")
Back to Journals » Journal of Pain Research » Volume 18
Mid-Term Functional Recovery After ACDF and ACCF in the Treatment of Adjacent Two-Level Cervical Spondylosis: A Comparative Study
Authors Wang X, Huang D, Han J, Luo J, Wang Y
Received 31 December 2024
Accepted for publication 31 May 2025
Published 17 June 2025 Volume 2025:18 Pages 3009—3016
DOI https://doi.org/10.2147/JPR.S515112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Xinyang Wang, Dingan Huang, Jianbang Han, Junjie Luo, Yingfeng Wang
Department of Spine Surgery, Peoples’ Hospital of Huangshan City, Huangshan, Anhui, 245000, People’s Republic of China
Correspondence: Yingfeng Wang, Department of Spine Surgery, Peoples’ Hospital of Huangshan City, No. 4 Liyuan Road, Tunxi District, Huangshan, Anhui, 245000, People’s Republic of China, Email [email protected]
Objective: This study aims to comparatively analyze the mid-term functional recovery following anterior cervical discectomy and fusion (ACDF) versus anterior cervical corpectomy and fusion (ACCF) in the treatment of adjacent two-level cervical spondylosis.
Methods: A retrospective analysis was conducted on the medical records of 123 patients with adjacent two-level cervical spondylosis treated at our hospital between January 1, 2018, and June 30, 2022. The patients were divided into the ACCF group (n=63) and the ACDF group (n=60) according to the surgical method. The clinical outcomes, surgical details, mid-term functional recovery, cervical Cobb angle (C2-7), overall cervical range of motion (ROM) (C2-7), adjacent segment ROM (upper and lower adjacent segments), and incidence of complications were compared between the two groups before surgery and at the final follow-up.
Results: Preoperatively, there were no significant differences between the groups in JOA, VAS, and NDI scores (P > 0.05). The ACDF group had shorter operative time, less intraoperative blood loss, and lower postoperative drainage volume compared to the ACCF group (P < 0.05). The incidence of postoperative complications was also lower in the ACDF group (P < 0.05). At 18 months postoperatively, both groups showed significant improvement compared to their preoperative status (P < 0.05), with no significant differences in the rate of excellent and good outcomes between the two groups (P > 0.05). There were no significant differences between the groups in terms of cervical Cobb angle, overall cervical ROM, or ROM of the upper and lower adjacent segments (P > 0.05). Additionally, there was no significant difference in the incidence of adjacent segment degeneration between the two groups (P > 0.05).
Conclusion: Both ACDF and ACCF are effective surgical options for patients with adjacent two-level cervical spondylosis, improving cervical function and alleviating pain. However, both procedures are associated with a certain incidence of complications and a reduction in cervical mobility postoperatively. Comparatively, ACDF offers advantages in terms of shorter operative time, less intraoperative blood loss, and lower postoperative drainage volume.
Keywords: two-level cervical spondylosis, double discectomy, partial corpectomy, cervical function, pain
Cervical spondylosis is a common and frequently occurring condition in clinical practice. In recent years, with the aging population and changes in lifestyle, the incidence of this disease has been steadily increasing, with a noticeable trend towards affecting younger individuals.1 Adjacent two-level cervical spondylosis, often seen in cases of cervical myelopathy, is a mixed type of cervical spondylosis. The primary clinical treatment principles for this condition include relieving nerve root or spinal cord compression, preventing further neurological deterioration, and improving cervical spine mobility.2 Anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) are the common surgical techniques used to treat this condition. Some researchers have found that ACDF provides direct decompression, restores intervertebral disc height, and reconstructs cervical spine lordosis, showing favorable outcomes in clinical application.3 ACCF effectively addresses anterior spinal cord compression and is suitable for most cases of radiculopathy and myelopathy. Both ACDF and ACCF are effective surgical options for patients with adjacent two-level cervical spondylosis, improving cervical function and alleviating pain. However, it is important to note that the balance of the cervical sagittal plane is directly related to cervical spine mobility and surgical prognosis, and the mechanisms by which these two surgeries affect cervical sagittal balance remain inconclusive. Therefore, to further explore the mid-term functional recovery following ACDF and ACCF in the treatment of adjacent two-level cervical spondylosis, this study retrospectively analyzed 123 patients with this condition who were treated at our hospital between January 1, 2018, and June 30, 2022, as detailed below.
