")
Back to Journals » Journal of Pain Research » Volume 18
Patient Perceptions on Opioid Therapy for Acute Pain Management in the Emergency Department and Post-Surgical Settings: A Qualitative Study
Authors Lucey E , Dean E, Chapman BP, Perugini R, Chai P , Goldfine CE, Carreiro S
Received 12 February 2025
Accepted for publication 23 May 2025
Published 14 June 2025 Volume 2025:18 Pages 2961—2972
DOI https://doi.org/10.2147/JPR.S518088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Evan Lucey,1– 3 Erica Dean,1,2 Brittany P Chapman,1,2,4 Richard Perugini,5 Peter Chai,6– 9 Charlotte E Goldfine,6 Stephanie Carreiro1,2
1Department of Emergency Medicine, Division of Medical Toxicology, UMass Chan Medical School, Worcester, MA, USA; 2Tox(In)novation Lab, Worcester, MA, USA; 3University of New England College of Osteopathic Medicine, Biddeford, ME, USA; 4School of Physician Assistant Studies, Massachusetts College of Pharmacy and Health Science, Worcester, MA, USA; 5Department of Surgery, UMass Chan Medical School, Worcester, MA, USA; 6Department of Emergency Medicine, Division of Medical Toxicology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA; 7The Koch Institute for Integrated Cancer Research, Massachusetts Institute of Technology, Cambridge, MA, USA; 8Department of Psychosocial Oncology and Palliative Care, Dana Farber Cancer Institute, Boston, MA, USA; 9The Fenway Institute, Boston, MA, USA
Correspondence: Stephanie Carreiro, Department of Emergency Medicine, University of Massachusetts Medical School, 55 Lake Avenue North, Worcester, MA, 01655, USA, Email [email protected]
Purpose: Opioids are highly effective in treating acute pain but have various detrimental, non-therapeutic effects that may lead to the development of opioid use disorder (OUD) in certain individuals. This creates a complex landscape of opioid prescribing and use. The present manuscript uses a qualitative research lens to understand the patient experience during opioid therapy for acute pain, including perceptions, behaviors, and factors that drive both during the third wave of the opioid epidemic.
Patients and Methods: Patients receiving opioids for acute pain were recruited from the emergency department and general surgery clinic as part of a larger study to perform continuous physiologic monitoring during opioid use. Semi-structured interviews were conducted within 10 days of hospital discharge. Interviews were recorded, transcribed verbatim and subject to applied thematic analysis by two independent coders.
Results: Of the 60 subjects that completed the parent study, 44 completed the semi-structured interviews (mean age 47 years, 50% female). Three main themes emerged from the interviews: the direct effects of opioid analgesia, internal factors and external factors that influenced therapy. Symptoms of opioid tolerance, withdrawal and dependence were described in a subset of participants, even with a relatively short duration of therapy. Participants expressed a desire for more education around opioid therapy, and more engagement with their plan of care.
Conclusion: Opioid therapy, even in short courses for acute pain, can be a complicated experience for patients to navigate. Prescribers should consider how patients’ unique experiences and perspectives shape their responses when providing counseling to patients and monitoring of response to opioid therapy.
Keywords: analgesia, tolerance, stigma, post-surgical pain, goals and expectations
Introduction
Acute pain is a frequent reason for presentation to the emergency department (ED) and a nearly universal experience for post-surgical patients.1–3 Untreated and undertreated pain have been associated with increased morbidity and mortality, and reduced quality of life.4–7 Opioids are highly effective in treating acute pain but have various detrimental, non-therapeutic effects, including opioid use disorder (OUD) in a small but important fraction of patients.8–11
The opioid epidemic in the US has progressed in three waves, centering around prescription opioids starting in the 1990s, transitioning to illicit heroin in the mid 2000s, and recently being dominated by synthetic opioids.12 Once viewed as the key to alleviate suffering, opioids often now have a more negative connotation in the general population. This is primarily driven by personal experiences, those of close contacts, and the depiction of opioids in the media.13–15 In fact, previous experiences and attitudes concerning opioid use may outweigh information provided by clinicians.16
Along with the changes in public perception, the landscape of opioid prescribing practices by clinicians has also evolved.17 The current World Health Organization (WHO) analgesic ladder suggests that acute pain should be treated by employing the strongest opioid required to control pain and should be de-escalated once the cause of pain is resolved (eg dissipation of post operative pain).18 The opioid epidemic in the United States has led to cautious and conservative legislation, policy, and individual practices surrounding opioid prescribing.17 These may lead to unintended undertreatment of pain, and patient self-management of pain levels through other illicit opioids.17,19 Adequate treatment of acute pain is an important responsibility by the clinician but must be balanced with risks, including side effects, stigma, or perpetuation of OUD.20–27
Obtaining a deeper understanding of the patient’s perspective and exposure to opioid therapy is an important initial step in the effective therapeutic management of acute pain. Prior quantitative and qualitative studies have evaluated stigma, patient-provider experience, or fear of OUD in people receiving therapeutic opioids.2,28 Historical qualitative studies have interviewed patients scheduled to undergo knee replacement in the pre-operative (presumably pre-opioid) period, and patients treated for pain in the ED.13,29 However, there is a paucity of contemporaneous qualitative studies in the literature. The objective of the present study is to elicit formative perceptions of opioid therapy and pain among individuals receiving opioids for acute pain through the lens of the current wave of the opioid epidemic in the US, understand behaviors surrounding use, and explore factors that drive both.
Materials and Methods
Study protocols were approved by the UMass Chan Medical School Institutional Review board (Protocol ID H00013774). All study participants provided written informed consent prior to participation including for the publication of anonymized responses and direct quotes. This study was conducted in accordance with the Declaration of Helsinki.
