")
Back to Journals » Drug Design, Development and Therapy » Volume 19
PCOS and Inositols – Advances and Lessons We are Learning. A Narrative Review
Authors Lentini G , Querqui A, Monti N, Bizzarri M
Received 25 February 2025
Accepted for publication 6 May 2025
Published 21 May 2025 Volume 2025:19 Pages 4183—4199
DOI https://doi.org/10.2147/DDDT.S524718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Guglielmo Lentini, Alessandro Querqui, Noemi Monti, Mariano Bizzarri
Department of Experimental Medicine, Space Biomedicine Laboratory, University Sapienza, Rome, Italy
Correspondence: Mariano Bizzarri, Email [email protected]
Introduction: This Expert Opinion covers recent updates in the use of Inositol in polycystic ovary syndrome (PCOS), highlighting the specific effects triggered upon ovarian steroidogenesis.
Areas Covered: An impressive body of evidence, obtained from molecular, animal and clinical studies, demonstrated the striking association between PCOS and the metabolism of myo-Inositol (myo-Ins) and its isomer D-Chiro-Inositol (DCI). Early investigations focused primarily on the metabolic consequences of inositol in modulating insulin transduction. However, recent advances disclosed that Inositols trigger direct effects on steroidogenesis. High DCI levels exacerbate androgen synthesis, and downregulate aromatase expression. Myo-Ins modulates insulin effects too, but exerts opposite actions on steroidogenesis, by increasing aromatase and FSH receptor expression. Clinical studies demonstrated myo-Ins efficacy, suggesting that an appropriate ratio in between myo-Ins/DCI (40:1) improves the reproductive function in PCOS women, even in absence of insulin resistance.
Expert Opinion: Inositol-based treatments in PCOS are gaining momentum, demonstrating safety and efficacy greater than those obtained with other pharmacological agents. The efficacy depends not only on the modulation of insulin sensitivity but also on the direct, steroidogenic effects upon the ovaries. Adequate adsorption of Inositol is a critical issue, and the association of α-Lactalbumin can significantly overcome this problem. However, if a treatment based on inositol could be equally effective on different phenotypes of PCOS needs a specific assessment.
Plain Language Summary: Myo-inositol (myo-Ins) and D-chiro-inositol (DCI) are two isomers of inositol playing a key role in insulin signaling throughout the body, mainly through their phosphoglycan derivatives. They act as important regulators of hormone production within the ovaries, modulating steroidogenesis.Molecular and clinical studies showed that myo-Ins enhances FSH and aromatase activity, while DCI stimulates androgenesis in the theca. These isomers seem to have opposite, yet complementary, actions upon ovarian function. In the last decades, inositols have emerged to treat Polycystic Ovary Syndrome (PCOS), one of the most common benign ovarian disorders affecting young, fertile women.Myo-Ins/DCI ratio in the blood averages 40:1, and this parameter has been used as a basis for establishing a pharmacological formula. Treatments based according to this ratio showed to be successful in the management of several symptoms and signs of PCOS. This is particularly evident in obese patients, whereby the low doses of DCI help in counteracting insulin resistance.Further extensive research, both at the molecular and clinical levels, is needed to better understand inositol biology in mammals. In particular, it should be clarified how myo-inositol modulates the nuclear steroidogenic factor-1 (SF-1) and other key enzymes involved in steroid production. This could be done through epigenetic modifications.
