")
Back to Journals » Infection and Drug Resistance » Volume 18
Long-Term Efficacy of Chlorine-Based Disinfectants Vs Multi-Enzymatic Detergent with Hypochlorous Acid for Waterline Disinfection in Inactive Dental Chair Units
Authors Zheng YY, Wang YY, Guo Q, Shen CY, Huang R, Wang L, Sun H
Received 25 December 2024
Accepted for publication 13 May 2025
Published 19 June 2025 Volume 2025:18 Pages 3055—3062
DOI https://doi.org/10.2147/IDR.S514325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Yu-Ying Zheng,1,2,* Yuan-Yuan Wang,1,3,* Qian Guo,1,4 Chan-Yuan Shen,1,5 Rong Huang,1,2 Li Wang,1,6 Huan Sun1,2
1State Key Laboratory of Oral & Maxillofacial Reconstruction and Regeneration, Key Laboratory of Oral Biomedicine Ministry of Education, Hubei Key Laboratory of Stomatology, School & Hospital of Stomatology, Wuhan University, Wuhan, 430079, People’s Republic of China; 2Department of Comprehensive Emergency, School & Hospital of Stomatology, Wuhan University, Wuhan, Hubei Province, 430079, People’s Republic of China; 3Center for Oral and Maxillofacial Surgery, School & hospital of stomatology (Optics Valley Branch), Wuhan University, Wuhan, Hubei Province, 430075, People’s Republic of China; 4Center for Orthodontics and Pediatric Dentistry, School & hospital of stomatology (Optics Valley Branch), Wuhan University, Wuhan, Hubei Province, 430075, People’s Republic of China; 5Department of Center for Emergency and General Dentistry, School & hospital of stomatology (Optics Valley Branch), Wuhan University, Wuhan, Hubei Province, 430075, People’s Republic of China; 6Department of Nursing, School & Hospital of Stomatology, Wuhan University, Wuhan, Hubei Province, 430079, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huan Sun, Department of Comprehensive Emergency, School & Hospital of Stomatology, Wuhan University, No. 237 of Luoyu Road, Hongshan District, Wuhan, 430079, Hubei Province, People’s Republic of China, Tel +86 13986003844, Email [email protected] Li Wang, Department of Nursing Department, School & Hospital of Stomatology, Wuhan University, No. 237 of Luoyu Road, Hongshan District, Wuhan, 430079, Hubei Province, People’s Republic of China, Tel +86 027-87686387, Email [email protected]
Objective: This study aimed to evaluate the long-term efficacy of two disinfection methods for waterline systems in inactive dental chair units (DCUs).
Methods: On-site sampling and quantitative bacterial analysis were conducted to compare the effectiveness of chlorine-based disinfectants and a combination of multi-enzymatic detergent with hypochlorous acid in controlling microbial contamination in waterline systems of inactive DCUs.
Results: No statistically significant differences in disinfection efficacy were observed between the treatment and control groups immediately after disinfection or on the third day post-disinfection (p > 0.05). However, significant differences were observed on the fifth day and seventh day following disinfection (p < 0.001).
Conclusion: Both chlorine-based disinfectants and the combination of multi-enzymatic detergent with hypochlorous acid effectively controlled contamination in waterline systems for DCUs inactive for up to three days. For periods of inactivity exceeding five days, the combination of multi-enzymatic detergent with hypochlorous acid demonstrated superior efficacy by reducing biofilm adhesion over time.
Keywords: chlorine-containing disinfectant, dental chair unit, hypochlorous acid, inactive, multienzyme, waterline disinfection
Introduction
The dental chair unit (DCU) is a complex system integrating water, electrical, and pneumatic pipelines, all essential for supporting various dental procedures. A vital component of the DCU, the dental unit waterline (DUWL), consists of interconnected plastic hoses and metal control valves.1 An inactive DCU refers to a unit temporarily underutilized due to specific circumstances in dental clinics or hospitals, such as limited patient appointments, rapid expansion of practices, altered clinician schedules, or seasonal fluctuations in patient volume. Unlike permanently decommissioned units, inactive DCUs remain operational but unused for a specified duration.
