")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Levofloxacin–Niflumate Salt Development as a Strategy for Improving Physicochemical Properties and Modulating Antibiotic Potency and Anti-Inflammatory Performance
Authors Nugrahani I, Uekusa H , Hori T, Wu Y, Wibowo MS , Garmana AN , Panjaitan FE
Received 1 January 2025
Accepted for publication 21 May 2025
Published 19 June 2025 Volume 2025:19 Pages 5311—5328
DOI https://doi.org/10.2147/DDDT.S515235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Ilma Nugrahani,1 Hidehiro Uekusa,2 Takaaki Hori,2 Yutong Wu,2 Marlia Singgih Wibowo,1 Afrillia Nuryanti Garmana,3 Febrina Ester Panjaitan1
1Department of Pharmacochemistry, School of Pharmacy, Bandung Institute of Technology, Bandung, West Java, 40132, Indonesia; 2Department of Chemistry, School of Science, Institute of Science Tokyo, Tokyo, 152-8551, Japan; 3Department of Pharmacology, School of Pharmacy, Bandung Institute of Technology, Bandung, West Java, 40132, Indonesia
Correspondence: Ilma Nugrahani, School of Pharmacy, Bandung Institute of Technology, Bandung, West Java, 40132, Indonesia, Email [email protected]
Purpose: This research aimed to develop and characterize a novel levofloxacin–niflumic acid salt, to improve its physicochemical properties, antibiotic potency, and anti-inflammatory effects.
Methods: A 1:1 molar ratio salt was synthesized and its crystal structure determined using single-crystal X-ray diffractometry (SCXRD) also characterized using powder X-ray diffractometry (PXRD), differential scanning calorimetry (DSC), and Fourier transform infrared spectroscopy (FTIR). Scalability was evaluated via neat grinding, solvent-dropped grinding, hot melt mixing, and slurry techniques. Stability under controlled conditions (70– 80%RH/25– 30°C) was assessed using PXRD, DSC, and HPLC solubility measurements, levofloxacin’s antibiotic potency (microdilution), and niflumic acid’s anti-inflammatory activity (in vivo in Wistar rats) were also evaluated.
Results: SCXRD confirmed the formation of a stable multicomponent salt, levofloxacin–niflumate. The slurry method successfully yielded a homogeneous powder with identical structural characteristics to the single crystal. Notably, the salt demonstrated enhanced physical and chemical stability compared to the individual drugs and their physical mixture. The solubility of niflumic acid was significantly increased, and the salt formation positively influenced both levofloxacin’s antibiotic potency and niflumic acid’s anti-inflammatory activity.
Conclusion: The successful development of the levofloxacin–niflumate salt offers a promising strategy to improve the stability and potency of levofloxacin, along with enhanced niflumic acid solubility that contributes to improved anti-inflammatory action. This enhanced profile suggests the potential for more effective and efficient therapeutic use, which could improve patient compliance given the frequent co-prescription of these drugs.
Keywords: levofloxacin, niflumic acid, multicomponent salt, stability, antimicrobial potency, anti-inflammatory activity
Introduction
Niflumic acid is a non-steroid anti-inflammatory drug (NSAID) belonging to the anthranilic acid class, known for its efficacy in managing both acute and chronic inflammatory conditions due to its analgesic and antipyretic properties.1 Its chemical structure (Figure 1A) contains a trifluoromethyl-substituted phenyl ring, endows it with the ability to interact with many kinds of synthon, forming hydrogen bonds, and many polymorphs.2 Based on its structure, this NSAID is poorly soluble in water and has pKa values of 1.9 and 5.3,3 which can limit its bioavailability and, consequently, its clinical application. To overcome these drawbacks, several multicomponent systems been developed. For instance, Kumar et al (2022) demonstrated improved solubility and dissolution profiles of niflumic acid through salt formation with acid-pyridine co-formers,4 which have shown promise in modulating its physicochemical properties. Interestingly, niflumic acid has also been reported to possess adjuvant activity with antibiotics like streptomycin and ampicillin, which might reduce the standard dose of antibiotics up to four times to treat Staphylococcus infections.5 This synergistic activity highlights the potential of NA in combination therapies.
 |
Figure 1 Molecular structure of (A) niflumic acid.2 and (B) levofloxacin.5 |
On the other hand, levofloxacin, is a fluoroquinolone antibiotic used to treat respiratory, urinary, and skin infections, is an amphoteric compound with pKa values of 5.35 and 6.72.6 Its structure (Figure 1B) contains a carboxylic acid moiety as the acidic site and an amine methylamine piperazine as the basic site. This compound is slightly soluble in water and has a solubility dependent on the pH of the environment, reaching its maximum within a narrow pH range of 6.7–6.9.7 To address this, considerable research has focused on developing multicomponent solid forms of levofloxacin with acidic excipients such as dihydroxybenzoic acids citric acid, and metacetamol.7 These approaches have successfully improved its solid-state characteristics, such as stability, solubility, and even palatability. Moreover, certain levofloxacin multicomponent systems have demonstrated enhanced antibacterial potency against clinically relevant pathogens such as Staphylococcus aureus and Escherichia coli,8 which is crucial in combating antibiotic resistance. For instance, Islam et al (2022) investigated the formation of a cocrystal/salt of levofloxacin with phthalimide and caffeic acid, highlighting this solid-state strategy as a promising avenue to improve its antimicrobial efficiency.9
Both levofloxacin and niflumic acid are known to be sensitive to light and moisture, posing challenges in storage and formulation.7,10 Therefore, combining niflumic acid with levofloxacin into a single solid-state structure became challenging and exciting to improve their individual limitations, such as stability, solubility, potency, and anti-inflammatory effects. Our previously investigations involved screening for an optimal molar ratio of levofloxacin and niflumic acid, leading to the identification of a 1:1 stoichiometry that suggested a balanced interaction. That multicomponent system was predicted to form a salt due to the difference of pKa is more than 3,11 named levofloxacin–niflumate.
Building upon these prior efforts to enhance the properties of individual drugs through multicomponent formation, this study aims to comprehensively characterize the novel levofloxacin–niflumate salt. Specifically, we intend to determine the three-dimensional structure using single-crystal X-ray diffraction (SCXRD); scale up the product using various techniques including neat grinding, hot melting, wet grinding, and slurry methods; thoroughly evaluate its stability and solubility; and observe the impact of salt formation on both the antibiotic potency and the anti-inflammatory activity. Solid-state characterization was conducted using electrothermal, differential scanning calorimetry, and Fourier transform infrared. A high performance liquid chromatography (HPLC) assay method was developed to assay the concentration simultaneously for the stability and solubility tests. The results were expected to provide integrative information about levofloxacin–niflumate, form the structure, preparation, solid-state character, stability, solubility, potency, and anti-inflammation performance, completing a clear explanation thoroughly. Furthermore, this research also considers the implementation of green chemistry principles throughout the development process, from initial screening to scale-up. The successful development of a stable, single solid-state form combining these two APIs is also expected to improve patient compliance through a more convenient dosage regimen.
