")
Back to Journals » Nature and Science of Sleep » Volume 16
Navigating Mendelian Randomization in Sleep Medicine: Challenges, Opportunities, and Best Practices
Authors BaHammam AS , Jahrami H
Received 9 September 2024
Accepted for publication 19 November 2024
Published 22 November 2024 Volume 2024:16 Pages 1811—1825
DOI https://doi.org/10.2147/NSS.S495411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Ahmed S BaHammam,1,2 Haitham Jahrami3,4
1The University Sleep Disorders Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Department of Psychiatry, Government Hospitals, Manama, Bahrain; 4Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain
Correspondence: Ahmed S BaHammam, Department of Medicine, College of Medicine, University Sleep Disorders Center, King Saud University, Box 225503, Riyadh, 11324, Saudi Arabia, Tel +966-11-467-9495, Fax +966-11-467-9179, Email [email protected]
Abstract: Mendelian randomization (MR) has become an influential method for elucidating causal links between sleep traits and disorders, and health outcomes. This article provides sleep medicine specialists with an overview of MR, emphasizing its applications and limitations in health research, particularly in the context of sleep research. The article addresses key challenges in conducting and interpreting MR studies on sleep, focusing on the core assumptions of relevance, exchangeability, and exclusion restriction. The importance of proper genetic instrument selection, bias mitigation, and cautious result interpretation is emphasized. Strategies are recommended to enhance the quality of MR studies in sleep medicine, including collaborations between MR experts and sleep specialists. The paper also explores sleep medicine-specific issues like analyzing binary traits and addressing heterogeneity in pooled analyses. Guidance is provided on transparent reporting of MR findings, stressing the need for comprehensive effect estimates, confidence intervals, and p-values. We conclude by advocating for rigorous MR implementation in sleep research to deepen our understanding of sleep-health relationships. By following best practices in study design, analysis, and reporting, researchers can reinforce the credibility and impact of MR findings in sleep medicine, ultimately improving patient care and public health strategies.
Keywords: causal inference, genetic epidemiology, pleiotropy, GWAS, sleep disorders
Introduction
Mendelian randomization (MR) is an analytical approach in epidemiology that leverages genetic variants as proxies to examine possible cause-and-effect relationships between a modifiable risk factor and a health outcome of interest. By using genetic information as instrumental variables, MR aims to overcome some of the limitations of traditional observational studies in inferring causality.1 The term “Mendelian randomization” was first used in the literature by Richard Gray and Keith Wheatley in the early 1990s and was named after Gregor Mendel (“the father of genetics”), as it relies on the fundamental principles of genetic inheritance.2 Genetic epidemiologists and biostatisticians often refer to MR as “nature’s randomized trials”, “nature as a trialist”, or a “naturally occurring randomized trial”.3 Thus, by leveraging the random assortment of genetic variants during meiosis, MR can mimic the design of a randomized controlled trial and overcome some limitations of observational studies, such as confounding and reverse causation.4
At its core, Mendelian randomization operates on a simple yet powerful principle: genetic variants inherited at conception can serve as natural randomizers of exposure, mimicking the randomization process in a clinical trial. Imagine genetic variants as ‘tickets’ randomly distributed during conception, where these genetic ‘tickets’ are associated with a specific exposure—in our case, a sleep trait—but are unaffected by potential confounding factors or reverse causation. These genetic variants act as instrumental variables that help researchers estimate the causal relationship between an exposure (like sleep duration) and an outcome (such as cardiovascular disease).1 By utilizing the random allocation of genetic variants during meiosis (cell division for reproduction), MR can provide insights that traditional observational studies cannot, effectively using an individuals genetic makeup as a natural experimental design. This approach is particularly valuable in sleep research, where complex interactions between sleep traits and health outcomes make establishing causality challenging through conventional methods.5 In sleep research, MR offers a robust framework to untangle the bidirectional influences and confounding factors that frequently complicate the study of causal relationships between sleep traits and health outcomes.6
MR has gained traction as a robust method for exploring causal relationships between sleep traits and health outcomes, helping overcome the limitations of traditional observational studies.7 Sleep disorders, such as “insomnia”, “sleep apnea”, and “circadian rhythm disorders”, as well as variations in sleep duration, are prevalent and associated with various adverse health outcomes. However, the causal nature of these associations is often unclear because of the intricate interaction between sleep, lifestyle factors, and comorbidities. Mendelian randomization has become an influential method for elucidating bidirectional causal relationships between sleep characteristics and health outcomes.8
The growing accessibility of large-scale genome-wide association studies (GWAS) for sleep traits and disorders has greatly enhanced the application of MR in sleep research.9 To illustrate this and obtain a rough estimate, we conducted a PubMed search using the terms (“Mendelian Randomization” OR “Mendelian randomisation”) AND (“Sleep Disorder” OR “Sleep Disorders” OR “Insomnia” OR “Sleep Apnea” OR “Circadian Rhythm Sleep Disorder” OR “Hypersomnia” OR “Restless Legs Syndrome” OR “Sleep-wake disorders”). This search retrieved 401 articles, covering the period from January 1, 2015, to August 31, 2024, showing a clear upward trajectory (Figure 1).
 |
Figure 1 Growth of Publications Using Mendelian Randomization (MR) in Sleep Research (2015–2024). This figure illustrates the annual number of publications retrieved from a PubMed search using the terms “Mendelian Randomization” OR “Mendelian randomisation” AND various sleep-related keywords such as “Sleep Disorder”, “Insomnia”, “Sleep Apnea”, “Circadian Rhythm Sleep Disorder”, “Hypersomnia”, “Restless Legs Syndrome”, and “Sleep-wake disorders”. The total number of articles retrieved from this search is 374, and the search was conducted up to August 31, 2024. Each bar in the figure represents the number of articles published in a specific year between 2015 and 2024, showing a steady increase in the use of Mendelian Randomization (MR) in sleep research over time. |
The rising number of MR studies highlights the growing acknowledgment of “Mendelian Randomization” as an effective method for investigating causal links between sleep and health outcomes. With the continued expansion of GWAS data and advancements in MR methodologies, the use of MR is expected to play an even more prominent role in resolving the complex interactions between sleep and health.
This article provides an overview of MR for sleep medicine researchers, reviewers, and clinicians. Our goal is to outline the potential benefits and challenges of using MR in sleep research, identify common errors in MR analysis and interpretation specific to sleep studies, and offer suggestions for maintaining the quality and reliability of MR studies in this field. We also aim to clarify key concepts and terminology in straightforward language, helping readers critically evaluate MR studies in sleep research. Through these efforts, we seek to encourage a better understanding of MR principles, strengths, and limitations as its use in sleep research expands.
