrational drug use timing, unreasonable course of treatment, combined drug use, drugs taken out of hospital, departments with large abnormal consumption, drugs with large abnormal consumption, and irrational use of special-use antibiotics.
 |
Figure 4 Fish bone diagram analysis of reasons for nonstandard use of antibacterial drugs. Abbreviation: DDDs, Defined Daily Doses. |

(2) Quantization of collected data.
From early July to early December, 2021, data were derived from the rational use of antibiotics module of HIS system, in which all cases can be extracted according to the two categories of surgery and non-surgery. Among them, surgical cases were selected according to the surgical types I, II and III marked on the first page of medical records. Specifically, all the cases of class I incision surgery were selected, and 100 cases of class II and class III incision surgery were randomly selected. A total of 100 non-surgical cases were randomly selected. At the same time, in the rational use of antibiotics module of HIS system, all cases of carbapenem antibiotics, cases of abnormal consumption of the top five antibiotics, cases of combined use of antibiotics, and cases of discharging antibiotics with drugs before and after improvement were extracted. When the data of special use grade antibiotics overlapped with the above surgical and non-surgical cases, only one of them was recorded, not repeated records. All cases collected were randomly selected by Excel.
The review and evaluation of irrational use was conducted by a team composed of clinical pharmacists in related professional fields, such as anti-infection clinical pharmacists, surgical clinical pharmacists, endocrine clinical pharmacists, digestive clinical pharmacists, cardiovascular clinical pharmacists, and anti-tumor clinical pharmacists, who used a unified evaluation table to review and evaluate the selected cases and analyze the data. The evaluation tables of class I incision operation, class II and III incision operation, carbapenem evaluation table, combined drug evaluation table, discharged drug evaluation table and abnormal consumption evaluation table were designed, respectively, and the evaluation was summarized. The formulation of these tables were mainly based on the guidelines for the clinical application of antibiotics (2015 edition), Sanford Guide Fever, National Antimicrobial Guidelines 2nd Edition, Guidelines for the Evaluation of Clinical Application of carbapenems, and Expert Consensus on the Clinical Application of carbapenems.12–15 After data analysis, quality control was carried out by the deputy senior clinical pharmacist of the anti-infection team. After that, the feedback was given to clinicians in each clinical department, and then they gave feedback on the evaluation of the cases according to clinical practice and evidence-based perspectives. Finally, members of the clinical pharmacist team, including the quality control pharmacist, and the clinician would discuss together.
Data Analysis (Analyze)
Looking for key management departments According to the data from January to June, 2021, rank the irrational drug use departments and the intensity of antimicrobial use, and find the key management departments. Analyze the distribution of irrational use from the department level.
Improvement Measures (Improve)
(1) Revise the related system of antimicrobial drug management.
In order to further strengthen the management of antimicrobial drugs and continuously improve the level of clinical rational drug use, according to the National Health Commission’s Notice on Further Strengthening the Management of Antimicrobial Drugs to Contain Drug Resistance (Guo Wei Yi Han [2021] No.73), the management measures for clinical application of antimicrobial drugs in hospitals were revised. A leading group and a management group for clinical application of antimicrobial drugs, headed by the hospital president and the dean in charge, have been set up, respectively, including the heads and business backbones of medical department, pharmacy department, infection office, nursing department, infectious diseases department, outpatient department, supervision room, medical experimental diagnosis center and clinical department, with clear division of labor and responsibility to people. Comprehensively strengthen the management of antimicrobial drugs, improve management measures, and improve the ability of diagnosis and treatment of infectious diseases and the level of rational drug use based on multidisciplinary cooperation.
An antibacterial drug dispensing system and an evaluation system for rational use of antibacterial drugs have been added, covering the whole process of management measures, selection and regular evaluation procurement, temporary procurement, grading management, combined use, intravenous application, prescription dispensing, use (perioperative period, therapeutic use and special use level), evaluation (doctor’s advice and prescription) and monitoring (bacterial resistance monitoring and early warning, clinical application monitoring).
(2) Improve the all-round training mechanism.
① With the help of nail cloud class, online and offline training and assessment on antibacterial drugs are conducted. After all doctors pass the examination, the medical department will grant the antibacterial drugs authority in accordance with the requirements of hierarchical management.
② Conduct targeted training in departments, and clinical pharmacists will combine the disease spectrum and main problems of departments to conduct training on the use policy and drug use norms of antibacterial drugs. And verify the causes of irrational use of antibacterial drugs on the spot, discuss one thing at a time, and negotiate solutions on the spot.
③ Hold a special lecture on rational use of antibacterial drugs and invite Professor Guo Yujin, secretary of Clinical Pharmacy Branch of Chinese Medical Association and chairman of Clinical Pharmacy Branch of Shandong Medical Association, to give a lecture in our hospital. Invite the leaders and key personnel of quality management department, pharmacy department, infection management office, cardiac surgery, pediatrics, neurosurgery, spinal surgery, parenteral department and other departments to attend. On-site retrieval in HIS system, direct analysis of clinical cases in our hospital.
