")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Nudging Health Behavior Change Among Home-Based Cardiac Rehabilitation Patients: A Scoping Review
Authors Yang Z , Jin D, Huang H , Zheng X , Liu S, Wang A
Received 3 January 2025
Accepted for publication 8 March 2025
Published 19 March 2025 Volume 2025:18 Pages 1639—1653
DOI https://doi.org/10.2147/JMDH.S515523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Charles V Pollack
Zhen Yang,1,* Dan Jin,2,* Hao Huang,3 Xutong Zheng,1 Shu Liu,1 Aiping Wang1
1Department of Public Service, the First Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China; 2Department of Nursing, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3School of Nursing, the Hong Kong Polytechnic University, Hong Kong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Aiping Wang, Department of Public Service, the First Affiliated Hospital of China, Medical University, No.155, Nanjing North Street, Heping District, Shenyang, Liaoning Province, People’s Republic of China, Email [email protected]
Background: In home-based cardiac rehabilitation practices, nudging has emerged and was actively explored to promote health behavior change among patients with heart disease. The literature on nudging strategy is fragmented and lacks comprehensive reviews.
Objective: This study aimed to identify nudging interventions to promote health behavior change among patients undergoing home-based cardiac rehabilitation, focusing on the scope, characteristics and delivery.
Methods: A scoping review was conducted from July to September 2023, during which databases including PubMed, Web of Science, and OVID (Embase, Cochrane Library, JBI) were searched. Search terms were constructed based on population-concept-context mnemonics approach. Reviewers screened articles independently and reviewed the included articles to extract key information about each nudge intervention.
Results: In included 25 studies, the majority (n=21) with the nudging strategy had positive results. 14 nudge strategies were identified and coded with the primary objective of changing health behaviors. The most common nudging strategy was goal setting, followed by feedback, and reminders and alerts. To capture the heterogeneity of nudging strategies, two independent dimensions were introduced to further classify them into four quadrants (active vs passive and synchronous vs passive). For example, some nudging strategies usually occur when the target behavior must be performed (synchronization) and requires the immediate participation of the home-based cardiac rehabilitation patients (active). In addition, digital nudging technology with gamification elements may become the mainstream in future research.
Conclusion: These studies reflected different objectives and implement nudging strategies in different ways. Despite the multiple nudging strategies are widely adopted, identifying the contributing components remains challenging.
Keywords: nudge, cardiac rehabilitation, decision architecture, health behavior, intervention
Introduction
Cardiac rehabilitation (CR) represents a multifaceted regimen aimed at ensuring the optimal physical, mental, and social functions of individuals suffering from heart diseases.1 The objective is for patients to regain their societal roles to the greatest extent possible through personal effort, thereby leading active and productive lives.1 As a Level 1A recommendation by clinical guidelines,2,3 CR is an essential component in the standardized care of those with cardiovascular conditions, offering marked improvements in clinical outcomes and quality of life. Nevertheless, the persistent nature of heart diseases, combined with logistical challenges such as transportation barriers, means that institution-based CR may be financially taxing and time-consuming for patients.4 As a solution, home-based cardiac rehabilitation (HBCR) provides a cost-effective and accessible alternative model that brings similar improvements in reducting cardiovascular risk, promoting mental and spiritual well-being, enhancing cardiac function and prognosis, and improving the quality of life for patients.5–9
However, these benefits depend on the patient’s long-term and regular HBCR practice. Unfortunately, this remains suboptimal on a global scale.10,11 Only a minority of patients with heart disease rigorously maintain exercise-based HBCR practices after institutional rehabilitation.12 Due to limited exercise endurance and knowledge, patients have poor self-efficacy and exercise motivation towards HBCR practices.13,14 Despite rigorous interventions, long-term and regular adherence to HBCR practices is relatively challenging,15,16 thereby potentially elevating cardiovascular risks and adversely impacting quality of life and clinical prognoses. In light of these considerations, it becomes imperative to develop and implement cost-effective intervention strategies designed to enhance health behaviors during HBCR, thereby improving clinical outcomes and quality of life.17
Increasingly, insights from behavioral economics are being applied to address this resistance and promote health behavior change.18,19 It explains the mechanisms underpinning individual judgment and decision-making in innovative ways.20 Nudging is defined as any element of the choice architecture that consistently influences individual behavior without restricting choices or significantly changing economic incentives.21 This means that limitations on choice, such as bans or information withholding, as well as modifications to incentive structures such as financial rewards or taxes, do not qualify as nudging.22,23 Nudging, as a novel complementary strategy, has been widely adopted to promote individual health behaviors. Examples of its application include sending text-based reminders to encourage vaccination and self-management of chronic diseases in patients,24,25 facilitating physician-patient discussions about serious illnesses through reminders and alerts,26 and promoting hand hygiene among healthcare professionals through goal setting and feedback.27
The term “nudge” later gave birth to the concept of nudge theory, which emphasizes understanding the complexity of behavior and rejects the assumption that individuals will inherently make the best choice when provided with the right information.28 Nudge theory, rooted in the dual-system theory,29 proposes two modes of thought (System 1 and System 2).30 In System 1, thoughts, associations, feelings, and actions occur effortlessly and rapidly, while System 2 involves slow, laborious, and deliberate thinking.30 This dual-system theory forms the basis of nudging as it elucidates our unconscious decision-making processes and presents us with the option to either consciously analyze our behavior (System 2) or alter the environment to guide us toward better choices without conscious effort (System 1).30 Nudge theory introduces fresh perspectives on individual behavior and provides new methodologies for nudging individuals toward making improved decisions.
In cardiovascular healthcare, especially in HBCR practices, nudging strategies have emerged and are actively investigated to promote health behavior change in patients.31–33 In many studies, HBCR practices for patients with heart disease benefited from a series of nudge strategies. However, the research and development of nudging strategies to promote HBCR practices is fragmented, and it is difficult to provide meta-knowledge to guide the selection of the most effective approaches or to comprehensively identify the characteristics, expected outcomes, and weaknesses of each strategy. Therefore, this study, using a systematic scoping review approach, aimed to identify studies of nudging strategies used to promote HBCR practices and to comprehensively understand how to construct measures based on the appropriateness or effectiveness of each strategy according to its purpose. Specifically, our research reviewed the trends in publications on nudging strategies for HBCR practices and evaluated literature related to HBCR and individual nudging strategies, analyzing their distinct characteristics and considerations. Additionally, we delved into the prospects of utilizing digital nudge strategies to enhance the advancement of HBCR practices.
Methods
Based on the methodological framework of the Joanna Briggs Institute (JBI)34 and the Preferred Reporting Items for Systematic Review and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR),35 this scoping review focused on mapping the current knowledge landscape and identifying gaps in supporting HBCR practices and defines key concepts. A scoping review is a widely embraced research method tailored for areas of study that have not been thoroughly explored previously. This pioneering scoping review concentrates on strategies for enhancing HBCR practices, offering vital insights and recommendations to steer future research in this domain.
