")
Back to Journals » Journal of Pain Research » Volume 18
Manual Therapy for Cervical Radiculopathy: Effects on Neck Disability and Pain – A Systematic Review and Network Meta-Analysis
Received 30 December 2024
Accepted for publication 9 April 2025
Published 14 April 2025 Volume 2025:18 Pages 2035—2045
DOI https://doi.org/10.2147/JPR.S513428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Michael A Ueberall
Xueliang Xu,1 Yan Ling2
1Department of Rehabilitation III, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, 610072, People’s Republic of China; 2Department of Pediatrics, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, 610072, People’s Republic of China
Correspondence: Yan Ling, Department of Pediatrics, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39 Shi-er-qiao Road, Chengdu, Sichuan Province, 610072, People’s Republic of China, Tel +86-13881816924, Email [email protected]
Objective: To evaluate the application effects of different manual therapy approaches in the treatment of cervical radiculopathy using a network meta-analysis.
Methods: Prospective randomized controlled trials on manual therapy for cervical radiculopathy published in PubMed, the Cochrane Library, and Embase databases were retrieved. The neck disability index and visual analogue scale for neck pain were collected and subjected to network meta-analysis.
Results: A total of 8 eligible studies involving 632 participants with a mean age range of 40– 47 years were included. The intervention duration ranged from 4 to 6 weeks. Three intervention groups were defined: Group C (exercise and other therapies without manual therapy), Group M (manual therapy without traction), and Group MT (manual therapy with traction). Larger circles indicate more patients, and thicker lines show more studies comparing interventions. Group M had the highest probability (68.1%) of improving the neck disability index, followed by Group MT (29.1%), with Group C the lowest (2.8%). Compared to Group C, neck disability index scores improved by 0.58 (95% CI: − 0.17, 1.33) in Group M and by 0.36 (95% CI: − 0.39, 1.11) in Group MT. The difference between Group M and Group MT was not significant (0.22, 95% CI: − 0.59, 1.03). For neck pain (visual analogue scale score), Group M had the highest probability (59.5%) of improvement, followed by Group MT (39.6%), with Group C the lowest (0.9%). Compared to Group C, the visual analogue scale score improved by 0.74 (95% CI: − 0.04, 1.52) in Group M and by 0.61 (95% CI: − 0.18, 1.40) in Group MT. The difference between Group M and Group MT was not significant (0.13, 95% CI: − 0.72, 0.98). Egger’s regression test showed no apparent publication bias.
Conclusion: Manual therapy is an effective approach for improving neck pain and neck disability index in patients with cervical radiculopathy, but more evidence-based support is needed regarding the use of cervical traction.
Keywords: radiculopathy, musculoskeletal manipulations, posterior neck pains
Introduction
Cervical radiculopathy (CR) is a clinical syndrome characterized by degenerative changes within the cervical intervertebral discs and pathological alterations in the surrounding tissues, leading to narrowing of the intervertebral foramina and subsequent compression or irritation of the exiting cervical nerve roots. This often manifests as pain, paresthesia, and other related neurological symptoms in the head, neck, and corresponding upper extremity dermatomes, with a close relationship to cervical posture and movement.1,2
CR is a common neurological condition caused by nerve root compression due to degenerative changes, disc herniation, or foraminal stenosis. It often presents with neck pain, radiating arm pain, sensory disturbances, and motor deficits, significantly impacting patients’ quality of life. Epidemiological data suggest that CR affects approximately 83 per 100,000 individuals annually, with peak incidence occurring between ages 40 and 50 years and a lifetime prevalence of 3.5% in the general population.3 Given its high burden, identifying effective non-invasive treatment strategies is critical. The underlying cervical spinal pathologies, including disc herniation, osteophyte formation, and spinal canal stenosis, are widely recognized as common precipitating factors for nerve root compression or inflammation in CR.3 Notably, the natural history of CR is often self-limiting, with symptom resolution observed in the majority of patients.4 Nonetheless, appropriate and timely management of CR can effectively mitigate symptoms and prevent disease progression.5,6
