")
Back to Journals » Infection and Drug Resistance » Volume 18
Lymphadenopathies: A Retrospective Study of Epidemiology, Characteristics, Diagnosis and Treatment Outcomes of Patients in a Tertiary Hospital in Mogadishu-Somalia
Authors Kıratlı K , Bulut M , Ali MA , Aysin M , Ali AM, Mohamed Hirsi I, Bashir AM
Received 17 September 2024
Accepted for publication 25 January 2025
Published 30 January 2025 Volume 2025:18 Pages 557—566
DOI https://doi.org/10.2147/IDR.S488617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kazım Kıratlı,1 Muhammet Bulut,2 Mukhtar Abdullahi Ali,1 Murat Aysin,3 Ahmed Mohamed Ali,1 Ibrahim Mohamed Hirsi,4 Ahmed Muhammad Bashir5
1Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, Mogadishu, Somalia; 2Sancaktepe Şehit Prof. Dr. Ilhan Varank Training and Research Hospital, Department of Radiology, Istanbul, Turkey; 3Balikesir University Faculty of Medicine, Department of Public Health, Balikesir, Turkey; 4Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Department of Pediatrics, Mogadishu, Somalia; 5Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Department of Internal Medicine, Mogadishu, Somalia
Correspondence: Kazım Kıratlı, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, Mogadishu, Somalia, Email [email protected]
Introduction: Lymphadenopathies, which can be caused by infections, malignant diseases, autoimmune disorders, and many other diseases, pose a challenge to clinicians in sub-Saharan Africa, as well as all over the world. The purpose of this research was to identify the clinical and diagnostic characteristics of Somalian patients suffering from swollen lymph nodes.
Methods: Under the purview of this study, the diagnoses, patient clinical courses, and treatment outcomes were ascertained retrospectively by analyzing the biochemical, microbiological, radiological, and pathological data of the cases in all age groups who underwent therapy for lymphadenitis at Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital between January 2016 and September 2023.
Results: During the study period, 317 patients were followed up, with 53.3% of the patients as female, 46.7% as male, 28.1% as pediatric, 63.1% as adult, and 8.8% were elderly patients. With 58.7% of diagnoses, tuberculous lymphadenitis was the most common, pursued by malignant causes (21.8%). The most commonly affected lymph node was the cervical region, the symptom detected was lymph node swelling, the radiological method used was ultrasonography, and the biopsy method was fine needle aspiration biopsy. It was determined that benign conditions, including tuberculosis were more common in pediatric group and younger adults (p< 0.001), and weight loss was a significant in terms of malignancy and tuberculosis (p< 0.001). White blood cell value (p< 0.001), erythrocyte sedimentation rate (p< 0.001), and C-reactive protein (p:0.001) revealed differences across the diagnostic groups.
Conclusion: Almost two-thirds of patients were diagnosed with tuberculosis lymphadenitis. Our finding revealed tuberculosis as the commonest cause of lymphadenopathy followed by malignant causes. Therefore, before screening for malignant causes, tuberculosis should be the first diagnosis considered in Somalia, particularly in a patient presenting with weight loss and swelling of the lymph nodes.
Keywords: immunization, lymphadenopathy, Somalia, sub-Saharan Africa, tuberculosis
Introduction
Lymphadenopathy (LAP) is the term used to describe the invasion of lymph nodes by different cells (cancer or inflammatory cells) and their multiplication there, which causes the lymph nodes to enlarge (>1 cm) and/or lose their consistency. On physical examination, nodules greater than 5 mm that are palpable in the popliteal, iliac, supraclavicular, or epitrochlear regions should be regarded as abnormal. A pathologic condition is suggested by hard, matted lymph nodes. Between the ages of two and ten, children’s lymph nodes are marginally more noticeable than those of adults.1–3 A number of factors, such as infections, autoimmune disorders, malignancies, and various other diseases, can cause these swelling of lymph nodes.4 The majority of pediatric LAP cases are benign or infectious, and nearly half of them involve healthy individuals. A comprehensive and healthy medical history is necessary to determine the etiology.5
Moreover, in order to provide appropriate treatment for LAP, it is imperative to have a comprehensive understanding of the underlying causes and associated clinical traits.6 The clinical manifestations of specific diseases, such as Kikuchi-Fujimoto disease, are distinguished by the presence of fever and painful swelling of the lymph nodes in the neck. It is crucial to identify these characteristics in order to make an accurate diagnosis and provide appropriate treatment.7
It is also crucial to comprehend the local epidemiology and illness patterns because the incidence and causes of LAP fluctuate among demographics and geographic areas.8 To top it all off, tuberculosis (TB) is still a huge problem, especially in high-risk regions; adequate management is essential, its clinical and pathological characteristics must be thoroughly evaluated.9,10 LAP has recently become more difficult to diagnose and treat due to the COVID-19 pandemic. One new complication is axillary LAP, which can develop after a COVID-19 vaccination and needs to be carefully distinguished from other, potentially cancerous reasons.11
Clinical signs of the illness may be limited to the patient’s LAP, which might be localized, regional, or extensive. The patient may experience pain, fever, a wide range of symptoms from pressure on the nearby organs, or abnormalities in several laboratory parameters. Cervical, supraclavicular, axillary, inguinal, femoral, or popliteal peripheral LAPs are readily identified by physical examination, and a biopsy is conducted to collect a sample. However, to identify and sample deep visceral LAP, advanced imaging techniques and surgical procedures (such as laparotomies) are required.1,12
The diagnostic evaluation of LAP encompasses a range of techniques, such as fine-needle aspiration biopsy (FNAB) and histological examinations, which are crucial for determining the root causes.13,14 For palpably located or challenging-to-reach deep lesions, FNAB is the primary procedure of choice. Preoperative diagnostics, clinical follow-up, decreased risk of tissue injury and infection, and increased patient comfort are just a few benefits. It is also recommended for the thyroid gland, large salivary glands, and other neoplastic lesions in the head and neck area in addition to lymph nodes. It is highly sensitive and specific in diagnosing cervical lymphadenitis associated with TB, and it is reasonably priced. One drawback would be the challenge of identifying small, relatively mobile masses.15,16
LAPs pose a diagnostic challenge in Somalia. There is a dearth of cytological data and research on the topic from other sub-Saharan African (SSA) nations, like Somalia. The purpose of this study was to characterize the prevalence of LAPs in Somalia’s pediatric and adult populations, as well as their location, clinical and laboratory characteristics, age and gender distribution, and diagnostic features.