Research Questions
The aim of this study was to use nudge theory to identify interventions to promote health behavior change among patients undergoing HBCR, focusing on nudge strategies, delivery systems, and empirical evidence. To address these knowledge gaps, this study sought to answer three questions: (1) What is the scope of nudging strategies in the existing literature to promote health behavior in patients with HBCR. (2) How nudging strategies to promote health behavior change in patients are delivered in the HBCR settings. (3) Whether these nudging strategies to promote health behavior change in HBCR patients provide sufficient empirical evidence of success.
Inclusion Criteria
The inclusion criteria of this study were developed based on the population-concept-context criteria recommended by the Joanna Briggs Institute for scoping reviews.34 (1) Population: patients aged ≥18 years with heart disease. (2) Concept: Interventions using any nudge strategy to promote health behavior change. There is no requirement that the interventions necessarily be labeled as a choice architecture or nudging, but it needs to meet the definitions of nudging.21 (3) Context: The patient is in a home-based, supervised or unsupervised cardiac rehabilitation environment. (4) Type of evidence: Empirical studies published in English within international peer-reviewed journals. Only randomized controlled trials, quasi-randomized controlled trial, and longitudinal (before and after) studies were considered. Additionally, if a preprint version is retrieved, the original research associated with the preprint will be retroactively incorporated. Studies were excluded if they were duplicates, lacked full-text access, or were conference abstracts.
Information Sources and Search Strategy
An iterative approach was adopted to develop the search strategy in collaboration with a librarian. Another librarian was invited to review the search strategy using the Peer Review of Electronic Search Strategies (PRESS) checklist.36 Firstly, a preliminary search was conducted on the librarian-recommended database (PubMed), and the results were briefly analyzed to assess the effectiveness of the search strategy. Subsequently, the first author (Y.Z.) conducted searches across three librarian-recommended databases - PubMed, Web of Science, and OVID (Embase, Cochrane Library, JBI) - to identify relevant topics in the title and abstract fields. The search strategies employed across all databases are presented in Additional file 1 of this scope review.
Screening and Selection Process
The search and selection process was conducted by the first author (Y.Z)., with consultation from the second author (Z.X.) throughout the review. Firstly, all the search results in the database were imported into the literature management software, NoteExpress (http://www.inoteexpress.com/), and the duplicate search results were automatically identified and deleted. In addition, all remaining results were screened by the first author (Y.Z.) by title and abstract according to pre-determined inclusion criteria, in consultation with the second author (Z.X). The search results identified as “probable” were discussed between the two authors. In case of disagreement, the third and fourth authors (H.H. and L.S.) were invited to discuss until consensus was reached. Finally, the preliminarily selected literature was reviewed by reviewing the full text to determine the final studies to be included. In this process, in order to ensure the consistency among reviewers, we randomly selected 25 search results, and the reviewers screened them according to the established criteria. When the consistency reached 75%, the formal literature screening began.
Data Coding and Charting
A data extraction table was collaboratively developed by two authors (Y.Z. and Z.X.) to determine the variables for extraction. Each author created a data chart, discussed the results, and iteratively updated the data chart format. In cases of disagreement during the production of the data chart, the third and fourth authors (H.H. and L.S.) were invited to discuss and decide on the final content. We used Microsoft Excel to construct evidence summary tables covering the following data elements: title, author, years, objective, design, study population, nudge strategy, nudge medium, and statistically positive results. An identified challenge in considering the System 1 and System 2 categories is their failure to capture whether the intervention is present at the time of the decision. To address this limitation, based on the classification method proposed by Sant’Anna et al37 and Wolf et al,38 we drew two independent dimensions and four quadrants for more accurate classification as defined by System 1 and System 2 (Figure 1). Synchronous vs Asynchronous: An intervention strategy is synchronous if its delivery is consistent with the decision or behavior it is intended to influence, while an asynchronous strategy can be executed at any time. Active vs Passive: An active strategy cannot be completed without the action of the target patient, while a passive strategy requires no action. These four quadrants are practical in describing how and when HBCR patients receive nudge interventions.
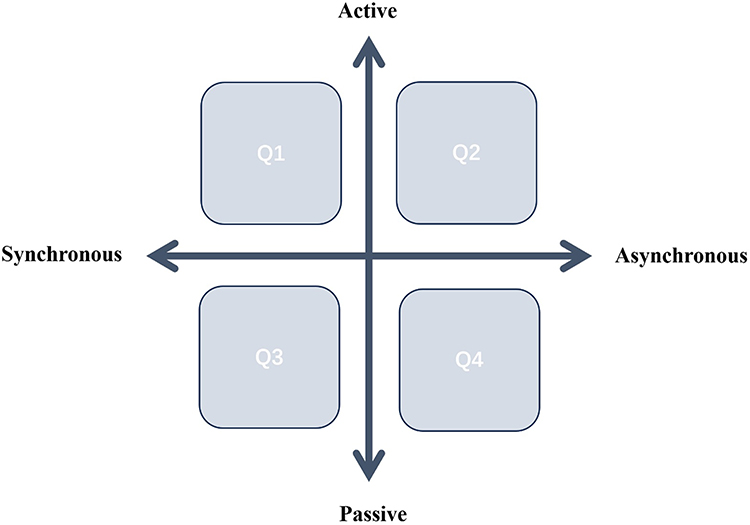 |
Figure 1 A two-dimensional view of nudging. Notes: Reproduced from Sant’Anna A, Vilhelmsson A, Wolf A. Nudging healthcare professionals in clinical settings: a scoping review of the literature. BMC Health Serv Res. 2021;21(1):543.37 |
Results
Article Selection
A total of 5975 studies were generated by this search strategy, and 4926 studies were screened after 1049 studies were eliminated. Based on inclusion criteria, 4670 studies were excluded by two authors at the title and abstract level. Of the remaining 256 studies, 231 studies were subsequently excluded after the authors read the full text, and 25 studies with a total of 8746 patients were retained, covering 3 drafts.39–41 (Figure 2). We went back and included the original research related to the three drafts.42–44
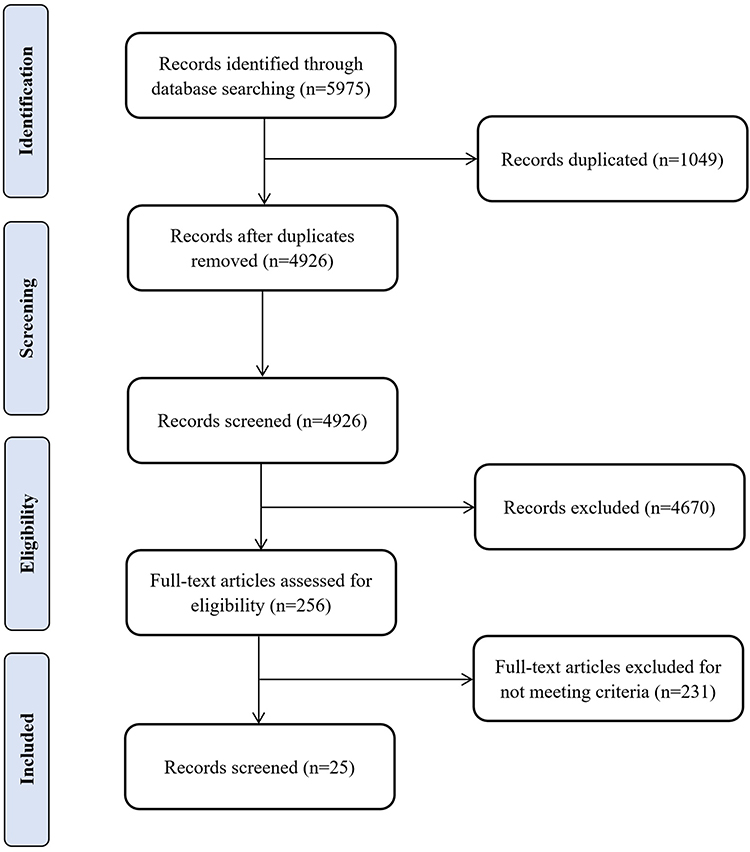 |
Figure 2 PRISMA flow diagram. |
Summary of Included Studies
Figure 3 shows the trends and regional distribution of publications across time for the 25 included studies. In this study, the years of the included studies range from 2009 to 2023, with the highest number of publications in 2022 (n=6). Some of the included studies (n=5) were conducted in the United States,45–49 and one study spanned across three countries, covering Spain, Netherlands, and China.50 Of the 25 studies, the majority employed randomized controls, including 23 randomised controlled clinical trials42–64 and one randomised controlled pilot study.65 Additionally, one study was classified as a quasi-experimental study.66 See Table 1 for details.