Conservative treatment modalities represent the mainstay of care for CR patients without severe neurological deficits, and also serve as the foundation for surgical interventions when warranted.7–9 Manual therapy (MT) is a prominent form of conservative treatment, typically provided by professional physical therapists, chiropractors, and, in some instances, other healthcare practitioners.10 It includes various hands-on techniques such as spinal manipulation, mobilization, and traction, aimed at reducing pain, improving joint mobility, and alleviating nerve compression. MT has been reported to enhance range of motion, muscular strength, and soft tissue healing, making it a valuable therapeutic option. MT can improve joint range of motion, enhance muscular strength, reduce pain and swelling, and decrease soft tissue inflammation.11 As a hands-on or mechanically-assisted technique applied to the patient’s body to treat or prevent disease, MT is a distinctive therapy for the management of cervical spondylosis.12 Traction, a specific type of MT, utilizes the principles of action and reaction forces, employing manual techniques, devices, or electromechanical systems to generate external forces acting on the spinal column or limb joints, resulting in appropriate tissue separation and stretching of the surrounding soft tissues to achieve therapeutic goals.13 Some studies suggest that cervical traction can relieve pressure on nerve roots, but others report that there are no additional functional improvements when compared to manual therapy alone.14 Núñez-Cabaleiro and Leirós-Rodríguez13 conducted a study which showed that the MT technique can effectively treat patients with cervicogenic headache. The combined use of the MT technique led to improved outcomes when compared to using the MT technique alone. However, its efficacy in relation to other conservative treatments, such as structured exercise programs or pharmacological interventions, still remains a matter of debate. Despite the widespread clinical use of MT in the management of CR, the available research on its efficacy remains limited, and consensus on its effects on neck disability index (NDI), pain, and range of motion has not been firmly established. This study aims to compare the effectiveness of different manual therapy approaches for CR using network meta-analysis, with a specific focus on whether cervical traction provides additional benefits in terms of pain relief and functional improvement (NDI, VAS). Although several studies have explored the benefits of MT for CR, their findings are inconsistent, and direct comparisons between different MT modalities are limited. Previous systematic reviews have primarily focused on pairwise comparisons, failing to establish a clear ranking of treatment efficacy. A network meta-analysis (NMA) offers a more robust approach, allowing for both direct and indirect comparisons across multiple interventions. By synthesizing available evidence, this review seeks to determine the most effective MT modality for improving patient outcomes. Unlike traditional meta-analysis, NMA allows for the simultaneous comparison of multiple interventions, even when direct comparative trials are limited. This approach ranks treatments based on their estimated probability of effectiveness, providing more comprehensive clinical guidance.
Methods
Study Design
This study was conducted as a meta-analysis of randomized controlled trials (RCTs), adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.14 It was preregistered in the International Platform of Registered Systematic Review and Meta-Analysis Protocols (INPLASY)-INPLASY202530079.
Literature Search Strategy
We conducted a comprehensive literature search in PubMed, Cochrane Library, and Embase up to June 2024. The search strategy incorporated a combination of Medical Subject Headings (MeSH) terms and free-text keywords to ensure a broad yet focused retrieval of relevant studies. Boolean operators were employed to refine the search, and appropriate filters were applied to enhance specificity. Additionally, we manually reviewed reference lists of pertinent systematic reviews and included studies to identify additional eligible articles. Database-Specific Search Strategies PubMed Search Strategy ((“Cervical Vertebrae”[MeSH] OR “Cervical Radiculopathy”[MeSH] OR “cervical” OR “radiculopathy”) AND (“Manual Therapy”[MeSH] OR “Physiotherapy”[MeSH] OR “manual therapy” OR “physiotherapy” OR “physical therapy”) AND (“Traction”[MeSH] OR “traction”)) Filters applied: Human studies, English language, publication date up to June 2024. Cochrane Library Search Strategy (“cervical” OR “cervical radiculopathy”) AND (“manual therapy” OR “physiotherapy” OR “physical therapy”) AND (“traction”) Filters applied: Trials, systematic reviews, English language, publication date up to June 2024. Embase Search Strategy (“cervical radiculopathy”/exp OR “cervical radiculopathy” OR “cervical”) AND (“manual therapy”/exp OR “manual therapy” OR “physiotherapy” OR “physical therapy”) AND (“traction”/exp OR “traction”) Filters applied: Human studies, English language, publication date up to June 2024.
Eligibility Criteria
The PICOS framework was applied to determine the inclusion criteria. P (Participants): Patients aged 18–80 years with unilateral or bilateral cervical radiculopathy, presenting with neck pain radiating to the corresponding upper extremity accompanied by sensorimotor dysfunction. I (Intervention): Manual therapy (M) or manual therapy combined with traction (MT). C (Comparison): Conventional treatment or sham MT therapy. O (Outcomes): Pain and functional outcomes, including NDI, Visual Analog Scale (VAS) or Numeric Rating Scale (NRS), and range of motion (ROM), assessed 4–6 weeks post-intervention. S (Study design): Randomized controlled trials.
