")
Back to Journals » International Journal of Nanomedicine » Volume 20
Mesenchymal Stromal Cell-Derived Extracellular Vesicles in the Management of Atopic Dermatitis: A Scoping Review of Therapeutic Opportunities and Challenges
Authors Al-Masawa ME , Elfawy LA, Ng CY , Ng MH , Law JX
Received 9 September 2024
Accepted for publication 31 January 2025
Published 4 March 2025 Volume 2025:20 Pages 2673—2693
DOI https://doi.org/10.2147/IJN.S494574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. RDK Misra
Maimonah Eissa Al-Masawa, Loai A Elfawy, Chiew Yong Ng, Min Hwei Ng, Jia Xian Law
Department of Tissue Engineering and Regenerative Medicine, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
Correspondence: Jia Xian Law, Department of Tissue Engineering and Regenerative Medicine, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia, Email [email protected]
Abstract: Atopic dermatitis (AD) is a global concern marked by inflammation, skin barrier dysfunction, and immune dysregulation. Current treatments primarily address symptoms without offering a cure, underscoring the need for innovative therapeutic approaches. Mesenchymal stromal cell-derived extracellular vesicles (MSC-EVs) have attracted attention for their potential in immunomodulation and tissue repair, similar to their parent cells. This review provides a comprehensive analysis of the current landscape of MSC-EV research for AD management. We identified 12 studies that met our predefined inclusion criteria. We thoroughly reviewed both human and animal studies, analyzing aspects such as the source, isolation, and characterization of MSC-EVs, as well as the animal and disease models, dosage strategies, efficacy, mechanisms, and adverse effects. While this review highlights the promising potential of MSC-EV therapy for AD, it also emphasizes significant challenges, including heterogeneity and insufficient reporting. Given that this research area is still in its early stages, addressing these uncertainties will require collaborative efforts among researchers, regulatory bodies, and international societies to advance the field and improve patient outcomes.
Keywords: exosome, eczema, atopic eczema, mesenchymal stem cells, cell-free therapy
Graphical Abstract:

Introduction
Atopic dermatitis (AD) is a chronic relapsing inflammatory dermal disorder of a complex multifactorial etiology involving several hereditary, immunologic, and environmental factors.1 AD, ranks among the most frequently diagnosed conditions by dermatologists worldwide. Globally, the number of prevalent pediatric AD cases grew by 5.7 million, while incident cases rose by 0.7 million between 1990 and 2019.2 Although AD typically manifests in early childhood and can persist into adulthood, about one-quarter of cases involve adult-onset AD.3 AD prevalence in adults ranges from 2.1% to 4.9%, with a rising trend each year.4 Moderate-to-severe AD leads to considerable financial costs and significantly diminishes the quality of life.5
AD cure is far an unmet medical need. Classical treatment for AD focuses on controlling long-term disease, preventing recurrence, symptomatic relief, and anti-inflammatory therapy.6 Immunosuppressive topical corticosteroids are the first-line medication in soothing acute flares.7 Topical emollients are recommended to be used to improve skin barrier function.8 To prevent recurrence, corticosteroids are used with topical calcineurin inhibitors (TCIs), to hamper the activation of T cells. In moderate-to-severe cases, systemic immunosuppressants are used. However, these could only be taken for short term due to severe adverse effects.8–10 Recently, there is an increased interest in developing targeted therapies for AD based on the latest understanding of the complex nature of AD pathogenesis. The use of biologics holds a great promise to treat AD. Dupilumab has been approved by the FDA in 2017, as an effective biologic agent in AD,11 in addition to the recent JAK-STAT inhibitors.12 Yet, further studies should be done to establish the long-term safety of such biologics.
On the other hand, propelling evidence from preclinical and clinical studies has shown that mesenchymal stromal cells (MSCs) are effective immunomodulators in a number of inflammatory diseases, including AD.13 However, several challenges have hindered MSC therapeutic effectiveness, including low engraftment efficiency, non-specific differentiation, potential tumor or embolism risk, short half-life, and challenges in quality control.14 Interest in EV therapy began to surge following key discoveries in the mid-2000s. Researchers demonstrated that EVs could transfer functional nucleic acids between cells.15–17 This growing interest was amplified by the parallel rise in stem cell research, particularly around MSC-EVs in 2009,18 demonstrating efficacy for treating acute myocardial infarction,19 highlighting EV potential in therapeutic applications.
EVs offer several advantages over MSCs in therapy. EVs can replicate MSC therapeutic effects through paracrine signaling without requiring cell engraftment. Unlike MSCs, EVs are nanosized and carry therapeutic factors such as lipids, miRNAs, and growth factors within a protective lipid bilayer. This protection enhances their stability and efficacy over extended periods and distances.20 EVs do not replicate and can be produced in larger quantities and sterilized through filtration, enabling a standardized, ready-to-use ”off-the-shelf” regenerative therapy, avoiding issues related to cell viability, high production costs, and batch variability, thus offering a safer, alternative for cell therapy.21,22 Additionally, EVs can cross physiological barriers like the blood–brain barrier.23 Thus, EVs present a promising, more practical cell-free approach that capitalizes on the therapeutic benefits of MSCs while addressing many of the challenges associated with whole-cell therapies.
MSC-EV therapy has been investigated in preclinical studies for a wide range of conditions, including intervertebral disc degeneration, cardiac, hepatic, respiratory, diabetic, wound healing, and inflammatory skin diseases.21,24 These studies provided proof of concept, demonstrating the potential of EV-based therapies across a variety of diseases. Early clinical investigations showed that the therapeutic use of MSC-EVs was safe and effective in a patient with refractory graft-versus-host disease.25 However, the progress of EVs to clinical application has been slow.26
The use of MSC-EVs in AD management is still in its infancy. This study offers an overview of the work investigating MSC-EVs effectiveness in the management of AD, whether as the primary treatment or as an adjunct therapy, mapping both animal and clinical studies on the topic. We examined the methods used for MSC-EV production, source selection, dosage regimens, and outcomes. Additionally, we explored the models studied and the challenges encountered that may hinder clinical translation.
Methods
We conducted a scoping review on the use of MSC-EVs in treating AD. This scoping review was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.27
We opted for a scoping review rather than a systematic review because this research area is still in its early stages. Our goal was to include all articles and map all relevant studies without the stringent inclusion criteria required by a systematic review approach. Yet, we conducted a systematic electronic search to comprehensively gather related studies, minimizing bias often present in narrative reviews. Our electronic search was conducted on March 29, 2024, including PubMed and Web of Science databases to identify relevant articles up to the end of March 2023, using the following keywords:
(atopic dermatitis OR eczema OR skin inflammation) AND (exosome* OR extracellular vesicle* OR microparticle OR nanovesicles OR secretome OR conditioned media OR derivatives) AND (mesenchymal stem cell* OR mesenchymal stromal cell*).
Articles were imported to EndNote software (Version 20.5, https://endnote.com/), and duplicate articles were removed. Subsequently, articles were screened by reading titles and abstracts. At this stage, the inclusion criteria specified the inclusion of articles that investigate MSC-EV therapy for AD in animal or human studies, which include peer-reviewed original articles, case studies, letters, and reports. We excluded conference abstracts, reviews, non-peer reviewed articles (including pre-prints), and non-EV- or AD-related studies. The second stage of screening was carried out by reading the full text. At this stage, only studies that used MSC-EVs for treatment of AD, either as a primary or adjunct therapy in animals and humans, were included. No limitations were imposed on the date of the study, language, EV size, or characterization criteria. Study screening was carried out by two reviewers independently (M.E.A., J.X.L). Disagreements were addressed through discussion with the third reviewer (A.M.H.N). For the qualitative analysis of the selected studies, information was collected from texts, tables, figures, supplementary materials, and organized in pre-prepared tables. Data collected included author name, country and year, funding, source of EVs, isolation techniques, storage method, characterization results and techniques, subject characteristics including age, sex, species, AD disease model, disease manifestation (symptoms of disease reported), sample size, dosage regimen including EV dose vs control dose (weight/vol), route of administration, frequency and treatment duration, outcomes, side effects, proposed mechanism of action, biodistribution or tracking of EVs, limitations of the studies, and final conclusion. We then checked the ongoing clinical trials on https://clinicaltrials.gov (accessed on 06 September 2024). This search was conducted using the same keywords as in the previous search.
Results
Search results
A search on the Web of Science and PubMed yielded 594 articles (PubMed = 347, WOS = 247). After removing 135 duplicates, 459 articles were screened by reading titles and abstracts, leading to the exclusion of 429 articles. Of the remaining 30 articles, 12 met the eligibility criteria and were included in the study. The study selection process is outlined in the flow chart shown in Figure 1.
 |
Figure 1 Flow diagram summarizing the study selection process based on the PRISMA guidelines. The diagram demonstrates the number of records identified through database searches, the number of duplicates removed, records screened, full-text articles assessed for eligibility, and studies included in the scoping review. Reasons for exclusion of articles at each stage are detailed in the diagram. The final selection comprises studies meeting the predefined inclusion criteria. |
Overview of Included Studies
The studies included were published between 2018 and 2024, involving ten animal studies14,28–36 and two focusing on human cases.37,38 Of these, two were conducted in China,30,32 while the other ten were carried out in Korea. Funding sources varied: six studies received government agency funding, four were funded by industry, one study was partially supported by the government, and one study did not receive any external grants.