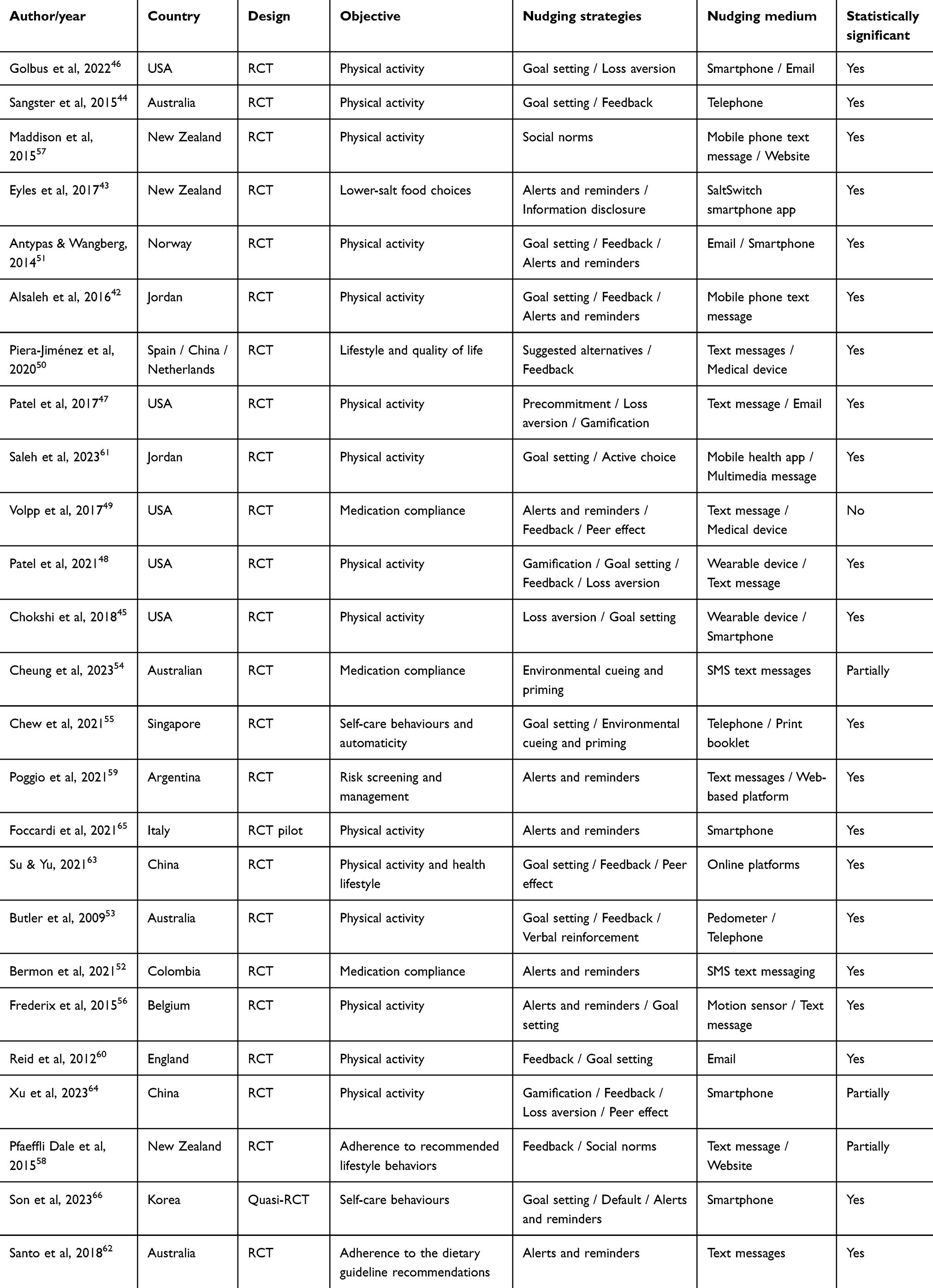 |
Table 1 Characteristics of the Articles Included in the Review |
 |
Figure 3 Intervention strategies over time, 2009–2023. |
Nudging Strategies and Objectives
In total, 55 instances of nudging were incorporated in the 25 studies, as the majority of studies (n=19) involved two or more nudgings.42–51,53,55,56,58,60,61,63,64,66 As shown in Table 2, we identified and coded 14 nudging strategies. Prominent strategies for nudging health behaviors encompassed goal setting, feedback, as well as alerts and reminders. Among the studies employing nudging strategies, the majority (n=21) reported positive results, while three studies yielded partially positive results54,58,64 and one study noted no positive results.49
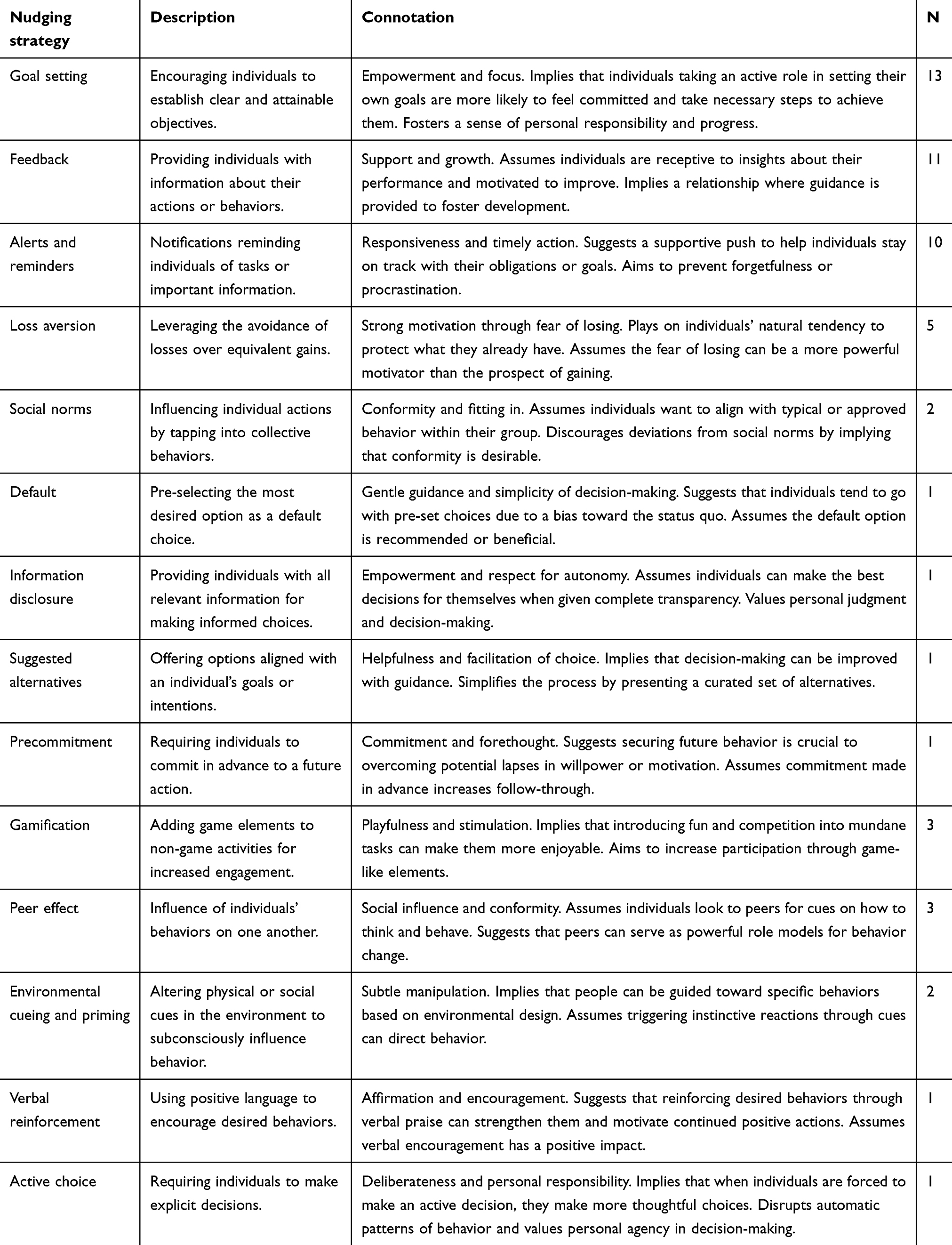 |
Table 2 Description of Nudging Strategies |
Out of the 25 studies, seven employed a nudging strategy with System 1,52,54,55,57,59,62,65 whereas five used a nudging strategy with System 2.44,50,60,61,63 System 1 nudging strategies predominantly involved alerts and reminders, followed by environmental cues/priming. Conversely, System 2 nudging strategies were predominantly labeled goal setting and feedback. Significantly, 13 studies integrated both System 1 and System 2 nudging strategies (multi-nudge strategies) in their interventions,42,43,45–49,51,53,56,58,64,66 with the most employed nudging strategy being goal setting, combined with various System 1 nudges such as alerts and reminders and loss aversion.
Based on the heterogeneity of outcomes, we clustered the studies into four different objectives for easy comparison. The primary objective of most studies is to increase physical activity among patients with heart disease in a HBCR setting.42,44–48,51,53,56,57,60,61,63–65 The second objective aims to nudge health promotion behaviors among patients with heart disease, including self-care and management and healthy lifestyles.50,55,58,59,66 Additionally, ensuring cardiovascular medication compliance among patients with heart disease is also concerned.49,52,54 The fourth objective focuses on improving home diet management behavior in patients with heart disease.43,62
Types of Nudging Strategies
The nudging strategies associated with System 2 will have an impact on health behaviors in HBCR only if participants choose to pay attention and there is a need for it. For example, a specific food nutrition label is displayed at a time when the food is not purchased (information disclosure). However, the participant may completely ignore it, failing to engage their analytical thinking. This is defined as an active nudging strategy. Additionally, some nudging strategies, such as setting the target option as the default option or working the power of the role model (default/social norm), can also occur without the knowledge