")
Back to Journals » Patient Preference and Adherence » Volume 18
Participation and Compliance in a Multimodal Prehabilitation Program for Colorectal Cancer (PACE): A Qualitative Study
Authors Sier MA , Cox MPPJ , Tweed TT, Servaas N , Greve JWM, Stoot JHMB
Received 5 June 2024
Accepted for publication 11 November 2024
Published 30 December 2024 Volume 2024:18 Pages 2709—2720
DOI https://doi.org/10.2147/PPA.S481567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Misha AT Sier,1,2 Maud PPJ Cox,1,3 Thaís TTT Tweed,4 Nick Servaas,1,3 Jan Willem M Greve,1,3 Jan HMB Stoot1
1Department of Surgery, Zuyderland Medical Center, Heerlen, 6419 PC, The Netherlands; 2School of Nutrition and Translational Research in Metabolism (NUTRIM), Maastricht University, Maastricht, The Netherlands; 3Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, 6211 LK, The Netherlands; 4Department of Surgery, Maastricht University Medical Center+, Maastricht, 6229 hX, The Netherlands
Correspondence: Misha AT Sier, Department of Surgery, Zuyderland Medical Center, Henri Dunantstraat 5, Heerlen, 6419 PC, The Netherlands, Tel +31-6-40953595, Email [email protected]
Purpose: Interest in prehabilitation, the preoperative enhancement of patients’ condition, is rising in the surgical field. Challenging factors appear to be patients’ motivation to participate in and their compliance with prehabilitation programs. The aim of this qualitative study was to study the real-life experience of prehabilitation by assessing the lived experience and perceptions of participants in a multimodal prehabilitation program and to explore factors that influence participation and compliance during prehabilitation.
Methods: Patients who underwent surgery for colorectal cancer and who had participated in the 4-week multimodal prehabilitation program “BEFORE” feasibility study were recruited. Their lived experiences were collected through semi-structured, individual, in-depth interviews. Interviews were transcribed verbatim and analyzed using a thematical approach. As no new information emerged after the interviews, data were considered saturated.
Results: Six patients were interviewed. Seven main themes were discussed during the interviews, including information provision, motivation for participation, and content of the program. The results of this study emphasize the importance of adequate patient education, in-hospital exercise with the supervision of physiotherapists, and a patient-centered program. Logistical problems and the impact of cancer diagnosis were most frequently reported as barriers to participation.
Conclusion: Participation could be improved by providing adequate information and solving logistical issues. Patient-centeredness of the program is an important feature in improving adherence.
Keywords: participation, compliance, prehabilitation, colorectal surgery, colorectal cancer
Introduction
Prehabilitation is increasingly being used to reduce the relatively high complication rates (33%) after colorectal cancer surgery.1 The rationale behind prehabilitation is that preoperative enhancement of functional status limits deterioration of function during the peri- and postoperative period and contributes to fast recovery.2,3
Although various studies have been conducted on prehabilitation, only some of them provide evidence for a significant improvement in postoperative recovery.4–8 Several studies were underpowered to detect significant differences in these outcome measures due to small study samples, and the content of prehabilitation programs was largely heterogeneous.9 This hampers drawing conclusions about the effects of prehabilitation. To determine the effect of prehabilitation, a large study population has to be studied. To accomplish this, recruitment rates and patient compliance must increase as studies often reported difficulties in recruiting participants and their adherence. For colorectal cancer, the majority of patients (53%) are 70 years or older.10 Frail, elderly patients who are known to have decreased physical reserves and adaptive capacity at baseline,11,12 are the population of interest. Most often the program appeared to be too demanding for patients.13–15 Participation in prehabilitation programs requires discipline, flexibility, and intrinsic motivation,13,16–18 which pose practical and motivational challenges to these patients.
In Zuyderland MC, a trial was conducted to assess the feasibility of a prehabilitation program consisting of a 4-week supervised in-hospital, personalized exercise program combined with a nutritional intervention.19 In line with previous research, the problem of low recruitment rates occurred here as nine out of the 30 patients (30%) gave informed consent.9,19,20
Patients who have participated in prehabilitation programs are of great value in achieving higher recruitment and compliance rates as their lived experiences can identify factors that impede recruitment or compliance. Some previous studies evaluated patients’ perspectives regarding preoperative physical exercise only,7,16,21,22 while others did not contain the lived experiences of patients.6,23–25 The perspective of the patients who have participated in the prehabilitation program at Zuyderland MC is unique, given the nutritional intervention with fresh food in the multimodal program. The aim of this study was to study the real-life experience of prehabilitation by assessing the lived experience and perceptions of participants in the “BEFORE” multimodal prehabilitation program and to explore factors that influence participation and compliance during prehabilitation.
Materials and Methods
Study Design, Setting, and Participants
Based on the expectation that all participants experienced their participation in the prehabilitation program differently, coming from different environments with different backgrounds, a constructivist paradigm was used in designing the study.26 A phenomenological approach was used to explore patients’ experiences with the prehabilitation program, as it was the aim to look for the shared lived experiences of the patients with the program.
The study took place at Zuyderland Medical Center, a large teaching hospital based in the southern part of the Netherlands. Annually, approximately 200–250 patients are operated for colorectal cancer.
Patients who participated in the “BEFORE” feasibility study were eligible for inclusion.19 They were recruited through telephone contact. The “BEFORE” prehabilitation program consisted of a 4-week supervised in-hospital, personalized exercise program (three sessions a week, twelve in total), and nutritional intervention (three fresh protein-rich meals and three snacks every day).19 Of the nine patients who participated in the “BEFORE” feasibility trial, two had since died, resulting in a potential maximum study population of seven patients. As the study population was fairly homogeneous and as purposive as possible (all patients who participated in the “BEFORE” program) six to eight data units were considered to be sufficient for a homogenous sample.27,28 During data collection, regular evaluation was performed to determine whether data saturation had been reached.29
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval for this research was received from the local Medical Research Ethics Committee (METC Z). The study objective and voluntary nature of the study were explained to participants, and written informed consent was obtained before the interviews. This informed consent included consent to publication of anonymized responses. The audio recordings and transcripts were encrypted and stored securely. The Standards for Reporting Qualitative Research guidelines30 were followed throughout this study, see Supplementary Material.
