")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Manuscript Title: Regulatory and Implications of Complementary and Alternative Medicine (CAM) Use for Infection Prevention: Insights From the Gulf Cooperation Council (GCC) Countries
Authors Alhomoud FK
Received 12 February 2025
Accepted for publication 17 June 2025
Published 24 June 2025 Volume 2025:18 Pages 2081—2090
DOI https://doi.org/10.2147/RMHP.S522405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Farah Kais Alhomoud
Department of Pharmacy Practice, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, The Kingdom of Saudi Arabia
Correspondence: Farah Kais Alhomoud, Department of Pharmacy Practice, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, the Kingdom of Saudi Arabia, King Faisal Ibn Abd Al Aziz Road, Imam Abdulrahman Bin Faisal University, Dammam, 34212, Tele +966133335547, Email [email protected]
Purpose: The growing use of complementary and alternative medicine (CAM) for infection prevention across Gulf Cooperation Council (GCC) countries raises important concerns regarding patient safety and the lack of evidence-based regulation. This study aimed to assess the prevalence of CAM use, identify associated demographic factors, and explore public perceptions to support healthcare policy development.
Patients and Methods: A cross-sectional online survey was conducted over a three-month period among GCC residents aged 18 years and older. A self-administered questionnaire was distributed via social media platforms (eg Facebook, WhatsApp, and Twitter) using a convenience sampling approach, supplemented by snowballing. Although the calculated target sample size was 385, a total of 340 participants completed the survey. The questionnaire included items related to demographics, CAM practices, knowledge, and beliefs. Data were analyzed using IBM SPSS Statistics version 26, and chi-square tests were used to explore associations between CAM use frequency and participant characteristics.
Results: Herbal products (62%) and spiritual healing (14%) emerged as the most commonly used CAM practices, with ginger, Curcuma longa, and garlic being the most frequently used herbs. More frequent CAM use was significantly associated with education level (χ²(3) = 19.01, p < 0.001, Cramér’s V = 0.160), country of residence (χ²(5) = 35.28, p < 0.001, Cramér’s V = 0.217), and prior infection experience (χ²(2) = 35.14, p < 0.001, Cramér’s V = 0.217). Higher usage was reported among Saudis, individuals with higher education, and those previously ill. No significant associations were found with age, health status, or fear of infection. Although 85% of users reported no side effects, reliance on informal sources and limited provider consultation raised safety concerns.
Conclusion: Widespread CAM use highlights the urgent need for regulatory oversight, provider education, and culturally sensitive public health strategies to ensure safe integration into infection prevention efforts.
Keywords: infections, complementary therapies, alternative medicine, integrative medicine, holistic health, middle east
Introduction
The coronavirus pandemic prompted individuals worldwide to adopt various protective measures, including complementary and alternative medicine (CAM), in response to the escalating cases and mortality rates, particularly in the Gulf Cooperation Council (GCC) countries. During the pandemic’s early stages, the vaccine availability delay further fueled the reliance on alternative preventive strategies.1–4
CAM refers to non-conventional medical practices used either alongside (complementary) or instead of (alternative) standard treatments. It includes therapies like herbal medicine, acupuncture, yoga, and dietary interventions, focusing on holistic and personalized care. While CAM aims to enhance overall health and well-being, its safety and effectiveness often require scientific validation.5,6
In the GCC, CAM methods are frequently used as alternatives or alongside conventional treatments for various infections. Despite the widespread belief in CAM’s efficacy, scientific evidence supporting its preventive capabilities against infections remains lacking, with many claims propagated through social networks.7–9 While CAM can promote general health, it is not proven to cure or prevent illnesses.10,11 Nevertheless, users frequently overlook potential adverse effects, drug-food interactions, and other risks due to misconceptions about its safety and effectiveness.12,13
The widespread reliance on CAM in the GCC for managing chronic and incurable conditions raises critical public health and regulatory concerns, particularly given the lack of scientific evidence supporting its effectiveness against viral infections, as the World Health Organization (WHO) noted.14,15 While previous studies on CAM in the region have focused primarily on herbal products in Saudi Arabia,3,4,16 broader insights into its prevalence, safety perceptions, and policy implications remain limited. This study aims to fill this gap by assessing CAM use across the GCC, evaluating public awareness, and identifying key factors influencing its adoption. The findings will help inform risk management strategies, regulatory policies, and evidence-based public health interventions to ensure CAM’s safe and informed use in infection prevention.
Materials and Methods
Study Setting, Recruitment and Data Collection
This cross-sectional, internet-based questionnaire study was conducted over three months (from October 2024 to January 2025) after obtaining ethical approval from the Institutional Review Board. A convenience sampling method supplemented by snowballing was employed. The survey was disseminated via social media platforms (Facebook, WhatsApp, and Twitter), targeting GCC residents aged 18 years and above. Participants who did not use CAM or failed to complete the questionnaire were excluded. These platforms were selected due to their high usage rates across GCC countries, making them effective for reaching a broad and diverse segment of the adult population. Their accessibility and widespread popularity facilitated efficient distribution, especially given the online nature of the study and the snowball sampling technique used. Data collection was facilitated through the QuestionPro online questionnaire service, with participants directed to the survey via a generated link. An introductory page outlined the study’s purpose and inclusion criteria, followed by a click-wrap agreement to confirm informed consent. Ethical approval was obtained from the Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB-2024-05-734, dated 15/10/2024), and informed consent was secured. In addition, this study was conducted in accordance with the principles of the Declaration of Helsinki.