Keywords: (polycystic ovary syndrome), PCOS, myo-Inositol, D-chiro-inositol, insulin resistance, hyperandrogenism, aromatase
Introduction: A Matter of Definition
Polycystic ovary syndrome (PCOS) is the most common endocrine disease in women of reproductive age. Identified by Stein and Leventhal in 1935,1 PCOS is one of the major causes of infertility overall, affecting 10–20% of infertile couples.2,3 However, the epidemiological incidence depends on the diagnostic criteria adopted and shows significant fluctuations: from 4–8% according to NIH/NICHD parameters, to 18–20% according to the Rotterdam criteria.4 Noticeably, incidence rate diverges dramatically among different countries – reflecting differences in genetic background and in exposure to environmental/dietary factors – showing an increasing trend in the last ten years.5 This picture is not unexpected, since PCOS is a syndrome (from the Greek σύνδρOμOν, meaning “concurrence”), ie set of medical signs and symptoms, which correlate with each other but that recognizes different pathogenic causes and mechanisms. The convergence of different «causative» factors – interacting each other accordingly to a non-linear dynamic – helps in explaining the nosological intricacies emerging in recognizing a proper definition, as acutely pointed out by Netter et al, who stated «the syndrome of Stein is a fugitive syndrome, with limits less well defined than those of the Sahara or the Sudan».6
Thereby, the epidemiological differences noticed in PCOS phenotypes and incidence can reflect differences in the pathogenic causes too. Interestingly, the overall epidemiological burden shows a significant worldwide increase from 1990 to 2019 (+54%),7 reflecting that environmental cues and changes in lifestyles likely play a relevant role. Moreover, the intricate participation of distinct pathogenic factors can help explaining a major issue, ie the presence of four clinical phenotypes, identified by clusters of biochemical signs and symptoms. According to Rotterdam Criteria,8 patient must present with at least two out of three major features: Ovulatory Dysfunction (OD), Hyperandrogenism (HA) and Polycystic Ovary Morphology (PCOM). Partitioning PCOS patients according to these principles resulted in the identification of four distinct phenotypes, namely A, B, C, and D (Table 1). Most frequent characteristics include hyperandrogenism with ovarian dysfunction, chronic oligo-anovulation, and/or polycystic morphology of the ovary. The androgenic phenotype is associated with more severe metabolic complications and it is even more resistant to conventional treatments.9 On the contrary, the PCOS phenotype deprived of HA has a lower risk of metabolic alterations and shows a better prognosis. However, the identification of the four Rotterdam phenotypes has not led to personalized treatments until now. Moreover, Rotterdam criteria do not include insulin resistance, a feature exhibited by the majority of women with PCOS.10 Overall, these considerations have prompted to reconsider the meaning of the syndrome, paving the way to a reinterpretation of the basic pathogenetic mechanisms as a key for establishing an appropriate, tailored treatment.11 Indeed, such issue enables to put in the right place the advancement performed in basic research during the last decades, namely by integrating genetic, biochemical and clinical data into a different framework.
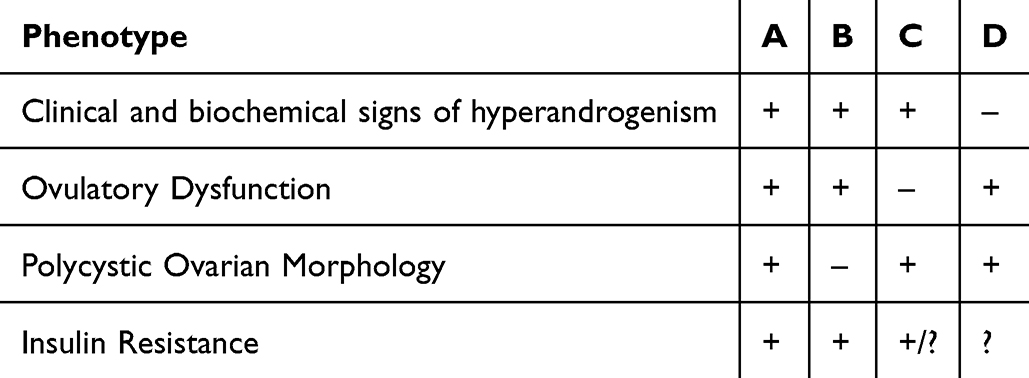 |
Table 1 Clinical Phenotypes of PCOS |
Fundamentals of Physiology of Reproduction; the Need for a Systems Biology Approach
The impairment of reproductive function is a common trait to all the PCOS phenotypes. Although PCOS can produce oocytes in a huge quantity, they are often of poor quality, leading to lower fertilization, cleavage and implantation rates.12 Infertility is a common denominator in almost all (from 75 to 90%) PCOS phenotypes.13 Conversely, PCOS is the predominant cause of infertility in young women.14 It is therefore mandatory to focus on the basic principles governing the reproductive system in humans.
