")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Overview and Prospects of the Clinical Application of Oliceridine
Authors Yi K , Sun W , Yu W, Chen S
Received 28 February 2025
Accepted for publication 10 June 2025
Published 26 June 2025 Volume 2025:19 Pages 5415—5430
DOI https://doi.org/10.2147/DDDT.S525471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Kun Yi,* Wenjie Sun,* Wen Yu, Shibiao Chen
Department of Anesthesiology, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shibiao Chen, Department of Anesthesiology, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, No. 17 Yongwai Zhengjie, Donghu District, Nanchang, Jiangxi Province, 330006, People’s Republic of China, Tel/Fax +862413870982918, Email [email protected]
Abstract: Opioids can effectively relieve pain but carry risks of addiction and adverse effects. Oliceridine, a G protein-biased μ-Opioid receptor (MOR) agonist, has emerged as a promising safer alternative. By preferentially activating G-protein-biased agonist targeting the μ-opioid receptor while downregulating β-arrestin2 recruitment, oliceridine (Olinvyk) achieves potent analgesia with reduced incidence of opioid-related adverse effects. Supported by robust preclinical data, oliceridine has demonstrated significant clinical potential, prompting global clinical trials to define its optimal indications and therapeutic scenarios. This review synthesizes current evidence on oliceridine’s efficacy, safety, and mechanistic specificity across diverse surgical settings, contrasting its profile with conventional opioids. Additionally, we discuss future research priorities, including dose optimization, expansion into chronic pain management, and long-term safety evaluation.
Keywords: oliceridine, G protein-biased opioids, pain management, β-arrestin2
Background
Pain represents a significant global health burden, particularly in surgical care settings. It is an unpleasant sensation caused by harmful stimuli detected by the nerve endings of nociceptive neurons. With the advancement of global healthcare, the number of surgical procedures performed worldwide is vast and continues to rise, with approximately 312 million surgeries conducted annually.1,2 Postoperative pain ranks among the most prevalent complications of invasive procedures, with epidemiological studies revealing that 30% of surgical patients report clinically relevant acute pain, including 11% enduring intense postsurgical pain requiring urgent intervention.3
Acute postoperative pain refers to pain occurring from the immediate postoperative period up to 7 days, caused by surgical trauma or related complications. Emerging evidence indicates that poorly controlled nociception not only delays functional recovery and prolongs hospitalization, but also elevates risks of extended analgesic dependence, opioid-induced hyperalgesia, and subsequent substance use disorders. From a pathophysiological perspective, unrelieved pain triggers multisystem complications, manifesting as sympathetic-driven cardiovascular stress, splinting-induced pulmonary compromise, ileus from autonomic dysregulation, and acute kidney injury secondary to catecholamine surges.4,5 While most acute pain subsides as tissues heal, it can also be chronicized through the descending pain modulation mechanisms, leading to persistent long-term pain. Inadequate treatment of acute postoperative pain can lead to chronic pain, defined as pain lasting for 2 months or more without any other apparent causes.6,7 Furthermore, inefficient postoperative analgesia amplifies patient safety risks through dose-escalation patterns, thereby potentiating opioid-related adverse drug events ranging from sedation to respiratory depression.8
MOR agonists are the most potent analgesics and are classified as full agonists, partial agonists, and biased agonists (Table 1). However, their therapeutic efficacy is limited by adverse effects, including respiratory depression, reduced gastrointestinal(GI) motility, sedation, nausea, vomiting, constipation, bloating, as well as direct cardiovascular effects, such as lowered blood pressure, vasodilation, and reduced cardiac workload.9–12 A retrospective study involving 135,379 surgical patients reported that 10.6% of patients experienced opioid-related adverse events (ORAEs).8 Current strategies to minimize opioid use in the perioperative setting include regional anesthesia and the individualized use of multimodal non-opioid analgesics, including nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and local infiltration anesthesia. Although opioid minimization strategies have achieved considerable success, an optimal balance between opioid analgesia and the side effects of opioids has yet to be reached in the majority of surgical populations.
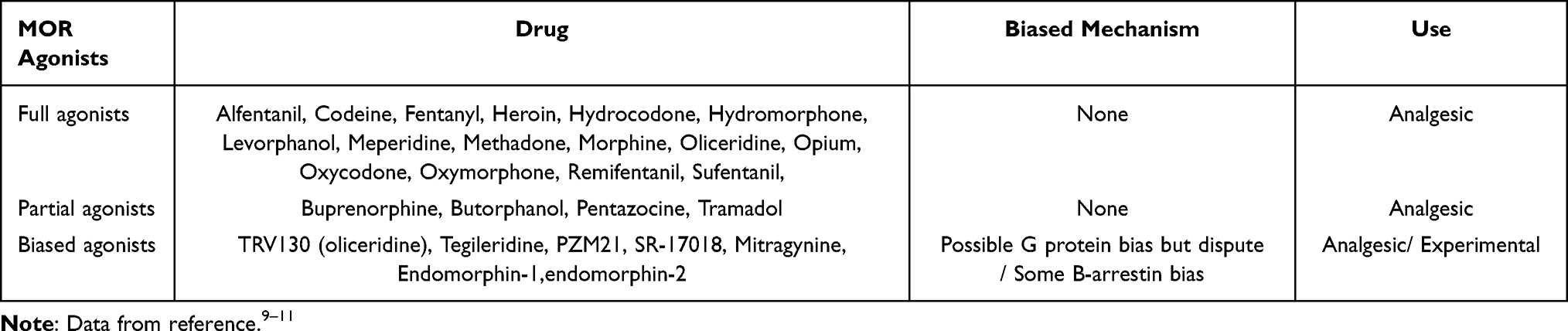 |
Table 1 Representative Examples of Clinical and Experimental MOR Agonists and Classification Based on Their Activity |
The phenomenon wherein ligands selectively activate one signaling pathway over another is termed “biased agonism” or “functional selectivity”.13 In recent years, the emergence of the biased agonism paradigm has advanced our understanding of β-arrestin’s role in GPCR signaling.13–15 This conceptual shift, coupled with the identification of biased ligands capable of eliciting distinct receptor activation profiles and the observation that even minor structural modifications can lead to significant shifts in functional selectivity, has generated substantial scientific interest in elucidating the physiological relevance, pharmacological implications, and structural mechanisms underlying this paradigm.13–18 Opioid receptors are G protein-coupled receptors (GPCRs) that exert their effects primarily through the activation of G-protein pathways and β-arrestin2 proteins.18 The prevailing view is that G-proteins mainly mediate analgesia, reward, and pleasure, while β-arrestin2 proteins regulate side effects such as respiratory depression and gastrointestinal responses, while also attenuating the analgesic effect.19–21 P-glycoprotein also plays essential role in the mechanism of action of oliceridine (Figure 1).22 Oliceridine can selectively biases towards the analgesic pathway of the MOR. It activates G-protein-coupled pathways and downregulates β-arrestin2 signalling, making oliceridine a promising candidate to resolve the clinical challenge of balancing analgesia with opioid side effects.19 Thus, this review will explore and analyze the effectiveness of oliceridine in pain management and its potential applications in various clinical scenarios.
