")
Back to Journals » Infection and Drug Resistance » Volume 18
Orbital Cellulitis Associated with Scleral Buckle Infection Caused by Macrolide-Resistant Mycobacterium abscessus Complex: A Case Report and Literature Review
Authors Rujkorakarn P , Patamatamkul S
Received 13 January 2025
Accepted for publication 6 May 2025
Published 13 May 2025 Volume 2025:18 Pages 2489—2495
DOI https://doi.org/10.2147/IDR.S516451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Ploysai Rujkorakarn,1 Samadhi Patamatamkul2
1Department of Ophthalmology, Faculty of Medicine, Prince of Songkla University, Hatyai, Songkhla, Thailand; 2Department of Medicine, Suddhavej Hospital, Faculty of Medicine, Mahasarakham University, Maha Sarakham, Thailand
Correspondence: Samadhi Patamatamkul, Department of Medicine, Suddhavej Hospital, Faculty of Medicine, Mahasarakham University, 77/99 Talat, Muang, Maha Sarakham, 44000, Thailand, Tel +66-43-021021, Fax +66-43-722991, Email [email protected]
Abstract: Ocular infections following scleral buckle placement for retinal detachment, though rare, can lead to significant complications such as orbital cellulitis and endophthalmitis. While Mycobacterium chelonae and M. fortuitum complexes were historically the most common nontuberculous mycobacteria (NTM) associated with these infections, cases caused by Mycobacterium abscessus complex (MABC) are rising, posing therapeutic challenges. We report a case of M. abscessus subsp. abscessus (MAB) scleral buckle infection with orbital cellulitis in a 69-year-old male, successfully managed with buckle removal and prolonged systemic antimicrobial therapy. The isolate demonstrated multidrug resistance, including phenotypic macrolide resistance, despite no genotypic mutations detected in erm(41) or rrl. Treatment with imipenem, amikacin, tigecycline, clofazimine, and azithromycin resolved the infection. A review identified 12 cases of MABC scleral buckle infections, underscoring the need for comprehensive surgical and pharmacologic approaches. This case highlights the importance of molecular diagnostics, phenotypic testing, and species-level identification in managing these challenging infections.
Keywords: Mycobacterium abscessus complex, MABC, scleral buckle infection, orbital cellulitis
Introduction
Ocular infections following scleral buckle placement as a treatment for retinal detachment, though rare, can result in significant complications such as orbital cellulitis, with or without abscess formation, and, most concerning, endophthalmitis.1,2 The etiology encompasses a wide range of microorganisms, with gram-positive bacteria accounting for 40–50% of cases (eg, coagulase-negative staphylococci, Corynebacterium spp., Bacillus spp.), and nontuberculous mycobacteria (NTM) being the second or third most common cause.1,2 Previously, M. chelonae complex and M. fortuitum complex were responsible for most buckle-associated NTM infections. However, infections caused by drug-resistant Mycobacterium abscessus complex (MABC) are becoming increasingly common, posing significant treatment challenges.3–5
For infectious disease specialists, who may not frequently encounter ocular infections, understanding the anatomical localization of NTM-related ocular infections is crucial, as the prognosis for visual outcomes varies significantly. Extensive surgical intervention and prolonged antimicrobial therapy may be required, especially in cases of endophthalmitis.6 Given the limited data on the therapy and outcomes of these infections, we report a case of M. abscessus subsp. abscessus (MAB) scleral buckle infection with orbital cellulitis as a complication, along with its management, complemented by a review of related literature.
Case Presentation
A 69-year-old man underwent multiple retinal surgeries on his right eye, including pars plana vitrectomy and scleral buckling, due to rhegmatogenous retinal detachment four years ago. Phacoemulsification with intraocular lens implantation and epimacular membrane peeling were performed a year later. He experienced right eye irritation, redness, and whitish discharge for the past 3 days. Moxifloxacin 0.5% eye drops (ED) and artificial tears were prescribed four times a day by a private clinic. Prior to the illness, the patient denied any injuries, exposure to water, or contact with ubiquitous fluids affecting the eye.