Potential Utility of MR in Sleep Medicine
The use of MR in sleep medicine could enhance our knowledge of the intricate connections between sleep and health. For example, MR studies can be used to explore the causal effects of sleep duration, quality, and timing on cardiometabolic diseases, mental health disorders, and cognitive function. Additionally, MR can be employed to investigate the bidirectional relationships between sleep disorders, like insomnia and sleep apnea, and other health conditions, including obesity, diabetes, and cardiovascular disease.10,11
Figure 2 illustrates the key concepts and assumptions of MR, which are central to understanding its application in sleep research.
 |
Figure 2 The flowchart illustrates the key concepts and assumptions of Mendelian randomization, a method used to assess the causal relationship between an exposure and an outcome using genetic variants. In the population, genetic variants are randomly allocated (A), ensuring they are not associated with confounding factors. Part A of Figure 2 visually illustrates the use of genetic variants as instrumental variables in MR, demonstrating how randomly inherited markers can act as proxies for exposures to help overcome limitations of traditional observational studies. For Mendelian randomization to be valid, three main assumptions must be met (B): (1) Relevance - The genetic variants must be associated with the exposure variable; (2) Exchangeability - The genetic variants should not be associated with confounding factors; and (3) Exclusion Restriction - The genetic variants should only affect the outcome through the exposure variable and not have a direct effect. When these assumptions hold, Mendelian randomization can provide evidence for a causal relationship between the exposure and clinical endpoints or health outcomes in the population. |
Furthermore, MR can be a valuable tool for identifying modifiable risk factors for sleep disorders and informing prevention and treatment strategies. By elucidating the causal pathways underlying these relationships, MR can help prioritize interventions that target the root causes of sleep disorders and their associated health consequences.12 For instance, an MR study revealed that gastroesophageal reflux disease (GERD) increases the risk of obstructive sleep apnea, insomnia, and snoring, suggesting that treating GERD could be an effective strategy for preventing and managing these conditions.13 This approach not only addresses the root causes but also has the potential to improve overall health outcomes related to sleep disorders.
As sleep medicine research progresses, the use of MR is anticipated to expand, offering fresh insights into the causal links between sleep and health. However, it is essential to recognize the limitations and assumptions of MR and to interpret the results of these studies cautiously.14 By combining evidence from MR studies with other lines of research, such as randomized controlled trials and mechanistic studies, we can achieve a deeper understanding of the impact of sleep on health and disease, ultimately leading to improved patient care and public health policies.
Common Pitfalls in MR Analysis and Interpretation
MR depends on three core assumptions: relevance, exchangeability, and exclusion restriction. These assumptions are frequently challenging to completely validate, which can introduce potential issues in interpreting MR findings.4 The three core assumptions of MR are depicted in Figure 2. Evaluating the plausibility of these assumptions is crucial for ensuring the validity of MR results in sleep research.
Part A of Figure 2 provides a comprehensive visual representation of the methodological framework and key principles underlying MR in sleep research. It illustrates the fundamental concept of genetic variants as instrumental variables, demonstrating how randomly inherited genetic markers can serve as proxies for exposures. This visual representation helps readers, particularly those less familiar with genetic epidemiology, understand how genetic inheritance mimics the randomization process in clinical trials. By showing the relationship between genetic variants, exposure, and outcome, Part A elucidates the core mechanism that allows MR to overcome traditional observational study limitations.
While MR has emerged as a powerful analytical tool, it is essential to recognize its inherent limitations and methodological complexities. MR studies primarily capture the genetic architecture of exposures, providing a valuable but partial perspective on complex biological relationships. Researchers must be aware that genetic variants represent only one dimension of a trait, inevitably excluding the crucial environmental and contextual factors that shape human biology. This limitation is particularly significant in fields like sleep research, where environmental influences such as light exposure, work schedules, and lifestyle factors profoundly interact with genetic predispositions. Computational biologists and researchers without specialized knowledge in medical domains, such as sleep medicine, may unintentionally oversimplify these intricate interactions. We strongly advocate for interdisciplinary collaboration to ensure that MR studies are both designed and interpreted with a comprehensive biological understanding. For reviewers and future researchers, this involves moving beyond statistical analysis alone to incorporate sophisticated biological insights, recognizing that genetic instruments offer a valuable but incomplete view into causal mechanisms.
The Three Core Assumptions of Mendelian Randomization
The first assumption, known as the “Relevance Assumption”, indicates that the genetic instrument must have a strong association with the exposure of interest. In the context of sleep research, this means that the chosen genetic variants need to exert a strong and consistent influence on the sleep trait or disorder being studied. Weak or inconsistent associations between the genetic instrument and the exposure can lead to weak instrument bias, which can distort the causal estimates and limit the power of the MR analysis.1 For example, if genetic variants chosen as instruments for sleep duration have only weak associations with actual sleep patterns, they violate the “Relevance Assumption”. This can introduce weak instrument bias, potentially leading to imprecise or biased estimates of sleep duration’s causal effects on health outcomes like obesity.
The second assumption, the “Exchangeability Assumption”, requires that the genetic instrument is not linked to any confounding factors affecting the exposure-outcome relationship. In sleep research, potential confounders may include factors such as age, sex, lifestyle habits, and comorbidities. Violation of this assumption can occur due to population stratification, assortative mating, or dynastic effects, which can introduce bias into the MR estimates.15 For instance, in an MR study examining the relationship between insomnia and cardiovascular disease, the “Exchangeability Assumption” could be violated if genetic variants associated with insomnia are also linked to socioeconomic status, which independently affects cardiovascular risk. This potential violation underscores the importance of considering factors like population stratification and lifestyle habits when interpreting MR results in sleep research.5
The third assumption, known as the “Exclusion Restriction Assumption”, indicates that the genetic instrument should influence the outcome solely through its impact on the exposure. In other words, the genetic instrument should have no direct effect on the outcome, and there should be no alternative pathways through which the instrument can impact the outcome. A breach of this assumption, commonly known as horizontal pleiotropy (Figure 3), may result in biased causal estimates and misleading conclusions about the exposure-outcome relationship.16 For instance, if a genetic variant related to insomnia also directly affects cardiovascular outcomes through biological pathways independent of sleep (such as inflammatory responses), it would violate the “Exclusion Restriction Assumption”. This horizontal pleiotropy could bias MR estimates, leading to incorrect conclusions about the causal effect of insomnia on heart disease.