 |
Figure 1 Mechanism of action of Oliceridine. Opioid receptors mainly act by activating the G-protein pathway and β-arrestin2. G protein mainly mediates analgesia, reward and pleasure, while β-arrestin2 acts as a positive regulator of side effects such as respiratory depression and gastrointestinal reactions, and can attenuate analgesia. P-glycoprotein significantly affects the brain exposure of oliceridine, its antineotoxic efficacy, and its ability to induce respiratory depression and potentiation. Created in BioRender. sdrhbv, g. (2025) https://BioRender.com/59oxboj. |
Development of Oliceridine
The initial discovery and subsequent understanding of the GPCRs were primarily driven by the Lefkowitz and Kobilka teams.23–26 In 1999, Bohn et al demonstrated that in mice with β-arrestin2 gene knockouts, morphine’s analgesic effects were enhanced, and its side effects were reduced, thus pioneering the research into biased opioid receptor agonists.27 Furthermore, subsequent studies in β-arrestin2-related mice further confirmed the feasibility and advantages of this research direction.17,28
In 2013, Trevena, Inc. initiated a lead discovery campaign by screening its internal compound library, identifying compound 1 (a 4-phenyl-4-(2-benzylaminoethyl)-tetrahydropyran analog) as a novel mu-opioid receptor (MOR) agonist.29 While this lead candidate exhibited submicromolar G-protein activity at MOR, it demonstrated suboptimal beta-arrestin2 recruitment efficiency (32% of morphine’s 100% response), prompting structure-activity relationship (SAR) optimization. Subsequent compounds were evaluated in rodent analgesic models and a murine constipation model to enhance MOR-mediated G-protein signaling while minimizing beta-arrestin2 engagement. Both (R)-19 and (R)-30 (TRV130) demonstrated promising in vivo pharmacological profiles, the former exhibited potent hERG channel current inhibition and cardiac conduction abnormalities in arterially perfused rabbit ventricular wedge preparations.29,30 This cardiovascular safety concern redirected development efforts toward (R)-30 ([(3-Methoxythiophen-2-yl)methyl]({2[(9R)‐9-(pyridin-2-yl)-6-oxaspiro-[4.5]decan-9-yl]ethyl})amine (TRV130)) (Figure 2), which successfully progressed through IND-enabling studies and is currently undergoing clinical trials for acute severe pain management.29 As research progressed, a variety of new G-protein-biased agonists were developed in different stages of drug discovery, aimed at identifying novel, highly efficient analgesics with minimal side effects. These included compounds such as PZM21 and oliceridine.31–33 To date, considerable progress has been made in the pharmacology of biased ligands targeting opioid receptors.31,34,35 Among these, the research on MOR biased agonists has outpaced studies on δ-opioid receptors (δOR) and κ-opioid receptors (κOR), with the most advanced ligand being TRV130 (Oliceridine). To be specific, preclinical evaluations reveal its exceptional pharmacological properties(Table 2).31,36–39 And it is noteworthy that oliceridine was the first MOR biased agonist to receive US Food and Drug Administration (FDA) approval in 2020. Future studies, particularly large-scale clinical trials, will provide a strong foundation for continued drug development and clinical application.
 |
Table 2 Preclinical Pharmacological Profile of TRV130 (Oliceridine) |
 |
Figure 2 Chemical structure for Oliceridine(Olinvyk). (National Center for Biotechnology Information. “PubChem Compound Summary for CID 66553195, Oliceridine” PubChem, https://pubchem.ncbi.nlm.nih.gov/compound/Oliceridine. Accessed 15 April, 2025). |
Safety of Oliceridine
Adverse Reactions and Safety Analysis
Preliminary safety studies suggest that, compared to morphine, Oliceridine (TRV-130) shows a lower risk of Opioid induced respiratory depression (OIRD) and gastrointestinal(GI) complications in mouse and rat models, as well as in a study involving 30 healthy male volunteers.31,40 Notably, in subsequent controlled clinical trials of Oliceridine (APoll1 and APoll2), the most common adverse effects (occurring in ≥10% of patients) were nausea, vomiting, dizziness, headache, constipation, pruritus, and hypoxia.41,42 A recent systematic review of Oliceridine’s safety revealed that, while more patients showed a significant response to Oliceridine compared to a placebo, the proportion of opioid responders was comparable to that seen with morphine. Importantly, the incidence of respiratory safety events was significantly lower with Oliceridine than with morphine.43 Studies comparing the benefits and risks of morphine and Oliceridine have demonstrated that, within clinically relevant concentrations, Oliceridine has a higher probability of providing analgesia than causing respiratory depression, whereas morphine exhibited the opposite trend, with a higher probability of inducing respiratory depression than providing pain relief. Increasing evidence suggests that Oliceridine has a better safety profile than morphine.19,43 However, scientific authorities highlight methodological concerns regarding the evidentiary foundation derived from preclinical evaluations and controlled clinical testing where adverse event monitoring was implemented as secondary endpoints, supplemented by retrospective investigations and post hoc evaluations. Consequently, these findings remain subject to potential confounding factors stemming from methodological variability across source investigations and the inherent constraints characteristic of post hoc analytical approaches. To further validate the safety differences between Oliceridine and traditional opioids, additional prospective clinical studies are needed.
Abuse Potential
To assess the abuse potential of GPCR-MOR agonists, researchers have employed methods such as conditioned place preference (CPP), intracranial self-stimulation (ICSS), and drug self-administration in animal models.44 In mouse experiments, the administration of a higher dose (10 mg/kg) of oliceridine resulted in a statistically significant conditioned place preference. Furthermore, the study revealed that oliceridine exhibited abuse-related effects similar to morphine in the ICSS paradigm.44,45 In a comparison between Oliceridine and oxycodone, using a progressive ratio reinforcement schedule for drug self-administration, the maximum number of injections for both drugs was similar, indicating that they have comparable abuse potential.46 These findings suggest that oliceridine maintains an abuse potential similar to that of traditional opioid analgesics. In human studies, researchers used a drug effects questionnaire to compare the abuse-related subjective effects of intravenous Oliceridine and morphine in healthy male volunteers. The results indicated that the effects of both drugs were similar at multiple time points.40 Nevertheless, current pharmacological research emphasizes that MOR-targeting agonists represent merely one methodological approach among diverse strategies under exploration for developing analgesics with mitigated misuse liability and improved safety profiles.47 Present evidence does not yet provide sufficient empirical basis to support definitive conclusions about their comparative abuse resistance relative to traditional opioid-based therapeutics.
Drug Resistance
In previous mouse models, β-arrestin2 knockout mice exhibited physical dependence on opioids without developing morphine tolerance, suggesting that tolerance and dependence are independent phenomena with distinct biochemical mechanisms.17 Opioid tolerance typically develops with prolonged drug use, requiring escalating doses to compensate for the reduced effectiveness over time. A significant body of research has demonstrated that, under equivalent analgesic conditions, Oliceridine shows better tolerance compared to morphine.17,48–51 Additionally, these results suggest that there may be a significant gap between the effective dose of oliceridine for MOR-mediated pharmacological effects and the dose required to induce tolerance.
Human Research of TRV130 (Oliceridine)
In 2014, the drug developer Trevena first conducted a dose-escalation clinical trial with TRV130 in healthy volunteers (n = 30) to explore its tolerance, pharmacokinetics, and pharmacodynamics. Experimental investigations demonstrated that TRV130 exhibits linear pharmacokinetic characteristics across administered doses, coupled with exposure-dependent pharmacodynamic activity, thereby establishing a quantifiable correlation between dosage levels and analgesic efficacy. Additionally, TRV130 demonstrated good tolerance across a wide dose range, with observed effects such as pupil constriction at higher doses and analgesic effects at therapeutic doses.52 Later that year, Trevena conducted a comparative study using a placebo and morphine in healthy volunteers to measure safety, tolerance, and analgesic efficacy. The study showed that the 3 mg and 4.5 mg TRV130 groups achieved higher peak analgesic effects and faster onset times than the 10 mg morphine group. Furthermore, the TRV130 groups experienced less significant reductions in respiratory drive and lower severity of nausea, suggesting that TRV130 holds promise for better analgesic potential.40 However, due to the limitation of experimental sample and size, the efficacy and tolerance of TRV130 in clinical pain management still require larger-scale studies to confirm these findings.