Materials and Methods
Setting and Study Population
This retrospective study was conducted at Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital. This hospital is one of the largest medical institutions providing healthcare in the entire SSA. Within the scope of the study, the medical records, biochemical, microbiological, radiological and pathological data in the hospital automation registration system of the cases who were followed up or consulted with the diagnosis of LAP (and other additional symptoms) in the Infectious Diseases and Clinical Microbiology Polyclinic/Clinic and the Radiology Polyclinic/Clinic between January 2016 and September 2023 were examined.
Case Definitions
For this study, we classified cases as “pediatric, adult, and geriatric” in addition to gender. Another main backbone of the study was the region where lymph node pathology was observed and the pathological findings. Region classification was made as “cervical, axillary, inguinal, intrabdominal, supraclavicular, subclavicular, submandibular/submental, mediastinal and others”. Radiological methods and biopsy procedures used in diagnosis were also examined within the framework of the study.
Data Collection
Demographic and Clinical Data
The patients’ symptoms (fever, weight loss, night sweats, etc), LAP-related hospitalization history and duration, disease course, treatment received (antibiotic, antiTB drugs, chemotherapy, etc), and treatment duration were also evaluated. We also analyzed the diagnoses of the patients in three main groups as TB lymphadenitis, malignancy and the others (bacterial LAP, chronic nonspecific LAP, other infections, autoimmune diseases and unknown etiology).
Laboratory Investigations
Complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), HbsAg, AntiHCV, AntiHIV and Syphilis antibody results were recorded. Since there were patients who underwent biopsy in our study, patients presenting with LAP due to HIV infection were not included in the study.
Imaging Findings and Invasive Investigations
Radiological methods (ultrasonography, computed tomography, etc) used for diagnostic purposes were examined one by one and recorded. Additionally, the techniques used for lymph node biopsy (fine needle aspiration biopsy, excisional biopsy, etc) were also reviewed and added to the data set.
Statistical Analysis
The characteristics of the patients were presented with descriptive statistics. Categorical data were presented as numbers and percentages. Continuous variables were evaluated with the Kolmogorov–Smirnov test and histogram in terms of normal distribution assumption. Continuous variables were presented as median (minimum-maximum) values. We tested the factors between disease groups in univariate analyses. Chi square test was used in the analysis of categorical variables. Kruskal Wallis and Mann Whitney U-tests were used in the analysis of continuous variables, and p<0.05 was considered statistically significant. All analyzes were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp. Armonk, NY: USA. Release Date 2017).
Ethical Approval
This retrospective study was approved by the Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital Ethics Committee (07.09.2023-MSTH/15313-832). Since the study was retrospective in nature, a waiver of informed consent was granted by the ethics committee and it was not deemed necessary to obtain participant consent. Furthermore, the “Ethical Principles of the World Medical Association Declaration of Helsinki” were taken into consideration when conducting the research.
Results
An analysis was conducted on the data of 317 individuals who were diagnosed with LAP and followed up or consulted between January 2016 and September 2023. The patients ranged in age from 1 to 90 years old, with a 25-year-old median. Among the patients, 169 (53.3%) were female and 148 (46.7%) were male. The rates were reported to be 28.1% (n:89), 63.1% (n:200), and 8.8% (n:28), respectively, when we categorized the patients as pediatric (0–18 years), adult (18–65 years), and geriatric (>65 years). A total of 83 patients (28.2%) were admitted to the hospital for LAP therapy and diagnostic procedures, with an average stay of 5 days (min-max: 2–29 days).
