")
Back to Journals » Infection and Drug Resistance » Volume 18
New Option for Antibiotic Susceptibility Testing in Clinical Practice: Performance Evaluation of AutoMic-i600 Automatic System Based on Broth Microdilution Method
Authors Lin C, Zhang H, Wu Q, Qiu X, Li Q, Wu G
Received 6 October 2024
Accepted for publication 18 January 2025
Published 28 January 2025 Volume 2025:18 Pages 543—556
DOI https://doi.org/10.2147/IDR.S499486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chenyao Lin,1 Hui Zhang,2 Qiaoping Wu,1 Xuedan Qiu,1 Qingcao Li,1 Guangliang Wu3
1Department of Clinical Laboratory, The Affiliated LiHuiLi Hospital of Ningbo University, Ningbo, People’s Republic of China; 2Department of Clinical Laboratory, Ninghai County Chengguan Hospital, Ningbo, People’s Republic of China; 3Department of Clinical Pharmacy, The Affiliated LiHuiLi Hospital of Ningbo University, Ningbo, People’s Republic of China
Correspondence: Qingcao Li, Department of Clinical Laboratory, The Affiliated LiHuiLi Hospital of Ningbo University, 57 Xingning Road, Ningbo, Zhejiang, 315000, People’s Republic of China, Tel +86 139-8931-6035, Email [email protected] Guangliang Wu, Department of Clinical Laboratory, The Affiliated LiHuiLi Hospital of Ningbo University, 57 Xingning Road, Ningbo, Zhejiang, 315000, People’s Republic of China, Tel +86 137-7709-1293, Email [email protected]
Background: The emergence of multidrug-resistant bacteria limits antibiotic efficacy, making accurate antimicrobial susceptibility testing (AST) essential for clinical decisions. Broth microdilution (BMD) is the gold standard but is impractical for routine application. Current automated AST systems improve efficiency but face accuracy or operational challenges, highlighting the need for reliable and user-friendly solutions.
Objective: This study aims to evaluate the performance of a novel automated AST system (AutoMic-i600) based on the BMD method for AST of common clinical bacteria.
Methods: A total of 229 clinical isolates (150 Gram-negative and 79 Gram-positive) were prospectively collected from microbiology laboratory between June 2023 and August 2023. We reported the comparison of the AutoMic-i600 and Vitek 2 systems for routine antibiotics, and also validated the detection performance of AutoMic-i600 for novel antibiotics, based on the BMD method.
Results: The overall essential agreement (EA) and categorical agreement (CA) between AutoMic-i600 and BMD were 93.2% and 93.5% for Gram-negative bacteria and 98.5% and 97.8% for Gram-positive bacteria, respectively. The overall EA and CA between Vitek 2 and BMD were 92.6% and 93.5% for Gram-negative bacteria and 97.9% and 97.4% for Gram-positive bacteria. Importantly, for drug-resistant bacteria, AutoMic-i600 demonstrated a higher overall agreement than Vitek 2 (EA: 98.1% vs 94.8%, CA: 97.5% vs 92.0%), especially in Gram-negative bacteria (EA: 97.7% vs 93.5%, CA: 97.7% vs 89.3%). The VME rate for Gram-negative bacteria using AutoMic-i600 was significantly lower than that of Vitek 2 (1.0% vs 2.9%). Novel antibiotics detected by AutoMic-i600 exhibited EA and CA rates exceeding 90.0%.
Conclusion: Based on these findings, we recommend that the AutoMic-i600 system could be a new option for routine AST testing in a clinical setting. Particularly for drug-resistant bacteria and novel antibiotics, detection with AutoMic-i600 may be more reliable, which could further contribute to the prevention and treatment of drug-resistant bacteria.
Keywords: antibiotic susceptibility testing, drug-resistant bacteria, AutoMic-i600 system, automate
Introduction
The widespread rise of multidrug-resistant and extensively drug-resistant bacteria is increasingly limiting the effectiveness of current drugs and significantly causing treatment failure. Antimicrobial susceptibility testing (AST), as an essential tool, generally plays a highly influential role in guiding treatment.1,2 Therefore, an accurate and reliable susceptibility test is crucial to directing clinical decisions.
Broth microdilution (BMD) is the reference method that can detect the minimum inhibitory concentration (MIC) of antimicrobial drugs accurately and effectively.3 But it is complex, costly, time-consuming, and not appropriate for daily testing in clinical laboratories. The Vitek 2 Compact system is widely used for commercial automated AST and employed in an overwhelming majority of hospitals in China.4,5 However, there is still some controversy about the AST results of Vitek 2, especially regarding the detection of drug-resistant bacteria and potential false-sensitivity.6–12 Similarly, the Phoenix automated system, another commonly used AST platform, has shown high concordance with reference methods for some antibiotics but exhibits reduced accuracy in determining the susceptibility of carbapenem-resistant Enterobacteriaceae (CRE) and methicillin-resistant S. aureus (MRSA) isolates.13,14 And its operation is relatively cumbersome, requiring manual sample pipetting and information entry. In addition, the MicroScan WalkAway system includes a broad range of antibiotics, but the relatively long detection cycle (16–24 hours) may limit its applicability in urgent testing scenarios.15 These findings underscore the importance of the accuracy and convenience in automated AST systems, enabling the rational selection of antimicrobial agents in clinical practice.
AutoMic-i600, a novel automatic microbial identification and susceptibility test system based on BMD, has been used in microbiology laboratories in recent years.16 Clinical breakpoints are completely covered in the detectable range, and four-wavelength detection technology is employed to detect the turbidity and/or colour intensity of microdilution wells. The MIC values are actually detected rather than predicted, which may contribute to the accuracy of the test results. It also supports a fully automatic system of sample pipetting, incubation, and detection, exhibiting a high degree of automation.17 Furthermore, the antibiotics on the single AST plate of AutoMic-i600 are more comprehensive and updated compared to Vitek 2, including the novel antibiotics, which are relatively newly incorporated into the automated AST system or approved and used in China recently with either under-reported or controversial performance, such as ceftazidime/avibactam, oritavancin, and cefoperazone/sulbactam. Currently, there is only one study demonstrating the accuracy of the AutoMic-i600 system in antifungal susceptibility testing.18 Our study is the first to evaluate the performance of the AutoMic-i600 system in bacterial AST.