MSC-EV Source
The studies investigated different sources for MSC-EVs. Of the twelve included studies, adipose tissue-derived MSCs (ASC) constituted the majority, with 58% (n=7). Two studies examined iPSC-derived MSCs, and two umbilical cord-derived MSCs (UC-MSC) (16.7%). Gingiva-derived MSCs (GMSC) accounted for 8.3% (n=1) of the sources examined. Naïve MSC-EVs were the most prevalent at 58.3% (n=7). Engineered EVs were also investigated, including those created by fusing grapefruit-derived nanovesicles encapsulated with CX5461 and with CCR6+ nanovesicles from engineered gingiva-derived MSC membranes, to produce hybrid nanovesicles FV-CX5461.30 Other engineering methods involved genetically modifying the source MSCs to produce SOD3 through lentiviral transfection.36 Studies also explored preconditioning MSCs (iPSC-MSC) with interferon gamma (IFN-γ) for 24 hours before EV isolation, encompassing 16.7% (n=2) of the studies.31,33 The studies predominantly utilized xenogenic and allogenic cells. Notably, the clinical studies used naïve allogenic ASCs as the source for EVs.37,38
MSC Characterization
To standardize studies of MSCs, the International Society for Cell and Gene Therapy (ISCT) has set minimal criteria for their characterization and identification.39 According to these criteria, MSCs should 1) adhere to plastic; 2) express CD105, CD73, and CD90, and do not express CD45, CD34, CD14 or CD11b, CD79a or CD19, and HLA-DR; and 3) demonstrate in vitro multi-lineage differentiation into osteogenic, adipogenic, and chondrogenic lineages under specific culture conditions. Of the studies reviewed, five (41.7%) did not report how MSCs were characterized, six (50%) met ISCT criteria, and one (8.3%) identified CD markers but did not cover the other criteria aspects. Furthermore, studies that manipulated MSC sources further characterized MSCs by confirming changes in the cells before EV isolation. For instance, studies preconditioned with IFN-γ checked for indoleamine 2.3-dioxygenase 1 (IDO1) gene expression and protein abundance as markers for successful preconditioning.31,33 IDO is an important immunoregulatory protein triggered by IFN-γ in preconditioned MSCs. However, it was unclear if IDO was present in the isolated EVs. When comparing preconditioned and naïve MSCs, no difference was observed in the expression of the MSC identification markers, both the positive and negative. Additionally, examination of engineered SOD3-MSC revealed that lentiviral transduction and overexpression of SOD3 enhanced MSC proliferation without affecting their capacity for trilineage differentiation, surface marker expression, or chromosomal stability.36 However, it increased the levels of galectins, ALCAM, B7-H1, Fas ligand, ALCAM, B7-H1, Fas ligand, IL-8, IL-6, thrombospondin (TSP)-1, and tissue inhibitor of metalloproteinase (TIMP)-2 involved in immunomodulation activity of MSCs.36
MSC-EV Enrichment and Characterization
All examined studies isolated EVs from cultured cells and collected conditioned media for EV enrichment, which was serum free (n=5) or supplemented with EV depleted FBS (n=3). A combination of enrichment methods was used by all studies (n=12). Interestingly, half of the studies (including the two clinical studies) employed 0.22 µm filtration and tangential flow filtration (TFF, n=7, 58%).14,28,29,34,35,37,38 TFF pore size used varied between 300 and 500 kDa. Ultracentrifugation was the second most frequently used enrichment method, used by 3 studies (25%),31,33,36 and precipitation kits used by one (8.3%).32 Huang et al (2023) employed a more complex method to prepare synthetic EVs derived from gingiva-derived MSCs. Grapefruits were blended, filtered, and subjected to differential ultracentrifugation and a sucrose gradient to obtain GEVs. CCR6-GMSCs were ground, centrifuged, and filtered to produce CCR6-GMSC-NVs. The GEVs were then loaded with CX5461 via electroporation, and finally, the CX5461-GEVs were extruded with CCR6-GMSC-NVs through a 0.22 µm filter to form the synthetic EVs.30
EV characterization is necessary to estimate the quantity of EVs, establish their presence, and evaluate the contributions of non-EV components to the observed function. The Minimal information for studies of extracellular vesicles MISEV2023 and MISEV2018 propose that the abundance of EVs be estimated by evaluating particle number, protein, and/or lipid content, visualizing EVs, as well as identifying EV markers and non-vesicular components.40,41 Pre-analytical parameter reporting, including the number of secreting cells, volume of biofluid, and mass of tissue, should also be considered. In the analyzed studies, a number of characterization procedures were employed (Table 1). Size distribution was analyzed by nanoparticle tracking analysis (NTA) (n=10). Two studies did not report the size or size distribution.32,36 Particle number was not reported in all the studies except one.29 Dynamic light scattering (DLS) used in two studies in combination with NTA.30,33 All studies reported EVs size under 200 nm, highlighting a focus on the small EVs category. Transmission electron microscopy (TEM) was used to visualize EVs in four studies and CryoTEM in three studies. Five studies did not report visualizing EVs. Protein quantification was not reported in all the studies except one.29 EV-specific markers were examined by Western blot only in four studies, and flow cytometry only in one study, or both in six studies. Only seven studies identified both positive cytosolic and surface markers in addition to negative EV markers fulfilling MISEV2023 criteria (Table 1). 14,30,31,33,34,37,38 A single study assessed the lipidomic profile of MSC-EVs.14 Global profiling of EV proteins14,33 or miRNA29 was also reported.
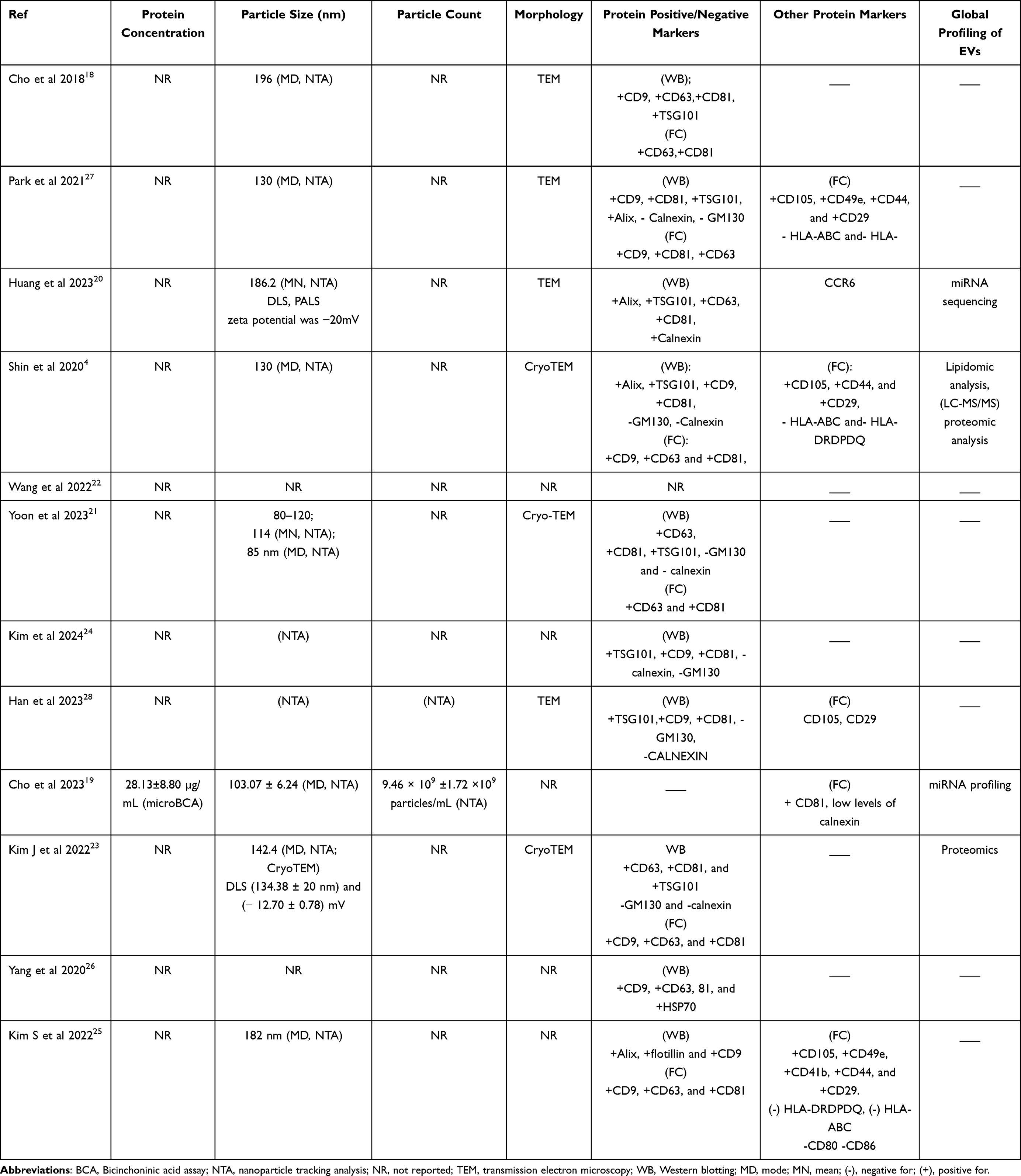 |
Table 1 Summary of MSC-EV Characterization Findings |
Animal Studies
Animal Characteristics
A variety of animal models were used to investigate EV therapeutic potential in AD,14,28–36 Table 2. NC/Nga mice were used in three studies,28,29,33 Additionally, BALB/c mice were included in four studies,30,31,35,36 while SKH-1 mice were used in a single study.14 One study did not specify the mice strain used.32 Apart from rodents, one study involved canine models.34 Regarding sex distribution, eight studies involved male subjects,28–30,32–36 and two studies included female subjects.14,31
 |
Table 2 Summary of Animal Studies |
Disease Model
Heterogenous protocols have been employed to induce AD in animal models across the evaluated studies. Five studies induced AD using 2.4-dinitrochlorobenzene (DNCB).30,32,33,35,36 Another three studies used Dermatophagoides farinae for AD induction.28,29,34 One study utilized Aspergillus fumigatus,31 while another applied oxazolone.14 AD induction methods varied considerably, with durations ranging from two weeks to seven weeks across these studies, Table 2.