Table 1 lists the percentages of body parts for which LAP was found, the range of symptoms that led to hospital admissions, and the diagnoses that were given to the patients. TB was the most common diagnosis (n:186, 58.7%), followed by all malignant diagnoses (n:69, 21.8%), including primary lymph node cancers and metastatic cases. Bacterial LAP, non-bacterial infectious LAP, autoimmune diseases, chronic non-specific LAP, and undiagnosed conditions are included in the group of other diagnoses (n:62, 19.5% in total). One carcinoid tumor, one glomus tumor, one malignant melanoma, and one spindle cell mesenchymal neoplasm were found under the four detected “others headings” in Table 1, which lists metastatic cancer types of known origin according to the organs.
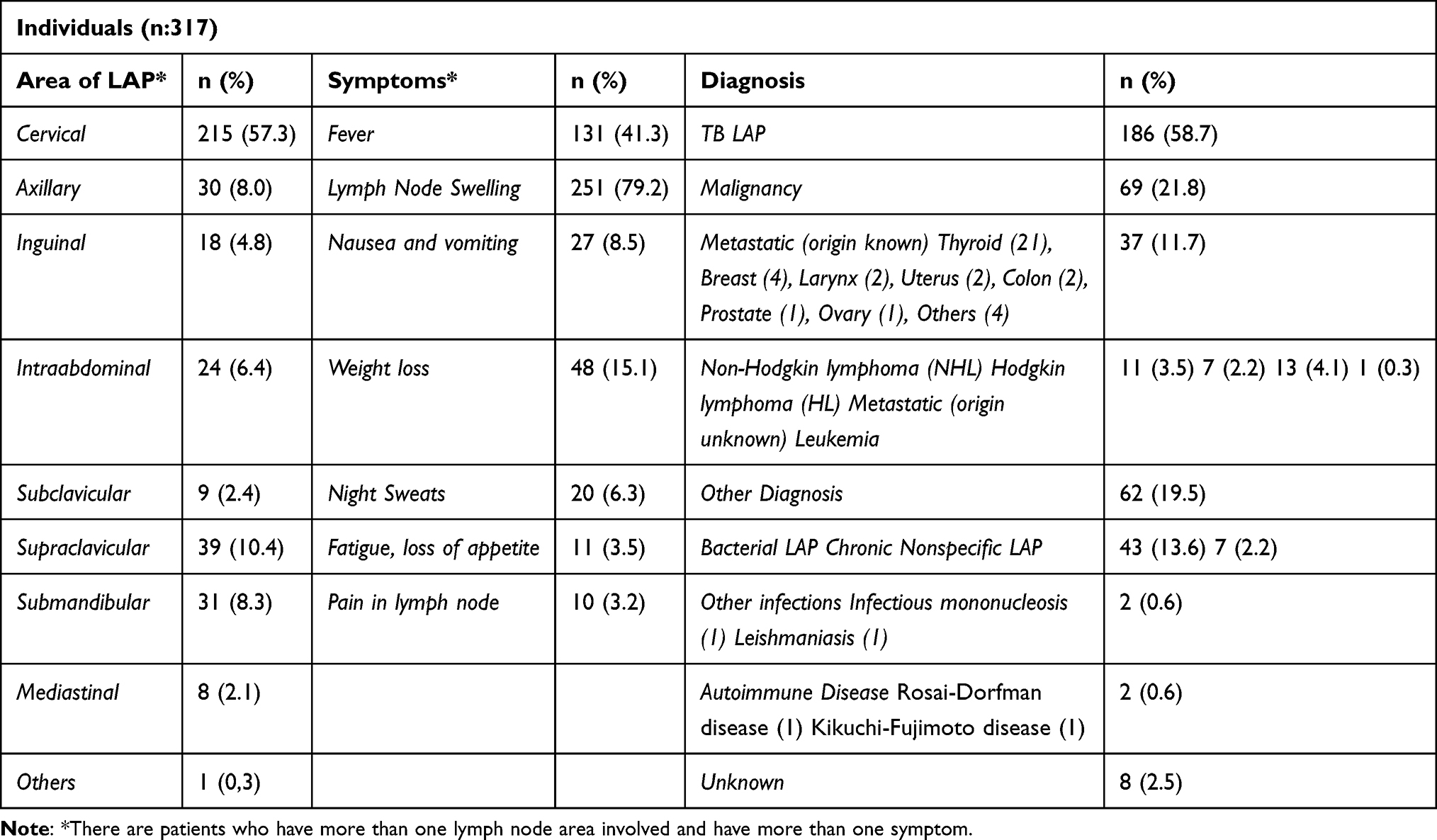 |
Table 1 Localization of the LAP, Symptoms and Diagnosis of Individuals |
Examining the biopsy techniques used for diagnostic purposes, we found that FNAB was used the most often (n:188, 59.3%). Among the other techniques, 34.4% (n:109) of cases involved excisional biopsy, while 6.3% (n:20) involved tru-cut biopsy. The frequencies of radiological techniques utilized for patient treatment, as well as treatment outcomes, are listed in Table 2. Six cases of HBV infection, one case of HCV infection, and one case of syphilis infection were found in this investigation (2.5% in total), which excluded patients with HIV.
 |
Table 2 Radiologic Method, Disease Course and Treatment |
Table 3 presents the distribution of gender, hospitalization and recovery status, lymph node localization (most common: cervical, supraclavicular and submandibular), and symptoms (most common: lymph node swelling, fever and weight loss). Furthermore, Table 4 presents the study of the biochemical (CBC, CRP, and ESR) and age-related and treatment duration-related differences among the three groups that we diagnostically differentiated.