In this study, we compared the detection performance of the AutoMic-i600 system with that of the Vitek 2 system for routine antibiotics, based on the reference BMD method. And the novel antibiotics, which were newly approved in China and not available in the commonly used test cards of Vitek 2, were detected and comparatively analyzed by the AutoMic-i600 and BMD method. The aim is to assess the performance of the AutoMic-i600 system in detecting antimicrobial susceptibility for both routine and novel antibiotics, including its accuracy, validity, and potential benefits. This may provide a reliable new option for clinical AST, and support timely and effective treatment decisions in the face of increasingly serious antimicrobial resistance.
Materials and Methods
Study Design and Bacterial Isolates
A total of 75 strains of Enterobacteriaceae (33 Klebsiella pneumoniae, 27 Escherichia coli, 15 Enterobacter spp)., 75 strains of non-fermenting bacteria (31 Pseudomonas aeruginosa, 10 Acinetobacter baumannii, 15 Burkholderia cepacia, 19 Stenotrophomonas maltophilia), and 79 strains of Gram-positive cocci (33 Staphylococcus aureus, 15 Coagulase-negative staphylococci, 26 Enterococcus faecalis, 5 Enterococcus faecium) clinical isolates were collected between June 2023 and August 2023 from a tertiary A hospital in China. All isolated clinical strains were identified using a mass spectrometer, the Zybio EXS 2600 system (Zybio Inc., China). The principle and operation method are shown in Supplementary File 1. The specimen sources mainly included respiratory secretions, urine, blood, wounds, tissues, and fluids. Duplicate bacteria from the same patient and site had been excluded. Quality control was ensured by concurrent testing of four quality control strains, including E. coli ATCC 25922, P. aeruginosa ATCC 27853, S. aureus ATCC 29213, and E. faecalis ATCC 29212.
AST by the AutoMic-i600 System
The AST was performed using the AutoMic-i600 system (Autobio Diagnostics CO., Ltd., Zhengzhou, China) with strict adherence to the manufacturer’s instructions (Supplementary File 2). Specifically, the measurement principles of the AutoMic-i600 system are based on the broth microdilution method combined with the redox method for detecting MIC values. The AST Plate is coated with varying concentrations of antimicrobial agents at appropriate well locations. 100 μL of the bacterial suspension (0.5 McFarland) and one drop of the indicator solution (colorimetric oxidation-reduction) are added to 1 vial of broth and mixed well to prepare the inoculum suspension. Then, the suspension and the corresponding AST plate are placed in the instrument. A 100 μL suspension is automatically dispensed into each well, followed by automated incubation of the AST plate. After incubation, four-wavelength detection technology is employed to detect the MICs based on changes in the indicator as well as bacterial turbidity. And all MIC values are actually detected rather than predicted (Figure 1). The corresponding Enterobacteriaceae (EB), non-fermenters (NF) and Gram-positive (GP) AST plates were used for Enterobacteriaceae, non-fermenting bacteria, and Gram-positive cocci, respectively.
 |
Figure 1 The detection method and principle of the AutoMic-i600 system. Clinical breakpoints were completely covered in the 120-well microdilution plate. Colorimetric and turbidimetric methods (four-wavelength) were combined to measured MIC values. Fully automated sample pipetting, incubation, detection and continuous interpretation (every 30 minutes regularly) were supported. |
AST by the Vitek 2 System and the BMD Method
We performed AST with the Vitek 2 system (bioMérieux, Marcy l’Etoile, France) according to the manufacturer’s instructions, using the software version 8.01 and the AST-GN13, AST-N335, and AST-GP67 cards for Enterobacteriaceae, non-fermenting bacteria, and Gram-positive cocci, respectively. The Vitek 2 system employs a solely turbidimetric method (three-wavelength), measuring bacterial growth by detecting 3–4 concentrations of antibiotics and inferring the MICs based on growth kinetics. We performed AST by the BMD method according to the Clinical and Laboratory Standards Institute (CLSI) M100-Ed33 guideline.19
Discrepancy Resolution and Data Analysis
The AutoMic-i600 system and Vitek 2 system AST results were compared with the BMD results. For most antibiotics, the clinical breakpoints were interpreted according to the CLSI M100-Ed33 standards.19 Since CLSI does not provide interpretive criteria for cefoperazone/sulbactam, we adopted the criteria reported in previous studies, which defined the breakpoints as susceptibility (≤16 mg/L), intermediate (32 mg/L), and resistance (≥64 mg/L).20 Moxifloxacin breakpoints for Enterobacteriaceae and colistin breakpoints for non-fermenting bacteria were referenced in European Committee on Antimicrobial Susceptibility Testing (EUCAST) standards.21 And tigecycline breakpoints were interpreted following the Food and Drug Administration (FDA) standards.22 The breakpoint criteria used by AutoMic-i600 are the same as those of Vitek 2 (Supplementary File 3). Essential agreement (EA) and bias were calculated according to the recommendations in the ISO 20776–2:2021 document.23 Congruent expected performances were as follows: EA ≥ 90%, −30% ≤ bias ≤ +30%. Rates of categorical agreement (CA), very major errors (VMEs, false susceptibility), major errors (MEs, false resistance) and minor errors (mEs, intermediate result instead of susceptible or resistant) were also calculated following the definitions from ISO 20776–2:2007.24,25 Expected congruent performances were: CA ≥ 90%, VMEs and MEs rates < 3%, and mE rates < 10%.