This is not an easy task, as the reproductive system behaves as a complex process, governed by different, interacting levels, which involves several pathways and molecular factors changing in times, as the ovary undergoes cyclic changes in coordination with the uterus and the menstrual cycle (Figure 1). In turn, the ovarian cycle rules the preparation of several endocrine-responsive apparatus (including breast and uterus), while orchestrating the maturation and release of the oocyte.
 |
Figure 1 The Hypothalamic-Pituitary-Gonadal axis. The HPG is subject to a set of regulatory rules, involving many levels, from the central nervous system to the local factor produced by the ovaries. The integrated network includes also stimulatory/inhibitory cues provided by the environment and the metabolism. |
When the secondary follicle is formed, the LH surge occurs to produce ovulation, with rapid growth of the follicle, completing the first meiotic division, and rupture of the mature follicle to be released from the ovary. If fertilization occurs within the next 24 hours, then the 2nd meiotic division is completed.
Schematically, we recognize two principal levels of regulation, a central one – represented by the coordinated release of hypothalamic-pituitary hormones – and a terminal one (intra-ovarian), where several cytokines, endocrine factors and biophysical cues concur. Two different clusters of signals – distributed along a top-bottom hierarchical tree – constitute the main drivers of the overall system: the Hypothalamic-Pituitary-Gonadal (HPG) axis produces gonadotropin-releasing hormone (GnRH), FSH and LH, whereas estrogens (Estrone, and 17β-Estradiol, E2) and Progesterone (P4) are synthetized by the steroidogenic ovarian pathway. GnRH neurons discharge GnRH in discrete pulse and the pituitary decodes the secretion rhythm in order to release selectively LH or FSH. In turn, LH and FSH regulate the E2 synthesis by ovaries as well as cyclical changes across the menstrual cycle. However, this is a simplified scenario, given that other neuropeptides and neurotransmitters – like Melatonin and Kisspeptin – participate in this complex regulation.
Melatonin seasonal changes are instrumental in inhibiting the reproductive function in both male and female animals,15 whereas, in humans, besides the direct effect exerted within the ovary in facilitating oocyte maturation, melatonin plays a significant role in regulating the ovulation cycle, given that the gonadotropin surges are controlled by cyclic light-dark photoperiods.16 Kisspeptin, a product of KISS1 gene, is a neuropeptide that stimulates the secretion of FSH and LH via increased release of GnRH. PCOS was associated with increased kisspeptin release, supporting the hypothesis that an over-stimulation of the KISS1 system that leads to hyper-stimulation of the HPG axis, causing irregular menstrual periods and excessive androgen secretion.17 Yet, the influence of Kisspeptin extends beyond the hypothalamus and the pituitary, given that the neuropeptide has direct effects on the ovaries, regulating processes such as follicle development, oocyte maturation, and ovulation. Unfortunately, investigations carried out either on PCOS patients or in animal models have not explored this area in depth.18
A central theme in PCOS research is the disruption in the pattern of GnRH release, with consequent deregulated LH and LH/FSH ratio.19 In the ovary, the relative suppression of FSH precludes proper follicular maturation, and LH predominance contributes to enact a sustained production of androgens by theca cells TCs.20 Unexpectedly, in PCOS women the GnRH pulse frequency is unaffected by Progesterone (P4)21 (in contrast to what happens in healthy females), and this effect is independent of androgens, as the administration of Flutamide (an androgen antagonist) do not reverse the observed abnormalities.22 However, the available experimental evidence does not help in clarifying if the deregulation of the HPG axis is either primary or secondary to other causes, as concomitant hyperandrogenism and metabolic associated complications (obesity and insulin resistance). Moreover, the cross-talk between HPG axis and androgen release, as important as it is, cannot provide a satisfactory explanation of several key issues, highlighted