 |
Figure 3 Vertical and Horizontal Pleiotropy in Sleep Research. This figure demonstrates the concepts of vertical and horizontal pleiotropy in Mendelian randomization studies focused on sleep traits and disorders. Panel A illustrates vertical pleiotropy, where Single Nucleotide Polymorphisms (SNPs) influence the cardiovascular (CVS) outcome through a linear pathway involving Sleep Apnea and Sleep Duration. This represents the desired causal pathway in MR studies. Panel B depicts horizontal pleiotropy, where SNPs can affect the CVS outcome through multiple pathways. In this case, SNPs independently influence both sleep apnea and sleep duration, which in turn affect CVS outcomes. Additionally, SNPs may have direct effects on the CVS outcome that are not mediated by sleep traits. This complex network of relationships highlights the challenges in interpreting MR results and the importance of accounting for potential pleiotropic effects when studying the causal relationships between sleep traits and health outcomes. Understanding these concepts is essential for researchers and clinicians interpreting MR studies in sleep medicine, as horizontal pleiotropy can lead to biased estimates of causal effects if not adequately addressed in the analysis. |
Table 1 summarizes how Richmond et al addressed the three core principles of Mendelian Randomization in their study on sleep traits and breast cancer risk.17
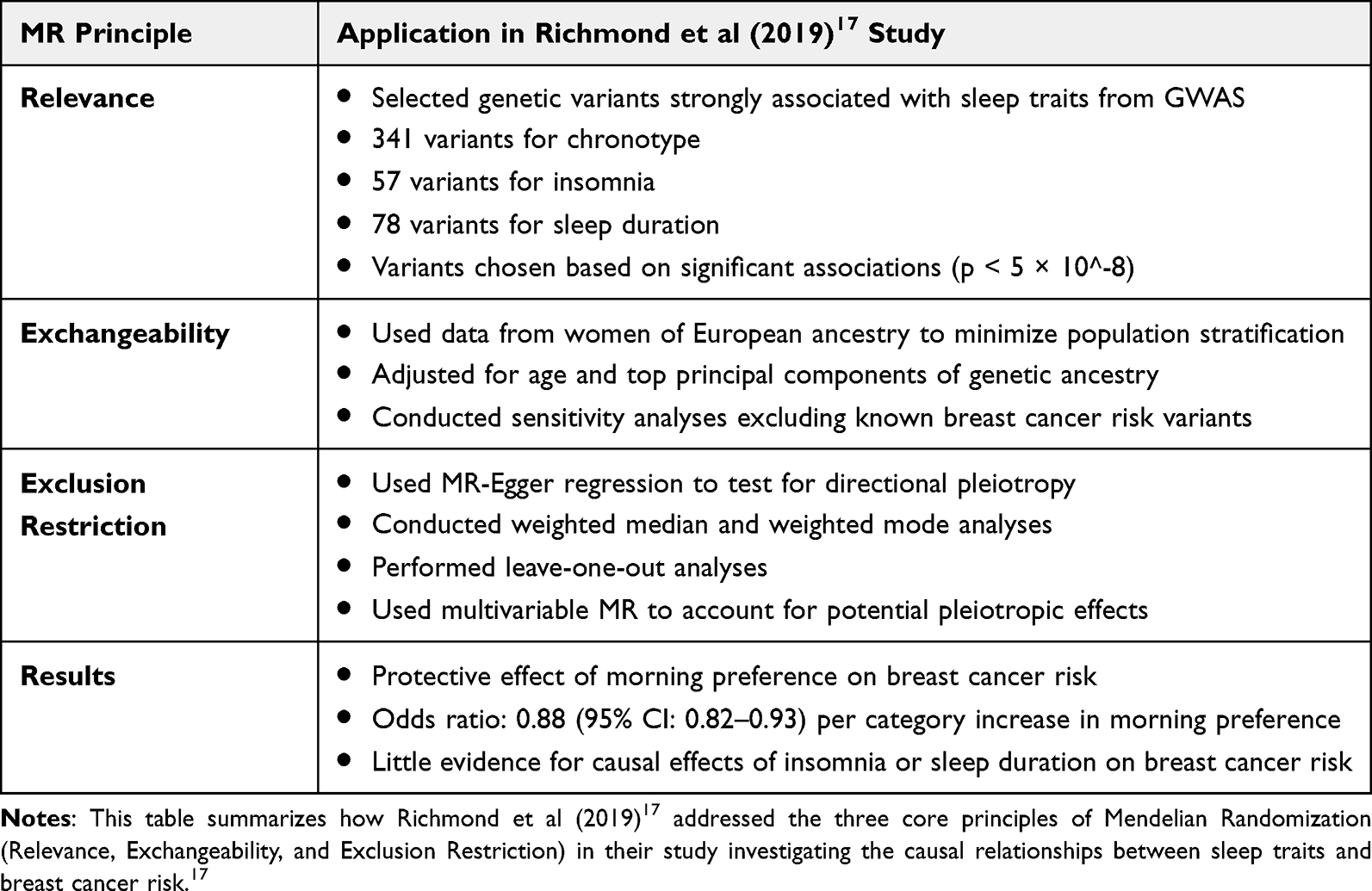 |
Table 1 Application of Mendelian Randomization Principles in Sleep Research |
Assessing the plausibility of the core assumptions in MR studies requires a thorough understanding of the biological mechanisms driving the exposure, outcome, and genetic instruments.18 This is particularly important in the context of sleep research, where the complex interplay between sleep traits, disorders, and health outcomes may not be fully understood by researchers who are not sleep medicine experts.
For researchers conducting MR studies on sleep, it is imperative to carefully consider the potential for violating these assumptions and to employ sensitivity analyses to test the robustness of their findings. However, without a comprehensive understanding of the biology of sleep and its associated disorders, researchers may overlook important factors that could lead to biased results or misinterpretations.
To address this issue, it is strongly recommended that researchers who are not sleep medicine experts collaborate with sleep specialists when designing and conducting MR studies in this field. Sleep specialists can provide valuable insights into the biological mechanisms underlying sleep traits and disorders, as well as the potential confounders and mediators that may influence the exposure-outcome relationship. They can also aid in selecting the most suitable genetic instruments and evaluating the plausibility of MR assumptions within the context of sleep research.
For reviewers evaluating MR studies on sleep, it is equally important to consider the expertise of the research team and the involvement of sleep specialists. Reviewers should carefully assess whether the researchers have adequately addressed the potential for violations of the MR assumptions and whether they have employed appropriate sensitivity analyses to test the robustness of their findings. If the research team lacks expertise in sleep medicine, reviewers may recommend seeking input from sleep specialists to strengthen the study’s validity and reliability.