Data from the American Dental Association (ADA) indicate that disparities in patient volume across clinics, as of the third quarter of 2024, have affected DCU utilization. Although some facilities experience overwork, approximately 24% to 28% of dentists have reported insufficient patient volumes, resulting in unused capacity and higher DCU inactivity rates.2 Similar trends are evident in China, where DCU inactivity rates surpass 50% in dental clinics within cities such as Beijing. Despite this underutilization, certification reports from Global Market Intelligence (GMI) highlight continued growth in the DCU market.3 However, the global economic downturn and ongoing supply-demand imbalances are expected to further increase DCU inactivity rates.
The increasing rates of inactivity in DCUs present significant challenges to maintaining disinfection of the waterline systems. Unlike frequently used DCUs, inactive units are more susceptible to management and hygiene issues, particularly within their waterline systems. Reduced or halted water flow promotes microbial growth and biofilm formation in pipelines, thereby elevating the risk of clinical infections.4,5 Existing physical interventions, such as flushing, filtration, and anti-backflow devices, provide moderate improvements in water quality but are ineffective against established biofilms. Both domestic and international guidelines recommend intermittent, regular, or continuous application of chemical disinfectants as an effective strategy to prevent biofilm formation in inactive DUWLs.6 Two methods including conventional chlorine-based disinfectants and a combination of multi-enzymatic detergent and hypochlorous acid disinfectant were used for disinfection. Hypochlorous acid is a weakly acidic and strongly oxidizing disinfectant. In aqueous solution, it dissociates into H+ and OCl−, followed by denaturating and aggregating protein. Hypochlorous acid also destroys the virus by chlorination to form chloramines and nitrogen-centered free radicals, resulting in single-and double-stranded DNA breaks and inactivation of virus. It has strong penetration of biofilm and may effectively clean the surface of implants contaminated by biofilm.7,8 It is widely used in water system disinfection, but its high concentration may cause corrosion of instruments and produce by-products. Multi-enzymatic detergent includes proteases, lipases, and amylases. These enzymes degrade proteins, lipids, polysaccharides and other organic components in biofilms through specific catalytic reactions, disintegrate biofilm structure and enhance the permeability of chemical disinfectants. Hypochlorous acid, a subsequent microbicide, can rapidly inactivate free microorganisms and inhibit biofilm regeneration. The combination of the two can quickly remove biofilms in the pipeline and reduce microbial contamination.9 However, the priority of the two disinfection methods was not determined. The selection of appropriate chemical disinfectant is therefore of critical importance. The comparative efficacy of a combination of multi-enzymatic detergent and hypochlorous acid disinfectant versus conventional chlorine-based disinfectants was evaluated for the disinfection of inactive DUWL. Additionally, the effectiveness of continuous disinfection strategies in controlling waterline contamination was assessed to provide a reference framework for selecting optimal disinfection methods for inactive DUWLs.
Materials and Methods
Materials
Experimental Units
Forty-five inactive DCUs of the same model were selected from a tertiary Class A stomatological hospital in Hubei Province. The units were randomly allocated into either the treatment or control group, with 15 DCUs in each group. Furthermore, the experimental design additionally incorporated a blank control group (15 DCUs) to ensure methodological rigor. Test specimens included independent water storage tanks, three-way spray lances, and water samples collected from the dental handpiece connection tubing.
Main Reagents
- Treatment group: Multi-enzymatic detergent combined with hypochlorous acid disinfectant.
- Control group: Chlorine-containing effervescent tablets.
- Blank control group: No disinfectant or treatment applied.
Methods
Study Protocol
Disinfection procedures were conducted weekly.10 Full-time nurses, trained in hospital infection control protocols, performed waterline disinfection of inactive DCUs every Monday morning prior to the commencement of clinic operations. Samples were collected before disinfection and on the third, fifth, and seventh day post-disinfection, with additional collections performed four times per week. Three sampling sites were established for each dental chair, and continuous sampling was conducted over a one-week period. The total sample size was determined by multiplying the number of dental chairs, sampling sites, and collection time points, resulting in 360 samples. These samples were equally distributed between the treatment and control groups, with 180 samples allocated to each group.