Procedures
Face-to-face, one-on-one, semi-structured interviews were conducted at a time convenient for patients in one of the outpatient clinics of Zuyderland MC (Sittard-Geleen or Heerlen). With the participant’s permission, the interviews were audio-recorded. The interviewer (MC) was a sixth-year medical student, who performed an in-depth (systematic) literature study and spoke in advance with healthcare providers involved in the “BEFORE” feasibility study to become familiar with the topic.
Before the start of the data collection, a literature study was performed to identify important themes for patients’ participation in and adherence to prehabilitation. A semi-structured interview guide was created (see Table 1 for the shortened version of the interview guide). The extensive guide includes themes, subthemes, and open-ended opening questions for each main topic. The interview guide was gradually modified through an iterative process, adding themes and topics as they emerged during the interviews and analysis, see Table 1.
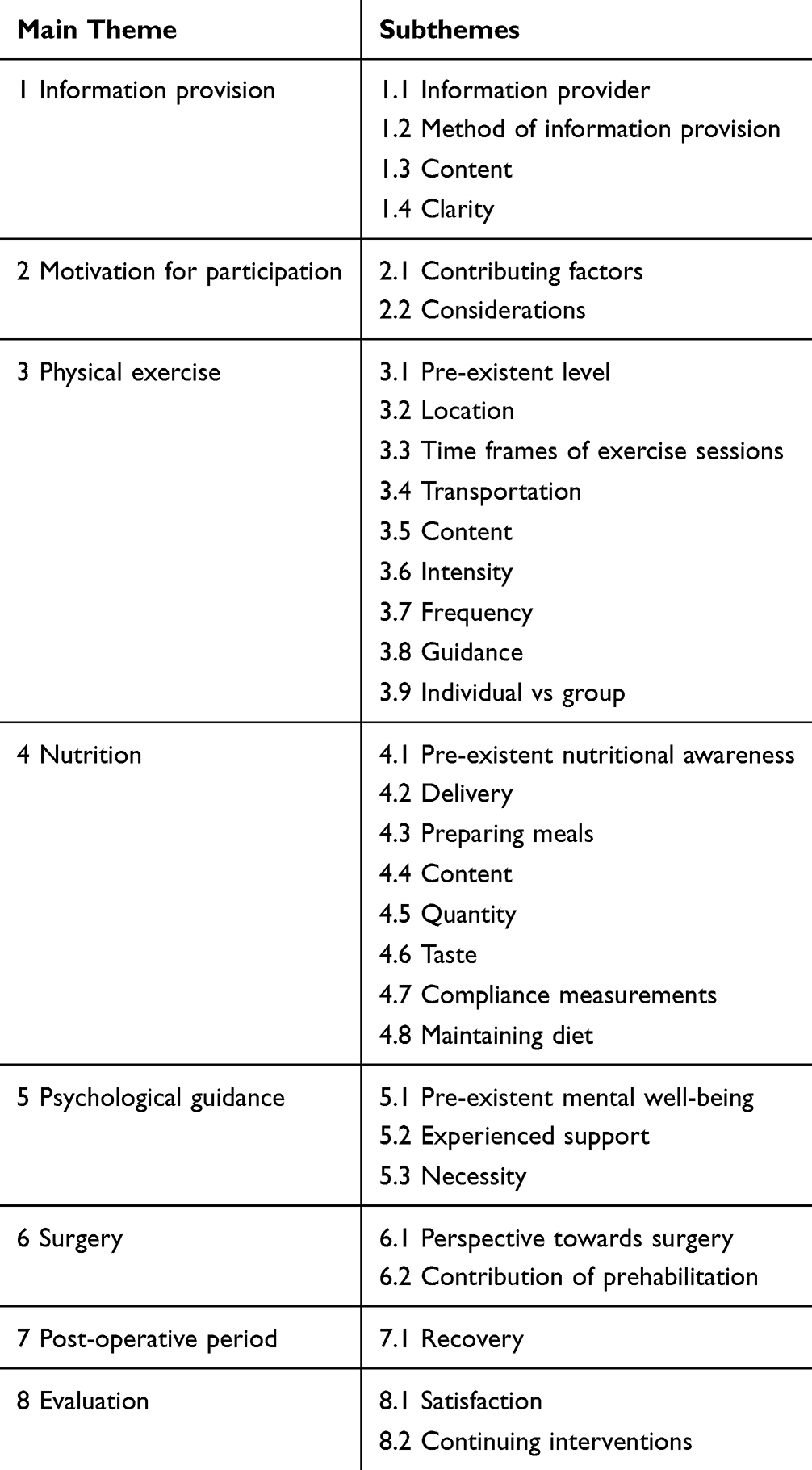 |
Table 1 Shortened Version of the Interview Guide |
A broad data-generating question was first used: “Please tell me about your experience with the prehabilitation program”. The following questions were open-ended, to obtain a detailed description of the different aspects of the prehabilitation program. Examples were: “What did you think of the information provision?”, “How did you experience the training sessions at the hospital?”. For each topic, follow-up questions were improvised based on patients’ responses to gain a deeper understanding.
Data collection occurred simultaneously with data analysis. The audio recordings were transcribed verbatim. In addition, notes on non-verbal cues and impressions were taken after the interview. A summary of the transcripts was sent by post to the participants to verify accuracy. Within one week, the participants were contacted by telephone to verify the accuracy of the transcript and if they had any additions.