Subsequent Phase II studies in patients undergoing bunionectomy (n = 144) and abdominoplasty (n = 200) found that, compared to morphine, oliceridine resulted in a greater reduction in early pain intensity. Furthermore, in the abdominoplasty cohort, oliceridine was associated with a lower incidence of nausea and vomiting compared to morphine, and no drug-related serious adverse events occurred.53,54 In addition, researchers utilized data from Phase I studies and Phase II trials, to develop and evaluate a pharmacokinetic-pharmacodynamic (PK-PD) model. This model demonstrated quantifiable correlations between circulating drug levels and analgesic response, enabling its operational integration into protocol development for oliceridine’s late-stage clinical evaluation.34,35
In two pivotal Phase III APOLLO efficacy trials, for postoperative pain following bunionectomy (n = 418) and abdominoplasty (n = 401), oliceridine demonstrated rapid analgesic relief compared to placebo. Compared with morphine, oliceridine showed excellent safety and tolerability with respect to both respiratory and gastrointestinal side effects. These results suggest that oliceridine could provide new treatment alternative for patients experiencing moderate-to-severe postoperative pain in need of intravenous analgesia.41,42
Additionally, the multicenter Phase III ATHENA safety study was conducted to assess the safety and tolerance of intravenous oliceridine in a diverse, real-world participant cohort (n = 768). This study included patients with a variety of surgical (94%) or non-surgical medical conditions, with the most common procedures being orthopedic (30%), colorectal (15%), or gynecological (15%) surgeries. Notably, 84% of patients received multimodal analgesia. The study results indicated a baseline average NRS pain score of 6.3 ± 2.1. Initial post-dose evaluation at 30 minutes revealed a mean reduction of −2.2 ± 2.3 in NRS pain scores from baseline, indicating prompt analgesic effects that persisted throughout the therapeutic period. Moreover, Treatment discontinuation rates attributable to insufficient therapeutic response remained below 5%, with no documented fatalities or clinically significant cardiopulmonary complications. Adverse event frequencies was low, and overall, oliceridine was found to be safe and well-tolerated in the diverse patient population studied.55
Subsequently, based on extensive research data, Trevena submitted a New Drug Application for oliceridine injection to the FDA in November 2017. In August 2020, the FDA approved oliceridine for the treatment of severe acute pain in adults who require opioid analgesics and for whom alternative treatments are insufficient (Figure 3).56
 |
Figure 3 Research basis and development process of oliceridine. (Created with Microsoft PowerPoint 2021). |
Application and Potential of Oliceridine in Patients with Clinical Pain
The ATHENA safety study demonstrated that oliceridine, either alone or as part of multimodal analgesia, is generally safe and well-tolerated in a broad population of adult patients with moderate-to-severe pain resulting from surgical or medical conditions.55 However, it is important to bear in mind that the study population was highly heterogeneous, and the sample size had certain limitations. On August 8, 2020, oliceridine has been authorised by the FDA for its clinical application. Given its status as an innovative opioid analgesic, it is inevitable that off-label uses will be prevalent. Currently, the application of oliceridine in various types of surgeries and pain conditions is expanding, and it holds significant potential in the ongoing advancements in analgesia and sedation techniques. The following section will analyze and summarize its various applications.
The Role of Oliceridine in Postoperative Acute Pain
Orthopaedics
Due to the insufficient description of the surgical scope in the ATHENA study, indications for oliceridine administration were consolidated through medical review.55 These clinical datasets remain proprietary to Trevena Inc. and lack public accessibility. The medical review exclusively reported primary indications (>5% incidence) for oliceridine administration, with stratification according to surgical categories and defined pain etiologies among emergency department and general medicine populations. The results showed that the main reasons for oliceridine administration in orthopedic patients of the ATHENA study were knee replacement (127 cases, 16.5%) and hip replacement (58 cases, 7.6%).55 Additionally, in the Phase III APOLLO-1 pivotal efficacy study, 418 patients with moderate-to-severe acute postoperative pain following cystectomy were treated with different doses of oliceridine (1.5 mg loading dose / (0.1 mg, 0.35 mg, 0.5 mg) on demand), placebo, and morphine. An exploratory analysis of the study results indicated that both 0.35 mg and 0.5 mg oliceridine regimens demonstrated non-inferiority to morphine (P < 0.01). Compared to placebo, oliceridine clearly demonstrated superior efficacy. Therapeutic parameters encompassing effectiveness, safety profiles, and tolerability deliver critical insights for appraising the risk-benefit ratio of intravenous oliceridine compared to morphine.48
A recent ITC methodology employing indirect comparisons leveraged pooled data from six RCTs (including oliceridine, hydromorphone, fentanyl, and morphine), using morphine as the reference arm, to assess the safety profiles of oliceridine versus fentanyl and hydromorphone. The ITC analysis revealed that, when compared with hydromorphone, manifested significantly lower rates of postoperative nausea/vomiting (PONV) and reduced rescue antiemetic requirements in orthopedic procedures. No significant differences were found in the use of orthopedic medications. On the other hand, the ITC comparison of oliceridine with fentanyl, using data from orthopedic surgeries and combined orthopedic and plastic surgery cases, demonstrated a risk attenuation pattern, but no statistical significance.57 The investigators postulated potential analytical confounding linked to elevated PONV rates documented in plastic surgery cohorts. Therefore, high-quality head-to-head clinical trials remain necessary.
General Surgery and Plastic Surgery
In the ATHENA study, among patients undergoing general surgery, the most common reasons (>5%) for receiving oliceridine treatment, categorized by surgical type, were colectomy (54 cases, 7.0%) and plastic surgery (46 cases, 6.0%).55
Additionally, in the Phase III APOLLO-2 pivotal efficacy study, 401 patients with moderate-to-severe acute postoperative pain following abdominoplasty were treated with a loading dose of placebo, oliceridine (1.5 mg), or morphine (4 mg), followed by patient-controlled analgesia with on-demand dosing (0.1, 0.35, or 0.5 mg oliceridine; 1 mg morphine; or placebo), with a lockout time of 6 minutes. The primary endpoint was the proportion of patients who were treatment responders with oliceridine compared to placebo for more than 24 hours. Secondary endpoints comprised a pre-specified rapid shallow breathing (RSB) metric quantifying total event-duration of respiratory episodes, along with responder rates versus morphine. Analyses demonstrated the 0.1 mg oliceridine dose exhibited placebo-beating efficacy yet remained suboptimal relative to morphine in therapeutic response. Dose-stratified safety assessments revealed morphine-comparable profiles exclusively at 0.35/0.5 mg oliceridine levels, which concurrently achieved non-inferior analgesia versus standard opioid regimens. Definitive analysis confirmed oliceridine’s superior safety profile relative to morphine in abdominoplasty cohorts, manifesting particularly in reduced respiratory depression incidence and lower gastrointestinal complication rates (nausea/vomiting). Pharmacovigilance data further validated its enhanced tolerability metrics across perioperative monitoring parameters.42
Gynecology and Obstetrics
In the ATHENA study, among obstetric and gynecological patients, the main reasons (>5%) for oliceridine administration, categorized by surgical type, were hysterectomy (72 cases, 9.4%).55 Currently, no studies have explored the role of oliceridine in labor analgesia, nor have there been any studies investigating the use of oliceridine in conjunction with intrathecal medications. Oliceridine has not been approved for use in labor, and the FDA approval documents specifically caution that the use of oliceridine in pregnant patients may pose a risk to the fetus. Notably, morphine holds exclusive regulatory approval from the FDA for intrathecal delivery among opioid analgesics within US clinical practice. This singular therapeutic authorization reflects rigorous risk-benefit evaluations of its neuroaxial administration profile. However, fentanyl and sufentanil are commonly used to enhance the potency of amide-type local anesthetics for use in cesarean section analgesia.58,59 Additionally, due to oliceridine’s rapid analgesic properties, intravenous administration of the drug in obstetric patients appears to be a potential area of further investigation.