General Study Overview
The purpose of this study was to analyze qualitative data specific to opioid analgesic therapy and pain through applied thematic analysis of the semi-structured interviews. This manuscript was drafted in accordance with the Standards for Reporting Qualitative Research (SRQR) guidelines (supplementary material section i).30
Qualitative data were obtained from a mixed-methods observational study completed at an urban academic medical center in New England. The parent study focused on wearable sensor-based monitoring of opioid use and the detection of dependence through physiologic data31. Study participants wore wearable sensors that continuously collected physiological data throughout the duration of opioid therapy, which included inpatient, nurse administered opioids and outpatient self-administered opioids if applicable. Upon completion of the physiological data collection period, each participant completed a standardized in depth semi-structured interview (supplementary material section ii) to probe themes related to using the sensor and their experience with opioid therapy32. Participants were compensated with $100 in retail gift cards for completing the entire study protocol (including the semi-structured interview).
Sampling and Data Collection Methods
Figure 1 provides an overview of the study recruitment criteria and flow. Recruitment took place between August 2016 and October 2021, and interviews continued until thematic saturation was reached. Potential participants were identified by screening an electronic ED tracking board and the outpatient surgical schedule. Study participants were never approached about the study or enrolled by a study team member who was involved in their clinical care. Participants were all at least 18 years of age and newly prescribed opioid analgesics for acute pain management (eg post-surgical pain or pain from an acute injury). Additional inclusion criteria were the ability to write and read English, and to provide informed consent. Criteria for exclusion were prisoner status, and pregnancy. Baseline data collection included demographic characteristics in addition to relevant historical information, including opioid use, chronic pain, psychiatric disorders, and substance use disorder (SUD). Opioid use was categorized as naive, occasional, or chronic using the following criteria. Participants without an opioid prescription within six months of study enrollment and without a history of OUD were classified as opioid naive. Chronic opioid use was classified as 1) prescribed maintenance opioids at baseline (ie, for chronic pain, medication assisted treatment; 2) actively using non-prescribed opioids at time of enrollment 3) history of OUD with less than five years of sustained recovery. The occasional opioid use classification was given to those who fell between naive and chronic criteria.
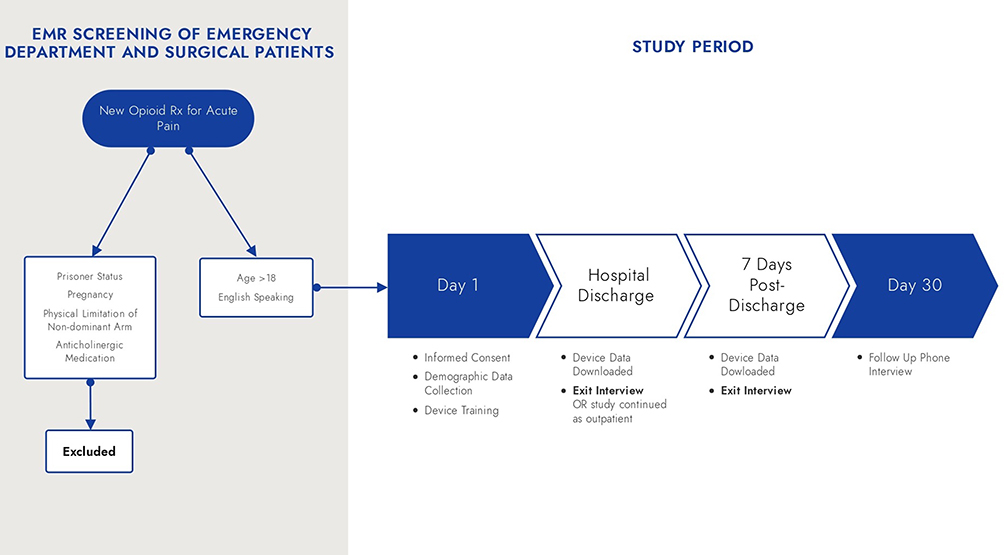 |
Figure 1 Study Flow Diagram. |
Participants completed a semi-structured exit interview either upon hospital discharge or 7–10 days post-discharge. Interviews were facilitated by two members of the research team (EL & BC) who were trained in qualitative interview techniques. Each interview was recorded, transcribed verbatim and deidentified. Specific to the scope of this paper, the interview guide consisted of open-ended questions that explored the physical and psychological effects of taking opioids, and the overall patient experience. Interviewers were permitted to ask related questions not listed on the interview guide to explore responses from the participant in more depth.
Data Analysis
Descriptive statistics (means/standard deviations, frequencies and percentages) were calculated for demographic data. To assess for potential bias in the sample, participants from the completion group (those from the parent study who completed the interview) were compared to those who did not (attrition group) based on demographics and treatment characteristics. Quantitative comparisons were also made for select demographic/clinical variables based on reported experiences (eg the experience of opioid withdrawal, report of opioid tolerance) to better contextualize findings. Continuous variables were compared using a t-test (if normally distributed) or a Kruskal–Wallis test (if not normally distributed). Categorical variables were compared using a Chi Square test or Fischer’s exact test. P values were reported for all hypothesis testing, and p value < 0.05 was consider significant.
Applied thematic analysis was chosen to allow for a systematic but flexible framework to interpret participant perceptions. This approach allowed us to identify meaningful patterns across the data, rather than test a specific hypothesis or generate a new theory. A coding structure was developed by the study team using the interview guide in addition to notable topics observed after transcript review. The initial coding structure was developed using deductive codes from the interview questions. However, after team members familiarized themselves with the data by reading through transcripts and reflection notes, the codebook was also supplemented with inductive codes generated through the review of transcripts. Each interview transcript was double coded independently by research staff (EL and BC) after training on the coding matrix by the principal investigator (SPC). After completion of independent coding, both coders collaborated and systematically resolved any discrepancies in coding for each interview transcript, any remaining discrepancies mediated by the principal investigator (SPC). The finalized codes were uploaded into NVivo qualitative analysis software (Version 12, Lumivero, Denver, CO, USA) for applied thematic analysis. Basic descriptive statistics (frequencies and percentages) were calculated for the number of participants who mentioned each code, and these were compared across two key demographics (sex a birth and opioid use history).