Disinfection methods
- Treatment group: A disinfectant solution was prepared by combining sterile distilled water and multi-enzymatic detergent (the MEDICOM ANIOS Endoscope-Specific Multi-Enzyme Cleaner; A.R.Medicom Inc.Healthcare (shanghai)Limited; Shanghai; China) in a ratio of 1500 mL to 22.5 mL. The enzyme activity unit was ≥ 800 U/mL with protease being 300 U/mL, lipase being 250 U/mL, and amylase being 250 U/mL. Samples were subsequently immersed in isolated water storage tanks for initial disinfection. The water volume was adjusted to maximum capacity, and the foot pedal was activated to ensure thorough filling of all waterlines. The system was left to soak for 30 minutes.11 The tank was drained, and a secondary solution was prepared by mixing sterile distilled water with sodium hypochlorite disinfectant (Bolanconi No-Rinse Hypochlorous Acid Disinfectant; Shanghai SEC JIE Technology Co., LTD; Shanghai; China) in a 1000 mL to 500 mL ratio. The available chlorine concentration was 50 ppm. The same procedural steps were repeated to complete the disinfection process.
- Control group: Chlorine-containing effervescent tablets (Jianzhisu; Beijing Jianzhisu Health Element Disinfection Technology Service Co. LTD; Beijing; China) were dissolved in sterile distilled water to prepare a disinfectant solution with a chlorine concentration of 500 mg/L.12,13 This solution was used to disinfect the isolated water storage tank through immersion. The water volume was subsequently adjusted to maximum capacity, and the foot pedal was activated to ensure all waterlines were completely filled and soaked for 30 minutes. Following the soaking period, the water storage tank and waterlines were thoroughly rinsed with sterile distilled water to eliminate any residual disinfectant.
Water Sample Collection
- Collection from the isolated water storage tank: The DCU power supply was disconnected, and the isolated water bottle was removed. A sterile pipette was used to collect 10 mL of water from the tank.14
- Collection from the three-way spray lance: The water outlet of the three-way spray lance, without the nozzle, was disinfected using 75% ethanol. The water was drained for 30 seconds before 10 mL was collected in a sterile container.14
- Collection from the dental handpiece connection tube: The metal cap was removed from the connection port, ensuring no handpiece was attached. The post was disinfected with 75% ethanol or a sterile water sampler. The water was then drained for 30 seconds, and 10 mL was collected in a sterile container.14
Outcome Measures
Bacterial cultures were quantified using the plate counting method. Water samples or their dilutions were inoculated directly onto solid media, and bacterial colonies were enumerated after incubation. Compliance was determined based on the total bacterial colony count, with a threshold of 500 colony-forming units per milliliter (CFU/mL), as specified by the oral hygiene water standards set by the Centers for Disease Control and Prevention (CDC).15 The logarithmic transformation of the colony count was subsequently calculated to facilitate statistical analysis.
Statistical Methods
The data accuracy was independently verified by two individuals prior to analysis. Statistical analyses were conducted using SPSS version 27.0. The Shapiro–Wilk test was applied to assess the normality of measurement data, with p-values exceeding 0.05, indicating that the data followed a normal distribution. Subsequently, an independent samples t-test and one-way ANOVA analysis were employed for further data evaluation.
Results
Disinfection Efficacy of Inactive DCUs on Day 3 Post-Disinfection
No statistically significant difference in bacterial colony counts was observed between the treatment group and the control group on the third day post-disinfection (p > 0.05), as presented in Table 1. However, the two disinfection procedures demonstrated beneficial effects (both p < 0.001).
