")
Back to Journals » Infection and Drug Resistance » Volume 17
Microbiological Characteristics, Risk Factors, and Short-Term Mortality of Carbapenem-Resistant Enterobacteriaceae Bloodstream Infections in Pediatric Patients in China: A 10-Year Longitudinal Study
Authors Liang Y, Zhao C , Lu Y, Liao K, Kong Y, Hong M, Li L , Chen Y
Received 2 September 2024
Accepted for publication 25 October 2024
Published 2 November 2024 Volume 2024:17 Pages 4815—4823
DOI https://doi.org/10.2147/IDR.S485001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yujian Liang,1,* Chenfeng Zhao,2,* Yuhang Lu,3,* Kang Liao,2 Yannan Kong,4 Mengzhi Hong,2 Liubing Li,2 Yili Chen2
1Department of Pediatric Intensive Care Unit, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, 510080, People’s Republic of China; 2Department of Laboratory Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 510080, People’s Republic of China; 3Zhongshan Medical School, Sun Yat-sen University, Guangzhou, Guangdong, 510080, People’s Republic of China; 4Department of Laboratory Medicine, the Nanhai’s Fifth People’s Hospital of Foshan, Foshan, Guangdong, 528231, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yili Chen; Liubing Li, Department of Laboratory Medicine, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 510080, People’s Republic of China, Email [email protected]; [email protected]
Background: Carbapenem-resistant Enterobacteriaceae (CRE) is rapidly becoming a major threat to hospitalized children worldwide. The purpose of this study was to summarize etiological characteristics and identify risk factors relevant to CRE bloodstream infection (BSI) and short-term mortality among pediatric patients in China.
Methods: In this study, we included 370 inpatients ≤ 17 years old with BSI caused by Enterobacteriaceae in China from January 2013 to December 2022. By collecting data on demographics, etiological features, and clinical outcomes, we conducted an in-depth analysis.
Results: Among the 370 BSI patients with infections caused by Enterobacteriaceae, 35 patients (9.46%) were caused by CRE. Among these CRE strains, Klebsiella pneumoniae (49.46%) was the most important pathogen of BSI in pediatric patients, followed by Escherichia coli (31.62%) and Enterobacter cloacae (5.95%). The most frequent carbapenemase was NDM (23/35, 65.71%), followed by KPC (8/35, 22.86%). The overall 28-day mortality rate of children with an Enterobacteriaceae BSI episode was 1.89% (7/370), of which CRE BSI patients (3/35, 8.57%) were significantly higher than CSE patients (4/335, 1.19%, P < 0.001). Congenital malformation (OR: 8.162, 95% CI: 3.859– 16.680, P < 0.001) and catheter-related (OR: 6.645, 95% CI: 3.159– 13.28, P: < 0.001) were associated with the development of CRE BSI in pediatric patients. A multivariate analysis showed that the infection of CRE (OR 7.758, 95% CI 1.869– 29.62, P = 0.021) were independent risk factors for 28-day mortality of Enterobacteriaceae BSI. When the MIC of any carbapenems was ≥ 8 μg/mL, the mortality rate in the ICU was higher (P < 0.05).
Conclusion: Congenital malformation, previous cephalosporin/carbapenems administration, and catheter-related conditions were closely related to the development of CRE BSI. The mortality rate of CRE BSI was higher. NDM was the predominant carbapenemase-producing mechanism in children.
Keywords: carbapenem-resistant Enterobacteriaceae, bloodstream infection
Introduction
Carbapenem-resistant Enterobacteriaceae (CRE) is increasingly isolated and poses a great threat to hospitalized children worldwide.1,2 Oncologic conditions, premature infants, and hospitalization in the intensive care unit (ICU) are frequently reported in available case series of pediatric CRE infections.3–5 Specifically, bloodstream infections (BSIs) caused by CRE are exceptionally intractable problems in children, with significant morbidity and mortality.6
Due to the limited treatment options available for children,7,8 the treatment of CRE BSI is challenging for the pediatrician. The key to successful prevention and treatment of CRE infection is to implement infection control measures and early identification of high-risk patients. Most of the information available on risk factors, clinical characteristics, therapeutic options, and prognosis was provided by adult population studies. It is reported risk factors for CRE-BSI in adults include extended hospital stay, critical illness, medical device intervention, long-term use of broad-spectrum antibiotics, and residency in nursing homes.9–11 There is still little research information on CRE-BSI in children.12,13
This study is aimed to summarize the etiological features and determine risk factors for CRE-BSI and predictors of 28-day mortality associated with the infection in a pediatric cohort.