To create an understanding of recruitment and compliance on the level of the patient population and assess both themes mentioned in literature and originated from lived experiences, reflexive thematic analysis was performed as described by Braun and Clarke.31 The transcripts were printed and coded manually. Without strictly defining codes beforehand, coding was performed in a predominantly deductive manner as the researchers focused on themes identified in previous studies.14,16,17 Likewise, theme development was directed by these themes. The coding was done independently by two researchers (MC, MS). After coding all six interviews, the results of both researchers were compared and discussed until a consensus was reached. Codes were analyzed to collate the different codes into initial themes and subthemes. After coding and re-reading all transcripts, these themes were evaluated and adjusted to define the final themes. The final coding template is shown in Table 2.
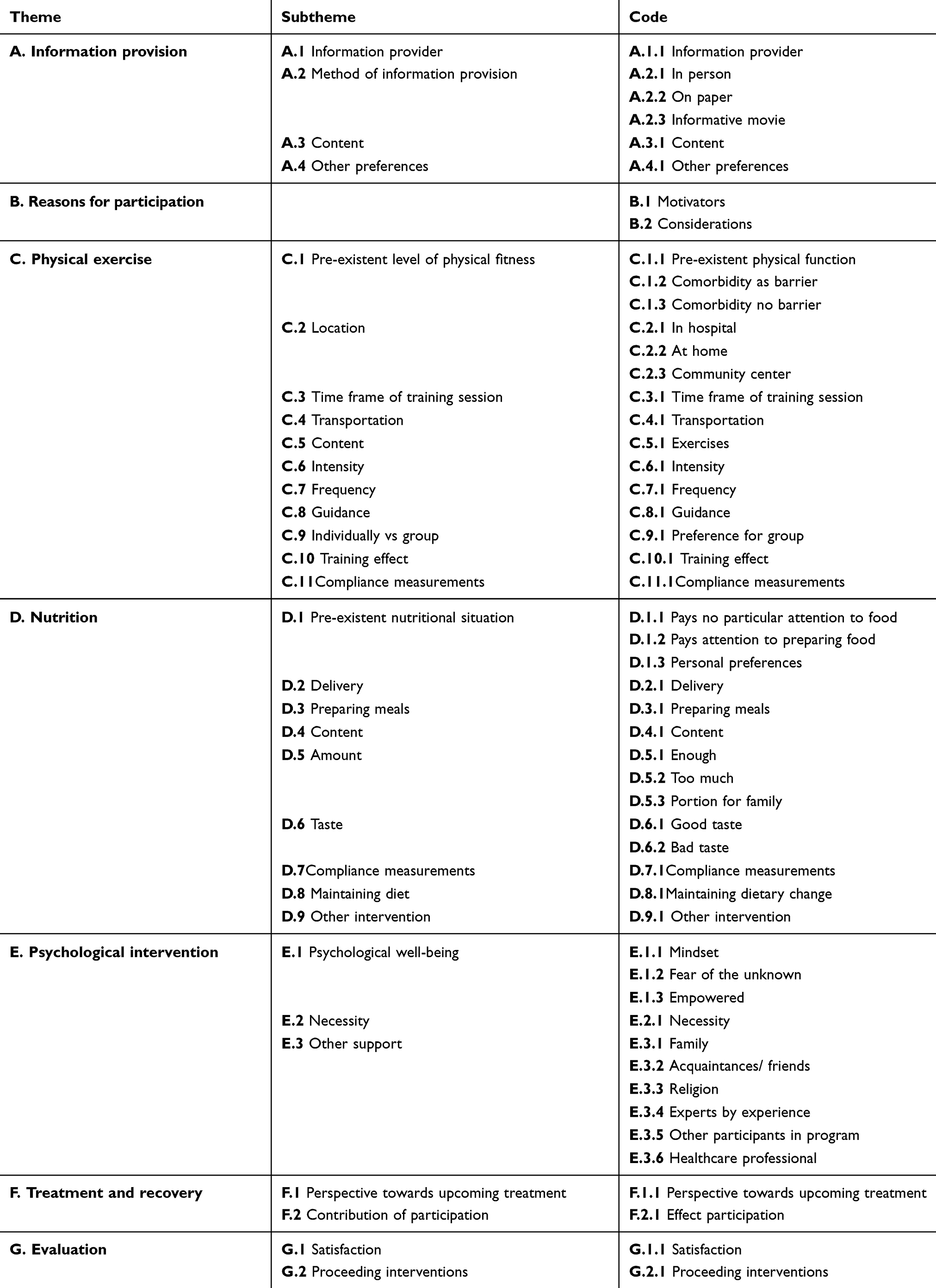 |
Table 2 Coding Template |
Results
Six out of seven patients eligible provided informed consent; one patient declined participation due to personal obligations, recruitment rate was 86%. Of the five interviews performed on-site, three were one-on-one. One interview was attended by a fellow researcher (MS), and during one interview her partner accompanied the patient because he had been involved in her prehabilitation. One patient was suffering from long-lasting post-COVID complaints and therefore could not come to the hospital. Oral informed consent was obtained, and the interview was conducted by telephone. For this interview, an abbreviated version of the interview was conducted in consultation with the patient. However, during the interview, no new themes emerged suggesting that data saturation had been reached.
Patient Characteristics
The baseline characteristics are shown in Table 3. Patients were between 72–77 years old, and an equal number of men and women participated.