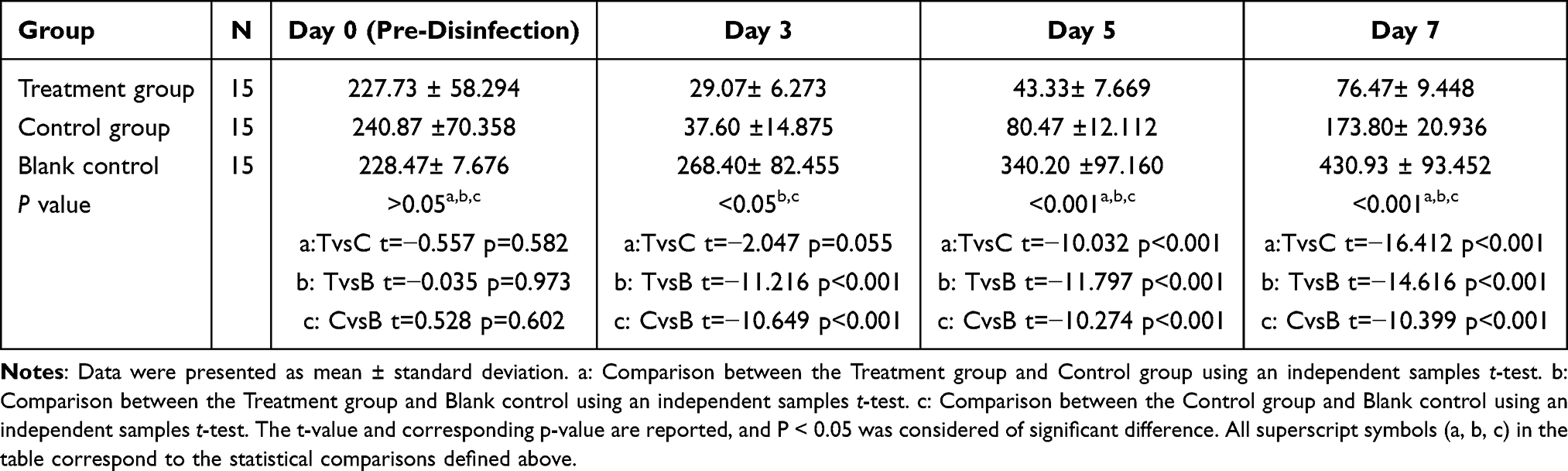 |
Table 1 Bacterial Colony Counts (CFU/mL) Across Groups |
Disinfection Efficacy of Inactive DCUs on Day 5 Post-Disinfection
On the fifth day post-disinfection, the two disinfection procedures also demonstrated beneficial effects (both p < 0.001). In addition, colony counts in the treatment group were significantly lower than those in the control group, with a statistically significant difference observed (p < 0.001), as detailed in Table 1.
Disinfection Efficacy of Inactive DCUs on Day 7 Post-Disinfection
On the seventh day post-disinfection, the bacterial colony counts in the treatment group and the control group were lower than that in the blank group. In addition, the treatment group demonstrated a significantly lower bacterial colony count compared to the control group, with a statistically significant difference (p < 0.001), as presented in Table 1.
Differences in Bacterial Colony Counts Among the Sampling Areas
There were no significant differences among the three sampling areas (the dental handpiece connection tubing, three-way spray lances and independent water storage tanks) within each group at all time points before and after disinfection (P > 0.05), as presented in Tables 2–4.