Results
Comparison of AST for Common Clinical Isolates
We included a total of 229 isolates (150 Gram-negative and 79 Gram-positive) isolated from clinical specimens, and performed tests against various antibiotics. For Gram-negative bacteria, 33 isolates of K. pneumoniae were tested against 13 antibiotics, 27 isolates of E. coli against 14 antibiotics, and other species against 4–11 antibiotics, resulting in 1544 organism/antimicrobial tests (Table 1). For Gram-positive bacteria, 48 isolates of staphylococci were tested against 15 antibiotics each, and 31 isolates of enterococci against 10 antibiotics each, totaling 1030 organism/antimicrobial tests (Table 2). All tests were performed using the AutoMic-i600 and Vitek 2 systems, with BMD as the reference method.
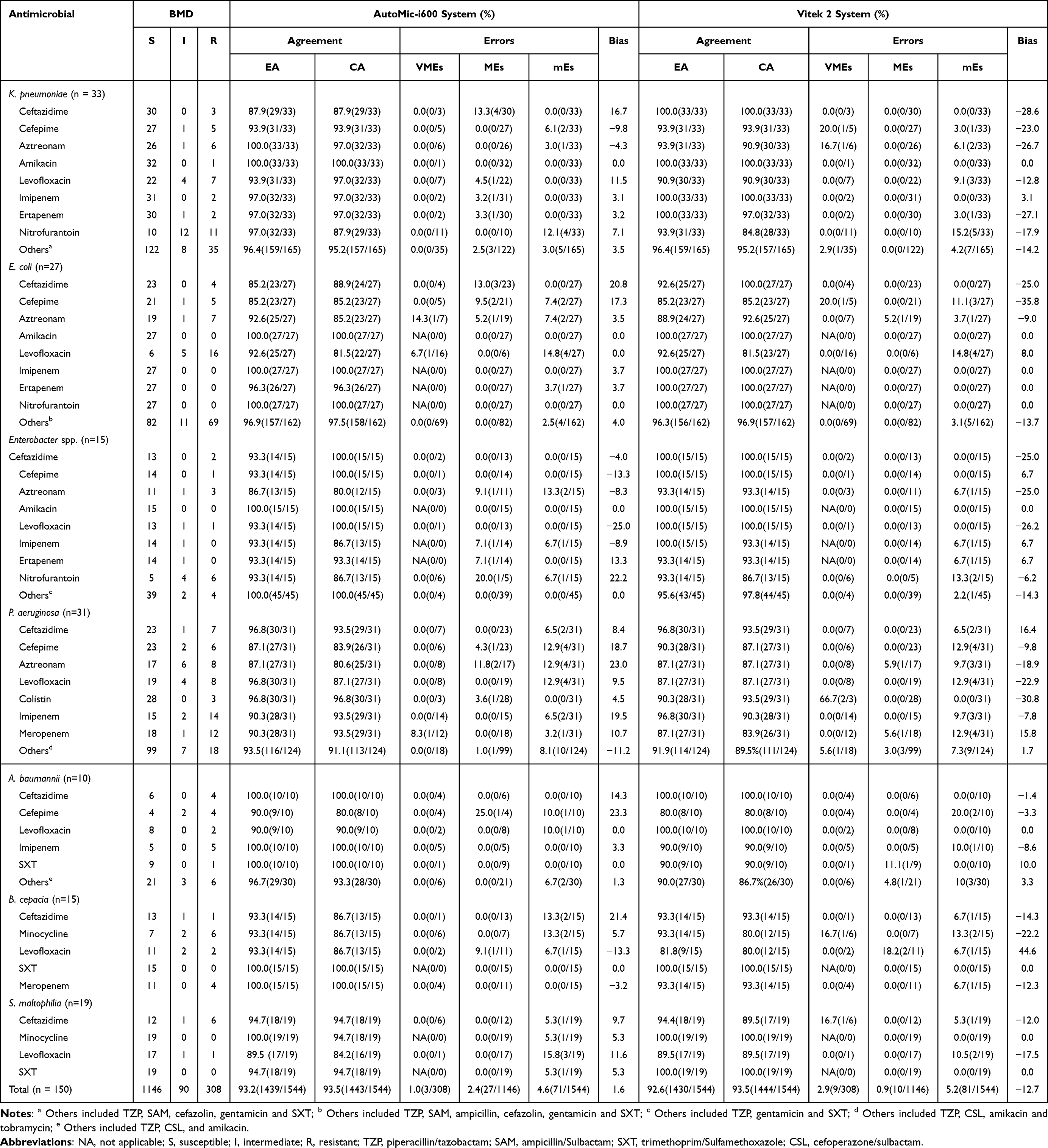 |
Table 1 Performance of the AutoMic-i600 and the Vitek 2 Systems Compared With BMD for Gram-Negative Bacterial Species (n = 150) |
 |
Table 2 Performance of the AutoMic-i600 and the Vitek 2 Systems Compared With BMD for Gram-Positive Bacterial Species (n = 79) |
Among Gram-negative bacteria, the AutoMic-i600 system exhibited 93.2% EA (1439/1544) with a bias of 1.6%, and the Vitek 2 system exhibited 92.6% EA (1430/1544) with a bias of −12.7%. The CA was 93.5% for both AutoMic-i600 (1443/1544) and Vitek 2 (1444/1544) systems (Table 1). In Gram-positive bacteria, the AutoMic-i600 system exhibited 98.5% EA (859/872) with a bias of 1.2%, and the Vitek 2 system exhibited 97.9% EA (854/872) with a bias of −5.3%. The CA was 97.8% (1007/1030) for the AutoMic-i600 system and 97.4% (1003/1030) for the Vitek 2 system (Table 2). The overall rates of VMEs, MEs and mEs were 1.1% (7/612), 1.7% (31/1840) and 3.3% (86/2574) with the AutoMic-i600, and 2.3% (14/612), 0.7% (13/1840) and 3.9% (100/2574) with the Vitek 2 (Tables 1 and 2).