On examination, the visual acuity in the right eye had dropped to 5/200, down from 20/200 at the last visit six months ago. Intraocular pressure was 2 mmHg and there was no sign of globe perforation, consistent with chronic postoperative hypotony, characterized by persistent low intraocular pressure following multiple vitreoretinal surgeries. Slit-lamp examination showed whitish discharge, conjunctival injection, an extruded scleral buckle in the nasal quadrant, no anterior chamber cells, and a posterior capsular intraocular lens (Figure 1A). Fundus examination revealed an attached retina with 360-degree retinal scarring. The left eye was unremarkable. Laboratory investigations showed mild monocytosis (white blood count 5120 cells/mm³, neutrophils 57%, lymphocytes 24.6%, monocytes 12.3%, absolute monocyte count 614 cells/mm³) and newly diagnosed diabetes mellitus with an HbA1C of 9.9%. Anti-interferon gamma antibodies were negative, and chest radiography was normal. Initial computed tomography (CT) of the orbits showed right orbital cellulitis without abscess formation.
 |
Figure 1 (A) Slit-lamp examination showing extrusion of a scleral buckle through the nasal conjunctiva with purulent discharge. (B) Coronal view of contrast-enhanced T1 fat-suppressed MRI of the orbits shows mild right proptosis with diffuse pre-septal and periorbital fat stranding, as well as diffuse scleral thickening. |
The silicone band and tires were removed the next day. During the procedure, after removing the scleral buckle, we irrigated the eye with povidone-iodine by injecting it into the subconjunctival space and left the conjunctiva open to allow drainage of eye discharge. A subconjunctival injection of ceftazidime was administered at the end of the procedure. Eye discharge and small pieces of the silicone band were sent for microorganism culture. Initial direct staining with KOH preparations and Gram staining were negative for microorganisms. Ziehl-Neelsen (ZN) staining was not performed. Postoperatively, the patient received levofloxacin 1.5% ED every two hours during the day, a combination of dexamethasone, neomycin, and polymyxin B eye ointment at bedtime, along with oral ciprofloxacin. At the 2-week follow-up, the clinical condition had mildly improved, with no eye discharge and reduced redness. The laboratory reported the growth of a pure Mycobacterium colony from both the removed silicone band and eye discharge, positive for acid-fast bacilli, which was confirmed as M. abscessus via MALDI-TOF MS (Matrix-Assisted Laser Desorption/Ionization-Time of Flight Mass Spectrometry) identification. After M. abscessus was identified, the patient underwent further MRI of the orbits to exclude micro-abscess formation. The contrast-enhanced MRI demonstrated mild right proptosis, diffuse right pre-septal and periorbital fat stranding, along with diffuse scleral thickening, compatible with right orbital cellulitis and scleritis (Figure 1B). The MRI reported concerns for endophthalmitis; however, after discussion with the ophthalmologist, ocular examination did not reveal any findings indicative of endophthalmitis.
Given the periocular soft tissue involvement, systemic induction therapy with imipenem (2 grams/day), amikacin (15 milligrams per kilogram per day), clofazimine (100 mg/day), and azithromycin (500 mg/day) was initiated for 4 weeks, along with topical amikacin eye drops. Initial GenoType NTM-DR (Hain Lifescience, Nehren, Germany) testing for macrolide- and aminoglycoside-associated mutations did not detect any mutations. However, tigecycline at a dose of 100 mg/day was added for 2 weeks after phenotypic drug susceptibility testing (DST) using broth microdilution revealed multidrug resistance, including resistance to clarithromycin (MIC >16 µg/mL), ciprofloxacin, doxycycline, linezolid, minocycline, tobramycin, and trimethoprim/sulfamethoxazole. The isolate showed susceptibility to amikacin (MIC 16 µg/mL) and intermediate susceptibility to imipenem (MIC 16 µg/mL) and cefoxitin (MIC 64 µg/mL), and MIC for tigecycline of 1 µg/mL without interpretative breakpoint according to the CLSI.7 Due to the protocol of the reference laboratory, which reports macrolide susceptibility only at 14 days, we were unable to determine whether the isolate exhibited inducible macrolide resistance. Further identification using the GenoType NTM-DR VER 1.0 line probe assay (Hain Lifescience, Nehren, Germany) confirmed M. abscessus subsp. abscessus (MAB).
Eye exams and CT of the orbits after 6 weeks of induction therapy showed complete resolution of all abnormalities. Maintenance with clofazimine and azithromycin was continued for 6 months, without recurrence on both clinical examination and CT imaging. There was no recurrent retinal detachment at the 6-month follow-up, and the visual acuity was 20/200 with pinhole correction. The intraocular pressure remained low during follow-up visits, ranged from 3 to 4 mmHg.