Results
Sample Demographics
Of the 60 participants that enrolled into the study, 44 completed a semi-structured exit interview upon the study’s conclusion (completion group) while 16 did not (attrition group). The completion group had a mean age of 47 years and was evenly split between male and female sex. Those in the completion group were more likely to be opioid naive (63.6%) at study enrollment compared to the attrition group (43.8%). Members of the attrition group were more likely to be male (62.5% vs 50%), fall within the chronic opioid use classification (43.8% vs 20.5%), have a history of SUD (78.6% vs 38.6%), and have a psychiatric diagnosis (81.2% vs 56.8%). However, only the difference in SUD history was statistically significant. Detailed demographic information of the completion group responders and the attrition group can be observed in Table 1.
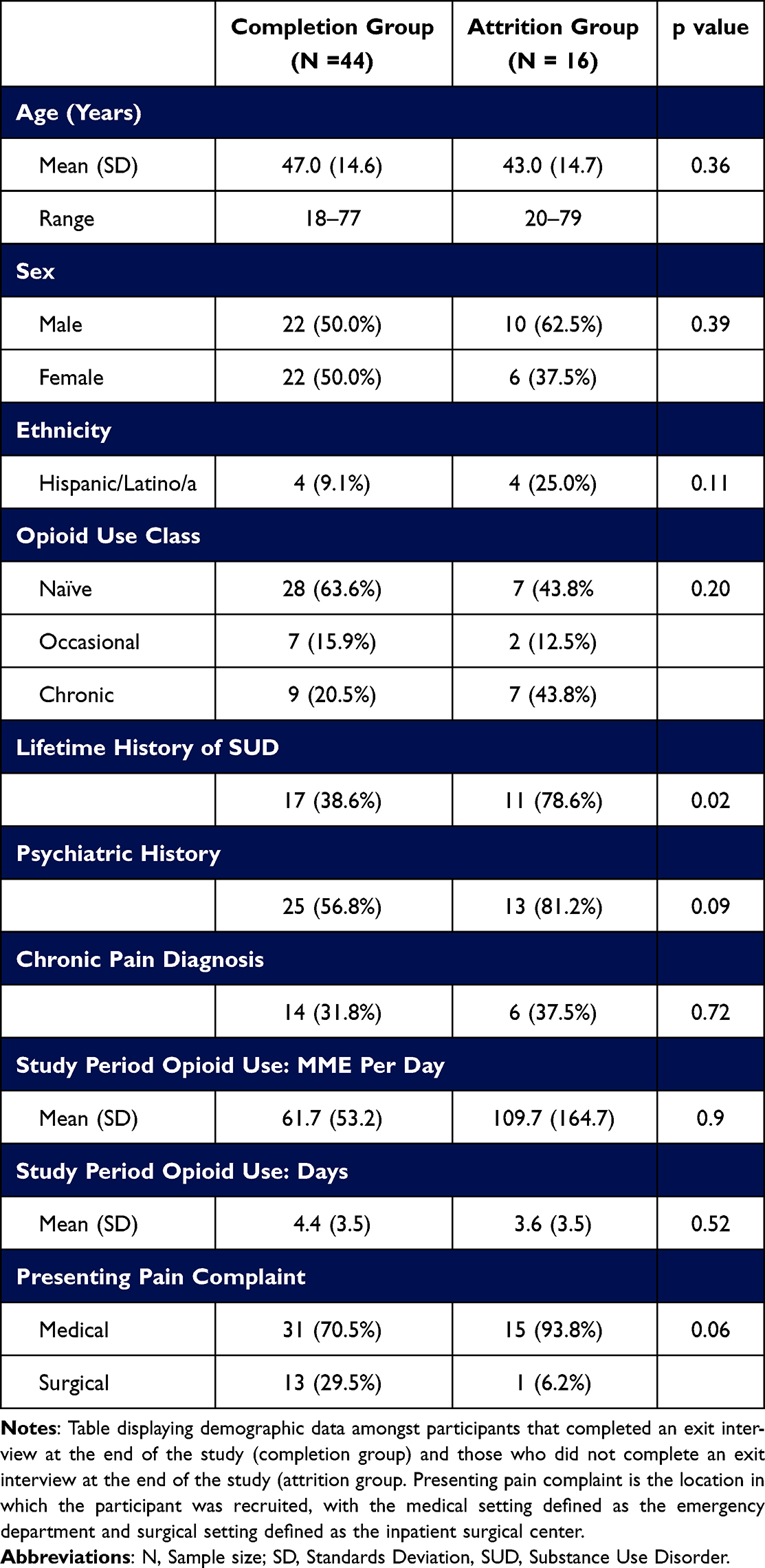 |
Table 1 Sample Demographics |
Applied Thematic Analysis
The qualitative analysis yielded three central themes. Table 2 summarizes the codebook, including the three emergent central themes, representative codes, code descriptions, and frequency of occurrence of each code (overall and by subgroups of sex and opioid use history). The first theme centered around the direct effect of opioids, with participants highlighting analgesia, euphoria, and a reduction in anxiety during opioid use, and symptoms of withdrawal after discontinuation. The second theme involved internal factors that influenced opioid therapy with participants expressing varying expectations, goals, and perceptions on the quantity of opioids prescribed to them for outpatient use. The third central theme centered on external factors that influenced opioid therapy, including prior experiences with prescription opioids and interactions with clinical staff.