Dosage Regimens
Diverse EV dose regimens have been shown by the examined studies, Table 2. The most common method of administration was subcutaneous injection (n=7), followed by intravenous injection (n=3) and topical application (n=2). Of these, one study compared IV administration of EVs and SC,28 and another compared SC with topical administration of EVs.31 Both studies reported no significant difference between the different methods of applications on AD amelioration. To note, for studies that subcutaneously injected EVs, it was not clear if this involved multiple sites or a single-site injection. Additionally, the doses used varied considerably among the studies (0.14–500 µg), and the basis for dose selection was not identified. For instance, studies administered EVs by IV, at a dose of 20 mg/kg@2 mg/kg;30 0.14, 1.4, and 10 μg per animal;28 1.5 mL of canine EVs (5 × 1010) or human EVs (7.5 × 10¹¹),34 respectively. Studies applied EVs by SC injections used doses of 0.14, 1.4, and 10 μg per animal;28 1, 3, and 10 μg per animal;14 25 μg;31 1.00 × 109, 3.33 × 109, and 1.00 × 1010 /mL;29 and 50 or 500 μg.33 In the topical application studies, Wang et al32 applied EVs at concentrations of 15 and 60 μg/mL, while Yoon et al31 administered a single topical dose of 25 μg in a moderate AD model, while in a severe model, they applied lower doses of 2.5 μg and 0.25 μg. Interestingly, all studies quantified the dose based on protein concentration except for three studies that used particle concentration.29,34,35 Also, frequency and number of doses applied differed among studies. Cho et al28 administered three times a week for four weeks totaling 12 injections (SC and IV); Kim J. et al33 SC injected once a week for five weeks. In contrast, Huang et al30 administered three dosages for a week. Shin et al14 applied three doses each week for four weeks. Wang et al32 applied EVs twice a day for seven days. Yoon et al31 injected EVs once, while Kim et al34 injected three times a week for four weeks. A single SC injection on the seventh day was administered by Yang et al.36 This collectively reflects the heterogeneous approaches employed in designing protocols for AD treatment by MSC-EVs.
Efficacy of EV Therapy in Ameliorating AD Symptoms in Animal Models
There was an overall improvement in AD animals treated with MSC-EVs, regardless of source and dosage regimens; dose, method of administration, frequency, and duration of application, Table 2. The studies that used naïve, IFN-γ preconditioned and engineered MSC-EVs reported improved AD scores as a result of improved erythema/hemorrhage, edema, excoriation/erosion, lichenification, and scaling/dryness.14,28–36 Histopathological analysis also revealed reduction in epidermal thickness14, 28–36 as well as reduced immune cell infiltration, including mast cells,14,29–31,33,35,36 eosinophils,28,31 neutrophils,31 or lymphocytes in general.31–33 A study reported a reduction in eosinophils but not in neutrophil or other WBCs infiltration in the skin of treated AD animals.28 Improved trans-epidermal water loss (TEWL) and improved levels of skin hydration14,31,33,34 were also reported.
Inflammatory cytokine levels were suppressed in response to MSC-EV treatment such as IL-2,34 IL-4,14,28,34 IL-5,14 IL-12,34 IL-13,14,34 IL-17,14 IL-31,28,34 IL-23,28 IL-1β,30 IFN-γ,14,29,34 thymic stromal lymphopoietin (TSLP),14,29,33,34 and TNF-α,14,28,30 similar to prednisolone.28 Serum IgE level reduction was reported in several studies as well.14,28,35
Moreover, EV therapy exhibited anti-pruritic effects, as shown by Kim et al (2024), who noted a decrease in IL-31 levels, a potent pruritogenic cytokine, providing relief from itching, a common symptom of AD.34 This alleviation was proposed to result from reduced IL-31/TRPA1-mediated pruritus and decreased activation of JAK/STAT signaling pathway.35 Additionally, IL-31Rα, OSMRβ, and their downstream signaling molecules (STAT1/5) were suppressed, which also contributed to the reduction in pruritic symptoms.33
Huang et al30 reported a reduction in spleen weight and a decreased percentage of Th17 and Th 2 cells within the CD4+ T cell population in the spleen, accompanied by a decline in the overall number of CD4+ T cells. They also observed an increase in CD4+CD25+Foxp3+ regulatory T cells (Tregs), in response to their engineered MSC-EVs. Additionally, there was a downregulation of CCL20 expression and reduced ROS levels in AD lesions.30 Additionally, increased anti-inflammatory cytokines such IL-10 and transforming growth factor-β were also reported.34 Interestingly, Kim et al34 found that MSC-EV therapy could notably enhance the diversity of the skin microbial population, as evidenced by an increase in operational taxonomic units (OTUs) and alpha diversity indices following treatment. This indicates MSC-EV therapy may counteract skin dysbiosis common in AD skin. Additionally, Shin et al14 examined the MSC-EV effect on epidermal lipids and reported enhanced expression of epidermal ceramides and dihydroceramides. This improvement was attributed to the induced production of lamellar layers at the junction between the stratum granulosum and the stratum corneum,14 also to the improved production of lipid synthesis-associated proteins such as serine palmitoyltransferase, HMG-CoA reductase, ceramide synthase 3 (CerS3), and ceramide synthase 4 (CerS4).33
Dose-dependent improvement was reported in all studies that tried different doses. Cho et al28 found that higher dose of 10 μg per animal was more effective than lower doses of 0.14 μg and 1.4 μg. Shin et al14 showed that 10 μg per animal yielded better results than 1 μg and 3 μg doses. Yoon et al,31 in a mild AD model, noted that topical application and SC injection at 25 μg were more effective, whereas in a severe AD model, 2.5 μg, topically applied, was more beneficial than 0.25 μg. Cho et al29 found better results with the highest particle concentration of 1.00 × 1010 particles/mL compared with 1.00 × 109 and 3.33 × 109 particles/mL. Additionally, Kim et al33 reported that SC injections of 500 μg of IFN-γ-iMSC-EVs were more effective than 50 μg. Conversely, Wang et al32 reported comparable improvement when using a higher concentration of 60 μg/mL MSC-EVs in contrast to 15 μg/mL. The observed improvement level was also equivalent to that achieved with the positive control, dexamethasone.32
Interestingly, both xenogeneic (human embryonic cell line derived EVs) and allogenic (canine adipose MSC derived EVs) were well tolerated in a canine AD model, and had a similar effect in ameliorating AD.34 To note, a higher dose was used for the xenogenic EVs: 7.5 × 10¹¹ EVs compared to 5 × 1010 EVs for allogenic canine EVs. The authors suggested that further investigation is necessary.