Risk of Bias Assessment
Two authors meticulously scrutinized the included studies, independently evaluating the risk of bias using the well-established Cochrane Risk of Bias tool.15 This rigorous assessment delved into seven crucial domains: selection bias (encompassing random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (addressing incomplete outcome data), reporting bias (scrutinizing selective reporting), and any other potential sources of bias. Each domain was judiciously categorized as “low risk”, “high risk”, or “unclear”, ensuring a comprehensive and unbiased evaluation of the studies.
Qualitative Sensitivity Review of Included Studies
A qualitative sensitivity review assesses the impact of individual studies based on factors like study design, sample size, intervention details, and risk of bias.
Data Extraction
We extracted the following data using a pre-designed Excel spreadsheet: first author, publication year, patient characteristics, sample size, patient age, intervention details, intervention duration, and outcome measures. The extracted data were cross-checked, and any discrepancies were resolved by a third researcher.
Statistical Analysis
The statistical analysis was performed using Stata and the gemtc package in R. The outcome measures included NDI, VAS, and ROM, which were continuous variables. Considering the potential differences in assessment methods across studies, we used standardized mean differences (SMDs) to pool the effect sizes. For studies reporting means and standard deviations, we directly pooled the data. For studies reporting medians and interquartile ranges, we converted the data to means and standard deviations using the methods described by Luo et al16 and Wan et al.17 We assessed publication bias using Egger’s regression test. We calculated the Surface Under the Cumulative Ranking Curve (SUCRA) values and generated forest plots using Stata. SUCRA values represent the probability of an intervention being the best, ranging from 0 to 100, with higher values indicating better treatment efficacy and higher rankings.
Results
Literature Screening Process
The initial literature search retrieved a total of 2280 articles from various databases, with an additional 12 articles identified from other sources. After importing the literature into EndNote and removing duplicates, 886 articles remained. Screening of titles and abstracts led to the exclusion of 857 articles, including non-clinical studies, studies not utilizing manual therapy, and non-RCT studies. Full-text review of the remaining 29 articles resulted in the exclusion of 21 more, due to the inability to extract the specified data, intervention duration not meeting the requirements, and unavailability of necessary data. Ultimately, 8 articles were included in the final analysis. The literature selection process is depicted in the flow chart shown in Figure 1.
 |
Figure 1 Flow diagram of study selection. |
Characteristics of Included Studies
The 8 included studies involved a total of 632 participants, with a mean age range of 40–47 years, and intervention durations ranging from 4 to 6 weeks. The interventions were categorized into three groups: Group C, which utilized exercises and other therapies without manual therapy; Group M, which employed manual therapy but no traction; and Group MT, which utilized manual therapy, including traction. The basic characteristics of the included studies are summarized in Table 1. The risk of bias is shown in Figure 2.