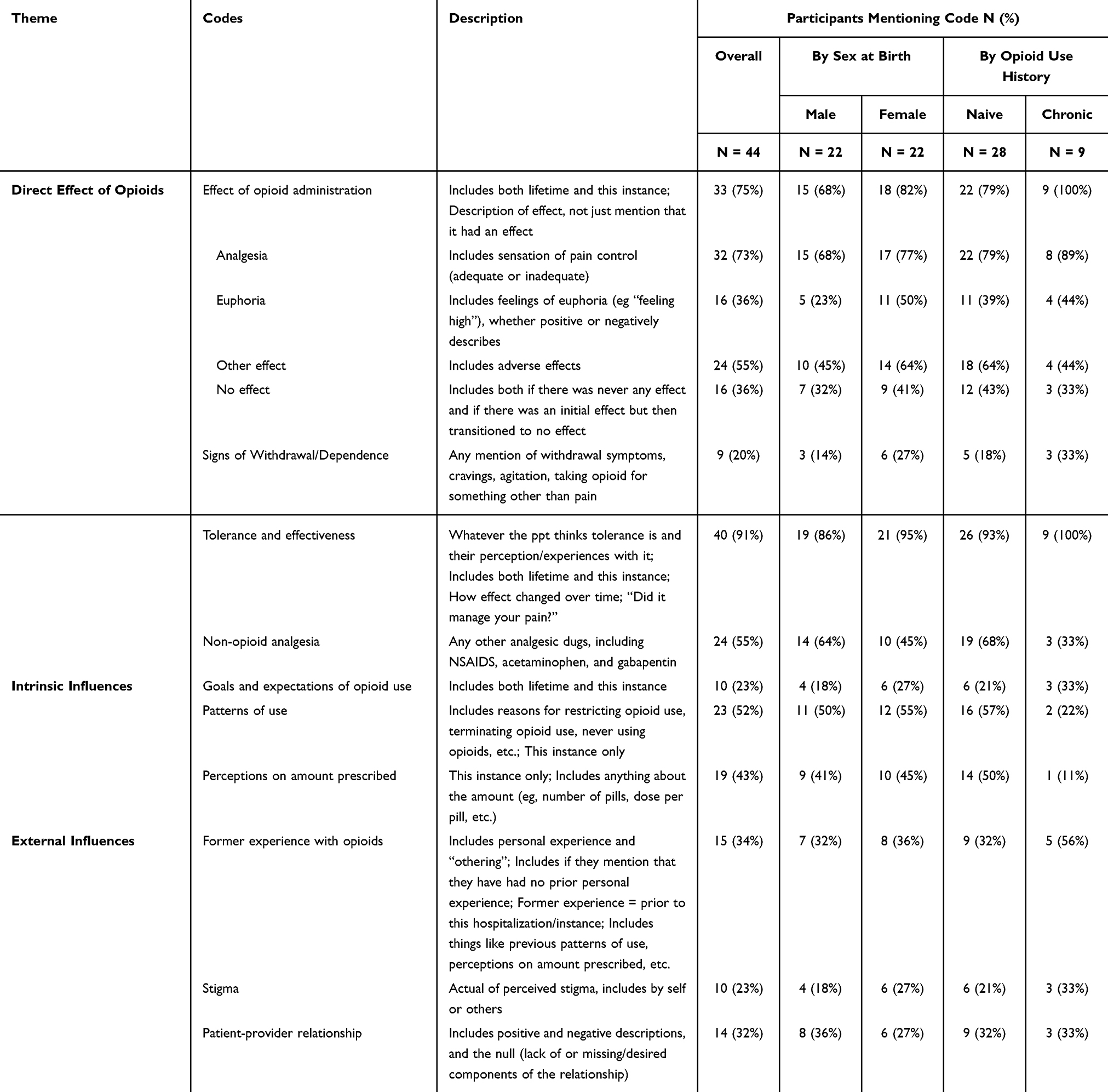 |
Table 2 Applied Thematic Analysis Codebook and Code Frequency: Overall and by Sex at Birth and Opioid Use History Classification |
Direct Effects of Opioids: Analgesia, Anxiolysis, Tolerance and Withdrawal
Participants observed differences in the onset of action, the degree of analgesia, and duration of oral versus intravenous (IV) opioid formulations. For most participants, the effects of IV opioids were felt almost instantaneously and were noted to be stronger, more effective for pain relief, and shorter lived when compared to oral opioids. Participants reported that IV opioids analgesia was more commonly accompanied by euphoria and cognitive effects, but most denied experiencing euphoria from oral opioids. When compared to NSAIDs, opioids were almost uniformly described to have stronger analgesic effects.
Opioids caused various other effects, with recurring themes involving anxiolysis, drowsiness, and subsequent withdrawal symptoms. While many participants stated that opioids had a relaxing effect, a few participants paradoxically experienced an increase in anxiety and energy. Nine participants described withdrawal symptoms in the days after cessation of opioid medications, including an increase in anxiety, agitation, headaches, night sweats, loss of appetite, and feeling more emotional. This was more commonly expressed in females (27%) and participants with a history of chronic opioid use (33%).
You’re, you’re, you’re craving more, so it’s kind of like I attribute it to like if I don’t have a cigarette for a few hours, kind of the same thing.– 35-year-old opioid naïve male
Participants who endorsed withdrawal symptoms has a slightly higher mean number of days of opioid use (5.3 days, SD = 3.4 vs 3.3 days, SD = 3.5) and MME per day (62.4, SD = 60.3 vs 61.5, SD = 51.9) than the overall study population. However, neither difference was statistically significant.
Other participants commented that they could see how opioids become addicting due to the euphoria they experienced.
…as quickly as it gave me relief, as quickly as it went through my body, and I needed more. And that’s what made me look back and say holy crap no I could see how people could be addicted. Because it was such a euphoric.– 41-year-old opioid naive female
I can see (how it can be addicting) because when the scripts gone, your like “aww, its gone”. Because you don’t have that feeling anymore of being high or anything.– 36-year-old opioid naive female
One of the participants quoted above, for example, considered calling their physician to refill the pain medication despite acknowledging that they were no longer in pain at the time.