Therefore, we conducted a retrospective analysis spanning 10 years. The 10-year time frame enhances the value of the epidemiological characteristics of CRE infections. Studies with a long-time span help to identify and validate long-term risk factors associated with the development of CRE BSI and allow for a more accurate assessment of the mortality rate of CRE BSI, which is crucial for guiding clinical treatment and prevention measures.
Methods
This study was carried out in the First Affiliated Hospital of Sun Yat-sen University from January 2013 to December 2022. A total of 370 episodes were enrolled in this study. Patients aged ≤17 years old with confirmed Enterobacteriaceae BSI were included. Based on the established criteria, Enterobacteriaceae BSI is defined as the presence of at least one positive blood culture with infectious symptoms and signs. Only the first phase of BSI was included. Patients with multi-bacterial BSI or patients with incomplete medical records were excluded. The included patients were followed up for 28 days from the date of the first positive blood culture.
CRE was defined as an isolate with a minimum inhibitory concentration (MIC) of ≥2 μg/mL for ertapenem (ETP) or ≥4 μg/mL for imipenem (IMP) or meropenem (MEM), according to the CLSI criteria (Clinical and Laboratory Standards Institute, 2022). Death within 28 days after the first positive blood culture was considered as the outcome evaluation.
The collected data included basic information, underlying diseases, length of hospital stay, admission to the intensive care unit (ICU), invasive surgery, immunosuppressive treatment 90 days prior to the onset of BSI, antibiotic treatment one month prior, pathogen characteristics, and patient outcomes.
Microbiological methods
Bact/ALERT® VIRTUO® blood cultures incubation (bioMérieux, Marcy l’Etoile, France) was used to incubate the blood specimen. Vitek 2 system (bioMérieux, Marcy l’Etoile, France) was used to identify the strains. Gram-negative susceptibility (GNS) cards (bioMérieux, Marcy l’Etoile, France) was employed to examine the antibiotic susceptibility tests for the strains. Antibiotic susceptibility testing results were interpreted according to the criteria recommended by the Clinical and Laboratory Standards Institute (CLSI, 2022). E. coli ATCC 25922 and K. pneumoniae ATCC 700603 were used as the quality control strains for antibiotic susceptibility testing. The carbapenemase was examined by immunochromatographic assay NG-test CARBA 5 kit (FOSUN DIAGNOSTICS, Changsha, China). This assay is able to detect the five most common carbapenemase among carbapenemase in Enterobacteriaceae: KPC (Klebsiella pneumoniae carbapenemase), NDM (New Delhi metallo‐β‐lactamase), IMP (imipenemase metallo‐β‐lactamase), VIM (Verona integron‐encoded metallo‐β‐lactamase) and OXA‐48 like (oxacillinase‐48‐like type carbapenemase).
Statistical Analysis
Numerical expressions for categorical variables are presented as percentages and figures. For continuous variables, the mean and standard deviation (SD) are provided for those following a normal distribution or the median with the interquartile range (IQR) for distributions that are not normal. Comparisons of categorical data were conducted using the Chi-square or Fisher’s exact test as appropriate. Continuous data were evaluated using the Student’s t-test or the Mann–Whitney U-test, depending on their distribution. The outcomes from the univariate analyses included the Odds ratio (OR), the 95% confidence interval (CI), and the P-value. Variables that demonstrated significance with a P-value of less than 0.05 were subsequently included in the binary logistic regression model to identify multivariate factors associated with the risk of CRE bloodstream infections (BSIs). The potential risk determinants for 28-day mortality due to CRE-BSI were examined using Cox logistic regression. The Forward LR method was employed in the multivariable assessment, integrating both binary logistic and Cox logistic regression. Survival curves were plotted using the Kaplan–Meier method to conduct survival analysis.
In the context of statistical testing throughout these analyses, a P-value threshold of less than 0.05 was indicative of statistical significance. The software utilized for all statistical evaluations was GraphPad Prism, version 10.0.