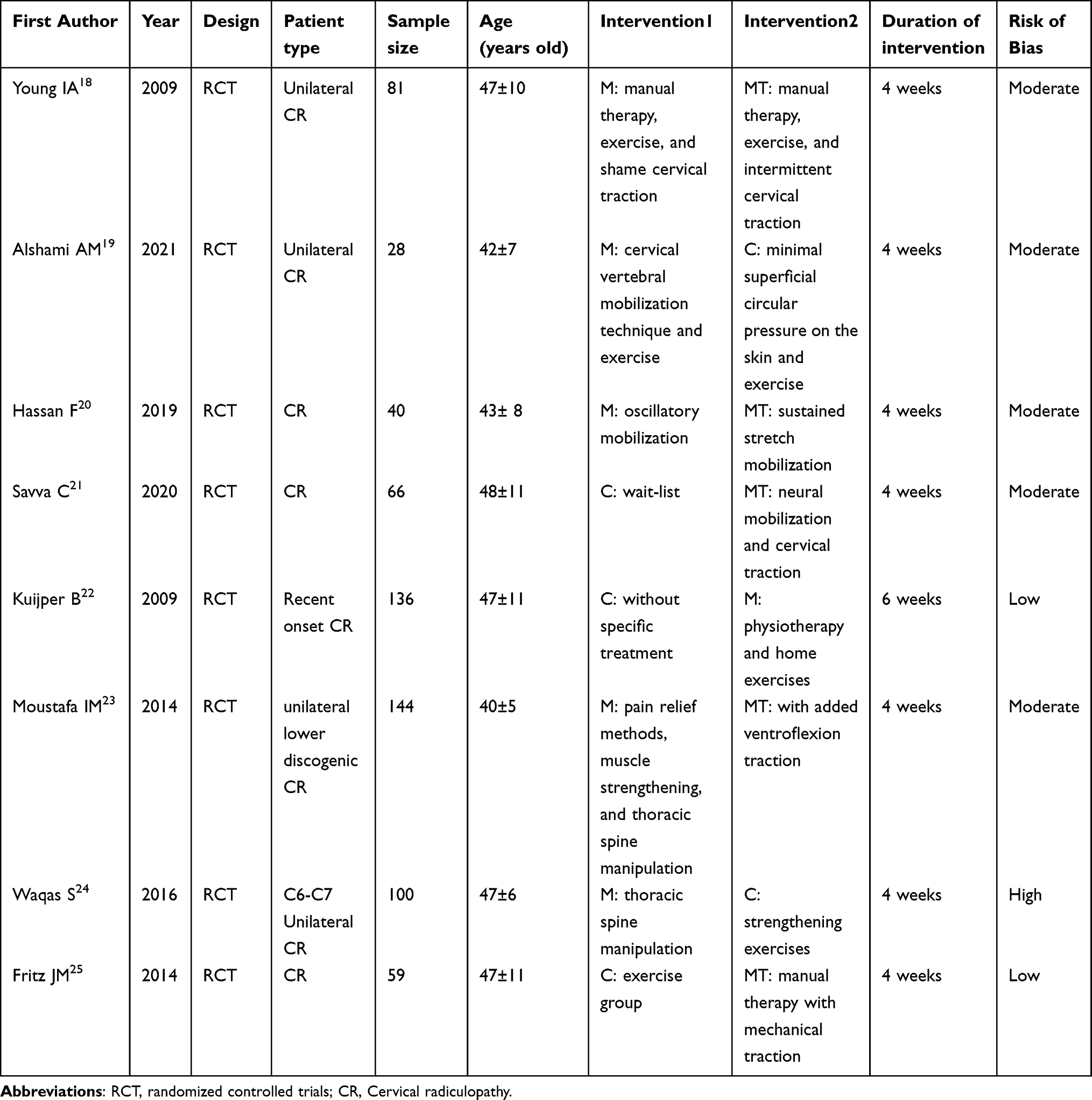 |
Table 1 Characteristics of Included Studies |
 |
Figure 2 Risk of bias summary. |
Main Results
Network Relationship Diagram
As shown in Figure 3a and b, the included studies with NDI and Neck VAS as outcomes formed a closed-loop network with the three intervention groups (C, M, and MT) as nodes. In the evidence network diagram, each point represents an intervention, and the lines between the points indicate direct comparisons between the two interventions. The thickness of the lines reflects the number of included studies comparing the two interventions, with thicker lines representing more studies. The size of the circles corresponds to the total number of patients who received the respective intervention. The network relationship diagram is presented in Figure 3.
 |
Figure 3 Network meta-analysis plots. (A) NDI, (B) VAS. |
Network Meta-Analysis Results for NDI
The effect sizes of the three treatment methods were analyzed, and the corresponding SUCRA (Surface Under the Cumulative Ranking Curve) values were calculated to determine the ranking of the optimal treatment combination. The cumulative ranking probability plot (Figure 4A) and the forest plot of pairwise comparisons (Figure 4B) were generated. The network meta-analysis results showed that for improving NDI, Group M had the best effect, with a 68.1% probability of achieving the best NDI improvement; Group MT had the second-best effect, with a 29.1% probability of achieving the best NDI improvement; and Group C had the worst effect, with a 2.8% probability of achieving the best NDI improvement. Pairwise comparisons revealed that compared to Group C, the NDI score decreased by 0.58 (95% CI: −0.17, 1.33) in Group M and 0.36 (95% CI: −0.39, 1.11) in Group MT; compared to Group M, the NDI score increased by 0.22 (95% CI: −0.59, 1.03) in Group MT, but the discrepancy was insignificant. The SUCRA and forest plots for the NDI outcome are shown in Figure 4.
 |
Figure 4 SUCRA and forest plot for NDI. (A) SUCRA plot; (B) Pairwise comparison forest plot. |
Network Meta-Analysis Results for Neck VAS
The effect sizes of the three treatment methods were analyzed, and the corresponding SUCRA values were calculated to determine the ranking of the optimal treatment combination. The cumulative ranking probability plot (Figure 5A) and the forest plot of pairwise comparisons (Figure 5B) were generated. The network meta-analysis results showed that for improving neck VAS, Group M had the best effect, with a 59.5% probability of achieving the best VAS improvement; Group MT had the second-best effect, with a 39.6% probability of achieving the best VAS improvement; and Group C had the worst effect, with a 0.9% probability of achieving the best VAS improvement. Pairwise comparisons revealed that compared to Group C, the VAS score decreased by 0.74 (95% CI: −0.04, 1.52) in Group M and 0.61 (95% CI: −0.18, 1.40) in Group MT; compared to Group M, the VAS score increased by 0.13 (95% CI: −0.72, 0.98) in Group MT, but the discrepancy was insignificant. The SUCRA and forest plots for the neck VAS outcome are shown in Figure 5.