(3) Multidisciplinary cooperation, implementation of Antimicrobial Stewardship (AMS)/Multi-disciplinary Treatment (MDT) and standardization of anti-infection diagnosis and treatment.
Under the leadership of the dean in charge, the working group on clinical application of antimicrobial drugs in the hospital was formed by the medical department, the pharmaceutical department and the infection management office, and a specialized AMS management team was established. All relevant departments and clinical departments cooperated with each other to give full play to the role of AMS team, implement AMS management strategy, actively establish anti-infection diagnosis and treatment norms and paths based on evidence-based medicine and pathogenic microbiology and drug resistance mode of our institution, and implement MDT for infectious diseases, severe, respiratory, infection, blood, pharmacy and surgery.
(4) Establish the control path of antibacterial drugs in departments.
First, the main problems in the department were found by drug evaluation and analysis, and then the evidence-based evidence analysis was used to identify the basis of drug use. Around whether to use, what to use, when to use it, how to use it, and how long to use it, the indications for drug use, drug selection, drug use timing, usage and dosage, adjustment and treatment suggestions were given, and specific cases were analyzed.
(5) Performance appraisal, dynamic evaluation of indicators
In order to further strengthen the management of antibacterial drugs in our hospital, promote the rational use of antibiotics in clinic and reduce the intensity of the use of antibacterial drugs in our hospital, according to the Guiding Principles for Clinical Application of Antibacterials (2015 Edition), Expert Consensus on Clinical Rational Use and Management of Carbapenem Antibacterials in Shandong Province and other related documents, the Evaluation Indicators and Requirements for Clinical Application Management of Antibacterials in our hospital were formulated, and the use of antibacterial drugs was included in the performance appraisal of departments, and the monitoring and supervision were dynamically evaluated.
(6) Closed-loop feedback of evaluation and monitoring shall be connected by special personnel.
Every month, the evaluation and monitoring situation will be fed back to the director of clinical department by nailing, and online communication will be carried out, and rectification opinions will be collected and publicized on the hospital intranet. A special person is set up for docking, clinical pharmacists are re-divided into feedback departments according to their specialties, and clinical departments are provided with quality control contacts for pharmaceutical affairs management, thus establishing a good medical communication platform to facilitate daily communication of pharmaceutical affairs management such as antibacterial drugs.
(7) Making a knowledge set of rational drug use
Develop a knowledge base suitable for the whole hospital, such as the knowledge of the use intensity of antibacterial drugs and the operation list of anaerobic ability of common antibacterial drugs. Make personalized suggestions on the rational use of antibacterial drugs in the department.
(8) Improvement of taking medicine out of hospital: increase the operating instructions for taking medicine out of hospital, and increase the production of medicine boxes for dispensing machines, so as to facilitate the packaging and distribution of antibiotics.
(9) Abnormal consumption drugs According to the evidence-based evidence, the daily consumption DDDs of some antibacterial drugs is set in the rational drug use system, and the abnormal consumption drugs are stopped when necessary, and the perioperative indications and duration are strictly used under endoscope.
(10) Informatization helps the cooperation between rational drug use and information department, optimizes the statistical method of antibacterial drug indicators, and eliminates skin tests, external use, washing, etc. to make it more accurate. Set the daily consumption DDDs of antibacterial drugs with the help of rational drug use system. To realize the consultation before the use of special-grade antibacterial drugs, and to open doctor’s orders after the consultation, so as to ensure the rationality of drug use.
Effect Confirmation and Control (Control)
(1) Effect confirmation
After analyzing the potential reasons leading to irrational use, the critical-to-quality (CTQs) measurement was decided by the team of clinical pharmacists mentioned above. The CTQs metrics assessed before and after implementing LSS-DMAIC included: discharge and combined use of antibacterial drugs, the irrational use of antibiotics in the perioperative period, carbapenem, drugs taken out of hospital, therapeutic use and combined use, the non-standard utilization rate, the intensity and utilization rate of antibacterial drugs, and the cost of antibacterial drugs.