As depicted in Tables 1 and 2, we analyzed the distributions of agreements and errors for each antimicrobial agent concerning Gram-negative and Gram-positive bacteria, respectively. We noted that amikacin showed complete agreement (EA and CA both of 100%) in the two systems for Enterobacteriaceae (n = 75), as well as penicillin for Gram-positive cocci (n = 79). In gram-negative bacteria, both systems yielded high rates of mEs for levofloxacin and nitrofurantoin. Apart from mEs, most errors of the AutoMic-i600 were caused by MEs (2.4%), mainly observed in the detection of ceftazidime (K. pneumoniae, 13.3%; E. coli, 13.0%), cefepime (E. coli, 9.5%), and aztreonam (P. aeruginosa, 11.8%). While as for Vitek 2, the majority of error rates, except mEs, were attributed to a high rate of VMEs (2.9%), mainly observed for polymyxin (P. aeruginosa, 66.7%), cefepime (K. pneumoniae, 20.0%; E. coli, 20.0%), aztreonam (K. pneumoniae, 16.7%), minocycline (B. cepacia, 16.7%), and ceftazidime (S. maltophilia, 16.7%) (Table 1). Among gram-positive bacteria, the inducible clindamycin resistance-related VMEs were predominantly observed when using Vitek 2 (Table 2).
Agreement of AST in Drug-Resistant Bacteria
This study included 166 isolates resistant to one or more antimicrobials. Overall, the AutoMic-i600 AST results demonstrated 98.1% (529/539) essential and 97.5% (597/612) categorical agreement, and the Vitek 2 AST results demonstrated 94.8% (511/539) essential and 92.0% (563/612) categorical agreement (Table 3). When the performance of each system was stratified by type of drug-resistant bacteria, the EA rates of the AutoMic-i600 and Vitek 2 systems were 97.7% (301/308) and 93.5% (288/308) for Gram-negative bacteria, and 98.7% (228/231) and 96.5% (223/231) for Gram-positive bacteria, respectively. And CA rates of the AutoMic-i600 and Vitek 2 systems were 97.7% (301/308) and 89.3% (275/308) for Gram-negative bacteria, and 97.4% (296/304) and 94.7% (288/304) for Gram-positive bacteria, respectively.
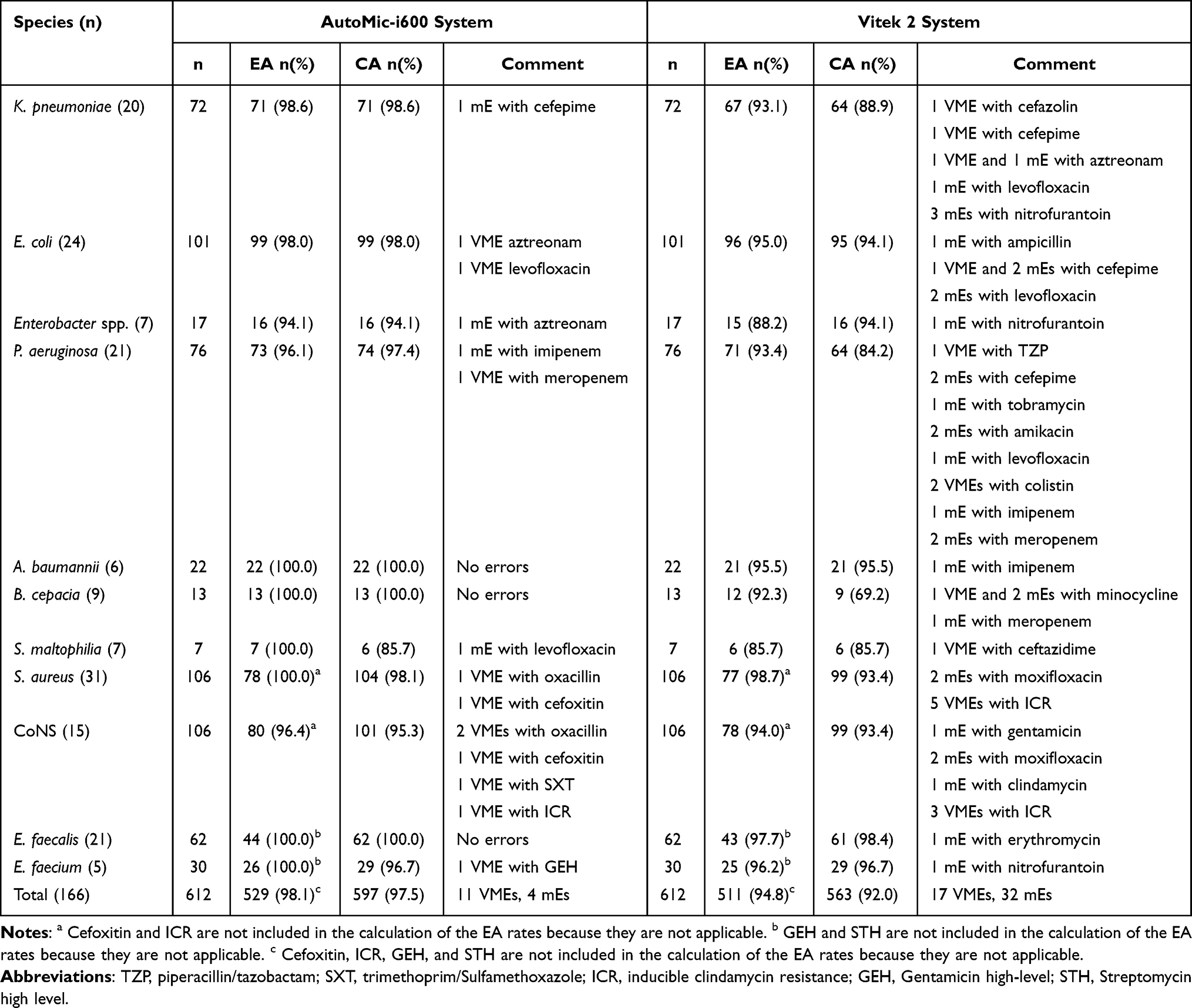 |
Table 3 AutoMic-i600 System and Vitek 2 System AST Results for Isolates Found to Be Resistant to at Least One Antimicrobial Agent by the Reference BMD Method |
Consistency Analysis of AST for Novel Antibiotics
We categorized the antibiotics, which are relatively newly incorporated into the automated AST system or approved and used in China in recent years with either under-reported or controversial performance as novel antibiotics. Using BMD as the reference method, we employed AutoMic-i600 to detect the sensitivity of K. pneumoniae (n = 33) and E. coli (n = 27) to cefoperazone/sulbactam, tigecycline, moxifloxacin, and ceftazidime/avibactam, as well as the sensitivity of staphylococci (n = 48) and enterococci (n = 31) to daptomycin, ceftaroline, and oritavancin.