Sample Size
The sample size was calculated using the Raosoft online calculator.17 Based on a GCC statistical Centre, the GCC population of 57.6 million of 2023 records,18 a minimum of 385 participants was required to achieve a 95% confidence level with a 5% margin of error.
Study Instrument Development and Validation
A questionnaire was developed based on prior studies,3,4,16 and reviewed by three external experts for content validity. Six volunteers pre-tested the questionnaire to ensure clarity and usability, with pilot data excluded from the analysis. The final English-language questionnaire comprised multiple domains: demographics and health status, as well as participants’ use, beliefs, and awareness of CAM as a preventive measure against infections.
Data Processing and Analysis
The completed survey was processed and analyzed using a quantitative approach in IBM SPSS Statistics version 26. All demographic characteristics were reported, and responses to the questionnaire were summarized using descriptive statistics. Chi-square tests examined associations between how often CAM is used and various demographic factors.
Results
Of the 747 respondents, 340 completed the questionnaire, resulting in a response rate of 46%. At the outset of the questionnaire, all respondents who accessed the survey (N = 747) were asked whether they used CAM. A total of 407 participants responded “No”, indicating non-use of CAM, and were therefore excluded from further analysis as they did not meet the study’s inclusion criteria. Consequently, the final analytical sample comprised 340 participants who reported using CAM and were assessed for their perceptions and experiences. An additional question was posed to these participants to evaluate the frequency of CAM use, asking whether they used CAM often or not. “Often” was defined as using CAM at least once per week. Among the 340 CAM users, 297 participants (87%) reported using CAM frequently (ie, at least once a week).