 |
Figure 5 SUCRA and forest plot for neck VAS. (A) SUCRA plot; (B) Pairwise comparison forest plot. |
Publication Bias
Due to the limited number of included studies for the NDI and VAS indicators, Egger’s regression test was employed to assess the publication bias of these two indicators. The intercept of Egger’s regression test was 1.25, and the P - value was 0.018 (P < 0.05), which indicated a possible publication bias. The slope was −0.05, and the corresponding P - value was 0.682 (P > 0.05), suggesting that the relationship between the effect size and the standard error was not significant. Regarding the 95% confidence interval (CI), the 95% CI of the intercept was (0.23, 2.27), which did not include 0, further supporting the presence of publication bias.
Qualitative Sensitivity Review of Included Studies
Blinding & Randomization
Studies with a higher risk of bias due to the lack of blinding included.19–24 Studies adopting single - blind designs18,21,22,25 had a relatively lower risk of bias. In terms of blinding and sample size, the study by Kuijper et al22 was of the highest quality, providing robust evidence for the comparison between physiotherapy and collar treatment.
Sample Size Considerations
Studies with small sample sizes (<70), such as,19–21,23,24 contributed to greater variability in results. Studies with larger sample sizes (>100), like,18,22,25 offered more reliable estimates of the treatment effect. Excluding small - sample studies increased the weight of the results from the studies by Kuijper et al22 and Fritz et al,25 which suggested that traction did not provide significant additional benefits.
Study Heterogeneity (Variations in Interventions)
Some studies directly compared the effects of traction21,23,25 while others focused on the comparison between manual therapy and exercise alone.18–20 Studies like that by Waqas et al24 only concentrated on the differences among different manual therapy techniques, limiting the generalizability of the findings to traction - based interventions. Including only studies that directly compared manual therapy alone with manual therapy plus traction18,21,23,25 refined the conclusions regarding the efficacy of traction.
Publication Year & Recent Data
Older studies (published before 2015), such as,18,22–25 contributed significantly to the research findings. Recent studies (from 2020–2021), like,19–21 were likely to better reflect modern clinical practice. If newer trials had yielded different conclusions about the effect of traction, conducting a sensitivity analysis by excluding older studies might have altered the research results.
Conclusion from Sensitivity Analysis
Excluding studies with a high risk of bias and small sample sizes19,20,23,24 further validated that manual therapy alone was superior to traction - based approaches. The most robust studies22,25 suggested that traction did not significantly improve treatment outcomes, which was consistent with the results of the network meta - analysis. Although recent trials21 still indicated some benefits of traction, the evidence remained inconsistent. Future research should have focused on high - quality, large - scale randomized controlled trials that directly compared manual therapy alone with manual therapy + traction and adopted standardized research protocols.