Adverse Effect Assessment
Safety assessment of MSC-EVs was not sufficiently investigated across the various studies. Cho et al28 and Kim J et al33 reported no side effects from EV treatment. Huang et al30 found no significant changes in body weight, organ structure, or tissue histology of the heart, liver, spleen, lung and kidney, or blood parameters in AD mice treated with different engineered MSC-EV formulations, demonstrating high biocompatibility. Similarly, Shin et al14 observed that ASC-EVs did not affect animal weight, unlike dexamethasone, which led to weight loss. Yoon et al31 noted that highly concentrated IFN-γ-iExo did not cause hypersensitivity responses in AD mice and resulted in clinical and histological outcomes equivalent to dexamethasone. Kim et al34 also reported no adverse events or anaphylaxis associated with IV administration of EV treatment.
In a detailed toxicity study, Cho et al29 assessed the safety of canine ASC-EVs (cASC-EVs) in both male and female ICR mice through single dose, and twenty-eight-day multiple-dose toxicity studies. In the single-dose toxicity study, ICR mice received doses of 7.45 × 108 (low dose), 2.98 × 109 (medium dose), and 1.19 × 1010 (high dose) particles/20 g. No animal deaths or adverse symptoms were detected. Although some animals experienced temporary weight loss, this was not statistically significant and had no toxicological implications. Necropsy assessment revealed no gross abnormalities, and the estimated lethal dose of ASC-EVs was determined to be 1.19 × 1010 particles/20 g or more. In the 28-day repeated-dose toxicity study, cASC-EVs were SC injected at a low dose of 7.45 × 108, medium dose of 2.98 × 109, and high dose of 1.19 × 1010 particles/20 g three times a week for 4 weeks. No deaths occurred, and no changes were detected in clinical evaluations, body weight, eating or drinking habits, or urinalysis outcomes. Although some blood parameters showed significant differences, such as increases in eosinophil levels, and decreases in red blood cell, hemoglobin, and hematocrit levels, that varied between males and females, these differences were within the range of biological variations. Similarly, changes in blood biochemistry, such as decreased total protein and increased chloride in males and decreased sodium in females, did not have toxicological implications. Organ weight analysis revealed a statistically significant decrease in the relative ovary weight in females treated with the highest dose, but no notable histopathological changes were observed. Overall, no gross or microscopic abnormalities related to ASC-EV administration were noted in any of the treated animals. The study concluded that the NOAEL (no observed adverse effect level) for the used cASC-EVs was 1.19 × 1010 particles/20 g and supported their safety for therapeutic use. While this finding is promising, further studies are necessary to evaluate both the short- and long-term safety of MSC-EV therapies. Nevertheless, the available evidence supports the safety of MSC-EVs in treating AD, with no significant adverse effects reported in the studies.
Proposed Mechanism of Action
Immunomodulation
Immunomodulation is proposed to be the primary mechanism of action (MOA) for MSC-EVs in managing AD, involving both the innate and adaptive immune systems.28,35 This immunomodulatory activity has been evidenced by MSC-EV ability to reduce key pro-inflammatory mediators, such as IFN-γ, IL-2, IL-4, IL-12, IL-13, IL-31 and IgE, their receptors like IL-4Rα, IL-13Rα1, IL-31Rα, CD23, and FcεRI,33,35 as well as chemokines such as TARC and RANTES while increasing anti-inflammatory cytokines including IL-10 and TGFβ,34,35 resulting in reducing inflammation, including Th2-induced responses, and associated symptoms. Additionally, other studies demonstrated MSC-EV ability to inhibit the activation and infiltration of immune cells, specifically T-cells and mast cells.14,29,31,35
Proteomic analysis of EV-treated skin revealed that MSC-EVs act by regulating pathways involved in T cell differentiation, particularly affecting Th1, Th2, and Th17 cells, which are critical in AD development.31 The anti-pruritic effects of MSC-EVs were linked to their ability to decrease IL-31 levels, reduce IL-31/TRPA1-mediated pruritus, inhibit activation of the JAK/STAT signaling pathway, and suppress IL-31Rα, OSMRβ, and downstream signaling molecules (STAT1/5).33–35 Inhibition of JAK1 and STAT6 phosphorylation was shown to be involved in MSC-EV MOA in ameliorating AD.33 Moreover, MSC-EV inhibition of TSLP expression may affect the NF-κB pathway, resulting in its decreased activity.33
miRNAs within EVs are essential in mediating their therapeutic effects. However, there has been limited research on this aspect concerning EV therapy for AD. Cho et al29 analyzed 798 miRNAs, and found let-7a, let-7b, miR-21, let7f, miRNA125-b, miR-24, and miR-29a being particularly abundant in ASC-EVs. These miRNAs are known to exert anti-inflammatory effects by regulating proinflammatory responses and aiding in the resolution of inflammation. The gene targets of these miRNAs are involved in intrinsic apoptotic signaling and protein kinase activity, and JAK-STAT pathway, further contributing to their immunomodulatory and anti-inflammatory effects of MSC-EVs.29
Skin Regeneration and Barrier Repair
Evidence collected from the analyzed studies suggests that MSC-EV therapy acts by restoring skin barrier function, often compromised in AD by modulating epidermal cells, confirming MSC-EV pro-regenerative potential. MSC-EVs promoted the release of ceramides and the formation of lamellar layers at the stratum granulosum-stratum corneum interface, enhancing skin barrier integrity.14 High-throughput RNA sequencing revealed that ASC-EVs restored significantly altered gene expression in AD, particularly genes involved in keratinocyte differentiation, epidermis development, and lipid metabolism, such as ceramide synthesis and sphingolipid metabolism. MSC-EV treatment may increase sphingosine and sphingosine-1-phosphate (S1P) levels by activating sphingosine kinase (Sphk) 1 and reducing their breakdown through decreased S1P lyase (S1PL) activity. These changes restored the skin barrier.14 The study also noted the downregulation of genes upregulated in AD, including those involved in cell cycle and inflammation activation. This resulted in a reduction in TEWL, indicating improved skin barrier integrity.14,34 These findings were supported by the observed enrichment in pathways related to skin barrier development, such as keratinization and cornified envelope generation, in EV-treated skins.31 Additionally, EVs enhanced levels of epidermal differentiation proteins such as filaggrin, keratin 1, and keratin 10, facilitating skin barrier repair and regeneration.33,35
Microbiome Regulation
Microbiota dysbiosis, marked by reduced microbial diversity, is common in AD. Research on the impact of EV therapy on this aspect is limited. A single study reported that MSC-EV therapy increased microbial diversity in AD skin, suggesting a positive effect on microbiome dysbiosis.34 However, the mechanisms behind this effect need further investigation.
Biodistribution and EV Tracking
Understanding the biodistribution of therapeutic agents is key for assessing their efficacy and safety. Only two studies reported tracking MSC-EVs administered via IV30 and SC injections.33
In the first study, engineered hybrid nanovesicles FV@CX5461 were labelled with Cy5.5 and administered intravenously to mice with AD.30 Biodistribution was monitored at 3-, 8-, 24-, 32-, and 48-hours post-injection. The study showed that the FV@CX5461 nanovesicles were detectable as early as 3 hours post-injection, showing more targeted accumulation in skin tissues compared to nonhybrid nanovesicle control, indicating improved homing capability in areas of AD lesions. Despite the gradual decline in signal intensity, labelled vesicles remained detectable up to 48 hours post-injection.30
The second study conducted a biodistribution investigation with DiR-labeled IFN-γ-iMSC-EVs injected subcutaneously into AD mice.33 Using an in vivo imaging system, the tracking of IFN-γ-iMSC-EVs in the body and main internal organs was performed after 8 hours. The study demonstrated that IFN-γ-iMSC-EVs specifically accumulated in skin tissues, as indicated by the fluorescent imaging.33
However, none of the studies reported assessing MSC-EV penetration through various skin layers or the precise localization across these layers. Further investigation into these aspects would be crucial for understanding penetration capabilities and MOA of MSC-EVs in skin therapeutic applications.
Human Studies and Clinical Trials
Two studies were conducted on human subjects, Table 3. 37,38 These studies examined the potential of using allogenic human adipose tissue-derived MSC-EVs (ASC-EVs) topically, to alleviate facial redness caused by dupilumab in patients with severe AD. Both studies separated small ASC-EVs by TFF and characterized them accordingly.