Result
Clinical and Demographic Characteristics of Patients
Among these 370 hospitalized children enrolled in the study, 35 (9.46%) presented a BSI by CRE. The 28-day mortality rate of children with an Enterobacteriaceae BSI episode was 1.89% (7/370). It was significantly higher for patients with CRE BSI (3/35, 8.57%) than for patients with CSE BSI (4/335, 1.19%, P = 0.021). The overall ICU-stay rate of children with an Enterobacteriaceae BSI episode was 8.11% (30/370), which was also significantly higher for patients with CRE BSI (7/35, 20.0%) than patients with CSE BSI (23/335, 6.87%, P = 0.0151).
In terms of the age distribution, preschool pediatric patients have a higher rate of CRE BSI, especially before the age of 6 years (OR: 2.921, 95% CI: 1.432–5.888, P = 0.0041). These pediatric patients with CRE BSI had a significantly higher rate of congenital malformations including congenital heart disease, biliary atresia, absence of kidney (OR: 8.162, 95% CI: 3.859–16.680, P<0.001) and indwelling catheters (OR: 6.645, 95% CI: 3.159–13.28, P < 0.001), as well as early long-term exposure to antibiotics, particularly carbapenems, which caused patients more likely to develop CRE BSI. The clinical and demographic characteristics of cohort patients with Enterobacteriaceae BSI isolates are shown in Table 1.
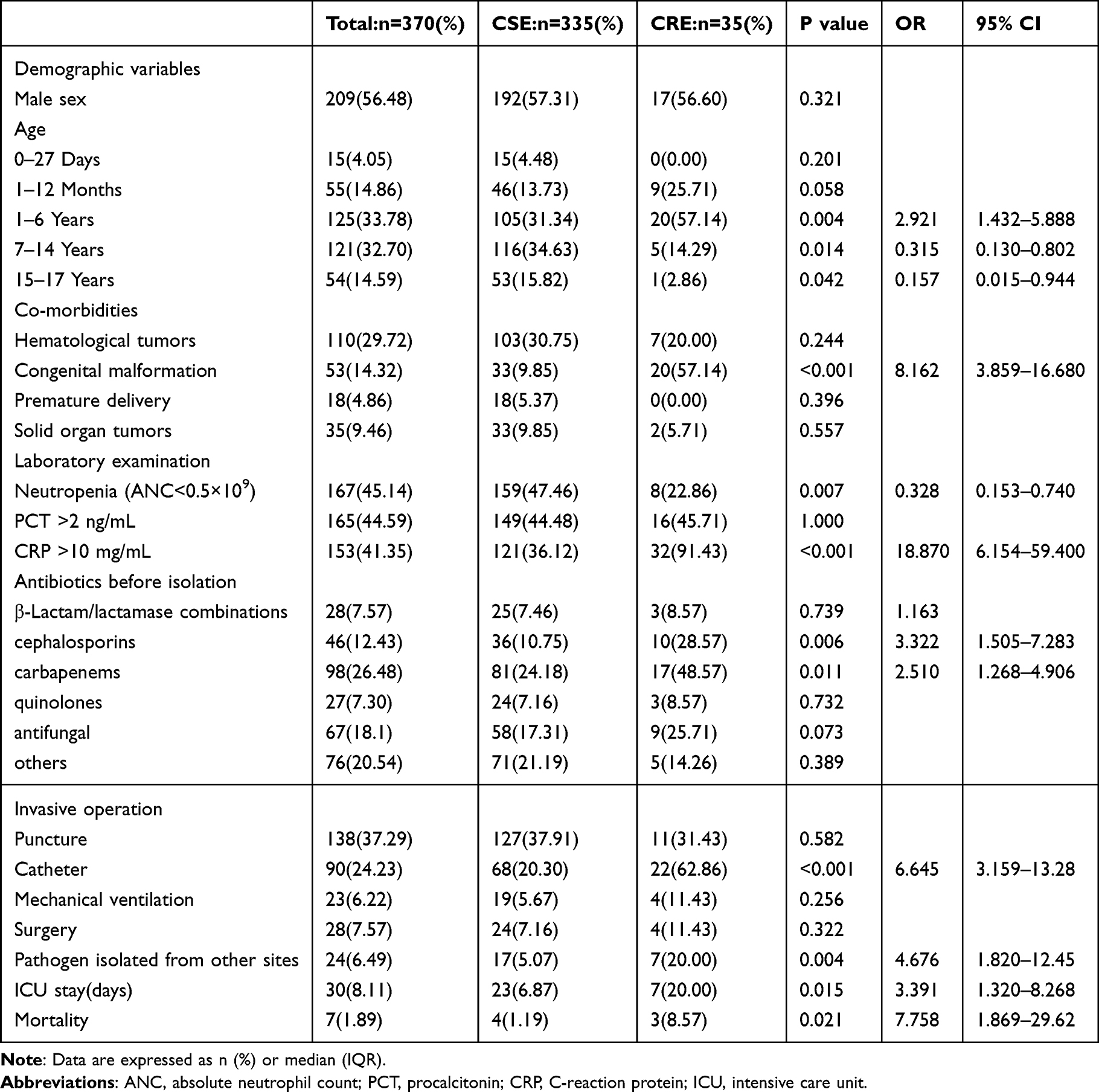 |
Table 1 Demographic Characteristics and Risk Factors of BSI Caused by CRE and BSI Patients Caused by CSE |
Microbiological Characteristics of Enterobacteriaceae Strains
The characteristics of strains are shown in Figure 1A. The top three species causing overall Enterobacteriaceae BSI in children were Klebsiella pneumoniae (Kpn, 183/370, 49.46%), Escherichia coli (Eco, 117/370, 31.62%), and Enterobacter cloacae (Ecl, 22/370, 5.95%). This ranking was consistent in both CRE BSI and CSE BSI. In addition, Other Enterobacteriaceae species involved were Klebsiella oxytoca (8/335, 2.39%), Salmonella bacteria (20/335, 5.97%), and other pathogens.
 |
Figure 1 (A) Microbiological characteristics of CRE and CSE strains, (B) Characteristics of carbapenemase in CRE strains. |