(2) Result control
In order to continuously improve and monitor the implementation measures and results, the project team adopted a number of control measures: (1) Index Monitoring. Index monitoring involves systematically assessing and reviewing key performance indicators across the entire hospital as well as within individual departments on a monthly basis. This comprehensive approach ensures that healthcare providers maintain a high standard of care and facilitates early identification of any emerging issues or areas for improvement. By consistently tracking these metrics, the hospital can implement timely interventions to enhance overall performance and patient outcomes. (2) Informatization for Rational Drug Use. The integration of informatization significantly contributes to the promotion of rational drug use within the healthcare system. A rational drug use system is employed to establish daily consumption guidelines in terms of DDDs for certain antibacterial medications. This framework aids healthcare professionals in conducting thorough prescription reviews and evaluating operation case histories. By utilizing data-driven insights, clinicians can make informed decisions regarding drug prescriptions, leading to improved patient safety and therapeutic efficacy. (3) Enhancing Knowledge on Rational Drug Use. To foster a culture of responsible medication practices, it is imperative to improve the knowledge base surrounding rational drug use among healthcare professionals. This can be achieved through ongoing education and training programs that emphasize the importance of evidence-based prescribing, potential drug interactions, and the implications of antimicrobial resistance. By equipping staff with up-to-date knowledge and best practices, the healthcare institution can ensure optimal patient care and minimize the risks associated with inappropriate drug use. (4) Monitoring Antimicrobial Resistance. In light of the growing concern surrounding drug-resistant bacteria, our hospital employs a proactive approach by issuing a comprehensive analysis and countermeasures report on bacterial drug resistance every quarter. By staying informed about the local resistance trends, the hospital can formulate targeted strategies to combat resistance, optimize antibiotic prescribing practices, and ultimately protect patients’ health. (5) Establish quality control standards and procedures for pharmaceutical evaluation of antibacterial drugs (Figure 5). To be specific, we established a quality control framework to evaluate the use of antibacterial drugs in different contexts, including non-surgical prophylactic medication, perioperative prophylactic medication, therapeutic drugs, and special use grade antibacterial drugs.
 |
Figure 5 Quality control standards and processes for the pharmacologic evaluation of antimicrobial drugs. |
Statistical Analysis
The data of normal distribution is represented by the average (standard deviation), and the data of non-normal distribution is represented by the median (quartile range). Classification variables are expressed in numbers (percentages). According to the distribution of variables, continuous variables are compared by paired data T test or analysis of variance, classification variables are compared by chi-square test, and the threshold of statistical significance is P <0.05 (two-tailed), unless a specific P value is provided. Statistical data analysis was conducted through Excel v16.0.15831.20186.
Results
The Distribution of Irrational Antimicrobial Drug Use
A detailed list of antimicrobials in the whole hospital is displayed in Supplementary Table S1. Discharge and combined use of antibacterial drugs in the whole hospital shows that the situation of taking antibiotics out of hospital and combining drugs has been obviously improved after the intervention in June, as shown in Table 1.
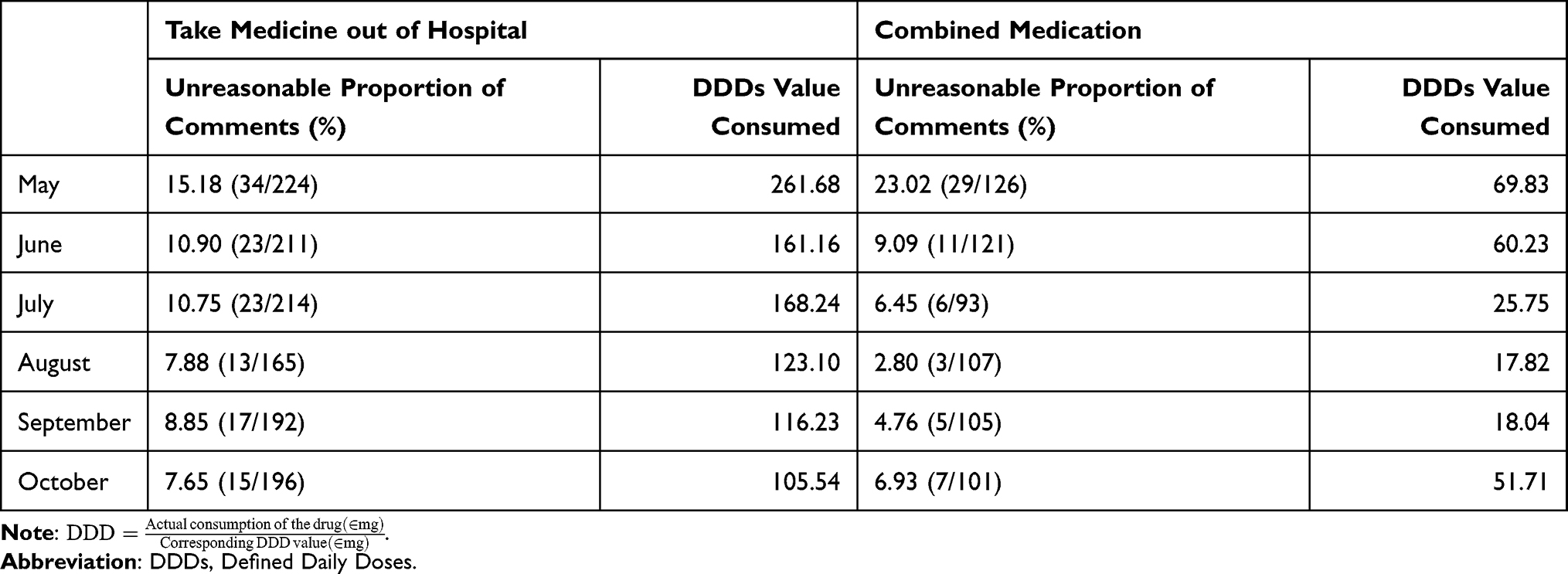 |
Table 1 Discharge and Combined Use of Antibacterials in the Hospital |
After analyzing the distribution of irrational use from the department level, we found that, taking a department as an example, there were 198 cases of irrational use from January to June in 2021 (Figure 6). The main problems were irrational perioperative preventive use (56%), irrational use of carbapenems (30%) and irrational prescription of drugs for discharge (11%). Perioperative preventive use is not standardized, which mainly focuses on unreasonable medication timing, medication course and drug selection, and the course of treatment is divided into over 24 hours and over 48 hours (Figure 7).