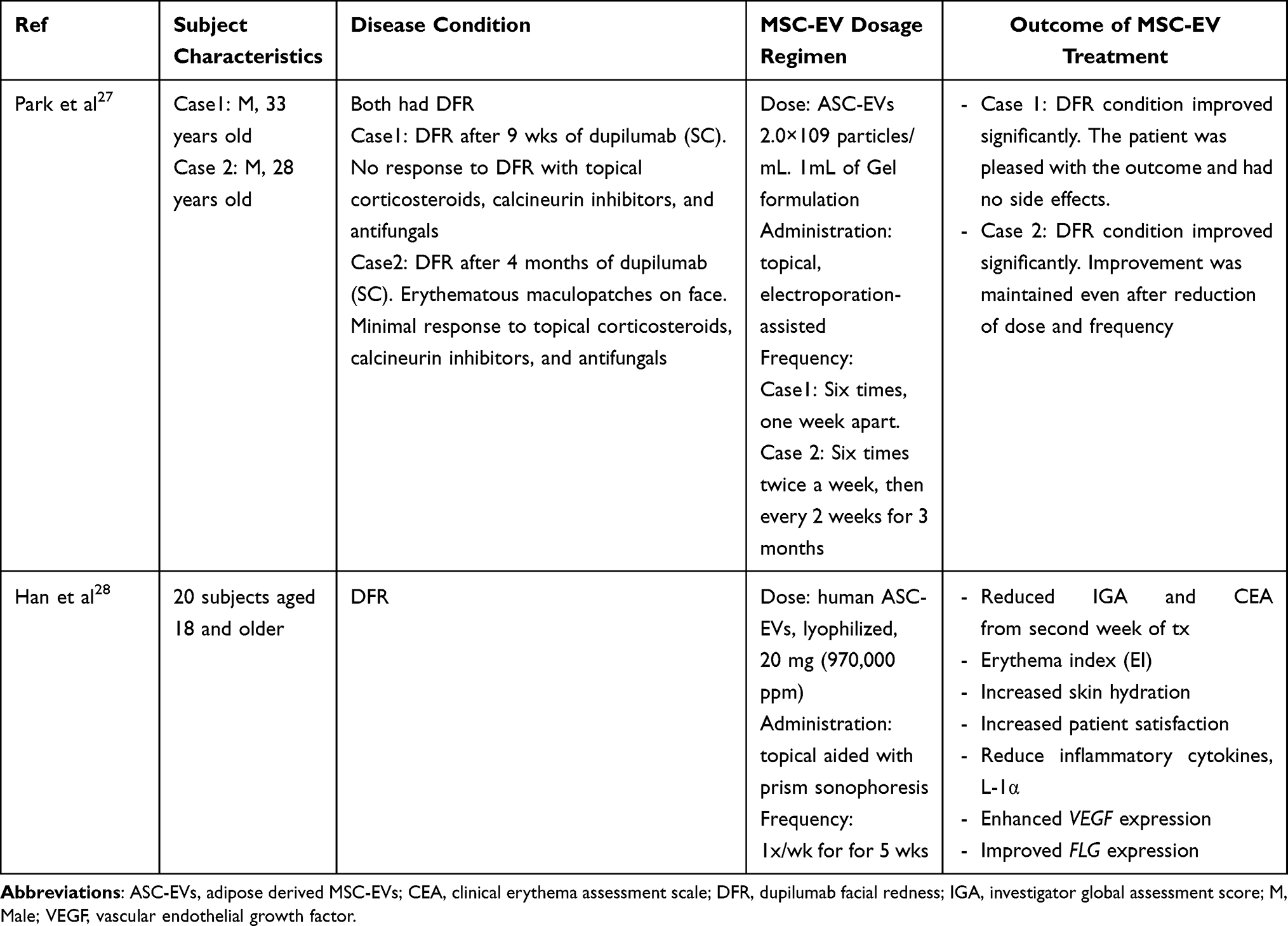 |
Table 3 Summary of Human Studies |
Park et al37 investigated the effects on two male subjects, aged 28 and 32 years old, who developed dupilumab facial redness (DFR) after dupilumab treatment. In Case 1, after 9 weeks of subcutaneous dupilumab treatment, a 33-year-old male with severe AD developed increased facial redness and scaling, which failed to respond to topical corticosteroids, calcineurin inhibitors, and antifungals. In Case 2, after 4 months of subcutaneous dupilumab treatment, a 28-year-old man with severe AD had an overall improvement in AD but developed increased erythematous maculopatches on his face, with minimal response to topical treatments. The treatment with ASC-EVs involved a dose of 2.0 × 109 particles/mL in a gel formulation containing 30% ASC-EVs, 2% 1.2-hexanediol, 1% glycerin, 0.6% ammonium acryloyldimethyltaurate/VP copolymer, 0.0045% L-arginine, and 66.3955% water, applied topically with electroporation assistance. In Case 1, the treatment was applied six times, once a week. In Case 2, the treatment was applied six times twice a week, then every two weeks for three months. Both cases showed significant improvement in DFR, with patients expressing satisfaction with the outcomes and no side effects reported. Case 2 maintained improvement even after reducing the dose and frequency of application.37
In Han et al38 study, twenty patients aged 18 and older, diagnosed with DFR, were treated with 20 mg (970,000 ppm) of lyophilized human ASC-EVs applied topically to the entire face. The treatment was followed by prism sonophoresis, creating ultrasonic waves to enhance the penetration of topical treatments into the skin. The ASC-EV therapy was administered once a week for five consecutive weeks, with follow-up lasting for eight weeks after the final ASC-EV treatment. The study reported that applying the ASC-EV topical formulation quickly resolved DFR symptoms, with improvements noted in Investigator Global Assessment (IGA) and Clinical Erythema Assessment (CEA) scores from the second week of treatment. The erythema scores decreased more rapidly than other DFR symptoms, such as papulation or infiltration. The erythema index also showed significant improvement. However, the average satisfaction index was highest in week 2 and gradually decreased thereafter, most likely because patients noticed significant changes after the initial treatment sessions but became less responsive to further improvements over time. The study also reported that ASC-EV treatment improved stratum corneum levels of epidermal proteins FLG and VEGF while reducing inflammatory cytokines IL-1α and TSLP.38
To get a comprehensive overview of the current state of AD therapy research involving MSC-EVs, we searched ClinicalTrials.gov database for ongoing trials. However, no relevant studies were identified.
Discussion and Future Perspective
This review provides a comprehensive analysis of the current landscape of MSC-EV research, in the context of AD treatment. Our search strategy identified 12 studies on MSC-EV therapy for AD, covering both human and animal models. The studies identified were primarily from East Asia, particularly Korea and China. The funding sources for these studies were diverse, ranging from government agencies to industry, reflecting a broad interest in the therapeutic potential of MSC-EVs for AD across different sectors in those regions.
Interestingly, there was greater interest in adipose-derived MSCs (ASCs) as the source of EVs, by over half of the studies, while only a few studies explored MSCs from umbilical cords and iPSCs. Other sources, such as bone marrow, amniotic fluid, or umbilical cord blood, were not investigated. Although it is too early to draw definitive conclusions due to the evolving nature of this research area, similar observations have been noted regarding the use of ASCs in AD cell therapy.13 ASCs were popular for AD treatment because of their accessibility, established safety profile, minimal ethical concerns, and immunomodulatory and regenerative effects.13 However, further studies are needed to explore alternative sources and compare their efficacy to identify the optimal choice for AD therapy.
Naïve MSCs were the primary choice for EV isolation, but there were also some attempts to boost EV therapeutic potential through genetic modifications or inflammatory preconditioning. These modifications have been shown to affect the composition and functionality of the resulting EVs. An interesting approach involved creating a hybrid of plant-derived exosome-like nanovesicles, which are effective antioxidants and drug carriers but have limited immunomodulatory and targeting potential, with MSC membranes engineered to overexpress the chemoattractant CCR6, targeting CCL20 in AD. The hybrid was also encapsulated with CX5461, an immunosuppressant and anti-proliferative agent. This created hybrid vesicles that leverage the advantages of all components and show enhanced efficacy and safety in the preclinical testing.30 Considering minimally manipulated sources may facilitate easier regulatory approval, it is crucial to weigh the pros and cons of each approach and explore various ways to enhance the efficacy of EVs.
Interestingly, small EVs were predominantly used in the studies. Studies used a combination of isolation methods and washing steps to enhance isolate purity. While ultracentrifugation has traditionally been the dominant method for isolating EVs for wound healing and skin regeneration interventions,24 it was interesting to find that TFF has become the preferred technique for concentrating and purifying MSC-EVs for AD therapy. Growing interest in TFF is due to its capacity to handle large volumes and scalability to produce clinical grade EVs.42,43 This technique is favored over centrifugal ultrafiltration or ultracentrifugation because it applies less force and pressure on EVs, minimizing stress and aggregation,44,45 hence, improving EV yield and potency.42,46
Guidelines such as MISEV2023 and the ISCT criteria play a critical role in ensuring the quality of research.39,41 MISEV2023 provides detailed recommendations to improve EV isolation, characterization, and methodological reporting, while the ISCT guidelines specifically outline criteria for identifying the MSCs. The primary aim of these guidelines is to promote rigor, transparency, and comparability, and facilitate successful clinical application of EV-based therapies.24,26 However, our study found that these guidelines were not consistently followed. For instance, many studies failed to fully adhere to ISCT’s identification criteria for MSC sources, and inconsistencies were common in the reporting of essential EV characterization parameters, such as protein concentration, particle number, and protein markers. More consistent adherence to the guidelines will be key to advancing the clinical potential of EV-based therapies. Moreover, establishing high purity of MSC-EV preparations is essential when attributing the examined effects to MSC-EVs.40 However, TFF does not consistently yield highly purified EVs,47 as a result, the lack of reported purity measures hinders the ability to determine the extent to which EVs contribute to the observed effects. Thorough validation of EV identity and enhanced reporting is strongly recommended.