Characteristics of the Study Participants
The majority of participants were aged 18–38 years (n=282, 83%), lived in urban areas (n=298, 88%), and were primarily from Saudi Arabia (n=100, 29%), followed by Kuwait (n=74, 22%) and Oman (n=54, 16%). Most respondents held a university degree (n=253, 74%), while 11% (n=36) had postgraduate qualifications (see Table 1). The study reports p-values using chi-square tests and effect sizes (Cramér’s V) to assess the strength of relationships between CAM used frequently and participant characteristics. A significant association was found between education level and more frequent CAM use (χ²(3) = 19.01, p <0.001, Cramér’s V = 0.160), indicating a modest relationship. Similarly, country of residence (χ²(5) = 35.28, p <0.001, Cramér’s V = 0.217) and prior experience of infection symptoms (χ²(2) = 35.14, p <0.001, Cramér’s V = 0.217) showed moderate associations with CAM use frequency. Higher CAM use was reported among participants from Saudi Arabia, those with higher educational attainment, and individuals who had previously experienced infection, suggesting that recent illness may influence adoption. In contrast, no significant associations were observed between frequent CAM use and age (Cramér’s V = 0.074, p =0.127), perceived health status (Cramér’s V = 0.018, p =0.614), or fear of disease (p =0.067). Although 85% of participants reported no side effects, the widespread reliance on informal sources and the low rate of consultation with healthcare providers raise concerns about the long-term safety of CAM and the potential for herb-drug interactions.
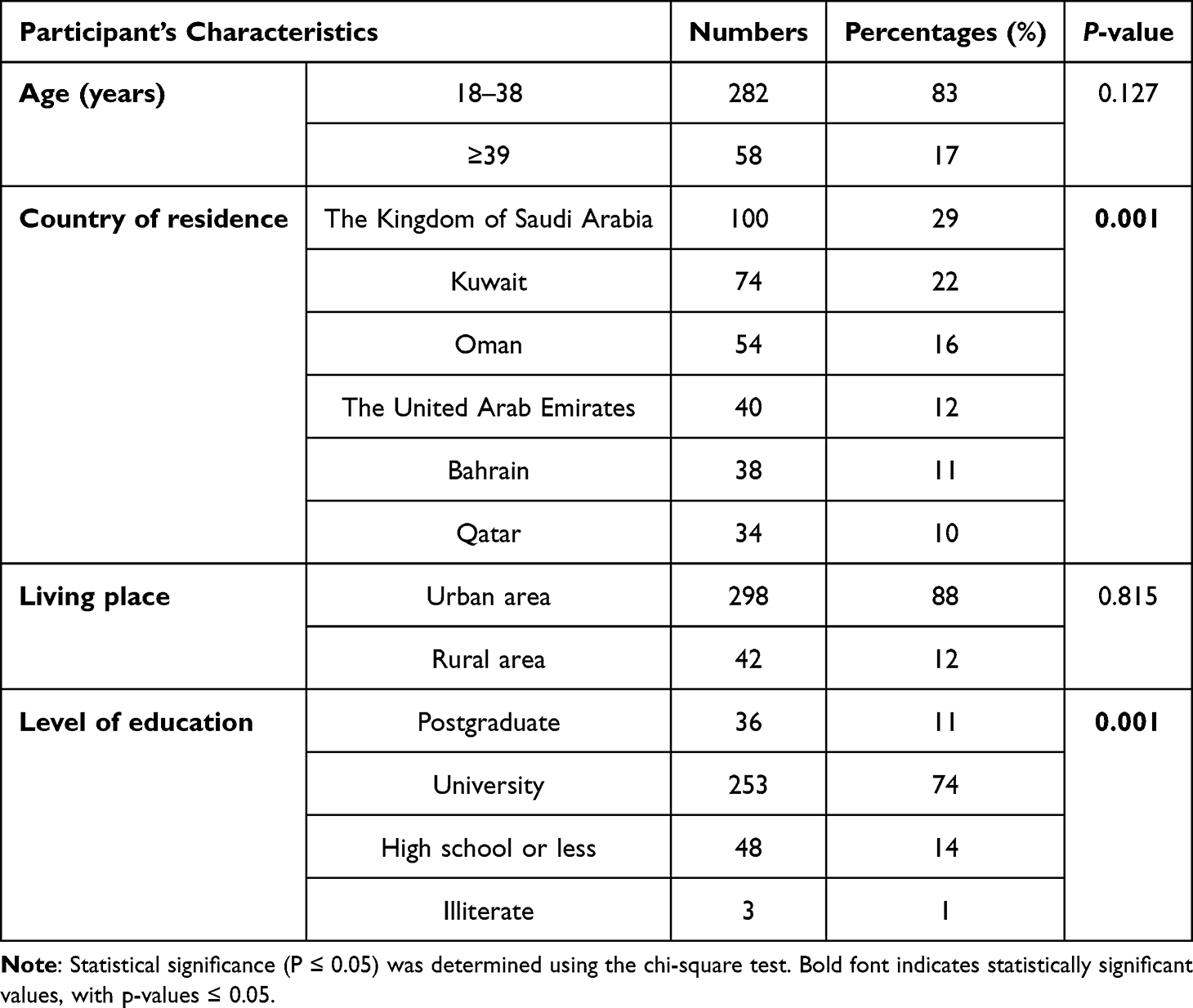 |
Table 1 Demographic Characteristics of Participants (n=340) |
Health Status of the Participants