Participant experience regarding perceived change in tolerance of varied. Most participants experienced adequate pain control throughout the course of therapy, however a subset of participants described a noticeable reduction in the ability of opioids to treat their pain effectively (N = 13). The decrease in effectiveness involved three recurring themes that suggest the development of tolerance: increased time to onset, less analgesia after the same dose, and a decreased duration of analgesia. Of the participants who reported developing tolerance or experiencing a reduction in opioid effectiveness over time, many found differences between IV and oral formulations. Participants described a slower change in tolerance while taking oral opioids, with notable changes occurring days to weeks after starting. In comparison, in the subset of participants that reported tolerance to IV opioids described a perception of tolerance in at little as 1–2 days.
Participants who endorsed ay symptoms of opioid tolerance has a higher mean number of days of opioid use (5.6 days, SD = 3.8 vs 2.9 days, SD = 3.1), higher MME per day (66.7, SD = 62.2 vs 61.3, SD = 58.1) and higher total number of doses (25.1 doses, SD = 22.9 vs 16. Doses, SD = 23.4) than those that did not. Only the number of days of therapy was statistically significant.
Intrinsic Influences: Goals and Expectations, Patterns of Use, and Perceptions of Amount Prescribed
Participants had varying goals and expectations of opioid therapy regarding analgesia: expectations ranged from complete elimination of pain to no effect. A minority desired just enough analgesia to maintain normal physical function and mobility. A few participants initially expected that the amount prescribed would be ineffective for treating their pain but ended up with satisfactory analgesia by the end of their outpatient treatment. Perceptions of effectiveness of inpatient and outpatient regimens differed: participants reported that their outpatient opioid regimen was unexpectedly weaker than what they received inpatient, resulting in failure to meet their ideal analgesic goals upon transition to an outpatient setting. Participants with a history of OUD (or other SUDs) had lower expectations of analgesia in general.
…some of the pain meds don’t work as well, they just take the edge off. But when you’ve abused it the way I have, I take responsibility for my own actions. I have to accept it and I’m willing to just settle for a little bit of the edge taken off.– 71-year-old female with a history of chronic opioid use and OUD
Analgesia was participants’ primary goal, but not their only goal. Approximately a quarter of participants discussed specific goals of opioid treatment, with females (27%) and people with a history of chronic opioid use (33%) providing more content in this area. Participants reported therapeutic goals beyond pain relief, with some participants reporting that they took the opioids to treat insomnia or agitation. When experiencing severe pain, many participants used opioids specifically to help them sleep and several participants exclusively used opioids at night because of the drowsiness. One participant stated that they tend to be restless at night and therefore took the opioid then to limit excessive movement that might reinjure the surgical site or cause pain. The primary use of opioids for some participants was to feel more relaxed even in the absence of significant pain reduction. Some participants reported feeling agitated after their surgical procedures and mentioned taking opioids primarily to “calm down”. One post-surgical participant stated that although they were not experiencing severe pain, they took the opioids to limit the agitation they were experiencing from dietary restrictions.
Participants utilized different dosing patterns and had different reasons for restricting or discontinuing use. Although opioids were always prescribed on an as needed basis, participants varied in their dosing strategy: some took a dose every 4–6 hours around the clock and others evaluated whether they felt they needed it or not. The most common reason for discontinuation was a decrease in pain levels that no longer required opioid therapy. A few participants stated that the opioids were no longer effective and therefore discontinued use. A minority of participants discontinued due to undesirable side effects, including a perception of “clouded judgment” and severe constipation. In the outpatient setting, many participants intentionally restricted the quantity of opioids they took citing fear of dependence. Several participants only used opioids prior to bed, most commonly to avoid daytime sleepiness.
Uhm, well I wasn’t really planning on taking any of the oxycodone’s in the first place so, the fact I even took any that first night, I was kind like ‘ah that sucks’. I don’t want to become dependent on them.– 26-year-old opioid naive male
Participants expressed various opinions on the amount they were prescribed. Most participants felt that the dose and number prescribed was adequate. More participants reported feeling like they were prescribed too many pills than too few. Of those who did not take any opioids, several did not fill their prescription: the most common reason was due to fear of addiction. Other stated reasons included perceived low levels of pain, religious beliefs, and personal history of alcohol use disorder (AUD). Two participants reported that their pain would have been better managed if they had requested additional opioids upon completion of the original prescription but opted not to request more due to fear of stigma and addiction.
Because I’m afraid of being dependent on it. I don’t want to depend on it, but when I reinjured myself, I felt like I needed more. But I won’t ask for it. It’s the fear, the stigma that comes with these medications that you’re like ‘no. I’m not going to do it, I’d rather be in pain because I don’t want to be a drug addict in the street’. That’s really what comes down to it.– 35-year-old opioid naive female
External Influences: Patient Provider Relationship, Stigma, Former Experience
Past experiences with opioids impacted current treatment. Just over one third of the participants discussed former experiences with opioids as an important driver in their current perceptions: this was similar in males and females (32% vs 38%) but was more common in people with a history of chronic opioid use compared to those who were opioid naive (56% vs 32%). There was a mix of past unique opioid experiences, including use for short term procedures, chronic use, and illicit use. One participant mentioned receiving poor treatment in the past by clinical staff for using methadone and having a history of substance use. One participant discussed transitioning from prescription opioid use to heroin use and was on methadone at the time of this study. Those that reported a history of prior illicit opioid use reported overall poorer pain control, but also a fear of speaking up about this. Another participant reported prior prescription opioid use for knee pain that transitioned to misusing the medication. This participant was subsequently denied opioid medication and continued to illegally obtain opioids from family and friends.