Despite the differences in models, dosing regimens, and MSC-EV sources, studies showed an improvement in AD symptoms after MSC-EV therapy. This improvement was seen in key indicators like reduced erythema, edema, scaling, pruritus, and TEWL, as well as improved histopathological features such as reduced epidermal thickness and immune cell infiltration. MSC-EVs also seemed to work by modulating immune responses. The studies reported a drop in pro-inflammatory cytokines like IL-4, IL-13, IL31, and TSLP—major drivers of AD48 and enhanced skin barrier. Interestingly, these cytokine levels were reduced to levels comparable to prednisolone, a commonly used anti-inflammatory drug,28 hinting that MSC-EVs might offer a promising alternative therapy.
Mechanistic studies of MSC-EVs for AD treatment are still limited. The analyzed research points to their involvement in regulating essential pathways related to epidermal differentiation, keratinization, ceramide production, and modulation of epidermal gene expression, all of which support enhanced skin regeneration.14,31,33 Our analysis further confirms what existing literature suggests: MSC-EVs manage AD mainly through immunomodulation, regulating pathways such as T cell differentiation and the JAK/STAT signaling pathway. These are key pathways commonly targeted by therapeutic strategies for treating AD.11,49 miRNAs within MSC-EVs seem to play an important role in regulating inflammatory responses and apoptotic signaling, which contributes to their anti-inflammatory and therapeutic effects.29 Additionally, MSC-EVs showed promise in influencing microbiome diversity in AD,34 though the precise mechanisms are not yet fully understood. More research is needed to uncover the detailed MOA and identify the key components responsible for these effects.
Safety assessment findings were generally positive, with no significant side effects reported. This is encouraging, particularly given the potential for EV therapy to provide a safer alternative to conventional AD treatments that often have significant side effects.50,51 Additionally, xenogenic and allogenic MSC-EVs were well tolerated and effective. These findings are consistent with previous research that supports the safety of MSC-EVs in treating various conditions.26 Despite numerous animal studies and clinical trials confirming MSC-EV biosafety, thorough safety evaluations are essential for any new therapeutic product. EV medicinal products are distinct in that the process significantly influences the product.52 Even when derived from the same source, different preparation methods produce a varied mixture of co-isolates and sEV subsets,53 each with unique characteristics. Regulatory approval is critical to ensure the safety and effectiveness of MSC-EV therapies before clinical application, as emphasized by the FDA’s warning regarding unlicensed exosome products.54 Additionally, factors like recurring administration, off-target effects, and overdose require further investigation. Therefore, additional studies are needed to assess the safety of EV therapies in both the short and long terms.
To note, the studies demonstrated considerable variability in dosage regimens and delivery methods, with SC injection being the most common, followed by IV injection and topical application. Local delivery of MSC-EVs avoids clearance by phagocytes in the circulatory system, boosting bioavailability in target tissues and reducing the required therapeutic dose.55 On the other hand, systemic administration tends to result in sEV accumulation in specific organs like the lungs, liver, kidneys, and spleen.56 Despite these variations, no significant differences in effectiveness were observed across the different methods for MSC-EVs administration.28,31
Interestingly, the studies that tested different dosing strategies reported that higher doses led to better results. This suggests that finding the right dose concentration could be crucial for getting the best outcomes. It is intriguing that in some of the experiments, MSC-EVs came from a similar source and prepared using similar isolation and preparation methods, yet the effective dose varied considerably. This underscores the need for clear standards to determine the best dosing approach.57 The lack of guidance on determining the appropriate dose for EV studies is the reason for the observed inconsistency in dose selection across studies, which affects reproducibility.
The animal models used in these studies were primarily rodent models, with a few canine models included. The diversity of species, alongside variations in sex distribution and AD induction methods, adds a layer of complexity to interpreting the results. The induction of AD in these models ranged from topical application of allergens like D. farinae to chemical inducers such as DNCB. This variation in models and induction methods introduces heterogeneity, which may limit the comparability of results and their broader applicability. Mouse models are vital for preclinical research on AD, but current models often fail to accurately replicate human AD’s clinical complexity, instead mimicking allergic or irritant contact dermatitis.58 Nevertheless, the disease manifestations reported here still resembled the characteristics of AD, and recent transcriptomic and metabolomic analyses showed considerable overlap between human AD and select murine models.59,60 Indeed, no single murine model captures all aspects of human AD,59,60 The challenge is further complicated by recent findings of distinct AD endotypes with varying Th1, Th2, Th17, and Th22 inflammation patterns, which are not fully represented in current animal models.59 This limits their predictive value for clinical outcomes and their utility in studying human AD pathophysiology. To address this, Gilhar et al (2021) proposed minimal criteria that effective AD mouse models should meet, including AD-like epidermal barrier defects with reduced filaggrin and hyperproliferation; increased expression of TSLP, periostin, and chemokines like TARC; characteristic dermal immune cell infiltrates with key cytokines such as IL-4, IL-13, IL-31, and IL-33; neurodermatitis features including sensory skin hyperinnervation and stress-triggered lesions; and responsiveness to standard AD therapies;58 some of which were reported by the examined studies. Nevertheless, it is still important for researchers to reach a consensus on how well these animal models reflect human disease and to identify the most suitable models for preclinical testing. Alternatives, such as xenograft and humanized skin mouse models, may offer promising options.58,61
The studies by Park et al37 and Han et al38 offer exciting insights into how allogenic human ASC-EVs can alleviate dupilumab facial redness (DFR).37,38 DFR, which manifests as an eczematous facial rash after starting dupilumab, was not described in the clinical trials of this monoclonal antibody.62 However, in real-world practice, it affects roughly 10% of patients and often leads to a significant drop in quality of life, as the visible nature of the redness can be distressing.63 Patients with DFR have limited treatment options, with topical corticosteroids, calcineurin inhibitors, and antifungal agents offering relief to only 25–30% of cases. Unfortunately, some patients discontinue treatment due to this adverse event.63 While the underlying causes of DFR are still poorly understood, as several theories exist, Park et al37 suggest that DFR might represent site-specific treatment failure by dupilumab rather than an allergic reaction. Encouragingly, all patients reported significant relief with no side effects, leading to improved satisfaction, even with varying treatment schedules. This relief was interestingly rapid compared to other therapies.38 ASC-EVs not only reduced facial redness but also improved other skin-related issues such as inflammation markers and barrier function, highlighting their potential as a more comprehensive treatment.38 The examined studies suggest that ASC-EVs could be particularly effective for DFR due to their immunomodulatory properties and pleiotropic effect, which allow them to target the diverse pathophysiology of the condition, particularly given the limitations of current therapies.37,38
Interestingly, ASC-EVs were applied noninvasively using topical methods enhanced by electroporation37 or sonophoresis,38 with both approaches proved effective. This non-invasive approach is advantageous as it enhances patient compliance, addressing challenges such as discomfort, complex regimens, and poor adherence that often impede the success of AD therapy.64 The dose was adapted from earlier research on skin regeneration but reduced to account for the damaged skin and barrier defects common in AD.37 The main limitation of these studies was the small sample size and absence of a control group, but the results are still promising. Larger, randomized controlled trials will be essential to confirm these findings and refine treatment protocols, yet ASC-EVs appear to offer a novel and effective solution for AD patients dealing with DFR.
Our search on ClinicalTrials.gov for ongoing trials on MSC-EVs for AD therapy yielded no relevant studies. However, we did come across an interesting Phase I study (NCT05523011), investigating the safety and tolerability of an MSC-derived exosome ointment for psoriasis, another inflammatory skin disease. The study reported no serious adverse events, indicating the potential safety of MSC-EVs as a therapeutic option. This emphasizes the need for more clinical studies to evaluate MSC-EVs, whether naïve or modified, as a standalone therapeutic agent for AD.