As depicted in Figure 1A, niflumic acid has hydroxyl (OH) and amine (NH) groups, along with three fluorine atoms, all of which can become interaction sites. Meanwhile, levofloxacin in Figure 1B has eight sites. The most acidic niflumic acid is carboxylate with pKa 1.9.3 Meanwhile, the basic element of levofloxacin is methyl amine piperazine with pKa 6.25.6 The significant pKa difference between these functional groups strongly suggests the formation of a salt through proton transfer. The salt reaction of levofloxacin has often been reported to improve its stability because the methyl amine-piperazine was sensitive to UV lighting and oxidation.7 On the other hand, the improvement of physicochemical properties of niflumic acid, which is also unstable towards humidity and lighting,10 has not yet been reported to be overcome by the salt reaction. Therefore, the results of our stability and the solubility enhancement studies would be exciting and valuable. Moreover, any observed improvements in the antibiotic potency and anti-inflammatory activity would represent valuable advancements in the therapeutic application of these drugs.
Materials and Methods
Materials
The material used in this experiment was niflumic acid 98%, levofloxacin hemihydrate 98% (Gracia, Bandung, Indonesia), and carrageenan from TCI (Tokyo, Japan). Next was ethanol 98%, methanol pro HPLC, triethylamine 98%, sodium hydrogen phosphate 98%, and potassium bromide (KBr) crystal from infrared in analytical grade (99%) were purchased from Merck-Sigma (Jakarta, Indonesia), Muller Broth Agar (MBA), and CMC/carboxymethylcellulose from Merck (Berlin, Germany). Bacteria colonies Staphylococcus aureus ATCC 25953 and Escherichia coli ATCC 9001 were provided by Microbiology Laboratory School of Pharmacy, and distillate water was prepared by Water Purification Center, Bandung Institute of Technology (Bandung, Indonesia).
Procedures
~300 mg of equimolar mixture of levofloxacin–niflumic acid was dissolved entirely in ethanol 98% until transparent. The clear solution was filtered and then stored to evaporate the solvent slowly under room conditions in a fume hood (25 ± 2°C) until the clear crystals were obtained. An appropriate size of the single crystal was selected under a microscope and then put in the SCXRD sample holder. Compared to the starting material, the crystal was characterized using PXRD, FTIR, and DSC.
Single Crystal X-Ray Diffraction (SCXRD)
An appropriate single crystal (0.16 × 0.07 × 0.05 mm3) was obtained from ethanol solution 98% and used for the SCXRD study. Rigaku XtaLAB Synergy R, DW system with HyPix X-ray detector and CuKα focused X-ray was used for the diffraction measurement. The initial crystal structure was determined by SHELXT software12 and refined by SHELXL software13 using the least squares method with an anisotropic thermal factor for non-hydrogen atoms. The positions of the hydrogen atoms were calculated geometrically and included in the least squares with the riding atom model. Some critical hydrogen atoms attached to oxygen and nitrogen atoms were located by different Fourier maps, and the positions were refined.
Scaling Up Optimization
The scaling-up technique was developed to prepare the salt quickly while adjusting the solid-state properties. Levofloxacin (~600 mg) and niflumic acid (~400 mg) were mixed thoroughly in a mortar with a stamper, became a physical mixture, and then treated as follows.
Neat Grinding
Ground continuously for 15–30 min without any solvent added.
Wet Grinding
Using a stamper, ground with 96% ethanol ~3 mL in the same mortar until a dry mass was collected.
Hot Melting
The homogenous physical mixture was moved into an evaporated pan and placed in an oven set at 100, 120, and 150°C. The mixture was heated until melting, and the best melting temperature and heating time were recorded.
Slurry Method
~2.5 mL ethanol was added into the levofloxacin–niflumic acid physical mixture (in a 1:1 molar ratio), shaken homogeneously without pressing/grinding, and mixed until white pasta formed. Let it dry under the room condition. The level of solvents was varied, 70,90, 96, and 98%, to investigate the best solvent composition.
Solid-State Characterization
PXRD (Powder X-Ray Diffractometry) Measurement
The powder sample (~50–100 mg) was spread in the hole of the sample holder and then placed in the instrument PXRD Rigaku Smartlab (Tokyo, Japan). Measurement was done at a 5°/min rate in the 2θ = 3–50°. Origin® software composed the diffractogram.
DSC (Differential Scanning Calorimetry) Analysis
The sample (2–5 mg) was filled in an aluminum pan, covered with a lid, and pressed using the hydraulic presser until tightly closed. Then, it was put in the holder of DSC Rigaku Thermoplus EVO2 (Tokyo, Japan) and heated under 20°C/min from room temperature to 250°C for both the starting component and the salt. Microsoft Excel 2023 was used to make the thermogram.
FTIR (Fourier Transform Infrared) Analysis
The background spectrum was recorded using a clean, dry KBr pellet before each sample measurement. Subsequently, 1% of the sample in the dried KBr crystal was compressed to prepare a clear pellet, which was then scanned in the range of 400–4000 cm−1 with FTIR Jasco 4200 Type-A (Oklahoma City, USA). The Origin® software graphed the data.
HPLC Method Development for Assay
The HPLC method was developed and validated for determining solubility and chemical stability. The procedure was as follows: A Zorbax Eclipse XDB-C18 column, 4.5×250 mm in dimension, with pores of 5 µm from Agilent (Santa Clara, California), was installed as a stationary phase in the Waters e2695 (Etten-Leur, Netherlands) HPLC, which used a UV detector. The mobile phase composition was methanol (p.a.)—buffer phosphate pH 2.7 (75:25).
The pH 2.7 phosphate buffer solution was prepared by mixing 4 g sodium dihydrogen phosphate with 400 mL aqua-bi-distillate and 7 mL triethylamine; then, the pH was adjusted to 2.7. All solution was filled into a volume flask of 500 mL, then diluted by aqua-bi-distillate until the sign of the fixed volume was seen. The mobile phase was prepared by mixing 460 methanol pro-HPLC added by 150 mL phosphate buffer solution pH 2.7, shaken and filtered with a filter membrane 0.2 µm, and sonicated for 15 min. The measurement was performed at λ = 290 nm, with an injection volume of 10 µL and a 1 mL/min flow rate. The calibration curves were constructed by measuring the AUC of the chromatogram of a series concentration of the levofloxacin and niflumic acid standard solutions, which should meet the linearity requirement with a coefficient correlation of r = 0.999, accurate, and precise.14,15
Solubility Test
A 500 mg sample was filled into an Erlenmeyer tube with 50 mL. After that, 25 mL of bi-distillate water was added and shaken by ultrasonication; continued added with the more powder sample until the sludge remained and no concentration increased, indicating the saturated condition being reached. Next, 2.5 mL solution was withdrawn and diluted into an appropriate concentration in the measurement range of the validated HPLC method. The sample solution was filtered using a filter membrane of 0.2 µm and injected 10 µL into the HPLC instrument with the validated system. The dilution with the bi-distillate water was done if needed.