Most of the CRE strains (32/35, 91.43%) were found to produce carbapenemases. The most frequent carbapenemase was NDM (23/35, 65.71%), followed by KPC (8/35, 22.86%). Two Kpn isolates showed IMP positive, and one co-harbored NDM and IMP (Figure 1B). The susceptibility testing results of isolates with statistically significant differences of MIC (P < 0.05) were compared in Figure 2. CRE isolates showed more common resistance to other types of antibiotics than CSE isolates. The results were displayed in the form of minimum inhibitory concentration (MIC) for piperacillin-tazobactam, ceftazidime, cefepime, aztreonam, amikacin, and ciprofloxacin. The MIC of piperacillin-tazobactam, ceftazidime, cefepime, and aztreonam was higher in the CRE strain (P < 0.0001), while amikacin was higher in the CSE strain (P < 0.001).
 |
Figure 2 Partly susceptibility testing results of CSE and CRE isolates in MIC (μg/mL), the dashed horizontal line at 4 μg/mL: breakpoint for the aforementioned drug *P<0.001, **P<0.0001. |
Table 2 presented the antimicrobial resistance patterns of 35 CRE strains, categorized based on the type of carbapenemase they produced. The findings revealed that CRE strains harboring NDM-type carbapenemases exhibited the most sensitive in vitro to colistin and tigecycline. While strains producing KPC-type carbapenemases demonstrated enhanced in vitro susceptibility to ceftazidime-avibactam, as well as to colistin and tigecycline.
 |
Table 2 Resistance of CRE Strains Stratified for Carbapenemase Type to Specific Antimicrobials |
Risk Factors and Outcome of CRE BSI versus CSE BSI
The univariate analysis identified potential risk factors for CRE BSI among pediatric patients, including congenital malformations, such as congenital heart disease, biliary atresia, and absence of kidneys (OR 8.162, 95% CI 3.859–16.680, P < 0.001), abnormal CRP values (OR 18.870, 95% CI 6.154–59.400, P < 0.001), and pathogens isolated from other sites (OR 4.674, 95% CI 1.820–12.450, P = 0.004). Further, ICU stays before BSI onset (OR 3.391, 95% CI 1.320–8.268, P = 0.015), catheter input (OR 6.645, 95% CI 3.159–13.280, P < 0.001), prior exposure to carbapenems (OR 2.510, 95% CI 1.268–4.906, P = 0.011) and cephalosporins (OR 3.322, 95% CI 1.505–7.283, P = 0.006) were identified associated with CRE BSI.