and awareness of the participant. This is referred to as a passive nudging strategy. In addition, some nudging interventions are delivered inconsistently with the participant’s decisions or behaviors, which we define as asynchronous nudging strategies. For example, some nudging interventions send emails with feedback that can be read at any time, not just when healthy behavior changes. The aim of this nudging strategy is to change health beliefs, ultimately influencing the transformation of health behaviors. In contrast, during HBCR, participants received immediate just-in-time adaptive nudging interventions that did not hesitate to bring about immediate changes in their health behaviors. We coded these interventions as synchronous nudging strategies.
In order to capture the heterogeneity of nudging strategies, we adopted the method introduced by Sant’Anna et al37 to classify nudging strategies (Figure 4). In this review, four nudging strategies were assigned to more than one quadrant, including reminders and alerts, feedback, peer effects, and environmental cueing and priming. Reminders and alerts usually occur when the target behavior must be performed (synchronous) and requires the participation of the HBCR patients (active). However, three reminders and alerts were divided into passive and asynchronous nudge strategies. In these cases, text messages were sent to remind participants about their daily healthy eating management, which could be read at any time and did not necessitate immediate action. Feedback, on the other hand, generally does not require active participation from home cardiac rehabilitation patients and is therefore classified as a passive nudging strategy. Nonetheless, there was heterogeneity observed, with feedback identified as synchronous five times and asynchronous six times, depending on whether the feedback information was consistent with the target behavior. Peer effects were consistently categorized as simultaneous nudging strategies since the priming object (peer connection) aligns with the target behavior (physical activity). However, two instances were classified as active, requiring active participation from patients in peer interactions and connections, while one instance was considered passive, employing anonymous peer comparison strategies without the participant’s awareness or knowledge. Among the 25 studies included, two environmental cueing and priming were adopted.54,55 One instance was classified as an active and asynchronous nudging strategy, as patients were exposed to relevant contexts through interviews that triggered reflection but did not result in immediate engagement in health-promoting behaviors. The other instance was classified as a passive and synchronous nudging strategy, as patients received carefully crafted messages and pictures during HBCR.