General Information and Methods
General Information
This study retrospectively analyzed the medical records of 123 patients with adjacent two-level cervical spondylosis who were treated at our hospital between January 1, 2018, and June 30, 2022. The patients were divided into two groups based on the surgical method: the ACCF group (n=63) and the ACDF group (n=60). The trial was conducted according to Good Clinical Practice guidelines developed by the International Council for Harmonisation and in compliance with the trial protocol. The protocol was approved by the institutional review boards or independent ethics committees at each site. All patients provided written informed consent per Declaration of Helsinki principles. An independent data monitoring committee monitored safety and efficacy data. Ethics No.: XHU20180101.
In the ACCF group, there were 38 males and 25 females, with an age range of 44 to 72 years (mean age: 58.00 ± 6.43 years). The affected segments were distributed as follows: C3-5 in 10 cases, C4-6 in 15 cases, and C5-7 in 38 cases. In the ACDF group, there were 32 males and 28 females, with an age range of 46 to 71 years (mean age: 58.50 ± 6.40 years). The affected segments were distributed as follows: C3-5 in 8 cases, C4-6 in 14 cases, and C5-7 in 38 cases. The baseline characteristics of the two groups were comparable (P > 0.05).
Diagnostic Criteria: The diagnosis was confirmed according to the criteria referenced in Cervical spondylosis.4 (1) A history of cervical spine trauma or chronic occupational strain, presenting with pain and soreness in the neck, shoulders, and upper back, often accompanied by radiating pain in the upper limbs; (2) Radiological evidence of cervical degenerative changes or structural deformities; (3) Frequent association with symptoms indicative of nerve compression; (4) A positive brachial plexus tension test; (5) CT or MRI findings demonstrating pathological changes in the intervertebral discs and surrounding tissues.
Inclusion Criteria
Patients were included if they had MRI-confirmed compression of the spinal cord at adjacent two levels, with clinical symptoms and signs consistent with this diagnosis; met the surgical indications; and provided informed consent for their data to be included in the study.
Exclusion Criteria
Patients were excluded if they had a history of cervical or neck trauma/surgery, multiple adjacent segments with disc protrusion and compression, spinal cord compression caused by other diseases, autoimmune deficiency, infectious diseases, concurrent fractures or tumors, or were unable to participate in postoperative follow-up.
Methods
ACCF Group
For the anterior cervical corpectomy and fusion procedure, patients were prepared preoperatively by guiding them through esophageal and tracheal retraction exercises for 1–2 consecutive days. Under general anesthesia, the patient was positioned supine with the head fixed, and a transverse incision was made on the right side of the neck. The skin was incised and subcutaneous tissues were dissected to expose the prevertebral space. The trachea and esophagus were retracted to the left, and the longus colli muscle and prevertebral fascia were separated to expose the anterior longitudinal ligament. The targeted intervertebral space was marked using a localization needle, and the position was confirmed with C-arm fluoroscopy. A localization needle was placed in both the upper and lower vertebral bodies, and the target intervertebral space was distracted using a Caspar retractor. The intervertebral disc was excised, and decompression was performed. The compressed dural sac was restored to its original contour. The same procedure was applied to the second targeted intervertebral space, and two cages were inserted to achieve interbody fusion. Fluoroscopic imaging was used to verify the positioning of the internal fixation and implants. The PEEK (polyether ether ketone) material was used for plate and screw fixation, a drainage tube was placed, and the incision was closed.
ACDF Group
For the anterior cervical discectomy and fusion procedure, using the C4-6 segments as an example, the preoperative preparations were identical to those in the ACCF group. The procedure began by exposing the midsection of the C5 vertebral body. The prevertebral fascia was incised, and the C-arm was used for precise localization. The anterior longitudinal ligament was incised anterior to the C5 vertebral body, exposing the C4-5 and C5-6 intervertebral discs. The discs were excised up to the anterior margin of the spinal canal, and decompression was performed at the posterior inferior edge of C4 and the posterior superior edge of C6. A partial resection of the C5 vertebral body was conducted, and lateral decompression was performed on C5. After thorough irrigation, the appropriate length of the titanium cage needed for interbody fusion from C4 to C6 was measured, filled with bone graft, and implanted between the C4 and C6 vertebral bodies. The position of the titanium cage was confirmed, and a 6-hole plate was placed on the anterior aspect of the cervical spine for fixation. The wound was irrigated, and the incision was closed.