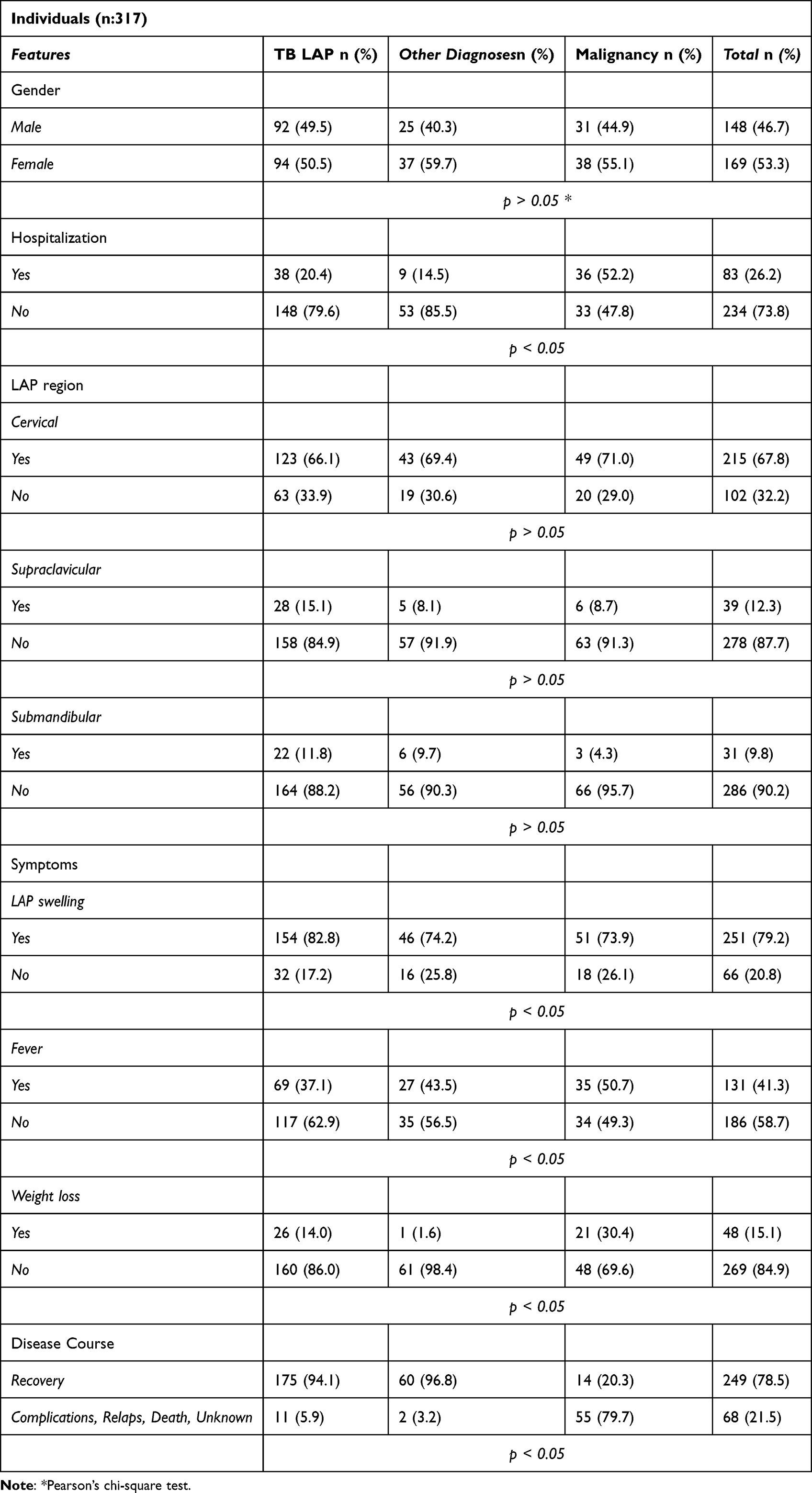 |
Table 3 Characteristics of Gender, Hospitalization, Area of Lymph Node Involvement, Symptoms and Disease Course According to Groups |
 |
Table 4 Distribution of Age, Treatment Duration and Laboratory Findings According to Groups |
Discussion
Somalia is among the world’s most challenging, least developed, and lowest-income per capita nations as a result of a civil war that has lasted for almost quarter of a century. Significant migratory movements have taken place as a result of the situation getting worse in recent years owing to hunger, severe drought, and floods, in addition to the war and violence in the southern and central areas. In terms of mother mortality and child death rates under five, it also tops the globe. Infectious diseases are the most frequent cause of these fatalities.17
In our study, 58.1% of LAP cases had TB, 21.8% had malignant LAP, and 19.5% had other benign reasons apart from these two diagnostic categories. With a prevalence of 57.3%, the cervical region lymph nodes are the most commonly affected location. The three most commonly observed LAP localization sites (p>0.05)—cervical, supraclavicular, and submandibular—did not differ significantly from one another according to differential diagnosis. Moreover, no statistically significant gender-related association was seen between the groups (p>0.05).