Most participants reported being healthy (n = 301, 89%) with no chronic health conditions. CAM was used just as often by healthy individuals as those with health issues, with no significant difference between the two groups (p = 0.614). However, participants who had experienced infection symptoms were significantly more likely to use CAM frequently (p = 0.001). On the other hand, fear of infection, reported by 58% of participants (n = 197), was not significantly linked to whether CAM was used often or not (p = 0.067) (see Table 2).
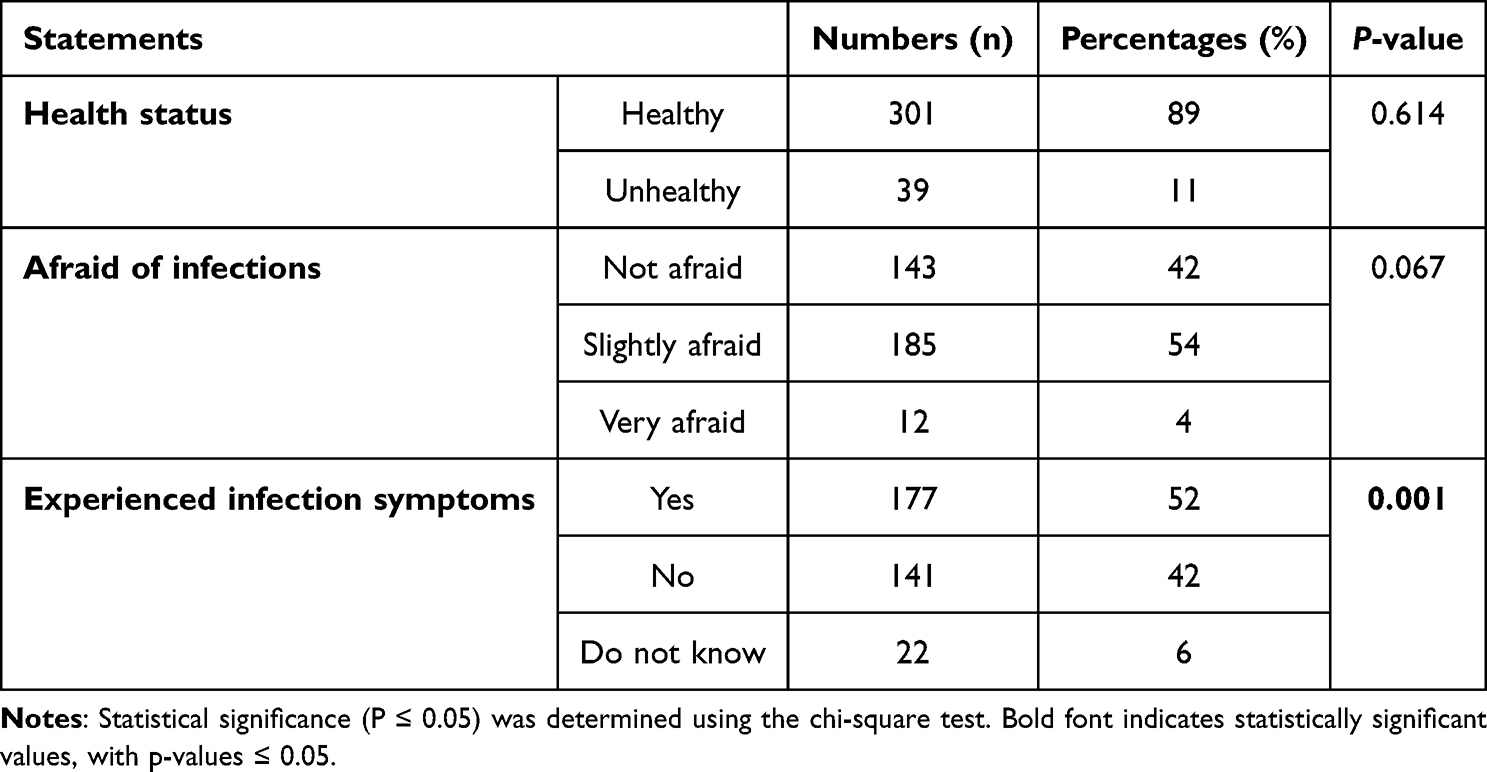 |
Table 2 Health Status of Participants (n=340) |
Practices Towards CAM
Nearly half of the participants (46%) used CAM as a preventive measure during the pandemic. The most common practices included herbal product use (n=210, 62%), spiritual healing (n=49, 14%), and hijamah (n=26, 8%). Self-practices included prayers (n=208, 61%) and breathing exercises (n=113, 33%). Frequently used CAM included vitamins or mineral supplements (71%), honey or bee products (63%), and herbs (60%), such as ginger (70%), Curcuma longa (43%), and garlic (41%). Most users reported no side effects (85%), while 14% experienced mild to moderate effects (see Table 3).
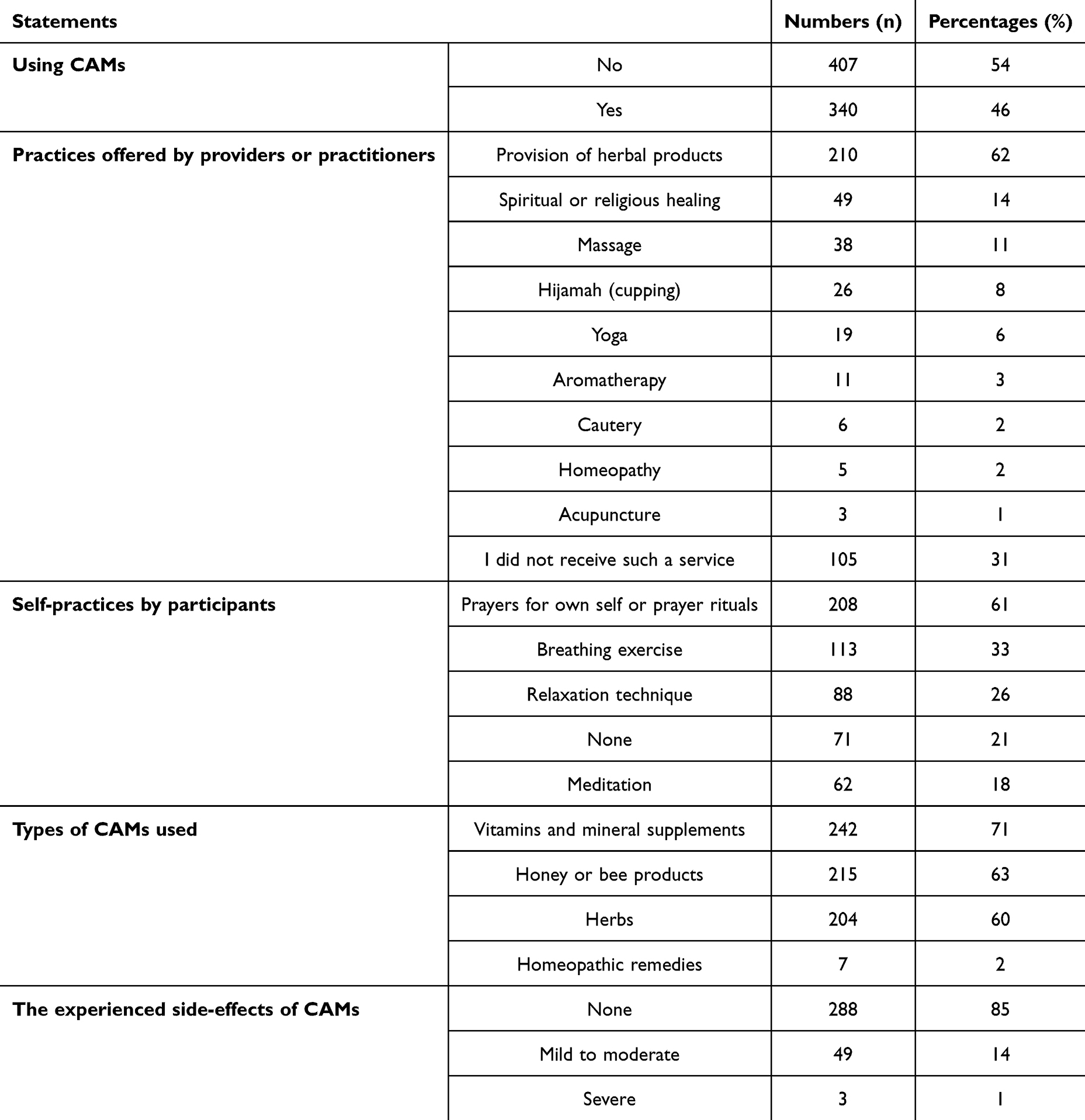 |
Table 3 Participants’ Practices and Experiences with Complementary and Alternative Medicine (CAM) (n=340) |
Knowledge of CAM
CAM knowledge was primarily sourced from family (73%) and the internet (43%). Only 20% consulted healthcare providers regarding CAM use, citing reasons such as lack of inquiry by medical staff (43%) and a belief that it was unnecessary (35%). Most participants viewed CAM as effective (49%) and safe (51%) and recommended its use to others (41%). However, 49% believed that healthcare providers might disagree with CAM use due to insufficient scientific evidence, and 26% noted concerns about drug interactions. See Table 4 for more information regarding participants’ knowledge and awareness.