Discussion
This study aimed to evaluate the effects of MT on the improvement of NDI and VAS scores in CR patients and to determine whether the addition of traction enhances these benefits. The results indicate that manual therapy, both with and without traction, significantly improves NDI and VAS scores. However, the supplementary use of traction did not provide additional benefits beyond those achieved with MT alone. The NMA results demonstrated that MT alone had the highest probability of achieving the greatest NDI improvement (68.1%), followed by MT with traction (29.1%), while conventional treatment had the lowest probability (2.8%). A similar trend was observed for VAS improvements, where MT alone was the most effective (59.5%), followed by MT with traction (39.6%), and conventional treatment had the least impact (0.9%). These findings suggest that MT alone may be the most effective intervention for improving disability and pain in CR patients. Despite these clear trends, previous studies on MT with or without traction have shown mixed results, with some reporting no significant difference between traction and sham traction, while others highlight positive effects. This variability may be attributed to several factors, including patient heterogeneity (eg, symptom severity, chronicity), differences in intervention duration and intensity, and methodological inconsistencies across studies. Additionally, the type of traction applied (manual vs mechanical) and the specific treatment protocols used may influence outcomes. Future research should aim to standardize intervention protocols and explore patient subgroups that may benefit more from traction-based therapies. In summary, while MT alone appears to be the most effective approach for improving NDI and VAS scores in CR patients, the role of traction remains unclear. MT alone should be prioritized when: The patient has mild to moderate CR with no severe nerve compression. The goal is to improve mobility, muscle strength, and pain relief without excessive mechanical strain. The patient has no contraindications to manual therapy (eg, osteoporosis, inflammatory arthritis). MT + traction may be considered when: The patient exhibits severe nerve root compression symptoms, including persistent radicular pain, neurological deficits, or significant motor weakness. Imaging confirms foraminal stenosis or disc herniation with nerve root impingement, suggesting that traction may help create additional space. Other conservative treatments have failed to provide sufficient symptom relief. While some previous studies suggest traction may benefit certain subgroups, patient selection is key—more research is needed to determine who benefits most from traction and under what conditions it is effective.26–28
Currently, multiple meta-analyses have explored the differences in the efficacy of various treatment modalities for CR. The meta-analysis by Zhu et al included 3 trials involving 502 participants and showed that manual therapy had better direct effects on pain relief compared to traction alone, but had less impact on function/disability.29 The meta-analysis by Salt et al found no statistically significant differences in the effectiveness of active traction and sham traction in terms of pain, function, or disability at post-intervention or various follow-ups.30 The meta-analysis by Thoomes EJ et al also indicated no difference in effects between traction and sham traction.7 To date, this is the first meta-analysis to compare the effectiveness of conventional treatment, MT without traction, and MT combined with traction on pain and disability in CR. Unlike previous studies, our study found that the addition of traction to other MT interventions did not significantly improve pain and function, and was even less beneficial, although the difference was not statistically significant. The possible reasons for this may be: 1) the included studies were single-center, and there were significant differences in the severity of patients and the intervention methods of the operators, which had a substantial impact on the outcomes; 2) the number of included studies was still relatively small, and the reliability of the conclusions was relatively low. Given the limited number of studies included for the NDI and neck VAS indicators, a funnel plot analysis was performed to assess potential publication bias. Visual examination of the funnel plot did not show any obvious asymmetry, which initially indicated no substantial publication bias. However, it is important to note that funnel plot analysis, despite being a valuable tool, has certain limitations, especially when the number of included studies is small, as is the case in this meta - analysis.
Although no strong evidence of publication bias was detected through the funnel plot, the possibility of selective reporting cannot be disregarded. Studies with small sample sizes are more prone to reporting bias, where only significant results are disseminated, while negative or inconclusive findings remain unpublished. This can lead to an over - representation of positive outcomes and distort the overall evidence base. Furthermore, industry - funded studies may have a higher tendency to report favorable results, potentially biasing the overall findings. To address these issues, future research should incorporate more quantitative assessment methods, such as Egger’s test or trim - and - fill analysis, to more comprehensively evaluate potential bias. In addition, mandating the pre - registration of clinical trials and ensuring the complete reporting of all outcomes can play a crucial role in reducing selective reporting in future research. Pre - registration allows for the transparency of study design and planned outcomes, making it easier to detect discrepancies between the initial study plan and the final reported results. Complete outcome reporting ensures that all relevant data, regardless of statistical significance, are made available to the scientific community, thereby enhancing the reliability and validity of research findings. This study also has certain limitations. 1) The quality of the data in the included literature was poor. Although the mean and standard deviation were used as the expression of the NDI and VAS indicators, these data were not normally distributed, and the use of SMD as the effect size for pooling has inherent statistical problems. 2) The intervention measures included in the literature were very complex, and in this study they were divided into MT without traction and MT combined with traction, which was inadequate and inappropriate. Since the studies included in this research were published between 2013 and 2016, and the analysis mainly referred to research from Western and Asian regions, this restricts the generalizability of the research findings across different healthcare settings. Manual therapy practices vary globally, influenced by clinical training, cultural preferences, and healthcare accessibility. Thus, a broader perspective is needed. An action plan for strengthening the research should be implemented to ensure the inclusion of all eligible studies published from 2023 to 2024. This aims to provide a more up - to - date and clinically relevant evidence synthesis, eliminate geographical biases, and enhance a global perspective. In the future, the literature search will be updated to incorporate recent randomized controlled trials and systematic reviews (2023–2024). The scope will be expanded to include non - English - language sources and studies from diverse regions. Additionally, a critical analysis of the geographical variability in MT and traction will be conducted to improve external validity. These improvements will enhance the credibility, relevance, and applicability of the research conclusions in the future.