TB, which largely affected the cervical region and accounted for 123 cases of LAP in our study, was the most common cause of the condition. The other most prevalent places in the research group, the supraclavicular and submandibular areas, were the sites where TB LAP was most commonly detected (28 and 22 cases, respectively). Furthermore, it was discovered that the mean ages of the groups with benign lesions and TB LAP were 23 and 22.5, respectively, whereas the group with malignant LAP had an average age of 46 (p: <0.001). These viewpoints suggest that, in the case of Somalian children and young adults with neck masses, TB LAP should be the initial diagnosis.
Fever, weight loss, and enlargement of the lymph nodes were the most frequent causes of hospital admission (79.2%, 41.3%, and 15.1%, respectively). Of these symptoms, weight loss showed a statistically significant difference between the groups (p<0.001). TB may be the first thing that comes to mind in the preliminary diagnosis of a patient who is investigated for the etiology of LAP after cancer has been ruled out and who describes weight loss.
For physicians, LAP may provide an etiological dilemma. A patient’s medical history, symptoms, physical examination, lymph node anatomy, swelling size and duration, laboratory results, and radiographic results can all provide information on whether or not their LAP is malignant. It can manifest in many different ways, ranging from benign infections in youth to cancers that are more prevalent in the elderly. Additionally, epidemiological differences by geography may be observable (for instance, TB-related cervical lymphadenitis is quite prevalent in several African nations).18,19
Neoplastic or chronic granulomatous processes are likely to be the source of LAP that lasts longer than six weeks. Thus, early differentiation between benign and malignant causes is advantageous for patient care.20 Tissue diagnosis is considered the gold standard for assessing LAP. Histopathological analysis and microbiological diagnosis (using techniques like culture, PCR, etc.) are provided via biopsy. Some of the signs that a biopsy is necessary include being older than 40, having supraclavicular lymph node enlargement, having a node diameter larger than 2.25 cm, having hard, firm tissue, and not experiencing any pain. Fever, night sweats, and an unexplained weight loss of more than 10% of body weight over a six-month period are indicative of either TB or HL or NHL.1
In comparison to lower body locations like inguinal, femoral, or popliteal lymph nodes, upper body sites like cervical, supraclavicular, and axillary lymph nodes had a higher chance of producing a conclusive diagnosis. The presence of nonspecific reactive or chronic inflammatory and fibrotic alterations was more common in pathology from lower sites.20 As it is a rapid, precise, minimally invasive, and safe method of patient evaluation and assistance in the triage of unexplained lymphadenopathy, FNAB cytology is typically chosen first.3
In a Deosthali et al6 comprehensive study of pediatric patients with cervical lymphadenitis, the majority of the 2687 individuals (two-thirds) had a benign etiology. Of the patients, 4.7% had cancer, with NHL making up the majority (46.0%), and 4.06% had granulomatous illness, with TB constituting up the majority (73.4%). In a research looking at adult patients with LAP in Nigeria, NHL and HL was found in half of the 190 patients between the ages of 18 and 94 (NHL: 31.6%, HL: 18.4%). Metastatic LAPs (20%), reactive lymphadenitis (15.3%) and TB lymphadenitis (9.5%) have been documented as the other etiological reasons.20
In another study conducted in Pakistan, the results of FNABs used to diagnose lymphadenitis were examined. It was found that patients under the age of 15 had reactive adenoid hyperplasia, older patients over 50 had metastatic carcinomas, and middle-aged patients (16–35 years old) had the highest number of cases of TB lymphadenitis across all age groups. Regarding the lesion location, cervical LAPs were more likely to be associated with TB lymphadenitis, whereas axillary and inguinal LAPs were more likely to exhibit metastatic etiology.21
Though most commonly associated with lung illness, TB may infect nearly every tissue in the body. The lymph nodes are the most frequently impacted organ in TB infections, with extrapulmonary involvement occurring in 15–20% of cases. A unilateral or bilateral, hard, non-tender lymph node that is typically linked to the underlying tissue and may appear with fever and other systemic symptoms is the hallmark of TB lymphadenitis, a condition that affects people of all ages, but is more common in those over five. Whereas 28–71% of patients exhibit abnormal chest radiographs, patients frequently have a history of tuberculosis exposure.22–24
In a Chinese series of 255 cases of lymphadenopathy, 204 people (80%) had TB lymphadenitis. In the remaining cases, metastases, lymphoma, and reactive lymphadenitis were discovered. The most prevalent symptom of peripheral lymphadenopathy was palpable swelling (100%), which was followed by loss of appetite (32.4%). The male/female ratio was determined to be 1:1.43. The most frequent site of peripheral TB LAP was the cervical region (92.6%). Just 14.7% of patients had a chest X-ray that showed signs of tuberculosis.9
Countries have different rates of TB, with an average of 130 cases per 100,000 people worldwide. SSA is home to 12% of the world’s population, yet it bears 29% of the TB burden.25,26 In Somalia, an SSA nation, TB is a major public health concern. Less than half of the 300 cases per 100,000 that were projected to be its incidence as of 2011 were actually discovered.27 A research handed out in Nigeria discovered that the most prevalent cause of cervical LAP among those under 45 was TB (35%).28