by investigations carried out with PCOS rodent models. In particular, female Sprague-Dawley rats gradually develop chronic anovulation associated with PCOS disease when exposed to continuous light, as well as typical histologic features suggesting a profound deregulation in ovary structure, with hyperplasia of the theca cell layer.23 The resulting anovulation is reversible when animals switched to light/dark light regimens, although the intensity, duration, and spectral characteristics of the light influence the rate at which chronic anovulation occurs. The mechanisms underlying anovulation in those models still require an extensive investigation. Besides stress, which can activate the sympathetic nervous system thus resulting in adrenal gland hypertrophy,24 melatonin can also participate in the pathogenic process given that continuous light exposure suppresses melatonin synthesis. As a proof of principle, ovulation was restored in 70% of female rats exposed a constant light regime when they received melatonin.25 Furthermore, feeding rats with a meal (polenta) deprived of tryptophan that impairs both the serotoninergic and melatoninergic pathway, several abnormalities occur, including reduced serotonin and increased LH levels.26 Overall, these data demonstrate that the anovulatory condition and several PCOS-like features can result from the experimental manipulation of the central hypothalamic-pituitary axis. Noticeably, androgen addiction is not required in these models for enacting the syndrome, albeit secondary hyperandrogenism can occur later.
It is remarkable that HPG displays alternative modules of functioning, a phenomenon known as bistability,27 which is disrupted in some reproductive disorders. For instance, in polycystic ovary syndrome (PCOS), alterations in the GnRH pulse generator and abnormal androgen feedback may lead to a persistent high LH-state.28 The switch between the two frameworks proceeds according to the cyclic phase of ovary activity, becoming evident especially during the transition between the follicular and luteal phases. Physiologically, under the influence of positive/negative feedback loops involving GnRH, LH, FSH, estrogen, and progesterone, the kisspeptin system drives the switch towards different, alternative issues, ending up into two distinct, stable states that orchestrated the cyclic ovulatory process. In PCOS, alterations in the normal pattern of GnRH activity can lead to a persistent high-LH state, becoming then insensitive to the inhibitory feedback exerted by estrogens and progesterone. This condition enacts a hyperandrogenic state. In turn, hyperandrogenism participate in self-perpetuating an abnormal pattern of endocrine release, characterized by a high LH/FSH ratio. Increased secretion of LH promotes the synthesis of androgens in TCs that cannot be properly converted into estrogens by granulosa cells (GCs). Finally, increased availability of androgens further compromises the HPG homeostasis and its capability to restore an appropriate regulatory loop.29
During the last years, the critical role of some factors – frequently underrated – has emerged as relevant in providing directionality and resilience to this transition. Namely, Inhibin A and B have been shown to plays a specific role in ensuring the switch in between the two endocrine states. In the follicular phase, sustained levels of Inhibin B – along with rising estrogen levels – contribute in suppressing FSH secretion. Once the tertiary follicle has been selected, Inhibin A – produced by the corpus luteum – becomes the dominant form. Consequently, at the end of the luteal phase Inhibin A favors the FSH rise, a mandatory step for recruitment of new ovarian follicles and the restart of the entire ovarian cycle.30