Burn Medicine
Acute pain following burns is complex and not fully understood. Burn patients often require large doses of opioids to alleviate pain associated with routine burn care. Although Phase III acute pain trials and post-marketing surveillance have validated oliceridine’s therapeutic benefits in surgical cohorts, critical evidence gaps persist regarding its application in refractory post-burn neuropathic pain populations.41,42,55 Recently, a prospective, historical control study was the first to explore the clinical analgesic use of oliceridine in patients with acute burn pain. Over seven days, 10 burn patients were compared with 20 patients receiving standard care (including fentanyl, oxycodone, hydromorphone, and morphine) in a randomized historical cohort. The results showed that the daily NRS pain scores were significantly lower with oliceridine [−7.31 (−10.53, −4.09), p < 0.0001] compared to the traditional opioid treatment group [−5.83 (−8.96, −2.70), p = 0.0004], demonstrating comparability in pain relief. There was no significant difference in opioid use over the 7 days between the oliceridine group and the historical treatment group [14.02 (67.22, 39.19), p = 0.5939], and longitudinal opioid usage within each treatment group showed no difference. Safety surveillance revealed no novel toxicological profiles associated with oliceridine during trial monitoring, with all documented adverse reactions aligning with established pharmacological expectations. Additionally, the significant pain relief achieved with oliceridine was maintained throughout the 7-day study period. While the control group showed initial pain relief, it was not sustained despite similar morphine milligram equivalents (MME).60
It is noteworthy that although the authors believe multimodal therapy may offer the greatest benefits, the researchers did not use multimodal analgesia in this study to truly evaluate the response to oliceridine. Apart from acetaminophen, oliceridine was the only permitted analgesic. Furthermore, the evidence quality in this study was limited by the historical control design and sample size. Therefore, high-quality data on the best approach to multimodal pain management in burn patients remains controversial or lacking. Overall, current practices and guidelines advocate for improved pain management in burn patients, and there is consensus that burn centers should consider incorporating oliceridine into both procedural and non-surgical pain management protocols.60–62
Application and Ongoing Research in Other Surgical Patients
In the ATHENA study, other surgical patients included those from urology (5.7%), neurology (5%), emergency medicine (4.3%), cardiothoracic surgery (2.4%), weight-loss surgery (2.4%), and internal medicine (1.4%).55 However, specific types of surgery for urology, neurology, emergency, and cardiothoracic patients were not disclosed. Moreover, due to the relatively lenient inclusion criteria for patient populations in the study, caution should be exercised when extrapolating these results to larger and more specific patient groups. Looking ahead, large-scale clinical trials of oliceridine will help provide new individualized pain management solutions for different pain populations and may even alter the use of opioid medications altogether (as detailed in Table 3). These future trials will be critical in refining our understanding of oliceridine’s potential across diverse clinical settings.
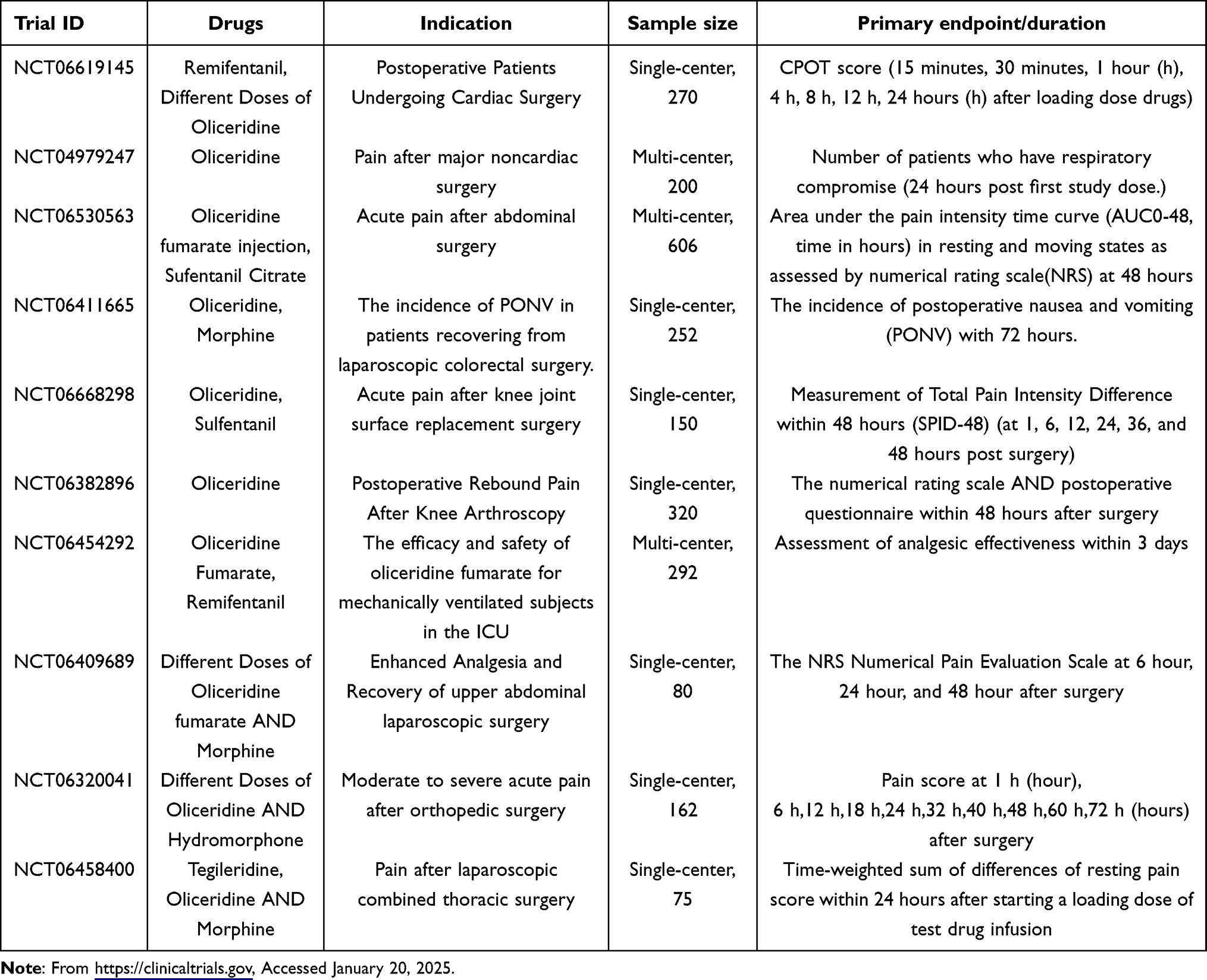 |
Table 3 Selected Ongoing Clinical Trials with Oliceridine |
Oliceridine‘s Role in Chronic Pain
Chronic pain has a wide range of etiologies, including idiopathic mechanisms, musculoskeletal injuries, cancer, and surgical interventions, all of which can exert profound biopsychosocial impacts on functional status.63 It is necessary to bear in mind that in patients who have experienced traumatic events similar to surgical procedures, the boundary between acute and chronic pain is often blurred. Currently, oliceridine has promising potential for managing postoperative acute pain, breakthrough pain, and acute flare-ups of chronic pain.62–66 Therefore, exploring its use in chronic pain remains crucial.
Emerging clinical pharmacology research has detailed first-in-population pharmacokinetic(PK) and safety evaluations through an open-label dose-ranging Phase I investigation of oliceridine in China’s refractory non-oncologic pain population.67 To ensured cohort pathophysiological consistency, the study selected 32 subjects with chronic non-cancer musculoskeletal pain—encompassing adhesive capsulitis, persistent lumbosacral pain, and myofascial dysfunction. The trial began with a preliminary test, where two subjects received a single injection of 0.75 mg. Subsequently, the main trial involved intravenous injection of escalating doses of oliceridine (0.75 mg to 3 mg) in 30 participants. Pharmacokinetic parameters were assessed using non-compartmental analysis. The safety evaluation included monitoring adverse events (AEs).