Perceived stigma around opioid use also impacted patients’ emotions on current use. Approximately one-quarter of the participants discussed stigma as an important factor in their perceptions: this was more common in females (27%) and individuals with a history of chronic opioid use (33%). Three participants believed they could have taken additional opioids for better pain management but did not due to the stigma associated with them. When asked for further about this topic, participants cited prior interactions with friends and relatives, and some associated any opioid use (even prescription use) with other illicit activities including injection drug use and prostitution.
I don’t want to be addicted to a drug, frankly… seen it happen to a good friend, you know?– 63-year-old opioid naïve male
Because I have seen girls that I know are only twenty, twenty-five at the most, look like they’re fifty-five prostituting out there because of the heroin….– 35-year-old opioid naive female
Several participants reported an element of fear of dependence and addiction as motivation to discontinue opioid prescription medications early. As an alternative perspective, a subset of participants engaged in othering, suggesting that other people may have trouble with opioids, saying “it’s all in their heads”. This suggestion of dependence or addiction as a sort of moral failing was projected on others and not onto themselves.
…I have experienced this many occasions in healthcare. I’ve seen patients think they need it and they are not actually in pain, it’s just all in their heads that they think they actually need it and their just addicted to it. And some people can’t pull themselves off of it and then there are other people that can pull themselves off and, you know, that are true to their word, and when they are in pain they are going to take that pain med.– 28-year-old opioid naive female
The concern of being labeled a “drug seeker” was prominent, particularly among those with a history of chronic opioid use. Participants who felt they were labeled in the past often refrained from requesting opioids out of fear of being labeled again. This was true for patients with history of OUD or other SUDs. One participant with a history of AUD refrained from asking clinical staff for any pain medication stronger than acetaminophen because they did not want to be labeled as “drug seeking” and chose to endure the pain instead. One participant was worried about being perceived as an addict if people discovered they were in an “opioid pain study”. One participant reinjured themselves but did not ask for additional opioids due to fear of becoming dependent and thought of as a “drug addict”.
… if you ask for more meds you’re labeled as either a seeker or something equally as lovely and I have a high pain threshold …so I just kind of sucked it up and took less.– 38-year-old opioid naive female
Participants desired more communication from providers around opioid use and sometimes felt pressure to use opioids. A subset of participants reported poor communication between the provider and themselves surrounding prescription opioid use. One participant was not informed of the side effects they may experience after discontinuing opioids and wished their physician had discussed withdrawal symptoms with them. An additional participant stated that they received no education of when they should take an opioid and how they would feel after they took it. Another participant, who was receiving 10 mg of oxycodone in the hospital and had a prescription for 5 mg of oxycodone outpatient, was not informed of this dose decrease and was frustrated with the perceived lack of communication. During inpatient care, one participant reported that clinical staff administered their opioids based on a set schedule and did not first consult the participant about their pain levels.
Experiences on the amount of opioid prescribed were heterogeneous, with some participants perceiving restricted prescribing, while others felt that opioid use was overly encouraged. Participants who felt that their physicians were restrictive in prescribing practices suspected that was due to fear of opioid misuse or liability. Participants noted concerns that individuals would seek illicit forms of opioids when physician’s discontinue opioid medications too quickly or are afraid to prescribe opioids at all. On the opposite end of the spectrum, other participants felt that opioid use was strongly encouraged by clinical staff regardless of the patient’s perceived need.
Discussion
Through qualitative interviews of 44 individuals receiving opioids for acute, non-cancer pain for a range of 1–14 days, several overarching themes emerged regarding how participants think about and use opioid analgesics. Even short course opioid therapy for acute pain management is a complicated experience, shaped by the perceived effects of the opioids, physiologic adaptations to the opioids (including tolerance and dependence), internal factors (including goals of therapy and behaviors) and external factors (including past experiences and interactions with clinical staff).
The direct effects of opioids during acute pain treatment were described homogenously among our study population. While IV opioids were described as having more rapid and effective analgesia, they were also described as inducing analgesic tolerance faster. A substantial number of participants (N = 13) described decreased analgesia from the same dose, a shorter duration of pain relief, and increased time to onset. Tolerance is a commonly described phenomenon with chronic opioid use, while the literature is conflicting about tolerance development short term.8,33 Some participants (N = 10) also reported increased anxiety, agitation, anorexia, night sweats, and heightened emotions (consistent with opioid withdrawal) upon discontinuation of opioids, even when the duration of use was relatively short. Others simply described using opioids for anxiolysis and insomnia, which raises the question of whether they were self-treating withdrawal symptoms. In some cases, symptoms were prominent enough to prompt requests for additional opioids after their prescription ended (in the absence of ongoing pain). Both tolerance and withdrawal were reported in participants with higher MME per day, longer durations on therapy and higher number of doses. But it is worth noting that they still were still experiencing these symptoms in a relatively short timeframes (around 5 days of therapy). These findings suggest that short term opioid use is not exempt from the development of tolerance and dependence.