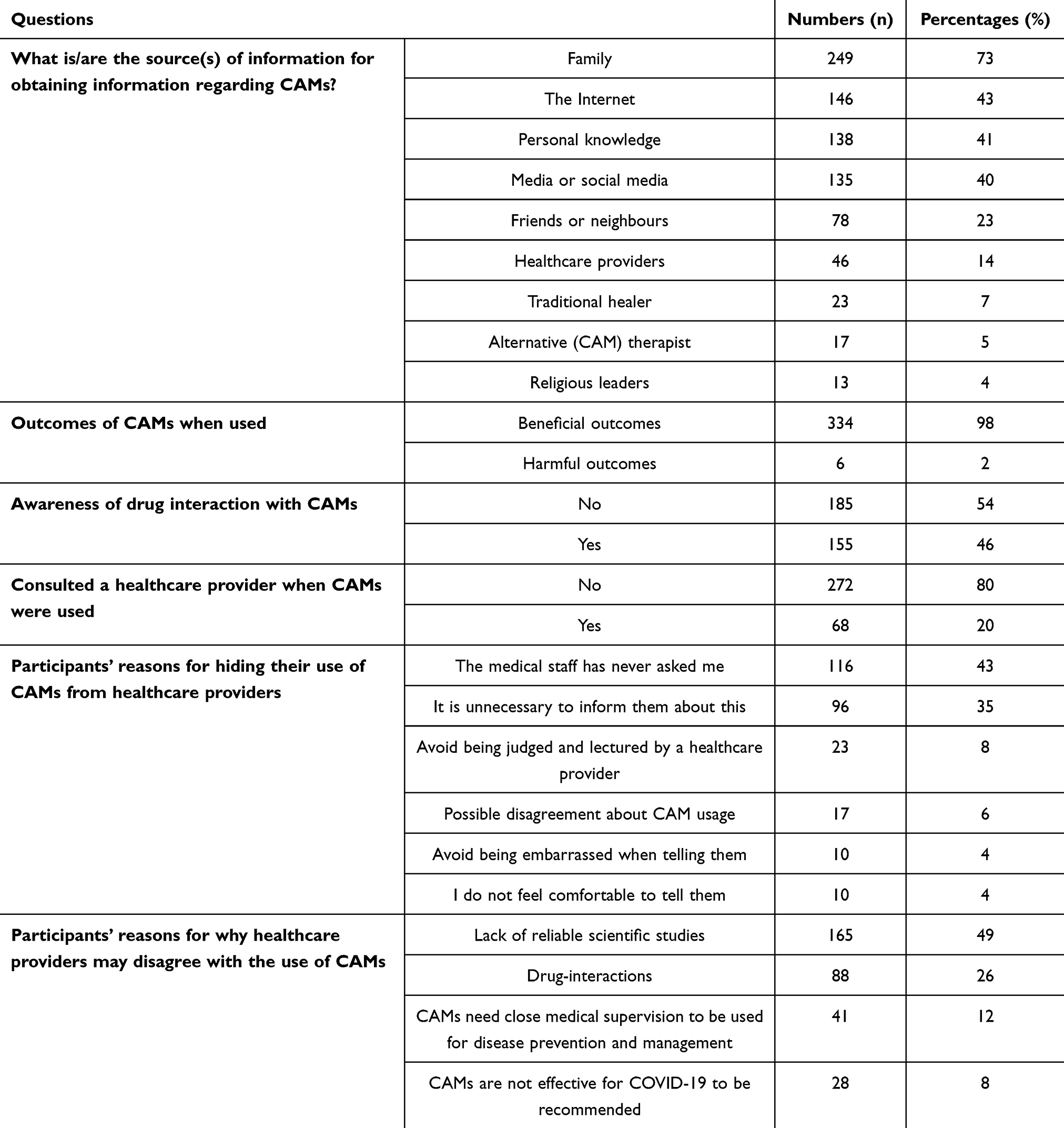 |
Table 4 Participants’ Knowledge, Perceptions, and Barriers to CAM Use |
Participants’ Perceptions of CAM
While 62% agreed CAM had therapeutic benefits, 30% preferred conventional medicines for infection prevention. CAM was perceived as popular (56%), effective (62%), and safe (51%), though a notable portion remained neutral or skeptical about its superiority over conventional medicine (see Figure 1).