Postoperative Care for Both Groups
Postoperatively, patients were monitored for changes in their condition, and the surgical wound was observed. Antibiotics were administered routinely, and functional rehabilitation exercises were guided based on the patient’s condition.
Outcome Measures
Surgical Efficacy
The surgical outcomes were evaluated at an average follow-up of 18 months postoperatively, with the final assessment conducted at the last follow-up. The outcomes were classified as follows: Excellent—complete resolution of symptoms; Good—mild symptoms without limitations in daily life or work; Fair—only slight improvement in symptoms; Poor—did not meet the above criteria.5 The surgical success rate was calculated as follows: Surgical success rate = (number of Excellent + Good cases) / total number of cases × 100%.
Surgical Parameters
The surgical duration, intraoperative blood loss, hospital stay, and postoperative drainage volume were recorded for both groups.
Mid-Term Functional Recovery
The relevant functional outcomes were assessed at an average follow-up of 18 months postoperatively, with the final assessment conducted at the last follow-up.
Functional Status
The Japanese Orthopaedic Association (JOA) score was used to evaluate the functional status of the patients, focusing on four aspects: upper limb function, lower limb function, sensory function, and bladder function. The total score ranges from 0 to 17, with lower scores indicating more severe functional impairment.6
Cervical Function
The Neck Disability Index (NDI) was utilized to assess cervical spine function. The NDI consists of 10 items, each scored from 0 to 5, with a total score ranging from 0 to 50. Higher scores indicate more severe functional impairment.7
Pain Severity
Pain was assessed using a visual analog scale (VAS), with a total score ranging from 0 to 10, where higher scores indicate more severe pain.8
Cervical Cobb Angle, Overall Cervical Range of Motion, and Adjacent Segment Motion
These parameters were evaluated at the final follow-up, with an average follow-up duration of 18 months postoperatively.
Cervical Cobb Angle
The Cobb angle was measured by drawing a horizontal line along the inferior endplate of the C2 vertebral body and another along the inferior endplate of the C7 vertebral body. Perpendicular lines were then drawn from each of these horizontal lines, and the angle formed between these two perpendiculars was recorded as the Cobb angle.
Overall Cervical Range of Motion
The overall cervical range of motion was measured using the method described by Gore.
Adjacent Segment Motion
The range of motion of the adjacent segments (both superior and inferior to the surgical site) was assessed using the Cobb angle method.
Complication Rate
The incidence of complications was recorded for both groups during the patients’ hospital stay. Common complications monitored included cerebrospinal fluid leakage, nerve root paralysis, dysphagia, hoarseness, respiratory difficulties, hematoma, and aspiration during drinking.
Adjacent Segment Degeneration Rate
The rate of adjacent segment degeneration was assessed at the final follow-up, with an average follow-up duration of 18 months postoperatively. The incidence of adjacent segment degeneration was calculated and compared between the two groups.
Statistical Methods
SPSS26.0 was used for statistical analysis. Continuous variables were expressed as mean ± SD, and t-test was used to compared the differences between groups. Categorical variables were expressed as n(%), and chi-square test was used to compared the differences between groups. P<0.05 was considered statistically significant.
