")
Back to Journals » Cancer Management and Research » Volume 17
Multimodal Framework in Lung Cancer Management: Integrating Liquid Biopsy with Traditional Diagnostic Techniques
Authors Qi W, Tian L, Xu J, Li Z, Wang T
Received 14 November 2024
Accepted for publication 26 February 2025
Published 3 March 2025 Volume 2025:17 Pages 461—481
DOI https://doi.org/10.2147/CMAR.S506630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Wenlong Qi,1 Lin Tian,2 Jianan Xu,2 Zhenyu Li,2 Tan Wang2
1Changchun University of Traditional Chinese Medicine, Changchun, Jilin, 130000, People’s Republic of China; 2Affiliated Hospital of Changchun University of Traditional Chinese Medicine, Changchun, Jilin, 130000, People’s Republic of China
Correspondence: Tan Wang, The Affiliated Hospital to Changchun University of Chinese Medicine, Changchun, 130021, People’s Republic of China, Email [email protected]
Abstract: Lung cancer is one of the most lethal malignancies worldwide, making early diagnosis and targeted treatment crucial for improving patient outcomes. Liquid biopsy, a rapidly advancing non-invasive diagnostic tool, has shown significant potential in lung cancer management through dynamic monitoring. This review explores the integration of liquid biopsy with traditional diagnostic techniques in lung cancer management. We first discuss the essential roles of traditional approaches, such as imaging and tissue biopsy, and then examine the concepts of liquid biopsy, emphasizing its unique advantages in early detection, treatment monitoring, and prognosis. Finally, we propose strategies for integrating liquid biopsy with traditional diagnostics, offering multimodal framework to enhance precision medicine in lung cancer.
Keywords: liquid biopsy, lung cancer, multimodal diagnosis, ctDNA, CTCs
Introduction
Lung cancer is one of the leading causes of cancer-related mortality worldwide, with both its incidence and mortality rates ranking among the highest for malignant tumors. Statistics indicate that in 2022, there were approximately 2.48 million new cases of lung cancer globally, accounting for 12.4% of all new cancer cases, thereby reaffirming its status as the most commonly diagnosed cancer type worldwide. Furthermore, lung cancer remains the primary cause of cancer-related death, with an estimated 1.8 million deaths that year, representing 18.7% of the global cancer mortality total.1 These figures not only underscore the high incidence of lung cancer but also reflect its extremely high mortality rate. Despite advancements in medical technology in recent years, which have improved the diagnosis and treatment of lung cancer, the overall survival rate remains relatively low, particularly for patients with advanced lung cancer, where the five-year survival rate is less than 20%.2
Early diagnosis and accurate staging are crucial for improving the prognosis of lung cancer patients. However, the biological heterogeneity of lung cancer and the complexity of the tumor microenvironment pose significant challenges to traditional diagnostic methods.3 Imaging techniques such as CT and PET-CT play a critical role in the early screening and staging of lung cancer, but their sensitivity in detecting small lesions is limited, and the potential for false-positive results increases diagnostic complexity.4 Tissue biopsy is widely regarded as the “gold standard” for lung cancer diagnosis, providing histological typing and molecular characterization of the tumor through pathological analysis. However, the invasive feature of tissue biopsy and the possibility of inadequate tumor cell content in samples, which may prevent sufficient biomarker detection, limit its clinical application.5 In addition, exhaled gas analysis for the diagnosis of lung cancer, as an emerging noninvasive diagnostic method, also has a high potential, a study6 have shown that typical compounds such as isoprene, acetone, and methanol are reduced in the exhaled gas of patients with lung cancer when compared to healthy controls, while many other compounds are only found in patients with lung cancer, but many of the compounds observed in the exhaled breath have never been previously studied in medical or biochemistry to allow effective identification of volatile compounds in exhaled breath, and therefore the method is not currently widely used in the clinic.
With the advancement of precision medicine, liquid biopsy has emerged as a promising non-invasive technique with significant potential in the diagnosis and management of lung cancer. Liquid biopsy involves the analysis of biomarkers such as circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), and exosomes or Extracellular vesicles (EVs) in bodily fluids like blood, urine, or saliva, enabling the acquisition of crucial tumor-related molecular information under non-invasive conditions.7 Compared to traditional invasive tissue biopsies, liquid biopsy offers several advantages, including ease of sample collection, higher specificity, and less susceptibility to tumor heterogeneity. Consequently, liquid biopsy demonstrates considerable potential not only in early diagnosis and dynamic monitoring but also in evaluating treatment efficacy, detecting resistance, and predicting recurrence.8 However, liquid biopsy faces certain technical challenges, such as limited sensitivity and specificity, as well as variability and complexity in data interpretation, which currently restrict its widespread clinical application.9 We summarize the diagnostic methods that are currently widely used with the clinic in Table 1.
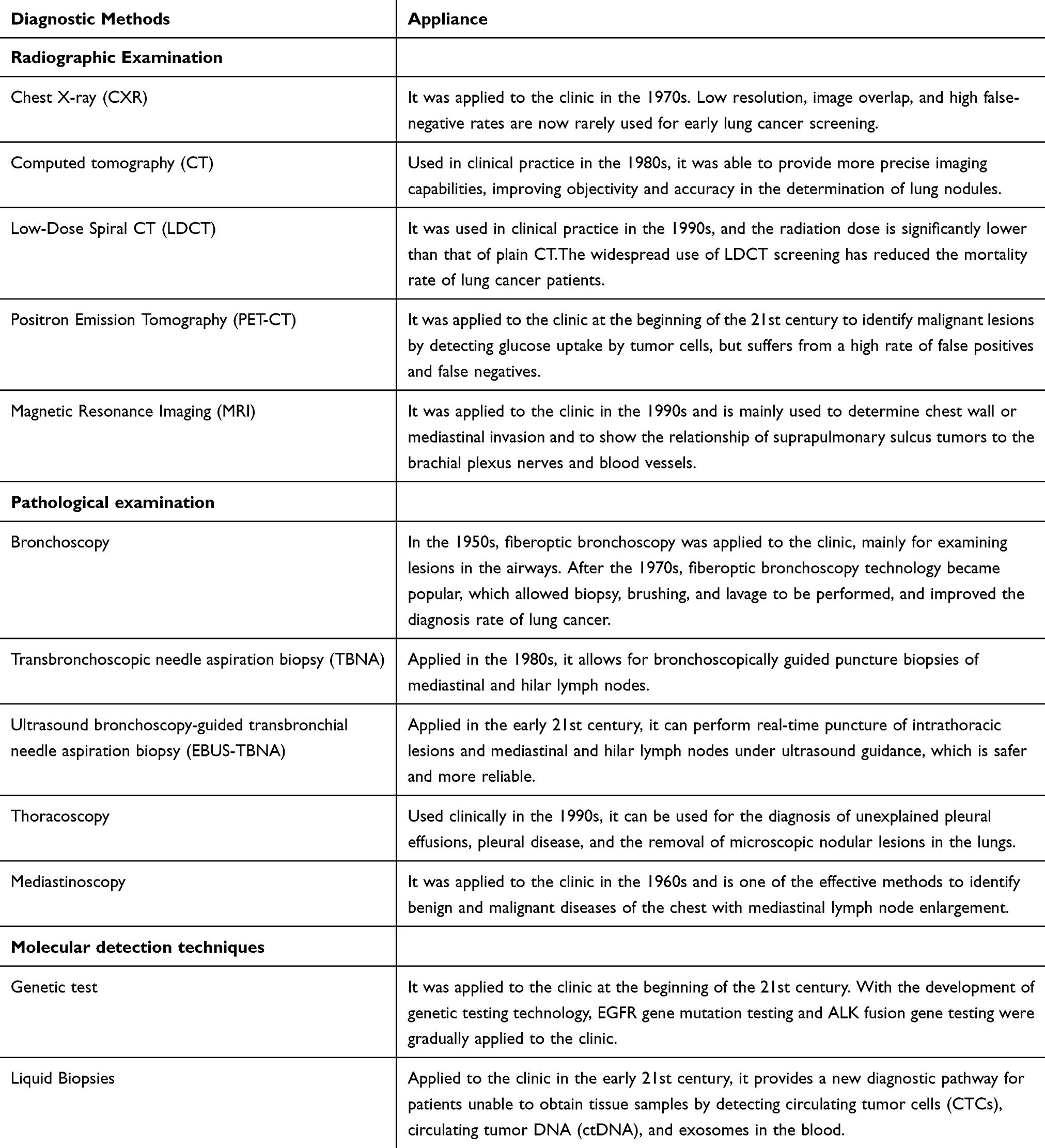 |
Table 1 Lung Cancer Diagnostic Program |
Given the distinct advantages and limitations of liquid biopsy and traditional diagnostic methods, this review aims to thoroughly examine the integration and complementarity of these approaches in the diagnosis and management of lung cancer. Specifically, it will analyze the synergistic effects of combining liquid biopsy with tissue biopsy, imaging techniques, and pathological analysis. The review proposes a multimodal diagnostic strategy that integrates liquid biopsy with traditional methods, accompanied by specific clinical operational procedures. This multimodal approach is designed to provide more comprehensive and precise diagnostic information by combining various diagnostic techniques, thus optimizing personalized treatment plans for patients. This integration not only addresses the limitations of individual methods but also enhances the accuracy of lung cancer diagnosis and the sensitivity of treatment monitoring through the synergistic effects of the combined approaches. Additionally, the review will discuss potential challenges in implementing multimodal diagnostic pathways, such as data standardization and the complexity of clinical application, and will propose solutions to these challenges. Ultimately, this review aims to offer theoretical support for the integrated use of liquid biopsy and traditional diagnostic methods and to provide direction for future research and clinical practice in the field of lung cancer.
The Role of Traditional Diagnostic Techniques in Lung Cancer Management
Traditional diagnostic techniques for lung cancer, including imaging (chest X-rays, CT, PET-CT), tissue biopsy, bronchoscopy, and sputum cytology, are vital for initial screening, accurate staging, and prognosis.10 While imaging assesses lesion size and extent, it falls short in determining tumor pathology. Histopathology, the diagnostic gold standard, provides critical molecular insights, while bronchoscopy aids in central lung cancer diagnosis. Despite its lower sensitivity, sputum cytology remains valuable in certain cases. To enhance detection of micro-lesions and molecular features, these methods should be integrated with advanced modern technologies.
Tissue Biopsy
Tissue biopsy remains the gold standard for diagnosing and classifying lung cancer by procuring a tumor tissue sample for pathological examination. It provides essential pathological and molecular insights, crucial for identifying tumor types, assessing disease progression, and formulating treatment strategies.11 Tissue biopsy allows for direct observation of cellular morphological changes, facilitating accurate cancer classification and grading. Advances in molecular diagnostics have further enhanced its utility, enabling the detection of gene mutations and protein expressions that inform targeted and immunotherapeutic approaches.12
The principal advantage of tissue biopsy lies in its provision of high-resolution pathological analysis. Microscopic examination allows pathologists to accurately identify the histological types of tumors, such as squamous cell carcinoma, adenocarcinoma, and large cell carcinoma.13 This is crucial for determining the specific type and grade of lung cancer. Additionally, the application of techniques such as immunohistochemistry (IHC) and in situ hybridization (ISH) enhances the diagnostic value of tissue biopsy at the molecular pathological level.14 For example, detection of Epidermal growth factor receptor (EGFR) mutations and ALK fusion genes can further guide the development of personalized treatment strategies. Furthermore, tissue biopsy typically provides a relatively abundant sample volume, especially in post-surgical specimen analysis. This ample sample allows for extensive analysis, yielding comprehensive pathological and molecular information. In some cases, tissue biopsy samples can even be subdivided for different types of tests, such as pathological analysis, molecular diagnostics, and experimental research.15
Despite the high-quality diagnostic information provided by tissue biopsy, its invasive nature presents a significant drawback. Traditional methods such as percutaneous needle biopsy or bronchoscopy-guided biopsy, while technically well-established, still carry certain risks including pneumothorax, bleeding, and infection.16 In lung cancer patients, the incidence of pneumothorax following lung biopsy ranges from 17% to 38%.17 Additionally, for some elderly or medically compromised patients, tissue biopsy may be contraindicated, complicating the diagnostic process. Furthermore, in certain instances, the sample obtained through tissue biopsy may be insufficient for comprehensive analysis. This is particularly true for fine-needle aspiration (FNA), where the limited number of cells retrieved may not provide adequate histological information. For 20–30% of patients with advanced non-small cell lung cancer (NSCLC), obtaining a sufficient quantity of suitable tissue for biomarker analysis can be challenging.17 This insufficiency may lead to ambiguous diagnoses and potentially impact treatment decisions. Moreover, inadequate sample volume may also restrict molecular testing, thereby affecting the evaluation of targeted and immunotherapy options.