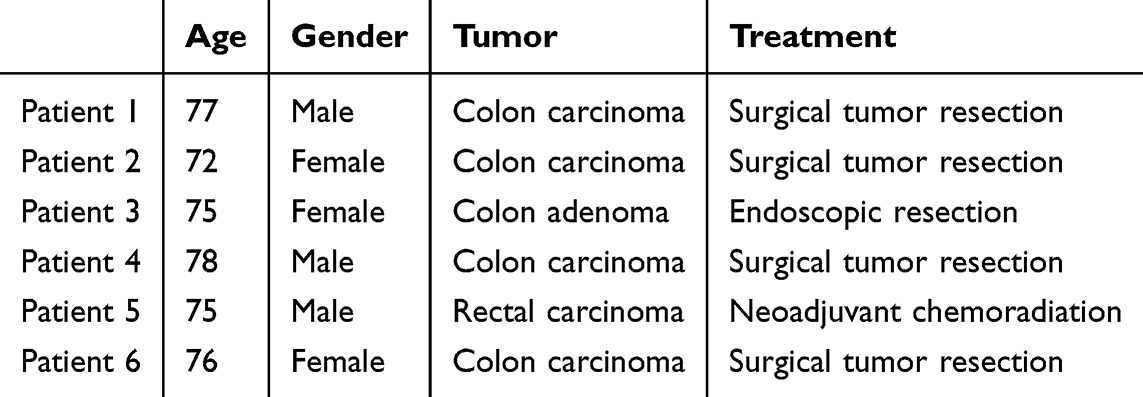 |
Table 3 Patient Characteristics |
The seven themes, as presented in the coding template (Table 2), formed the foundation for displaying the results.
Information Provision
Information about the “BEFORE” prehabilitation program was provided by telephone contact or in person during consultation with the surgeon or researcher. Patients unanimously preferred being recruited in person, as they felt these were pleasant and valuable encounters.
As patients received a lot of information after the cancer diagnosis, they preferred obtaining the information on paper as well. Three patients expressed the wish to bring an extra person with them to the consultation. The provided information was clear, hence most patients did not see any additional value in an informational video.
The doctor who was there. I don’t remember her name, but she was an excellent mentor. She also came every time to see if everything was all right. Yes, very kind. So I had a very positive experience with her. - Patient 3
The content of the information should at least consist of a clear explanation of the benefits of prehabilitation and a confirmation that participation will not delay treatment.
Yes, I had doubts about it, wouldn’t the surgery have been sooner if I didn’t have to sport all those weeks and consume the meals, right? Although it was mentioned in the letter this wasn’t the case; that you would have to wait those weeks until surgery anyway. - Patient 2.
One patient, who was recruited a little later, had a shorter prehabilitation period because he did not want to postpone surgery to prehabilitate for the full period.
The date has been set a long time ago, I hold on to it. I want that thing out of my body, I want to get rid of that tumor, I am not going to wait again. - Patient 4
Reasons for Participation
Patients were most motivated by the expected beneficial impact of prehabilitation on preoperative physical fitness and postoperative recovery. Getting through their treatment in the best way possible usually drove patients, and this program offered them the opportunity to play a role in their own recovery. This made them receptive to such an offer, especially when it was recommended by their healthcare professional.
[…] the intention is to join forces, to get stronger, to undergo surgery with a good feeling about it. - Patient 4.
Furthermore, patients were on the verge of entering an intense trajectory of cancer treatment. The ignorance of what would happen during treatment motivated the participants to take advantage of all available opportunities to help them get through it in the best possible way. Other factors that stimulated participation were the support of family, the fact that the program was free, having sufficient time to participate due to retirement, and previous experience with on-site rehabilitation.
Factors that were considered carefully before consenting to participate were the commitment that had to be made and the timespan of prehabilitation. The challenging aspect of the commitment was traveling to the hospital three times a week, apart from other hospital appointments.
Prehabilitation Program
I was talking to my children about it and they said ‘yeah mom, it would be good for you, for your endurance’. Especially since I have problems with my lungs. Yes, they both said ‘Mom, it would only be the best for you, because you are under good guidance and then you’ll at least be a bit stronger for the surgery’. - Patient 3
Physical Exercise
During the physical exercises, one patient perceived his comorbidity as a barrier. The other patients with comorbidities did not perceive this as a barrier and adjusted the exercises together with the physiotherapist if necessary. A notable characteristic of almost all patients was that they were already physically active to a certain extent in advance (eg gardening, walking the dog, physiotherapy, etc). All patients preferred an in-hospital exercise program, because of the expertise of the staff and the facilities available.
Yes, yes it [fitness center in the hospital] was at its finest. I think it’s a good location, good devices, good therapists, also I thought the guidance was excellent. - Patient 4
When assessing patients’ perspectives regarding other exercise locations, patients indicated that they had no confidence in a home-based exercise program due to the lack of supervision and the anticipation of constantly postponing the exercises. Furthermore, the patients with experience in physiotherapy in the community preferred the in-hospital training because, in their experience, physiotherapists in the community generally have less time, attention, and expertise.
Three sessions per week were sufficient for all patients. All patients preferred training on weekdays, in the morning or afternoon. The content of the exercise program, a circuit of several strength exercises and high-intensity exercises, can remain the same according to all patients. Some patients experienced the intensity as heavy in the beginning, but overall, it was manageable. They also reported the importance of the patients indicating themselves when exercises are too hard, as too demanding exercises could lead to non-compliance. Patients should be instructed to speak up because some might be afraid to do so.
Yes, and I think it’s important that it is mentioned, that when there is something you can’t manage: indicate it! So, they (patients) don’t keep muddling on and be sore afterward. - Patient 2
Transport to the hospital was not a problem for the patients who had a car and could drive themselves. However, two patients were dependent on others (eg family, neighbor) to bring them. They felt uncomfortable having to bother them. They stated that public transport is difficult for them, and the taxi is unreliable and expensive. They introduced the following solutions: providing a public transport description or organizing a shuttle service.
Patients were very satisfied with the guidance of the physiotherapists as the ratio of one physiotherapist per two to three patients implicated getting full attention, a sense of safety, and the approachability of therapists.
All patients preferred to exercise in a group of approximately three patients because it was sociable and motivational, and they could get in touch with fellow sufferers (some of them are still in touch). Patients were also motivated by the feedback on the progression they made, both during exercising and afterward at the final measurement with the sports and exercise physician.