Discussion
Ocular NTM infections are increasingly reported worldwide.1,2,8,9 Among rapid-growing NTM, M. chelonae complex and M. fortuitum complex were previously the most commonly reported groups causing scleral buckle infections.9 However, reports of drug-resistant MABC, particularly M. abscessus subsp. abscessus (MAB), are increasing.5,10 The changing epidemiology of ocular NTM infections may be explained by the increasing use of topical fluoroquinolones, which are highly active against M. chelonae complex and M. fortuitum complex, driving selective pressure for MABC, which is generally resistant to most fluoroquinolones.3,5 Additionally, prior to 1992, M. abscessus complex and M. chelonae complex were considered the same species, which may have underestimated the prevalence of MABC infections.3 In our case, it is unclear how the patient acquired the microorganisms. However, we hypothesize that daily exposure to contaminated water, combined with the presence of an ocular foreign body, may have contributed to this infection episode. Previous studies have indicated that water supply systems in community settings might be sources of human infections.3 Surgical contamination from the scleral buckle procedure is very unlikely, given the many years that elapsed between the surgery and the onset of this infection.
We conducted a comprehensive search to identify relevant literature on scleral buckle infections caused by MABC. Using PubMed, a free-text search with the terms (“scleral buckle infection” OR “scleral surgery infection”) AND (“Mycobacterium abscessus” OR “nontuberculous mycobacteria”) yielded 12 papers. A search restricted to MeSH terms, (“Scleral Buckling” [MeSH] AND “Mycobacterium Infections, Nontuberculous” [MeSH]), returned 6 papers, while another MeSH-based search, (“Scleral Buckling” [MeSH]) AND (“Mycobacterium Infections, Nontuberculous” [MeSH] OR “Mycobacterium abscessus”) AND (“Eye Infections, Bacterial” [MeSH] OR “Postoperative Complications” [MeSH]), yielded 7 papers. Combining MeSH terms and free text using the search string (“Scleral Buckling” [MeSH] OR “scleral buckle”) AND (“Mycobacterium Infections, Nontuberculous” [MeSH] OR “Mycobacterium abscessus”) identified 11 papers. Additionally, a Scopus search using the free-text query TITLE-ABS-KEY(“scleral buckle infection” OR “scleral surgery infection”) AND (“Mycobacterium abscessus” OR “nontuberculous mycobacteria”) resulted in 3 papers. From these searches, we identified 3 studies reporting on MABC infections following scleral buckling, collectively accounting for 12 cases of Mycobacterium abscessus complex (MABC) infection.4,5,11
Symptom onset varied from 3 days to a chronic course exceeding 3 weeks.4,11 The median time from buckle placement to infection was 4 years (IQR 4–6), slightly longer than previously reported for other infections following scleral buckling, which ranged from 30 days to 4 years.2,10 Risk factors for MABC infection included immunosuppressive conditions, reported in 2/13 cases (15.4%), such as diabetes mellitus (our report) and prior topical steroid treatment for ocular sarcoidosis.4 Orbital cellulitis was reported in our case; however, its true prevalence remains uncertain, as other papers did not clearly report this complication. Endophthalmitis occurred in 7.7% (1/13) of cases, leading to visual loss and enucleation.5 This is a crucial complication, as the prognosis for endophthalmitis with other NTMs is usually poor, often resulting in enucleation in up to 22.2% of cases.6
Systemic antimicrobial therapy was used in two cases, with only topical treatment in one case, while the remaining studies did not report on systemic treatment. Systemic therapy in our case was prompted by orbital involvement, while the other case involved worsening symptoms.11 Treatment in all cases included buckle removal and topical antimicrobial therapy. Detailed information is provided in Table 1.