Results
Surgical Efficacy
At 18 months postoperatively, the comparative analysis of surgical outcomes between the two intervention groups demonstrated no statistically significant difference in the proportion of patients achieving excellent outcomes (P > 0.05, Table 1). These findings suggest that both surgical approaches may offer comparable long-term efficacy in terms of clinical improvement and patient-reported outcomes. The absence of a statistically significant difference in surgical efficacy between the two groups raises several important considerations. First, it is possible that both procedures effectively address the underlying pathology to a similar extent, leading to equivalent functional recovery and symptom relief. Second, patient-specific factors such as baseline disease severity, anatomical variations, and postoperative rehabilitation adherence may exert a greater influence on long-term outcomes than the choice of surgical technique itself.
 |
Table 1 Comparative Analysis of Surgical Outcomes [n(%)] |
Surgical Details
The ACDF group demonstrated a significantly shorter operative duration, reduced intraoperative blood loss, and lower postoperative drainage volume compared to the ACCF group (P < 0.05). However, there was no significant difference in hospital stay duration between the two groups (P > 0.05) Table 2. These findings suggest that ACDF may offer a surgical advantage in terms of reduced operative complexity and perioperative morbidity, likely due to its more targeted approach, which avoids the extensive bone removal required in ACCF. The shorter operative duration and lower blood loss in ACDF could contribute to a more favorable intraoperative hemodynamic profile and reduced surgical stress, potentially leading to a smoother early recovery phase.
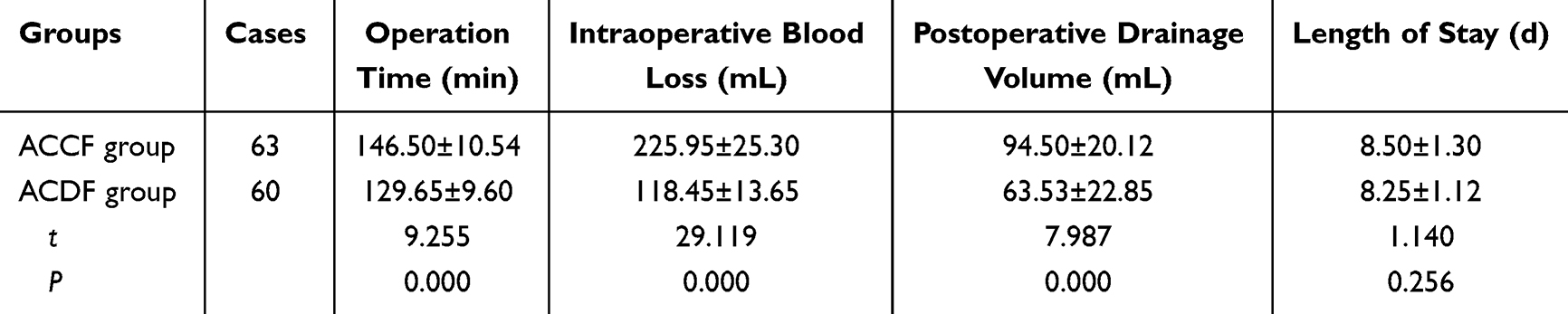 |
Table 2 Comparative Analysis of Surgical Details (±s) |
Midterm Functional Recovery
Preoperatively, there were no significant differences in JOA, NDI, or VAS scores between the two groups (P > 0.05). At the 18-month follow-up, both groups showed significant improvements compared to preoperative values (P < 0.05), but there were no notable differences between the groups (P > 0.05) Table 3. The comparable improvements in JOA, NDI, and VAS scores between the two groups suggest that both ACDF and ACCF effectively restore neurological function, reduce pain, and enhance cervical spine-related quality of life in the midterm postoperative period. These findings indicate that, despite differences in surgical complexity and perioperative parameters, the long-term functional outcomes of these procedures may be largely equivalent.