Stability Test
The stability test was performed in a natural condition in Bandung, Indonesia, from August to September 2024. The recorded humidity and temperature were 25–30°C and 70–80% RH. A ~500 mg sample was spread in a watch glass and placed on a table beside the glass window to make intensive contact with sunlight. Characterization was done periodically with PXRD and DSC, elaborated with chemical content determination using the validated HPLC assay method. Sampling was done every week for four weeks.
Potency Test
This experiment used a microdilution method to investigate the impact of salt formation on the potency compared to the parent API, especially levofloxacin, and the physical mixture of levofloxacin and niflumic acid, following the guidance in ISO.16 The testing bacteria Staphylococcus and Escherichia sp. were inoculated in the agar media at 37°C for 18–24 h, under sterile conditions. After that, they were taken and inoculated in Mueller-Hinton Broth (MHB) in a growing glass until ~0.5 McFarland turbidity was obtained. They were diluted with MHB 20 folds to find a concentration equal to 106 CFU/mL. The microbe cell number was confirmed by calculating the total plate count.
Next, the bacterial suspension was diluted 10 times with sterile distilled water, and then 0.5 mL of that suspension was added with 4.5 mL of sterile distillate water and homogenized. 0.5 mL was retaken from that solution and put into the next vial containing 4.5 mL of distillate aqua. This step was repeated until the 5th dilution. A total of 1 mL of the 4th (10−4) and 5th (10−5) dilutions were pipetted into a Petri dish, added 15 mL of nutrient agar, and homogenized. Those Petri dishes were labeled, closed with the dish cover, and incubated for 24 h at 37°C.
Afterward, a microdilution method was conducted with 96 wells of the microplate plates, in order of 12 columns and 8 rows. Firstly, the controls were prepared. First, MBH was filled in the number 1 column of wells without bacteria and became a negative control. The second well (column 2) was filled with MHB and bacterial suspension as the positive control. In the three rows, other wells were filled with 100 µL of MHB for each sample concentration. The levofloxacin niflumate and levofloxacin hemihydrate solutions were prepared in equal molarity with levofloxacin content and diluted twice with the MHB solution.
In the measurement step, 100 µL of the sample drug solution in column 12 was mixed with 100 µL MHB, then 100 µL was withdrawn and homogenized with 100 µL of MHB in the 11th column. This procedure was repeated for columns 10, 9, 8, and 3, representing that the wells were filled with equal volume but contained various sample concentrations. Finally, 10 µL of diluted bacterial suspension was added into the microplate columns 12–2, except column 1 as the negative control; they were closed, labelled, and incubated at 37°C for 24 h.
In-vivo Anti-Inflammatory Test
This test was conducted on Wistar rats based on the Ethical Clearance guidance published by the Ethical Committee Bandung, Islamic Institute Bandung, number 198/KEPK-Unisba/VIII/2024.17 As part of the preparation, the male Wistar rats consumed enough water and food for a month until they reached an appropriate weight of 150–200 g. The healthy rats were collected and separated into five groups, each consisting of 5–6 rats. Groups 1–5 were treated as follows.
Group (1) was given CMC-Na suspension only (control). Group (2) was delivered niflumic acid only, and (3) levofloxacin hemihydrate. Next, Group (4) was given a levofloxacin–niflumic acid physical mixture and Group (5) levofloxacin–niflumate salt. After 30 min, they were injected with 1% carrageenan suspension in 0.9% CMC-Na in their left foot paw to induce inflammation. Based on the measured inflammation grade’s paw volume change, the drug effect was observed at 30, 60, 120, 180, 240, 300, and 360 min after the induction. The experiment was carried out following the procedure illustrated in Figure 2. Data were initially recorded in Microsoft Excel 2023. Statistical analysis compared to the significance of differences between the treatment group was performed using one-way analysis of variance (ANOVA) followed by a post-hoc Tukey’s Honestly Significant Difference (HSD) test. A confidence level of 95% was considered statistically significant. For comparison between only two groups, an independent Student’s t-test was used.18 All statistical analyses were conducted using Minitab. Following ethical clearance, the animals were treated appropriately after the experiment.
 |
Figure 2 Experimental illustration of anti-inflammatory test. |
Results
Crystal Morphology and Single Crystal X-Ray Diffraction (SCXRD)
Single crystal preparation from an equimolar solution of levofloxacin and niflumic acid in 98% ethanol by slow evaporation yielded rectangular/diamond-shaped crystals (Figure 3A) and different solid-state characteristics (Figure 3B). This morphology was visually distinct from the needle-like crystals of levofloxacin and the rod—shaped crystals of niflumic acid. Next, SCXRD successfully determined the three-dimensional levofloxacin niflumate crystal structure, as shown in Figure 4, with the crystallographic data summarized in Table 1. The data can be obtained free from The Cambridge Crystallographic Data Centre via www.ccdc.cam.ac.uk/structures, with the submission number 2411188.19
 |
Figure 3 (A) The crystals (200x); (B) The solid-state characteristic data of the levofloxacin–niflumic acid system: DSC (i), X-ray powder diffractogram (ii), and Fourier Transform Infrared spectra (iii). |