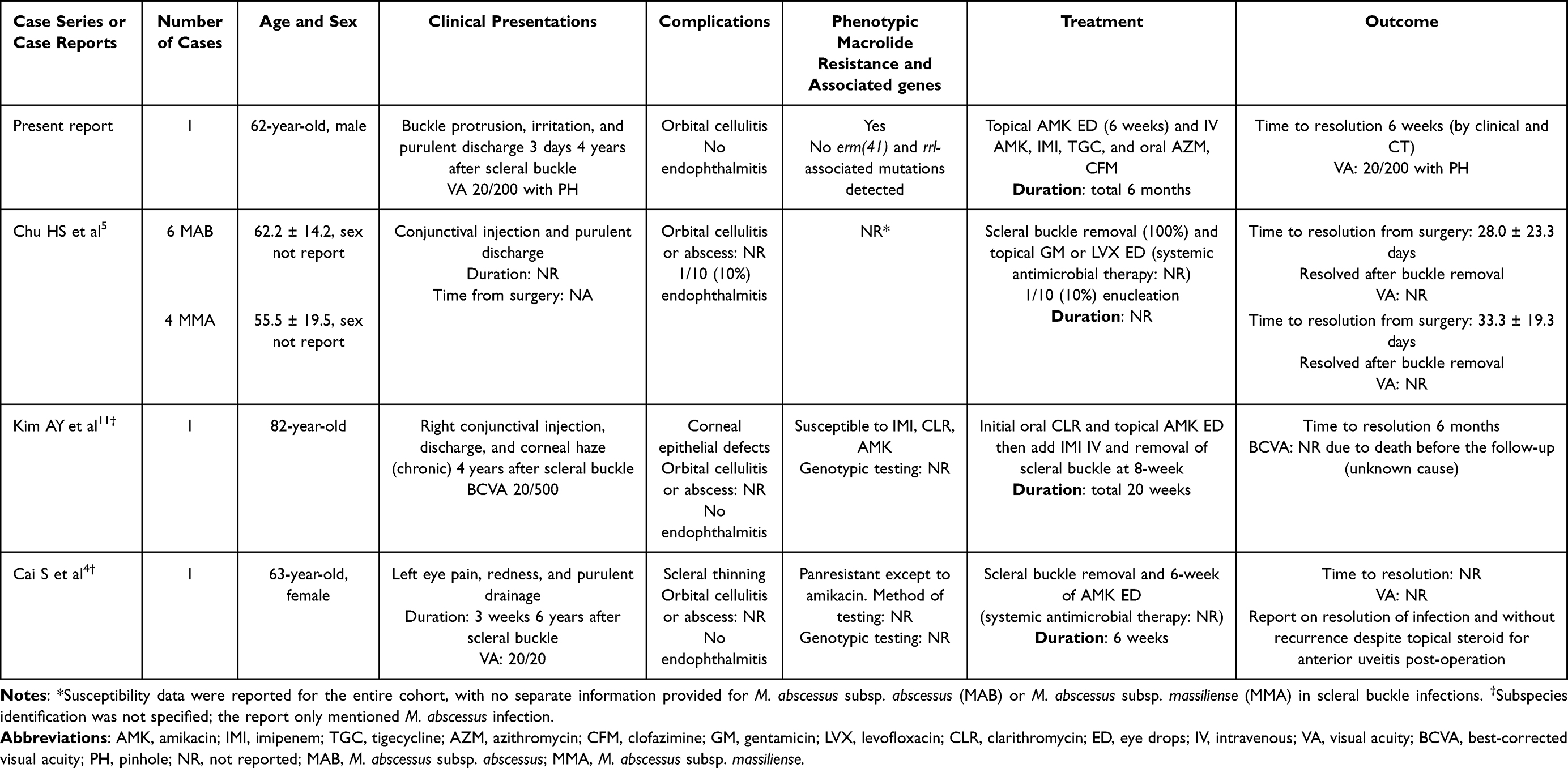 |
Table 1 Summary of Related Literature on MABC Infections Associated with Scleral Buckle |
Owing to the lack of well-controlled trials and the paucity of cases, there is no standard recommendation for optimal regimens or duration of treatment for orbital MABC infections associated with scleral buckles. A previous review12 suggested that scleritis associated with scleral buckle infections without orbital involvement could be treated with buckle explantation and a 6-week course of combined topical aminoglycosides and systemic intravenous therapy (amikacin or cefoxitin plus ciprofloxacin) for susceptible isolates.12 According to a recent meta-analysis and review, orbital involvement typically requires prolonged systemic and topical antimicrobial therapy, with at least 6 weeks of intravenous aminoglycosides plus other susceptible agents, such as oral macrolides, for a total duration from 6 weeks to 6 months.8,12 Despite orbital involvement, there was no loss of vision or need for enucleation, evisceration, or exenteration.8 The largest case series reported that surgical removal is key to resolving the infection, with topical antimicrobial therapy playing a minor role.5 This was also observed in our case. A shorter course of topical therapy combined with systemic antimicrobial therapy for 6 weeks may be reasonable if total scleral buckle explantation is performed and there is no extensive orbital involvement. However, uncertainties remain regarding the necessity of combination therapy involving multiple agents during the intensive phase for infections limited to the sclera or conjunctiva.