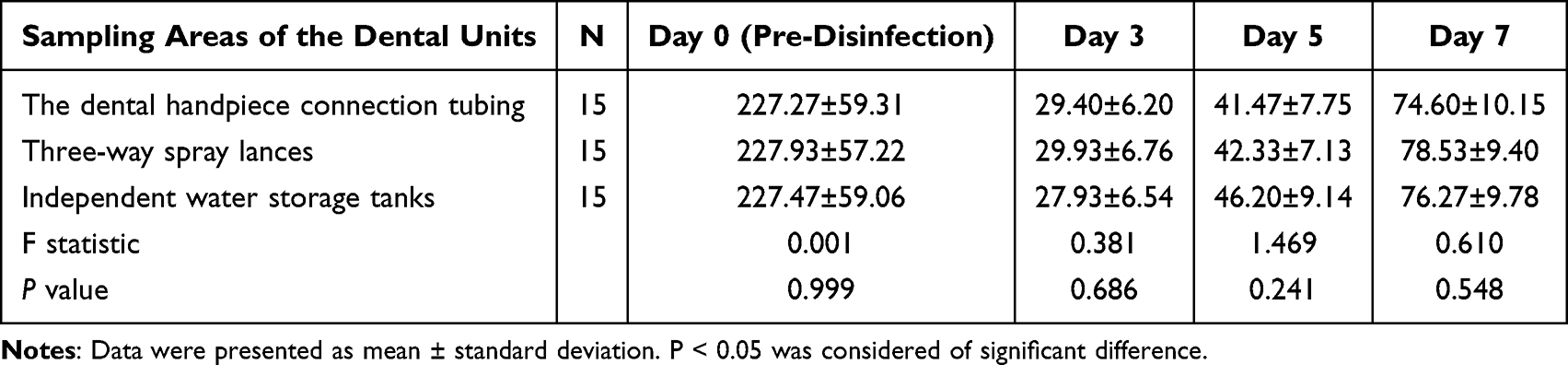 |
Table 2 Bacterial Colony Counts (CFU/mL) in Treatment Group |
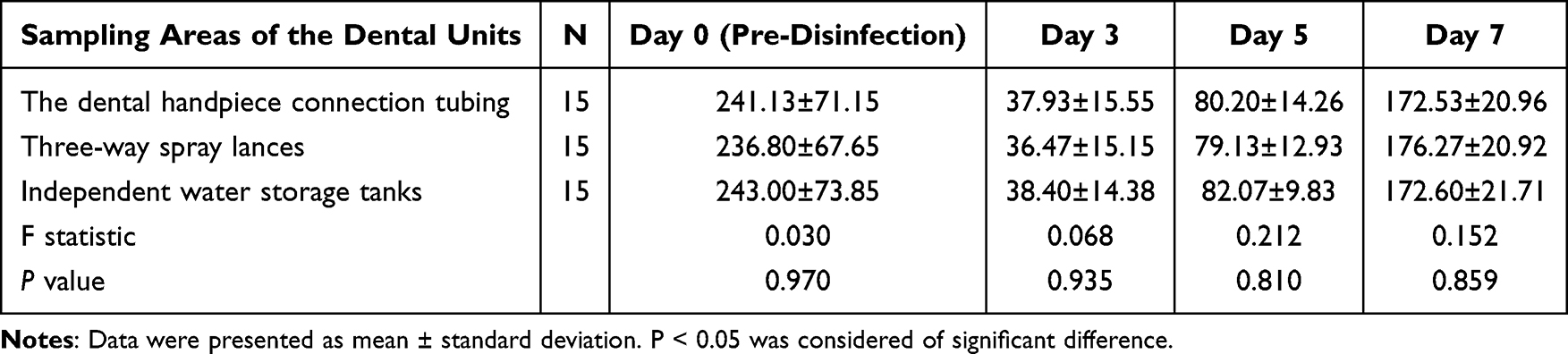 |
Table 3 Bacterial Colony Counts (CFU/mL) in Control Group |
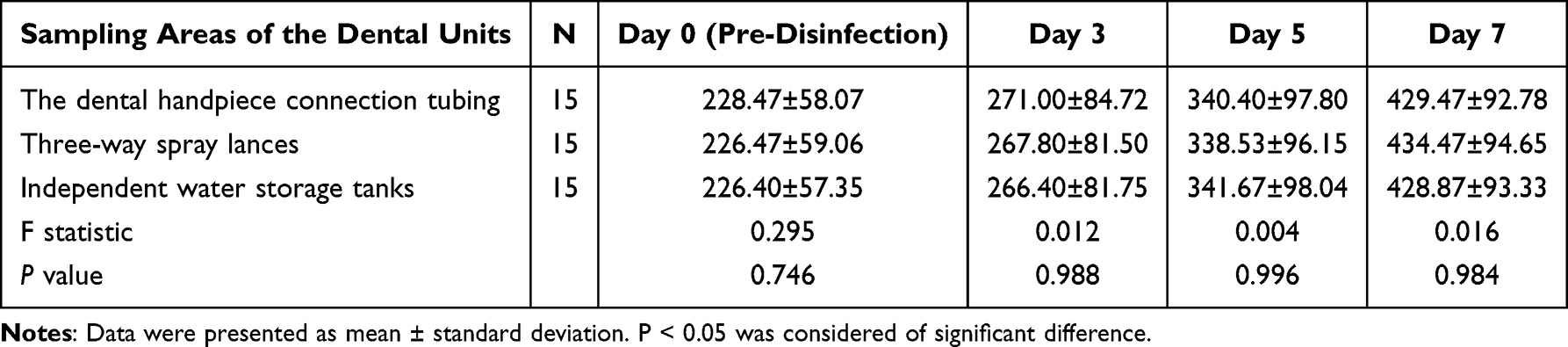 |
Table 4 Bacterial Colony Counts (CFU/mL) in Blank Group |
Discussion
Opportunistic pathogens, such as Legionella and Pseudomonas aeruginosa, are the primary contaminants in inactive DCUs.16–18 As these DCUs are not used by patients, retrograde contamination is an unlikely source; instead, contamination predominantly originates from the DUWLs.19 Without prompt elimination of microorganisms and biofilms, subsequent use of the DCUs can pose a significant infection risk, particularly for individuals with compromised immune systems.20,21 As indicated in Tables 1–3, bacterial counts post-disinfection in both groups consistently remained below 500 CFU/mL, confirming the substantial bactericidal efficacy of both disinfection methods. Notably, the data (as shown in Table 1) indicated no statistically significant differences between disinfection methods for DCUs inactive for up to three days, suggesting that either method is equally effective under such conditions.