Binary Exposure Variable
Another challenge is that many exposures and outcomes of interest in sleep research are binary traits, meaning they have only two possible outcomes, such as whether a sleep disorder is present or absent. When conducting MR analyses with binary traits, researchers face additional challenges, as the assumptions of linear and uniform causal effects may not apply.19
In sleep research, many outcomes of interest, such as the presence or absence of a sleep disorder, are binary. Analyzing binary traits in MR necessitates specific considerations and the application of suitable statistical techniques, such as the ratio estimator or the two-stage estimator, to obtain valid causal estimates.20
Moreover, the assumption of homogeneous causal effects suggests that the effect of the exposure on the outcome is consistent across all individuals in the population, which may not hold true for binary traits. The impact of a binary exposure on a binary outcome may differ based on factors like the baseline risk of the outcome or the presence of additional risk factors.21
To address these challenges, researchers must use appropriate statistical methods when analyzing binary traits in MR studies. One common approach is the use of the “ratio estimator”, which involves assessing the genetic association with both the exposure and the outcome separately and then calculating their ratio. Another approach is the “two-stage estimator”, which first estimates the genetically predicted probability of the binary exposure and then uses this predicted probability as the exposure variable in a second-stage regression analysis.20
It is important for researchers to carefully consider the assumptions underlying these statistical methods and to interpret the results cautiously. The causal estimates obtained from MR analyses with binary traits may not have the same straightforward interpretation as those obtained from analyses with continuous traits. Researchers should also be aware of potential biases that can arise when dealing with binary traits, such as “collider bias” or “selection bias”.22
For non-genetic-epidemiologists, it is essential to understand that analyzing binary traits in MR studies requires specialized statistical methods and careful interpretation of the results. When reviewing MR studies on sleep disorders or other binary outcomes, it is important to assess whether the researchers have used appropriate methods and have adequately addressed the challenges associated with binary traits. Collaborating with statisticians or genetic epidemiologists can help ensure that the analysis is conducted correctly and that the results are interpreted appropriately.
Advanced MR Methodological Considerations
Sample Overlap in Two-Sample MR
Two-sample Mendelian randomization (MR) studies can be susceptible to bias when there is overlap between the samples used to estimate genetic associations with the exposure and outcome. This overlap can lead to inflated type I error rates and biased causal estimates, particularly when the same individuals contribute data to both samples.23 To address this issue, researchers have developed several methods to detect and correct for sample overlap in two-sample MR analyses.
When using large biobanks or overlapping datasets, researchers can employ the MRlap method to assess and correct for potential sample overlap bias.24 This approach uses linkage disequilibrium score regression to estimate the degree of overlap between exposure and outcome samples, allowing for more accurate causal estimates. MRlap also corrects for biases such as weak instrument bias and winner’s curse, which are especially relevant when exposure and outcome samples overlap significantly. In these scenarios, traditional inverse variance weighted Mendelian randomization (IVW-MR) methods might underestimate or overestimate the causal effects, depending on the degree of overlap. MRlap tackles these issues by analytically correcting for the bias, making it robust even with high levels of polygenicity or low heritability traits.24 For instance, a recent study by Hu et al examining the causal link between sleep duration and leukocyte telomere length emphasizes the significance of addressing potential overlap in genetic datasets.25 This investigation employed genetic epidemiological methods, specifically MR and colocalization techniques, to examine the potential relationship linking reduced sleep time and morning chronotype to telomere length, demonstrating the utility of MRlap for minimizing bias and improving the reliability of results when datasets overlap.25 However, researchers should be aware that applying MRlap to sleep studies may face challenges such as the complex genetic architecture of sleep traits and potential unmeasured confounders specific to sleep behaviors. Despite these limitations, MRlap holds the promise of greatly enhancing the precision of causal estimates in sleep genetics research, potentially offering more reliable insights into the genetic basis of sleep disorders and their connections to other health outcomes. In addition to MRlap, other methods like LD Score Regression (Linkage Disequilibrium Score Regression) and SOMR (Sample Overlap MR) can also be utilized to identify and adjust for sample overlap in two-sample MR studies. While LD Score Regression primarily addresses genetic confounding through linkage disequilibrium patterns, MRlap provides a direct correction for overlap bias, offering a more comprehensive solution for improving causal inference accuracy. By implementing these methods, researchers can enhance the reliability of their findings and mitigate concerns about bias due to sample overlap.
Network Mendelian Randomization
Network MR extends traditional MR by examining multiple exposures and outcomes simultaneously, allowing for the exploration of complex causal pathways in sleep research.26 This approach is particularly useful for investigating mediating effects and identifying potential causal mechanisms linking sleep traits to various health outcomes.27 For instance, network MR has been employed to elucidate the causal pathway from insomnia to type 2 diabetes, considering multiple potential mediators such as body mass index (BMI) and blood glucose levels.28 While network MR offers enhanced insights into complex relationships, it requires careful consideration of assumptions and potential biases, particularly when dealing with multiple binary traits common in sleep disorders research.29
Multivariable Mendelian Randomization
Multivariable Mendelian Randomization (MVMR) represents a sophisticated extension of traditional MR methods, allowing researchers to simultaneously account for multiple potential confounding exposures. In sleep research, MVMR is particularly powerful for disentangling complex, interrelated traits. For instance, consider a scenario investigating the causal relationship between sleep duration and cardiovascular disease while simultaneously controlling for BMI and inflammatory markers. Traditional single-exposure MR might conflate these relationships, but MVMR can provide a more nuanced understanding by estimating the direct effect of sleep duration on cardiovascular risk, independent of BMI and inflammation. Sanderson and colleagues’ seminal work provides a robust framework for conducting MVMR analyses, emphasizing the importance of carefully selecting genetic instruments that are conditionally independent across multiple exposures.30 In practice, this means ensuring that the genetic variants used as instruments for sleep duration do not simultaneously serve as strong predictors of BMI or inflammatory markers, thus maintaining the core MR assumptions of relevance and exclusion restriction across multiple exposures. This careful selection is essential; if genetic variants influence both the primary exposure (sleep duration) and confounders (BMI or inflammatory markers), it could bias the results, misrepresenting the causal effect of sleep duration on cardiovascular disease.
These advanced methodological approaches—sample overlap correction, network MR, and multivariable MR—represent critical refinements in causal inference techniques for sleep research. By addressing potential biases, exploring complex causal pathways, and accounting for multiple exposures simultaneously, these methods enhance our ability to explore the complex relationships between sleep traits, disorders, and health outcomes. As sleep medicine continues to evolve, these sophisticated analytical techniques will be instrumental in providing more precise, reliable insights into the causal mechanisms underlying sleep-related health phenomena.
Selecting Appropriate Genetic Instruments in Sleep MR Studies
Researchers face a trade-off when choosing genetic markers (SNPs) for MR studies. Using less stringent selection criteria (like P<5×10−6) increases the number of available SNPs, but this may include variants that are weakly linked to the sleep trait being studied, potentially leading to unreliable results. A looser threshold also raises the risk of including SNPs that affect the outcome through multiple pathways, not just through the sleep trait we are interested in. This is called horizontal pleiotropy and can bias findings.31 When selecting genetic instruments, researchers should also consider the strength of these instruments using F-statistics.