Imaging Examination
Imaging examination are a crucial component in the management of lung cancer, encompassing the entire spectrum from early screening to advanced follow-up. These examinations not only aid in the diagnosis and staging of lung cancer but also play a significant role in assessing treatment response and monitoring for recurrence.18 Commonly employed imaging modalities include chest X-ray, computed tomography (CT), positron emission tomography-computed tomography (PET-CT), and magnetic resonance imaging (MRI).19 Among these, CT and PET-CT are the preferred tools for diagnosing and managing lung cancer,20 while MRI offers unique advantages in evaluating brain metastases and other soft tissue lesions.21
CT scanning is the most commonly utilized tool for lung cancer screening, especially among high-risk populations such as long-term smokers. Low-dose spiral CT has been demonstrated to significantly reduce lung cancer mortality rates. In comparison to traditional chest X-rays, CT scans provide high-resolution images that clearly depict the size, shape, and anatomical relationships of pulmonary masses, facilitating precise determination of lesion location and dimensions.22 PET scanning, using tracers like 18F-FDG, offers images reflecting tumor metabolic activity, which is crucial for differentiating between malignant and benign lesions. This technique is particularly advantageous for lymph node staging and detecting distant metastases.23 MRI, with its superior soft tissue resolution, is the preferred modality for evaluating brain metastases from lung cancer.24 Moreover, imaging plays a vital role in treatment planning and efficacy assessment, allowing physicians to tailor therapeutic strategies based on imaging results, thereby enhancing patient survival rates and quality of life.
Despite the pivotal role of imaging in lung cancer management, its limitations are significant. First, imaging has limited specificity, making it challenging to differentiate between benign and malignant nodules, particularly in the presence of inflammation or other benign conditions, which may result in false-positive findings and lead to misdiagnosis or overdiagnosis.25 This issue is particularly pronounced with CT and PET-CT, which, although highly sensitive for detecting early lung cancer, still struggle with distinguishing inflammatory nodules from malignant ones. Additionally, imaging has limited resolution for detecting micro-lesions, especially in tumors with low metabolic activity, such as certain types of NSCLC, where PET-CT sensitivity may be compromised.26 The interpretation of imaging results is highly dependent on the radiologist’s expertise, and variability in interpretation can lead to differing clinical decisions.27
Imaging plays an irreplaceable role in the early detection, accurate staging, and efficacy monitoring of lung cancer, significantly advancing personalized treatment. However, it is essential to complement imaging with other diagnostic methods to enhance diagnostic accuracy and comprehensiveness, thereby minimizing the impact of its limitations on patient management.
Bronchoscopy and Sputum Cytology
Bronchoscopy is an indispensable tool in the management of lung cancer, particularly in the diagnostic and staging processes. It allows for direct visualization of the airways and the acquisition of tissue biopsy samples for pathological analysis to confirm or exclude the presence of lung cancer.28 The primary advantages of bronchoscopy lie in its directness and flexibility, providing additional diagnostic evidence when imaging studies fail to yield definitive results. Moreover, advancements in technology have evolved bronchoscopy from traditional rigid bronchoscopes to more advanced fiberoptic bronchoscopes with higher resolution and improved maneuverability. Additionally, endobronchial ultrasound (EBUS) combined with FNA allows for the collection of deep lung tissue samples without damaging major blood vessels.29 This technique plays a crucial role in lung cancer staging, particularly in assessing mediastinal and hilar lymph node metastases, with precision that significantly surpasses traditional imaging methods.30 However, bronchoscopy has limitations. It may be challenging to access peripheral lung cancers, especially those located in small airways or peripheral lung parenchyma, leading to inadequate sampling or inaccurate diagnoses.31 Furthermore, as an invasive procedure, bronchoscopy carries risks of complications such as bleeding, infection, or pneumothorax, especially if performed improperly or in patients with serious underlying conditions.32
Sputum cytology is a non-invasive method for lung cancer screening and diagnosis, particularly useful for early detection of central lung cancers. By analyzing sputum samples, cytology can detect the presence of cancer cells, indicating a potential lung cancer diagnosis.33 Due to its simplicity and minimal patient burden, sputum cytology is often used as an initial screening tool for high-risk groups, including long-term smokers and individuals with chronic bronchitis or other respiratory diseases. Compared to other diagnostic methods, sputum cytology is advantageous for its low cost and widespread accessibility, making it a significant screening tool, especially in resource-limited settings.34 Nonetheless, sputum cytology has lower sensitivity, particularly for peripheral lung cancers and non-squamous cell carcinomas, due to the difficulty in detecting cancer cells in the sputum.35 The quality of sputum samples also impacts diagnostic accuracy, with improper collection or interference from non-tumor cells potentially leading to false-negative results.36 Therefore, while sputum cytology has its value in lung cancer management, it is not sufficient on its own for accurate diagnosis. It typically needs to be complemented by other diagnostic methods, such as imaging studies and bronchoscopy, to enhance lung cancer detection rates and diagnostic precision.
The Concept and Common Types of Liquid Biopsy
Liquid biopsy refers to the technique of detecting biomarkers in body fluids such as blood, urine, saliva, pleural fluid, and cerebrospinal fluid for tumor diagnosis and monitoring. These biomarkers include circulating tumor cells, circulating tumor DNA, cell-free DNA (cfDNA) including mRNA, long non-coding RNA (lncRNA), microRNA (miRNA), extracellular vesicles (EVs), tumor-derived platelets, proteins, and metabolites.37,38 This method is characterized by its non-invasive nature, real-time monitoring capabilities, and its ability to reflect the overall tumor burden. Additionally, it helps mitigate the impact of tissue heterogeneity on tumor molecular profiling. Consequently, liquid biopsy shows significant potential in early cancer detection, molecular profiling, treatment response monitoring, and recurrence prediction.39,40 Common biomarkers in liquid biopsy include CTCs, ctDNA, and EVs/exosomes.
Circulating Tumor Cells (CTCs)
The concept of CTCs was first introduced by the Australian physician Ashworth in 1869.41 CTCs are tumor cells that have shed from primary or metastatic tumors and entered the bloodstream. In the peripheral blood, tumor cells may undergo apoptosis or phagocytosis. However, some tumor cells can evade these processes through epithelial-mesenchymal transition (EMT).42 EMT endows these cells with enhanced motility, increased adhesion, and the ability to penetrate vascular walls, thus augmenting their invasiveness and metastatic potential.43 As CTCs reflect the heterogeneity and dynamic changes of tumors, their detection and analysis provide valuable insights for cancer diagnosis and treatment.
Despite their importance, the extraction of these extremely rare CTCs from circulating blood has posed significant technical challenges, and it has only been over the past century that the critical role of CTCs in cancer metastasis has been progressively elucidated.44 Advances in CTC isolation technologies over the past two decades have enabled detailed studies of CTC biology. Current primary methods for CTC detection include 1) Physical property-based separation methods: These methods exploit differences in size, density, and electrophoretic mobility between CTCs and the majority of normal blood cells to isolate CTCs.45 2) Biological property-based separation methods: These techniques utilize the expression of specific biomarkers (eg, EpCAM) and immunological separation technologies, such as positive selection, negative selection, immunomagnetic bead separation, and fluorescence-activated cell sorting (FACS), to capture and isolate CTCs.46 3) Microfluidic chip technology: This approach combines physical properties and biomarker-based selectivity, capturing and isolating CTCs through fluid flow in microchannels and specific antibody interactions. This method offers high sensitivity and specificity, and can process small sample volumes within a shorter timeframe.47 4) Genomic separation methods: These involve analyzing blood samples for the presence of specific CTC-associated gene expressions (eg, CK19, MUC1, CEA) to indirectly detect and isolate CTCs.48
CTCs, as biomarkers carrying tumor morphological and genetic information, hold significant clinical value. Their detection can provide a range of information, including tumor genotype, classification, and stratification.39 Research indicates that CTCs play a pivotal role in the early diagnosis of lung cancer, metastasis prediction, recurrence monitoring, and assessment of treatment efficacy, offering real-time insights into treatment responses. Huang et al further highlighted that CTC detection is closely associated with tumor clinical-pathological features and serves as an important prognostic tool, with detection results significantly correlating with disease-free survival and overall survival rates.49 Some studies have confirmed a significant association between CTC counts and patient survival. For instance, in breast cancer patients, an increase in CTC count to over one per 7.5 milliliters of blood is associated with a significantly shorter progression-free survival (PFS), and a count exceeding five correlates with a markedly reduced overall survival (OS).50 Analysis of CTCs expressing specific molecules can also effectively monitor tumor metastasis and recurrence. Ishiguro et al found that the presence of N-cadherin positive CTCs preoperatively in gastric cancer patients was associated with a recurrence rate of up to 90%.51 Additionally, dynamic changes in CTCs can be used to monitor treatment efficacy. For example, Pierga et al observed that breast cancer patients whose CTC counts fell to below five per 7.5 milliliters of blood after three cycles of anti-HER2 treatment showed better therapeutic responses.50 In castration-resistant prostate cancer (CRPC) patients, changes in CTC counts can reflect treatment effects even earlier than prostate-specific antigen (PSA) levels.52 Genomic sequencing of CTCs can reveal various gene mutations, including those in estrogen receptor gene (ESR1), PIK3CA gene, and fibroblast growth factor receptor gene (FGFR2). Testing drug sensitivity on these mutated CTCs can aid in developing more precise personalized treatment plans.53 However, CTC detection and analysis technologies still require further optimization for better translation from laboratory research to clinical application. Kang et al found that using a centrifugal microfluidic system for CTC separation in gastric cancer diagnosis had a high false-negative rate of up to 38%, indicating that sensitivity needs improvement.54 Since cancer patients express specific biomarkers, detecting CTCs with high expression of these biomarkers can significantly reduce false negatives and improve detection sensitivity.55 Current technologies are continuously evolving. For instance, the RUBYchip™ technology identifies CTCs based on cell size and shape, overcoming the limitations of traditional label-dependent methods and significantly improving CTC capture rates.56 Overall, CTCs provide rich molecular and genetic information and enable personalized treatment through dynamic monitoring. However, widespread clinical application of CTCs still faces numerous technical and methodological challenges.
Circulating Tumor DNA (ctDNA)
ctDNA is composed of DNA fragments released into the bloodstream by tumor cells. Unlike CTCs, ctDNA enters the bloodstream through apoptosis, necrosis, or active secretion, and thus is more broadly present in body fluids. ctDNA carries genetic information from tumors, including alterations such as point mutations, copy number variations, deletions, and methylation patterns.57 Consequently, the detection of ctDNA has emerged as a crucial tool in precision oncology, demonstrating substantial potential particularly in driving gene mutation detection, monitoring resistance mutations, and assessing tumor burden.
Various technologies are available for the detection and analysis of ctDNA, including: 1) Digital PCR (dPCR): This method partitions samples into numerous micro-reactors and quantitatively measures fluorescence signals. Its high sensitivity and specificity allow for precise identification and quantification of low-abundance mutations in ctDNA, making it particularly suitable for detecting low-frequency mutations.58 2) Quantitative PCR (qPCR): This technique quantifies specific gene mutations. Although its sensitivity is lower than dPCR, qPCR is often used for known gene mutations due to its simplicity and lower cost, although it may have limitations in detecting low-abundance mutations.59 3) Hybrid Capture-NGS: Combining specific oligonucleotide probes with ctDNA target sequences for enrichment, followed by next-generation sequencing, this method is suited for comprehensive analysis of multiple gene loci and can perform deep sequencing.60 4) Methylation-Specific PCR (MSP): Utilizing specific primers to amplify methylation states at specific loci in ctDNA, MSP shows promise for detecting methylation changes in cancer-related genes, especially useful for early cancer detection.61 5) Next-Generation Sequencing (NGS): This technique performs deep sequencing on ctDNA, detecting various gene mutations, insertions, deletions, copy number variations, and gene fusions with high sensitivity and throughput, covering entire genomes or multiple target genes, and is currently a mainstream method for ctDNA analysis.62 6) Bayesian Analysis and Machine Learning Algorithms: These methods efficiently process and interpret complex data, significantly enhancing the sensitivity and specificity of ctDNA detection, and are particularly suitable for large-scale, multi-gene, or whole-genome projects.63 Each technique has specific advantages and limitations, and researchers often select appropriate methods based on research goals, sample characteristics, and the type of mutations being analyzed. In practice, combining multiple methods is common to improve the accuracy and comprehensiveness of ctDNA detection.