 |
Figure 6 Distribution of irrational use of antibiotics in a certain department. |
 |
Figure 7 Category and number of cases of prophylactic use of antibiotics during perioperative period. |
Unreasonable analysis of taking medicine out of hospital: The problem of taking medicine out of hospital to prescribe antibacterial drugs mainly focuses on the temporary prescription in boxes, and some drugs cannot be put in pieces, so they are always asked to bring their own.
Unreasonable analysis of combined use of anti-anaerobic drugs: The unnecessary combined use of anti-anaerobic drugs focuses on the combined use of piperacillin tazobactam or meropenem and nitroimidazole. Clinically, they are worried that the first two cannot cover anaerobic bacteria or that the clinical manifestations of the disease are serious and need to be strengthened. On-site verification, one reason is insufficient understanding of antibacterial spectrum of antibacterial drugs, and the other is different understanding of serious diseases and infections.
Analysis of Abnormal Drug Consumption
Through the review of 323 cases of abnormal drug consumption, it was found that 137 cases involved perioperative preventive medication, and 114 cases involved endoscopic operation. The main problems were inappropriate course of medication and drug selection. In terms of usage and dosage, etimicin is different from the instructions and guidelines.
Generally speaking, there is a big difference between departments. Perioperative preventive medication is mainly manifested in inappropriate medication timing, medication course and drug selection, the use of carbapenem antibiotics needs to be strengthened, there are unreasonable combination medication and unreasonable doctor’s advice, and awareness, system and quality control need to be strengthened.
After the improvement through LSS-DMAIC, the irrational use of antibiotics in the perioperative period, carbapenem, drugs taken out of hospital in the department decreased significantly compared with that before the improvement (P < 0.05), whereas therapeutic use and combined use showing no significant change, and the use intensity of antibiotics significantly decreased in department (P < 0.0001), as shown in Table 2.
 |
Table 2 Non-Standard Use of Antibacterials in Departments and Their Intensity of Use |
Overall Situation of Antibacterial Drug Use in the Whole Hospital
After the improvement, the non-standard utilization rate, intensity and utilization rate of antibacterial drugs in the hospital were significantly reduced, and the per capita antibacterial drug cost significantly decreased (P < 0.0001), as shown in Table 3. To be specific, as far as the whole hospital is concerned, the non-standard utilization rate of antibacterial drugs has significantly dropped from 32.5% to 11.3% (P < 0.0001), achieving the set target. In 2021, the use intensity of antibacterial drugs in hospitals dropped to 38.82 DDDs (P < 0.0001), which met the national requirements. It can benefit 35,439 inpatients (source: HIS antibacterial drug index) every year, and the utilization rate of antibacterial drugs has dropped from 43.61% to 40.16% (P < 0.0001). In order to save patients’ cost, the average cost of antibacterial drugs for inpatients decreased from 1909.59 RMB/person before improvement to 1675.20 RMB/person (P < 0.0001) (source: HIS antibacterial drug index), and the cumulative annual savings were 234.39 RMB/person ×35439 person/year = 8.3 million RMB/year. Strengthening the awareness of rational use and drug resistance of antibacterial drugs, improving the quality of rational use of antibacterial drugs, is conducive to the implementation of diagnosis-related group (DRG). Strengthen the monitoring of adverse drug reactions of antibacterial drugs, collect a total of 138 cases of reports, and form hospital-level pharmacovigilance and clinical medication suggestions every quarter to ensure the safety of patients’ medication.