Lymph nodes are the sites of greatest metastatic accumulation in malignancies, and lymphadenitis may be the initial symptom. Beyond basic lymphohematogenous cancer forms, such as NHL and HL, lymph nodes can also harbor metastases from any other type of neoplasm.29
TB and HL may share some common laboratory, clinical and radiological features. A delayed or incorrect diagnosis might result from these circumstances. As a result, before beginning needless TB therapy, the diagnosis must be confirmed.30 In African nations, children with HL at all stages who are treated with CT alone have a poorer overall survival rate. Mortality and morbidity rates are negatively impacted by a number of infectious disorders, including Epstein-Barr virus, Herpes virus, HIV infection, and malaria, which co-occur often.31
Of the participants in our study with primary lymph node malignancies, 11 (3.5%) had NHL and 7 (2.2%) had HL. One patient was diagnosed with leukemia, whereas 37 patients (11.7%) with known origins and 13 patients (4.1%) with unknown origins received a diagnosis of metastatic LAP. In comparison to the TB LAP and other diagnosis groups, the hospitalization rate of the malignancy group was greater and statistically significant (p<0.001). As previously stated, in those who have lost weight, it ought to be one of the first diagnoses that come to mind, along with TB. It is statistically significant (p<0.001) that the malignancy group’s low recovery rate of 20.3% is attributable to major gaps and deficiencies in Somalia’s cancer treatment capacity. It is possible to identify malignancies with a primary location in a distinct region in the lymph node where the initial stage of metastasis occurred, as demonstrated by the 37 metastatic LAPs in the study that had a known primary.
In addition, several disorders such as Kikuchi-Fujimoto disease and Kawasaki disease have unique clinical characteristics. Male patients with Kikuchi-Fujimoto illness display a different profile marked by a greater occurrence of fever, headache, and bilateral LAP. Additionally, there is a presence of thrombocytopenia and increased liver enzymes, CRP and lactate dehydrogenase.32 Patients with Kawasaki illness who primarily exhibit cervical LAP are at a high risk of being misdiagnosed. This highlights the importance of using precise diagnostic procedures to avoid delays in effective treatment and the occurrence of sequelae.33
One individual with Rosai-Dorfman disease and one with Kikuchi-Fujimoto disease were identified among the 317 cases. Though uncommon, it is important to remember that these disorders might occur, and to stress again how beneficial a pathology diagnosis will be in this situation. Apart from the typical bacterial etiology of LAP, other causes like viruses, fungi, or parasites can also lead to LAP. Among non-bacterial infectious causes, infectious mononucleosis and leishmaniasis were identified in two cases each based on LAP pathology and supported by advanced biochemical and microbiological diagnostic techniques.
Anti-TB treatment was evidently the longest-lasting type of treatment when analyzed in terms of treatment duration (p<0.001). Upon analyzing the data concerning laboratory results, we discovered that the ESR values were highest in the TB group and second in the malignancy group, respectively. These findings demonstrated a statistically significant difference between the three groups (p <0.001). The study revealed that the group with malignancy had a lower CRP value (p:0.001), the group with “Other diagnosis” had a higher WBC value (p<0.001), and the group with TB had higher PLT values (p:0.009). The groups’ HGB levels did not significantly differ from one another (p>0.05).
The cervical and axillary regions were the most commonly affected in an Indian study examining the efficacy of FNAB. TB (44.02%) was shown to be the most common cause, followed by reactive lymphadenitis (42.64%) and metastatic lesions (9.5%). It was highlighted as a consequence of the study that FNAB is a simple, inexpensive, repeatable, dependable, reasonably quick, and painless procedure.34 According to a different study, children with peripheral LAP can benefit from FNAB application under standard clinical settings, with a 95% accuracy rate for diagnosis.35 It has been noted that the FNAB’s accuracy in determining the lymphoma subtype ranges from 38% to 88.8%.36
USG, which is inexpensive, accessible, yields data relatively quickly, and may be utilized as a biopsy auxiliary method, was the most commonly employed radiological modality in our study (78.5%). FNAB, which offers characteristics and application ease comparable to USG, was the most popular biopsy type (59.3%). Given that malignancy rates will be higher in nations with low TB rates, it can now be concluded that FNAB may not be adequate.
The high diagnostic ability of FNAB thus provides earlier reactions for TB lymphadenitis with minimal side effects and rapid evaluation support, in addition to clinical, laboratory, and radiological findings, in underdeveloped countries with high TB incidence where advanced medical tests are not available.
Limitations
The retrospective character of this study is one of its major limitations. The possibility of information bias resulting from data extraction from a single registry, the potential for missing information, and the potential exclusion of some cases of lymphadenopathy are further limitations. In particular, the diagnosis of TB patients is based on clinical, laboratory, radiographic, and cytological results because advanced microbiological techniques are not available in Somalia. Studies on a particular area (specifically the head and neck region) or age group are frequently carried out in the literature. The fact that our study covers all age groups and all body parts can be considered a strength of our research. In this regard, the data shows more accurate outcomes. Taking all of these factors into account, we believe that this study—which is the most thorough on LAP in Somalia across all age groups—will provide insight for further research.