 |
Figure 4 (A) Thermal ellipsoid plot with hydrogen bond (light blue line) with 50% probability, (B) Packing structure viewed on the ab plane, (C) molecular stacking diagram viewed along [–1 1 1] direction, (D) Comparison between calculated (upper) and measured (lower) PXRD. |
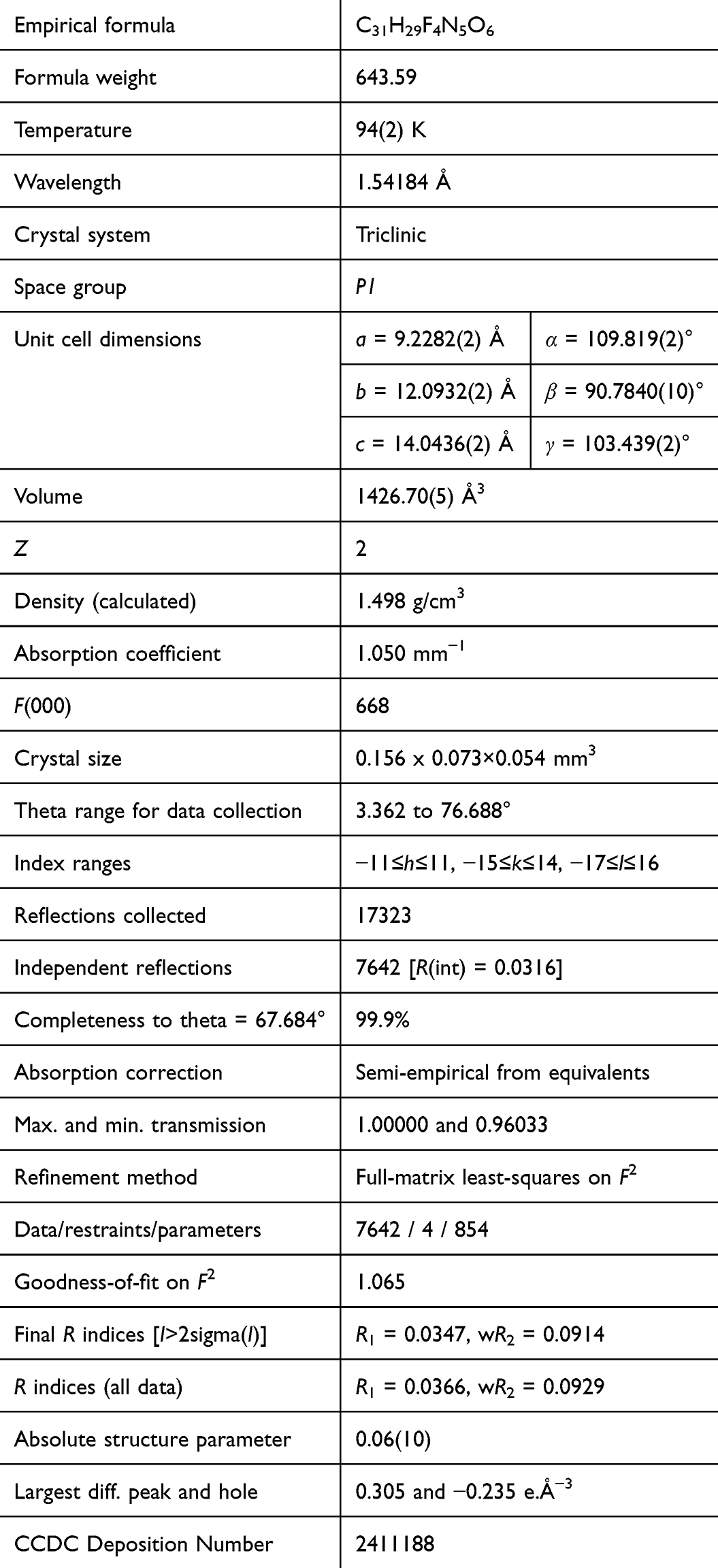 |
Table 1 Crystal Data and Structure Refinement for Levofloxacin Niflumate |
Scaling-Up Methods and Solid-State Characterization
Scaling-up methods were used to increase the product mass for the following experiment stages, including stability, solubility, antibiotic potency, and anti-inflammation tests, using some greener methods than slow evaporation. Four green methods were used: neat grinding, hot melting, wet grinding, and slurry techniques. Figure 5 compiles the diffractogram (A) and thermogram (B) of all techique’s product. The physical mixture and the neat grinding thermograms were melted at a significantly lower temperature, 103°C, named eutectics,20 compared to the components, 229 and 207°C (Figure 3B(i)), without diffractogram change. As information, in the screening, when grinding, the (1:1) levofloxacin hemihydrate was melted with its counterpart, niflumic acid, and became a sticky mass. Meanwhile, the hot melting and wet grinding products had different diffractograms and thermograms. However, only the slurry method using ethanol 96% obtained the same diffractogram and thermogram with the solved single crystal structure. It successfully produced the white powder multicomponent salt, levofloxacin niflumate.
 |
Figure 5 Diffractogram (A) and DSC thermogram (B) of the levofloxacin–niflumic acid physical mixture and levofloxacin niflumate produced by neat grinding, wet grinding, hot melting, and slurry methods. The slurry method product showed a diffractogram and thermogram similar to the structure determined by SCXRD of levofloxacin niflumate. |
Stability and Solubility Test
The possibility of physical and chemical transformation was investigated by conducting a stability test for 4 weeks under a natural room condition, monitored by PXRD and DSC analysis, resulting in data in Figure 6. No significant changes were observed in the salt diffractogram and thermogram, indicating that both forms were stable for 4 weeks under the stability test conditions. In contrast, the PXRD pattern of levofloxacin showed transformation to its monohydrate form.21
 |
Figure 6 Stability sample data for 4 weeks. All samples were stable except for the levofloxacin hemihydrate, which transformed into its monohydrate phase.20 |
Next, Figure 7 depicts the chemical stability data, showing the percentage of decrease in the content of the singular components. The levofloxacin starting material was reduced by ~5%, while the singular niflumic acid content decreased by ~1%. Meanwhile, the salt content was reduced slightly, not more than 1%. Table 2 provides the detailed mass measurement for each week. In a separate experiment, the solubility of levofloxacin niflumate salt was directly compared to that of the individual parent drugs, levofloxacin and niflumic acid. The comparative solubility data are illustrated in Figure 8. Analysis of this data reveals a significant impact of salt formation on the solubility of niflumic acid. Specifically, the solubility of niflumic acid was enhanced by more than tenfold in the salt form compared to its solubility as a single entity. Conversely, the solubility of levofloxacin appeared to decrease upon salt formation.
 |
Figure 7 Chemical stability data for 4 weeks of storage in an open container under 75–85%RH/25-30°C (n = 3). |
 |
Figure 8 Solubility study result (n=6). |
 |
Table 2 Sample Mass Change for 4 weeks During Stability Testing |
Antibiotic Potency Test
The in vitro antibacterial activity of the novel levofloxacin niflumate salt was evaluated against both Gram-positive (Staphylococcus aureus) and Gram-negative (Escherichia coli) bacterial strains. These results were directly compared to the activity of levofloxacin alone and a physical mixture of levofloxacin and niflumic acid. The comparative minimum inhibitory concentration (MIC) values obtained from these assays are presented in Figure 9. The data indicate that levofloxacin alone and the physical mixture of levofloxacin and niflumic acid exhibited the same MIC values against both tested bacterial species. In contrast, the levofloxacin niflumate salt demonstrated lower MIC values, suggesting an increase in its in vitro antibiotic potency compared to levofloxacin in its individual form and in the physical mixture.
 |
Figure 9 Antibiotic potency data of levofloxacin niflumate salt (LNS) compared to levofloxacin hemihydrate (LF) and physical mixture of levofloxacin and niflumate (PM LN). |
Anti-Inflammatory Test
The in-vivo anti-inflammatory performance of levofloxacin niflumate salt was compared to four distinct groups: a negative control, a group treated with niflumic acid alone, a group treated with levofloxacin alone, and a group treated with physical mixture of levofloxacin and niflumic acid. The comparative data on the anti-inflammatory response over time are presented in Figure 10. The result indicates a statistically significant difference in anti-inflammatory performance for the levofloxacin niflumate salt compared to all other groups, particularly when contrasted with the niflumic acid-treated group. This significant difference was observed during the period from 30 to 120 min following the induction of inflammation.