I also went to the sports and exercise physician. And well he was surprised, that in such a short period of time, I made a lot of progress in physical condition on several aspects. - Patient 4
Most patients expressed that compliance could best be measured by the physiotherapists. They mentioned that several devices, like the bikes, automatically measured their performances and that they could also count the number of repetitions themselves. They did not see the need for or could think of other ways to measure compliance more accurately.
Nutrition
Patients’ opinions were mixed about the nutritional intervention, resulting in two perspectives. The first perspective reflected the satisfaction of patients who considered the nutrition to be tasteful and the provided boxes a great service. Others appreciated the efforts made but did not like the content and taste of the meals. Patients who stated in advance to be difficult eaters expressed the second vision most often. These patients did not consume the whole meal with all the required nutrition due to oversized portions. They shared the food with family or neighbors or stored it in their freezer.
It was way too much. We couldn’t finish the whole meal. So eh, so our neighbor also received a bit sometimes.. - Patient 4.
Furthermore, the compliance measurements (weighing the dishes before and after consumption, taking pictures of the meals before and after, and keeping a food diary for one week) were experienced as an extra burden. Although most patients did not find it difficult to perform, one patient stated that this was the least appealing part of the whole program. Nevertheless, participants could not think of more convenient ways to measure compliance.
It is an obligation, you have to do it very precisely. […] It’s not the easiest obligation. … It’s the same as saying ‘You have to fulfill three appointments each day’. - Patient 4.
Patients appreciated the well-organized delivery of the food boxes in the hospital after the exercise sessions, the easy preparation of the meals, and the extra portion that was provided for patients who had a family member who lived with them.
And if the patient gets home, to immediately start cooking and everything, it’s too much. And that’s why the food boxes were so ideal. - Partner of patient 2
Patients suggested improving adherence by allowing patients to fill in preferences regarding the content and quantity of meals. Also, medical conditions (such as diabetes) should be taken into account in the composition of the boxes. One patient, suffering from diabetes, would have preferred receiving a diet list rather than food boxes with contents he could not always consume.
Psychological Intervention
The “BEFORE” study did not contain a psychological intervention, but participants were asked how they would have felt about psychological support. All patients stated that this would be unnecessary for them, even though fear of the unknown was frequently brought up. Reasons that were mentioned for this were “not for me, maybe for others”, “an outsider could have never changed the way I felt at that time” and one patient implicated that a psychologist is only for patients with mental illnesses.
No, definitely not. No. That’s [psychological support] not necessary for me. No, it’s something you have to deal with yourself. - Patient 2
Two patients stated that it is a personal preference and therefore it should at least be offered. Other types of support were more important to them. Family support appeared the most important support, followed by support from acquaintances or friends, religion, medical experts, and fellow sufferers.
Yes indeed, the chemo, that was a heavy and difficult period. And sometimes you got to the point where my wife said, ‘Just quit’. On such a moment is actually your wife, your partner, is the psychologist. - Patient 4
Two patients would have preferred a conversation or extra time with their healthcare professional instead of a session with a psychologist. It was noted that all patients had one of the following characteristics: being realistic, positive-minded, and showing perseverance. This mindset could have affected their point of view.
Treatment and Recovery
Patients were asked what feeling they had when they entered their treatment after prehabilitation. One patient reported unawareness of the impact of surgery on physical well-being. Others reported that they felt more confident or better prepared to undergo surgery after prehabilitation. All patients who underwent surgery recovered quite fast, and a complication was rare. They were surprised by their fast recovery and acknowledged the contribution of prehabilitation to postoperative recovery. One patient did not think that the participation was connected to his fast recovery.
The day after, I already walked down the hallway and back, as they advised me. So, I assume that, if I hadn’t participated, it might have been harder to already be able to do that. That is possible. I can’t prove it. - Patient 4
The one patient that received neoadjuvant chemoradiotherapy (NACRT) reported withstanding the therapy very well. Therefore, he thought that he could have continued the prehabilitation during chemoradiation.
Several patients also marked their faith in their healthcare professional as an important factor.
Evaluation
Most patients would recommend others to participate in such a prehabilitation program and were very satisfied with it. It was stated several times that participation provided mental distraction and a sense of structure. Patients would do the physical exercise again, but some were unsure about the nutritional intervention or would not do it again.
Yes, I do recommend it. You can send them all to me (to convince them to participate). - Patient 4
Discussion
This study aimed to determine how to improve patients’ motivation to participate in prehabilitation programs and their compliance during prehabilitation. The results of this study emphasize the importance of eg adequate patient education, in-hospital exercise with supervision, and a patient-centered/tailored program. Most often, logistical problems and the impact of cancer diagnosis were reported as barriers to participation.
Consistent with the literature concerning information provision, the results point out the importance of informing patients adequately about the benefits of prehabilitation and clarifying that participation does not delay treatment.6,32–34 Reasons for participation were mostly comparable between the literature findings and interview results; the expected beneficial effect of prehabilitation is an important motivator.
The interviewed patients were all physically active and did not perceive their comorbidities as a barrier to prehabilitation. This finding differs from previous studies describing that pre-existential good physical fitness and comorbidities limit participation.5,6,8,16,17,32–39 A possible explanation for this may be the patients’ mindsets, as they all showed characteristics of perseverance.
In contrast to the literature findings, interviewed patients were satisfied with the in-hospital training circuit. Several studies recommended home-based prehabilitation or prescribing daily physical activities that are easy to perform and therefore could increase compliance.6,9,17,25,34,38,40 These differences may be explained by the fact that two of these studies explored patients’ vision, without patients having actually participated in a prehabilitation program.17,25 In the conducted studies patients could only reflect on the exercise program they received, thus the preference for home-based exercising or hospital-based training might be more anticipation rather than a preference due to the lack of experience. As high compliance rates were reported with an in-hospital exercise intervention,9 we recommend exploring ways to make this location more attractive for patients, for example, by offering a try-out training at an in-hospital fitness center or strategies to improve compliance on other training locations. The results underlining the importance of patient-centered exercising are consistent with literature findings,13,17,21,34,40,41 which entail personalization of the exercise program, offering group sessions, and providing feedback on progress.4,6,9,16,17,20,21,34 Solving transportation problems can increase both participation and compliance, eg shuttle bus provided by the hospital or exercise center.34,36–38,42–44
The fresh, protein-rich meals in our prehabilitation program were experienced differently. Literature findings regarding nutrition showed heterogeneity of the intervention and a lack of information about compliance and patient perspectives.6,8,40,43,45–52 The results implied that incorporating patients’ preferences regarding the content and size of meals could improve compliance. However, it remains unclear which type of nutritional intervention achieves the highest compliance.