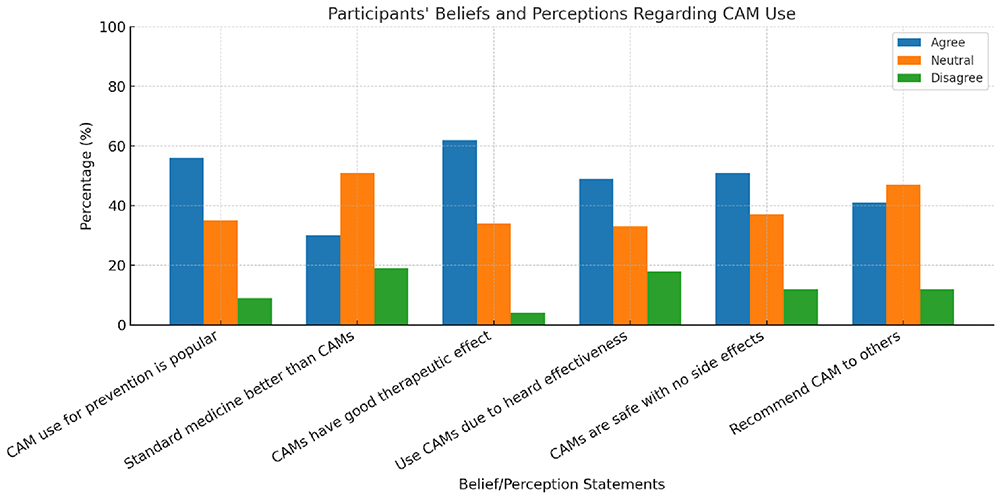 |
Figure 1 Participants’ Beliefs and Perceptions Regarding CAM Use. |
Discussion
This study is the first to comprehensively examine the prevalence, practices, and perceptions of CAM use across the GCC region. The findings highlight the widespread use of CAM since the beginning of the COVID-19 pandemic, particularly for infection prevention, aligning with previous research conducted in single-country contexts, such as Saudi Arabia,3,4,16 India,13 Bangladesh,19 and Ghana.20 This study underscores the role of demographic factors, such as education and nationality, in influencing CAM use. Participants with higher educational attainment and those from Saudi Arabia reported significantly greater CAM usage, reflecting the impact of cultural and academic contexts on health behaviors.
Consistent with earlier findings,3,4,16,20 herbal products, vitamins, and honey were the most commonly used CAM, with minimal reported adverse effects. Specific herbs like ginger, garlic, and Curcuma longa were particularly popular, likely due to their cultural significance and perceived health benefits. However, while most participants perceived CAM as effective and safe, concerns remain about the lack of evidence-based use and potential drug-herb interactions. This is particularly critical as most participants relied on informal sources, such as family and the Internet, rather than consulting healthcare providers for CAM information. Such reliance on unverified information could lead to inappropriate or unsafe practices, a concern previously noted in similar studies.9,10
This study identified statistically significant associations between how often CAM is used, educational level, and country of residence (p = 0.001), suggesting that participants from Saudi Arabia and more educated individuals tend to use CAM more frequently. Additionally, participants who had previously experienced infection were significantly more likely to use CAM often (p = 0.001), indicating that recent illness may motivate individuals to adopt alternative preventive measures. In contrast, CAM was not used more often by those who reported fear of infection (p = 0.067) or those with different health statuses (p = 0.614). This lack of association with fear differs from findings in previous studies, which often highlight fear as a driver of increased CAM use during public health crises. This discrepancy may reflect distinct cultural or contextual factors in the GCC region. Overall, the frequency of CAM use is more influenced by personal health experiences and education rather than emotional factors such as fear. Although 85% of participants reported no side effects from CAM use, these findings are based on short-term, self-reported data and may not reflect potential long-term adverse effects or herb-drug interactions. The widespread and frequent reliance on informal sources, such as family and the Internet, and the low rate of consultation with healthcare providers raise concerns about the safety of CAM use. Without professional guidance or structured follow-up, the accurate safety profile of frequently used CAM remains unclear, particularly when combined with conventional treatments. Future research should focus on the long-term safety and interaction risks of commonly used CAM therapies, especially among vulnerable populations and individuals with chronic health conditions.
The fact that only 20% of participants consulted healthcare providers about CAM use highlights a significant gap in both clinical practice and public health communication. Many participants did not disclose their CAM use either because they felt it was irrelevant or were not asked by their providers, while others feared disapproval due to a perceived lack of scientific support. This limited interaction represents a missed opportunity to integrate CAM into healthcare systems safely. It may hinder the early identification of potential herb-drug interactions, reduce opportunities for patient education, and compromise coordinated infection prevention efforts.
From a public health perspective, these findings emphasize the need to foster trust, promote open dialogue, and encourage evidence-based discussions about CAM in clinical settings. Risk mitigation efforts should enhance patient-provider communication, normalize routine inquiry about CAM use, and integrate CAM-related topics into standard healthcare interactions. Educational campaigns targeting healthcare providers and the public can support this process by encouraging disclosure and bridging knowledge gaps especially in contexts where concurrent use of CAM and conventional treatments is common. Notably, while 46% of participants acknowledged awareness of potential drug interactions, only a small proportion reported them, underscoring the need for healthcare providers to be equipped with the knowledge and tools necessary to screen for such risks.