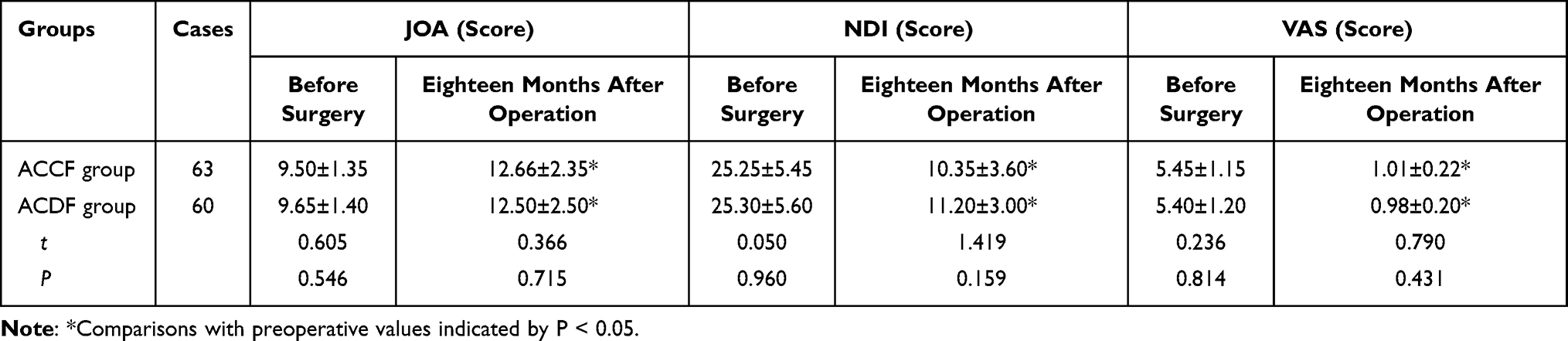 |
Table 3 Comparative Analysis of Midterm Functional Recovery [(±s), Scores] |
Cervical Cobb Angle, Cervical Range of Motion, and Segmental Mobility
Preoperatively, there was no significant difference in the Cobb angle between the two groups (P > 0.05). At 18 months postoperatively, the Cobb angle, overall cervical range of motion, and segmental mobility above and below the adjacent segments were similar between the two groups (P > 0.05) Table 4. The comparable postoperative Cobb angle and cervical mobility between the two groups suggest that both surgical techniques effectively maintain cervical sagittal alignment and dynamic function over the midterm follow-up. Despite the structural differences in the extent of decompression and fusion between ACDF and ACCF, neither approach appears to confer a distinct advantage or disadvantage in terms of overall spinal balance and motion preservation.
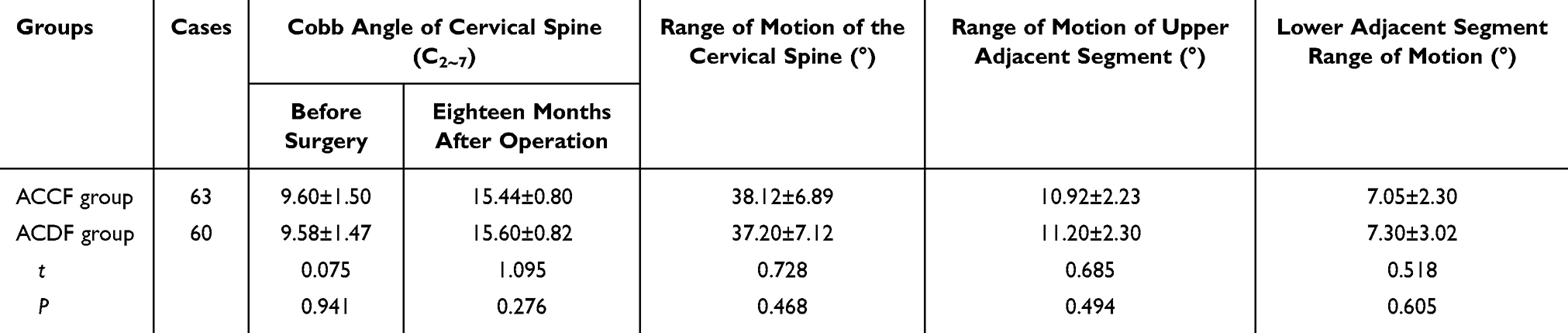 |
Table 4 Cervical Cobb Angle, Cervical Range of Motion, and Segmental Mobility |
Complication Rates
The incidence of complications was lower in the ACDF group compared to the ACCF group (P < 0.05) Table 5.
 |
Table 5 Incidence of Complications [n(%)] |
Incidence of Adjacent Segment Degeneration
All patients were followed for an average of 18 months. At the final follow-up, adjacent segment degeneration occurred in 11 cases (17.46%) in the ACCF group and in 10 cases (16.67%) in the ACDF group. The comparison between the two groups showed no significant difference (χ²=0.013, P=0.906, P>0.05).