Psychological support was not included in the “BEFORE” prehabilitation program. Although the literature is scarce and heterogeneous on compliance or patients’ perspectives concerning psychological interventions, both interviewed patients and the literature stated that psychological support for all patients is neither desired nor necessary.40,45,47–50 For some patients, other ways of support sufficed. Future research is needed to explore for whom psychological support is useful and in which form it provides the highest compliance rates.
Finally, there is a need for future trials to explore the effect of personalized prehabilitation programs on participation and compliance rates. Several studies recommend future trials to offer patient-centered interventions. However, to date, no feasibility trials with personalization of all prehabilitation modalities have been conducted. Results of this study suggest that a personalized prehabilitation program, in which patient preferences are taken into account as well, can increase participation and compliance rates. This, along with the other proposed modifications, needs to be evaluated in future research.
Limitations
The generalizability of the results is subject to certain limitations. First of all, the six patients who were interviewed all participated in the prehabilitation program. Consequently, there was a lack of perspectives of patients who declined participation. However, the reasons for non-participation were reported in the “BEFORE” feasibility trial.19 These reasons are similar to the barriers identified by the literature research. The study population, consisting of six patients, was small, but purposive. Another limiting factor was the long period (two years) between the prehabilitation and the interviews. As a consequence, some memories might have been hard to remember. Nonetheless, five out of six patients did not give the impression that memories were faded as they responded fast and elaborately to the posed questions. Furthermore, one interview was conducted in a shortened version, consequently, not all topics were covered, and answers were less detailed. Therefore, these two interviews might be less representative. The quality of the interviews might have been affected by the lack of specific training before conducting interviews. As the interviewer prepared extensively, this effect is considered to be minor.
Strengths
Despite these limitations, this study evaluated patients’ experiences profoundly. While studies often used questionnaires with prescribed answering options to evaluate their prehabilitation program, the one-on-one interviews allowed patients to extensively share their experiences. We observed a difference in results from the “BEFORE” evaluation form compared to the results obtained by the interviews.19 In some aspects, the results from the questionnaires were more favorable than the results of the interviews. This discrepancy could be attributed to the fact that the interviewer was independent of the previously performed feasibility trial. This might have given patients a sense of being able to share anything and to be critical. Due to the time between prehabilitation and the interviews, patients had time to properly reflect on their participation compared to when they filled in the questionnaires directly after completing the prehabilitation program.
Lastly, this research was strengthened by the fact that it addressed all intervention modalities of prehabilitation programs, instead of exercise only. The results demonstrated that relatively little is known about compliance to and patient perspectives on nutritional and psychological interventions. The perspective of the interviewed patients was unique because they received fresh protein-rich food while most programs offer dietary advice.
Conclusion
This present study was conducted to assess the lived experience and perceptions of participants in the “BEFORE” multimodal prehabilitation program and to explore factors that influence participation and compliance during prehabilitation. The participants reported that extensive and clear information contributed to their inclination to participate. The personalized, physical exercise program performed in-hospital with supervision was highly appreciated. Reported burdens were logistical issues and fixed meals in large portions. In order to improve participation and compliance, ensuring a feasible training location and personalized program for both physical exercise and food during prehabilitation seems important. Future research is necessary to establish the effects of these adjustments and determine the optimal nutritional and psychological interventions that achieve high compliance rates.
Data Sharing Statement
Data are available upon request from the first author (M.A.T. Sier).
Statement of Ethics
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Medisch-Etische Toetsingscommissie Zuyderland (METC Z) (Medical Research Ethics Committee (MREC) Zuyderland) (METCZ20210151/27-08-2021). Informed consent was obtained from all subjects involved in the study.
Acknowledgment
We thank all the study participants. We also thank Esther Bergman for her guidance in designing this study. In addition, we thank Marion Heymans for her assistance with the literature review and we thank the members of the prehabilitation team at Zuyderland Medical Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. JA Govaert, M Fiocco, WA Van Dijk. et al. Costs of complications after colorectal cancer surgery in the Netherlands: building the business case for hospitals. Eur J Surg Oncol. 2015;41:1059–1067.
2. Bruns ERJ, van Rooijen SJ, Argillander TE, et al. Improving Outcomes in Oncological Colorectal Surgery by Prehabilitation. Am J Phys Med Rehab. 2019;98(3):231–238. doi:10.1097/PHM.0000000000001025
3. Li C, Carli F, Lee L, et al. Impact of a trimodal prehabilitation program on functional recovery after colorectal cancer surgery: a pilot study. Surg Endosc. 2013;27(4):1072–1082. doi:10.1007/s00464-012-2560-5
4. Berkel AEM, Bongers BC, Kotte H, et al. Effects of Community-based Exercise Prehabilitation for Patients Scheduled for Colorectal Surgery With High Risk for Postoperative Complications: results of a Randomized Clinical Trial. Ann Surg. 2022;275(2):E299–E306. doi:10.1097/SLA.0000000000004702
5. Barberan-Garcia A, Ubré M, Roca J, et al. Personalised Prehabilitation in High-risk Patients Undergoing Elective Major Abdominal Surgery: a Randomized Blinded Controlled Trial. Ann Surg. 2018;267(1):50–56. doi:10.1097/SLA.0000000000002293
6. Chia CLK, Mantoo SK, Tan KY. ‘Start to finish trans-institutional transdisciplinary care’: a novel approach improves colorectal surgical results in frail elderly patients. Colorectal Dis. 2016;18(1):O43–O50. doi:10.1111/codi.13166
7. Soares SMTP, Nucci LB, da Silva MMC, Campacc TC. Pulmonary function and physical performance outcomes with preoperative physical therapy in upper abdominal surgery: a randomized controlled trial. Clin Rehabilitat. 2013;27(7):616–627. doi:10.1177/0269215512471063
8. EM Minnella, R Awasthi, SE Loiselle, et al. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: a Randomized Clinical Trial. Arch Surg. 2018;153:1081–1089.