From a microbiological perspective, identifying subspecies using molecular methods aids treatment decisions, as MAB is more resistant than other subspecies.3,13 In Thailand, nearly 30% of MAB isolates are resistant to clarithromycin, a core drug for treating this pathogen.13 Amikacin remains the most effective drug, with susceptibility rates of 91% and 82% among MABC and MAB isolates, respectively.13
It is interesting that no mutations in the erm(41) and rrl genes were detected using the GenoType NTM-DR assay (Hain Lifescience, Nehren, Germany). This might be due to resistance mechanisms outside the assay’s targeted regions, suggesting alternative pathways such as intrinsic resistance mediated by whiB7 (from the MAB_3508c isolate), a transcriptional activator gene that regulates the influx of macrolides; an ATP-binding cassette F (ABC-F) gene (from the MAB_2355c isolate) that regulates ATP hydrolysis activity, thereby protecting ribosomes from macrolides; or acquired resistance through other targets.14 Additionally, undetected mutations in erm(41) may contribute to the phenotype.14,15
Current guidance recommends combining genotypic screening with GenoType NTM-DR assay and phenotypic DST for comprehensive assessment.14 In cases of discordant results, whole-genome sequencing is suggested to identify potential undetected mutations not captured by the GenoType NTM-DR assay.14 Although the assay’s sensitivity and specificity compared to phenotypic DST are very high, 96.3% and 100%, respectively.16 Additionally, for clarithromycin resistance, the assay’s mutation detection in rrl yielded high concordant results of 99.3% (144/145) with multigene sequencing and 98.6% (143/145) with drug susceptibility testing (DST).16 Notably, a rare instance was reported in which 1 out of 28 tested isolates of MABC exhibited an undetected mutation in the rrl gene.17 It should be noted that the GenoType NTM-DR assay for macrolide resistance detects alterations at position 28 in the erm(41) gene (either T28 or C28) and mutations at positions 2058 or 2059 in the rrl gene; however, mutations other than T28 or C28 in erm(41) and at positions other than 2058 or 2059 in rrl, may not be detected by the assay.17,18 This underscores the importance of performing susceptibility testing in accordance with CLSI standards, as PCR-based detection of specific mutations may not identify all genetic variations associated with macrolide resistance.7
In conclusion, this case highlights the rising incidence of drug-resistant MABC infections following scleral buckle procedures and underscores the importance of susceptibility testing and species-level identification for appropriate management. Discordant genotypic testing should be confirmed with phenotypic testing and whole-genome sequencing. Effective management, including prompt surgical intervention and targeted antimicrobial therapy, led to favorable outcomes.
Ethical Approval
This study was approved by the Ethics Committee of Mahasarakham University (No. 581-602/2024). According to the Ethics Committee of Mahasarakham University, no additional institutional approval was required for publication of the case details.
Patient Consent Statement
The patient provided informed consent for the publication of both clinical details and images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research project was financially supported by Mahasarakham University.
Disclosure
The authors have no competing interests to declare in this work.