Given that ctDNA can be released from various tumor regions or multiple lesions, it better represents the molecular heterogeneity of a particular cancer compared to single-site biopsies. De Mattos-Arruda et al found that ctDNA levels in cerebrospinal fluid (CSF) of central nervous system tumor patients were higher than in plasma. Analysis and sequencing of CSF ctDNA provide a more comprehensive characterization of genomic changes in brain tumors and aid in diagnosing leptomeningeal disease.64 Furthermore, deep sequencing of ctDNA can uncover tumor heterogeneity and gene mutations present only in a subset of cells, which typically requires extensive CTCs or multiple tissue biopsies for equivalent information. For example, another study by De Mattos-Arruda revealed that ctDNA analysis of plasma samples identified all mutations present in primary and/or liver metastatic tumors, which were not fully detectable in primary and/or liver metastatic tumors alone.65 Importantly, ctDNA can provide information on tumor size, reflecting disease progression and response to therapy. Studies have shown that mutation allele frequency (VAF) of ctDNA is linearly related to tumor volume in NSCLC and high-grade serous ovarian cancer (HGSOC).66,67 ctDNA also has prognostic value; for instance, the presence of ctDNA after curative surgery or chemotherapy is a strong marker of cancer recurrence and poor prognosis. Its predictive capacity for recurrence has been validated in colorectal cancer, ovarian cancer, lung cancer, and breast cancer patients.66,68,69 Additionally, ctDNA analysis can identify tumor resistance markers, such as KRAS mutations in colorectal cancer patients undergoing anti-EGFR therapy,70 and PIK3CA, MED1, EGFR mutations in breast cancer patients,71 as well as EGFR T790M resistance mutations in lung cancer patients treated with EGFR-targeted TKIs.72 WANG et al found that HER2+ ctDNA levels are a useful tool for monitoring the efficacy of trastuzumab therapy; HER2+ ctDNA levels decrease following treatment but rebound with the development of resistance.73 These advantages position ctDNA as a promising biomarker in precision oncology. However, challenges such as low ctDNA levels in plasma, gene variations due to cellular aging, and insufficient detection sensitivity need to be addressed.74,75
Extracellular Vesicles (EVs) and Exosomes
EVs is membrane-bound vesicles released by cells, encompassing exosomes, microvesicles, and other vesicles.76 Exosomes, a specific type of EV, typically range from 30 to 150 nanometers in diameter and are primarily released via the endosome-lysosome pathway. They carry a variety of biomolecules, including proteins, RNA, DNA, and lipids.77 Despite some subtle differences in definition and characteristics, the terms EVs and exosomes are often used interchangeably in liquid biopsy contexts. In cancer, exosomes are considered critical mediators of intercellular communication, playing significant roles in tumor progression, metastasis, and resistance development. The nucleic acid and protein components of exosomes reflect the state of their originating cells, making exosome analysis a promising tool for liquid biopsies.78
Techniques for detecting and analyzing exosomes include ultracentrifugation, electrophoresis, immunocapture, nanoparticle tracking analysis, and mass spectrometry: 1) Differential Centrifugation: One of the most commonly used methods for exosome separation, it involves multiple centrifugation steps to isolate exosomes from other extracellular vesicles and macromolecules. Although simple, this method may have limitations in efficiency and purity and requires extended processing time.79 2) Immunoaffinity Capture: This method employs antibodies specific to exosome membrane markers (eg, CD63, CD81, CD9) to enrich exosomes using immunoaffinity columns or magnetic beads. While it provides high purity, it is limited by the availability of specific antibodies and is challenging for large-scale applications.80 3) Nanoparticle Tracking Analysis (NTA): Utilizing laser scattering technology, NTA measures the size and concentration of exosomes, allowing real-time tracking of nanoparticle movement to analyze size distribution and quantity. Although highly sensitive, this method may have detection errors in mixed samples.81 4) Mass Spectrometry (MS): Mass spectrometry analyzes proteins, lipids, and metabolites within exosomes, offering high-throughput and high-sensitivity profiling of exosome components.82
Exosomes have potential clinical applications as diagnostic and prognostic biomarkers in various diseases, including cancer, neurodegenerative diseases, and cardiovascular conditions. They serve as crucial regulators in tumorigenesis and progression, influencing adhesion, signaling pathways, inflammatory responses, and immune evasion. Exosomes also play vital roles in tumor diagnosis, treatment evaluation, and prognosis. Research by Peinado et al demonstrated that exosomes can penetrate blood vessels, induce inflammation, and recruit bone marrow progenitor cells to promote tumor metastasis.83 Hoshino et al revealed that lung-derived exosomes redirect bone-metastatic tumor cells. Different integrins on exosomes are associated with metastasis to various organs, with α6β4 and α6β1 linked to lung metastasis, and αvβ5 associated with liver metastasis. Thus, the integrin expression profile of plasma exosomes from cancer patients can serve as a prognostic factor for predicting future metastatic sites.84 Moreover, exosomal RNA, DNA, and protein can be used to detect actionable mutations and other molecular changes. For instance, Qu et al identified exosomes carrying EGFR mutations in lung adenocarcinoma, with exosome gene testing showing 100% sensitivity and 96.55% specificity.85 Exosomes are also explored for therapeutic purposes, such as drug delivery carriers and immune modulation. For example, engineered exosomes combined with the anticancer drug 5-FU and the miR-21 inhibitor oligonucleotide (miR-21i) were delivered to Her2-expressing cancer cells, showing significant antitumor effects and reversing drug resistance, markedly enhancing the cytotoxicity of 5-FU in resistant colorectal cancer cells.86 However, due to the heterogeneity and complexity of exosomes, further research and technological advancements are needed for clinical applications, such as improving exosome isolation purity, standardizing detection processes, and interpreting the biological significance of various exosome components.87,88
Application of Liquid Biopsy in Comprehensive Management of Lung Cancer
With advances in understanding the biological characteristics of lung cancer and the continuous development of diagnostic technologies, liquid biopsy has emerged as a crucial tool in the comprehensive management of lung cancer (Figure 1). Due to its non-invasive nature and ability to provide real-time, dynamic monitoring, liquid biopsy is transforming traditional diagnostic approaches. It plays a pivotal role in early detection, guiding personalized treatment strategies, and predicting prognosis. By analyzing key biomarkers in bodily fluids such as blood, cerebrospinal fluid, and pleural effusion, liquid biopsy offers clinicians accurate and reliable insights, thereby enhancing the overall management of lung cancer.
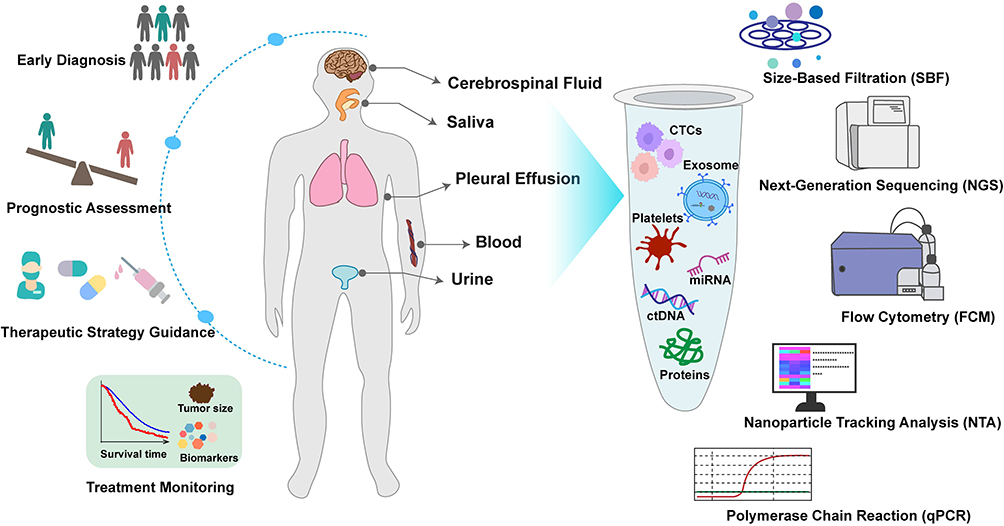 |
Figure 1 Clinical application of liquid biopsy in lung cancer management.Liquid biopsy in lung cancer management involves the non-invasive collection of bodily fluids such as cerebrospinal fluid, saliva, pleural effusion, blood, and urine. Advanced separation and detection techniques are applied to analyze key biomarkers, including circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), exosomes, platelets, microRNAs (miRNAs), and proteins. These biomarkers contribute to early diagnosis, prognosis evaluation, the development of personalized treatment plans, and dynamic monitoring of therapeutic responses, providing a minimally invasive and real-time approach to optimizing lung cancer care. |
Early Diagnosis
In the preliminary diagnosis of lung cancer, early detection and accurate staging are critical for determining patient prognosis and treatment strategies. Traditional imaging modalities, such as chest CT and PET-CT, play a significant role in early screening and staging. However, their sensitivity and specificity can be affected by lesion size and tissue characteristics, which may lead to false negatives or false positives, particularly when detecting small lesions or atypical imaging findings.26 Liquid biopsy, as an emerging non-invasive diagnostic tool, shows substantial potential in the early diagnosis of lung cancer. By analyzing biomarkers such as ctDNA, CTCs, and EVs in blood samples, liquid biopsy provides key information about tumor presence and characteristics.37 Compared to traditional tissue biopsies, liquid biopsy offers advantages such as ease of sampling, high repeatability, and the ability to monitor tumor changes in real-time, making it increasingly valued in early lung cancer detection.89
Phallen et al analyzed ctDNA mutation profiles from 58 cancer-related genes and found that 62% of lung cancer patients had positive ctDNA results. Furthermore, ctDNA sensitivity increased with disease stage: 45% in stage I, 72% in stage II, 75% in stage III, and 83% in stage IV.90 Klein et al combined artificial intelligence with analysis of targeted ctDNA methylation, evaluating ctDNA specificity and sensitivity. Their study revealed a sensitivity of 75% for ctDNA methylation in lung cancer patients. Moreover, ctDNA detection rates were closely correlated with tumor burden, with positivity rates of 20.9% for stage I, 79.5% for stage II, 90.7% for stage III, and 95.2% for stage IV.91 In another study involving all histological types of lung cancer, Mathios et al used machine learning models to detect whole-genome ctDNA fragment patterns in 365 cancer-risk individuals, finding an 80% detection specificity for ctDNA across all stages. Sensitivity was 91% for stage I/II and 96% for stage III/IV.92 This approach provides a convenient method for non-invasive lung cancer detection.
CTCs, as another liquid biopsy biomarker, also hold significant value in the early diagnosis of lung cancer. However, the limited presence of CTCs in the blood poses a major challenge for timely diagnosis of early-stage lung cancer. Advances in detection technology are gradually uncovering the application value of CTCs in early tumor diagnosis.93 Notably, dPCR-based CTC isolation and capture techniques can detect mutations in KRAS and EGFR genes relevant to treatment decisions. Additionally, the implementation of this technology and NGS for CTCs has increased the detection rate of CTCs in stage I/II non-small cell lung cancer to 62.5%.93,94 Pfarr et al demonstrated that CTC NGS technology could identify four high-frequency mutation genes (NOTCH1, IGF2, EGFR, and PTCH1) and ten lung cancer-specific metabolites, which have potential clinical value in early lung cancer diagnosis.95,96 The unique rarity of CTCs in non-cancerous individuals underscores their specificity as biomarkers for early lung cancer diagnosis. However, there is a pressing need to continuously develop and optimize other technologies to enhance CTC detection sensitivity.