9. Hijazi Y, Gondal U, Aziz O. A SYSTEMATIC REVIEW OF PREHABILITATION PROGRAMS IN ABDOMINAL CANCER SURGERY. International Journal of Surgery (London, England). 2017;39:156–162. doi:10.1016/j.ijsu.2017.01.111
10. IKNL.
11. Hoogeboom TJ, Dronkers JJ, Hulzebos EHJ, van Meeteren NLU. Merits of exercise therapy before and after major surgery. Curr Opin Anaesthesiol. 2014;27(2):161–166. doi:10.1097/ACO.0000000000000062
12. Minnella EM, Awasthi R, Gillis C, et al. Patients with poor baseline walking capacity are most likely to improve their functional status with multimodal prehabilitation. Surgery. 2016;160(4):1070–1079. doi:10.1016/j.surg.2016.05.036
13. Brunet J, Price J, Delluc C. An exercise trial for adults undergoing neoadjuvant chemoradiotherapy for rectal cancer proves not feasible: recommendations for future trials. Current Controlled Trials Cardiovas Med. 2021;22:26.
14. Agasi-Idenburg CS, Zuilen MK-V, Westerman MJ, et al. “I am busy surviving” - Views about physical exercise in older adults scheduled for colorectal cancer surgery. J Geriatric Oncol. 2020;11(3):444–450. doi:10.1016/j.jgo.2019.05.001
15. Morielli AR, Usmani N, Boulé N, et al. A Phase I Study Examining the Feasibility and Safety of an Aerobic Exercise Intervention in Patients With Rectal Cancer During and After Neoadjuvant Chemoradiotherapy. Oncol nurs forum. 2016;43(3):352–362. doi:10.1188/16.ONF.352-362
16. Sun V, Raz DJ, Kim JY, et al. Barriers and facilitators of adherence to a perioperative physical activity intervention for older adults with cancer and their family caregivers. J Geriatric Oncol. 2020;11(2):256–262. doi:10.1016/j.jgo.2019.06.003
17. Beck A, Vind Thaysen H, Hasselholt Soegaard C, Blaakaer J, Seibaek L. What matters to you? An investigation of patients’ perspectives on and acceptability of prehabilitation in major cancer surgery. Eur J Cancer Care. 2021;30(6):e13475–n/a. doi:10.1111/ecc.13475
18. West MA, Loughney L, Lythgoe D, et al. Effect of prehabilitation on objectively measured physical fitness after neoadjuvant treatment in preoperative rectal cancer patients: a blinded interventional pilot study. Br J Anaesth. 2015;114(2):244–251. doi:10.1093/bja/aeu318
19. Tweed TTT, Sier MAT, Van Bodegraven AA, et al. Feasibility and Efficiency of the “BEFORE” (Better Exercise and Food, Better Recovery) Prehabilitation Program. Nutrients. 2021;13(10):3493. doi:10.3390/nu13103493
20. Loughney L, Cahill R, O’Malley K, McCaffrey N, Furlong B. Compliance, adherence and effectiveness of a community-based pre-operative exercise programme: a pilot study. Perioperative Med. 2019;8(1):17. doi:10.1186/s13741-019-0126-y
21. Burke SM, West MA, Grocott MPW, Brunet J, Jack S. Exploring the experience of adhering to a prescribed pre-surgical exercise program for patients with advanced rectal cancer: a phenomenological study. Psychol Sport Exercise. 2015;16:88–95. doi:10.1016/j.psychsport.2014.09.005
22. Burke SM, Brunet J, Sabiston CM, et al. Patients’ perceptions of quality of life during active treatment for locally advanced rectal cancer: the importance of preoperative exercise. Support Care Cancer. 2013;21(12):3345–3353. doi:10.1007/s00520-013-1908-2
23. Karlsson E, Dahl O, Rydwik E, Nygren-Bonnier M, Bergenmar M. Older patients’ attitudes towards, and perceptions of, preoperative physical activity and exercise prior to colorectal cancer surgery—a gap between awareness and action. Support Care Cancer. 2020;28(8):3945–3953. doi:10.1007/s00520-019-05237-7
24. Kang D, Chung JY, Lee MK, et al. Exercise Barriers in Korean Colorectal Cancer Patients. Asian Pacific J Cancer Prevent. 2014;15(18):7539–7545. doi:10.7314/APJCP.2014.15.18.7539
25. Peeters C, Stewart A, Segal R, et al. Evaluation of a cancer exercise program: patient and physician beliefs. Psycho-Oncol. 2009;18(8):898–902. doi:10.1002/pon.1406
26. Bergman E, de Feijter J, Frambach J, et al. AM last page: a guide to research paradigms relevant to medical education. Acad Med. 2012;87(4):545. doi:10.1097/ACM.0b013e31824fbc8a
27. Holloway I, Wheeler S. in Qualitative Research in Nursing and Healthcare, Third Edition. Wiley; 2013.
28. Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers. Vol. XV. 2003.
29. Mason M. Sample size and saturation in PhD studies using qualitative interviews. Forum Qual Soc Res. 2010. 11(19–11):3.