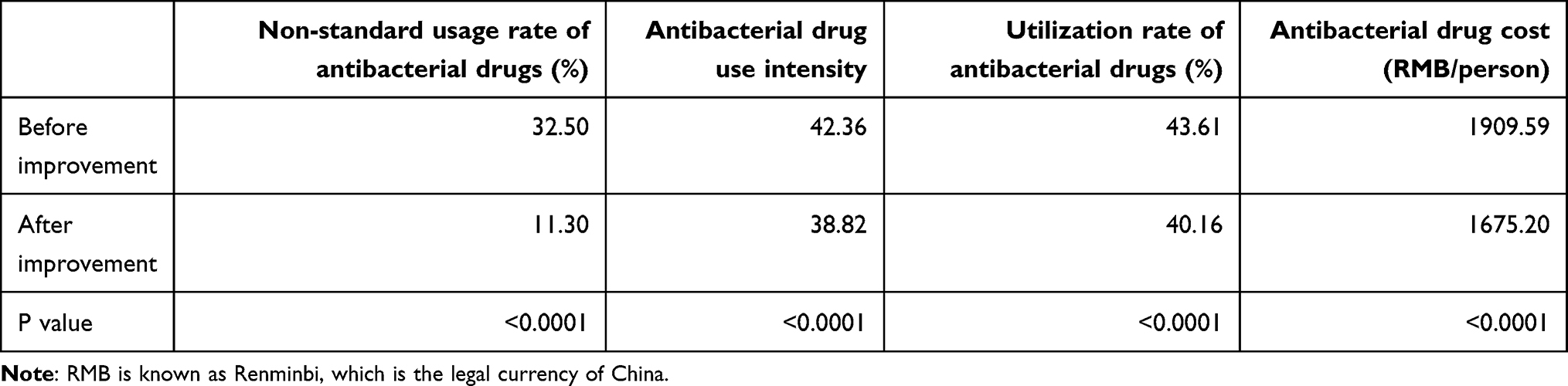 |
Table 3 Overall Situation of Antimicrobial Use in the Whole Hospital |
Discussion
In the current global scope, antimicrobial resistance has become a serious public health challenge, which has brought great pressure and challenge to the medical system.16,17 According to the data of the WHO, antimicrobial resistance has become a serious problem threatening human health and life, which may lead to the increase of infection cases, the increase of treatment failure rate and the increase of medical expenses.1 Abuse and irrational use of antibacterial drugs is one of the main reasons leading to the development of drug resistance.18 Therefore, strengthening the rational use of antibacterial drugs has become one of the urgent tasks facing the current medical system. Abuse and irrational use of antibacterial drugs is one of the main reasons leading to the development of drug resistance. Therefore, strengthening the rational use of antibacterial drugs has become one of the urgent tasks facing the current medical system.19,20
In order to effectively deal with the problem of antimicrobial resistance, countries have formulated a series of policies and measures, including strengthening the management of antimicrobial agents and promoting the rational use of antimicrobial agents. In this context, lean management, as an effective management method, has been widely used in medical institutions and achieved certain results.21 Lean management aims at minimizing waste, and improves the quality of medical services by optimizing processes, improving efficiency, reducing costs, so as to realize the rational allocation and utilization of medical resources.22 In the field of antibacterial drug management, the application of lean management can not only help hospitals to use antibacterial drugs rationally, reduce abuse and unnecessary use, but also improve the awareness and skills of medical staff and promote the standardization and scientific use of antibacterial drugs.23 However, there are still some problems and challenges in the application of lean management in the use of antibacterial drugs in hospitals, such as imperfect management system, insufficient training and education of medical staff, and incomplete collection and analysis of antibacterial drug use data. Therefore, how to further strengthen the application of lean management in the use of antibacterial drugs in hospitals and improve the management level and effect has become one of the important problems to be solved urgently.
In this study, it can be found that the overall use of antibacterial drugs in hospitals has been significantly improved by using lean management to help intervene. This shows that lean management can promote the use and management of clinical drugs. This is also consistent with the previous research results of Wraae D A C and others.22 The main reasons are as follows: lean management emphasizes improving efficiency and reducing costs by optimizing the process, and in the use management of antibacterial drugs in hospitals, lean management can help departments optimize the prescription, approval and distribution of antibacterial drugs, thus reducing unnecessary use of antibacterial drugs and avoiding abuse and overuse.24 At the same time, in the process of lean management, hospitals can strengthen the training and education of medical staff by establishing standardized antibacterial drug use processes and operating norms, ensure the standardization and scientificity of antibacterial drug use, and then reduce the risk of drug resistance development to some extent. In addition, the lean management data used in this study are all from the hospital medical records. By using the lean management method, a data monitoring and evaluation system of antibacterial drug use can be established to a certain extent, and the existing problems can be found and solved in time, thus optimizing the efficiency and level of antibacterial drug use management, and further promoting the management of clinical drug use to a certain extent.