The 28-day mortality rate of CRE BSI relative to CSE BSI was compared in Figure 3. Kaplan–Meier survival analysis showed a significant difference in the 28-day survival rate between CRE BSI patients and CSE BSI patients, with CRE patients having a higher mortality rate (8.57% vs 1.19%, P < 0.001).
 |
Figure 3 The 28-day survival rate of CRE BSI versus CSE BSI in the Kaplan–Meier curve. |
The susceptibility of carbapenem antibiotics to the isolated strains was detected, and it was found that different MICs significantly affected the mortality and ICU hospitalization of patients (P < 0.05) (Figure 4). When the MIC of carbapenems was ≥8 μg/mL, the admission rate and mortality rate in the ICU were higher.
 |
Figure 4 Effect of ETP, MEM, IMP drug susceptibility of isolated strains affect mortality and ICU hospitalization, *: P<0.001. |
Discussion
In this retrospective observational study, we analyzed 370 children with BSI caused by Enterobacteriaceae and found that nearly 10% of patients developed BSI caused by CRE. According to the China Antimicrobial Resistance Surveillance Network (CHINET), the detection rate of CRE strains in China has increased from 2.7% in 2012 to 9.7% in 2022. Our research findings are marginally elevated, which could be attributed to the more severe condition of BSI patients, who are more prone to developing CRE infections. Notably, the incidence of CRE BSI was the highest in the age group under 6 years of age. This may be because the majority of patients in this study came from the hematology-oncology ward. Children with hematologic cancers have an early onset of disease, weakened immunity, and long-term exposure to prophylactic antibiotics. It is reported that carriers of carbapenem-resistant Enterobacteriaceae in children with hematologic disorders with neutropenia are at high risk of bloodstream infection.14
Among the 35 CRE strains, Klebsiella pneumonia remained the most important pathogen of BSI in pediatric patients, followed by Escherichia coli and Enterobacter cloacae. We also found that NDM was the predominant carbapenemase-producing mechanism in children, which was consistent with CHINET’s data. However, Ruvinsky’s research found that in Argentina, KPC is the most dominant enzyme form in children, indicating that carbapenemase-producing Enterobacteriaceae has different molecular and epidemiological characteristics in different geographical regions.14,15 In China, the main mechanism causing carbapenem resistance was KPC-producing among adults,16,17 and ceftazidime/avibactam (CZA) is widely used to treat CRE infection with KPC-producing CRE, which is ineffective against NDM-producing isolates.18 In fact, for children suspected of CRE bloodstream infection, after determining the pathogen and enzyme production mechanism, CZA combined with aztreonam can be considered for the treatment of metallo-enzyme-producing strains including NDM and IMP.19
According to our study, we showed that congenital malformation (including congenital heart disease, biliary atresia, absence of kidney), previous cephalosporin, and carbapenems administration were independent risk factors for CRE BSI. Patients with congenital malformations typically undergo surgical procedures, more frequent exposure to healthcare, longer antibiotic treatment times, and more medical interventions. All these factors will increase the risk of infection.20,21 Laura et al1 reported that 84% of CRE BSI children had underlying diseases and most of them (46%) suffered from hematological malignancies or solid tumors. The 28-day mortality rate (8.57%) of the CRE group was also lower than previous reports.2,22 Recently, Montagnani et al reported that 4 out of 9 children in Italy (44.4%) died of CRE BSI.3 Another study showed that the CRE-BSI-related mortality rate in the Indian pediatric population was 52%.1 Therefore, closely monitoring the epidemic characteristics of CRE infection in local children is beneficial for early identification of infection risks and improving cure rates.
The relationship between meropenem MIC and increased patient mortality has been previously reported.23,24 Similarly, in our study, the MIC values of carbapenems in CRE strains can also predict a higher mortality rate in children. In adults, it is suggested that improved survival in patients receiving combinations of two or more in vitro active antibiotics, mainly in patients with a higher probability of death.25,26 This result has been inferred as a prediction for pediatric patients.4
The limitation of this study is that it was a retrospective study conducted in a single center, which may affect the ability to summarize research results. Further large-scale prospective multicenter investigations are needed.
In conclusion, congenital malformations, prior administration of cephalosporins/carbapenems, and the presence of indwelling catheters were associated with the development of CRE bloodstream infections (BSI). NDM was the primary carbapenemase-producing mechanism contributing to carbapenem resistance. Consequently, given the varying characteristics of patients infected with different strains of carbapenem-resistant Enterobacteriaceae (CRE), it is essential to apply individualized antimicrobial therapy.