The rates of EA (ranging from 90.3% to 100.0%), CA (ranging from 92.6% to 100.0%) and bias (ranging from −30.0 to 19.8) were acceptable for all antibiotic-pathogen combinations. Two VMEs (50%) were observed for ceftazidime/avibactam, both in K. pneumoniae isolates. Three MEs were observed for cefoperazone/sulbactam, two in K. pneumoniae isolates (6.7%), and one in an E. coli isolate (4.0%) (Figure 2). Besides, two VMEs were observed in staphylococci, including one for daptomycin in a Staphylococcus haemolyticus isolate (100.0%) and one for oritavancin in a S. aureus isolate (100.0%). And four MEs were noted for oritavancin, two in S. aureus isolates (4.3%) and two in E. faecalis isolates (6.5%) (Figure 3).
 |
Figure 2 MICs of novel antibiotics for K. pneumoniae and E. coli using the AutoMic-i600 system compared with the BMD reference method. (a) Comparison of MICs obtained for cefoperazone/sulbactam-K. pneumoniae combination. (b) Comparison of MICs obtained for tigecycline-K. pneumoniae combination. (c) Comparison of MICs obtained for moxifloxacin-K. pneumoniae combination. (d) Comparison of MICs obtained for ceftazidime/avibactam-K. pneumoniae combination. (e) Comparison of MICs obtained for cefoperazone/sulbactam-E. coli combination. (f) Comparison of MICs obtained for tigecycline-E. coli combination. (g) Comparison of MICs obtained for moxifloxacin-E. coli combination. (h) Comparison of MICs obtained for ceftazidime/avibactam-E. coli combination. MICs corresponding to EA are in grey, VME in Orange and ME in blue. Hatching on the grey boxes within the orange (VME) and blue (ME) boxes corresponds to MICs that are also in the EA. Abbreviations: VME, very major error; mE, minor error. |
 |
Figure 3 MICs of novel antibiotics for staphylococci and enterococci using the AutoMic-i600 system compared with the BMD reference method. (a) Comparison of MICs obtained for daptomycin-staphylococci combination. (b) Comparison of MICs obtained for ceftaroline-staphylococci combination. (c) Comparison of MICs obtained for oritavancin-staphylococci combination. (d) Comparison of MICs obtained for daptomycin-enterococci combination. (e) Comparison of MICs obtained for oritavancin-enterococci combination. MICs corresponding to EA are in grey, VME in Orange and ME in blue. Hatching on the grey boxes within the orange (VME) and blue (ME) boxes corresponds to MICs that are also in the EA. Abbreviations: VME, very major error; mE, minor error. |
Discussion
Antimicrobial resistance in bacteria constitutes a worldwide challenge and poses a significant threat to public health.26 Accurate AST is an effective means of guiding treatment strategies.27 Broth microdilution (BMD) is the gold standard but is impractical for routine application. Current automated AST systems improve efficiency but face accuracy or operational challenges, highlighting the need for reliable and user-friendly solutions. AutoMic-i600 as a novel fully automated system based on the dual-detection of turbidimetry and colorimetry, may be a reliable new option for AST. However, few studies have evaluated the performance of the AutoMic-i600 system for susceptibility test.18
Here, we reported a comparison of the AutoMic-i600 and Vitek 2 systems for routine antibiotics, and also validated the detection performance of AutoMic-i600 for novel antibiotics, based on the reference BMD method. In our study, the AutoMic-i600 system performed reliably with both Gram-negative and Gram-positive bacteria, with EA rates of 93.2% and 98.5% and CA rates of 93.5% and 97.8%, respectively, which was overall equivalent (or slightly superior) to that of Vitek 2 (EA: 92.6% and 97.9%, CA: 93.5% and 97.4%, respectively). Importantly, for drug-resistant bacteria, the overall agreement of AutoMic-i600 was obviously higher than that of Vitek 2 (EA: 98.1% vs 94.8%, CA: 97.5% vs 92.0%), especially for Gram-negative bacteria (EA: 97.7% vs 93.5%, CA: 97.7% vs 89.3%). It is indicated that the AutoMic-i600 system may provide greater reliability for AST of drug-resistance bacteria compared to the Vitek 2 system. These findings align with the reports indicating the limitations of Vitek 2 in accurately testing drug-resistant strains.28 Another commonly used AST platform, Phoenix automated system, also exhibited reduced accuracy in determining the susceptibility of CRE and MRSA isolates.13,14 Therefore, we suggested that the AutoMic-i600 could potentially serve as a reliable and efficient new option for AST of drug-resistant bacteria.
The lower VME rate for Gram-negative bacteria with AutoMic-i600 (1.0% vs 2.9% for Vitek 2) was a notable advantage. Consistent with previous studies, we observed high VME rates with Vitek 2 for colistin in P. aeruginosa ((66.7%, bias = −30.8%) and cefepime in K. pneumoniae (20.0%, bias = −23.0%) and E. coli (20.0%, bias = −35.8%).5–9 For example, recent reports have indicated that colistin testing of Gram-negative bacilli isolates by the Vitek 2 system had high rates of VME.6,29 Jang et al similarly found that high VME rates were observed for cefepime in K. pneumoniae and E. coli with the Vitek 2 system.7 These findings underscore the need to exercise caution when interpreting results from Vitek 2 for these antibiotics. The AutoMic-i600 system, by contrast, indicating its potential to reduce false sensitivity in drug-resistant bacteria.