Based on the detailed analysis, we found a dramatic reduction in the non-standard utilization rate of antibacterial drugs, which dropped from 32.5% to 11.3%. This substantial improvement can be attributed to the implementation of the strict guidelines of LSS-DMAIC, monitoring systems, and quality control measures. In addition, the use intensity of antibacterial drugs decreased to 38.82 DDDs, meeting national requirements. This reduction seemed less dramatic than the non-standard utilization rate because use intensity is influenced by both the volume and duration of antibiotic use. While interventions may have reduced unnecessary prescriptions, the intensity metric also depends on the severity of infections and patient conditions, which are less controllable. Certain cases (severe infections or immunocompromised patients) still require prolonged or high-dose antibiotic therapy, limiting the overall reduction in use intensity. Moreover, the utilization rate of antibacterial drugs decreased from 43.61% to 40.16%, showing a relatively modest improvement. After all, antibiotics are essential for treating bacterial infections, and their use cannot be eliminated entirely. Our focus was on reducing inappropriate use rather than overall utilization. At the same time, by curbing unnecessary prescriptions and optimizing drug selection, the per capita cost of antibacterial drugs decreased, leading to a reduced overall expenditure on antibiotics. Nevertheless, some departments or clinicians may have been slower to adopt new practices, particularly in areas where antibiotic use is deeply ingrained in clinical routines, which affects the utilization rate of antibacterial drugs and the relevant cost. Future efforts should focus on sustaining these improvements, addressing department-specific challenges, and further enhancing clinician awareness and adherence to guidelines.
The results of the study are consistent. The main reasons are as follows: lean management emphasizes improving efficiency and reducing costs by optimizing the process, and in the use management of antibacterial drugs in hospitals, lean management can help departments optimize the prescription, approval and distribution of antibacterial drugs, thus reducing unnecessary use of antibacterial drugs and avoiding abuse and overuse. At the same time, in the process of lean management, hospitals can strengthen the training and education of medical staff by establishing standardized antibacterial drug use processes and operating norms, ensure the standardization and scientificity of antibacterial drug use, and then reduce the risk of drug resistance development to some extent. In addition, the lean management data used in this study are all from the hospital medical records. By using the lean management method, a data monitoring and evaluation system of antibacterial drug use can be established to a certain extent, and the existing problems can be found and solved in time, thus optimizing the efficiency and level of antibacterial drug use management, and further promoting the management of clinical drug use to a certain extent.
In this study, we used LSS-DMAIC to help standardize antimicrobial use intensity in our hospital. Compared with the FOCUS-PDSA (Find, Organize, Clarify, Understand, Select, Plan, Do, Study, Act) management tool, in this context, LSS-DMAIC has some advantages. First, LSS-DMAIC provides a highly structured, data-driven methodology that is particularly effective in addressing complex healthcare challenges like antimicrobial stewardship.7 Unlike FOCUS-PDSA, which is more iterative and exploratory, LSS-DMAIC emphasizes rigorous data collection and analysis at every stage.25 Furthermore, LSS-DMAIC involves advanced tools (eg fishbone diagrams) to identify root causes of problems. Using this approach, for instance, the study revealed that irrational drug use timing was a potential reason leading to irrational use of antibacterial drugs. Such insights are less likely to emerge from the simpler FOCUS-PDSA framework, which focuses more on iterative testing of solutions rather than deep problem analysis.25 Overall, LSS-DMAIC has the advantages of data-driven decision-making, emphasizing long-term monitoring and control to ensure continuity and stability of improvement, and is more suitable for complex context requiring in-depth analysis.7
The success of LSS in improving healthcare quality, such as antimicrobial stewardship, depends on tailoring the methodology to the specific context of each institution. The LSS model could be adapted for smaller hospitals by focusing on a single department and using simpler tools, while larger hospitals could scale it across multiple departments and leverage advanced data analytics. Herein, LSS has proven effective in achieving short-term gains, but its long-term sustainability necessitates sustained leadership support, integration into routine workflows, regular feedback loops, staff engagement and ongoing training, and technology integration and innovation. In terms of the staff engagement, we formed a team that includes representatives from various departments (eg, pharmacy, nursing, infection control, and clinical specialties) to ensure diverse perspectives and expertise, provided training and education about LSS, and hold regular meetings to review progress, address challenges, and adjust strategies as needed. The successful implementation of LSS not only needs senior leadership to allocate resources and provide overarching framework but also needs the specific interventions (eg, optimizing perioperative medication timing) developed by clinicians and pharmacists. In short, the implementation of LSS project requires a collaboration that combines top-down leadership with staff engagement.
Addressing the challenges of implementing LSS-DMAIC requires a systematic approach that includes cross-departmental collaboration, data-driven analytics, targeted improvements, and continuous monitoring and feedback. To be specific: strengthen training of clinicians in data collection and analysis and the understanding of rational use of antibiotics; conduct in-depth analysis on the specific problems of different departments and formulate targeted measures; standardize the timing, course and selection of perioperative preventive drugs; long-term monitoring of antimicrobial drug use indicators, timely detection and correction of problems; publish hospital-level pharmacovigilance and clinical medication recommendations on a quarterly basis to ensure the effectiveness of improvement measures; and incorporate improvement measures into the hospital’s quality management system to ensure their long-term implementation.