Therefore, future research should clarify the role of MT and traction in CR management, and address the following gaps, (1) Larger, Multicenter RCTs with diverse populations: Most existing studies have small sample sizes, limiting generalizability. Future trials should include larger cohorts across multiple clinical settings to improve external validity. (2) Standardized MT protocols: studies use varied MT techniques (mobilization, manipulation, soft tissue therapy, etc)., making direct comparisons difficult. Future trials should adopt standardized treatment protocols to determine which MT techniques are most effective. (3)Patient-specific treatment strategies: current research lacks subgroup analysis to identify which patients benefit from MT alone vs MT with traction. Future studies should examine factors like symptom severity, chronicity, and imaging findings to refine clinical recommendations. (4) Long-term outcomes and follow-up: most trials assess outcomes at 4–12 weeks, but long-term effectiveness remains unclear. RCTs with 6–12 month follow-up periods should be conducted to evaluate sustained benefits and recurrence rates. By addressing these gaps, future research can establish clearer clinical guidelines for optimizing manual therapy interventions in cervical radiculopathy.
However, this study also showed that the application of MT, regardless of the specific technique used, could effectively reduce neck pain and decrease the neck disability index in the short term. It is necessary to reach a consensus on the definition and standardization of MT for CR in order to further analyze the effectiveness of MT for CR.
Conclusions
This study confirms that MT is an effective intervention for improving neck pain and disability in patients with CR. The findings suggest that MT alone provides the greatest improvement in both the NDI and VAS scores, with traction offering no additional benefits. While traction remains widely used in clinical practice, current evidence does not strongly support its routine application alongside MT. The results indicate that MT alone should be prioritized unless specific patient criteria warrant the use of traction. However, due to variability in existing studies, further high-quality, large-scale RCTs with standardized protocols are needed to determine which patient subgroups, if any, may benefit from traction. In summary, MT alone should be considered the first-line conservative treatment for CR, and the role of traction requires further investigation before it can be widely recommended.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Study on the correlation between positive signs on X-ray of the upper neck segment and head and neck symptoms, Specialized Project of Traditional Chinese Medicine Research in Sichuan Province, 2024MS192.
Disclosure
The authors declare that they have no competing interests.
References
1. Jajeh H, Lee A, Charls R, Coffin M, Sood A, Elgafy H. A clinical review of hand manifestations of cervical myelopathy, cervical radiculopathy, radial, ulnar, and median nerve neuropathies. J Spine Surg. 2024;10:120–134. doi:10.21037/jss-23-39
2. Kim KT, Kim YB. Cervical radiculopathy due to cervical degenerative diseases: anatomy, diagnosis and treatment. J Korean Neurosurg Soc. 2010;48:473–479. doi:10.3340/jkns.2010.48.6.473
3. Zhang AS, Myers C, McDonald CL, Alsoof D, Anderson G, Daniels AH. Cervical myelopathy: diagnosis, contemporary treatment, and outcomes. Am J Med. 2022;135:435–443. doi:10.1016/j.amjmed.2021.11.007
4. Casey E. Natural history of radiculopathy. Phys Med Rehabil Clin N Am. 2011;22:1–5. doi:10.1016/j.pmr.2010.10.001
5. Kang KC, Lee HS, Lee JH. Cervical radiculopathy focus on characteristics and differential diagnosis. Asian Spine J. 2020;14:921–930. doi:10.31616/asj.2020.0647
6. Bono CM, Ghiselli G, Gilbert TJ, et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11:64–72. doi:10.1016/j.spinee.2010.10.023
7. Thoomes EJ, Scholten-Peeters W, Koes B, Falla D, Verhagen AP. The effectiveness of conservative treatment for patients with cervical radiculopathy: a systematic review. Clin J Pain. 2013;29:1073–1086. doi:10.1097/AJP.0b013e31828441fb
8. Engquist M, Löfgren H, Öberg B, et al. Factors affecting the outcome of surgical versus nonsurgical treatment of cervical radiculopathy: a randomized, controlled study. Spine. 2015;40:1553–1563. doi:10.1097/BRS.0000000000001064
9. Gross A, Kay TM, Paquin JP, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2015;1:Cd004250. doi:10.1002/14651858.CD004250.pub5
10. Kerry R, Young KJ, Evans DW, et al. A modern way to teach and practice manual therapy. Chiropr Man Therap. 2024;32:17. doi:10.1186/s12998-024-00537-0
11. Borrella-Andrés S, Marqués-García I, Lucha-López MO, et al. Manual therapy as a management of cervical radiculopathy: a systematic review. Biomed Res Int. 2021;2021:9936981. doi:10.1155/2021/9936981