Generally, an F-statistic greater than 10 indicates a strong instrument.32 However, while F-statistics help evaluate instrument strength, they have limitations, particularly when relaxed p-value thresholds are used. In sleep research, where genetic architecture is often complex, relying solely on F-statistics can be misleading. Researchers should transparently report both their p-value threshold choices and corresponding F-statistics, discussing potential impacts on results. This promotes a rigorous methodology and enhances the accuracy of MR findings in sleep studies.33,34
Another key factor when choosing genetic instruments for sleep MR studies is the application of “Steiger filtering”. This technique helps mitigate potential reverse causation by ensuring that the selected genetic variants are more strongly associated with the exposure (eg, sleep trait) than with the outcome.35 In sleep research, where bidirectional relationships are common (eg, between sleep duration and obesity), Steiger filtering can help strengthen causal inferences. For instance, researchers investigating the causal effect of sleep duration on BMI would use Steiger filtering to select genetic variants that are more strongly associated with sleep duration than with BMI. This approach reduces the risk of including variants that primarily influence BMI and only secondarily affect sleep duration, which could lead to biased estimates of the causal effect.36
To address these issues, researchers often perform additional checks. They might rerun their analysis with a stricter SNP selection (like P<5×10−8) to see if the results hold up. They also use special statistical techniques, such as MR-Egger regression, to spot and adjust for SNPs that might be influencing the outcome in unexpected ways.37 By taking these extra steps, researchers can be more confident that MR results truly reflect the relationship between sleep traits and health outcomes.38
In sleep research, where the genetic architecture of many traits is still being uncovered, balancing statistical power and instrument validity is necessary. Researchers should consider the sample size of the original genome-wide association studies used to identify genetic instruments when selecting an appropriate threshold.1 By carefully justifying their threshold choice and conducting thorough sensitivity analyses, researchers can enhance the reliability and interpretability of their MR findings in sleep medicine, contributing to a more robust understanding of causal relationships between sleep traits, disorders, and health outcomes.18
Justifying the Selection of Exposure and Outcome Variables
Justifying the selection of exposure and outcome variables is necessary for the validity and interpretability of sleep-related MR studies. Researchers should provide a clear rationale for their chosen variables based on prior knowledge, biological plausibility, and the availability of robust genetic instruments.38 Sleep traits should be carefully defined and measured using validated tools,8 and outcome variables should be clinically relevant with a plausible biological link to sleep exposure.17 For instance, in an MR study investigating the causal effect of sleep duration on the risk of type 2 diabetes, the researchers should select sleep duration as the exposure variable based on prior evidence linking sleep patterns to metabolic health. Type 2 diabetes would be a suitable outcome due to its plausible biological connection to sleep regulation, supported by existing literature.
When selecting genetic instruments, researchers should prioritize variants with a strong and specific association with sleep exposure, as supported by well-powered GWAS.9 The choice of genetic instruments should also consider possible confounding factors, like population stratification and pleiotropy.31 Additionally, genetic instruments used should be derived from well-powered GWAS showing a robust association with sleep duration, while accounting for confounders like population stratification to ensure valid conclusions.
Challenges in Interpreting Pooled Results (Heterogeneity)
The heterogeneity of effects across different populations can pose challenges when interpreting the results of pooled MR studies in sleep research.38 This is especially important for non-genetic-epidemiologists to understand since they may not fully comprehend the intricacies of genetic associations and how these can differ across various subgroups when studying sleep traits and disorders. For example, in a pooled MR study investigating the relationship between sleep apnea and hypertension across multiple populations, environmental factors such as urban noise exposure may differ significantly between populations. If these environmental differences are correlated with both the genetic variants associated with sleep apnea and the hypertension outcome, they could introduce heterogeneity and violate MR assumptions. Without accounting for this variation, the pooled causal estimate might overstate or understate the true effect in any given population.
When combining data from multiple populations in an MR study of sleep, it is mandatory to consider these potential sources of heterogeneity. Failure to account for these differences can lead to biased or misleading results, as the pooled causal estimate may not accurately represent the true effect in any single population.36 This is particularly concerning when heterogeneity is related to environmental factors, such as noise exposure or light pollution, as these factors may be correlated with both the genetic instruments and the sleep outcomes, violating the MR assumptions.39
To address this issue, researchers can employ various methods to explore and account for heterogeneity in MR studies of sleep. One approach is to use “meta-regression”, which allows for the investigation of study-level covariates that may explain the variability in effect sizes across different populations.40 Another approach is to conduct “subgroup analyses”, stratifying the data by factors such as ancestry, age, or sex, and estimating causal effects separately within each subgroup.38
Researchers should be aware of these potential sources of heterogeneity when interpreting the results of pooled MR studies in sleep research. They should carefully assess whether the researchers have adequately explored and accounted for these differences, and consider the implications of any observed heterogeneity for the generalizability and validity of the findings. Collaborating with genetic-epidemiologists or statisticians can help ensure these issues are properly addressed and the results are interpreted appropriately.
Factors Influencing Causal Effects
In MR studies of sleep, the strength and direction of causal effects may vary depending on factors such as ancestry, age, sex, and environmental context.39 For example, genetic variants associated with a sleep disorder like insomnia may have different effect sizes in populations of European ancestry compared to those of African ancestry. Similarly, the causal effect of sleep exposure, such as sleep duration, on a health outcome may be stronger in older individuals compared to younger ones, or in males compared to females.6
Interpreting Clinical Relevance of MR Findings
When interpreting MR studies on sleep traits and disorders, it is necessary to consider the clinical relevance of identified mediating effects, even if they appear modest. Small effect sizes can still offer important insights into the complex interactions between sleep and health.38 Researchers should evaluate whether the observed effects align with existing literature, as consistency can strengthen the credibility of results and highlight potential clinical implications.41 For example, in an MR study investigating the causal relationship between insomnia and cardiovascular disease, a small but significant effect size may suggest that insomnia contributes modestly to cardiovascular risk. While the clinical impact of this small effect might be limited on an individual level, it could still have substantial public health implications, given the high prevalence of insomnia in the population.5
Acknowledging the limitations of small effect sizes is important. While they may have limited immediate clinical impact on an individual level, they can contribute to understanding underlying mechanisms linking sleep and health outcomes.11 Moreover, small effects in large, well-powered MR studies may indicate causal relationships with meaningful implications on a population scale, particularly given the widespread occurrence of sleep disorders.12
To build upon findings with small mediating effects, researchers should discuss the need for future investigations to further explore and validate causal pathways. This may involve larger, more diverse MR studies and complementary research methods to triangulate evidence and assess consistency across different study designs.38,42
Pleiotropy
Pleiotropy is a fundamental concept in MR studies that can significantly influence the validity of the results. In simple terms, pleiotropy arises when a single genetic variant affects multiple traits or outcomes. If not properly addressed, this can result in biased estimates, as the genetic variant might influence the outcome through pathways unrelated to the exposure under investigation.31
For non-specialists, it is essential to understand that pleiotropy can manifest in two main ways: vertical and horizontal. Vertical pleiotropy occurs when the genetic variant influences the outcome through exposure, which is the desired pathway in MR studies. However, horizontal pleiotropy occurs when a genetic variant directly affects the outcome, independent of the exposure, potentially causing biased results in MR studies. This direct effect on the outcome, not mediated by the exposure, violates the “exclusion restriction assumption” and can distort the causal estimates, making it challenging to interpret the findings accurately.16 For instance, if a genetic variant associated with sleep duration also directly affects cardiovascular health through a separate pathway, the MR analysis may incorrectly attribute the effect on cardiovascular health to sleep duration, leading to misleading conclusions.