Moving forward, there are several areas for future research. Although ASCs are currently favoured, exploring other MSC sources, such as umbilical cord, and comparing their efficacy and safety, will be vital for identifying the most effective treatments for AD. Standardizing isolation and preparation methods for MSC-EVs may be challenging, making adherence to guidelines like MISEV2023 and ISCT criteria essential. Detailed reporting and clear identity markers for MSC-EV preparations will enhance the interpretation, reproducibility, and comparability of results. Additionally, more research is needed to elucidate the mechanisms through which MSC-EVs exert their effects on AD, including studies on MSC-EV pharmacokinetics, biodistribution, and localization to understand their fate and target cells. Exploring ways to improve EV penetration, targeting, and overall therapeutic outcomes will also be important. While initial safety assessments are promising, comprehensive evaluations of long-term effects, potential off-target impacts, and implications of repeated administration are necessary. Rigorous safety studies and regulatory oversight will be critical for the successful translation of MSC-EV therapies to clinical practice. Furthermore, the limitations of current animal models in replicating human AD highlight the need for more accurate models, to improve the relevance of preclinical findings and facilitate the translation of therapies to human trials. Additionally, identifying measurable biomarkers for MSC-EV and their source potency and functionality are needed as they remain a challenge.65,66
Conclusion
In conclusion, MSC-EV therapy for AD holds a significant promise but is still in its early stages. While current research demonstrates the potential of MSC-EVs in modulating immune responses and promoting skin regeneration, several challenges remain, including gaps in mechanistic understanding, safety concerns, and the need for optimization of treatment strategies. More research is needed to explore different MSC sources, refine isolation techniques, and improve preclinical models. It is also crucial to interpret the findings with caution, as several key areas remain inadequately understood, in addition to the critical issue of lacking guideline compliance, which must be addressed to drive progress in the field. Overcoming these challenges will require collaborative efforts from researchers, regulatory bodies, and international societies. While MSC-EVs show significant promise as a novel therapy for AD, further research is essential to bridge existing gaps, ensuring the safe and effective clinical translation of this promising approach.
Acknowledgments
This research was funded by grants from Universiti Kebangsaan Malaysia (GUP-2021-033) and the Faculty of Medicine, Universiti Kebangsaan Malaysia (FF-2021-096). Grateful acknowledgment is extended to the Organization for Women in Science for the Developing World (OWSD) and the Swedish International Development Cooperation Agency (Sida) for providing a PhD fellowship to Maimonah E. Al-Masawa in support of her studies. The graphical abstract was produced using BioRender.com. The authors acknowledge the use of an AI tool (ChatGPT, GPT-4o) for language refinement but confirm that they fully authored, synthesized, researched, reviewed, and verified the content, taking full responsibility for its accuracy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Silverberg JI. Public health burden and epidemiology of atopic dermatitis. Dermatologic Clinics. 2017;35(3):283–289. doi:10.1016/j.det.2017.02.002
2. Cao X, Wang M, Zhou M, et al. Global, regional and national burden of paediatric atopic dermatitis: a trend and geographic inequalities analysis. Clin Exp Immunol. 2024;54(10):747–759. doi:10.1111/cea.14558
3. Vakharia PP, Silverberg JI. Adult-onset atopic dermatitis: characteristics and management. Am J Clin Dermatol. 2019;20(6):771–779. doi:10.1007/s40257-019-00453-7
4. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–1293. doi:10.1111/all.13401
5. Ariëns LFM, van Nimwegen KJM, Shams M, et al. Economic burden of adult patients with moderate to severe atopic dermatitis indicated for systemic treatment. Acta Derm Venereol. 2019;99(9):762–768. doi:10.2340/00015555-3212
6. Parekh K, Mehta TA, Dhas N, Kumar P, Popat A. Emerging nanomedicines for the treatment of atopic dermatitis. AAPS Pharm Sci Tech. 2021;22:1–14. doi:10.1208/s12249-021-01920-3
7. Weidinger S, Novak N. Dermatitis atópica. Lancet. 2016;387:1109–1122. doi:10.1016/S0140-6736(15)00149-X
8. Wollenberg A, Fölster-Holst R, Saint Aroman M, Sampogna F, Vestergaard C. Effects of a protein-free oat plantlet extract on microinflammation and skin barrier function in atopic dermatitis patients. J Eur Acad Dermatol Venereol. 2018;32(S1):1–15. doi:10.1111/jdv.14846
9. Frazier W, Bhardwaj N. Atopic dermatitis: diagnosis and treatment. Am Family Phys. 2020;101(10):590–598.
10. Pena J, Zameza PA, Pixley JN, Remitz A, Feldman SR. A comparison of topical corticosteroids and topical calcineurin inhibitors for the treatment of atopic dermatitis. j Allergy Clin Immunol Pract. 2023;11(5):1347–1359. doi:10.1016/j.jaip.2023.03.022
11. Seegräber M, Srour J, Walter A, Knop M, Wollenberg A. Dupilumab for treatment of atopic dermatitis. Expert Rev Clin Pharmacol. 2018;11(5):467–474. doi:10.1080/17512433.2018.1449642
12. Rodrigues MA, Torres T. JAK/STAT inhibitors for the treatment of atopic dermatitis. J Dermatological Treat. 2020;31:33–40. doi:10.1080/09546634.2019.1577549
13. Yang J, Xiao M, Ma K, et al. Therapeutic effects of mesenchymal stem cells and their derivatives in common skin inflammatory diseases: atopic dermatitis and psoriasis. Front Immunol. 2023;14. doi:10.3389/fimmu.2023.1092668
14. Shin KO, Ha DH, Kim JO, et al. Exosomes from human adipose tissue-derived mesenchymal stem cells promote epidermal barrier repair by inducing de novo synthesis of ceramides in atopic dermatitis. Cells. 2020;9(3):680. doi:10.3390/cells9030680
15. Ratajczak J, Miekus K, Kucia M, et al. Embryonic stem cell-derived microvesicles reprogram hematopoietic progenitors: evidence for horizontal transfer of mRNA and protein delivery. Leukemia. 2006;20(5):847–856. doi:10.1038/sj.leu.2404132
16. Valadi H, Ekström K, Bossios A, Sjöstrand M, Lee JJ, Lötvall JO. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol. 2007;9(6):654–659. doi:10.1038/ncb1596
17. Skog J, Würdinger T, van Rijn S, et al. Glioblastoma microvesicles transport RNA and proteins that promote tumour growth and provide diagnostic biomarkers. Nat Cell Biol. 2008;10(12):1470–1476. doi:10.1038/ncb1800
18. Bruno S, Grange C, Deregibus MC, et al. Mesenchymal stem cell-derived microvesicles protect against acute tubular injury. J Am Soc Nephrol. 2009;20(5):1053–1067. doi:10.1681/asn.2008070798
19. Lai RC, Arslan F, Lee MM, et al. Exosome secreted by MSC reduces myocardial ischemia/reperfusion injury. Stem Cell Res. 2010;4(3):214–222. doi:10.1016/j.scr.2009.12.003
20. Cocucci E, Meldolesi J. Ectosomes and exosomes: shedding the confusion between extracellular vesicles. Trends Cell Biol. 2015;25(6):364–372. doi:10.1016/j.tcb.2015.01.004
21. Tieu A, Lalu MM, Slobodian M, et al. An analysis of mesenchymal stem cell-derived extracellular vesicles for preclinical use. ACS Nano. 2020;14(8):9728–9743. doi:10.1021/acsnano.0c01363
22. Nguyen VVT, Welsh JA, Tertel T, et al. Inter-laboratory multiplex bead-based surface protein profiling of MSC-derived EV preparations identifies MSC-EV surface marker signatures. J Extracell Vesicles. 2024;13(6):e12463. doi:10.1002/jev2.12463
23. Lefebvre FA, Lécuyer E. Small luggage for a long journey: transfer of vesicle-enclosed small RNA in interspecies communication. Front Microbiol. 2017;8. doi:10.3389/fmicb.2017.00377.