12. Gross AR, Lee H, Ezzo J, et al. Massage for neck pain. Cochrane Database Syst Rev. 2024;2:Cd004871.
13. Núñez-Cabaleiro P, Leirós-Rodríguez R. Effectiveness of manual therapy in the treatment of cervicogenic headache: a systematic review. Headache. 2022;62(3):271–283. doi:10.1111/head.14278
14. Parums DV. Editorial: review articles, systematic reviews, meta-analysis, and the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. Med Sci Monit. 2021;27:e934475. doi:10.12659/MSM.934475
15. Nejadghaderi SA, Balibegloo M, Rezaei N. The Cochrane risk of bias assessment tool 2 (RoB 2) versus the original RoB: a perspective on the pros and cons. Health Sci Rep. 2024;7:e2165. doi:10.1002/hsr2.2165
16. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27:1785–1805. doi:10.1177/0962280216669183
17. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
18. Young IA, Michener LA, Cleland JA, Aguilera AJ, Snyder AR. Manual therapy, exercise, and traction for patients with cervical radiculopathy: a randomized clinical trial. Phys Ther. 2009;89:632–642. doi:10.2522/ptj.20080283
19. Alshami AM, Bamhair DA. Effect of manual therapy with exercise in patients with chronic cervical radiculopathy: a randomized clinical trial. Trials. 2021;22:716. doi:10.1186/s13063-021-05690-y
20. Hassan F, Osama M, Ghafoor A, Yaqoob MF. Effects of oscillatory mobilization as compared to sustained stretch mobilization in the management of cervical radiculopathy: a randomized controlled trial. J Back Musculoskelet Rehabil. 2020;33:153–158. doi:10.3233/BMR-170914
21. Savva C, Korakakis V, Efstathiou M, Karagiannis C. Cervical traction combined with neural mobilization for patients with cervical radiculopathy: a randomized controlled trial. J Bodyw Mov Ther. 2021;26:279–289. doi:10.1016/j.jbmt.2020.08.019
22. Kuijper B, Tans JT, Beelen A, Nollet F, de Visser M. Cervical collar or physiotherapy versus wait and see policy for recent onset cervical radiculopathy: randomised trial. BMJ. 2009;339:b3883. doi:10.1136/bmj.b3883
23. Moustafa IM, Diab AA. Multimodal treatment program comparing 2 different traction approaches for patients with discogenic cervical radiculopathy: a randomized controlled trial. J Chiropr Med. 2014;13:157–167. doi:10.1016/j.jcm.2014.07.003
24. Waqas S, Ahmad A, Ahmad S, Shafi T, Shahid HA. Comparison of maitland thoracic spine manipulation versus maitland cervical spine mobilization in chronic unilateral C6 – C7 cervical radiculopathy. Ann King Edw Med Univ. 2016;22. doi:10.21649/akemu.v22i2.1285
25. Fritz JM, Thackeray A, Brennan GP, Childs JD. Exercise only, exercise with mechanical traction, or exercise with over-door traction for patients with cervical radiculopathy, with or without consideration of status on a previously described subgrouping rule: a randomized clinical trial. J Orthop Sports Phys Ther. 2014;44:45–57. doi:10.2519/jospt.2014.5065
26. Kim DG, Chung SH, Jung HB. The effects of neural mobilization on cervical radiculopathy patients’ pain, disability, ROM, and deep flexor endurance. J Back Musculoskelet Rehabil. 2017;30:951–959. doi:10.3233/BMR-140191
27. Parenteau CS, Lau EC, Campbell IC, Courtney A. Prevalence of spine degeneration diagnosis by type, age, gender, and obesity using Medicare data. Sci Rep. 2021;11:5389. doi:10.1038/s41598-021-84724-6
28. Kuligowski T, Skrzek A, Cieślik B. Manual therapy in cervical and lumbar radiculopathy: a systematic review of the literature. Int J Environ Res Public Health. 2021;19:18. doi:10.3390/ijerph19010018
29. Zhu L, Wei X, Wang S. Does cervical spine manipulation reduce pain in people with degenerative cervical radiculopathy? A systematic review of the evidence, and a meta-analysis. Clin Rehabil. 2016;30:145–155. doi:10.1177/0269215515570382
30. Salt E, Wright C, Kelly S, Dean A. A systematic literature review on the effectiveness of non-invasive therapy for cervicobrachial pain. Man Ther. 2011;16:53–65. doi:10.1016/j.math.2010.09.005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.