The study has several limitations, including: a) The research was conducted in a single hospital, which may impact the generalizability of the findings. Future studies should include a larger sample size from multi-centers; b) The intervention period was relatively short, lasting only six months, which may not be sufficient to observe long-term changes. We plan to collect more long-term data in the future to supplement the effect; c) A control group was not included, making it challenging to justify changes in the LSS; d) There may be biases in the HIS data source due to incomplete or inaccurate data entry; e) Selection bias could exist concerning the departments, staff, and patients involved; f) Potential confounders, such as changes in hospital protocols, other interventions, or external factors like seasonal variations in infections, were not controlled for, which could influence the outcomes. This should be addressed in future studies; g) The LSS project commenced in July 2021, and study samples were collected around this time point. A power analysis of sample size was not performed. The sample size should be specified in future studies to detect meaningful differences in antimicrobial use and costs; h) There is a lack of patient-centered metrics and outcomes (such as infection rates, adverse drug reactions, length of stay, and readmission rates), which should be incorporated in future research to strengthen the argument for the impact of LSS, specifically regarding cost reduction while maintaining the same clinical outcomes; i) The study does not include a formal cost-effectiveness analysis, such as time-driven activity-based costing (TDABC), which should be included in future studies; j) The focus on process measures was limited, such as process improvements, LSS waste reduction, IV to PO conversion, physician compliance with hospital antimicrobial use guidelines, rates of multidrug-resistant organisms, hand hygiene, length of stay, and case mix. This is an important aspect that should be concerned in the future.
Conclusion
The implementation of LSS as a management tool has proven to be an effective evidence-based strategy for standardizing antimicrobial use in hospital settings. The structured approach of LSS facilitates rigorous data collection and analysis, enabling healthcare professionals to pinpoint root causes of inefficiencies and implement targeted interventions.
By applying the LSS-DMAIC framework, our study successfully identified and addressed the irrational use of antibacterial drugs, leading to a significant reduction in the non-standard utilization rate of antibacterial drugs from 32.5% to 11.3% (P < 0.0001) in the whole hospital, and the intensity of antibacterial drug use decreased to 38.82 DDDs, meeting national standards. Additionally, significant reductions were also observed in the utilization rate of antibacterial drugs from 43.61% to 40.16%, and the average cost of antibacterial drugs per inpatient from 1909.59 RMB to 1675.20 RMB (both P < 0.0001), resulting in substantial annual savings.
For these improvements to be sustainable in the long term, it is crucial to integrate LSS principles into the hospital’s routine workflows. In addition, challenges such as resistance to change, insufficient training, and data management issues must be proactively addressed. This requires ongoing leadership support, regular training for staff, and the establishment of continuous feedback mechanisms. Additionally, fostering a culture of collaboration among multidisciplinary teams will enhance adherence to antimicrobial stewardship practices and ensure that all stakeholders are engaged in the process. By providing comprehensive training programs, establishing clear protocols, and utilizing technology for data tracking and analysis, hospitals can overcome these barriers. Ultimately, the successful integration of LSS into antimicrobial management not only enhances patient safety and treatment outcomes but also contributes to the broader goal of combating antimicrobial resistance in healthcare settings.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Helsinki Declaration of 1964, and approved by the hospital Ethics Committee of Central Hospital Affiliated to Shandong First Medical University (No. 20241010005). Study data have been fully deidentified, and confidential information of patients has been deleted in accordance with the CIOMS/WHO International Ethical Guidelines for Health-related Research Involving Humans (2016), consequently, the study was deemed exempt from informed consent by study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Jinan Municipal Health Commission Science and Technology Big Data Project (No.2022-BD-01); Discussion on the integrated management mode of central pharmacy in tertiary hospitals, Shandong Provincial Pharmaceutical Association (No. Kjyw 2024-13).
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Gonabadi NSA, Menbari S, Farsiani H, et al. Antimicrobial susceptibility and virulence gene analysis of Shigella species causing dysentery in Iranian children: implications for fluroquinolone resistance. Heliyon. 2024;10(14):e34384. doi:10.1016/j.heliyon.2024.e34384
2. Meles HN, B. B. A, Gebregergis MW, et al. Prevalence, antimicrobial susceptibility patterns and associated factors of Streptococcus pyogenes among apparently healthy school children in Mekelle city primary schools, Northern Ethiopia. Heliyon. 2024;10(14):e34769. doi:10.1016/j.heliyon.2024.e34769
3. Xiao Y. Antimicrobial stewardship in China: systems, actions and future strategies. Clinl Infect Dis. 2018;67(suppl_2):S135–S141. doi:10.1093/cid/ciy641
4. Klein PA, Wagner GA, Barr RJ, et al. Empiric intralesional tumescent drug delivery of antimicrobials effectively treated a painful necrotizing skin infection. JAAD Case Rep. 2024;50:40–43. doi:10.1016/j.jdcr.2024.03.008
5. Abdallah AB, Alkhaldi RZ. Lean bundles in health care: a scoping review. J Health Organ Manag. 2019;33(4):488–510. doi:10.1108/JHOM-09-2018-0263
6. Ahmed S. Integrating DMAIC approach of Lean Six Sigma and theory of constraints toward quality improvement in healthcare. Rev Environ Health. 2019;34(4):427–434. doi:10.1515/reveh-2019-0003
7. Niñerola A, Sánchez-Rebull MV, B H-LA. Quality improvement in healthcare: six Sigma systematic review. Health Policy. 2020;124(4):438–445. doi:10.1016/j.healthpol.2020.01.002
8. Lei Ding Zongfeng Y, Gengwen H. Comparative analysis of performance appraisal indicators of public medical and health institutions in China. Chin J Hosp Admin. 2021;37(07):534–537.