Exosomes, small vesicles secreted by cells, contain a wealth of molecular information, including proteins, RNA, and DNA. Tumor-derived exosomes have been identified as potential biomarkers for early lung cancer diagnosis.97 Identifiable lung cancer-associated markers, such as PTX3 and THBS1, as well as exosome markers like CD63, in plasma, aid in lung cancer screening and diagnosis. A study utilizing a machine learning-based nanoparticle technology strategy successfully distinguished early lung cancer from benign lung conditions, achieving sensitivities and specificities of 92.3% and 100%, respectively, compared to traditional CT scan sensitivities (92.3%) and specificities (71.4%).98 Currently, strategies for early cancer diagnosis using exosomes focus on detecting miRNA or lncRNA carried by exosomes. Research indicates that EVs can detect significant and stable increases in miR-520c-3p and miR-1274b in non-small cell lung cancer patients, with levels decreasing significantly after tumor resection, highlighting their potential value in early diagnosis.99 However, standardization of exosome isolation and detection technologies is still needed to advance their widespread application in cancer early diagnosis, and further clinical studies are essential to validate their efficacy.
Overall, liquid biopsy through the detection of ctDNA, CTCs, and EVs/exosomes provides new insights and tools for early lung cancer diagnosis. While these technologies still require improvements in sensitivity, their advantages in specificity and real-time monitoring make them important complementary methods for early screening and diagnosis of lung cancer in the future.
Therapeutic Strategy Guidance
Personalized treatment has emerged as a significant advancement in the management of lung cancer in recent years, with liquid biopsy playing an increasingly critical role in shaping treatment strategies. Liquid biopsy allows clinicians to monitor changes in molecular characteristics of patients in real-time, thereby optimizing therapeutic decisions. By analyzing ctDNA, CTCs, and EVs in patient bodily fluids, liquid biopsy provides insight into the tumor’s genetic mutation profile, which is essential for guiding targeted and immunotherapies.
Firstly, liquid biopsy aids in identifying driver gene mutations and informing the selection of targeted therapies. EGFR mutations are among the most common oncogenic driver mutations in NSCLC. The incidence of EGFR mutations is approximately 15% in the United States, but it can be as high as 62% in Asian populations.100,101 EGFR tyrosine kinase inhibitors (TKIs) are the standard first-line systemic treatment for patients with EGFR-mutant lung cancer.102 Thus, detecting EGFR mutations is crucial for guiding the use of EGFR TKIs. A meta-analysis encompassing 40 studies evaluated the impact of ctDNA on EGFR mutations detected in tissue and liquid biopsies. The study found that ctDNA detection of EGFR mutations had a pooled sensitivity of 68%, specificity of 98%, and diagnostic odds ratio of 88%, indicating that peripheral liquid biopsy has high specificity for detecting EGFR mutations in NSCLC patients.103 Thompson et al demonstrated that NGS based on liquid biopsy provided a higher guideline-recommended treatment rate and significantly shortened the time before first-line treatment compared to traditional tissue-based NGS,104 highlighting the value of liquid biopsy in guiding lung cancer treatment strategies.
Tissue biopsy is not always feasible in patients with advanced lung cancer, especially those who have received prior therapy and have progressed, and may fail to detect acquired resistance mutations, whereas serial plasma sampling allows for the study of dynamic changes in ctDNA and the repeated detection of the emergence of acquired resistance mutations in a way that tissue biopsy does not.105 Moreover, baseline ctDNA load and dynamic changes have prognostic implications, and the use of ositinib guided by plasma ctDNA epidermal growth factor receptor (EGFR) status achieves the expected response rate, progression-free survival, and overall survival.
Furthermore, liquid biopsy enables early identification of treatment efficacy and timely adjustment of treatment plans to extend patient survival. In NSCLC patients undergoing surgery, chemotherapy, radiotherapy, targeted therapy, or immunotherapy, reductions in CTC concentration are associated with tumor treatment response, while increases in CTC count correlate with disease progression.106 The expression of PD-L1 in tumor cells and tumor-infiltrating immune cells is associated with improved efficacy of anti-PD-1/PD-L1 inhibitors in advanced NSCLC. Research shows that the PD-L1 status in CTCs is highly correlated with PD-L1 expression in tumor tissues, with a concordance rate of 93%. Moreover, patients with PD-L1 positive CTCs or immune cells have shown poorer survival trends after cisplatin-based chemotherapy. These findings suggest that CTC evaluation has the potential to serve as a non-invasive, real-time tool for assessing PD-L1 expression, aiding treatment decisions for advanced NSCLC patients.107
The potential of liquid biopsy in monitoring lung cancer drug resistance is also noteworthy. Murtaza et al conducted ctDNA exon sequencing on plasma samples from six patients with advanced cancer and found that increased expression of mutated alleles in plasma was closely associated with the development of resistance during different treatments. Their results indicate that exon analysis of circulating tumor DNA can serve as a non-invasive complement to traditional biopsy methods for identifying mutations associated with cancer drug resistance.71 Buttitta et al found that plasma monitoring of ctDNA could early identify resistance mutations in NSCLC patients treated with EGFR-TKIs. Among EGFR-positive patients, 89% showed significant plasma response after one month of treatment, while 11% developed resistance mutations, suggesting that plasma monitoring could rapidly identify and detect resistance mutations early.108
In a Phase II APPLE trial, longitudinal monitoring of ctDNA EGFR T790M enabled timely conversion from gefitinib to osimertinib, resulting in an 18-month PFS rate of 67.2%, significantly higher than the survival rate of patients who continued on gefitinib or switched to osimertinib only after disease progression (53.5%). Furthermore, patients who received timely conversion from gefitinib to osimertinib showed a superior median PFS compared to those on other treatment regimens. This study demonstrates that continuous monitoring of ctDNA T790M aids in optimizing treatment strategies and improving patient PFS and overall survival.109
In summary, liquid biopsy provides real-time, dynamic molecular information about tumors, significantly enhancing the ability to develop tailored treatment strategies for lung cancer. Although liquid biopsy technologies require further optimization and standardization, their application in lung cancer treatment holds substantial promise.
Predicting Prognosis
Liquid biopsy has demonstrated significant clinical value in predicting the prognosis of lung cancer, particularly in NSCLC patients. Utilizing liquid biopsy markers such as ctDNA can effectively predict patient outcomes, thereby aiding in the formulation of more personalized treatment strategies.
Zhang et al employed the Amplification Refractory Mutation System (ARMS) PCR technique and found that changes in EGFR mutation status in plasma ctDNA after EGFR-TKI therapy were closely related to prognosis. Specifically, patients whose T790M mutation status changed from negative to positive had a significantly shorter progression-free survival compared to those whose EGFR mutation status remained unchanged. This underscores the importance of closely monitoring EGFR mutation status in plasma ctDNA for predicting treatment efficacy and prognosis in NSCLC patients.110 Additionally, Hartmaier et al discovered that the clearance rate of EGFRm ctDNA was associated with longer PFS in NSCLC patients, with overall response rate (ORR) and PFS being consistent. Continuous ctDNA monitoring not only predicts the longitudinal development of acquired resistance mutations but also reveals that about half of the patients exhibit clear resistance mechanisms during savolitinib combined with osimertinib treatment. However, limitations exist in using ctDNA to analyze resistance mechanisms, particularly in detecting copy number variations.111
Another study explored the role of liquid biopsy in predicting postoperative relapse risk. Chaudhuri et al, through CAPP-seq analysis, demonstrated that ctDNA analysis can reliably detect molecular residual disease (MRD) after lung cancer treatment and identify it months before radiographic progression. The study showed that 94% of patients who experienced recurrence had detectable ctDNA in the first post-treatment blood sample, confirming the accuracy of MRD identification. Therefore, early detection of ctDNA mutation profiles aids in the early intervention of personalized adjuvant therapy.112 An additional study evaluated the optimal timing for ctDNA kinetics and MRD detection in NSCLC patients. Chen et al investigated perioperative ctDNA dynamics and found that ctDNA levels dropped rapidly after tumor resection, with a median half-life of 35.0 minutes. Patients with detected MRD had a significantly slower ctDNA half-life, indicating a higher risk of recurrence. Furthermore, ctDNA detection on postoperative day 3 could serve as a baseline for post-surgical lung cancer monitoring, aiding in early identification of recurrence risk.113 MicroRNAs have emerged as useful clinical biomarkers in tissue and liquid biopsies. Sanchez-Cabrero et al assessed seven candidate miRNAs in 120 samples from 88 NSCLC patients, finding that miR-124 levels increased during disease progression and had potential as a disease progression marker in both early and late stages. Bioinformatics analysis further identified KPNA4 and SPOCK1 as potential miR-124 targets in NSCLC. Results suggest that miR-124 levels could help differentiate early NSCLC patients with higher relapse risk.114
Interestingly, Eslami-S et al investigated whether CTCs, ctDNA, and EVs, either alone or in combination, could predict prognosis in heterogeneous unbiased NSCLC patients. Their data indicated that the combined analysis of CTCs and high PD-L1+ sEV concentrations effectively predicted OS and PFS in NSCLC patients. The combination of CTCs and high PD-L1+ sEV concentrations was significantly associated with poorer prognosis, independent of ctDNA mutations. Combined biomarker analysis may contribute to more accurate prognosis assessment in advanced NSCLC patients.115
In summary, the application of liquid biopsy in lung cancer prognosis prediction offers a non-invasive and efficient means to accurately forecast patient survival and relapse risk, providing crucial guidance for clinical decision-making.
Integration Strategies for Liquid Biopsy and Other Diagnostic Methods
The Concept and Necessity of Multimodal Diagnostic Approaches
The integration of various diagnostic methods is increasingly recognized in the contemporary management of lung cancer. The core concept of a multimodal diagnostic approach is to enhance diagnostic accuracy and comprehensiveness by combining multiple diagnostic methods, such as liquid biopsy, tissue biopsy, imaging examination, and pathological analysis. Lung cancer, characterized by its high heterogeneity, exhibits significant variability in its biological behavior and clinical presentation due to individual patient differences.116 While traditional single diagnostic methods have notable advantages in specific domains, they often fall short in capturing the full scope and dynamic changes of the disease comprehensively. By integrating multiple diagnostic modalities, a multimodal diagnostic approach can provide complementary information across different levels, facilitating more accurate disease assessment, personalized treatment planning, and dynamic monitoring of treatment outcomes.
Recent advances in liquid biopsy technology have underscored the necessity of multimodal diagnostic approaches. Liquid biopsy, with its non-invasive nature, convenience, and ability to enable dynamic monitoring, addresses some of the limitations of traditional tissue biopsy, such as challenges in sample acquisition and the need for frequent testing.117 However, the sensitivity and specificity of liquid biopsy are still constrained by the current state of technology, necessitating its integration with other traditional methods to ensure data accuracy and clinical feasibility.118 Therefore, combining liquid biopsy with conventional diagnostic techniques not only enhances diagnostic comprehensiveness and accuracy but also optimizes patient management workflows, thereby reducing the risk of misdiagnosis and missed diagnoses.
Integration of Liquid Biopsy and Tissue Biopsy
The integration of liquid biopsy and tissue biopsy in lung cancer diagnosis represents a significant advancement in precision medicine. While tissue biopsy is widely recognized as the “gold standard” for lung cancer diagnosis, providing critical data for tumor typing, gene mutation assessment, and protein expression through detailed pathological and molecular analysis,14 its invasiveness and limitations in sample acquisition pose challenges, particularly in advanced or inoperable patients where obtaining sufficient tissue samples for analysis can be quite difficult.17 In this context, liquid biopsy, as a non-invasive and repeatable method, complements tissue biopsy by analyzing CTCs, ctDNA, and exosomes in blood or other body fluids.