As presented in TableS 2 and 3, the treatment group exhibited a statistically significant difference from the control group (p < 0.01). The combined use of multi-enzymatic detergent and hypochlorous acid disinfectant demonstrated superior efficacy and prolonged effectiveness compared to conventional chlorine-based disinfectants, particularly in addressing contamination in inactive DUWLs. This dual approach proved highly effective in mitigating biofilm adhesion, especially in DCUs that had remained inactive for extended periods (5 days or more).
Biofilm accumulation within inactive DUWLs represents a significant infection risk for both dental staff and patients.22 While traditional disinfection protocols can remove biofilms, their frequent application may result in waterline corrosion and a reduction in service life. Pre-treatment with multi-enzymatic detergents effectively degrades the organic components of biofilms, thereby enhancing the subsequent action of chemical disinfectants. Unlike harsher chemical agents, multi-enzyme formulations help preserve the integrity of dental equipment, reduce material corrosion, and are suitable for long-term use.
Hypochlorous acid, a potent broad-spectrum antibacterial agent, has demonstrated significant efficacy against prevalent DUWL pathogens, including Pseudomonas, Legionella, and non-Mycobacterium tuberculosis.23 Its antimicrobial mechanism involves the rapid destruction of microbial cells by disrupting cell membranes and intracellular components. In DUWL systems, hypochlorous acid effectively controls microbial contamination, eliminates biofilms, and maintains water quality within the prescribed safety limits. Its relatively low corrosivity and minimal impact on equipment materials make it well-suited for long-term use, minimizing damage to dental instruments. Clinically, hypochlorous acid is frequently used in conjunction with adjunctive treatments, such as multi-enzymatic detergents, to optimize disinfection outcomes. A sequential approach—where multi-enzymatic detergents first remove organic matter and biofilm, followed by hypochlorous acid for sterilization—has proven to achieve superior microbial control within DUWL systems. This combination also extends the contact time of the disinfectant with the waterlines, thereby improving its efficacy against opportunistic pathogens.9,24,25
A variety of disinfection methods have been developed for DCU waterlines, yet few specifically target inactive DCUs. Effective infection control strategies are essential for mitigating risks associated with the disinfection for inactive equipment.17,26 Effective and long-lasting disinfection strategies are critical to minimize potential hazards during diagnosis and therapeutic procedures. The selection of an optimal method disinfection enables the implementation of systematic protocols specifically tailored to inactive DCUs. These protocols reduce microbial growth within waterline systems, prevent cross-contamination during oral procedures, and maintain high standards of medical service quality. Additionally, efficient disinfection practices ensure that frequency of interventions aligns with varying periods of inactivity, mitigating both the risks of excessive disinfection and bacterial proliferation due to delayed intervention. Adopting appropriate disinfection methods also improves operational efficiency by ensuring that inactive equipment remains hygienically safe for use while extending its lifespan through the prevention of waterline-related contamination and associated malfunctions. Collectively, these measures help reduce operational costs for dental clinics and hospitals while optimizing the use of inactive resources.
The combination of multi-enzyme cleaners and sodium hypochlorite disinfectants offers several advantages over traditional chlorine-based disinfectants. It provides stronger cleaning power by breaking down organic pollutants such as blood, mucus, and grease, while traditional chlorine-based disinfectants mainly rely on oxidation and have weaker cleaning abilities. Additionally, this combination is less corrosive, making it safer for precision instruments and medical devices. It also has less irritating odor and is safer to use, with reduced risk to the respiratory system, skin, and eyes. Furthermore, multi-enzyme cleaners are more environmentally friendly, as they are biodegradable and cause less pollution compared to traditional chlorine-based disinfectants.