The results confirmed that the pharmacokinetic parameters and characteristics of oliceridine in the Chinese population were comparable to those observed in the initial trials in the United States, particularly within the 0.75 mg to 3.0 mg dose range. Notably, no serious adverse events (SAEs) were reported, and the nature and severity of treatment-emergent adverse events (TEAEs) were very similar to those observed in the original trials, with no unexpected TEAEs. This study demonstrated the acceptable safety, tolerability, and pharmacokinetic suitability of oliceridine injection, strengthening its potential for continued clinical development and application in the Chinese patient population.
Impact and Potential in Pain Management
Intensive Care Unit (ICU)
Critically ill patients often endure painful experiences that trigger various pathophysiological consequences. Midazolam and fentanyl (occasionally with diphenhydramine) are commonly used for moderate sedation techniques.68,69 Previous review on emerging methods of intravenous moderate and deep sedation highlighted the specific roles of remimazolam and oliceridine in providing these types of sedation.68,70 They may serve as adjuncts to more established sedatives like propofol, etomidate, ketamine, and dexmedetomidine, as well as in ICU procedural sedation. While no current studies have proven their potential in moderate and deep sedation, the authors anticipate that oliceridine will play a role in this field.
Recently, A nationwide, single-masked, active-comparator RCT in 24 tertiary ICU centres across China will evaluate the efficacy and safety of remifentanil and oliceridine in 292 mechanically ventilated ICU patients. The primary outcome of the study is the percentage of time within the target pain range during drug administration. Secondary outcomes include gastrointestinal dysfunction, respiratory depression, sedative use, duration of mechanical ventilation, ICU stay, and extubation failure rates. While currently enrolling participants across 24 ICUs, this multisite randomized investigation is positioned to generate high-grade evidence informing precision analgesia protocols for critical care populations, thereby enhancing oliceridine’s clinical translation potential.71
Gastrointestinal Endoscopy Center
Providing ideal comfort and sedation for patients undergoing gastrointestinal (GI) endoscopic procedures has long been a shared goal for anesthesiologists and endoscopy room physicians and nurses.69,70 Propofol is commonly considered the first-choice drug for screening colonoscopies and complex biliary interventions like endoscopic retrograde cholangiopancreatography (ERCP). Short-acting, strong opioids like fentanyl and remifentanil are often used in combination with propofol, particularly in viscerally provocative interventions like esophagogastroduodenoscopy (EGD).68,69 Administering oliceridine could reduce the amount of propofol required and eliminate the need for opioids like fentanyl, which are known to increase the risk of respiratory depression. This would reduce the risks of hypoventilation and hypoxemia.70 Therefore, oliceridine has the potential to make sedation for GI endoscopies both safe and cost-effective. As noted in previous acute pain management guidelines and reviews on oliceridine, through dual preservation of hemodynamic stability and ventilatory function, oliceridine, when combined with remimazolam (once it becomes available), is likely to revolutionize sedation practices for colonoscopy screenings and more advanced EGDs and ERCPs. Oliceridine has broad potential for use in sedation for GI endoscopy patients.61,70
Considerations for Clinical Scenario Application
It is important to note that clinical scenarios are highly complex, and each pain patient should have their analgesic treatment individualized. In a previous Phase I, open-label, single-dose study, the pharmacokinetics and safety of 0.5 mg intravenous oliceridine were evaluated in patients with hepatic and renal dysfunction.51 The study included patients with end-stage renal disease (ESRD, n = 9) who received a 0.5 mg intravenous dose and healthy controls (n = 8) who received 1 mg, assessing the pharmacokinetics and safety of the drug. Additionally, the pharmacokinetics and safety of a 0.5 mg IV dose were evaluated in patients with varying degrees of liver dysfunction (mild, n = 10; moderate, n = 10; severe, n = 6) compared with healthy controls (n = 8).The results showed no difference in clearance rates between subjects with normal renal function and those with end stage renal disease (ESRD), indicating that dosage adjustments are not necessary. For patients with mild or moderate liver dysfunction, no dosage adjustments are needed. However, in patients with severe liver dysfunction, consideration should be given to reducing the initial dose due to the longer half-life observed in these individuals.51
Recently, a study involving 20 healthy male and female volunteers (randomized, double-blind, placebo-controlled, dose-ranging, partial-block design) evaluated the neurocognitive effects of oliceridine compared with morphine.72 The study utilized pharmacokinetic and pharmacodynamic analysis to establish an efficacy function. Neurocognitive tests, cold pressor tests, and plasma drug concentration measurements were conducted before and after administration. The results indicated that the latency to a hand withdrawal (analgesic benefit) increased by 50% or more, and the probability of neurocognitive dysfunction was reduced by at least 25%. Therefore, considering both pain relief and neurocognitive function, oliceridine appears to be a safe analgesic with minimal neurocognitive impairment.72
Furthermore, the oliceridine prescribing information includes a number of important clinical application considerations. The latest corrections and updates to the prescribing information have added new content, including indications and usage, dosage and administration, warnings, and precautions. These updates address risks related to opioid-induced hyperalgesia (OIH) and the potential for opioid hypersensitivity, misuse, abuse, addiction, overdose, and death, as well as risks of hypoglycemia.36,73 Overall, for patients with insufficient alternative treatment options, oliceridine should be prescribed alongside other opioids while limiting the dose and duration to the minimum required. If any serious adverse reactions occur, oliceridine should be discontinued immediately.36
Cost-Effectiveness of Oliceridine
Compared to traditional opioid morphine, oliceridine may provide an economically viable alternative for postoperative pain management. A recent study on the cost-effectiveness of oliceridine established a decision-analysis model to calculate the medication and management costs associated with the most common AEs—such as oxygen saturation < 90%, vomiting, and drowsiness—following the use of either oliceridine or morphine post-surgery.74 The results showed that the cost of managing AEs with oliceridine was $528,424, while for morphine, it was $852,429, resulting in a net savings of $324,005. The study suggests that, despite a slight increase in drug costs, oliceridine has a favorable overall impact on the total cost of postoperative care compared to morphine.74 Subsequently, the research team further developed a budget impact model based on evidence from Phase III clinical trials. By analyzing the differences in analgesic costs and resource utilization when oliceridine was selectively used in high-risk patients (including elderly and obese individuals), compared to morphine use in low-risk patients, the team expanded the economic evaluation. The results demonstrated that, in postoperative care for high-risk patients, the use of oliceridine provided favorable health economic benefits compared to morphine.75 However, the two modeling studies were limited to a 24-hour time frame, which may have led to an underestimation of the costs for patients with multiple comorbidities. Therefore, when considering hospital settings with a significant proportion of such patients, the estimated cost savings may be even greater. Furthermore, future research and economic modeling should not solely focus on respiratory depression, vomiting, and sedation, but should also take into account all observed ORAEs, such as constipation and postoperative ileus.74
Discussion
The research into the mechanism of action of G-protein-biased opioid receptor agonists is ongoing and evolving. Extensive studies have indicated that opioid analgesia is mediated by G-protein-dependent signaling, while adverse effects are thought to be triggered by pathways involving β-arrestin2 proteins. This view is widely accepted. However, contemporary genetic interrogation of pan-tissue β-arrestin2 ablation models and MOR-coupled β-arrestin2 pathway disruption fails to corroborate the purported mechanistic link to opioid-related adverse sequelae (respiratory compromise, gastrointestinal dysmotility, pharmacological tachyphylaxis) in preclinical validation studies.22,76–78 These findings suggest that β-arrestin2 signaling and G-protein-dependent signaling are not simply separable in the context of opioid side effects.