Conclusion
Due to the lack of adequate healthcare resources, the high frequency of infectious illnesses, and their concomitant existence, diagnosing, treating, and managing LAPs present unique challenges in Somalia. In this context, definitive diagnostic approaches that consider distinct clinical aspects, contemporary technologies, and the elimination of obstacles to healthcare access are critical for the proper management of LAPs. Different patterns of LAP can be partially attributed to infectious diseases and site-specific environmental variables. SSA’s healthcare system will benefit from more thorough research involving larger patient populations.
Children and young adults had significantly greater prevalence of TB and benign etiology. People in nations where TB is highly prevalent are typically exposed to higher levels of exposure and get the disease at younger ages. This is supported by the observation that cervical TB LAP is more common in young individuals due to TB LAP’s status as an early postprimary consequence. Our research provides evidence that Somalian youth and children are at risk for TB. The high prevalence of TB lymphadenitis highlights the continued inadequacy of immunization efforts in developing nations and the urgency of accelerating effort into this area.
Acknowledgment
The abstract of this paper was presented at the 12th Turkey EKMUD Scientific Congress as a poster presentation with interim findings (Susesi Hotel, Belek-Antalya, Turkey, 18-22 May 2024). The poster’s abstract was published in “Poster Abstracts” in Mediterr J Infect Microb Antimicrob 2024; 13:Supplement 1:73-74. https://d2v96fxpocvxx.cloudfront.net/new/d363ec1e-9e5e-4591-a00a-d656bfcabb80/articles/ee511b9e-710b-4dcd-8c91-78f287f2e6ad/2024-poster- sunumlar.pdf.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Ali M, Elhatw A, Hegazy M, et al. The evaluation of lymphadenopathy in a resource-limited setting. Cureus. 2022;14(10):e30623. doi:10.7759/cureus.30623
2. Chang SSY, Xiong M, How CH, Lee DM. An approach to cervical lymphadenopathy in children. Singapore Med J. 2020;61(11):569–577. doi:10.11622/smedj.2020151
3. Gaddey HL, Riegel AM. Unexplained lymphadenopathy: evaluation and differential diagnosis. Am Fam Physician. 2016;94(11):896–903.
4. Patel K. A clinical study of tuberculous cervical lymphadenopathy: surgeon’s perspectives. Int Surg J. 2019;6(2):581–585. doi:10.18203/2349-2902.isj20190407
5. King D, Ramachandra J, Yeomanson D. Lymphadenopathy in children: refer or reassure?. Arch Dis Child Educ Pract Ed. 2014;99:101–110. doi:10.1136/archdischild-2013-304443
6. Deosthali A, Donches K, DelVecchio M, Aronoff S. Etiologies of pediatric cervical lymphadenopathy: a systematic review of 2687 subjects. Glob Pediatr Health. 2019;6:2333794X19865440. doi:10.1177/2333794X19865440
7. Alsolami A, Altirkistani R, Tayeb S, et al. A case of recurrent cervical lymphadenopathy due to Kikuchi-Fujimoto disease. Am J Case Rep. 2021;22:e928760. doi:10.12659/AJCR.928760
8. Ng SC, Bernstein CN, Vatn MH, et al. Epidemiology and natural history task force of the International Organization of Inflammatory Bowel Disease (IOIBD). geographical variability and environmental risk factors in inflammatory bowel disease. Gut. 2013;62(4):630–649. doi:10.1136/gutjnl-2012-303661
9. Singh SK, Tiwari KK. Tuberculous lymphadenopathy: experience from the referral center of Northern India. Niger Med J. 2016;57(2):134–138. doi:10.4103/0300-1652.182077
10. Kim JB, Lee SS, Kim SH, et al. Peripancreatic tuberculous lymphadenopathy masquerading as pancreatic malignancy: a single-center experience. J Gastroenterol Hepatol. 2014;29(2):409–416. doi:10.1111/jgh.12410
11. Lim J, Lee SA, Khil EK, Byeon SJ, Kang HJ, Choi JA. COVID-19 vaccine-related axillary lymphadenopathy in breast cancer patients: case series with a review of literature. Semin Oncol. 2021;48(4–6):283–291. doi:10.1053/j.seminoncol.2021.10.002
12. Mohseni S, Shojaiefard A, Khorgami Z, Alinejad S, Ghorbani A, Ghafouri A. Peripheral lymphadenopathy:Approach and diagnostic tools. Iran J Med Sci. 2014;39(2 Suppl):158–170.
13. Andhika D, Handayati A, Woelansari ED. Diagnostic test fine needle aspiration biopsy (FNAB) examination on gold standard histopathological tests for identification of colli lymphadenopathy patients at RSPAL Dr ramelan surabaya. Int J Adv Health Sc Tech. 2023;3.