The study has some limitations. The study only included 45 DCUs of the same type, and did not cover different brands or old equipment, which might limit the generalizations of the conclusions. The influence of external factors such as water hardness, environmental temperature and humidity on the disinfection effect has not been systematically analyzed, and such variables need to be included in subsequent studies to improve the evaluation system. The experiment used fixed concentration parameters, and the influence of different concentration gradients on disinfection efficacy was not evaluated, which might affect the applicability of the conclusion. The current data are based on the observation of a single disinfection cycle, and the stability of the results of multiple repeated experiments needs to be performed in the further study. This study did not detect and observe the biofilm in the pipeline straightly, which might lead to bias.
Conclusion
For DCUs with shorter periods of inactivity, either chlorine-based disinfectants or the combination of multi-enzymatic detergents and hypochlorous acid can effectively maintain waterline hygiene. However, for DCUs that remain inactive for more than five days, the combination of multi-enzymatic detergent and hypochlorous acid exhibits superior efficacy in preventing biofilm adhesion and ensuring long-lasting disinfection.
Abbreviations
DCU, Dental Chair Unit; DUWL, Dental unit waterline; ADA, American Dental Association; GMI, Global Market Intelligence; CDC, Centers for Disease Control and Prevention.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author Huan Sun.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of The School & Hospital of Stomatology, Wuhan University(Approval number is WDKQ2024B115). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was not appropriate for this research and was waived by the Ethics Committee.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Disclosure
The authors declare that they have no competing interests.
References
1. Shuai T, Shao T, Yi L, et al. The effect of different types of water sources on dental unit waterline contamination: a systematic review and meta analysis. Heliyon. 2024;10(16):e35745. PMID: 39220891; PMCID: PMC11365326. doi:10.1016/j.heliyon.2024.e35745
2. Economic Outlook and Emerging Issues in Dentistry Insights from Data from Q3 2024.American Dental Association.2024.
3. GMI3446. Dental Chair Market - By Product (Ceiling Mounted Chair, Mobile Independent Chair, Dental Chair Mounted Unit), Technology (Powered, Non-powered), By Operation, By Configuration, By Application, By Dental Specialty, By End-use & Forecast, 2024-2032. Global Market Intelligence. 2024.
4. Best practices for dental unit water quality. Centers for Disease Control and Prevention.2024.
5. Samaranayake L, Fakhruddin K, Sobon N, Osathanon T. Dental unit waterlines: disinfection and management. Int Dent J. 2024;74 Suppl 2(Suppl 2):S437–S445. PMID: 39515931; PMCID: PMC11583879. doi:10.1016/j.identj.2024.07.1269
6. Shannon EM, Nuala P. Dental unit water quality: organization for safety, asepsis and prevention white paper and recommendations-2018. J Dental Infection Control Safety. 2018;1(1):1–24.
7. Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78(9):1461–1466. Epub 2020 Jun 25. PMID: 32653307; PMCID: PMC7315945. doi:10.1016/j.joms.2020.06.029
8. Romanowski EG, Stella NA, Yates KA, Brothers KM, Kowalski RP, Shanks RMQ. In vitro evaluation of a hypochlorous acid hygiene solution on established biofilms. Eye Contact Lens. 2018;44 Suppl 2(Suppl 2):S187–S191. PMID: 29369234; PMCID: PMC6046278. doi:10.1097/ICL.0000000000000456
9. Zhang XH, Deng ZH, Luo WJ, et al. Effectiveness and sustainability of multi-enzyme cleaning agents in control of contamination of dental unit waterlines. Chin J Nosocomio. 2023;33(02):295–299.
10. Chang J, Dang Y, Wang C, Li X. Effect of using hydrogen peroxide for periodic disinfection combined with continuous disinfection to control contamination in dental unit waterline. J Sichuan Univ. 2024;55(1):217–223. doi:10.12182/20240160210
11. China Health Supervision Association. Technical Regulation for Cleaning and Disinfection of Dental Unit Waterlines T/WSJD 40-2023; 2023.