References
1. Pathengay A, Karosekar S, Raju B, Sharma S, Das T. Hyderabad Endophthalmitis Research Group. Microbiologic spectrum and susceptibility of isolates in scleral buckle infection in India. Am J Ophthalmol. 2004;138(4):663–664. doi:10.1016/j.ajo.2004.04.056
2. Chhablani J, Nayak S, Jindal A, et al. Scleral buckle infections: microbiological spectrum and antimicrobial susceptibility. J Ophthalmic Inflamm Infect. 2013;3(1):67. PMCID: PMC4029454. doi:10.1186/1869-5760-3-67
3. Lee MR, Sheng WH, Hung CC, Yu CJ, Lee LN, Hsueh PR. Mycobacterium abscessus complex infections in humans. Emerg Infect Dis. 2015;21(9):1638–1646. doi:10.3201/2109.141634
4. Cai S, Song A, Borkar DS. Mycobacterium abscessus scleral buckle infection. Retin Cases Brief Rep. 2023;17(6):744–746. doi:10.1097/ICB.0000000000001277
5. Chu HS, Chang SC, Shen EP, Hu FR. Nontuberculous mycobacterial ocular infections: comparing the clinical and microbiological characteristics between Mycobacterium abscessus and Mycobacterium massiliense. PLoS One. 2015;10(1):e0116236. doi:10.1371/journal.pone.0116236
6. Shah M, Relhan N, Kuriyan AE, et al. Endophthalmitis caused by nontuberculous Mycobacterium: clinical features, antimicrobial susceptibilities, and treatment outcomes. Am J Ophthalmol. 2016;168:150–156. doi:10.1016/j.ajo.2016.03.035
7. CLSI. Susceptibility Testing of Mycobacteria, Nocardia Spp. and Other Aerobic Actinomycetes.
8. Kheir WJ, Sheheitli H, Abdul Fattah M, Hamam RN. Nontuberculous mycobacterial ocular infections: a systematic review of the literature. Biomed Res Int. 2015;2015:164989. doi:10.1155/2015/164989
9. Das S, Murthy SI, Padhi TR, et al. Ocular infections associated with atypical mycobacteria: a review. Indian J Ophthalmol. 2024;72(1):19–28. doi:10.4103/IJO.IJO_560_23
10. Mohan N, Kar S, Padhi TR, Basu S, Sharma S, Das TP. Changing profile of organisms causing scleral buckle infections: a clinico-microbiological case series. Retina. 2014;34(2):247–253. doi:10.1097/IAE.0b013e3182979e4a
11. Kim AY, Davis AS, Moreau A, Drevets DA, Melendez DP. Management of nontuberculous mycobacterial infections of the eye and orbit: a retrospective case series. Am J Ophthalmol Case Rep. 2020;20:100971. PMCID: PMC7610038. doi:10.1016/j.ajoc.2020.100971
12. Moorthy RS, Valluri S, Rao NA. Nontuberculous mycobacterial ocular and adnexal infections. Surv Ophthalmol. 2012;57(3):202–235. PMID: 22516536. doi:10.1016/j.survophthal.2011.10.006
13. Sukmongkolchai S, Petsong S, Oudomying N, et al. Clinical characteristics and drug susceptibility profiles of Mycobacterium abscessus complex infection at a medical school in Thailand. Ann Clin Microbiol Antimicrob. 2023;22(1):87. doi:10.1186/s12941-023-00637-4
14. Tunesi S, Zelazny A, Awad Z, Mougari F, Buyck JM, Cambau E. Antimicrobial susceptibility of Mycobacterium abscessus and treatment of pulmonary and extra-pulmonary infections. Clin Microbiol Infect. 2024;30(6):718–725. doi:10.1016/j.cmi.2023.09.019
15. Hurst-Hess K, Rudra P, Ghosh P. Mycobacterium abscessus WhiB7 regulates a species-specific repertoire of genes to confer extreme antibiotic resistance. Antimicrob Agents Chemother. 2017;61(11):e01347–17. PMCID: PMC5655061. doi:10.1128/AAC.01347-17
16. Huh HJ, Kim SY, Shim HJ, et al. GenoType NTM-DR performance evaluation for identification of Mycobacterium avium complex and Mycobacterium abscessus and determination of clarithromycin and amikacin resistance. J Clin Microbiol. 2019;57(8):e00516–19. PMCID: PMC6663903. doi:10.1128/JCM.00516-19
17. Kehrmann J, Kurt N, Rueger K, Bange FC, Buer J. GenoType NTM-DR for identifying Mycobacterium abscessus subspecies and determining molecular resistance. J Clin Microbiol. 2016;54(6):1653–1655. PMCID: PMC4879307. doi:10.1128/JCM.00147-16
18. Mougari F, Loiseau J, Veziris N, et al. Evaluation of the new GenoType NTM-DR kit for the molecular detection of antimicrobial resistance in non-tuberculous mycobacteria. J Antimicrob Chemother. 2017;72(6):1669–1677. doi:10.1093/jac/dkx021
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.