We found that participants who had prior exposure to opioids, either from personal experience or through family, friends, or previous providers, may be more reluctant to treat their pain with opioids. Participants with prior experiences commonly associated prescription opioid use with a fear of becoming (or being labeled as) a “drug seeker”. This fear of SUD and becoming dependent on opioids sometimes resulted in early discontinuation (or refusal to initiate) of opioid medications and underreporting of pain. We found that the negative connotation surrounding opioid use continues to persist and influences treatment adherence. Discussion of stigma was more prominent in female participants, and those that had a history of chronic opioid use. These findings add to to the results described by other clinical studies, being that there commonly exist negative associations with prescription opioid use and SUD, and that these fears can influence a patient’s willingness to treat their pain.21,34 Anand et al described that perceptions of opioid therapy were influenced by first-hand experience or observations of illicit opioid use within their social circles, with patients who had friends or family with OUD being likely to have negative attitudes towards opioid therapy and to limit their use after a procedure.13
The decision of whether (or how) to take opioids is complicated, and there are numerous patient perspectives that physicians may not always consider. Communication with, and approval from, healthcare providers had substantial impact on participants opioid taking experiences. Participants reported a desire for more education from providers about opioids and potential side effects. Concern for being perceived as a “drug seeker” influenced their decision for whether and how to report pain, and whether to treat it. Additionally, regardless of how they perceived their providers’ communication, participants desired more engagement in decisions surrounding their analgesic plan. Some participants felt pressured by providers to take opioids when they did not desire to do so, both in the inpatient and outpatient setting. Of note, we did not directly measure the amount of content of education provided to participants in the hospital setting: it is possible that desired information was provided but not retained or was misinterpreted. Several comparable trends were found in a recent qualitative study following knee arthroscopy, observing that patients felt that better communication would have enhanced their expectations with opioid therapy.13 Another qualitative study by Smith et al following patients experiencing acute pain in the ED reported concerns about opioid dependence, and influence by prior knowledge from friends, family, and the media, which were consistent with our findings.29 This study also elicited common misconceptions around opioids, dependence, and “addiction”, such as participants believing that opioid misuse is a choice or a weakness.29 Our study reflected similar misconceptions, while adding perspectives on how quickly symptoms of tolerance and withdrawal are experienced, how stigma may be disproportionately experienced across groups, and patients’ desire for more dialogue and with their medical team surrounding opioid therapy.
Our study has many strengths, but we recognize several limitations. Our study sample size is relatively large for qualitative analysis compared to much of the existing literature. The larger sample size and semi-structured interview methodology allowed us to understand more variety and breadth in responses. However, of the 60 participants enrolled in the parent study, 16 did not participate in the interview, presenting the possibility for an attrition bias. Specifically, the study population has statistically lower percentage of individuals with a history of SUD (compared to the parent study sample) raising the possibility that this important group was underrepresented in our sample. The study population was recruited in a predominantly Caucasian population at a single tertiary care medical center in an urban New England area, limiting conclusions that can be drawn with other geographic and demographic samples. Identifying information of the participants was removed from the transcripts to best control for bias during the review process, nonetheless, the open-ended characteristics of the data could have created a mechanism for a reviewer to identify a participant based on their responses. Lastly, with many of the interview questions being related to opioids, their effects, and OUD, it is possible that participants may have catered their responses to be more socially acceptable to their interviewer.
Future work can expand on these findings by exploring other demographics and leveraging the results to create patient-centered treatment protocols. Triangulating self-report data with actual opioid use patterns and relevant outcomes (eg opioid misuse, development of OUD, development of chronic pain) would provide further insight into how reported effects and perceptions impact behaviors. Additionally, obtaining similar data from geographically and socioeconomically diverse populations may highlight key differences in patient populations. Educational initiatives including spaced repetition with material delivered in various formats, ongoing assessment of individual needs, and tailored educational plans should all be explored. Opioid tolerance, and perhaps more importantly, withdrawal should be proactively discussed, assessed, and addressed. Interventions that align analgesic protocols with patient values and goals, as well as ongoing evaluation of physiologic adaptations (eg tolerance and dependence) would allow for early identification and proactive mitigation of risk.
Conclusion
Opioid therapy, even in short courses, can be a complicated experience for patients to navigate. Participants in this qualitative study described internal and external factors in addition to the effects of the opioids themselves as influencing their behaviors and experience. Symptoms of opioid tolerance, withdrawal and dependence were described in a subset of participants, even with a relatively short duration of therapy. Participants expressed a desire for more education around opioid therapy, and more engagement with their plan of care, but also may be fearful of initiating discussion surrounding opioids due to perceived stigma. Prescribers should consider how patients’ unique experiences and perspectives shape their responses when providing counseling to patients and monitoring of response to opioid therapy. The variable and dynamic response to opioids over time suggests that education and engagement should be ongoing and should be tailored to the patient experience.
Funding
This work was generously supported by the NIH/National Institute on Drug Abuse (K23DA045242, PI: Carreiro and R25DA058490 MPI Carreiro/Chai).
Disclosure
Peter Chai reports grants from NIDA, during the conduct of the study; grants from Gates Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Cordell WH, Keene KK, Giles BK, Jones JB, Jones JH, Brizendine EJ. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165–169. doi:10.1053/ajem.2002.32643
2. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesthesia Analg. 2003;97(2):534–540. doi:10.1213/01.ANE.0000068822.10113.9E
3. McCaig LF, Nawar EW. National hospital ambulatory medical care survey: 2004 emergency department summary. Adv Data. 2006;1–29.
4. Forst J, Wolff S, Thamm P, Forst R. Pain therapy following joint replacement.A randomized study of patient-controlled analgesia versus conventional pain therapy. Arch Orthop Trauma Surg. 1999;119(5–6):267–270. doi:10.1007/s004020050407
5. Matot I, Oppenheim-Eden A, Ratrot R, et al. Preoperative cardiac events in elderly patients with Hip fracture randomized to epidural or conventional analgesia. Anesthesiology. 2003;98(1):156–163. doi:10.1097/00000542-200301000-00025
6. Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;11(12):1859–1871. doi:10.1111/j.1526-4637.2010.00983.x
7. Sborov KD, Dennis BM, de Oliveira Filho GR, et al. Acute pain consult and management is associated with improved mortality in rib fracture patients. Reg Anesth Pain Med. 2022;47(10):643–648. doi:10.1136/rapm-2022-103527
8. Nafziger AN, Barkin RL. Opioid therapy in acute and chronic pain. J Clin Pharmacol. 2018;58(9):1111–1122. doi:10.1002/jcph.1276
9. National Academies of Sciences E, Medicine. Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use. Washington, DC: The National Academies Press; 2017.