12. Pankhurst CL, Coulter WA. Basic guide to infection prevention and control in dentistry (Basic Guide Dentistry Series) second ed. Available from: https://www.nature.com/articles/vital1022. (
13. Yue C, Yuya H, Zhihuan L, Zimo W, Jianying F. Study on the disinfection effect of chlorine dioxide disinfectant (ClO2) on dental unit waterlines and its in vitro safety evaluation. BMC Oral Health. 2024;24(1):648. PMID: 38824549; PMCID: PMC11143753. doi:10.1186/s12903-024-04391-7
14. Chinese Academy of Stomatology. Guidelines for infection control and management in dental unit waterlines T/CHSA 023-2023.2023.
15. Kohn WG, Harte JA, Malvitz DM, Collins AS, Cleveland JL, Eklund KJ; Centers for Disease Control and Prevention. Guidelines for infection control in dental health care settings--2003. J Am Dent Assoc. 2004;135(1):33–47. PMID: 14959873. doi:10.14219/jada.archive.2004.0019
16. Lizon J, Florentin A, Martrette JM, Rivier A, Clement C, Rabaud C. Microbial control of dental unit water: feedback on different disinfection methods experience. Am J Infect Control. 2016;44(2):247–249. Epub 2015 Oct 9. PMID: 26455869. doi:10.1016/j.ajic.2015.08.029
17. Buitrago JM, Kolbe RJ, Siqueira MF. Dental unit waterline testing practices: an 11-year retrospective study. BMC Oral Health. 2023;23(1):867. PMID: 37968643; PMCID: PMC10652605. doi:10.1186/s12903-023-03590-y
18. Chen P, Zeng J, Hong F, Li C, Wang H, Yu X. The importance of biofilm contamination control for dental unit waterlines: a multicenter assessment of the microbiota diversity of biofilm in dental unit waterlines. J Oral Microbiol. 2023;16(1):2299496. PMID: 38174123; PMCID: PMC10763872. doi:10.1080/20002297.2023.2299496
19. Baudet A, Lizon J, Florentin A, É M. Initial waterline contamination by Pseudomonas aeruginosa in newly installed dental chairs. Microbiol Spectr. 2024;12(6):e0396223. Epub 2024 Apr 23. PMID: 38652098; PMCID: PMC11237434. doi:10.1128/spectrum.03962-23
20. Li N, Cai QM, Hu NY, et al. Pyrosequencing analysis of bacterial community changes in dental unit waterlines after chlorogenic acid treatment. Front Cell Infect Microbiol. 2024;14:1303099. PMID: 38299116; PMCID: PMC10828043. doi:10.3389/fcimb.2024.1303099
21. Hamilton KA, Kuppravalli A, Heida A, et al. Legionnaires’ disease in dental offices: quantifying aerosol risks to dental workers and patients. J Occup Environ Hyg. 2021;18(8):378–393. Epub 2021 Aug 2. PMID: 34161202. doi:10.1080/15459624.2021.1939878
22. Xing M, Zhang H, Zhang L, Qian W. Construction of ZnO/PCL antibacterial coating potentially for dental unit waterlines. J Funct Biomater. 2023;14(4):225. PMID: 37103315; PMCID: PMC10144832. doi:10.3390/jfb14040225
23. Patil R, Hindlekar A, Jadhav GR, et al. Comparative evaluation of effect of sodium hypochlorite and chlorhexidine in dental unit waterline on aerosolized bacteria generated during dental treatment. BMC Oral Health. 2023;23(1):865. PMID: 37964280; PMCID: PMC10647182. doi:10.1186/s12903-023-03585-9
24. Marino F, Mazzotta M, Pascale MR, Derelitto C, Girolamini L, Cristino S. First water safety plan approach applied to a Dental Clinic complex: identification of new risk factors associated with Legionella and P. aeruginosa contamination, using a novel sampling, maintenance and management program. J Oral Microbiol. 2023;15(1):2223477. PMID: 37346998; PMCID: PMC10281406. doi:10.1080/20002297.2023.2223477
25. Zhu C, Hong FH, Yu X. Anti biofilm effect of low concentration chlorine containing disinfectant assisted by multi enzyme detergent in dental unit waterlines. New Microbiol. 2021;44(2):117–124. Epub 2021 May 1. PMID: 33978196.
26. Vinh R, Azzolin KA, Stream SE, et al. Dental unit waterline infection control practice and knowledge gaps. J Am Dent Assoc. 2024;155(6):515–525.e1. PMID: 38839239. doi:10.1016/j.adaj.2024.02.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.