 |
Figure 10 Anti-inflammatory performance shown by the percentage of inflammation volume change (mean ± standard deviation). Abbreviations: CMC Na, carboxymethylcellulose group as the negative control; NA, niflumic acid group; LF, levofloxacin group; PM LN, levofloxacin–niflumic acid physical mixture group; LNS, levofloxacin niflumate salt group. Note: n = 5-6. Star signs (*) represent statistically significant differences at a confidence level 95% (p < 0.05). |
Discussion
Single Crystal Characterization
Figure 3A depicts the different habits of three crystals: levofloxacin hemihydrate and niflumic acid in needle-like form and the salt in rectangular shape. In some cases, the change of crystal habit may be used as a sign of a new solid-state structure formation.22,23 However, solid-state characterization should indeed be performed to confirm it intrinsically. Then, PXRD, DSC, and FTIR analyses confirmed the new phase formation shown in Figure 3B. Figure 3B shows the crystal’s DSC thermogram, X-ray diffractogram, and FTIR spectra. The thermogram showed a specific melting point of the salt at ~178°C compared to the starting materials, niflumic acid at 207°C and levofloxacin at ~229°C with a water release at 113°C. The diffractogram of multicomponent crystal indicated a new crystal was formed with the distinct peaks at 2θ = 5, 8, and 17°, and the FTIR spectra at 1712, 1604, and 1334 cm−1 represented the new interaction involved carboxylic acid and amine moiety.9,24,25
The characteristic carbonyl stretching band (C=O) of niflumic acid, observed at approximately 1720 cm−1 in its pure form, shifted to 1712 cm−1 in the salt, indicating a change in its electronic environment upon interaction. In the spectral region associated with levofloxacin’s methylamine piperazine, a band around 1604 cm−1 was observed, which can be attributed to the deformation vibration of the protonated amine (NH+), indicating proton transfer from niflumic acid. Furthermore, a new band appeared at 1334 cm−1, potentially corresponding to the stretching vibration of the carboxylate anion (COO−), further supporting the deprotonation of niflumic acid. All data confirmed the new solid phase of salt from the reaction of the niflumic acid’s carboxylic with the methyl-amine piperazine of levofloxacin as the most basic and reactive moiety.7
Three-Dimensional Structure Determination Using SCXRD
Next, the molecular and crystal structure shown in Figure 4 confirmed the salt form of levofloxacin–niflumate three-dimensionally, matching the FTIR data. Hydrogen bonding is an essential interaction in this structure. Intra-molecular hydrogen bond in levofloxacin and inter-molecular hydrogen bond between levofloxacin and niflumic acid, along with the proton transfer site, stabilized the molecular and crystal structure. The C–O length of COO– moieties geometrically confirmed these hydrogen bonds.
One cell unit had two units of levofloxacin cation and niflumate anion salt structure in the space group of non-centrosymmetric P1. However, the molecular arrangement was almost centrosymmetric except for the chiral part of levofloxacin. One H atom transferred from the COOH of niflumic acid to the terminal N atom (methyl-amine) of levofloxacin, which was confirmed by the residual electron density on N indicating H atom and the C–O lengths (1.24, 1.29 and 1.24, 1.28Å) of niflumate COO–.
An intra-molecular hydrogen bond was observed in the levofloxacin cation, and an inter-molecular hydrogen bond was observed between the levofloxacin cation and niflumate anion, forming a discrete salt unit structure. The molecular structures with hydrogen bonds and the packing structure are shown in Figure 3A and B, respectively. In the crystal structure, the benzene rings and benzene–COOH stacked by π–π interactions in a ca. 3.5 Å distance along [–1 1 1] direction, as shown in Figure 4C. This feature resulted in a columnar structure composed of cations and anions, leading to a more stable crystal. Completing the data, the calculated and measured PXRD diagram comparison proved that the powder crystals used in all measurements were of the same phase as the single crystal analyzed by SCXRD (Figure 3(D)).
Product Scaling Up Data
In the scaling-up development, four methods: grinding, wet grinding, hot melting, and the slurry technique26 were attempted to multiply the massed salt production, which will be used for further experiments. Neat and hot grinding was developed to reduce solvent usage maximally, which has been reported effective in the multicomponent solid preparation, ie, olanzapine26 and aripiprazole27 multicomponent dosage forms.
As a result, Figure 5 depicts the salt diffractogram and DSC thermogram from the different processes. First, Figure 5A reveals that the neat grinding product had the same diffractogram pattern as the levofloxacin monohydrate-niflumic acid physical mixture, indicating no changes. Meanwhile, the hot melting method produced peaks similar to the measured single crystal but still exhibited the peaks of the starting component. Next, the wet grinding salt’s diffractogram differed from the determined one. Only the slurry product showed the same diffraction pattern as the determined single crystal salt, confirmed as levofloxacin niflumate, under the open room conditions (75–80%RH/25–30°C).
The diffractogram data was elaborated with the DSC thermogram in Figure 5B. The neat grinding failed to produce the targeted salt and only showed an eutectic point at ~103°C; they melted at a significantly lower temperature than their singular phase, 229 and 207°C, still the same as the physical mixture thermogram. Practically, eutectic properties caused grinding and heating to produce sticky matter that is hard to handle in manufacturing.28 This method did not create the new phase, even though it had melted and back to be solidified together.22,29
Next, the hot melting and conventional wet grinding products had a melting point equal to the determined salt, but many other endothermic curves still existed. That profile indicated the possibility of the solvent/water or the remaining unreacted matter. The hot melting failed to repel all entrapped water molecules, which might come from the levofloxacin hemihydrate or environment. Meanwhile, dropped grinding facilitated crystal expansion as the solvent/water was absorbed. That process produced the solvate/hydrate, represented by the broad endothermic curves before the melting point, referred to as a new phase shown in the diffractogram in Figure 5A.
These situations led to the selection of the slurry technique, which provided the same conditions as solvent evaporation but involved only a tiny solvent and the minimization of contact energy. The PXRD data in Figure 5A confirmed that the technique successfully produced the targeted salt, a stable white powder of levofloxacin niflumate. This phenomenon may be caused the slurry technique provided enough time and proper condition for levofloxacin and niflumic acid to ionize, react, and form the stable salt, before any solvent was entrapped.