A study by Raez et al involving 170 NSCLC patients demonstrated that liquid biopsy offers clear advantages in detection success rates and speed, with an average time to results being 26.8 days faster than tissue biopsy and a consistency in biomarker detection ranging from 94.8% to 100%. Liquid biopsy successfully identified key biomarkers in 76.5% of patients, compared to a 54.9% success rate for tissue biopsy, suggesting that liquid biopsy can not only supplement but in some cases replace tissue biopsy to effectively guide NSCLC treatment decisions.89 Another study found that nearly 70% of Japanese patients with advanced non-squamous NSCLC had tumor genomic alterations, primarily EGFR mutations. In patients with no EGFR driver gene alterations detected by tissue biopsy, ctDNA next-generation sequencing revealed predefined gene changes in 29.2% of cases. Therefore, ctDNA liquid biopsy serves as a valuable supplementary tool when no alterations are detected after initial tissue testing, particularly aiding in identifying pathogenic gene changes before first-line treatment.119
Furthermore, in a study focusing on osimertinib resistance in advanced EGFR-mutant NSCLC, the concordance of gene typing between liquid and tissue biopsies showed an 87.5% agreement for EGFR activation mutations, whereas concordance for molecular resistance mechanisms was lower at 22.7%. MET amplification was identified as the most common resistance mechanism, highlighting the high heterogeneity of resistance mechanisms. Liquid biopsy, as an effective supplementary tool, can integrate tissue biopsy results and investigate resistance mechanisms.120 Liang et al further emphasized the importance of combined testing of EGFR mutations in tumor tissue and plasma during first-line EGFR-TKI treatment, noting that combined testing, particularly in TP53-mutant patients, provided more accurate predictions of poor prognosis with a 91.3% combined detection rate of EGFR mutations.121 In EGFR-TKI resistant lung cancer patients, combining liquid and tissue biopsies for NGS detection allows for a more comprehensive identification of targetable drivers, with studies indicating that targeted mutations were detected in two-thirds of patients either through liquid or tissue testing, while T790M mutations were found in some patients only through tissue or cfDNA. This underscores the significant complementarity of the two methods. Thus, it is recommended to conduct both tissue and liquid NGS testing after EGFR-TKI resistance to enhance the detection rate and efficacy of targeted therapies.122
The integration of liquid biopsy and tissue biopsy demonstrates significant complementary value in lung cancer diagnosis and treatment. Liquid biopsy, with its non-invasive nature, efficiency, and advantages in detection success rates and speed, serves as an important complement to tissue biopsy, particularly showing higher sensitivity in detecting driver gene mutations and resistance mechanisms. Combining these methods enhances the precision and efficacy of targeted treatments, providing stronger support for personalized therapy in lung cancer.
Integration of Liquid Biopsy and Imaging Techniques
Imaging techniques, particularly CT and PET scans, are crucial tools for early screening and staging of lung cancer. However, these methods primarily rely on detecting anatomical changes in tumors and exhibit limited sensitivity when identifying small or subtle lesions. Additionally, imaging results may be affected by false positives or false negatives due to factors such as severe infection or inflammation, which can impact the accuracy of clinical decisions.25 Consequently, the integration of liquid biopsy with imaging techniques provides robust support for overcoming these limitations. Liquid biopsy, by detecting molecular markers in circulation, offers insights into the molecular characteristics of tumors, demonstrating particular advantages in cases where imaging is less effective, such as with small or ambiguous lesions.
In early-stage NSCLC patients, studies have shown a positive correlation between plasma ctDNA levels and tumor glucose metabolism activity measured by 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT), including metabolic tumor volume (MTV) and total lesion glycolysis (TLG). This suggests a potential association between liquid biopsy and PET/CT. However, ctDNA detection serves as an independent negative prognostic factor with intrinsic value in predicting OS and PFS. This finding indicates that liquid biopsy can provide additional prognostic information independent of PET/CT, offering a more comprehensive perspective for clinical management.123 Research by Fiala et al further supports the combined use of liquid biopsy and PET/CT. They found a significant correlation between ctDNA levels and PET/CT metabolic parameters (MTV, TLG, and intrinsic activity (IC)) during treatment follow-up in advanced NSCLC patients. Specifically, integrating ctDNA results with changes in PET/CT’s SUVmax during follow-up provided a more accurate assessment of treatment response and PFS. This indicates a synergistic effect of combining ctDNA with PET/CT, offering an effective tool for monitoring and prognostication in advanced NSCLC patients.118 Similarly, ctDNA and 18F-FDG PET/CT-derived metabolic parameters have been identified as potential non-invasive predictive biomarkers. Studies show that a positive ctDNA status at baseline correlates significantly with shorter PFS, while early metabolic response (MR) derived from 18F-FDG PET/CT significantly improves PFS and OS. Baseline PET/CT parameters are significantly associated with the frequency of EGFR mutations in ctDNA, and ctDNA EGFR clearance at t1 is closely related to MR. These findings suggest that ctDNA and PET/CT metabolic parameters are important biomarkers for predicting the efficacy of osimertinib treatment.124
In summary, the integration of liquid biopsy and imaging techniques demonstrates significant application value in lung cancer management. By combining molecular information from ctDNA with metabolic parameters from PET/CT, clinicians can more comprehensively assess patient prognosis and treatment response. Particularly in advanced NSCLC patients, this multimodal approach helps overcome the limitations of single diagnostic methods, thereby optimizing personalized treatment plans and improving clinical outcomes.
Synergistic Role of Liquid Biopsy and Pathological Analysis
Pathological analysis remains central to the diagnosis, classification, and prognostic evaluation of lung cancer. However, this method relies on the acquisition of tissue samples, which can be challenging, especially in advanced stages of the disease or when tumors are located deep within the body.125 Liquid biopsy offers a powerful complement to pathological analysis by providing dynamic tumor-related information through the detection of molecular markers in bodily fluids.
Guibert et al demonstrated that high-sensitivity genetic profiling of cfDNA extracted from the supernatant of FNA can detect key driver gene mutations even with limited sample volumes. In lung cancer patients, FNA-supernatant (FNA-S) successfully identified multiple driver and resistance mutations, including EGFR, KRAS, and HER2, highlighting its potential in diagnosis and treatment monitoring, particularly when tissue samples are insufficient for pathological analysis. This underscores the value of liquid biopsy in rapid cancer gene profiling under constrained sample conditions.126
Additionally, research by Russo et al showed that early use of liquid biopsy (LBx) for comprehensive genomic profiling (CGP) significantly reduces the time to treatment initiation in patients with advanced non-small cell lung cancer (aNSCLC). Among 1,076 patients, 56 (5.2%) underwent liquid biopsy before pathological diagnosis, and these patients experienced a significantly shorter median time from diagnosis to treatment compared to those who had LBx after pathological diagnosis (21 days vs 35 days). Although pre-diagnostic use of LBx remains rare in real-world settings, it demonstrates potential advantages in accelerating diagnosis and treatment, serving as an effective adjunct to pathological analysis.127
Moreover, liquid biopsy can aid in confirming gene mutations or biomarkers detected by pathological analysis, thereby enhancing diagnostic accuracy. For example, in ALK-positive NSCLC patients, liquid biopsy can detect ALK fusion genes in the blood, assisting in confirming the presence of this molecular marker identified by pathological analysis and enabling real-time monitoring of early adverse prognosis and recurrence risk during disease progression.128 This synergy allows liquid biopsy and pathological analysis to complement each other, collectively improving diagnostic accuracy and personalizing treatment.
In summary, the integration of liquid biopsy with traditional diagnostic methods offers a new approach and perspective for comprehensive lung cancer management. By employing a multimodal diagnostic strategy, clinicians can better integrate information from various sources, leading to more accurate diagnoses and optimized treatment decisions. This integrative approach not only enhances the comprehensiveness of diagnosis but also enables dynamic monitoring and timely adjustments to treatment plans, ultimately improving patient outcomes.
Clinical Procedures for Multimodal Diagnostic Pathways
In lung cancer management, multimodal diagnostic pathways aim to optimize diagnostic accuracy and comprehensiveness by integrating various diagnostic techniques, thereby improving patient prognosis. This strategy not only encompasses initial diagnosis and treatment decision-making but also extends to long-term monitoring and recurrence detection. To achieve these objectives, it is essential to establish a well-defined set of clinical operational procedures that ensure the coherent integration and efficient application of each diagnostic modality.
Clinical Workflow for Integrated Strategies
In the management of lung cancer, the clinical operational procedures for multimodal diagnostic pathways should encompass the entire process from initial screening to treatment monitoring, ensuring diagnostic precision and personalized therapy. This workflow can be divided into four primary stages (Figure 2).
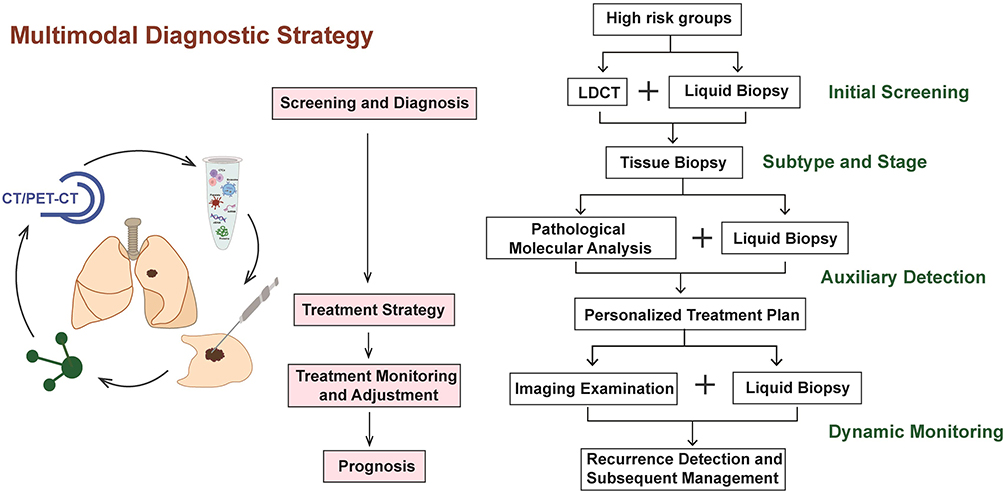 |
Figure 2 Multimodal diagnostic strategy for lung cancer management.The workflow is structured into four key stages: (1) Initial screening and early diagnosis, utilizing low-dose CT (LDCT) to detect suspicious lesions, with liquid biopsy serving as a complementary tool for cases with ambiguous imaging findings. (2) Formulation of personalized treatment strategies, informed by tissue biopsy for histopathological confirmation and molecular marker analysis, supplemented by dynamic liquid biopsy monitoring to assess tumor mutations and burden. (3) Treatment monitoring and dynamic adjustment, where liquid biopsy evaluates therapeutic efficacy and identifies resistance mutations or relapse risk, while imaging assists in tumor staging and progression assessment. (4) Recurrence detection and long-term management, leveraging liquid biopsy for early detection of molecular changes indicating potential relapse, followed by imaging to localize the recurrence and re-stage the disease, guiding subsequent treatment decisions. This multimodal approach optimizes diagnostic accuracy and facilitates personalized therapy. |
First, during the initial screening and diagnosis stage, LDCT (Low-dose Computed Tomography) is employed for preliminary screening to identify suspicious lesions. For cases with indeterminate imaging results or small lesions, liquid biopsy (including ctDNA, CTCs, and exosome analysis) can be used as an adjunctive tool to confirm the presence of a tumor and its molecular characteristics. When liquid biopsy results indicate the presence of a tumor, a tissue biopsy should be performed for pathological confirmation and to analyze the tumor’s histological type and molecular markers.
Next, in the treatment strategy formulation stage, samples obtained from tissue biopsy undergo detailed pathological analysis to determine the lung cancer subtype and associated molecular markers. Combined with dynamic monitoring through liquid biopsy, this assessment of tumor genetic mutations and tumor burden provides a reliable basis for formulating personalized treatment strategies. Additionally, imaging techniques are employed for tumor staging, offering a comprehensive evaluation of local tumor spread and distant metastasis, thereby aiding in the development of the optimal comprehensive treatment plan.
During the treatment monitoring and adjustment stage, continuous monitoring of ctDNA levels through liquid biopsy is essential for evaluating treatment efficacy and the early detection of resistance mutations or the risk of recurrence. An increase in ctDNA levels, as indicated by liquid biopsy, may suggest tumor recurrence or treatment failure, necessitating timely adjustments to the therapeutic strategy. Furthermore, imaging follow-up helps assess tumor regression or progression, providing morphological support to the findings from liquid biopsy.
Finally, in the recurrence detection and subsequent management stage, liquid biopsy is valuable for the early detection of potential recurrence risks, particularly when imaging has yet to reveal definitive lesions. Minor molecular changes in ctDNA can signal possible recurrence. Once liquid biopsy suggests recurrence, further imaging studies should be conducted to confirm the location and extent of tumor recurrence, followed by re-staging to guide subsequent treatment decisions.