Discussion
Patients with adjacent two-level cervical spondylosis commonly experience symptoms such as cervical pain and limb dysfunction, which severely disrupt their daily work and quality of life. The underlying pathology involves anterior cervical compression of the spinal cord, and achieving complete decompression, relieving compression, and restoring the normal alignment of the spine are widely accepted as the clinical treatment goals for this condition. For patients with adjacent two-level cervical spondylosis, ACDF and ACCF are the two most commonly employed and effective surgical techniques, both of which can significantly alleviate clinical symptoms.9 However, there is a relative paucity of reports on the mid-term functional recovery following these two surgical approaches in the treatment of adjacent two-level cervical spondylosis.
Yang Wei et al10 reported that both ACCF and ACDF achieve satisfactory outcomes in the treatment of adjacent two-level cervical spondylosis, with the ACDF group showing shorter operative times and less intraoperative blood loss (P<0.05). In this study, we found no significant difference in the surgical success rates between the two groups. However, the ACDF group exhibited shorter operative times, reduced intraoperative blood loss, and less postoperative drainage (P<0.05), consistent with the findings of Yang Wei et al. This further confirms that while both surgical techniques are effective, ACDF offers superior perioperative advantages. The ACCF procedure involves direct resection of the vertebral body between the affected segments, providing a broader surgical field and allowing for a more extensive decompression. Additionally, the resected vertebral body can be utilized as an autologous bone graft in the fusion process, enhancing the efficacy of the surgery.11 In contrast, ACDF preserves the vertebral body while effectively removing the intervertebral disc or osteophytes, thereby significantly relieving nerve compression and stabilizing the spine. The ACDF technique does not involve the resection of the superior vertebra, resulting in a smaller surgical field and space. Consequently, the procedure has a shorter operative time and less intraoperative blood loss, allowing patients to recover more quickly and facilitating earlier discharge from the hospital.12
This study also found that, at 18 months postoperatively, both the JOA, NDI, and VAS scores had improved compared to preoperative values in both groups, with no significant differences between the groups. This suggests that both surgical approaches provide favorable mid-term functional recovery. Both ACDF and ACCF effectively relieve neural compression, stabilize the cervical spine, and prevent exacerbation of disc herniation, leading to significant improvements in postoperative mobility and contributing positively to the restoration of cervical and limb function in the medium to long term. Further data analysis revealed no significant differences between the groups in terms of cervical Cobb angle, overall cervical range of motion, or adjacent segment motion (P > 0.05). It was observed that, under normal conditions, cervical flexion, extension, and lateral bending can reach up to 45°. However, postoperative cervical range of motion was notably reduced, with adjacent segment motion being more pronounced. This reduction in range of motion and increased adjacent segment movement are primarily attributable to the restrictions imposed by the surgical fixation, which can accelerate degeneration of the adjacent segments.
The study further revealed that the incidence of complications during the hospital stay was lower in the ACDF group compared to the ACCF group (P<0.05), indicating that while both surgical approaches are associated with certain complications, ACDF generally presents fewer. The rate of adjacent segment degeneration at follow-up showed no significant difference between the groups (P>0.05). The occurrence of postoperative complications, such as dysphagia and dura mater tears, is influenced by various factors, including postoperative soft tissue swelling and prolonged traction on the esophagus. Given that the ACDF procedure involves a shorter operative time, it is associated with a reduced risk of these symptoms. Both surgical methods involve the use of autologous bone grafts from the resected material during decompression for the Cage and titanium mesh, which promotes bone fusion and reduces the risk of complications.13
In summary, both ACDF and ACCF demonstrate effective surgical outcomes and significant mid-term functional recovery for patients with adjacent two-level cervical spondylosis. However, ACDF is advantageous due to its shorter operative time, reduced intraoperative blood loss, and less postoperative drainage. Thus, ACDF is recommended for broader application in clinical practice. This study presents a comprehensive midterm comparison of ACDF and ACCF for adjacent two-level cervical spondylosis, offering novel insights into their relative efficacy and biomechanical impact. Unlike previous research focusing on single-level pathology or short-term outcomes, this study extends the follow-up to 18 months, enabling a more robust assessment of functional recovery, cervical alignment, and segmental mobility. A key innovation lies in the detailed evaluation of segmental mobility, particularly at adjacent levels, providing valuable data on postoperative spinal dynamics. The findings indicate that both procedures effectively preserve cervical sagittal balance and overall range of motion, addressing a critical question in surgical decision-making—whether one technique predisposes patients to adjacent segment degeneration or altered biomechanics. Clinically, these results inform surgical strategy optimization by demonstrating comparable functional recovery and postoperative stability between ACDF and ACCF. The similarity in midterm outcomes underscores the importance of patient-specific factors—such as baseline pathology, bone quality, and anatomical variation—over a presumed superiority of one approach. Additionally, these findings may guide postoperative rehabilitation strategies, ensuring targeted interventions that promote recovery without unnecessary mobility restrictions. Future research with extended follow-up and advanced imaging could further elucidate the long-term implications of these procedures on adjacent segment degeneration and fusion integrity. By deepening the understanding of cervical biomechanics and surgical efficacy, this study contributes to more personalized, evidence-based approaches in the management of multilevel cervical spondylosis.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available in the Manuscript.