In a study using cell-based assays or mutant strains, it was found that oliceridine exhibited weak intrinsic efficacy, and the favorable therapeutic window and reduced adverse effects (such as respiratory depression) were attributed to partial agonism rather than biased agonism.79 However, current mechanistic insights predominantly originate in heterologous expression systems under controlled in vitro conditions, which inherently lack the spatiotemporal resolution to model system-level pharmacodynamics. Emerging translational pharmacology now employs integrated experimental paradigms encompassing cellular assays and preclinical murine models to deconvolute oliceridine’s biodistribution kinetics and target engagement dynamics in whole-organism contexts. The results supported the idea that oliceridine’s functional selectivity is attributed to low intrinsic potency at the MOR and demonstrated marked influence of P-glycoprotein (P-gp) on oliceridine’s pharmacokinetics, pharmacodynamics, and efficacy profile.22 It’s important to note that Stahl and Bohn, in their reanalysis of these findings, clarified that the quantification of ligand-directed signaling phenotypes (intrinsic efficacy/biased agonism) is contingent upon the cellular signaling architecture (including receptor abundance, effector stoichiometry, and signal transduction cascades) in conjunction with reference ligand selection criteria. Different cell systems can lead to different signaling characteristics.80 In summary, oliceridine indeed exhibits biased agonism toward G-protein signaling, and its partial agonist action in both G-protein signaling and β-arrestin2 recruitment helps improve the therapeutic window. However, intrinsic efficacy is not related to biased agonism.62 The specific mechanism remains to be further explored.
Oliceridine has significant potential to enhance the safety profile of opioid medications. However, many of its clinical trials are still ongoing, and there is a lack of head-to-head studies to determine oliceridine’s efficacy across different clinical scenarios, as well as to directly compare its performance with other traditional opioids. As a result, much of the current data comes from secondary analyses. One retrospective cohort study involving three Phase III trials evaluated OIRD in two cohorts.81 The primary outcome was the incidence of OIRD as defined by surgery, while secondary outcomes included intergroup comparisons of OIRD rates in high-risk patient subgroups. The results indicated that oliceridine had a lower incidence of emergency OIRD compared to patients receiving intravenous morphine alone or in combination with other opioids.
Additionally, exploratory studies from three Phase III trials48,82,83 found that oliceridine, compared to morphine, was associated with reduced vomiting and a lower risk of requiring antiemetic rescue medication, demonstrating better gastrointestinal tolerability. Pooled analysis of the trials showed a significant reduction in opioid-related respiratory complications, independent of demographic/anthropometric covariates (age/BMI). Under equivalent analgesia conditions, oliceridine showed better overall tolerability and was less likely to result in composite safety endpoints composed of ORAEs.
As mentioned earlier, indirect comparisons via ITC (Indirect Treatment Comparison) analysis have been performed, but these findings are based on lower-level evidence and lack real-world head-to-head comparisons. In conclusion, the quality of evidence from these studies may be impacted by factors such as the heterogeneity of the original research, differences in trial designs, and the limitations of retrospective analyses. There is a critical need for high-quality prospective trials to better understand oliceridine’s benefits and safety compared to traditional opioids.
Conclusion
Oliceridine has emerged as a promising analgesic with excellent efficacy and safety profiles in postoperative pain management. Compared to traditional opioids, oliceridine offers significant advantages in reducing side effects such as respiratory depression, addiction risks, and gastrointestinal dysfunction, making it a safer alternative for clinicians when selecting analgesic medications. The exploration of personalized and multimodal pain management strategies represents a key direction for future pain management. Due to its unique mechanism of action, oliceridine holds great potential in various patient populations. Moreover, it has demonstrated favorable outcomes across a range of surgical types, showcasing its broad clinical prospects. Although current research supports the use of oliceridine, future studies should focus on optimizing its dosing regimens to enhance efficacy and minimize potential adverse effects. Additionally, exploring oliceridine’s effectiveness in a wider array of clinical scenarios, including post-surgery applications across different surgical procedures and its potential in chronic pain management, is crucial for future research. Large-scale clinical trials and longitudinal studies will be essential in further validating oliceridine’s efficacy and safety, which will, in turn, facilitate its widespread clinical adoption.
Abbreviations
FDA, Food and Drug Administration; MOR, μ-Opioid receptor; GI, gastrointestinal; ORAEs, opioid-related adverse events; NSAIDs, nonsteroidal anti-inflammatory drugs; GPCRs, G protein-coupled receptors; SAR, structure-activity relationship; δOR, δ-opioid receptors; κOR, κ-opioid receptors; CPP, conditioned place preference; ICSS, intracranial self-stimulation; PK-PD, pharmacokinetic-pharmacodynamic; PONV, postoperative nausea/vomiting; RSB, rapid shallow breathing; MME, morphine milligram equivalents; PK, pharmacokinetic; AEs, adverse events; SAEs, serious adverse events; TEAEs, treatment-emergent adverse events; ICU, Intensive Care Unit; ERCP, endoscopic retrograde cholangiopancreatography; EGD, esophagogastroduodenoscopy; ESRD, end stage renal disease; OIH, opioid-induced hyperalgesia; P-gp, P-glycoprotein; ITC, Indirect Treatment Comparison.
Acknowledgments
The authors acknowledge financial supports from National Natural Science Foundation of China (No. 82360385), Wu Jieping Medical Foundation (320.6750.2024-15-139).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Weiser TG, Haynes AB, Molina G, et al. Size and distribution of the global volume of surgery in 2012. Bull World Health Organ. 2016;94(3):201–209F. doi:10.2471/BLT.15.159293
2. Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014;30(1):149–160. doi:10.1185/03007995.2013.860019
3. McGrath B, Elgendy H, Chung F, Kamming D, Curti B, King S. Thirty percent of patients have moderate to severe pain 24 hr after ambulatory surgery: a survey of 5,703 patients. Can J Anaesth J Can Anesth. 2004;51(9):886–891. doi:10.1007/BF03018885
4. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–2298. doi:10.2147/JPR.S144066
5. Soffin EM, Lee BH, Kumar KK, Wu CL. The prescription opioid crisis: role of the anaesthesiologist in reducing opioid use and misuse. BJA Br J Anaesth. 2019;122(6):e198–e208. doi:10.1016/j.bja.2018.11.019
6. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet Lond Engl. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
7. Ossipov MH, Morimura K, Porreca F. Descending pain modulation and chronification of pain. Curr Opin Support Palliat Care. 2014;8(2):143–151. doi:10.1097/SPC.0000000000000055
8. Shafi S, Collinsworth AW, Copeland LA, et al. Association of opioid-related adverse drug events with clinical and cost outcomes among surgical patients in a large integrated health care delivery system. JAMA Surg. 2018;153(8):757–763. doi:10.1001/jamasurg.2018.1039
9. Opioids. Opioid Antagonists. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547864/.
10. Kelly E, Conibear A, Henderson G. Biased agonism: lessons from studies of opioid receptor agonists. Annu Rev Pharmacol Toxicol. 2023;63:491–515. doi:10.1146/annurev-pharmtox-052120-091058
11. Dhillon S. Tegileridine: first Approval. Drugs. 2024;84(6):717–720. doi:10.1007/s40265-024-02033-4
12. Paul AK, Smith CM, Rahmatullah M, et al. Opioid analgesia and opioid-induced adverse effects: a review. Pharmaceuticals. 2021;14(11):1091. doi:10.3390/ph14111091
13. Rankovic Z, Brust TF, Bohn LM. Biased agonism: an emerging paradigm in GPCR drug discovery. J Med Chem. 2017;60:5943–5954. doi:10.1021/acs.jmedchem.6b01469
14. Therapeutic potential of β-arrestin- and G protein-biased agonists - PMC. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3628754/.
15. Functional selectivity at the μ-opioid receptor: implications for understanding opioid analgesia and tolerance - PMC. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3186080/.
16. Development of functionally selective, small molecule agonists at kappa opioid receptors - PMC. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3868780/.
17. Bohn LM, Gainetdinov RR, Lin FT, Lefkowitz RJ, Caron MG. Mu-opioid receptor desensitization by beta-arrestin-2 determines morphine tolerance but not dependence. Nature. 2000;408(6813):720–723. doi:10.1038/35047086
18. Bohn LM, Dykstra LA, Lefkowitz RJ, Caron MG, Barak LS. Sci-hub | relative opioid efficacy is determined by the complements of the G Protein-Coupled receptor desensitization machinery. Mol Pharmacol. 2004;66(1):106–112. doi:10.1124/mol.66.1.106
19. Dahan A, van Dam CJ, Niesters M, et al. Benefit and risk evaluation of biased μ-receptor agonist oliceridine versus morphine. Anesthesiology. 2020;133(3):559–568. doi:10.1097/ALN.0000000000003441
20. Beta-arrestin-biased ligands at seven-transmembrane receptors - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/17644195/.