Physical Stability Profile
Figure 6 summarizes data after 4 weeks of storage and shows that the diffractogram and thermogram of the salts did not change, proving this multicomponent salt was stable during that period. As shown in the crystal structure in Figure 4C, levofloxacin and niflumic acid were stacked by dispersion forces in the multicomponent salt crystal. They formed one-dimensional columnar structure, significantly strengthening the lattice structure. Meanwhile, levofloxacin hemihydrate alone became a monohydrate21 after 3 weeks, as shown in the diffractogram and thermogram changes. The diffractogram showed the monohydrate peaks at 2θ = 8°,11°,16°,21 and the thermogram became broader than before.
Chemical Stability Profile
Chemical stability measured the content level after storage. As reported, levofloxacin7 and niflumic acid10 are sensitive to UV lighting. Hence, the chemical stability of levofloxacin and niflumic acid in the salt was investigated to compare it to the single components. The validated HPLC method explained in the Methods was employed. The samples were stored in the open air, and their chemical content was observed weekly for four weeks. The chemical content stability data was then plotted in a graph in Figure 7.
Based on the mass change of levofloxacin, it can be predicted that not only did levofloxacin hemihydrate transformation occur, but chemical degradation due to environmental disturbances, such as oxygen and UV lighting, caused oxidation on both starting materials. Levofloxacin content decreased by ~5%, related to the change of hemihydrate to monohydrate. Besides, lighting caused its chemical degradation at the methyl piperazine site, which is oxidation sensitive.7,30 Meanwhile, the chemical content of niflumic acid decreased by 1.5%, which was in line with the report that this drug is also unstable in lighting.10
On the other hand, levofloxacin niflumate was stable As previously mentioned, the benzene rings and benzene–COOH stacked by π–π stacking along [–1 1 1] site, made the cations and anions arranged in the columnar structure as shown in Figure 4C and then stabilized the crystal. Moreover, the unstable site of niflumic acid is predicted as the hydroxyl of the carboxylic moiety, and levofloxacin is at its methyl-amine-piperazine site. Hereafter, both sides of instability masked each other after the salt reaction. After 4 weeks, the chemical content of levofloxacin niflumate (molecular weight: 644) in that salt form was only reduced by ~1%, which was probably only due to a small amount of water absorbed but not insignificantly altering the physical and chemical stability.
Solubility Test
The most powerful property of an ideal API is high solubility, especially for oral delivery systems. The more soluble an API is, the faster it will work. Therefore, many efforts were developed to improve solubility, including salt construction. Figure 8 depicts the significant solubility improvement of niflumic acid in the salt form. This enhancement can be attributed to the altered crystal lattice energy and increased polarity resulting from the ionic interactions within the salt structure, as suggested by the new crystal packing observed in Figure 4. The levofloxacin niflumate had more hydrogen bond donor and acceptor sites than niflumic acid, with free sites present after salt formation. This contrasted with parent niflumic acid crystals where all sites are occupied.30 In addition, the interaction with a more polar substance (levofloxacin) assisted niflumic acid in becoming more polar than before, which also affected its activity.31 As an acid, the base environment could push the solubility. In addition, based on the physical properties, the salt was hygroscopic, consequently enhancing solubility.32
All physicochemical observation results met expectations. Besides improving levofloxacin stability, levofloxacin niflumate was proven to increase the solubility of niflumic acid to 11-fold. Conversely, Figure 8 also reveals a decrease in the solubility of levofloxacin in the salt form. This phenomenon can be primarily explained by the common ion effect.33 When levofloxacin niflumate dissolves in water, it dissociates into levofloxacin cations (protonated at the piperazine nitrogen) and niflumate anions (deprotonated carboxylate). The presence of the niflumate counter-ion in solution can shift the dissolution equilibrium of any undissociated levofloxacin species back towards the solid phase, thereby reducing its overall solubility. Additionally, levofloxacin exists as a zwitterion in aqueous solutions around physiological pH.34 The crystal packing and the energy required to break the salt lattice also play a role in the solubility of each component.35 The stronger ionic interactions in the salt lattice might require more energy for levofloxacin to dissolve compared to its individual state.
The enhanced solubility of niflumic acid likely contributes to the accelerated anti-inflammatory effect which will be discussed in the subsequent part. The impact of the decreased levofloxacin solubility on its antibacterial activity needs to be carefully considered in formulation development and in vivo efficacy studies. Further investigations into the dissolution rate and pharmacokinetic profiles of the individual components from the salt are warranted to fully understand the implications of these solubility changes.
Potency Improvement
Furthermore, the potency test also showed that the antimicrobial strength of levofloxacin niflumate was higher than levofloxacin alone, both in the positive and negative Gram bacteria, as shown in Figure 9. Besides the change of permeability, the higher potency toward Staphylococcus aureus and Escherichia coli could be caused by the adjuvant effect of niflumic acid for streptomycin and ampicillin, as mentioned before.4 The change in the molecular environment could influence antibiotics’ polarity and absorptivity, improving their capability to interact with the bacteria membrane and enter the microbe cell.36,37 Moreover, it also affected the anti-inflammation effect of niflumic acid, which was then tested by an in vivo experiment using Wistar rats following the Ethical Guidance and yielded data in Figure 10.
Anti-Inflammatory Activity Improvement
The anti-inflammatory activity profile of the levofloxacin niflumate salt, as shown in Figure 10, revealed a significant reduction in paw edema volume within the first two hours after carrageenan-induced inflammation. Specifically, an increase in paw volume of approximately 8–16% was observed within 30 minutes in the control group. In contrast, the salt-treated group consistently exhibited the lowest inflammation levels compared to all other groups, including those treated with niflumic acid alone. This trend remained stable through the first two hours post-injection.
Statistical analysis using Student’s t-test and ANOVA (p < 0.05) confirmed significant differences in anti-inflammatory efficacy between the salt and niflumic acid at 30, 60, and 120 min, suggesting that levofloxacin niflumate elicited a better inflammatory response during this time frame than niflumic acid alone during the early phase of inflammation. A plausible explanation for this behavior lies in the improved solubility of niflumic acid in the salt form, which likely facilitated faster absorption and onset of pharmacological action. As solubility often plays a critical role in the bioavailability and onset of NSAID effects, the rapid action observed in the salt form supports its enhanced physicochemical performance.
Interestingly, the anti-inflammatory effect of the salt plateaued after 2 hours, while the niflumic acid group began to exhibit increased efficacy starting at the 3-hour mark. This delayed response may reflect the slower dissolution and absorption of the free acid form due to its lower intrinsic solubility. By 4–6 hours post-administration, the anti-inflammatory effects of both treatments appeared to converge, indicating an eventual equilibrium in systemic drug levels and pharmacodynamic outcomes.