Ethics Approval and Consent to Participation
This study did not involve any special intervention or handling of sensitive information, and therefore did not require ethical review. The Peoples’ Hospital of Huangshan City has agreed to exemption from review.
Acknowledgments
Thanks to the reviewers and editors for their sincere comments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Wang H, Jia J. Interpretation of rehabilitation guidelines and expert consensus on cervical spondylosis from the perspective of full-cycle rehabilitation. Chin Med J. 2021;56(8):825–829.
2. Kocaman H, Yıldız NT, Canlı M, Alkan H. Comparison of the effects of Mulligan mobilisation technique combined with cervical stabilisation exercises with the effects of cervical stabilisation exercises alone in chronic neck pain: a randomised controlled study. Karya J Health Sci. 2023;4(3):227–234. doi:10.52831/kjhs.1374767
3. Ceylan İ, Canlı M, Kuzu Ş, et al. The effectiveness of two different treatment approaches in individuals with chronic non-specific neck pain: a randomised control trial. 2023.
4. Editorial Board of Chinese Journal of Surgery. Expert consensus on classification, diagnosis, and non-surgical treatment of cervical spondylosis (2018). Chin J Surg. 2018;56(6):401–402.
5. Cao K, Wang Y, Zhou Y, et al. Efficacy and complications of anterior cervical discectomy and fusion for two-level myelopathy cervical spondylosis. Pract Hosp Clin J. 2019;16(6):150–153.
6. Lin Z, Li Y, Xie X, et al. Comparative efficacy of two surgical techniques for multilevel cervical spondylosis. Clin Orthop J. 2020;23(3):314–317.
7. Jiang D, Liu Z, Shi J, et al. Observation of implant subsidence following ACDF versus ACCF for cervical spondylosis. J Neck Low Back Pain. 2021;42(5):651–653, 656.
8. Yang S, Gong C, Zhou S. Effects of ACDF versus ACCF on cervical range of motion and complications in patients with multilevel cervical spondylosis. J Hebei Med Univ. 2021;42(8):896–899.
9. Sun Y, Jiang X, Yi P. Comparative efficacy of ACDF versus ACCF in the treatment of two-level myelopathy cervical spondylosis. J Neck Low Back Pain. 2020;41(1):117–118.
10. Yang W, Li X. Comparison of anterior cervical corpectomy versus anterior cervical discectomy and fusion for adjacent two-level cervical spondylosis. Chin J Bone Joint Inj. 2022;37(11):1154–1157.
11. Chen E, Wang N, Quan R. Efficacy Analysis of Two Anterior Cervical Decompression and Fusion Techniques for Two-Level Myelopathy Cervical Spondylosis. Chin J Orthop Traumatol. 2020;33(9):841–847.
12. Fang Q, Zhou J, Wei J. Comparative study of single-level ACCF versus two-level ACDF in the treatment of adjacent two-level myelopathic cervical spondylosis. Shandong Med J. 2019;59(20):65–68.
13. Ye F, Yin X, Lin F, et al. Comparative study of two decompression and fusion techniques for multilevel myelopathic cervical spondylosis. Chin J Orthop Surg. 2022;30(7):608–613.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.