Figure 3 illustrates the concepts of vertical and horizontal pleiotropy in the context of sleep research.
To address pleiotropy, researchers use various methods, such as “MR-Egger regression”, which allows for the estimation of a non-zero intercept to account for directional pleiotropy.16 Other approaches include the use of weighted median and mode-based estimators, which can be more robust to outliers and pleiotropic effects.43 These methods help ensure that the causal estimates obtained from MR studies are reliable and not influenced by pleiotropic effects.
To ensure the accurate interpretation of MR studies, readers and reviewers must be cautious about the potential for horizontal pleiotropy. When reading MR studies and interpreting reported results, it is essential to assess whether the researchers have employed methods to detect and adjust for pleiotropic effects, such as “MR-Egger regression” or “weighted median estimators”, to ensure the robustness of the causal estimates. This scrutiny helps distinguish between true causal effects and those biased by direct influences of genetic variants on the outcome.
Limitations Related to Databases Used in MR Studies
Limitations related to the databases used in MR studies can significantly impact the validity and generalizability of the findings, particularly in the context of sleep disorders research. One crucial aspect that non-sleep medicine specialist researchers might overlook is the accuracy of sleep disorder diagnoses in the databases.41,44 Misclassification or inconsistencies in the diagnostic criteria used across different databases can lead to biased estimates of the causal effects and hinder the comparability of results across studies.45,46
The UK Biobank is a commonly used resource in MR studies due to its large sample size and extensive genetic and phenotypic data.47 However, it is important to recognize that the UK Biobank may not be representative of all populations, as it primarily consists of individuals of European ancestry from the United Kingdom.48 This limitation can affect the generalizability of the findings to other populations with different genetic backgrounds and environmental exposures.4
Furthermore, sample sizes and statistical power may be limited for less common sleep disorders, such as narcolepsy or circadian rhythm sleep-wake disorders.8 Smaller sample sizes can lead to increased uncertainty in the causal estimates and reduced ability to detect significant associations.49 This issue is particularly relevant when investigating the causal effects of rare genetic variants or when stratifying the analyses by subgroups, such as age or sex.15
To address these limitations, researchers should carefully evaluate the quality and consistency of sleep disorder diagnoses in the databases used for MR studies. Collaborating with sleep medicine experts can help ensure that the diagnostic criteria are appropriate and uniformly applied across the datasets. Additionally, researchers should be cautious when extrapolating the findings from specific populations to diverse groups and consider the potential impact of population stratification on the results.
When dealing with less common sleep disorders, researchers may need to combine data from multiple sources or use alternative study designs, such as two-sample MR, to increase the sample size and statistical power.50,51 To address issues related to small sample sizes in MR studies, researchers can employ several strategies:
Power calculations: Conducting a priori power calculations can help determine the minimum sample size needed to detect a meaningful effect, guiding researchers on the feasibility of their study.52
Two-sample MR: This approach can increase statistical power by using summary data from large GWAS for both exposure and outcome, potentially overcoming small sample size limitations in individual studies.53
Allele score approach: Using multiple genetic variants combined into an allele score can increase the proportion of variance explained in the exposure, thereby improving power.54
Bias correction methods: Techniques like MRlap can simultaneously correct for weak instrument bias and winner’s curse while accounting for potential sample overlap, which is particularly useful when working with small samples.24
Efficient study design: In some cases, using subsample approaches to measure the exposure can maintain statistical power while reducing costs, but ensuring a sufficiently large sample size remains essential to minimize bias.55
These approaches, used individually or in combination, can help address the challenges posed by small sample sizes in MR studies, improving the reliability and interpretability of results. This is especially important in the context of rare sleep disorders, where small sample sizes may limit the power to detect causal relationships.
Recommendations for Authors and Reviewers
Authors’ Responsibilities
When conducting MR studies on sleep traits and disorders, it is essential for authors to meticulously evaluate and justify the plausibility of the three core MR assumptions.56 This involves providing a clear rationale for the selection of genetic instruments, demonstrating their strong association with the exposure, and assessing potential violations of these assumptions, such as horizontal pleiotropy.31 Authors should also be transparent about the limitations of their study and the potential impact of assumption violations on the interpretation of the results.
For instance, they should discuss how they addressed issues like pleiotropy, which can arise when a genetic variant influences multiple traits, potentially leading to biased estimates if not properly accounted for.31 Additionally, authors should consider the robustness of their findings by using sensitivity analyses and alternative approaches to minimize the effects of assumption violations.18
Reporting MR Results
When presenting bidirectional MR results, it is important to report comprehensive statistical information. This includes effect estimates, confidence intervals, and p-values for both directions of the analysis (exposure to outcome and vice versa). Clear reporting of these metrics allows for accurate interpretation of the magnitude, precision, and statistical significance of the estimated causal effects.18 For example, in sleep research, one might report: “A genetically predicted 1-hour increase in sleep duration was associated with a 0.5 kg/m² decrease in BMI (95% CI: −0.8 to −0.2, p=0.001)”. This level of detail allows readers to evaluate the robustness and dependability of the evidence supporting causal relationships between sleep traits and health outcomes.1 Consistent reporting practices also facilitate comparisons across studies and meta-analyses, enhancing the overall quality of evidence in sleep medicine research.56
Reviewers’ Responsibilities
Reviewers play a critical role in ensuring the quality and reliability of MR studies in sleep research. They should critically appraise the appropriateness of the databases and phenotype definitions used, ensuring that these are valid and consistent across different datasets.38 This includes evaluating the study population’s representativeness and the precision of sleep disorder diagnoses, which are essential components of the research methodology.45 Reviewers should also scrutinize the authors’ justification of the MR assumptions and their efforts to address potential violations, such as the use of sensitivity analyses and alternative methods.18 If the research team lacks expertise in sleep medicine, reviewers may recommend seeking input from sleep specialists to strengthen the study’s validity and reliability.
Interpreting Results
Results from MR studies on sleep traits and disorders should be interpreted cautiously, considering potential assumption violations, heterogeneity, and consistency with other lines of evidence.39 Authors should acknowledge the limitations of their findings and avoid overstating causal claims, particularly when the assumptions are not fully met or when there is inconsistency across different analyses.57 Reviewers should ensure that authors offer a well-rounded interpretation of the findings, considering both the strengths and limitations of the study design, as well as the broader context of the research question.38
Biological Plausibility and Mechanisms
When interpreting MR results in sleep research, examining the biological plausibility of identified causal relationships is necessary. Researchers should consider known sleep physiology and pathways, such as circadian rhythm regulation or neurotransmitter systems, to contextualize findings.58 For instance, an MR study linking insomnia to cardiovascular disease should explore potential mechanisms like autonomic dysfunction or inflammation.5 Integrating MR results with experimental studies, such as animal models or human interventions, can provide deeper insights into causal mechanisms.9 This approach enhances the credibility of MR findings and guides future research directions in sleep medicine.