 |
Figure 4 Nudging strategies across quadrants. |
Digital Nudging Strategies
For nudging medium, none focused solely on the physical environment, and 16 involved informatization media, including email, smartphones, and pedometers.42,44,46,47,51–55,57,58,60,62,64–66 Frequently, smartphones were used to send text messages with reminders to improve participants’ physical activity level. As an advanced stage of informatization, there were nine studies involving digital nudging medium, covering smart health applications, digital medical devices, and online internet platforms.43,45,48–50,56,59,61,63 The digital wearables and platforms were used to collect and feedback participants’ behavioral characteristics to implement just-in-time adaptive behavioral nudging. In addition, gamification has become a crucial component of digital nudging strategies. Interestingly, among the nine studies employing digital nudging strategies, three specifically incorporated gamification, all of which demonstrated a positive impact on the primary outcome.47,48,64
Discussion
The aim of this study was to review the literature on nudging health behavior change in HBCR patients to clarify the scope and delivery of nudging strategies. A total of 25 studies from the database were eventually included, and we identified and coded 14 nudging strategies. The most nudging strategies aimed to increase physical activity levels among patients undergoing HBCR. 14 nudging strategies were divided into four quadrants to capture their heterogeneity. In terms of form and content, it has changed from single nudging strategy to multiple ones, and from information nudging strategies to digital nudging strategies. Notably, the incorporation of gamification as a prominent nudging element yielded positive outcomes in the studies. This scope review clarified the scope and delivery of nudging strategies for health behavior change among HBCR patients, completed practical and meaningful classification and explanation, and provided a new digital nudging perspective and trend for understanding the role of nudging strategies in promoting HBCR practice.
HBCR holds significant importance in improving disease prognosis and quality of life for patients with heart disease.5–8 It is especially necessary for patients with heart disease to nudge healthy behavior change during routine HBCR. Nudging has received a lot of attention since 2008 as a simple, low-cost, and easy-to-implement behavior change strategy,21 and surprisingly, only 25 studies were included in this scope review. Most studies focused on the last 4 years, suggesting that nudging is becoming popular in health behavior interventions for HBCR. Of the 25 studies included, a total of 55 nudgings were used, as the vast majority of studies used the multi-nudge strategies. All but one of the studies with multiple nudging strategies had positive results in whole or in part. Although the multi-nudge strategies seems to increase the likelihood that an intervention will be effective, it is difficult to determine which elements are the effective components of an intervention success. In addition, adding an educational element to nudge interventions may be one way to make them sustainable. This study found that the multi-nudge interventions often included an education element, although education has not traditionally been seen as a nudging strategy,21 which could partly explain their long-term positive effects.
Considering two challenges of System 1 and System 2, one is that they ignore whether nudging intervention occurs with the knowledge and awareness of the participants, and the other is that they do not capture whether nudging intervention occurs at the time of decision-making. Therefore, based on a novel classification proposed by Sant’Anna et al, 37 a matrix with two dimensions and four quadrants was plotted to capture the heterogeneity of nudging strategies for health behavior change among HBCR patients. Reminders and alerts have been widely recognized as convenient and low-cost nudging strategies to influence individual health promotion behavior.67–69 However, its long-term effect on the primary outcome remains controversial, potentially due to their categorization as passive nudging interventions. Similarly, default, feedback, and social norms were also classified as passive nudging strategies because they often occur without the patient’s knowledge and awareness. It is worth noting that when nudging interventions cease, patients may struggle to maintain the desired health-promoting behavior, indirectly highlighting the limitations of System 1 within the nudging theory.70–72 However, in all but one study in this review, the passive nudging strategies had a partial or full positive effect on the outcome of the studies. This could be attributed to the utilization of multiple nudging strategies and the inclusion of educational elements as supplementary components.
In this review, active and synchronized nudging strategies showed superiority in terms of both quantity and impact on primary outcomes. The main nudging strategies concentrated in this quadrant were loss aversion and gamification. Loss aversion is a cognitive bias that refers to the tendency of individuals to strongly prefer avoiding losses over acquiring equivalent gains. In other words, people tend to feel the pain of losing something more strongly than the pleasure of gaining something of equal value.73,74 Encouragingly, the review revealed that all the nudging strategies incorporating loss aversion had positive impacts on the research outcomes, further validating the effectiveness of this approach.45–48,64 In addition, we were surprised to find that gamified intervention strategies were always combined with loss aversion theory to promote health behavior change in patients with HBCR. The efficacy of gamification interventions in improving primary outcomes and enhancing patient adherence to interventions has been well-established.75,76 In this review, the gamification nudges with loss aversion theory had a positive effects on the primary outcomes of the studies.47,48,64 This could be attributed to the active participation and synchronization with health promotion behaviors that both gamification and loss aversion require from patients. This combination ensures not only participants’ enthusiasm but also the immediate occurrence of target behaviors, thus substantiating the rationale behind merging these two strategies.
In addition, the first quadrant (active and asynchronous) focuses on three nudging strategies, including goal setting, precommitment, and environmental cueing and priming. Of the 25 studies included, goal-setting was the most commonly adopted motivational strategy, with a focus on nudging physical activity levels among HBCR patients. The goal behavior requires the active participation of the patient, but goal setting is asynchronous with the patient’s efforts. In this review, goal-setting nudging strategies had a positive impact on the results. According to goal setting theory,77,78 goals possess an inherent motivational quality that can convert an individual’s needs into effective efforts. Motivated by the goal, patients’ needs for HBCR will be transformed into intrinsic motivation to promote health behavior change. As a self-control strategy, precommitment is an effective way to help individuals ensure long-term benefits in intertemporal decision-making.79 Similar to goal setting, precommitted behaviors are generated by the patient but are not required to be synchronized with health behavior change. Despite being asynchronous, precommitment as an effective nudging strategy had a positive impact on the findings in this review.47 However, limited research exists on the application of precommitment to promote health behavior change among HBCR patients, and its effectiveness should be further demonstrated in future studies.
In this review, two key trends of nudging strategies were found, one is that multiple nudging strategies have become the mainstream, and the other is that nudging strategies have changed from informatization to digitalization. Of the 25 studies included, the majority covered multi-nudge strategies, and all but one multi-nudge interventions had a positive impact on the primary outcome. Multi-nudge strategies can address various dimensions of patients’ fundamental psychological needs, thereby fostering intrinsic motivation and facilitating its internalization, which ultimately drives behavior change. Although combining multiple nudging strategies seems to increase the likelihood of an intervention being effective, the contributing nudging components remains challenging to identify. Therefore, a systematic integration of intervention strategies is recommended to promote health behavior change in HBCR patients, ensuring a balance between complexity and burden. In addition, the use of digital technology increases the convenience of the implementation of the nudging strategy and greatly reduces the nudging cost.80,81 This review revealed that email, smartphones, and pedometers were commonly used as informatization medium. As a higher stage, especially in recent years, digital nudging medium, covering smart health applications, digital medical devices, and online internet platforms, enable nudging interventions have a positive impact on the primary outcomes of studies with their advantages of convenience, novelty, diversity, and acceptability.43,45,48–50,56,59,61,63 It should be further verified in the future research. Additionally, gamification can enhance participants’ intrinsic motivation by increasing engagement and immersion, providing real-time feedback and goal orientation, fostering social interaction and competition, and improving acceptability and adherence, all of which contribute to sustained behavior change. A key barrier to implementation is participants’ acceptance of digital tools, particularly in populations with limited access to technology or lower digital literacy. Furthermore, privacy concerns and the complexity of integrating multiple strategies may present challenges during implementation. Therefore, future research should focus on overcoming these obstacles by improving accessibility, personalizing nudging strategies, and ensuring user-friendly design to enhance the scalability and effectiveness of nudging interventions.