21. Biased mu-opioid receptor ligands: a promising new generation of pain therapeutics - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/27936408/.
22. Ventriglia E, Rizzo A, Gomez JL, et al. Essential role of P-glycoprotein in the mechanism of action of oliceridine. Neuropsychopharmacology. 2022;48(5):831. doi:10.1038/s41386-022-01507-x
23. Goudra B. Oliceridine- opioid of the 21st century. Saudi J Anaesth. 2022;16(1):69. doi:10.4103/sja.sja_510_21
24. Benovic JL, Strasser RH, Caron MG, Lefkowitz RJ. Beta-adrenergic receptor kinase: identification of a novel protein kinase that phosphorylates the agonist-occupied form of the receptor. Proc Natl Acad Sci U S A. 1986;83(9):2797–2801. doi:10.1073/pnas.83.9.2797
25. Lohse MJ, Benovic JL, Codina J, Caron MG, Lefkowitz RJ. beta-Arrestin: a protein that regulates beta-adrenergic receptor function. Science. 1990;248(4962):1547–1550. doi:10.1126/science.2163110
26. Rasmussen SGF, DeVree BT, Zou Y, et al. Crystal structure of the β2 adrenergic receptor-Gs protein complex. Nature. 2011;477(7366):549–555. doi:10.1038/nature10361
27. Bohn LM, Lefkowitz RJ, Gainetdinov RR, Peppel K, Caron MG, Lin FT. Enhanced morphine analgesia in mice lacking β-arrestin 2. Science. 1999;286(5449):2495–2498. doi:10.1126/science.286.5449.2495
28. Raehal KM, Walker JKL, Bohn LM. Morphine side effects in beta-arrestin 2 knockout mice. J Pharmacol Exp Ther. 2005;314(3):1195–1201. doi:10.1124/jpet.105.087254
29. Chen XT, Pitis P, Liu G, et al. Structure-activity relationships and discovery of a G protein biased μ opioid receptor ligand, [(3-methoxythiophen-2-yl)methyl]({2-[(9R)-9-(pyridin-2-yl)-6-oxaspiro-[4.5]decan-9-yl]ethyl})amine (TRV130), for the treatment of acute severe pain. J Med Chem. 2013;56(20):8019–8031. doi:10.1021/jm4010829
30. Blinded validation of the isolated arterially perfused rabbit ventricular wedge in preclinical assessment of drug-induced proarrhythmias - PMC. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC1955432/.
31. DeWire SM, Yamashita DS, Rominger DH, et al. A G protein-biased ligand at the μ-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344(3):708–717. doi:10.1124/jpet.112.201616
32. Manglik A, Kruse AC, Kobilka TS, et al. Crystal structure of the μ-opioid receptor bound to a morphinan antagonist. Nature. 2012;485(7398):321–326. doi:10.1038/nature10954
33. Manglik A, Lin H, Aryal DK, et al. Structure–based discovery of opioid analgesics with reduced side effects. Nature. 2016;537(7619):185. doi:10.1038/nature19112
34. Fossler MJ, Sadler BM, Farrell C, et al. Oliceridine (TRV130), a novel G protein–biased ligand at the μ-opioid receptor, demonstrates a predictable relationship between plasma concentrations and pain relief. I: development of a pharmacokinetic/pharmacodynamic model. J Clin Pharmacol. 2018;58(6):750–761. doi:10.1002/jcph.1076
35. Fossler MJ, Sadler BM, Farrell C, et al. Oliceridine, a novel G protein–biased ligand at the μ‐opioid receptor, demonstrates a predictable relationship between plasma concentrations and pain relief. II: simulation of potential phase 3 study designs using a pharmacokinetic/pharmacodynamic model. J Clin Pharmacol. 2018;58(6):762–770. doi:10.1002/jcph.1075
36. Drugs@FDA. FDA-approved drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=BasicSearch.process.
37. Novel molecular targets of dezocine and their clinical implications - PMC. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3944410/.
38. Sci-Hub. Delta opioid receptors: learning and motivation. Handbook of Experimental Pharmacology. Available from: https://sci-hub.st/10.1007/164_2016_89.
39. Sci-Hub. The concise guide to pharmacology 2021/22: enzymes. Br J Pharmacol. 178(S1). doi:10.1111/bph.15542
40. Soergel DG, Subach RA, Burnham N, et al. Biased agonism of the μ-opioid receptor by TRV130 increases analgesia and reduces on-target adverse effects versus morphine: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Pain. 2014;155(9):1829–1835. doi:10.1016/j.pain.2014.06.011
41. Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the µ-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;12:927. doi:10.2147/JPR.S171013
42. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO‐2: a randomized, placebo and active‐controlled phase
43. Safety evaluation of oliceridine for the management of postoperative moderate-to-severe acute pain: Expert Opinion on Drug Safety: Vol 20, No 11 - Get Access. Available from: https://www.tandfonline.com/doi/full/10.1080/14740338.2021.1965989.
44. Liang DY, Li WW, Nwaneshiudu C, Irvine KA, Clark JD. Pharmacological characters of oliceridine, a μ-opioid receptor G-protein-biased ligand in mice. Anesth Analg. 2019;129(5):1414–1421. doi:10.1213/ANE.0000000000003662
45. Altarifi AA, David B, Muchhala KH, Blough BE, Akbarali H, Negus SS. Effects of acute and repeated treatment with the biased mu opioid receptor agonist TRV130 (oliceridine) on measures of antinociception, gastrointestinal function & abuse liability in rodents. J Psychopharmacol Oxf Engl. 2017;31(6):730–739. doi:10.1177/0269881116689257
46. Zamarripa CA, Edwards SR, Qureshi HN, Yi JN, Blough BE, Freeman KB. The G-protein biased mu-opioid agonist, TRV130, produces reinforcing and antinociceptive effects that are comparable to oxycodone in rats. Drug Alcohol Depend. 2018;192:158–162. doi:10.1016/j.drugalcdep.2018.08.002
47. Negus SS, Freeman KB. Abuse potential of biased mu opioid receptor agonists. Trends Pharmacol Sci. 2018;39(11):916. doi:10.1016/j.tips.2018.08.007
48. Hammer GB, Khanna AK, Michalsky C, et al. Oliceridine exhibits improved tolerability compared to morphine at equianalgesic conditions: exploratory analysis from two phase 3 randomized placebo and active controlled trials. Pain Ther. 2021;10(2):1343–1353. doi:10.1007/s40122-021-00299-0
49. Muchhala KH, Jacob JC, Dewey WL, Akbarali HI. Role of β-arrestin-2 in short- and long-term opioid tolerance in the dorsal root ganglia. Eur J Pharmacol. 2021;899:174007. doi:10.1016/j.ejphar.2021.174007
50. Singleton S, Baptista-Hon DT, Edelsten E, McCaughey KS, Camplisson E, Hales TG. TRV130 partial agonism and capacity to induce anti-nociceptive tolerance revealed through reducing available μ-opioid receptor number. Br J Pharmacol. 2021;178(8):1855–1868. doi:10.1111/bph.15409
51. Nafziger AN, Arscott KA, Cochrane K, Skobieranda F, Burt DA, Fossler MJ. The influence of renal or hepatic impairment on the pharmacokinetics, safety, and tolerability of oliceridine. Clin Pharmacol Drug Dev. 2020;9(5):639–650. doi:10.1002/cpdd.750
52. Soergel DG, Ann Subach R, Sadler B, et al. First clinical experience with TRV130: pharmacokinetics and pharmacodynamics in healthy volunteers. J Clin Pharmacol. 2014;54(3):351–357. doi:10.1002/jcph.207