10. Kosten TR, George TP. The neurobiology of opioid dependence: implications for treatment. Sci Pract Perspect. 2002;1(1):13–20. doi:10.1151/spp021113
11. Zanza C, Romenskaya T, Zuliani M, et al. Acute traumatic pain in the emergency department. Diseases. 2023;11(1):45. doi:10.3390/diseases11010045
12. Ciccarone D. The triple wave epidemic: supply and demand drivers of the US opioid overdose crisis. Int J Drug Policy. 2019;71:183–188. doi:10.1016/j.drugpo.2019.01.010
13. Anand A, Roche D, Wright SR, Tjong VK, Rana JK, Abouali J. A qualitative assessment of perceptions and attitudes toward postoperative pain and opioid use in patients undergoing elective knee arthroscopy. Can J Surg. 2022;65(4):E440–e6. doi:10.1503/cjs.004321
14. Do U, El-Kefraoui C, Pook M, et al. Feasibility of prospectively comparing opioid analgesia with opioid-free analgesia after outpatient general surgery: a pilot randomized clinical trial. JAMA Network Open. 2022;5(7):e2221430. doi:10.1001/jamanetworkopen.2022.21430
15. McGinty EE, Stone EM, Kennedy-Hendricks A, Barry CL. Stigmatizing language in news media coverage of the opioid epidemic: implications for public health. Prev Med. 2019;124:110–114. doi:10.1016/j.ypmed.2019.03.018
16. Dolan AR, Goldberg EB, Cannuscio CC, et al. Patient perceptions about opioid risk communications within the context of a randomized clinical trial. JAMA Network Open. 2022;5(8):e2227650. doi:10.1001/jamanetworkopen.2022.27650
17. Manchikanti L, Singh VM, Staats PS, et al. Fourth wave of opioid (Illicit Drug) overdose deaths and diminishing access to prescription opioids and interventional techniques: cause and effect. Pain Physician. 2022;25(2):97–124.
18. Anekar AA, Hendrix JM, Cascella M. WHO analgesic ladder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024
19. Cohen SP, Hooten WM. Balancing the risks and benefits of opioid therapy: the pill and the pendulum. Mayo Clin Proc. 2019;94(12):2385–2389. doi:10.1016/j.mayocp.2019.10.006
20. Cogan J, Ouimette MF, Vargas-Schaffer G, Yegin Z, Deschamps A, Denault A. Patient attitudes and beliefs regarding pain medication after cardiac surgery: barriers to adequate pain management. Pain Manag Nurs. 2014;15(3):574–579. doi:10.1016/j.pmn.2013.01.003
21. Conrardy M, Lank P, Cameron KA, et al. Emergency department patient perspectives on the risk of addiction to prescription opioids. Pain Med. 2016;17(1):114–121. doi:10.1111/pme.12862
22. Greer SM, Dalton JA, Carlson J, Youngblood R. Surgical patients’ fear of addiction to pain medication: the effect of an educational program for clinicians. Clin J Pain. 2001;17(2):157–164. doi:10.1097/00002508-200106000-00008
23. Juprasert JM, Obeid L, Yeo HL. Public perception on opioids & pain management after major surgery. Am J Surg. 2022;223(2):280–286. doi:10.1016/j.amjsurg.2021.03.044
24. Lewis ET, Combs A, Trafton JA. Reasons for under-use of prescribed opioid medications by patients in pain. Pain Med. 2010;11(6):861–871. doi:10.1111/j.1526-4637.2010.00868.x
25. Moskovitz BL, Benson CJ, Patel AA, et al. Analgesic treatment for moderate-to-severe acute pain in the United States: patients’ perspectives in the physicians partnering against pain (P3) survey. J Opioid Manag. 2011;7(4):277–286. doi:10.5055/jom.2011.0069
26. Punches BE, Brown JL, Soliman S, et al. Patient pain experiences and the emergency department encounter: a qualitative analysis. Pain Manag Nurs. 2022;23(4):391–396. doi:10.1016/j.pmn.2022.03.012
27. Tanabe P, Buschmann M. A prospective study of ED pain management practices and the patient’s perspective. J Emerg Nurs. 1999;25(3):171–177. doi:10.1016/S0099-1767(99)70200-X
28. Bulls HW, Hoogland AI, Craig D, et al. Cancer and opioids: patient experiences with stigma (COPES)-A pilot study. J Pain Symptom Manage. 2019;57(4):816–819. PMID: 30703463; PMCID: PMC6433506. doi:10.1016/j.jpainsymman.2019.01.013
29. Smith RJ, Rhodes K, Paciotti B, Kelly S, Perrone J, Meisel ZF. Patient perspectives of acute pain management in the era of the opioid epidemic. Ann Emergency Med. 2015;66(3):246–252. doi:10.1016/j.annemergmed.2015.03.025
30. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
31. Chapman BP, Gullapalli BT, Rahman T, Smelson D, Boyer EW, Carreiro S. Impact of individual and treatment characteristics on wearable sensor-based digital biomarkers of opioid use. NPJ Digital Med. 2022;5(1):123. doi:10.1038/s41746-022-00664-z
32. Chapman BP, Lucey E, Boyer EW, Babu KM, Smelson D, Carreiro S. Perceptions on wearable sensor-based interventions for monitoring of opioid therapy: a qualitative study. Front Digital Health. 2022;4. doi:10.3389/fdgth.2022.969642
33. Collett BJ. Opioid tolerance: the clinical perspective. Br J Anaesth. 1998;81(1):58–68. PMID: 9771273. doi:10.1093/bja/81.1.58
34. Chavez MN, Tyson DM, Lake PW, et al. ‘They say you can get addicted’: exploring factors that fuel the fear of addiction to prescription opioids among cancer survivors. Eur J Cancer Care. 2022;31(3):e13582. PMID: 35354227. doi:10.1111/ecc.13582
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.