Limitations
This scoping review has several limitations that should be acknowledged. Firstly, databases outside of medicine and healthcare were not searched in this scope review because we wanted to focus on using nudging strategies to influence health behavior change among HBCR patients. The disadvantage of this decision is that there are potentially important studies not indexed by PubMed, Web of Science, OVID (Embase, Cochrane Library, JBI). Secondly, due to the internal heterogeneity of nudging strategies, although we have identified a series of nudge-related search terms and strategies based on rigorous expert discussions, it is still inevitable that some relevant articles will be missed. Therefore, relevant nudging terms and strategies will be continuously updated and improved in future research. Thirdly, due to the lack of consensus on the theoretical framework of nudging and the heterogeneity of nudging strategies, a challenge arose in classifying and coding the nudging strategies. To address this, we employed a classification method based on Sant’Anna et al,37 which offers a practical way for non-experts to comprehend the nudge strategies influencing health behavior change among HBCR patients. However, future studies should further investigate and validate the terms used in this classification.
Conclusion
In HBCR procedures, health behaviors, such as physical activity, medication compliance, and diet management, play a critical role in the clinical prognosis and quality of life of patients with heart disease, which depends on the patient’s long-term compliance. However, health behavior decisions can be influenced by emotional and cognitive biases. Nudging strategies offer a valuable approach to addressing these biases. This review provides the latest insights on how nudging strategies can be applied and implemented in HBCR settings to promote health behavior change among patients with heart disease.
Acknowledgments
We would like to thank the librarian for her help in developing the literature search strategy.
Funding
This research was sponsored by a grant (Y2023FH-HLFH15-07) from the 2023 Clinical nursing research project of Nursing Branch of the Chinese Research Hospital Association.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baman JR, Sekhon S, Maganti K. Cardiac rehabilitation. JAMA. 2021;326(4):366. doi:10.1001/jama.2021.5952
2. Heidenreich PA, Bozkurt B, Aguilar D, et al. AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2022;145(18):e895–e1032. doi:10.1161/CIR.0000000000001063
3. McDonagh TA, Metra M, Adamo M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
4. Bakhshayeh S, Sarbaz M, Kimiafar K, Vakilian F, Eslami S. Barriers to participation in center-based cardiac rehabilitation programs and patients’ attitude toward home-based cardiac rehabilitation programs. Physiother Theory Pract. 2021;37(1):158–168. doi:10.1080/09593985.2019.1620388
5. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22(1):35–74. doi:10.1177/2047487313501093
6. Imran HM, Baig M, Erqou S, et al. Home-based cardiac rehabilitation alone and hybrid with center-based cardiac rehabilitation in heart failure: a systematic review and meta-analysis. J Am Heart Assoc. 2019;8(16):e012779. doi:10.1161/JAHA.119.012779
7. Krishnamurthi N, Schopfer DW, Shen H, Whooley MA. Association of mental health conditions with participation in cardiac rehabilitation. J Am Heart Assoc. 2019;8(11):e011639. doi:10.1161/JAHA.118.011639
8. Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G. Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
9. Chen YW, Wang CY, Lai YH, et al. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine (Baltimore). 2018;97(4):e9629. doi:10.1097/MD.0000000000009629
10. Nielsen J, Duncan K, Pozehl B. Patient-selected strategies for post cardiac rehabilitation exercise adherence in heart failure. Rehabil Nurs. 2019;44(3):181–185. doi:10.1097/rnj.0000000000000127
11. Yang Z, Jia H, Wang A. Predictors of home-based cardiac rehabilitation exercise adherence among patients with chronic heart failure: a theory-driven cross-sectional study. BMC Nurs. 2023;22(1):415. doi:10.1186/s12912-023-01566-5
12. Schopfer DW, Nicosia FM, Ottoboni L, Whooley MA. Patient perspectives on declining to participate in home-based cardiac rehabilitation: a MIXED-METHODS STUDY. J Cardiopulm Rehabil Prev. 2020;40(5):335–340. doi:10.1097/HCR.0000000000000493
13. Howarter AD, Bennett KK, Barber CE, Gessner SN, Clark JMR. Exercise self-efficacy and symptoms of depression after cardiac rehabilitation: predicting changes over time using a piecewise growth curve analysis. J Cardiovasc Nurs. 2014;29(2):168–177. doi:10.1097/JCN.0b013e318282c8d6
14. Yang Z, Huang H, Xu L, Gao Y, Zhang C, Wang A. From need to action: decoding the role of motivation in adherence to home-based cardiac rehabilitation exercise in chronic heart failure patients. BMC Nurs. 2024;23(1):913. doi:10.1186/s12912-024-02617-1
15. Miyazaki S, Kanbara K, Kunikata J, et al. Heartbeat tracking task performance, an indicator of interoceptive accuracy, is associated with improvement of exercise tolerance in patients undergoing home-based cardiac rehabilitation. Eur Heart J Digit Health. 2022;3(2):296–306. doi:10.1093/ehjdh/ztac008
16. Nagatomi Y, Ide T, Higuchi T, et al. Home-based cardiac rehabilitation using information and communication technology for heart failure patients with frailty. ESC Heart Fail. 2022;9(4):2407–2418. doi:10.1002/ehf2.13934
17. Yang Z, Zheng X, Gao Y, Zhang C, Wang A. Strategies for enhancing home-based cardiac rehabilitation self-management for patients with coronary heart disease: a qualitative study. BMC Nurs. 2025;24(1):27. doi:10.1186/s12912-025-02690-0
18. Hare AJ, Patel MS, Volpp K, Adusumalli S. The role of behavioral economics in improving cardiovascular health behaviors and outcomes. Curr Cardiol Rep. 2021;23(11):153. doi:10.1007/s11886-021-01584-2
19. Vuchinich RE, Tucker JA, Acuff SF, Reed DD, Buscemi J, Murphy JG. Matching, behavioral economics, and teleological behaviorism: final cause analysis of substance use and health behavior. J Exp Anal Behav. 2023;119(1):240–258. doi:10.1002/jeab.815
20. Zamani Z, Ghalichi-Zave Z, Ahmadi Mazhin S, Eshaghzadeh M, Hami M, Zahirian Moghadam T. Systematic review of health policy and behavioral economics: a neglected point in health promotion. J Educ Health Promot. 2022;11(1):285. doi:10.4103/jehp.jehp_989_21
21. Thaler RH, Sunstein CR. Nudge: Improving Decisions about Health, Wealth, and Happiness. Yale University Press; 2008. Available from: https://book.douban.com/subject/3996331/.