Impact
- The key message of the article is that we summarized etiological characteristics and identify risk factors relevant to CRE bloodstream infection and short-term mortality among pediatric patients in China.
- Our study provides new insights into the etiology and risk factors of CRE bloodstream infections among pediatric patients, including congenital malformation, CRP levels, and catheter-related conditions. Our findings suggest that CRE infections are associated with a higher mortality rate compared to carbapenem-susceptible Enterobacteriaceae (CSE) infections and that NDM was the most common carbapenemase-producing mechanism among the CRE isolates.
- In terms of impact, our study may have a significant impact on the management of CRE infections in pediatric patients by providing clinicians with a better understanding of the disease and its risk factors. This information may lead to improved patient outcomes and reduce the burden of CRE infections in pediatric patients.
Abbreviations
CRE, Carbapenem-resistant Enterobacteriaceae; CSE, Carbapenem-susceptible Enterobacteriaceae; BSI, Bloodstream infection; ICU, Intensive care unit; MIC, Minimum inhibitory concentration; ANC, absolute neutrophil count; PCT, procalcitonin; CRP, C-reaction protein; Kpn, Klebsiella pneumoniae; Ecl, Enterobacter cloacae; Eco, Escherichia coli.
Data Sharing Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board and Ethics Committee of The First Affiliated Hospital of Sun Yat-sen University and conducted according to the Declaration of Helsinki (Approved No. of ethics committee: [2024]-200). The ethics committee approved the waiver of informed consent owing to the retrospective nature of the review. All research data were de-identified and anonymously analyzed.
Consent for Publication
NA
Acknowledgments
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4192614/v1
Funding
This work was supported by the National Natural Science Foundation of China (82302599), Guangdong Natural Science Foundation (2023A1515011252) and Guangdong Basic and Applied Basic Research Foundation (2022A1515110060).
Disclosure
The authors declare that they have no competing interests.
References
1. Nabarro L, Shankar C, Pragasam AK, et al. Clinical and bacterial risk factors for mortality in children with carbapenem-resistant Enterobacteriaceae bloodstream infections in India. Pediatr Infect Dis J. 2017;36(6):e161–e166. doi:10.1097/INF.0000000000001499
2. Chiotos K, Tamma PD, Flett KB, et al. Increased 30-day mortality associated with carbapenem-resistant Enterobacteriaceae in children. Open Forum Infect Dis. 2018;5(10):y222. doi:10.1093/ofid/ofy222
3. Montagnani C, Prato M, Scolfaro C, et al. Carbapenem-resistant Enterobacteriaceae infections in children: an Italian retrospective multicenter study. Pediatr Infect Dis J. 2016;35(8):862–868. doi:10.1097/INF.0000000000001188
4. Pannaraj PS, Bard JD, Cerini C, Weissman SJ. Pediatric carbapenem-resistant Enterobacteriaceae in Los Angeles, California, a high-prevalence region in the United States. Pediatr Infect Dis J. 2015;34(1):11–16. doi:10.1097/INF.0000000000000471
5. Colombo S, Scolfaro C, Calitri C, et al. Carbapenemase-producing Enterobacteriaceae (CPE) in the pediatric setting: results from an 18-month survey. Infect Control Hosp Epidemiol. 2014;35(5):599–601. doi:10.1086/675843
6. Ruvinsky S, Voto C, Roel M, et al. Carbapenem-resistant Enterobacteriaceae bloodstream infections: a case-control study from a pediatric referral hospital in Argentina. Front Public Health. 2022;10:983174. doi:10.3389/fpubh.2022.983174
7. Maltezou HC, Kontopidou F, Katerelos P, Daikos G, Roilides E, Theodoridou M. Infections caused by carbapenem-resistant Gram-negative pathogens in hospitalized children. Pediatr Infect Dis J. 2013;32(4):e151–e154. doi:10.1097/INF.0b013e3182804b49
8. Logan LK. Carbapenem-resistant Enterobacteriaceae: an emerging problem in children. Clin Infect Dis. 2012;55(6):852–859. doi:10.1093/cid/cis543