In light of the regional findings, it is also critical to understand how these results align globally. Issues such as the popularity of specific herbs (eg, ginger, garlic, Curcuma longa) and the dominance of informal information sources should be understood within the broader challenges of misinformation and risk perception. The widespread reliance on family and internet-based information reflects vulnerabilities in health literacy and public health messaging. This underscores the importance of targeted, culturally informed public health campaigns, incorporating CAM content in health education curricula, and developing policy frameworks that ensure safe and informed CAM use—particularly during public health emergencies.
To strengthen the broader relevance of our findings, it is essential to situate the regulatory gaps observed in the GCC within the international context. For instance, several countries,21–23 such as Germany, Canada, and Australia, have established robust frameworks for regulating CAM, including licensing, quality control, and mandatory reporting of adverse effects. In contrast, most GCC countries still lack unified, enforceable policies governing CAM use, which may contribute to the continued reliance on informal information sources and unverified practices. Comparing the GCC’s fragmented oversight with global best practices highlights the urgent need for harmonized, evidence-based regulation. Drawing on international models may support the development of regionally adapted frameworks that ensure patient safety, regulate herbal product standards, and guide provider-patient discussions about CAM use.
In addition to descriptive findings, this study provides a platform for proposing region-specific, multi-level strategies tailored to the GCC’s healthcare and cultural context. While the popularity of herbal remedies and informal knowledge channels is well-known, the findings highlight the need for structured responses that align with GCC countries’ unique public health, regulatory, and social environments.
At the regulatory level, GCC nations should work toward unified guidelines for CAM regulation, including safety standards, product registration protocols, and post-market surveillance. A GCC-wide authority or collaborative framework could help address disparities in current regulatory practices, especially given the transnational movement of CAM products and shared cultural beliefs.
At the healthcare system level, incorporating CAM education into academic curricula for medical, pharmacy, and nursing students is essential. This would equip future professionals to handle CAM-related queries competently and promote safe, evidence-informed recommendations. Ministries of health should also develop and disseminate national clinical guidelines for evidence-based CAM use, developed in collaboration with regulatory bodies and academic institutions.
At the community level, public awareness campaigns should be customized to the GCC’s cultural context, engaging trusted societal figures such as religious leaders, family elders, and local influencers. These campaigns should use regionally popular digital platforms (eg, WhatsApp, Instagram, Snapchat) to disseminate scientifically sound, multilingual health content to reduce misinformation and improve health literacy.
Investment in government-supported research centers dedicated to CAM is vital at the research and policy level. These centers could focus on conducting local clinical trials, studying herb-drug interactions, and establishing national CAM databases. Moreover, inter-GCC collaboration would promote regulatory harmonization, shared research outputs, and coordinated responses to future public health challenges.
In summary, these multi-tiered, regionally grounded strategies address the key gaps identified in this study and move beyond generic recommendations. They offer practical solutions for safe and effective CAM integration rooted in the GCC’s social, cultural, and healthcare landscape. Coordinated efforts by ministries of health, academic institutions, and regulatory bodies will be essential to ensure that CAM practices contribute meaningfully to infection prevention and broader public health outcomes in the region.
Limitations and Suggestions for Future Research
While this study offers valuable insights into using CAM in the GCC region, several limitations should be acknowledged. First, cross-sectional design limits the ability to establish causal relationships and may introduce information bias. The reliance on self-reported data could also affect the accuracy of responses due to recall or social desirability bias. Additionally, convenience sampling supplemented by snowballing may have introduced selection bias, limiting the generalizability of the findings to the broader GCC population. Although the target sample size was 385, only 340 participants completed the questionnaire. This shortfall may have reduced statistical power for subgroup analyses and increased the risk of Type II error. Notably, because only CAM users (n = 340) completed the whole questionnaire, non-users (n = 407) were excluded after initial screening, and demographic and health data were not collected from this group. This restricted our ability to conduct logistic regression or other multivariate analyses to identify independent predictors of CAM use and adjust for potential confounding variables. Future research should adopt longitudinal designs, include a more diverse age distribution, and collect complete data from users and non-users to enable more comprehensive and comparative modeling of CAM use predictors.
Conclusion
This study provides important insights into the widespread use and public perceptions of CAM for infection prevention in the GCC region. Although it does not evaluate CAM’s clinical efficacy or safety, it identifies key usage patterns and demographic influences, particularly the roles of education and prior illness. The reliance on informal sources and limited consultation with healthcare providers highlights health literacy and regulation gaps. These findings call for culturally appropriate, evidence-informed public health strategies, better communication in clinical settings, and future research on the safety and effectiveness of commonly used CAM therapies.
Acknowledgments
We express our gratitude to everyone who participated in this study.
Funding
This is an unfunded project. The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares that there are no conflicts of interest, financial or otherwise, that could have influenced the outcomes or interpretations presented.