14. Zada B, Durrani S, Billah M, Iqbal J, Khan A, Nadeem M. Evaluation of treatment efficacy of surgical interventions for tubercular cervical lymphadenopathy. Pak J Med Health Sci. 2022;16(10):752–754. doi:10.53350/pjmhs221610752
15. Santos AP, Sugaya NN, Pinto Junior Ddos S, Lemos Junior CA. Fine needle aspiration biopsy in the oral cavity and head and neck region. Braz Oral Res. 2011;25(2):186–191. doi:10.1590/S1806-83242011000200015
16. Bayazit YA, Bayazit N, Namiduru M. Mycobacterial cervical lymphadenitis. ORL J Otorhinolaryngol Relat Spec. 2004;66(5):275–280. doi:10.1159/000081125
17. Sindani I, Fitzpatrick C, Falzon D, et al. Multidrug-resistant tuberculosis, Somalia, 2010–2011. Emerg Infect Dis. 2013;19:478–480. doi:10.3201/eid1903.121287
18. Wilczynski A, Görg C, Timmesfeld N, et al. Value and diagnostic accuracy of ultrasound-guided full core needle biopsy in the diagnosis of lymphadenopathy: a retrospective evaluation of 793 cases. J Ultrasound Med. 2020;39(3):559–567. doi:10.1002/jum.15134
19. Ochicha O, Edino ST, Mohammed AZ, Umar AB, Atanda AT. Pathology of peripheral lymph node biopsies in Kane, Northern Nigeria. Ann Afr Med. 2007;6(3):104–108. doi:10.4103/1596-3519.55725
20. Ugwu NI, Iyare FE, Ugwu CN, et al. Lymphoma and other lymph node pathologies among adult patients with lymphadenopathy in Abakaliki, Nigeria. Niger J Clin Pract. 2024;27(1):68–73. doi:10.4103/njcp.njcp_450_23
21. Hashmi AA, Naz S, Ahmed O, et al. Utility of Fine Needle Aspiration Cytology in the Evaluation of Lymphadenopathy. Cureus. 2020;12(12):e11990. doi:10.7759/cureus.11990
22. Rodriguez‐Takeuchi SY, Renjifo ME, Medina FJ. Extrapulmonary Tuberculosis. Radiographics. 2019;39:
23. Lee JY. Diagnosis and treatment of extrapulmonary tuberculosis.. Tuberc Respir Dis. 2015;78:
24. Rosenberg TL, Nolder AR. Pediatric cervical lymphadenopathy.. Otolaryngol Clin North Am. 2014;47:721–731. doi:10.1016/j.otc.2014.06.012
25. World Health Organization. Global Tuberculosis Report‐2019. Geneva, Switzerland: WHO; 2019.
26. Zumla A, Petersen E, Nyirenda T, Chakaya J. Tackling the tuberculosis epidemic in sub‐Saharan Africa‐‐unique opportunities arising from the second European Developing Countries Clinical Trials Partnership (EDCTP) programme 2015‐2024. Int J Infect Dis. 2015;32:
27. World Health Organization. Global tuberculosis report 2012 (WHO/HTM/TB/2012.6). Geneva. 2012. Available from: https://www.who.int/publications/i/item/9789241564502.
28. Olu-eddo AN, Omoti CE. Diagnostic evaluation of primary cervical adenopathies in a developing country. Pan Afr Med J. 2011;10:52.
29. Zhou H, Lei PJ, Padera TP. Progression of metastasis through lymphatic system. Cells. 2021;10:627. doi:10.3390/cells10030627
30. Peyam S, Bansal D. Empirical antitubercular treatment for lymphadenopathy: a luring trap! Indian J Pediatr. 2023;90(8):745–746. doi:10.1007/s12098-023-04734-2
31. Kabahweza HM, Spencer A. Childhood Hodgkin lymphoma in Sub-Saharan Africa: a systematic review on the effectiveness of the use of chemotherapy alone. Glob Pediatr Health. 2024;11:2333794X231223266. doi:10.1177/2333794X231223266
32. Jung IY, Ann HW, Kim JJ, et al. The incidence and clinical characteristics by gender differences in patients with Kikuchi-Fujimoto disease. Medicine. 2017;96(11):e6332. doi:10.1097/MD.0000000000006332
33. Jun WY, Ann YK, Kim JY, et al. Kawasaki disease with fever and cervical lymphadenopathy as the sole initial presentation. Korean Circ J. 2017;47(1):107–114. doi:10.4070/kcj.2016.0160
34. Malhotra AS, Lahori M, Nigam A, Khajuria A. Profile of lymphadenopathy: an institutional based cytomorphological study. Int J Appl Basic Med Res. 2017;7(2):100–103. doi:10.4103/2229-516X.205812
35. Richardson C, Redfern A, Sher-Locketz CL, Schubert PT, Schaaf HS. Fine needle aspiration biopsy of peripheral lymph nodes in children: practical experience in a tertiary hospital. J Trop Pediatr. 2021;67(3):fmaa040. doi:10.1093/tropej/fmaa040
36. Jin M, Wakely PE Jr. Endoscopic/endobronchial ultrasound‐guided fine needle aspiration and ancillary techniques, particularly flow cytometry, in diagnosing deep‐seated lymphomas. Acta Cytol. 2016;60:
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.