9. Tian L, Tan R, Chen Y, et al. Epidemiology of Klebsiella pneumoniae bloodstream infections in a teaching hospital: factors related to the carbapenem resistance and patient mortality. Antimicrob Resist Infect Control. 2016;5(1):48. doi:10.1186/s13756-016-0145-0
10. Jiao Y, Qin Y, Liu J, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization and predictors of mortality: a retrospective study. PATHOG GLOB HEALTH. 2015;109(2):68–74. doi:10.1179/2047773215Y.0000000004
11. Smith J. Prevalence and mortality of ceftazidime/avibactam-resistant KPC-producing Klebsiella pneumoniae bloodstream infections (2018–2022)[J]. Eur. J. Clin. Microbiol. Infect. Dis. 2023;45(6):1234–1250. doi:10.1007/s10096-023-04712-8
12. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
13. Bowers DR, Huang V. Emerging issues and treatment strategies in Carbapenem-Resistant Enterobacteriaceae (CRE). Curr Infect Dis Rep. 2016;18(12):48. doi:10.1007/s11908-016-0548-3
14. Frederic M, Nambiar S. review of carbapenemases and AmpC-beta lactamases. Pediatr Infect Dis J. 2011;30(12):1094–1095. doi:10.1097/INF.0b013e31823c0e47
15. Zhang R, Liu L, Zhou H, et al. Nationwide surveillance of clinical carbapenem-resistant Enterobacteriaceae (CRE) strains in China. Ebiomedicine. 2017;19:98–106. doi:10.1016/j.ebiom.2017.04.032
16. Cheng J, Zhao D, Ma X, Li J. Molecular epidemiology, risk factors, and outcomes of carbapenem-resistant Klebsiella pneumoniae infection in a tertiary hospital in eastern China: for a retrospective study conducted over 4 years. FRONT MICROBIOL. 2023;14:1223138. doi:10.3389/fmicb.2023.1223138
17. Elshamy AA, Aboshanab KM. A review on bacterial resistance to carbapenems: epidemiology, detection and treatment options. Future Sci OA. 2020;6(3):O438. doi:10.2144/fsoa-2019-0098
18. Lu G, Tang H, Xia Z, et al. In vitro and in vivo antimicrobial activities of ceftazidime/avibactam alone or in combination with aztreonam against carbapenem-resistant enterobacterales. Infect Drug Resist. 2022;15:7107–7116. doi:10.2147/IDR.S385240
19. Liu S, Lin Q, Ouyang L, Zhou C, Wang H. Successful treatment of ceftazidime/avibactam combined with aztreonam in the NDM-producing Klebsiella pneumoniae bloodstream and intestinal infections in a NK/T lymphoma patient with agranulocytosis during autologous hematopoietic stem cell transplantation: a case report. Eur J Clin Microbiol Infect Dis. 2022;1–4. doi:10.1007/s10096-022-04523-3
20. Markel M, Derraugh G, Lacher M, et al. Congenital lung malformation patients experience respiratory infections after resection: a population-based cohort study. J Pediatr Surg. 2022;57(5):829–832. doi:10.1016/j.jpedsurg.2021.12.042
21. Megli CJ, Coyne CB. Infections at the maternal-fetal interface: an overview of pathogenesis and defence. NAT REV MICROBIOL. 2022;20(2):67–82. doi:10.1038/s41579-021-00610-y
22. Meng H, Yang J, Niu M, Zhu H, Zhou Y, Lu J. Risk factors and clinical outcomes of carbapenem-resistant Klebsiella pneumoniae bacteraemia in children: a retrospective study. Int J Antimicrob Agents. 2023;62(4):106933. doi:10.1016/j.ijantimicag.2023.106933
23. O’Donnell JN, Rhodes NJ, Biehle LR, et al. Assessment of mortality stratified by meropenem minimum inhibitory concentration in patients with Enterobacteriaceae bacteraemia: a patient-level analysis of published data. Int J Antimicrob Agents. 2020;55(2):105849. doi:10.1016/j.ijantimicag.2019.11.006
24. Patel TS, Nagel JL. Clinical outcomes of Enterobacteriaceae infections stratified by carbapenem MICs. J Clin Microbiol. 2015;53(1):201–205. doi:10.1128/JCM.03057-14
25. Hsu AJ, Tamma PD. Treatment of multidrug-resistant Gram-negative infections in children. Clin Infect Dis. 2014;58(10):1439–1448. doi:10.1093/cid/ciu069
26. Giamarellou H. Multidrug-resistant Gram-negative bacteria: how to treat and for how long. Int J Antimicrob Agents. 2010;36(Suppl 2):S50–S54. doi:10.1016/j.ijantimicag.2010.11.014
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.