30. O’Brien B, Harris I, Beckman T, Reed D, Cook D. Standards for Reporting Qualitative Research: a Synthesis of Recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
31. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
32. Moug SJ, Mutrie N, Barry SJE, et al. Prehabilitation is feasible in patients with rectal cancer undergoing neoadjuvant chemoradiotherapy and may minimize physical deterioration: results from the REx trial. Colorectal Dis. 2019;21(5):548–562. doi:10.1111/codi.14560
33. Heldens AFJM, Bongers BC, de Vos-Geelen J, van Meeteren NLU, Lenssen AF. Feasibility and preliminary effectiveness of a physical exercise training program during neoadjuvant chemoradiotherapy in individual patients with rectal cancer prior to major elective surgery. Eur J Surg Oncol. 2016;42(9):1322–1330. doi:10.1016/j.ejso.2016.03.021
34. Ferreira V, Agnihotram RV, Bergdahl A, et al. Maximizing patient adherence to prehabilitation:: what do the patients say? Support Care Cancer. 2018;26(8):2717–2723. doi:10.1007/s00520-018-4109-1
35. Karlsson E, Farahnak P, Franzén E, et al. Feasibility of preoperative supervised home-based exercise in older adults undergoing colorectal cancer surgery – a randomized controlled design. PLoS One. 2019;14(7):e0219158. doi:10.1371/journal.pone.0219158
36. Boereboom CL, Blackwell JEM, Williams JP, Phillips BE, Lund JN. Short‐term pre‐operative high‐intensity interval training does not improve fitness of colorectal cancer patients. Scand J Med Sci Sports. 2019;29(9):1383–1391. doi:10.1111/sms.13460
37. Suen M, Liew A, Turner JD, et al. Short‐term multimodal prehabilitation improves functional capacity for colorectal cancer patients prior to surgery. Asia-Pac J Clini Oncol. 2022;18(2):e103–e110. doi:10.1111/ajco.13564
38. Valkenet K, Trappenburg JCA, Schippers CC, et al. Feasibility of Exercise Training in Cancer Patients Scheduled for Elective Gastrointestinal Surgery. Digestive Surg. 2016;33(5):439–447. doi:10.1159/000445958
39. Morielli AR, Boulé NG, Usmani N, et al. Predictors of adherence to aerobic exercise in rectal cancer patients during and after neoadjuvant chemoradiotherapy. Psychol Health Med. 2018;23(2):224–231. doi:10.1080/13548506.2017.1344356
40. Scheede‐Bergdahl C, Minnella EM, Carli F. Multi‐modal prehabilitation: addressing the why, when, what, how, who and where next? Anaesthesia. 2019;74(S1):20–26. doi:10.1111/anae.14505
41. Huang GH, Ismail H, Murnane A, Kim P, Riedel B. Structured exercise program prior to major cancer surgery improves cardiopulmonary fitness: a retrospective cohort study. Support Care Cancer. 2016;24(5):2277–2285. doi:10.1007/s00520-015-3028-7
42. Northgraves MJ, Arunachalam L, Madden LA, et al. Feasibility of a novel exercise prehabilitation programme in patients scheduled for elective colorectal surgery: a feasibility randomised controlled trial. Support Care Cancer. 2020;28(7):3197–3206. doi:10.1007/s00520-019-05098-0
43. Macleod M, Steele RJC, O’Carroll RE, et al. Feasibility study to assess the delivery of a lifestyle intervention (TreatWELL) for patients with colorectal cancer undergoing potentially curative treatment. BMJ Open. 2018;8(6):e021117. doi:10.1136/bmjopen-2017-021117
44. Timmerman H, de Groot JF, Hulzebos HJ, et al. Feasibility and preliminary effectiveness of preoperative therapeutic exercise in patients with cancer: a pragmatic study. Physiother Theory Pract. 2011;27(2):117–124. doi:10.3109/09593981003761509
45. Waller E, Sutton P, Rahman S, et al. Prehabilitation with wearables versus standard of care before major abdominal cancer surgery: a randomised controlled pilot study (trial registration: NCT04047524). Surg Endosc. 2022;36(2):1008–1017. doi:10.1007/s00464-021-08365-6
46. Janssen TL, Steyerberg EW, Langenberg JCM, et al. Multimodal prehabilitation to reduce the incidence of delirium and other adverse events in elderly patients undergoing elective major abdominal surgery: an uncontrolled before-and-after study. PLoS One. 2019;14(6):e0218152. doi:10.1371/journal.pone.0218152
47. van Rooijen S, Molenaar CJL, Schep G, et al. Making Patients Fit for Surgery: introducing a Four Pillar Multimodal Prehabilitation Program in Colorectal Cancer. Am J Phys Med Rehab. 2019;98(10):888–896. doi:10.1097/PHM.0000000000001221
48. Gillis C, Li C, Lee L, et al. Prehabilitation versus Rehabilitation. Anesthesiology. 2014;121(5):937–947. doi:10.1097/ALN.0000000000000393
49. Bousquet-Dion G, Awasthi R, Loiselle S-È, et al. Evaluation of supervised multimodal prehabilitation programme in cancer patients undergoing colorectal resection: a randomized control trial. Acta oncologica. 2018;57(6):1–859. doi:10.1080/0284186X.2017.1423180
50. Minnella E, Ferreira V, Awasthi R, et al. Effect of two different pre-operative exercise training regimens before colorectal surgery on functional capacity: a randomised controlled trial. Eur J Anaesthesiol. 2020;37(11):969–978. doi:10.1097/EJA.0000000000001215
51. Yamamoto K, Nagatsuma Y, Fukuda Y, et al. Effectiveness of a preoperative exercise and nutritional support program for elderly sarcopenic patients with gastric cancer. Gastric Cancer. 2017;20(5):913–918. doi:10.1007/s10120-016-0683-4
52. Xu Y, et al. A Walk‐and‐Eat Intervention Improves Outcomes for Patients With Esophageal Cancer Undergoing Neoadjuvant Chemoradiotherapy. Oncologist. 2015;20:1216–1222.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.