Moreover, liquid biopsy has been shown to have high sensitivity in detecting EGFR mutations in non-small cell lung cancer (NSCLC), and is particularly excellent in detecting EGFR mutations in non-small cell lung cancer (NSCLC), especially in detecting mutations sensitive to tyrosine kinase inhibitors (TKIs) as well as drug-resistant mutations (eg, T790M).129 In addition, studies have shown that ctDNA or circulating tumor cell (CTC) dynamic monitoring can be used to assist in the assessment of NSCLC progression, detecting drug resistance earlier than imaging or tumor markers, and helping clinicians to determine the mechanism of resistance and adjust new treatment regimens in a timely manner.130
In conclusion, the application of multimodal diagnostic pathways in lung cancer management offers significant advantages, not only enhancing diagnostic accuracy but also optimizing therapeutic decision-making. Additionally, these pathways improve the sensitivity of recurrence detection through dynamic monitoring, thereby holding the potential to improve long-term patient outcomes. However, the clinical effectiveness of such diagnostic approaches still requires further prospective studies and large-scale clinical validation.
Challenges and Future Directions of Multimodal Diagnostic Pathways
Despite the significant advantages demonstrated by multimodal diagnostic pathways in lung cancer management, several challenges remain in their clinical implementation. Firstly, the sensitivity and specificity of liquid biopsy need further enhancement, particularly in the detection of early-stage lung cancer. While liquid biopsy can identify molecular alterations in tumors, its efficacy in detecting such changes in cases of low tumor burden requires improvement.131
Secondly, the implementation of multimodal diagnostic pathways must address the issue of data standardization. The data derived from various sources—such as liquid biopsy, imaging, and pathological analysis—may exhibit a degree of heterogeneity. Standardizing and integrating these data to support consistent clinical decision-making is a critical area for future research.132 Currently, interdisciplinary collaboration and multicenter studies hold promise for advancing this field, as they facilitate the sharing of data and technology, thereby optimizing the clinical application of multimodal diagnostic pathways.
Moreover, the clinical application of multimodal diagnostic pathways involves balancing cost and complexity. The combined use of liquid biopsy, imaging, and tissue biopsy may increase the financial burden on patients and complicate the diagnostic and treatment processes.133 Future research should explore how technological innovation and process optimization can reduce the cost of multimodal diagnostics and simplify their clinical workflows.
The application of multimodal diagnostic pathways in lung cancer management holds great promise and carries significant clinical implications. However, as technology advances and clinical research progresses, the implementation and optimization of these pathways will continue to face numerous challenges. With ongoing improvements in liquid biopsy technology and strengthened interdisciplinary collaboration, multimodal diagnostic pathways are expected to become an indispensable tool in lung cancer management, enhancing diagnostic accuracy and treatment efficacy, ultimately improving long-term patient outcomes.
Conclusion
In this review, we comprehensively examine the roles of traditional diagnostic methods and liquid biopsy in lung cancer management, along with strategies for their integration. Traditional diagnostic approaches, such as imaging examination and tissue biopsy, have been instrumental in the early detection and pathological classification of lung cancer. However, these methods have limitations in detecting small lesions, monitoring therapeutic efficacy, and early identification of recurrence. Liquid biopsy, as an emerging non-invasive technology, offers dynamic insights into the molecular characteristics and evolution of tumors by analyzing biomarkers such as CTCs, ctDNA, and exosomes. This provides critical support for early screening, treatment monitoring, and prognostic evaluation in lung cancer.
The clinical value of liquid biopsy in comprehensive lung cancer management has gained widespread recognition, particularly in precision medicine and the study of resistance mechanisms to targeted therapies. However, liquid biopsy is not without its limitations; its sensitivity and specificity still pose challenges. Therefore, integration with traditional diagnostic methods is essential. In this review, we delve into the integration strategies of liquid biopsy with tissue biopsy and imaging techniques, proposing a clinical operational framework for multimodal diagnostic pathways, thereby providing theoretical support and practical recommendations for clinical application.
In conclusion, the integration of liquid biopsy with traditional diagnostic methods offers a novel pathway for the precision management of lung cancer. Future research should focus on further optimizing multimodal diagnostic strategies to enhance diagnostic accuracy and therapeutic outcomes. By continuously exploring the synergy between new technologies and existing methods, we can expect to further improve the prognosis of lung cancer patients and advance the development of personalized medicine.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Kratzer TB, Bandi P, Freedman ND, et al. Lung cancer statistics, 2023. Cancer. 2024;130(8):1330–1348. doi:10.1002/cncr.35128
3. Wu F, Fan J, He Y, et al. Single-cell profiling of tumor heterogeneity and the microenvironment in advanced non-small cell lung cancer. Nat Commun. 2021;12(1):2540. doi:10.1038/s41467-021-22801-0
4. Zhang H, Tian S, Wang S, Liu S, Liao M. CT-guided percutaneous core needle biopsy in typing and subtyping lung cancer: a comparison to surgery. Technol Cancer Res Treat. 2022;21:15330338221086411. doi:10.1177/15330338221086411
5. Hiraki T, Mimura H, Gobara H, et al. CT fluoroscopy-guided biopsy of 1,000 pulmonary lesions performed with 20-gauge coaxial cutting needles: diagnostic yield and risk factors for diagnostic failure. Chest. 2009;136(6):1612–1617. doi:10.1378/chest.09-0370
6. Bajtarevic A, Ager C, Pienz M, et al. Noninvasive detection of lung cancer by analysis of exhaled breath. BMC Cancer. 2009;9:348. doi:10.1186/1471-2407-9-348
7. Reckamp KL, Melnikova VO, Karlovich C, et al. A highly sensitive and quantitative test platform for detection of NSCLC EGFR mutations in urine and plasma. J Thorac Oncol. 2016;11(10):1690–1700. doi:10.1016/j.jtho.2016.05.035
8. Li W, Liu JB, Hou LK, et al. Liquid biopsy in lung cancer: significance in diagnostics, prediction, and treatment monitoring. mol Cancer. 2022;21(1):25. doi:10.1186/s12943-022-01505-z
9. Moser T, Heitzer E. Surpassing sensitivity limits in liquid biopsy. Science. 2024;383:
10. Pulumati A, Pulumati A, Dwarakanath BS, Verma A, Papineni RVL. Technological advancements in cancer diagnostics: improvements and limitations. Cancer Rep. 2023;6(2):e1764. doi:10.1002/cnr2.1764
11. Mata DA, Harries L, Williams EA, et al. Method of tissue acquisition affects success of comprehensive genomic profiling in lung cancer. Arch Pathol Lab Med. 2023;147(3):338–347. doi:10.5858/arpa.2021-0313-OA
12. Gompelmann D, Sinn K, Brugger J, et al. Correlation of PD-L1 expression on tumour cells between diagnostic biopsies and surgical specimens of lung cancer in real life with respect to biopsy techniques and neoadjuvant treatment. J Cancer Res Clin Oncol. 2023;149(5):1747–1754. doi:10.1007/s00432-022-04080-4
13. Liu Y, Xu J. High-resolution microscopy for imaging cancer pathobiology. Curr Pathobiol Rep. 2019;7(3):85–96. doi:10.1007/s40139-019-00201-w
14. Livi V, Paioli D, Cancellieri A, et al. Diagnosis and molecular profiling of lung cancer by percutaneous ultrasound-guided biopsy of superficial metastatic sites is safe and highly effective. Respiration. 2021;100(6):515–522. doi:10.1159/000514316
15. Matsuoka T, Sonobe M, Date H. Intraoperative fine-needle aspiration biopsy (FNA) for lung cancer: diagnostic value and risk of pleural dissemination. Surg Today. 2015;45(6):695–699. doi:10.1007/s00595-014-1029-7
16. Nam BD, Yoon SH, Hong H, Hwang JH, Goo JM, Park S. Tissue adequacy and safety of percutaneous transthoracic needle biopsy for molecular analysis in non-small cell lung cancer: a systematic review and meta-analysis. Korean J Radiol. 2021;22(12):2082–2093. doi:10.3348/kjr.2021.0244
17. Huo YR, Chan MV, Habib A-R, Lui I, Ridley L. Pneumothorax rates in CT-guided lung biopsies: a comprehensive systematic review and meta-analysis of risk factors. Br J Radiol. 2020;93(1108):20190866. doi:10.1259/bjr.20190866
18. Xu Y, Hosny A, Zeleznik R, et al. Deep learning predicts lung cancer treatment response from serial medical imaging. Clin Cancer Res. 2019;25(11):3266–3275. doi:10.1158/1078-0432.Ccr-18-2495
19. Ryvolova M, Chomoucka J, Drbohlavova J, et al. Modern micro and nanoparticle-based imaging techniques. Sensors. 2012;12(11):14792–14820. doi:10.3390/s121114792
20. Mu W, Jiang L, Zhang J, et al. Non-invasive decision support for NSCLC treatment using PET/CT radiomics. Nat Commun. 2020;11(1):5228. doi:10.1038/s41467-020-19116-x
21. Bizzi A, Pascuzzo R. Is brain MRI unnecessary for early-stage non-small cell lung cancer? Radiology. 2022;303(3):644–645. doi:10.1148/radiol.220234
22. Yoshida R, Arakawa H, Kaji Y. Lung cancer in chronic interstitial pneumonia: early manifestation from serial CT observations. AJR Am J Roentgenol. 2012;199(1):85–90. doi:10.2214/ajr.11.7516
23. Zhong Y, Cai C, Chen T, et al. PET/CT based cross-modal deep learning signature to predict occult nodal metastasis in lung cancer. Nat Commun. 2023;14(1):7513. doi:10.1038/s41467-023-42811-4
24. Weber JD, Spiro JE, Scheffler M, et al. Reproducibility of dynamic contrast enhanced MRI derived transfer coefficient Ktrans in lung cancer. PLoS One. 2022;17(3):e0265056. doi:10.1371/journal.pone.0265056
25. Kim KY, Park HL, Kang HS, et al. Clinical characteristics and outcome of pathologic N0 Non-small cell lung cancer patients with false positive mediastinal lymph node metastasis on FDG PET-CT. Vivo. 2021;35(3):1829–1836. doi:10.21873/invivo.12444
26. Lopci E, Kobe C, Gnanasegaran G, Adam JA, de Geus-Oei LF. “PET/CT variants and pitfalls in lung cancer and mesothelioma”. Semin Nucl Med. 2021;51(5):458–473. doi:10.1053/j.semnuclmed.2021.04.002
27. Burnett-Hartman AN, Carroll NM, Honda SA, et al. Community-based lung cancer screening results in relation to patient and radiologist characteristics: the PROSPR consortium. Ann Am Thorac Soc. 2022;19(3):433–441. doi:10.1513/AnnalsATS.202011-1413OC
28. Ortiz-Jaimes G, Reisenauer J. Real-world impact of robotic-assisted bronchoscopy on the staging and diagnosis of lung cancer: the shape of current and potential opportunities. Pragmat Obs Res. 2023;14:75–94. doi:10.2147/por.S395806
29. Zhang R, Ying K, Shi L, Zhang L, Zhou L. Combined endobronchial and endoscopic ultrasound-guided fine needle aspiration for mediastinal lymph node staging of lung cancer: a meta-analysis. Eur J Cancer. 2013;49(8):1860–1867. doi:10.1016/j.ejca.2013.02.008
30. Wang G, Ionescu DN, Lee CH, et al. PD-L1 testing on the EBUS-FNA cytology specimens of non-small cell lung cancer. Lung Cancer. 2019;136:1–5. doi:10.1016/j.lungcan.2019.07.033
31. Yu DH, Shafiq M, Batra H, et al. Comparing modalities for risk assessment in patients with pulmonary lesions and nondiagnostic bronchoscopy for suspected lung cancer. BMC Pulm Med. 2022;22(1):442. doi:10.1186/s12890-022-02181-x
32. Saito Z, Oi I, Ito T, et al. Safety of flexible bronchoscopy and clinical course for elderly patients with suspected primary lung cancer. Thorac Cancer. 2024;15(8):614–621. doi:10.1111/1759-7714.15228
33. Hubers AJ, Prinsen CF, Sozzi G, Witte BI, Thunnissen E. Molecular sputum analysis for the diagnosis of lung cancer. Br J Cancer. 2013;109(3):530–537. doi:10.1038/bjc.2013.393
34. Gressard L, DeGroff AS, Richards TB, et al. A qualitative analysis of smokers’ perceptions about lung cancer screening. BMC Public Health. 2017;17(1):589. doi:10.1186/s12889-017-4496-0
35. Jiang Y, Jin P, Chang RS, et al. Analysis of sensitivity and specificity of sputum cytology screening for lung cancer with different positive criteria. Zhonghua Yu Fang Yi Xue Za Zhi. 2011;45(7):605–608.