24. Al-Masawa ME, Alshawsh MA, Ng CY, et al. Efficacy and safety of small extracellular vesicle interventions in wound healing and skin regeneration: a systematic review and meta-analysis of animal studies. Theranostics. 2022;12(15):6455–6508. doi:10.7150/thno.73436
25. Kordelas L, Rebmann V, Ludwig AK, et al. MSC-derived exosomes: a novel tool to treat therapy-refractory graft-versus-host disease. Leukemia. 2014;28(4):970–973. doi:10.1038/leu.2014.41
26. Van Delen M, Derdelinckx J, Wouters K, Nelissen I, Cools N. A systematic review and meta-analysis of clinical trials assessing safety and efficacy of human extracellular vesicle-based therapy. J Extracell Vesicles. 2024;13(7):e12458. doi:10.1002/jev2.12458
27. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/m18-0850
28. Cho BS, Kim JO, Ha DH, Yi YW. Exosomes derived from human adipose tissue-derived mesenchymal stem cells alleviate atopic dermatitis. Stem Cell Res Ther. 2018;9(1):187. doi:10.1186/s13287-018-0939-5
29. Cho BS, Kim SB, Kim S, Rhee B, Yoon J, Lee JW. Canine mesenchymal-stem-cell-derived extracellular vesicles attenuate atopic dermatitis. Animals. 2023;13(13). doi:10.3390/ani13132215
30. Huang R, Jia B, Su D, et al. Plant exosomes fused with engineered mesenchymal stem cell-derived nanovesicles for synergistic therapy of autoimmune skin disorders. J Extracell Vesicles. 2023;12(10):e12361. doi:10.1002/jev2.12361
31. Yoon J, Lee SK, Park A, et al. Exosome from IFN-γ-primed induced pluripotent stem cell-derived mesenchymal stem cells improved skin inflammation and barrier function. Int J mol Sci. 2023;24(14):11635. doi:10.3390/ijms241411635
32. Wang M, Zhao Y, Zhang Q. Human mesenchymal stem cell-derived exosomes accelerate wound healing of mice eczema. J DermatolTreat. 2022;33(3):1401–1405. doi:10.1080/09546634.2020.1820935
33. Kim J, Lee SK, Jung M, et al. Extracellular vesicles from IFN-γ-primed mesenchymal stem cells repress atopic dermatitis in mice. J Nanobiotechnol. 2022;20(1):526. doi:10.1186/s12951-022-01728-8
34. Kim SW, Lim KM, Cho SG, et al. Efficacy of allogeneic and xenogeneic exosomes for the treatment of canine atopic dermatitis: a pilot study. Animals. 2024;14(2). doi:10.3390/ani14020282
35. Kim SY, Yoon TH, Na J, et al. Mesenchymal stem cells and extracellular vesicles derived from canine adipose tissue ameliorates inflammation, skin barrier function and pruritus by reducing JAK/STAT signaling in atopic dermatitis. Int J mol Sci. 2022;23(9). doi:10.3390/ijms23094868
36. Yang JW, Seo Y, Shin TH, et al. Extracellular vesicles from SOD3-transduced stem cells exhibit improved immunomodulatory abilities in the murine dermatitis model. Antioxidants. 2020;9(11). doi:10.3390/antiox9111165
37. Park KY, Han HS, Park JW, Kwon HH, Park GH, Seo SJ. Exosomes derived from human adipose tissue-derived mesenchymal stem cells for the treatment of dupilumab-related facial redness in patients with atopic dermatitis: a report of two cases. J Cosmet Dermatol. 2022;21(2):844–849. doi:10.1111/jocd.14153
38. Han HS, Koh YG, Hong JK, Roh YJ, Seo SJ, Park KY. Adipose-derived stem cell exosomes for treatment of dupilumab-related facial redness in patients with atopic dermatitis. J DermatolTreat. 2023;34(1):2220444. doi:10.1080/09546634.2023.2220444
39. Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The international society for cellular therapy position statement. Cytotherapy. 2006;8(4):315–317. doi:10.1080/14653240600855905
40. Théry C, Witwer KW, Aikawa E, et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the international society for extracellular vesicles and update of the MISEV2014 guidelines. J Extracell Vesicles. 2018;7(1):1535750. doi:10.1080/20013078.2018.1535750
41. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13(2):e12404. doi:10.1002/jev2.12404
42. Lenzini S, Jung J, Cramer M, Zakhem E, Rowley JA. SCALABLE GMP-COMPATIBLE PROCESS SOLUTION FOR MSC-EV PURIFICATION WITH 10X YIELD IMPROVEMENTS. Cytotherapy. 2024;26(6, Supplement):S86. doi:10.1016/j.jcyt.2024.03.162
43. Börger V, Dittrich R, Staubach S, Zumegen S, Horn P, Giebel B. Tangential flow filtration, a potential method for the scaled preparation of extracellular vesicles. Cytotherapy. 2019;21(5, Supplement):S57. doi:10.1016/j.jcyt.2019.03.431
44. Li P, Kaslan M, Lee SH, Yao J, Gao Z. Progress in exosome isolation techniques. Theranostics. 2017;7(3):789–804. doi:10.7150/thno.18133
45. Visan KS, Lobb RJ, Ham S, et al. Comparative analysis of tangential flow filtration and ultracentrifugation, both combined with subsequent size exclusion chromatography, for the isolation of small extracellular vesicles. J Extracell Vesicles. 2022;11(9):e12266. doi:10.1002/jev2.12266
46. Zeng X, Yi X, Chen L, et al. Characterization and bioassays of extracellular vesicles extracted by tangential flow filtration. Regen Med. 2022;17(3):141–154. doi:10.2217/rme-2021-0038
47. Clos-Sansalvador M, Monguió-Tortajada M, Roura S, Franquesa M, Borràs FE. Commonly used methods for extracellular vesicles’ enrichment: implications in downstream analyses and use. Eur J Cell Biol. 2022;101(3):151227. doi:10.1016/j.ejcb.2022.151227
48. Tokura Y, Phadungsaksawasdi P, Ito T. Atopic dermatitis as Th2 disease revisited. J Cutaneous Immunol Allergy. 2018;1(5):158–164. doi:10.1002/cia2.12033
49. Szalus K, Trzeciak M, Nowicki RJ. JAK-STAT inhibitors in atopic dermatitis from pathogenesis to clinical trials results. Microorganisms. 2020;8(11):1743. doi:10.3390/microorganisms8111743
50. Newsom M, Bashyam AM, Balogh EA, Feldman SR, Strowd LC. New and emerging systemic treatments for atopic dermatitis. Drugs. 2020;80(11):1041–1052. doi:10.1007/s40265-020-01335-7
51. Tanei R. Atopic dermatitis in older adults: a review of treatment options. Drugs Aging. 2020;37(3):149–160. doi:10.1007/s40266-020-00750-5
52. Rohde E, Pachler K, Gimona M. Manufacturing and characterization of extracellular vesicles from umbilical cord-derived mesenchymal stromal cells for clinical testing. Cytotherapy. 2019;21(6):581–592. doi:10.1016/j.jcyt.2018.12.006
53. Mol EA, Goumans M-J, Doevendans PA, Sluijter JPG, Vader P. Higher functionality of extracellular vesicles isolated using size-exclusion chromatography compared to ultracentrifugation. Nanomed Nanotechnol Biol Med. 2017;13(6):2061–2065. doi:10.1016/j.nano.2017.03.011
54. Public safety notification on exosome products FDA. 2019. Available from: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/public-safety-notification-exosome-products.
55. Wei Z, Chen Z, Zhao Y, et al. Mononuclear phagocyte system blockade using extracellular vesicles modified with CD47 on membrane surface for myocardial infarction reperfusion injury treatment. Biomaterials. 2021;275:121000. doi:10.1016/j.biomaterials.2021.121000
56. Kang M, Jordan V, Blenkiron C, Chamley LW. Biodistribution of extracellular vesicles following administration into animals: a systematic review. J Extracell Vesicles. 2021;10(8):e12085. doi:10.1002/jev2.12085
57. Gupta D, Zickler AM, El Andaloussi S. Dosing extracellular vesicles. Adv Drug Deliv Rev. 2021;178:113961. doi:10.1016/j.addr.2021.113961
58. Gilhar A, Reich K, Keren A, Kabashima K, Steinhoff M, Paus R. Mouse models of atopic dermatitis: a critical reappraisal. Exp Dermatol. 2021;30(3):319–336. doi:10.1111/exd.14270
59. Choi J, Sutaria N, Roh YS, et al. Translational relevance of mouse models of atopic dermatitis. J Clin Med. 2021;10(4):613. doi:10.3390/jcm10040613
60. Ewald DA, Noda S, Oliva M, et al. Major differences between human atopic dermatitis and murine models, as determined by using global transcriptomic profiling. J Allergy Clin Immunol. 2017;139(2):562–571. doi:10.1016/j.jaci.2016.08.029
61. Guerrero-Aspizua S, Carretero M, Conti CJ, Del Río M. The importance of immunity in the development of reliable animal models for psoriasis and atopic dermatitis. Immunol cell biol. 2020;98(8):626–638. doi:10.1111/imcb.12365
62. Waldman RA, DeWane ME, Sloan B, Grant-Kels JM. Characterizing dupilumab facial redness: a multi-institution retrospective medical record review. J Am Acad Dermatol. 2020;82(1):230–232. doi:10.1016/j.jaad.2019.06.026
63. Jo CE, Finstad A, Georgakopoulos JR, Piguet V, Yeung J, Drucker AM. Facial and neck erythema associated with dupilumab treatment: a systematic review. J Am Acad Dermatol. 2021;84(5):1339–1347. doi:10.1016/j.jaad.2021.01.012
64. Tier HL, Balogh EA, Bashyam AM, et al. Tolerability of and adherence to topical treatments in atopic dermatitis: a narrative review. Dermatol Ther. 2021;11(2):415–431. doi:10.1007/s13555-021-00500-4
65. Witwer KW, Van Balkom BWM, Bruno S, et al. Defining mesenchymal stromal cell (MSC)-derived small extracellular vesicles for therapeutic applications. J Extracell Vesicles. 2019;8(1):1609206. doi:10.1080/20013078.2019.1609206
66. Gimona M, Brizzi MF, Choo ABH, et al. Critical considerations for the development of potency tests for therapeutic applications of mesenchymal stromal cell-derived small extracellular vesicles. Cytotherapy. 2021;23(5):373–380. doi:10.1016/j.jcyt.2021.01.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.