22. Hansen PG, Skov LR, Skov KL. Making healthy choices easier: regulation versus nudging. Annu Rev Public Health. 2016;37(1):237–251. doi:10.1146/annurev-publhealth-032315-021537
23. Hertwig R, Grüne-Yanoff T. Nudging and boosting: steering or empowering good decisions. Perspect Psychol Sci. 2017;12(6):973–986. doi:10.1177/1745691617702496
24. Reñosa MDC, Landicho J, Wachinger J, et al. Nudging toward vaccination: a systematic review. BMJ Glob Health. 2021;6(9):e006237. doi:10.1136/bmjgh-2021-006237
25. Shade MY, Rector K, Soumana R, Kupzyk K. Voice assistant reminders for pain self-management tasks in aging adults. J Gerontol Nurs. 2020;46(10):27–33. doi:10.3928/00989134-20200820-03
26. Lakin JR, Arnold CG, Catzen HZ, et al. Early serious illness communication in hospitalized patients: a study of the implementation of the Speaking About Goals and Expectations (SAGE) program. Healthc. 2021;9(2):100510. doi:10.1016/j.hjdsi.2020.100510
27. Hansen PG, Larsen EG, Modin A, Gundersen CD, Schilling M. Nudging hand hygiene compliance: a large-scale field experiment on hospital visitors. J Hosp Infect. 2021;118:63–69. doi:10.1016/j.jhin.2021.09.009
28. Oullier O. Behavioural insights are vital to policy-making. Nature. 2013;501(7468):463. doi:10.1038/501463a
29. Kannengiesser U, Gero JS. Design thinking, fast and slow: a framework for Kahneman’s dual-system theory in design. Design Sci. 2019;5:E10. doi:10.1017/dsj.2019.9
30. Kahneman D. Thinking, Fast and Slow. Penguin Books Ltd; 2012. Available from: https://book.douban.com/subject/10797165/.
31. Ahmad FS, Persell SD. Nudging to improve cardiovascular care-clinicians, patients, or both. JAMA Cardiol. 2023;8(1):31–32. doi:10.1001/jamacardio.2022.4382
32. Chen Y, Harris S, Rogers Y, Ahmad T, Asselbergs FW. Nudging within learning health systems: next generation decision support to improve cardiovascular care. Eur Heart J. 2022;43(13):1296–1306. doi:10.1093/eurheartj/ehac030
33. Tørris C, Mobekk H. Improving cardiovascular health through nudging healthier food choices: a systematic review. Nutrients. 2019;11(10):2520. doi:10.3390/nu11102520
34. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi:10.1097/XEB.0000000000000050
35. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
36. McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75(75):40–46. doi:10.1016/j.jclinepi.2016.01.021
37. Sant’Anna A, Vilhelmsson A, Wolf A. Nudging healthcare professionals in clinical settings: a scoping review of the literature. BMC Health Serv Res. 2021;21(1):543. doi:10.1186/s12913-021-06496-z
38. Wolf A, Sant’Anna A, Vilhelmsson A. Using nudges to promote clinical decision making of healthcare professionals: a scoping review. Prev Med. 2022;164:107320. doi:10.1016/j.ypmed.2022.107320
39. Alsaleh E, Blake H, Windle R. Behavioural intervention to increase physical activity among patients with coronary heart disease: protocol for a randomised controlled trial. Int J Nurs Stud. 2012;49(12):1489–1493. doi:10.1016/j.ijnurstu.2012.07.004
40. Eyles H, McLean R, Neal B, Doughty RN, Jiang Y, Ni Mhurchu C. Using mobile technology to support lower-salt food choices for people with cardiovascular disease: protocol for the SaltSwitch randomized controlled trial. BMC Public Health. 2014;14(1):950. doi:10.1186/1471-2458-14-950
41. Sangster J, Furber S, Allman-Farinelli M, et al. A population-based lifestyle intervention to promote healthy weight and physical activity in people with cardiac disease: the PANACHE (Physical Activity, Nutrition And Cardiac HEalth) study protocol. BMC Cardiovasc Disord. 2010;10(1):17. doi:10.1186/1471-2261-10-17
42. Alsaleh E, Windle R, Blake H. Behavioural intervention to increase physical activity in adults with coronary heart disease in Jordan. BMC Public Health. 2016;16(1):643. doi:10.1186/s12889-016-3313-5
43. Eyles H, McLean R, Neal B, et al. A salt-reduction smartphone app supports lower-salt food purchases for people with cardiovascular disease: findings from the SaltSwitch randomised controlled trial. Eur J Prev Cardiol. 2017;24(13):1435–1444. doi:10.1177/2047487317715713
44. Sangster J, Furber S, Allman-Farinelli M, et al. Effectiveness of a pedometer-based telephone coaching program on weight and physical activity for people referred to a cardiac rehabilitation program: a randomized controlled trial. J Cardiopulm Rehabil Prev. 2015;35(2):124–129. doi:10.1097/HCR.0000000000000082
45. Chokshi NP, Adusumalli S, Small DS, et al. Loss-framed financial incentives and personalized goal-setting to increase physical activity among ischemic heart disease patients using wearable devices: the ACTIVE REWARD randomized trial. J Am Heart Assoc. 2018;7(12):e009173. doi:10.1161/JAHA.118.009173
46. Golbus JR, Gupta K, Stevens R, et al. Understanding baseline physical activity in cardiac rehabilitation enrollees using mobile health technologies. Circ Cardiovasc Qual Outcomes. 2022;15(7):e009182. doi:10.1161/CIRCOUTCOMES.122.009182
47. Patel MS, Benjamin EJ, Volpp KG, et al. Effect of a game-based intervention designed to enhance social incentives to increase physical activity among families: the BE FIT randomized clinical trial. JAMA Intern Med. 2017;177(11):1586–1593. doi:10.1001/jamainternmed.2017.3458
48. Patel MS, Bachireddy C, Small DS, et al. Effect of goal-setting approaches within a gamification intervention to increase physical activity among economically disadvantaged adults at elevated risk for major adverse cardiovascular events: the ENGAGE randomized clinical trial. JAMA Cardiol. 2021;6(12):1387–1396. doi:10.1001/jamacardio.2021.3176
49. Volpp KG, Troxel AB, Mehta SJ, et al. Effect of electronic reminders, financial incentives, and social support on outcomes after myocardial infarction: the heartstrong randomized clinical trial. JAMA Intern Med. 2017;177(8):1093–1101. doi:10.1001/jamainternmed.2017.2449
50. Piera-Jiménez J, Winters M, Broers E, et al. Changing the health behavior of patients with cardiovascular disease through an electronic health intervention in three different countries: cost-effectiveness study in the do cardiac health: advanced new generation ecosystem (Do CHANGE) 2 randomized controlled trial. J Med Internet Res. 2020;22(7):e17351. doi:10.2196/17351
51. Antypas K, Wangberg SC. An Internet- and mobile-based tailored intervention to enhance maintenance of physical activity after cardiac rehabilitation: short-term results of a randomized controlled trial. J Med Internet Res. 2014;16(3):e77. doi:10.2196/jmir.3132
52. Bermon A, Uribe AF, Pérez-Rivero PF, et al. Efficacy and safety of text messages targeting adherence to cardiovascular medications in secondary prevention: TXT2HEART Colombia randomized controlled trial. JMIR mHealth and uHealth. 2021;9(7):e25548. doi:10.2196/25548