53. Viscusi ER, Webster L, Kuss M, et al. A randomized, Phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157(1):264–272. doi:10.1097/j.pain.0000000000000363
54. Singla N, Minkowitz HS, Soergel DG, et al. A randomized, Phase IIb study investigating oliceridine (TRV130), a novel µ-receptor G-protein pathway selective (μ-GPS) modulator, for the management of moderate to severe acute pain following abdominoplasty. J Pain Res. 2017;10:2413–2424. doi:10.2147/JPR.S137952
55. Bergese SD, Brzezinski M, Hammer GB, et al. ATHENA: a phase 3, open-label study of the safety and effectiveness of oliceridine (TRV130), A G-protein selective agonist at the µ-opioid receptor, in patients with moderate to severe acute pain requiring parenteral opioid therapy. J Pain Res. 2019;12:3113–3126. doi:10.2147/JPR.S217563
56. Markham A. Oliceridine: first approval. Drugs. 2020;80(16):1739–1744. doi:10.1007/s40265-020-01414-9
57. Biskupiak J, Oderda G, Brixner D, Wandstrat TL. Gastrointestinal adverse effects associated with the use of intravenous oliceridine compared with intravenous hydromorphone or fentanyl in acute pain management utilizing adjusted indirect treatment comparison methods. J Comp Eff Res. 2024;13(5):e230041. doi:10.57264/cer-2023-0041
58. Sheng LB, Wang W, Qiang WZ, et al. Efficacy and safety of local anesthetics bupivacaine, ropivacaine and levobupivacaine in combination with sufentanil in epidural anesthesia for labor and delivery: a meta-analysis. Curr Med Res Opin. 2014;30(11):2279–2289. doi:10.1185/03007995.2014.946127
59. Goudra BO. Opioid of the 21st Century. Saudi J Anaesth. 2022;16(1):69–75. doi:10.4103/sja.sja_510_21
60. Hill DM, Todor LA. A prospective, historical-controlled evaluation of oliceridine for moderate or severe pain in patients with acute burn injuries. Burns. 2025;51(2):107343. doi:10.1016/j.burns.2024.107343
61. Romanowski KS, Carson J, Pape K, et al. American burn association guidelines on the management of acute pain in the adult burn patient: a review of the literature, a compilation of expert opinion, and next steps. J Burn Care Res off Publ Am Burn Assoc. 2020;41(6):1129–1151. doi:10.1093/jbcr/iraa119
62. Hill DM, DeBoer E. State and future science of opioids and potential of biased-ligand technology in the management of acute pain after burn injury. J Burn Care Res off Publ Am Burn Assoc. 2023;44(3):524. doi:10.1093/jbcr/irad004
63. Gress K, Charipova K, Jung JW, et al. A comprehensive review of partial opioid agonists for the treatment of chronic pain. Best Pract Res Clin Anaesthesiol. 2020;34(3):449–461. doi:10.1016/j.bpa.2020.06.003
64. Daksla N, Wang A, Jin Z, Gupta A, Bergese SD. Oliceridine for the management of moderate to severe acute postoperative pain: a narrative review. Drug Des Devel Ther. 2023;17:875. doi:10.2147/DDDT.S372612
65. Wolf A, Unterberg M, Witowski A, Adamzik M, Wolf A. Efficacy, safety, and side effects of oliceridine in acute postoperative pain, a protocol for a systematic review and meta-analysis. PLoS One. 2024;19(2):e0299320. doi:10.1371/journal.pone.0299320
66. Liu Y, Hu Q, Yang J. Oliceridine for the management of acute postoperative pain. Ann Pharmacother. 2021;55(10):1283–1289. doi:10.1177/1060028020987679
67. Ni Y, Huang R, Yang S, et al. Pharmacokinetics and safety of oliceridine fumarate injection in Chinese patients with chronic non-cancer pain: a phase I, single-ascending-dose, open-label clinical trial. Drug Des Devel Ther. 2024;18:2729. doi:10.2147/DDDT.S461416
68. Goudra B, Mason KP. Emerging approaches in intravenous moderate and deep sedation. J Clin Med. 2021;10(8):1735. doi:10.3390/jcm10081735
69. Bazerbachi F, White RM, Forbes N, et al. Endo-anesthesia: a primer.
70. Goudra B, Singh PM. Oliceridine and its potential to revolutionize GI endoscopy sedation. Saudi J Anaesth. 2020;14(3):349. doi:10.4103/sja.SJA_813_19
71. Chao LJ, Lu S, liang FX, et al. Comparison of oliceridine to remifentanil for optimal analgesia in mechanical ventilation (CO-ROAM): study protocol for a multicenter randomized controlled trial. Pain Ther. 2024;13(6):1695. doi:10.1007/s40122-024-00669-4
72. Moss L, Hijma H, Demitrack M, et al. Neurocognitive effect of biased µ-opioid receptor agonist oliceridine, a utility function analysis and comparison with morphine. Anesthesiology. 2023;139(6):746–756. doi:10.1097/ALN.0000000000004758
73. Capone RL. Corrected supplement approval.
74. Simpson KN, Fossler MJ, Wase L, Demitrack MA. Cost-effectiveness and cost-benefit analysis of oliceridine in the treatment of acute pain. J Comp Eff Res. 2021;10(15):1107–1119. doi:10.2217/cer-2021-0107
75. Simpson KN, Fossler MJ, Wase L, Demitrack MA, Wandstrat TL. Budget impact and pharmacy costs with targeted use of oliceridine for postsurgical pain in patients at high risk of opioid-related adverse events. Expert Rev Pharmacoecon Outcomes Res. 2022;22(4):671–681. doi:10.1080/14737167.2022.2038137
76. Kliewer A, Schmiedel F, Sianati S, et al. Phosphorylation-deficient G-protein-biased μ-opioid receptors improve analgesia and diminish tolerance but worsen opioid side effects. Nat Commun. 2019;10:367. doi:10.1038/s41467-018-08162-1
77. Kliewer A, Gillis A, Hill R, et al. Morphine‐induced respiratory depression is independent of β‐arrestin2 signalling. Br J Pharmacol. 2020;177(13):2923–2931. doi:10.1111/bph.15004
78. Azevedo Neto J, Costanzini A, De Giorgio R, Lambert DG, Ruzza C, Calò G. Biased versus partial agonism in the search for safer opioid analgesics. Molecules. 2020;25(17):3870. doi:10.3390/molecules25173870
79. Gillis A, Gondin AB, Kliewer A, et al. Low intrinsic efficacy for G protein activation can explain the improved side effect profiles of new opioid agonists. Sci Signal. 2020;13(625):eaaz3140. doi:10.1126/scisignal.aaz3140
80. Stahl EL, Bohn LM. Low intrinsic efficacy alone cannot explain the improved side effect profiles of new opioid agonists. Biochemistry. 2021;61(18):1923. doi:10.1021/acs.biochem.1c00466
81. Bergese S, Berkowitz R, Rider P, et al. Low incidence of postoperative respiratory depression with oliceridine compared to morphine: a retrospective chart analysis. Pain Res Manag. 2020;2020:7492865. doi:10.1155/2020/7492865
82. Brzezinski M, Hammer GB, Candiotti KA, et al. Low incidence of opioid-induced respiratory depression observed with oliceridine regardless of age or body mass index: exploratory analysis from a phase 3 open-label trial in postsurgical pain. Pain Ther. 2021;10(1):457–473. doi:10.1007/s40122-020-00232-x
83. Beard TL, Michalsky C, Candiotti KA, et al. Oliceridine is associated with reduced risk of vomiting and need for rescue antiemetics compared to morphine: exploratory analysis from two phase 3 randomized placebo and active controlled trials. Pain Ther. 2021;10(1):401–413. doi:10.1007/s40122-020-00216-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.