36. Agustí C, Xaubet A, Montón C, et al. Induced sputum in the diagnosis of peripheral lung cancer not visible endoscopically. Respir Med. 2001;95(10):822–828. doi:10.1053/rmed.2001.1173
37. Batool SM, Yekula A, Khanna P, et al. The liquid biopsy consortium: challenges and opportunities for early cancer detection and monitoring. Cell Rep Med. 2023;4(10):101198. doi:10.1016/j.xcrm.2023.101198
38. Pantel K, Alix-Panabières C. Liquid biopsy and minimal residual disease - latest advances and implications for cure. Nat Rev Clin Oncol. 2019;16(7):409–424. doi:10.1038/s41571-019-0187-3
39. Zhao L, Wu X, Zheng J, Dong D. DNA methylome profiling of circulating tumor cells in lung cancer at single base-pair resolution. Oncogene. 2021;40(10):1884–1895. doi:10.1038/s41388-021-01657-0
40. Buder A, Heitzer E, Waldispühl-Geigl J, et al. Somatic copy-number alterations in plasma circulating tumor DNA from advanced EGFR-mutated lung adenocarcinoma Patients. Biomolecules. 2021;11(5):618. doi:10.3390/biom11050618
41. Tjamj A. A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Aust Med J. 1869;14:146.
42. Na TY, Schecterson L, Mendonsa AM, Gumbiner BM. The functional activity of E-cadherin controls tumor cell metastasis at multiple steps. Proc Natl Acad Sci U S A. 2020;117(11):5931–5937. doi:10.1073/pnas.1918167117
43. Zhang Z, Wuethrich A, Wang J, Korbie D, Lin LL, Trau M. dynamic Monitoring of EMT in CTCs as an indicator of cancer metastasis. Anal Chem. 2021;93(50):16787–16795. doi:10.1021/acs.analchem.1c03167
44. Alix-Panabières C, Pantel K. Challenges in circulating tumour cell research. Nat Rev Cancer. 2014;14(9):623–631. doi:10.1038/nrc3820
45. Shimmyo N, Furuhata M, Yamada M, Utoh R, Seki M. Process simplification and structure design of parallelized microslit isolator for physical property-based capture of tumor cells. Analyst. 2022;147(8):1622–1630. doi:10.1039/d2an00052k
46. Chauhan A, Pal A, Sachdeva M, et al. A FACS-based novel isolation technique identifies heterogeneous CTCs in oral squamous cell carcinoma. Front Oncol. 2024;14:1269211. doi:10.3389/fonc.2024.1269211
47. Li G, Ji Y, Wu Y, et al. Multistage microfluidic cell sorting method and chip based on size and stiffness. Biosens Bioelectron. 2023;237:115451. doi:10.1016/j.bios.2023.115451
48. Shou X, Li Y, Hu W, et al. Six-gene Assay as a new biomarker in the blood of patients with colorectal cancer: establishment and clinical validation. Mol Oncol. 2019;13(4):781–791. doi:10.1002/1878-0261.12427
49. Huang X, Gao P, Sun J, et al. Clinicopathological and prognostic significance of circulating tumor cells in patients with gastric cancer: a meta-analysis. Int, J, Cancer. 2015;136(1):21–33. doi:10.1002/ijc.28954
50. Pierga JY, Hajage D, Bachelot T, et al. High independent prognostic and predictive value of circulating tumor cells compared with serum tumor markers in a large prospective trial in first-line chemotherapy for metastatic breast cancer patients. Ann Oncol. 2012;23(3):618–624. doi:10.1093/annonc/mdr263
51. Ishiguro Y, Sakihama H, Yoshida T, et al. Prognostic significance of circulating tumor cells with mesenchymal phenotypes in patients with gastric cancer: a prospective study. Ann Surg Oncol. 2021;28(2):1178–1186. doi:10.1245/s10434-020-08827-6
52. de Bono JS, Scher HI, Montgomery RB, et al. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res. 2008;14(19):6302–6309. doi:10.1158/1078-0432.Ccr-08-0872
53. Yu M, Bardia A, Aceto N, et al. Cancer therapy. Ex vivo culture of circulating breast tumor cells for individualized testing of drug susceptibility. Science. 2014;345:
54. Kang HM, Kim GH, Jeon HK, et al. Circulating tumor cells detected by lab-on-a-disc: role in early diagnosis of gastric cancer. PLoS One. 2017;12(6):e0180251. doi:10.1371/journal.pone.0180251
55. Watanabe T, Okumura T, Hirano K, et al. Circulating tumor cells expressing cancer stem cell marker CD44 as a diagnostic biomarker in patients with gastric cancer. Oncol Lett. 2017;13(1):281–288. doi:10.3892/ol.2016.5432
56. Carneiro A, Piairo P, Teixeira A, et al. Discriminating epithelial to mesenchymal transition phenotypes in circulating tumor cells isolated from advanced gastrointestinal cancer patients. Cells. 2022;11(3):376. doi:10.3390/cells11030376
57. Mouliere F, Chandrananda D, Piskorz AM, et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci Transl Med. 2018;10(466). doi:10.1126/scitranslmed.aat4921
58. Fujisawa R, Iwaya T, Endo F, et al. Early dynamics of circulating tumor DNA predict chemotherapy responses for patients with esophageal cancer. Carcinogenesis. 2021;42(10):1239–1249. doi:10.1093/carcin/bgab088
59. Kok PS, Lee K, Lord S, et al. Clinical utility of plasma EGFR mutation detection with quantitative PCR in advanced lung cancer: a meta-analysis. Lung Cancer. 2021;154:113–117. doi:10.1016/j.lungcan.2021.02.027
60. Shen W, Shan B, Liang S, et al. Hybrid capture-based genomic profiling of circulating tumor DNA from patients with advanced ovarian cancer. Pathol Oncol Res. 2021;27:581534. doi:10.3389/pore.2021.581534
61. Balgkouranidou I, Chimonidou M, Milaki G, et al. SOX17 promoter methylation in plasma circulating tumor DNA of patients with non-small cell lung cancer. Clin Chem Lab Med. 2016;54(8):1385–1393. doi:10.1515/cclm-2015-0776
62. Economopoulou P, Spathis A, Kotsantis I, et al. Next-generation sequencing (NGS) profiling of matched tumor and circulating tumor DNA (ctDNA) in head and neck squamous cell carcinoma (HNSCC). Oral Oncol. 2023;139:106358. doi:10.1016/j.oraloncology.2023.106358
63. Liang N, Li B, Jia Z, et al. Ultrasensitive detection of circulating tumour DNA via deep methylation sequencing aided by machine learning. Nat Biomed Eng. 2021;5(6):586–599. doi:10.1038/s41551-021-00746-5
64. Mattos-Arruda L D, Mayor R, Ng CKY, et al. Cerebrospinal fluid-derived circulating tumour DNA better represents the genomic alterations of brain tumours than plasma. Nat Commun. 2015;6:8839. doi:10.1038/ncomms9839
65. Mattos-Arruda L D, Weigelt B, Cortes J, et al. Capturing intra-tumor genetic heterogeneity by de novo mutation profiling of circulating cell-free tumor DNA: a proof-of-principle. Ann Oncol. 2014;25(9):1729–1735. doi:10.1093/annonc/mdu239
66. Abbosh C, Birkbak NJ, Wilson GA, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545(7655):446–451. doi:10.1038/nature22364
67. Parkinson CA, Gale D, Piskorz AM, et al. Exploratory analysis of TP53 mutations in circulating tumour DNA as biomarkers of treatment response for patients with relapsed high-grade serous ovarian carcinoma: a retrospective study. PLoS Med. 2016;13(12):e1002198. doi:10.1371/journal.pmed.1002198
68. Tie J, Wang Y, Tomasetti C, et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci Transl Med. 2016;8(346):346ra392. doi:10.1126/scitranslmed.aaf6219
69. Olsson E, Winter C, George A, et al. Serial monitoring of circulating tumor DNA in patients with primary breast cancer for detection of occult metastatic disease. EMBO Mol Med. 2015;7(8):1034–1047. doi:10.15252/emmm.201404913
70. Mohan S, Heitzer E, Ulz P, et al. Changes in colorectal carcinoma genomes under anti-EGFR therapy identified by whole-genome plasma DNA sequencing. PLoS Genet. 2014;10(3):e1004271. doi:10.1371/journal.pgen.1004271
71. Murtaza M, Dawson SJ, Tsui DW, et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature. 2013;497(7447):108–112. doi:10.1038/nature12065
72. Sacher AG, Paweletz C, Dahlberg SE, et al. Prospective validation of rapid plasma genotyping for the detection of EGFR and KRAS mutations in advanced lung cancer. JAMA Oncol. 2016;2(8):1014–1022. doi:10.1001/jamaoncol.2016.0173
73. Wang H, Li B, Liu Z, et al. HER2 copy number of circulating tumour DNA functions as a biomarker to predict and monitor trastuzumab efficacy in advanced gastric cancer. Eur J Cancer. 2018;88:92–100. doi:10.1016/j.ejca.2017.10.032
74. Vona G, Sabile A, Louha M, et al. Isolation by size of epithelial tumor cells: a new method for the immunomorphological and molecular characterization of circulating tumor cells. Am J Pathol. 2000;156(1):57–63. doi:10.1016/s0002-9440(10)64706-2
75. Watanabe F, Suzuki K, Tamaki S, et al. Longitudinal monitoring of KRAS-mutated circulating tumor DNA enables the prediction of prognosis and therapeutic responses in patients with pancreatic cancer. PLoS One. 2019;14(12):e0227366. doi:10.1371/journal.pone.0227366
76. Yang C, Xue Y, Duan Y, Mao C, Wan M. Extracellular vesicles and their engineering strategies, delivery systems, and biomedical applications. J Control Release. 2024;365:1089–1123. doi:10.1016/j.jconrel.2023.11.057
77. Kimiz-Gebologlu I, Oncel SS. Exosomes: large-scale production, isolation, drug loading efficiency, and biodistribution and uptake. J Control Release. 2022;347:533–543. doi:10.1016/j.jconrel.2022.05.027
78. Mashouri L, Yousefi H, Aref AR, Ahadi AM, Molaei F, Alahari SK. Exosomes: composition, biogenesis, and mechanisms in cancer metastasis and drug resistance. mol Cancer. 2019;18(1):75. doi:10.1186/s12943-019-0991-5
79. Qiu S, Xie L, Lu C, et al. Gastric cancer-derived exosomal miR-519a-3p promotes liver metastasis by inducing intrahepatic M2-like macrophage-mediated angiogenesis. J Exp Clin Cancer Res. 2022;41(1):296. doi:10.1186/s13046-022-02499-8
80. Greening DW, Xu R, Ji H, Tauro BJ, Simpson RJ. A protocol for exosome isolation and characterization: evaluation of ultracentrifugation, density-gradient separation, and immunoaffinity capture methods. Methods mol Biol. 2015;1295:179–209. doi:10.1007/978-1-4939-2550-6_15
81. Deng Z, Wang J, Xiao Y, et al. Ultrasound-mediated augmented exosome release from astrocytes alleviates amyloid-β-induced neurotoxicity. Theranostics. 2021;11(9):4351–4362. doi:10.7150/thno.52436
82. Brown BA, Zeng X, Todd AR, et al. Charge detection mass spectrometry measurements of exosomes and other extracellular particles enriched from bovine milk. Anal Chem. 2020;92(4):3285–3292. doi:10.1021/acs.analchem.9b05173
83. Peinado H, Alečković M, Lavotshkin S, et al. Melanoma exosomes educate bone marrow progenitor cells toward a pro-metastatic phenotype through MET. Nat Med. 2012;18(6):883–891. doi:10.1038/nm.2753
84. Hoshino A, Costa-Silva B, Shen TL, et al. Tumour exosome integrins determine organotropic metastasis. Nature. 2015;527(7578):329–335. doi:10.1038/nature15756
85. Qu X, Li Q, Yang J, et al. Double-stranded DNA in exosomes of malignant pleural effusions as a novel DNA source for EGFR mutation detection in lung adenocarcinoma. Front Oncol. 2019;9:931. doi:10.3389/fonc.2019.00931