The superior performance of AutoMic-i600 may be attributed to its dual-detection principle, which combines turbidimetry and colorimetry (four-wavelength), enabling it to detect smaller changes in bacterial growth compared to Vitek 2, which relies solely on turbidimetry (three-wavelength).17 Furthermore, the AutoMic-i600 system covers the clinical breakpoints completely and provides directly measured MIC values, whereas the Vitek 2 system calculates the bacterial growth status by detecting 3–4 antibiotic concentrations and extrapolates the MICs based on growth kinetics, which may lead to potential calculation errors. However, the rate of ME in Gram-negative bacteria detected by AutoMic-i600 was higher than that by Vitek 2 (2.4% vs 0.9%). These false-resistant results were mainly observed for K. pneumoniae, E. coli and P. aeruginosa. We traced back these false-resistant strains and found that most were mucoid strains. The potential reason could be the insufficient grinding, resulting in the presence of tiny bacteria clumps, which might be amplified by the sensitive detection technology of AutoMic-i600. Additionally, the rates of VMEs and MEs were equivalent between the AutoMic-i600 and Vitek 2 systems in Gram-positive bacteria, which was similar to the previous study.11
In the context of the automated AST system, the antibiotics relatively newly incorporated into the automated AST system or approved and used in China in recent years with either under-reported or controversial performance were regarded as novel antibiotics. Specifically, ceftazidime/avibactam and oritavancin are tested for the first time in an automated AST system (ie, AutoMic-i600). Additionally, daptomycin and ceftaroline are less commonly applied in automated AST systems, and neither is included in the routine AST cards of the Vitek 2 system. Furthermore, cefoperazone/sulbactam, tigecycline, and moxifloxacin are approved and used in China for a relatively short period of time, and their performance in other automated AST systems is either under-reported or controversial.30–32
The inclusion of novel antibiotics brings critical new advancements to the treatment of multidrug-resistant bacteria.33 Cefoperazone/sulbactam, tigecycline, moxifloxacin, and ceftazidime/avibactam are considered effective for treating CRE and ESBL-producing Enterobacteriaceae.28,30,34,35 And daptomycin, ceftaroline, and oritavancin are reported as therapeutic options for MRSA and vancomycin-resistant enterococci (VRE).36–38 These novel antibiotics, along with routine antibiotics, are simultaneously used for usual AST with AutoMic-i600. Compared to Vitek 2, which requires the combination of multiple AST cards, AutoMic-i600 offers a more convenient way to detect drug-resistant bacteria. In our research, the AST results of novel antibiotics by AutoMic-i600 showed high agreement with BMD (EA > 90.3%, CA > 92.6%), which could provide reliable evidence for clinical treatment decisions.
As reported previously, cefoperazone/sulbactam had high rates of error in E. coli by Vitek 2 (VME 40%, ME 8.5%).30 The AutoMic-i600 system yielded no VMEs and only three MEs (K. pneumoniae 6.7%, E. coli 4.0%) for cefoperazone/sulbactam, which were much lower than those of Vitek 2. An early study has demonstrated a high rate of false non-susceptible Vitek 2 tigecycline categorization for Enterobacteriaceae and recommended the BMD method to verify such Vitek 2 results.31 According to our research, no VMEs or MEs were noted for the tigecycline-K. pneumoniae and tigecycline-E. coli combinations. Besides, there was limited reporting on the detection performance of moxifloxacin susceptibility testing methods in Enterobacteriaceae. We found that moxifloxacin showed complete agreement between the AutoMic-i600 and BMD methods (100% EA and CA). It can be seen that the AutoMic-i600 system could serve as an effective alternative for the detection of cefoperazone/sulbactam, tigecycline, and moxifloxacin. In addition, two VMEs were noted for ceftazidime/avibactam in K. pneumoniae, which does not exclude the possibility of accidental error caused by the uneven distribution of certain mucoid strains.
It has been confirmed that the Vitek 2, disc diffusion, and MicroScan prompt inoculation methods are not reliable for daptomycin in enterococci, leaving laboratories with few options for testing this agent.32 In our analysis, the AutoMic-i600 system exhibited complete agreement for daptomycin in enterococci with the BMD method (100% EA and CA). Currently, few studies have reported the detection performance of different susceptibility tests for ceftaroline in staphylococci. We found that AutoMic-i600 showed high agreement (97.9% EA and CA), and no VME or ME were observed for ceftaroline. Consequently, the AutoMic-i600 system could be considered a reliable alternative method for AST of daptomycin and cephalothin, which may perhaps make up for the shortcomings and limitations of existing AST methods. Nevertheless, one VME (S. aureus) and four MEs (2 of S. aureus and 2 of E. faecalis) occurred in the test with oritavancin. Although oritavancin is covered for the first time by the automated AST system, further refinement and optimisation of its detection performance are still necessary.
Potential shortcomings of this study include the possibility of accidental errors caused by insufficient grinding of mucoid strain. Also, the numbers of certain strains were limited, such as E. faecium and A. baumannii strains; further research is needed to increase the sample size and strengthen the conclusions that can be drawn.
In conclusion, the AutoMic-i600 system provides a reliable and convenient option for AST in clinical practice, particularly for drug-resistant bacteria and novel antibiotics. Its ability to achieve high agreement with BMD and reduce false sensitivity in drug-resistant Gram-negative bacteria highlights its potential to assist clinicians in making timely and accurate treatment decisions, thereby addressing the growing challenge of antimicrobial resistance.
Data Sharing Statement
Data will be made available by the author Chenyao Lin upon reasonable request.
Ethics Statement
The ethics committee of the Affiliated LiHuiLi Hospital of Ningbo University approved this study (approval number KY2023SL347-01) and waived the requirement for informed consent. This study used residual samples from the prior relevant study, which had already obtained informed consent from participants. The prior informed consent form explicitly informed participants that any remaining samples could be used for subsequent clinical research. Furthermore, all patient data and samples have been handled with strict confidentiality, in accordance with the ethical standards set forth in the Declaration of Helsinki. All data were anonymized and securely stored to ensure privacy and protect the identities of the participants.