53. Butler L, Furber S, Phongsavan P, Mark A, Bauman A. Effects of a pedometer-based intervention on physical activity levels after cardiac rehabilitation: a randomized controlled trial. J Cardiopulm Rehabil Prev. 2009;29(2):105–114. doi:10.1097/HCR.0b013e31819a01ff
54. Cheung NW, Redfern J, Thiagalingam A, et al. Effect of mobile phone text messaging self-management support for patients with diabetes or coronary heart disease in a chronic disease management program (SupportMe) on blood pressure: pragmatic randomized controlled trial. J Med Internet Res. 2023;25(e38275):e38275. doi:10.2196/38275
55. Chew HSJ, Sim KLD, Choi KC, Chair SY. Effectiveness of a nurse-led temporal self-regulation theory-based program on heart failure self-care: a randomized controlled trial. Int J Nurs Stud. 2021;115:103872. doi:10.1016/j.ijnurstu.2021.103872
56. Frederix I, Hansen D, Coninx K, et al. Medium-term effectiveness of a comprehensive internet-based and patient-specific telerehabilitation program with text messaging support for cardiac patients: randomized controlled trial. J Med Internet Res. 2015;17(7):e185. doi:10.2196/jmir.4799
57. Maddison R, Pfaeffli L, Whittaker R, et al. A mobile phone intervention increases physical activity in people with cardiovascular disease: results from the HEART randomized controlled trial. Eur J Prev Cardiol. 2015;22(6):701–709. doi:10.1177/2047487314535076
58. Pfaeffli Dale L, Whittaker R, Jiang Y, Stewart R, Rolleston A, Maddison R. Text message and internet support for coronary heart disease self-management: results from the Text4Heart randomized controlled trial. J Med Internet Res. 2015;17(10):e237. doi:10.2196/jmir.4944
59. Poggio R, Prado C, Santero M, Nejamis A, Gutierrez L, Irazola V. Effectiveness of financial incentives and message framing to improve clinic visits of people with moderate-high cardiovascular risk in a vulnerable population in Argentina: a cluster randomized trial. Prev Med. 2021;153:106738. doi:10.1016/j.ypmed.2021.106738
60. Reid RD, Morrin LI, Beaton LJ, et al. Randomized trial of an internet-based computer-tailored expert system for physical activity in patients with heart disease. Eur J Prev Cardiol. 2012;19(6):1357–1364. doi:10.1177/1741826711422988
61. Saleh ZT, Elshatarat RA, Elhefnawy KA, et al. Effect of a home-based mobile health app intervention on physical activity levels in patients with heart failure: a randomized controlled trial. J Cardiovasc Nurs. 2023;38(2):128–139. doi:10.1097/JCN.0000000000000911
62. Santo K, Hyun K, de Keizer L, et al. The effects of a lifestyle-focused text-messaging intervention on adherence to dietary guideline recommendations in patients with coronary heart disease: an analysis of the TEXT ME study. Int J Behav Nutr Phys Act. 2018;15(1):45. doi:10.1186/s12966-018-0677-1
63. Su JJ, Yu DSF. Effects of a nurse-led eHealth cardiac rehabilitation programme on health outcomes of patients with coronary heart disease: a randomised controlled trial. Int J Nurs Stud. 2021;122:104040. doi:10.1016/j.ijnurstu.2021.104040
64. Xu L, Tong Q, Zhang X, et al. Smartphone-based gamification intervention to increase physical activity participation among patients with coronary heart disease: a randomized controlled trial. J Telemed Telecare. 2023:1357633X221150943. doi:10.1177/1357633X221150943.
65. Foccardi G, Vecchiato M, Neunhaeuserer D, et al. Effectiveness of text messaging as an incentive to maintain physical activity after cardiac rehabilitation: a randomized controlled pilot study. Int J Environ Res Public Health. 2021;18(12):6645. doi:10.3390/ijerph18126645
66. Son YJ, Kim SW, Lee WS, et al. The effects of a 24-week interactive text message-based mobile health intervention for enhancing self-care behaviours of patients with heart failure: a quasi-experimental study. Nurs Open. 2023;10(9):6309–6319. doi:10.1002/nop2.1878
67. Lum E, Jimenez G, Huang Z, et al. Decision support and alerts of apps for self-management of blood glucose for type 2 diabetes. JAMA. 2019;321(15):1530–1532. doi:10.1001/jama.2019.1644
68. Monsen CB, Liao JM, Gaster B, Flynn KJ, Payne TH. The effect of medication cost transparency alerts on prescriber behavior. J Am Med Inform Assoc. 2019;26(10):920–927. doi:10.1093/jamia/ocz025
69. Perri-Moore S, Kapsandoy S, Doyon K, et al. Automated alerts and reminders targeting patients: a review of the literature. Patient Educ Couns. 2016;99(6):953–959. doi:10.1016/j.pec.2015.12.010
70. Codagnone C, Veltri GA, Lupiáñez-Villanueva F, Bogliacino F. The challenges and opportunities of “nudging. J Epidemiol Community Health. 2014;68(10):909–911. doi:10.1136/jech-2014-203948
71. Mortensen AH, Nordhaug M, Lohne V. Nudging in nursing. Nurs Ethics. 2019;26(6):1601–1610. doi:10.1177/0969733018779226
72. Sundar S. Public health needs to go back to basics, not rely on nudge theory. BMJ. 2021;
73. Kahneman D, Tversky A. Prospect Theory: an Analysis of Decision under Risk. Econometrica. 1979;47(2):263–291. doi:10.2307/1914185
74. Levy H, Levy M. Prospect theory, constant relative risk aversion, and the investment horizon. Savona R, ed. PLoS One. 2021;16(4):e0248904. doi:10.1371/journal.pone.0248904
75. Abas SA, Ismail N, Zakaria Y, et al. A Gamified Real-time Video Observed Therapies (GRVOTS) mobile app via the modified nominal group technique: development and validation study. JMIR Serious Games. 2023:
76. Menna B, Noelle O, Hugo van W, Parisa E, Matt J, Ann J. Gamification and adherence to web-based mental health interventions: a systematic review. JMIR Mental Health. 2016;3(3). doi:10.2196/mental.5710
77. Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation: a 35-year odyssey. Am Psychologist. 2002;57(9):705–717. doi:10.1037/0003-066X.57.9.705
78. Locke EA, Latham GP. The development of goal setting theory: a half century retrospective. Motivation Sci. 2019;5(2):93–105. doi:10.1037/mot0000127
79. Kurth-Nelson Z, Redish AD, Kaur P, Asea A. Don’t let me do that! – models of precommitment. Front Neurosci. 2012;6:6. doi:10.3389/fnins.2012.00138
80. Berger M, Lange T, Stahl B. A digital push with real impact – mapping effective digital nudging elements to contexts to promote environmentally sustainable behavior. J Cleaner Prod. 2022;380:134716. doi:10.1016/j.jclepro.2022.134716
81. Özdemir Ş. Digital nudges and dark patterns: the angels and the archfiends of digital communication. Digital Scholarship in the Humanities. 2020;35(2):417–428. doi:10.1093/llc/fqz014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.