References
1. Singh AK, Gillies CL, Singh R, et al. Prevalence of co-morbidities and their association with mortality in patients with COVID-19: a systematic review and meta-analysis. Diabetes Obes Metab. 2020;22(10):1915–1924. doi:10.1111/dom.14124
2. Honorato-Cia C, Cacho-Asenjo E, Martinez-Simon A, Aquerreta I, Núñez-Córdoba JM. Long COVID research, 2020–2024: a PubMed-based bibliometric analysis. Healthcare. 2025;13(3):298. doi:10.3390/healthcare13030298
3. AlNajrany SM, Asiri Y, Sales I, AlRuthia Y. The commonly utilized natural products during the covid-19 pandemic in Saudi Arabia: a cross-sectional online survey. Int J Environ Res Public Health. 2021;18(9):4688. doi:10.3390/ijerph18094688
4. Alyami HS, Orabi MAA, Aldhabbah FM, et al. Knowledge about COVID-19 and beliefs about and use of herbal products during the COVID-19 pandemic: a cross- sectional study in Saudi Arabia. Saudi Pharm J. 2020;28(11):1326–1332. doi:10.1016/j.jsps.2020
5. Moquin B, Blackman MR, Mitty E, Flores S. Complementary and alternative medicine (CAM). Geriatr Nurs. 2009;30(3):196–203. doi:10.1016/j.gerinurse.2009.03.002
6. Steel A, Gallego-Perez DF, Ijaz N, et al. Integration of traditional complementary and integrative medicine in the institutionalization of evidence-informed decision-making the world health organization meeting report. J Integr Complement Med. 2025;31(4):388–394. doi:10.1089/jicm.2024.0837
7. World health organization (WHO) [Online]. Coronavirus disease (COVID-19) advice for the public: mythbusters. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters.
8. Lin J, Huang G, Su Y. Efficacy analysis and research progress of complementary and alternative medicines in the adjuvant treatment of COVID-19. J Biomed Sci. 2023;30(1):30. doi:10.1186/s12929-023-00923-5
9. Jeremy Y. Global research trends at the intersection of coronavirus disease 2019 (COVID-19) and traditional, integrative, complementary, and alternative medicine: a bibliometric analysis. BMC Complement Med Ther. 2020;20(1):353. doi:10.1186/s12906-020-03151-8
10. Mahish PK, Mahobia R, Yadav J. Use and awareness of herbal medicine among literate population. Int J Pharma Bio Sci. 2016;7(4):174–178. doi:10.22376/ijpbs.2016.7.4.p174-178
11. Ang L, Lee HW, Choi JY, Zhang J, Lee MS. Herbal medicine and pattern identification for treating COVID-19: a rapid review of guidelines. Integr Med Res. 2020;9(2):100407. doi:10.1016/j.imr.2020.100407.08.023
12. Djuv A, Nilsen OG, Steinsbekk A. The co-use of conventional drugs and herbs among patients in Norwegian general practice: a cross-sectional study. BMC Complement Altern Med. 2013;13:295. doi:10.1186/1472-6882-13-295
13. Charan J, Bhardwaj P, Dutta S, et al. Use of complementary and alternative medicine (CAM) and home remedies by COVID-19 patients: a telephonic survey. Indian J Clin Biochem. 2021;36(1):108–111. doi:10.1007/s12291-020-00931-4
14. Aljofan M, Alkhamaiseh S. Prevalence and factors influencing use of herbal medicines during pregnancy in hail, Saudi Arabia: a cross-sectional study. Sultan Qaboos Univ Med J. 2020;20(1):71–76. doi:10.18295/squmj.2020.20.01.010
15. Challenger A, Sumner P, Bott L. COVID-19 myth-busting: an experimental study. BMC Public Health. 2022;22(1):131. doi:10.1186/s12889-021-12464-3
16. Alotiby AA, Al-Harbi LN. Prevalence of using herbs and natural products as a protective measure during the COVID-19 pandemic among the Saudi population: an online cross-sectional survey. Saudi Pharm J. 2021;29(5):410–417. doi:10.1016/j.jsps.2021.04.001
17. Raosoft Sample Size Calculator. [online]. Available from: http://www.raosoft.com/samplesize.html.
18. News of Bahrain [online]. GCC population surges by 4 million in two years. 2023. Available from: https://www.newsofbahrain.com/bahrain/101373.html?utm_source=chatgpt.com.
19. Ahmed I, Hasan M, Akter R, et al. Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: a cross-sectional study. PLoS One. 2020;15(12):e0243706. doi:10.1371/journal.pone.0243706
20. Kretchy IA, Boadu JA, Kretchy J, et al. Utilization of complementary and alternative medicine for the prevention of COVID-19 infection in Ghana: a national cross-sectional online survey. Prev Med Rep. 2021;24:101633. doi:10.1016/j.pmedr.2021.101633
21. World Health Organization (WHO) [Online]. WHO global report on traditional and complementary medicine 2019. Available from: https://www.who.int/publications/i/item/978924151536.
22. Therapeutic Goods Administration (TGA) [Online]. Complementary medicines regulation in Australia. Australian government department of health and aged care 2022. Available from: https://www.tga.gov.au/complementary-medicines.
23. Health Canada. Canadians’ views and use of natural health products, non-prescription drugs and health products containing cannabidiol: findings report. Ottawa: Health Canada; 2024. Available from: https://epe.lac-bac.gc.ca/100/200/301/pwgsc-tpsgc/por-ef/health/2024/059-23-e/POR059-23-report.html?utm_source=chatgpt.com.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.