Acknowledgments
We thank Autobio Diagnostics CO., Ltd., Zhengzhou, China, for providing the AutoMic-i600 system modules and test reagents. Autobio Diagnostics CO., Ltd. had no role in study design, data collection or interpretation of the results. We thank the Autobio Diagnostics team of diagnostic technicians for their expert technical assistance and the discrepancy analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Medical and Health Research Project of Zhejiang Province (Grant No. 2024KY288), the Traditional Chinese Medicine Research Project of Zhejiang Province (Grant No. 2024ZL940), and the Ningbo Medical Science and Technology Project (Grant No. 2022Y03).
Disclosure
The authors declare no competing interests.
References
1. Pierce VM, Bhowmick T, Simner PJ. Guiding antimicrobial stewardship through thoughtful antimicrobial susceptibility testing and reporting strategies: an updated approach in 2023. J Clin Microbiol. 2023;61(11):e0007422. doi:10.1128/jcm.00074-22
2. Larsson DGJ, Flach CF. Antibiotic resistance in the environment. Nat Rev Microbiol. 2022;20(5):257–269. doi:10.1038/s41579-021-00649-x
3. Jayol A, Nordmann P, Andre C, Poirel L, Dubois V. Evaluation of three broth microdilution systems to determine colistin susceptibility of Gram-negative bacilli. J Antimicrob Chemother. 2018;73(5):1272–1278. doi:10.1093/jac/dky012
4. Zhou M, Wang Y, Liu C, et al. Comparison of five commonly used automated susceptibility testing methods for accuracy in the China Antimicrobial Resistance Surveillance System (CARSS) hospitals. Infect Drug Resist. 2018;11:1347–1358. doi:10.2147/IDR.S166790
5. Khan A, Arias CA, Abbott A, Dien Bard J, Bhatti MM, Humphries RM. Evaluation of the Vitek 2, Phoenix, and MicroScan for antimicrobial susceptibility testing of stenotrophomonas maltophilia. J Clin Microbiol. 2021;59(9):e0065421. doi:10.1128/JCM.00654-21
6. De Angelis G, Posteraro B, Menchinelli G, Liotti FM, Spanu T, Sanguinetti M. Antimicrobial susceptibility testing of pathogens isolated from blood culture: a performance comparison of accelerate pheno and VITEK(R) 2 systems with the broth microdilution method. J Antimicrob Chemother. 2019;74(Suppl 1):i24–i31. doi:10.1093/jac/dky532
7. Jang W, Park YJ, Park KG, Yu J. Evaluation of MicroScan WalkAway and Vitek 2 for determination of the susceptibility of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae isolates to cefepime, cefotaxime and ceftazidime. J Antimicrob Chemother. 2013;68(10):2282–2285. doi:10.1093/jac/dkt172
8. Sader HS, Fritsche TR, Jones RN. Accuracy of three automated systems (MicroScan WalkAway, VITEK, and VITEK 2) for susceptibility testing of pseudomonas aeruginosa against five broad-spectrum beta-lactam agents. J Clin Microbiol. 2006;44(3):1101–1104. doi:10.1128/JCM.44.3.1101-1104.2006
9. Mazzariol A, Aldegheri M, Ligozzi M, Lo Cascio G, Koncan R, Fontana R. Performance of Vitek 2 in antimicrobial susceptibility testing of pseudomonas aeruginosa isolates with different mechanisms of beta-lactam resistance. J Clin Microbiol. 2008;46(6):2095–2098. doi:10.1128/JCM.02216-07
10. Fadana V, Thomas T, von Knorring N. Retrospective analysis of Vitek((R))2 performance compared to manual broth micro-dilution for colistin susceptibility testing of Acinetobacter baumanniicomplex isolates in South Africa. Afr J Lab Med. 2022;11(1):1597. doi:10.4102/ajlm.v11i1.1597
11. Huh HJ, Song DJ, Shim HJ, et al. Performance evaluation of the QMAC-dRAST for staphylococci and enterococci isolated from blood culture: a comparative study of performance with the VITEK-2 system. J Antimicrob Chemother. 2018;73(5):1267–1271. doi:10.1093/jac/dky015
12. Nana T, Perovic O, Chibabhai V. Comparison of carbapenem minimum inhibitory concentrations of Oxacillin-48-like Klebsiella pneumoniae by Sensititre, Vitek 2, MicroScan, and Etest. Clin Microbiol Infect. 2022;28(12):1650e1651–1650e1655. doi:10.1016/j.cmi.2022.06.023
13. Haffler ZJ, Kulengowski B, Ribes JA, Burgess DS. Evaluation of the BD phoenix automated system for determining antimicrobial susceptibility against carbapenem-resistant Enterobacteriaceae compared with broth microdilution. Int J Antimicrob Agents. 2019;54(2):249–254. doi:10.1016/j.ijantimicag.2019.05.002
14. Al-Rawahi GN, Chorlton S, Dhaliwal S, Golding GR, Tilley P. Performance of the BD phoenix automated microbiology system for trimethoprim-sulfamethoxazole susceptibility testing of staphylococcus aureus. J Clin Microbiol. 2019;58(1). doi:10.1128/JCM.00994-19
15. Jacobs MR, Good CE, Abdelhamed AM, Bonomo RA. Accuracy of direct antimicrobial susceptibility testing of gram-negative bacteria from positive blood cultures using microscan system and value of using expert rules for beta-lactam agents. Antimicrob Agents Chemother. 2022;66(3):e0214821. doi:10.1128/aac.02148-21
16. AutoMic-i600. Available from: https://en.autobio.com.cn/Product/productDetail/fid/63/cid/2/id/151.html.
17. Zheng YXZ, Yu F. Inventor. automated microbiology system for identification and antimicrobial susceptibility testing: china, 209722106. 2019.