9. Mitrani-Gold FS, Kaye KS, Gupta V, et al. Older patient age and prior antimicrobial use strongly predict antimicrobial resistance in Escherichia coli isolates recovered from urinary tract infections among female outpatients. PLoS One. 2023;18(5):e0285427. doi:10.1371/journal.pone.0285427
10. C. R, Yin L, Tian L, et al. Correlation analysis between the characteristics of Helicobacter pylori resistance and the antibiotic use density in a hospital from 2012 to 2018. J Healthcare Eng. 2021;2021:5031667. doi:10.1155/2021/5031667
11. China National Health Commission of the People’s Republic Of. Notice of the general office of the national health and wellness commission on continuous management of clinical application of antibacterials [Guo Wei Ban Yi Fa (2020) No. 08] [R], 2020.
12. China National Health Commission of the People’s Republic Of. National health commission of the People’s Republic of China. Guidelines for the clinical application of antimicrobial agents (2015 Edition) [Guo Wei Ban Yi Fa (2015) No. 43] [R]. 2015.
13. China National Health Commission of the People’s Republic Of. National health commission of the People’s Republic of China. Notice on issuing three technical documents including the expert consensus on the clinical application of carbapenem antibiotics [Guo Wei Ban Yi Han (2018) No. 822] [R], 2018.
14. Gilbert Dn Chambers H, Saag M, Pavia AT, Freedman DO, Black D. The Sanford Guide to Antimicrobial Therapy.
15. Commission National Health. National Antimicrobial Guidelines.
16. Mcquaid CF, Ryckman TS, Menzies NA, et al. Potential of pan-tuberculosis treatment to drive emergence of novel resistance. Emerg Infect Dis. 2024;30(8):1571–1579. doi:10.3201/eid3008.240541
17. Xie X, Li X, Huang J, et al. Mutation of the envelope stress-responsive protein CpxA capable of regulating the antimicrobial resistance and virulence of bacteria. Sheng Wu Gong Cheng Xue Bao. 2024;40(7):2022–2037. doi:10.13345/j.cjb.240021
18. Cirillo D, Anthony R, Gagneux S, et al. A successful UN high-level meeting on antimicrobial resistance must build on the 2023 UN high-level meeting on tuberculosis. Lancet Glob Health. 2024;12(8):e1225–e1226. doi:10.1016/S2214-109X(24)00229-8
19. Akande-Sholabi W, Oyesiji E. Antimicrobial stewardship: knowledge, perceptions, and factors associated with antibiotics misuse among consumer’s visiting the community pharmacies in a Nigeria Southwestern State. J Pharm Policy Pract. 2023;16(1):120. doi:10.1186/s40545-023-00629-x
20. Udas S, Chand OB, Shrestha B, et al. The facilitators of and barriers to antimicrobial use and misuse in Lalitpur, Nepal: a qualitative study. BMC Public Health. 2024;24(1):1219. doi:10.1186/s12889-024-18690-9
21. Zdęba-Mozoła A, Rybarczyk-Szwajkowska A, Czapla T, et al. Implementation of lean management in a multi-specialist hospital in Poland and the analysis of waste. Int J Environ Res Public Health. 2022;19(2):800. doi:10.3390/ijerph19020800
22. Wraae CAD, Opstrup N, Kyvik KO, et al. The use and application of lean management methods to research processes-a scoping review protocol. BMJ Open. 2024;14(5):e074207. doi:10.1136/bmjopen-2023-074207
23. Shuya Yang Yang Z, Liang Q, Al E. Application of lean six sigma in the management of antibiotics for class I incisions. Strait Pharm J. 2022;34(03):185–188.
24. Alharthy SH, Ayaad O, Al Mashari AAA, et al. Improving care continuity in oncology settings: a lean management approach to minimize discharges without follow-up appointments. Asian Pac J Cancer Prev. 2024;25(4):1293–1300. doi:10.31557/APJCP.2024.25.4.1293
25. Taylor MJ, Mcnicholas C, Nicolay C, et al. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual Saf. 2014;23(4):290–298. doi:10.1136/bmjqs-2013-001862
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.