86. Liang G, Zhu Y, Ali DJ, et al. Engineered exosomes for targeted co-delivery of miR-21 inhibitor and chemotherapeutics to reverse drug resistance in colon cancer. J Nanobiotechnology. 2020;18(1):10. doi:10.1186/s12951-019-0563-2
87. Yamashita T, Takahashi Y, Takakura Y. Possibility of exosome-based therapeutics and challenges in production of exosomes eligible for therapeutic application. Biol Pharm Bull. 2018;41(6):835–842. doi:10.1248/bpb.b18-00133
88. Yu W, Hurley J, Roberts D, et al. Exosome-based liquid biopsies in cancer: opportunities and challenges. Ann Oncol. 2021;32(4):466–477. doi:10.1016/j.annonc.2021.01.074
89. Raez LE, Brice K, Dumais K, et al. Liquid biopsy versus tissue biopsy to determine front line therapy in metastatic Non-Small Cell Lung Cancer (NSCLC). Clin Lung Cancer. 2023;24(2):120–129. doi:10.1016/j.cllc.2022.11.007
90. Phallen J, Sausen M, Adleff V, et al. Direct detection of early-stage cancers using circulating tumor DNA. Sci Transl Med. 2017;9(403). doi:10.1126/scitranslmed.aan2415
91. Klein EA, Richards D, Cohn A, et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann Oncol. 2021;32(9):1167–1177. doi:10.1016/j.annonc.2021.05.806
92. Mathios D, Johansen JS, Cristiano S, et al. Detection and characterization of lung cancer using cell-free DNA fragmentomes. Nat Commun. 2021;12(1):5060. doi:10.1038/s41467-021-24994-w
93. Gasiorowski L, Dyszkiewicz W, Zielinski P. In-vivo isolation of circulating tumor cells in non-small cell lung cancer patients by CellCollector. Neoplasma. 2017;64(6):938–944. doi:10.4149/neo_2017_618
94. Gorges TM, Penkalla N, Schalk T, et al. Enumeration and molecular characterization of tumor cells in lung cancer patients using a novel in vivo device for capturing circulating tumor cells. Clin Cancer Res. 2016;22(9):2197–2206. doi:10.1158/1078-0432.Ccr-15-1416
95. Pfarr N, Penzel R, Klauschen F, et al. Copy number changes of clinically actionable genes in melanoma, non-small cell lung cancer and colorectal cancer-A survey across 822 routine diagnostic cases. Genes Chromosomes Cancer. 2016;55(11):821–833. doi:10.1002/gcc.22378
96. Yang D, Yang X, Li Y, et al. Clinical significance of circulating tumor cells and metabolic signatures in lung cancer after surgical removal. J Transl Med. 2020;18(1):243. doi:10.1186/s12967-020-02401-0
97. Zhang W, Campbell DH, Walsh BJ, Packer NH, Liu D, Wang Y. Cancer-derived small extracellular vesicles: emerging biomarkers and therapies for pancreatic ductal adenocarcinoma diagnosis/prognosis and treatment. J Nanobiotechnology. 2022;20(1):446. doi:10.1186/s12951-022-01641-0
98. Yuan L, Chen Y, Ke L, et al. Plasma extracellular vesicle phenotyping for the differentiation of early-stage lung cancer and benign lung diseases. Nanoscale Horiz. 2023;8(6):746–758. doi:10.1039/d2nh00570k
99. Zhong Y, Ding X, Bian Y, et al. Discovery and validation of extracellular vesicle-associated miRNAs as noninvasive detection biomarkers for early-stage non-small-cell lung cancer. Mol Oncol. 2021;15(9):2439–2452. doi:10.1002/1878-0261.12889
100. Kawaguchi T, Koh Y, Ando M, et al. Prospective analysis of oncogenic driver mutations and environmental factors: Japan molecular epidemiology for lung cancer study. J Clin Oncol. 2016;34(19):2247–2257. doi:10.1200/jco.2015.64.2322
101. Shi Y, Au JS, Thongprasert S, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9(2):154–162. doi:10.1097/jto.0000000000000033
102. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
103. Wang N, Zhang X, Wang F, et al. The diagnostic accuracy of liquid biopsy in EGFR-mutated NSCLC: a systematic review and meta-analysis of 40 studies. SLAS Technol. 2021;26(1):42–54. doi:10.1177/2472630320939565
104. Thompson JC, Aggarwal C, Wong J, et al. Plasma genotyping at the time of diagnostic tissue biopsy decreases time-to-treatment in patients with advanced NSCLC-results from a prospective pilot study. JTO Clin Res Rep. 2022;3(4):100301. doi:10.1016/j.jtocrr.2022.100301
105. Ang YLE, Zhao X, Reungwetwattana T, et al. A phase II study of osimertinib in patients with advanced-stage non-small cell lung cancer following prior epidermal growth factor receptor tyrosine kinase inhibitor (EGFR TKI) therapy with EGFR and T790M mutations detected in plasma circulating tumour DNA (PLASMA study). Cancers. 2023;15(20). doi:10.3390/cancers15204999
106. Pérez-Callejo D, Torrente M, Romero A. Clinical and investigational applications of liquid biopsy in non-small cell lung cancer. J Tumor. 2016;4(5–6):461–468.
107. Ilié M, Szafer-Glusman E, Hofman V, et al. Detection of PD-L1 in circulating tumor cells and white blood cells from patients with advanced non-small-cell lung cancer. Ann Oncol. 2018;29(1):193–199. doi:10.1093/annonc/mdx636
108. Buttitta F, Felicioni L, Lorito AD, et al. Early prediction of resistance to tyrosine kinase inhibitors by plasma monitoring of EGFR mutations in NSCLC: a new algorithm for patient selection and personalized treatment. Oncotarget. 2020;11(11):982–991. doi:10.18632/oncotarget.27517
109. Remon J, Besse B, Aix SP, et al. Osimertinib treatment based on plasma T790M monitoring in patients with EGFR-mutant non-small-cell lung cancer (NSCLC): EORTC Lung Cancer Group 1613 APPLE phase II randomized clinical trial. Ann Oncol. 2023;34(5):468–476. doi:10.1016/j.annonc.2023.02.012
110. Zhang C, Wei B, Li P, et al. Prognostic value of plasma EGFR ctDNA in NSCLC patients treated with EGFR-TKIs. PLoS One. 2017;12(3):e0173524. doi:10.1371/journal.pone.0173524
111. Hartmaier RJ, Markovets AA, Ahn MJ, et al. Osimertinib + savolitinib to overcome acquired MET-mediated resistance in epidermal growth factor receptor-mutated, MET-amplified non-small cell lung cancer: TATTON. Cancer Discov. 2023;13(1):98–113. doi:10.1158/2159-8290.Cd-22-0586
112. Chaudhuri AA, Chabon JJ, Lovejoy AF, et al. early detection of molecular residual disease in localized lung cancer by circulating tumor DNA profiling. Cancer Discov. 2017;7(12):1394–1403. doi:10.1158/2159-8290.Cd-17-0716
113. Chen K, Zhao H, Shi Y, et al. Perioperative dynamic changes in circulating tumor DNA in patients with lung cancer (DYNAMIC). Clin Cancer Res. 2019;25(23):7058–7067. doi:10.1158/1078-0432.Ccr-19-1213
114. Sanchez-Cabrero D, Garcia-Guede Á, Burdiel M, et al. miR-124 as a liquid biopsy prognostic biomarker in small extracellular vesicles from NSCLC patients. Int J mol Sci. 2023;24(14):11464. doi:10.3390/ijms241411464
115. Eslami SZ, Cortés-Hernández LE, Sinoquet L, et al. Circulating tumour cells and PD-L1-positive small extracellular vesicles: the liquid biopsy combination for prognostic information in patients with metastatic non-small cell lung cancer. Br J Cancer. 2024;130(1):63–72. doi:10.1038/s41416-023-02491-9
116. de Sousa VML, Carvalho L. Heterogeneity in lung cancer. Pathobiology. 2018;85(1–2):96–107. doi:10.1159/000487440
117. Adhit KK, Wanjari A, Menon S, K S. Liquid biopsy: an evolving paradigm for non-invasive disease diagnosis and monitoring in medicine. Cureus. 2023;15(12):e50176. doi:10.7759/cureus.50176
118. Fiala O, Baxa J, Svaton M, et al. Combination of circulating tumour DNA and (18)F-FDG PET/CT for precision monitoring of therapy response in patients with advanced non-small cell lung cancer: a prospective study. Cancer Genomics Proteomics. 2022;19(2):270–281. doi:10.21873/cgp.20319
119. Uemura T, Kenmotsu H, Hazama D, et al. Liquid biopsy detects genomic drivers in NSCLC without EGFR mutations by single-plex testing: WJOG13620L. Cancer Med. 2023;12(23):21097–21110. doi:10.1002/cam4.6668
120. Leonetti A, Verzè M, Minari R, et al. Resistance to osimertinib in advanced EGFR-mutated NSCLC: a prospective study of molecular genotyping on tissue and liquid biopsies. Br J Cancer. 2024;130(1):135–142. doi:10.1038/s41416-023-02475-9
121. Liang X, Zhang W, Li J, et al. Clinical implications of ctDNA for EGFR-TKIs as first-line treatment in NSCLC. J Cancer Res Clin Oncol. 2023;149(3):1211–1220. doi:10.1007/s00432-022-03952-z
122. Lin YT, Ho CC, Hsu WH, et al. Tissue or liquid rebiopsy? A prospective study for simultaneous tissue and liquid NGS after first-line EGFR inhibitor resistance in lung cancer. Cancer Med. 2024;13(1):e6870. doi:10.1002/cam4.6870
123. Ottestad AL, Johansen H, Halvorsen TO, et al. Associations between detectable circulating tumor DNA and tumor glucose uptake measured by (18)F-FDG PET/CT in early-stage non-small cell lung cancer. BMC Cancer. 2023;23(1):646. doi:10.1186/s12885-023-11147-z
124. Leonetti A, Cervati V, Minari R, et al. Liquid biopsy and 18F-FDG PET/CT derived parameters as predictive factors of osimertinib treatment in advanced EGFR-mutated NSCLC. Clin Lung Cancer. 2024;25(8):e436–e445.e9. doi:10.1016/j.cllc.2024.07.016
125. Popper H. Pathologic diagnosis of lung cancer - recent developments. Curr Opin Oncol. 2024;36(1):57–62. doi:10.1097/cco.0000000000001011
126. Guibert N, Tsukada H, Hwang DH, et al. Liquid biopsy of fine-needle aspiration supernatant for lung cancer genotyping. Lung Cancer. 2018;122:72–75. doi:10.1016/j.lungcan.2018.05.024
127. Russo A, Lee JK, Pasquina LW, et al. Liquid biopsy of lung cancer before pathological diagnosis is associated with shorter time to treatment. JCO Precis Oncol. 2024:
128. Li J, Dong W, Liu LN, Huang YJ, Xiao MF. Liquid biopsy for ALK-positive early non-small-cell lung cancer predicts disease relapse. Future Oncol. 2021;17(1):81–90. doi:10.2217/fon-2020-0554
129. Cai J, Wang W, Zhang W. A meta-analysis of liquid biopsy versus tumor histology for detecting EGFR mutations in non-small cell lung cancer. Transl Oncol. 2024;47:102022. doi:10.1016/j.tranon.2024.102022
130. Ricordel C, Friboulet L, Facchinetti F, Soria JC. Molecular mechanisms of acquired resistance to third-generation EGFR-TKIs in EGFR T790M-mutant lung cancer. Ann Oncol. 2018;29(suppl_1):i28–i37. doi:10.1093/annonc/mdx705
131. Garcia J, Kamps-Hughes N, Geiguer F, et al. Sensitivity, specificity, and accuracy of a liquid biopsy approach utilizing molecular amplification pools. Sci Rep. 2021;11(1):10761. doi:10.1038/s41598-021-89592-8
132. Boehm KM, Khosravi P, Vanguri R, Gao J, Shah SP. Harnessing multimodal data integration to advance precision oncology. Nat Rev Cancer. 2022;22(2):114–126. doi:10.1038/s41568-021-00408-3
133. Liu C, Shi J, Wang H, et al. Population-level economic burden of lung cancer in China: provisional prevalence-based estimations, 2017-2030. Chin J Cancer Res. 2021;33(1):79–92. doi:10.21147/j.issn.1000-9604.2021.01.09
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.