Guidelines for Reporting MR Studies
To enhance the reporting quality of MR studies, authors can follow guidelines similar to those outlined in the STROBE-MR checklist.56 This includes providing detailed descriptions of the study design, data sources, genetic instrument selection, and statistical methods used. Authors should also report any sensitivity analyses conducted to evaluate the reliability of the results and address the clinical significance and generalizability of the findings.
Rigorous and transparent reporting of MR studies on sleep traits and disorders requires a collaborative effort from authors, reviewers, and editors. By carefully evaluating the plausibility of assumptions, critically appraising data sources and methods, and interpreting results cautiously, the scientific community can ensure that MR findings in sleep research are reliable, informative, and contribute to advancing our understanding of the causal relationships between sleep and health outcomes.
Conclusion
MR is a potent tool with the potential to significantly advance sleep medicine research by uncovering causal relationships between sleep traits, disorders, and various health outcomes. However, like any research methodology, MR comes with its own unique challenges and limitations that need to be carefully managed to guarantee the robustness and reliability of the findings.
This article has underscored several critical issues that researchers, reviewers, and readers should be aware of when conducting, evaluating, or interpreting MR studies in sleep research. These involve the need to assess the credibility of the core MR assumptions, recognizing and mitigating potential biases such as pleiotropy, and interpreting results cautiously in the context of assumption violations, heterogeneity, and consistency with other lines of evidence.
To ensure that MR studies in sleep medicine meet the highest standards and contribute meaningfully to our understanding of the causal relationships between sleep and health, the scientific community must be aware of these challenges and limitations. Researchers should adhere to best practices in study design, analysis, and reporting, while reviewers and editors should critically evaluate the suitability of the methods employed and the accuracy of the conclusions reached.
By enhancing awareness and scrutiny of the key issues highlighted in this editorial, we can promote a more rigorous and reliable application of MR in sleep research. This increased rigor will help advance our understanding of the complex interplay between sleep and health, ultimately leading to improved patient care and more effective public health policies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
2. Davey Smith G. Capitalizing on Mendelian randomization to assess the effects of treatments. J R Soc Med. 2007;100(9):432–435. doi:10.1177/014107680710000923
3. Swanson SA, Tiemeier H, Ikram MA, Hernán MA. Nature as a Trialist?: deconstructing the Analogy Between Mendelian Randomization and Randomized Trials. Epidemiology. 2017;28(5):653–659. doi:10.1097/EDE.0000000000000699
4. Davey Smith G, Ebrahim S. ‘Mendelian randomization’: can genetic epidemiology contribute to understanding environmental determinants of disease?*. Int J Epidemiol. 2003;32(1):1–22. doi:10.1093/ije/dyg070
5. Lane JM, Jones SE, Dashti HS, et al. Biological and clinical insights from genetics of insomnia symptoms. Nat Gen. 2019;51(3):387–393. doi:10.1038/s41588-019-0361-7
6. Wang J, Wang Y, Jiang CQ, et al. Associations Between Sleep Traits and Social Isolation: observational and Bidirectional Mendelian Randomization Study. J Gerontol a Biol Sci Med Sci. 2024;79(1):233. doi:10.1093/gerona/glad233.
7. Hu Y, Shmygelska A, Tran D, Eriksson N, Tung JY, Hinds DA. GWAS of 89,283 individuals identifies genetic variants associated with self-reporting of being a morning person. Nat Commun. 2016;7(1):10448. doi:10.1038/ncomms10448
8. Dashti HS, Redline S, Saxena R. Polygenic risk score identifies associations between sleep duration and diseases determined from an electronic medical record biobank. Sleep. 2019;42(3). doi:10.1093/sleep/zsy247
9. Wang H, Lane JM, Jones SE, et al. Genome-wide association analysis of self-reported daytime sleepiness identifies 42 loci that suggest biological subtypes. Nat Commun. 2019;10(1):3503. doi:10.1038/s41467-019-11456-7
10. Li P, Dong Z, Chen W, Yang G. Causal Relations Between Obstructive Sleep Apnea and Stroke: a Mendelian Randomization Study. Nat Sci Sleep. 2023;15:257–266. doi:10.2147/NSS.S398544
11. Zhang X, Sun Y, Ye S, et al. Associations between insomnia and cardiovascular diseases: a meta-review and meta-analysis of observational and Mendelian randomization studies. J Clin Sleep Med. 2024;2024:11326. doi:10.5664/jcsm.11326
12. Li Y, Miao Y, Tan J, Zhang Q. Association of modifiable risk factors with obstructive sleep apnea: a Mendelian randomization study. Aging. 2023;15(23):14039–14065. doi:10.18632/aging.205288
13. Qin S, Wang C, Wang X, Wu W, Liu C. Causal association of gastroesophageal reflux disease with obstructive sleep apnea and sleep-related phenotypes: a bidirectional two-sample Mendelian randomization study. Front Neurol. 2023;14:1283286. doi:10.3389/fneur.2023.1283286
14. Evans DM, Davey SG. Mendelian Randomization: new Applications in the Coming Age of Hypothesis-Free Causality. Annu Rev Genomics Hum Genet. 2015;16:327–350.
15. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
16. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
17. Richmond RC, Anderson EL, Dashti HS, et al. Investigating causal relations between sleep traits and risk of breast cancer in women: Mendelian randomisation study. BMJ. 2019;365:l2327. doi:10.1136/bmj.l2327
18. Burgess S, Davey Smith G, Davies NM, et al. Guidelines for performing Mendelian randomization investigations: update for summer 2023. Wellcome Open Res. 2023;4:186. doi:10.12688/wellcomeopenres.15555.3
19. Burgess S, Labrecque JA. Mendelian randomization with a binary exposure variable: interpretation and presentation of causal estimates. Eur J Epidemiol. 2018;33(10):947–952. doi:10.1007/s10654-018-0424-6
20. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
21. VanderWeele TJ, Hernán MA. Results on Differential and Dependent Measurement Error of the Exposure and the Outcome Using Signed Directed Acyclic Graphs. Am J Epidemiol. 2012;175(12):1303–1310. doi:10.1093/aje/kwr458
22. Gkatzionis A, Burgess S. Contextualizing selection bias in Mendelian randomization: how bad is it likely to be? Int J Epidemiol. 2018;48(3):691–701. doi:10.1093/ije/dyy202
23. Burgess S, Davies NM, Thompson SG. Bias due to participant overlap in two-sample Mendelian randomization. Genet Epidemiol. 2016;40(7):597–608. doi:10.1002/gepi.21998
24. Mounier N, Kutalik Z. Bias correction for inverse variance weighting Mendelian randomization. Genet Epidemiol. 2023;47(4):314–331. doi:10.1002/gepi.22522
25. Hu J, Lu J, Lu Q, Weng W, Guan Z, Wang Z. Mendelian randomization and colocalization analyses reveal an association between short sleep duration or morning chronotype and altered leukocyte telomere length. Commun Biol. 2023;6(1):1014. doi:10.1038/s42003-023-05397-7
26. Burgess S, Foley CN, Zuber V. Inferring Causal Relationships Between Risk Factors and Outcomes from Genome-Wide Association Study Data. Annu Rev Genomics Hum Genet. 2018;19(1):303–327. doi:10.1146/annurev-genom-083117-021731
27. Zhao Q, Wang J, Hemani G, Bowden J, Small DS. Statistical inference in two-sample summary-data Mendelian randomization using robust adjusted profile score. Ann Stat. 2020;48(3):1742–1769. doi:10.1214/19-AOS1866
28. Xiuyun W, Jiating L, Minjun X, Weidong L, Qian W, Lizhen L. Network Mendelian randomization study: exploring the causal pathway from insomnia to type 2 diabetes. BMJ Open Diabetes Res Care. 2022;10(1):e002510. doi:10.1136/bmjdrc-2021-002510
29. Sanderson E, Spiller W, Bowden J. Testing and correcting for weak and pleiotropic instruments in two-sample multivariable Mendelian randomization. Stat Med. 2021;40(25):5434–5452. doi:10.1002/sim.9133
30. Sanderson E. Multivariable Mendelian Randomization and Mediation. Cold Spring Harb Perspect Med. 2021;11(2):a038984. doi:10.1101/cshperspect.a038984
31. Hemani G, Bowden J, Davey Smith G. Evaluating the potential role of pleiotropy in Mendelian randomization studies. Hum Mol Genet. 2018;27(R2):R195–r208. doi:10.1093/hmg/ddy163
32. Staiger D, Stock JH. Instrumental Variables Regression with Weak Instruments. Econometrica. 1997;65(3):557–586. doi:10.2307/2171753
33. Burgess S, Thompson SG, Collaboration CCG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
34. Davies NM, von Hinke Kessler Scholder S, Farbmacher H, Burgess S, Windmeijer F, Smith GD. The many weak instruments problem and Mendelian randomization. Stat Med. 2015;34(3):454–468. doi:10.1002/sim.6358
35. Hemani G, Tilling K, Davey Smith G. Orienting the causal relationship between imprecisely measured traits using GWAS summary data. PLoS Genet. 2017;13(11):e1007081. doi:10.1371/journal.pgen.1007081
36. Bowden J, Spiller W, Del Greco MF, et al. Improving the visualization, interpretation and analysis of two-sample summary data Mendelian randomization via the Radial plot and Radial regression. Int J Epidemiol. 2018;47(4):1264–1278. doi:10.1093/ije/dyy101
37. Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan NA, Thompson JR. Assessing the suitability of summary data for two-sample Mendelian randomization analyses using MR-Egger regression: the role of the I2 statistic. Int J Epidemiol. 2016;45(6):1961–1974. doi:10.1093/ije/dyw220
38. Lawlor DA, Wade K, Borges MC, et al. A Mendelian Randomization Dictionary: Useful Definitions and Descriptions for Undertaking, Understanding and Interpreting Mendelian Randomization Studies. 2019.
39. Wang S, Ojewunmi OO, Kamiza A, et al. Accounting for heterogeneity due to environmental sources in meta-analysis of genome-wide association studies. bioRxiv. 2024;2024:594687.
40. Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted? Stat Med. 2002;21(11):1559–1573. doi:10.1002/sim.1187
41. Dashti HS, Daghlas I, Lane JM, et al. Genetic determinants of daytime napping and effects on cardiometabolic health. Nat Commun. 2021;12(1):900. doi:10.1038/s41467-020-20585-3
42. Zhu Y, Bi Y, Zhu T. Mendelian randomization highlights sleep disturbances mediated the effect of depression on chronic pain. Brain Behav. 2024;14(7):e3596. doi:10.1002/brb3.3596
43. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
44. Birney E. Mendelian randomization. Cold Spring Harb Perspect Med. 2021;a041302. doi:10.1101/cshperspect.a041302
45. Lane JM, Liang J, Vlasac I, et al. Genome-wide association analyses of sleep disturbance traits identify new loci and highlight shared genetics with neuropsychiatric and metabolic traits. Nat Gen. 2017;49(2):274–281. doi:10.1038/ng.3749
46. Zheng J, Baird D, Borges MC, et al. Recent Developments in Mendelian Randomization Studies. Curr Epidemiol Rep. 2017;4(4):330–345. doi:10.1007/s40471-017-0128-6
47. Bycroft C, Freeman C, Petkova D, et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562(7726):203–209. doi:10.1038/s41586-018-0579-z
48. Fry A, Littlejohns TJ, Sudlow C, et al. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am J Epidemiol. 2017;186(9):1026–1034. doi:10.1093/aje/kwx246
49. Brion M-JA, Shakhbazov K, Visscher PM. Calculating statistical power in Mendelian randomization studies. Int J Epidemiol. 2012;42(5):1497–1501. doi:10.1093/ije/dyt179
50. Zuk O, Schaffner SF, Samocha K, et al. Searching for missing heritability: designing rare variant association studies. Proc Natl Acad Sci U S A. 2014;111(4):E455–464. doi:10.1073/pnas.1322563111
51. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG, Consortium E-I. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
52. Freeman G, Cowling BJ, Schooling CM. Power and sample size calculations for Mendelian randomization studies using one genetic instrument. Int J Epidemiol. 2013;42(4):1157–1163. doi:10.1093/ije/dyt110
53. Burgess S. Sample size and power calculations in Mendelian randomization with a single instrumental variable and a binary outcome. Int J Epidemiol. 2014;43(3):922–929. doi:10.1093/ije/dyu005
54. Burgess S, Thompson SG. Use of allele scores as instrumental variables for Mendelian randomization. Int J Epidemiol. 2013;42(4):1134–1144. doi:10.1093/ije/dyt093
55. Pierce BL, Burgess S. Efficient design for Mendelian randomization studies: subsample and 2-sample instrumental variable estimators. Am J Epidemiol. 2013;178(7):1177–1184. doi:10.1093/aje/kwt084
56. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization: the STROBE-MR Statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
57. Munafò MR, Tilling K, Taylor AE, Evans DM, Davey Smith G. Collider scope: when selection bias can substantially influence observed associations. Int J Epidemiol. 2017;47(1):226–235. doi:10.1093/ije/dyx206
58. Dashti HS, Jones SE, Wood AR, et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat Commun. 2019;10(1):1100. doi:10.1038/s41467-019-08917-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.