Furthermore, levofloxacin alone exhibited a modest yet noticeable reduction in paw inflammation compared to the negative control (CMC-Na), suggesting an inherent anti-inflammatory property. This observation aligns with prior studies that report levofloxacin’s ability to attenuate inflammation independently of its antibacterial action. For example, levofloxacin has been shown to reduce pulmonary inflammation through inhibition of pro-inflammatory cytokines and chemokines such as TNF-α, IL-6, and MCP-1.38–40 Other studies also explained that levofloxacin inhibited the production of cytokines and chemokines.41,42 These mechanisms might have contributed to the enhanced overall anti-inflammatory response of the levofloxacin–niflumate salt, indicating potential pharmacological synergy between the two components.
All data supporting the summary that this antibiotic-antiinflammation multicomponent salt combined the benefits of both components, improving solubility, stability, potency, and anti-inflammation activity, make this salt very suitable for further development. In particular, this salt reaction can handle specific eutectic characteristics, which cause problems in the mixing process in manufacturing. Moreover, combining two drugs can increase patient compliance and be more economical than the separated dosage form. This salt combination in a solid packing is suggested to be formulated in solid and liquid dosage forms, such as tablets, capsules, syrup/elixir, and injections, to kill the microbes and treat the pain in one way.
Conclusion
Levofloxacin reacted with niflumic acid to form a stable salt, which was successfully determined by SCXRD and named levofloxacin niflumate in a stable packing structure. Due to the eutectic phenomenon of their starting material mixture, this combination formation process was sensitive to mechanical and thermal stress before producing a salt. While various solid-state phases were encountered during scaling-up attempts, the slurry method proved to be the only effective technique for producing pure salt, consistent with the single crystal structure. Notably, the formation of this novel salt resulted in a significant (~14-fold) enhancement of niflumic acid’s aqueous solubility and improved the chemical stability of both active pharmaceutical ingredients. Furthermore, the multicomponent salt also demonstrated a 2-times potency of levofloxacin and accelerated and modulated the action on the Wistar mice in-vivo. The development of this stable antibiotic-anti-inflammatory multicomponent system holds significant potential for improving combination therapy. This single entity could offer a more convenient and potentially efficacious approach for simultaneously treating microbial infections and associated inflammatory symptoms, potentially enhancing patient compliance and simplifying treatment regimens. Moreover, the enhanced solubility of niflumic acid and the improved stability of both drugs within the salt could lead to formulations with improved pharmacokinetic profiles and shelf-life, paving the way for novel pharmaceutical formulations with enhanced therapeutic benefits.
Ethics Statement
This study was conducted under the guidelines for the care and use of laboratory animals and was approved by the Ethical Committee Bandung, Islamic Institute Bandung, number 198/KEPK-Unisba/VIII/2024.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Research, Community Services Program, and Innovation Funding, LPPM ITB (Research and Community Service Institution, Bandung Institute of Technology, contract number 036/E5/PG.02.00.PL/2024) (I.N.). JSPS KAKENHI Grant Numbers JP22K05032 and JP24H00005 (HU) supported part of this work.
Disclosure
Prof. Dr. Ilma Nugrahani reports a patent: levofloxacin niflumate salt with the superior potency and anti-inflammation effect” pending. Prof. Dr. Hidehiro Uekusa reports grants from JSPS (Japan Society for the Promotion on Science), during the conduct of the study; grants from JNC Corporation, and grants from Sumitomo Chemical Co., Ltd., outside the submitted work. The authors declare no known financial conflicts of interest or personal relationships that could have influenced the findings presented in this study.
References
1. Tsai CC, Lin HM, Lee MJ. Solubility of niflumic acid and celecoxib in supercritical carbon dioxide. J Supercritical Fluids. 2014;95:17–23. doi:10.1016/j.supflu.2014.07.026
2. Cruz-Cabeza AJ, Bernstein J. Conformational polymorphism. Chem Rev. 2014;114(4):2170–2191. doi:10.1021/cr400249d
3. DrugBank. Niflumic Acid; 2024. Available from: https://go.drugbank.com/drugs/DB04552.
4. Kumar V, Goswami PK, Balendra, et al. Multicomponent solids of niflumic and mefenamic acids based on acid-pyridine synthon. Front Chem. 2022;10. doi:10.3389/fchem.2022.729608
5. Chakraborty J, Mondal R, Sultana J, Banerjee S, Mandal AK, Sarkar H. Repurposing of dibucaine and niflumic acid as antimicrobial agents in combination with antibiotics against Staphylococcus aureus. Journal of Antibiotics. 2024;77:746–756. doi:10.1038/s41429-024-00759-7
6. DrugBank. Levofloxacin; 2024. Available from: https://go.drugbank.com/drugs/DB01137.
7. Shinozaki T, Ono M, Higashi K, Moribe K. A novel drug-drug cocrystal of levofloxacin and metacetamol: reduced hygroscopicity and improved photostability of levofloxacin. J Pharm Sci. 2019;108(7):2383–2390. doi:10.1016/j.xphs.2019.02.014
8. Le-Deygen IM, Mamaeva PV, Skuredina AA, Safronova AS, Belogurova NG, Kudryashova EV. Combined system for the simultaneous delivery of levofloxacin and rifampicin: structural and functional properties and antibacterial activity. J Funct Biomater. 2023;14(7):381. doi:10.3390/jfb14070381
9. Islam NU, Umar MN, Khan E, et al. Levofloxacin cocrystal/salt with phthalimide and caffeic acid as promising solid-state approach to improve antimicrobial efficiency. Antibiotics. 2022;11(6):797. doi:10.3390/antibiotics11060797
10. ThermoFisher. Niflumic acid, 99+%, thermo scientific chemicals; 2024. Available from: https://www.thermofisher.com/order/catalog/product/J60489.06.
11. Lemmerer A, Govindraju S, Johnston M, Motloung X, Savig KL. Co-crystals and molecular salts of carboxylic acid/pyridine complexes: can calculated p K a’s predict proton transfer? A case study of nine complexes. CrystEngComm. 2015;17(19):3591–3595. doi:10.1039/c5ce00102a
12. Sheldrick GM. SHELXT – integrated space-group and crystal-structure determination. Acta Crystallogr A. 2015;71(1):3–8. doi:10.1107/S2053273314026370
13. Sheldrick GM. Crystal structure refinement with SHELXL. Acta Crystallogr C Struct Chem. 2015;71. doi:10.1107/S2053229614024218
14. European Medicines Agency. ICH guideline Q14 on analytical procedure development - Step 2b. Committee for Human Medicinal Products (CHMP): EMA/CHMP/ICH/195040/2022.