18. Shen T, Liu P, Chen D, et al. Novel automated antifungal susceptibility testing system for yeasts based on dual-detection algorithm of turbidimetry and colorimetry. J Med Microbiol. 2024;73(3). doi:10.1099/jmm.0.001811
19. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing M100-Ed33. CLSI, Wayne, PA, USA, 2023.
20. Lin SY, Lu PL, Wu TS, et al. Correlation between cefoperazone/sulbactam MIC values and clinical outcomes of Escherichia coli bacteremia. Infect Dis Ther. 2022;11(5):1853–1867. doi:10.1007/s40121-022-00672-2
21. European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of mics and zone diameters, version 13.1. Available from: https://www.eucast.org/ast_of_bacteria/previous_versions_of_documents.
22. US Food and Drug Administration (FDA). Antibacterial susceptibility test Interpretive criteria. Available from: https://www.fda.gov/drugs/development-resources/antibacterial-susceptibility-test-interpretive-criteria.
23. ISO 20776-2. Clinical laboratory testing and in vitro diagnostic test systems - Susceptibility testing of infectious agents and evaluation of performance of antimicrobial susceptibility test devices - Part 2: evaluation of performance of antimicrobial susceptibility test devices against reference broth micro-dilution. 2021. ITEH Standards. Available from: https://standards.iteh.ai/catalog/standards/cen/92fc193a-5135-4d74-b3b5-a6962a16e505/en-iso-20776-2-2022.
24. ISO 20776-2. Clinical laboratory testing and in vitro diagnostic test systems - Susceptibility testing of infectious agents and evaluation of performance of antimicrobial susceptibility test devices - Part 2: evaluation of performance of antimicrobial susceptibility test devices. 2007. ITEH Standards. Available from: https://standards.iteh.ai/catalog/standards/cen/e58114a5-4af0-488d-addf-f410a8445ee0/en-iso-20776-2-2007.
25. ISO 20776-1. Susceptibility testing of infectious agents and evaluation of performance of antimicrobial susceptibility test devices. Part 1: broth micro-dilution reference method for testing the in vitro activity of antimicrobial agents against rapidly growing aerobic bacteria involved in infectious diseases. 2019. ITEH Standards. Available from: https://standards.iteh.ai/catalog/standards/cen/e697de2b-10a8-449a-813b-23f9da71c30c/en-iso-20776-1-2020.
26. Qiao M, Ying GG, Singer AC, Zhu YG. Review of antibiotic resistance in China and its environment. Environ Int. 2018;110:160–172. doi:10.1016/j.envint.2017.10.016
27. Burnham CD, Leeds J, Nordmann P, O’Grady J, Patel J. Diagnosing antimicrobial resistance. Nat Rev Microbiol. 2017;15(11):697–703. doi:10.1038/nrmicro.2017.103
28. Yin D, Guo Y, Li M, et al. Performance of VITEK 2, E-test, Kirby-Bauer disk diffusion, and modified Kirby-Bauer disk diffusion compared to reference broth microdilution for testing tigecycline susceptibility of carbapenem-resistant K. pneumoniae and A. baumannii in a multicenter study in China. Eur J Clin Microbiol Infect Dis. 2021;40(6):1149–1154. doi:10.1007/s10096-020-04123-z
29. Chew KL, La MV, Lin RTP, Teo JWP. Colistin and polymyxin B susceptibility testing for carbapenem-resistant and mcr-positive Enterobacteriaceae: comparison of Sensititre, MicroScan, Vitek 2, and Etest with broth microdilution. J Clin Microbiol. 2017;55(9):2609–2616. doi:10.1128/JCM.00268-17
30. Jean SS, Liao CH, Sheng WH, Lee WS, Hsueh PR. Comparison of commonly used antimicrobial susceptibility testing methods for evaluating susceptibilities of clinical isolates of Enterobacteriaceae and nonfermentative Gram-negative bacilli to cefoperazone-sulbactam. J Microbiol Immunol Infect. 2017;50(4):454–463. doi:10.1016/j.jmii.2015.08.024
31. Idelevich EA, Busing M, Mischnik A, Kaase M, Bekeredjian-Ding I, Becker K. False non-susceptible results of tigecycline susceptibility testing against Enterobacteriaceae by an automated system: a multicentre study. J Med Microbiol. 2016;65(8):877–881. doi:10.1099/jmm.0.000281
32. Bobenchik AM, Hindler JA, Giltner CL, Saeki S, Humphries RM. Performance of Vitek 2 for antimicrobial susceptibility testing of Staphylococcus spp. and Enterococcus spp. J Clin Microbiol. 2014;52(2):392–397. doi:10.1128/JCM.02432-13
33. Chang RYK, Nang SC, Chan HK, Li J. Novel antimicrobial agents for combating antibiotic-resistant bacteria. Adv Drug Deliv Rev. 2022;187:114378. doi:10.1016/j.addr.2022.114378
34. Haque MA, Hossain MT, Islam MS, et al. Isolation of multidrug-resistant Escherichia coli and salmonella spp. from sulfonamide-treated diarrheic calves. Vet World. 2022;15(12):2870–2876. doi:10.14202/vetworld.2022.2870-2876
35. Shirley M. Ceftazidime-avibactam: a review in the treatment of serious gram-negative bacterial infections. Drugs. 2018;78(6):675–692. doi:10.1007/s40265-018-0902-x
36. Bender JK, Cattoir V, Hegstad K, et al. Update on prevalence and mechanisms of resistance to linezolid, tigecycline and daptomycin in enterococci in Europe: towards a common nomenclature. Drug Resist Updat. 2018;40:25–39. doi:10.1016/j.drup.2018.10.002
37. Roy A, Poddar N, Panigrahi K, et al. Evaluation of in-vitro activity of ceftaroline against methicillin-resistant staphylococcus aureus clinical isolates. Cureus. 2023;15(12):e49859. doi:10.7759/cureus.49859
38. Saravolatz LD, Stein GE. Oritavancin: a Long-Half-Life Lipoglycopeptide. Clin Infect Dis. 2015;61(4):627–632. doi:10.1093/cid/civ311
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.