15. Pharmacopeia US. USP-NF < 1225> Validation of Compendial Methods. USP 32 - NF27. Published online 2009.
16. Leber AL. Synergism Testing: broth Microdilution Checkerboard and Broth Macrodilution Methods. In: Clinical Microbiology Procedures Handbook. 2016:5.16.1–5.16.23. doi:10.1128/9781555818814.ch5.16
17. Kiani AK, Pheby D, Henehan G, et al. Ethical considerations regarding animal experimentation. J Prev Med Hyg. 2022;63(2). doi:10.15167/2421-4248/jpmh2022.63.2S3.2768
18. Yang XW, Liu FQ, Guo JJ, et al. Antioxidation and anti-inflammatory activity of Tang Bi Kang in rats with diabetic peripheral neuropathy. BMC Complement Altern Med. 2015;15(1). doi:10.1186/s12906-015-0600-0
19. The Cambridge Crystallographic Data Centre. Deposit number 2411188; 2024. Available from: www.ccdc.cam.ac.uk/structures.
20. Bazzo GC, Pezzini BR, Stulzer HK. Eutectic mixtures as an approach to enhance solubility, dissolution rate and oral bioavailability of poorly water-soluble drugs. Int J Pharm. 2020;588. doi:10.1016/j.ijpharm.2020.119741
21. Freitas J, Viana O, Cabral de Melo C, Bitencourt M, de Araújo M, Doriguetto A. Phase transition and solubility of levofloxacin crystal forms: anhydrates versus hydrates. J Therm Anal Calorim. 2024;149:7345–7354. doi:10.1007/s10973-024-13252
22. Tiwary AK, Jindal M. Crystal Habit Changes and Dosage Form Performance. In: Encyclopedia of Pharmaceutical Science and Technology.
23. Ji X, Wang J, Wang T, et al. Understanding the role of solvent in regulating the crystal habit. Cryst Eng Comm. 2022;24(12):2226–2240. doi:10.1039/d1ce01486b
24. Chemguide. Interpreting an infra-red spectrum; 2014. Available from: https://www.chemguide.co.uk/analysis/ir/interpret.html.
25. LibreTexts. Spectroscopy of Carboxylic Acids and Nitriles. Available from: https://chem.libretexts.org/Bookshelves/Organic_Chemistry/Organic_Chemistry_(OpenStax)/20%3A_Carboxylic_Acids_and_Nitriles/20.08%3A_Spectroscopy_of_Carboxylic_Acids_and_Nitriles.
26. Sarmah KK, Nath N, Rao DR, Thakuria R. Mechanochemical synthesis of drug-drug and drug-nutraceutical multicomponent solids of olanzapine. Cryst Eng Comm. 2020;22(6):1120–1130. doi:10.1039/c9ce01504c
27. Butreddy A, Almutairi M, Komanduri N, Bandari S, Zhang F, Repka MA. Multicomponent crystalline solid forms of aripiprazole produced via hot melt extrusion techniques: an exploratory study. J Drug Deliv Sci Technol. 2021;63. doi:10.1016/j.jddst.2021.102529
28. Hoang Pham UG. Pharmaceutical applications of eutectic mixtures. J Dev Drugs. 2013;02(03). doi:10.4172/2329-6631.1000e130
29. Li W, Shi P, Jia L, et al. Eutectics and salt of dapsone with hydroxybenzoic acids: binary phase diagrams, characterization and evaluation. J Pharm Sci. 2020;109(7):2224–2236. doi:10.1016/j.xphs.2020.04.003
30. Lv H, Han P, Li X, et al. Electrocatalytic degradation of levofloxacin, a typical antibiotic in hospital wastewater. Materials. 2021;14(22):6814. doi:10.3390/ma14226814
31. Egorova KS, Gordeev EG, Ananikov VP. Biological activity of ionic liquids and their application in pharmaceutics and medicine. Chem Rev. 2017;117(10):7132–7189. doi:10.1021/acs.chemrev.6b00562
32. Ng LH, Ling JKU, Hadinoto K. Formulation strategies to improve the stability and handling of oral solid dosage forms of highly hygroscopic pharmaceuticals and nutraceuticals. Pharmaceutics. 2022;14(10):2015. doi:10.3390/pharmaceutics14102015
33. David SE, Timmins P, Conway BR. Impact of the counterion on the solubility and physicochemical properties of salts of carboxylic acid drugs. Drug Dev Ind Pharm. 2012;38(1):93–103. doi:10.3109/03639045.2011.592530
34. Lambert A, Regnouf-de-Vains JB, Ruiz-López MF. Structure of levofloxacin in hydrophilic and hydrophobic media: relationship to its antibacterial properties. Chem Phys Lett. 2007;442(4–6):281–284. doi:10.1016/j.cplett.2007.05.077
35. Elder DP, Holm R, De Diego HL. Use of pharmaceutical salts and cocrystals to address the issue of poor solubility. Int J Pharm. 2013;453(1):88–100. doi:10.1016/j.ijpharm.2012.11.028
36. Almeida-Bezerra J, Menezes S, Silva J, et al. Analysis of the antibiotic-potentiating activity, absorption, distribution, metabolism, and excretion (ADME) and the molecular docking properties of phytol against multi-drug-resistant (MDR) strains. Antibiotics. 2024;13(12):1171. doi:10.3390/antibiotics13121171
37. Ritsema JAS, Herschberg EMA, Borgos SE, et al. Relationship between polarities of antibiotic and polymer matrix on nanoparticle formulations based on aliphatic polyesters. Int J Pharm. 2018;548(2):730–739. doi:10.1016/j.ijpharm.2017.11.017
38. Tsivkovskii R, Sabet M, Tarazi Z, Griffith DC, Lomovskaya O, Dudley MN. Levofloxacin reduces inflammatory cytokine levels in human bronchial epithelia cells: implications for aerosol MP-376 (levofloxacin solution for inhalation) treatment of chronic pulmonary infections. FEMS Immunol Med Microbiol. 2011;61(2):141–146. doi:10.1111/j.1574-695X.2010.00755.x
39. Uriarte SM, Molestina RE, Miller RD, et al. Effects of Fluoroquinolones on the Migration of Human Phagocytes through Chlamydia pneumoniae -Infected and Tumor Necrosis Factor Alpha-Stimulated Endothelial Cells. Antimicrob Agents Chemother. 2004;48(7):2538–2543. doi:10.1128/AAC.48.7.2538-2543.2004
40. Badari MS, Elgendy SG, Mohamed AS, Hassan AT. Immunomodulatory effects of levofloxacin on patients with pneumonia in Assiut University Hospitals. Egyptian J Immunol. 2015;22(1).
41. González-Chávez SA, Salas-Leiva JS, Salas-Leiva DE, et al. Levofloxacin induces differential effects in the transcriptome between the gut, peripheral and axial joints in the Spondyloarthritis DBA/1 mice: improvement of intestinal dysbiosis and the overall inflammatory process. PLoS One. 2023;18(2):e0281265. doi:10.1371/journal.pone.0281265
42. Yudhawati R, Wicaksono NF. Immunomodulatory effects of fluoroquinolones in community-acquired pneumonia-associated acute respiratory distress syndrome. Biomedicines. 2024;12(4):761. doi:10.3390/biomedicines12040761
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.