Disruptions in the bistable nature of the HPG axis have been implicated in various reproductive disorders and recognizes several pathogenic causes, including genetic, drug administration, endocrine disruptors, nutritional habits, psycho-neurological disorders and environmental factors.31 Intriguingly, women with eating disorders tend to manifest ovulatory problems (oligomenorrhea and amenorrhea), meanwhile starvation or bulimia favor deactivation of HPG, thus blocking ovarian and uterine cycles.32 Similarly, toxicants and endocrine disruptors can dramatically impair the HPG axis, especially when exposure undergoes in pre-natal periods or girlhood.33 Interestingly, pre-natal exposure to androgens, endocrine disruptors or nutritional deficiencies, affects development of PCOS in adulthood,34 demonstrating that time at which exposure occurs is a critical determinant in enacting the syndrome. However, many other endocrine factors participate in modulating the principal axis of control by acting at several, intertwined levels: prolactin,35 melatonin,16 thyroid hormones, IGF-1,36 not to mention ACTH and androgens secreted by the adrenals.37
Relevance of pre-natal exposure to androgens has been extensively investigated, since it was ascertained that female pseudo-hermaphrodite monkeys exposed to testosterone in uterus resulted in PCOS-like symptoms and hyperandrogenemia in adulthood.38 Similarly, sheep exposed to testosterone during-gestation develop oligo-ovulation, PCOS morphology, LH deregulation and hyperandrogenism.39 Noticeably, obesity fostered by overfeeding amplifies the reproductive defects in these animals that show also insulin resistance.40,41 Similar results have been obtained in rodent models,42 in which testosterone administration causes increased LH and testosterone and reduced FSH, in addition to estrous cycle irregularities and ovarian cysts. Moreover, in this specie, even a small dose of 5 mg/d prenatal testosterone may also lead to metabolic disturbances, including increased body weight, hyperinsulinemia, and dyslipidemia.43 Accumulated data shows thus that the disruptions in the pattern of GnRH release may be partially primed during the pre-natal period, particularly through exposure to androgen excess that may permanently alter steroid negative and positive feedback regulatory mechanisms through changes affecting via changes in neural network and steroid receptors (reviewed in44).
This overall evidence indicates that systemic factors and higher levels of control regulate both ovarian steroidogenesis and reproductive function. The regulation displays bistability and it is sensitive even to mild fluctuations of critical parameters, according to a non-linear dynamic, varying in space and times,45 in both humans and animals.46 Remarkably, the HPG axis establishes an intricate cross talk with intra-ovarian factors that contribute significantly in shaping steroidogenesis and reproductive function. As privileged levels of «causation» are not recognizable in complex systems,47 the intrinsic dynamic of the ovarian apparatus can be caught only by considering the interplay in between the two aforementioned tiers: systemic and intra-ovarian according to a systems biology approach. Unfortunately, besides some preliminary attempts,48 this field has not received the attention it deserves.
Intra-Ovarian Factors in PCOS Pathogenesis
The single follicle is the fundamental unit of the ovary and is composed of an oocyte surrounded by specialized endocrine cells, partitioned in the theca and granulosa cell layers, respectively. Steroid synthesis occurs in a compartmentalized system in which TCs produced androgens (mostly testosterone), which are then converted into estrogens by GCs. The coordinated action of sex steroid hormones, in association with the concerted participation of several other molecular factors and cytokines – including Bone Morphogenetic Proteins (BMPs), Inositol (myo-Ins), Activin, AMH, IGF-1, Inhibin A and B), modulate the regulate follicle cell growth and maturation of the oocyte49 (Figure 2). Cytoskeleton (CSK) architecture provides a critical support in performing such tasks, enabling cholesterol transport into ovarian cells under the stimulus of ACTH,50 and it is noteworthy that some factors involved in ovarian regulation may influence the dynamical changes of CSK.51
 |
Figure 2 Ovarian steroidogenesis. Steroidogenesis in the ovary encompasses two principal phases. First, LH (in association with insulin (IN) promotes androgens synthesis and androgen receptors (AR) expression, mostly by up-regulating CYP17A1. IGF-1, AMH, and Inhibin-B progressively increase, amplifying LH-induced stimulation, meanwhile blocking CYP19A1 activation. PI3K overexpression/hyperactivation is required. Correspondently, the primordial follicle progresses to reach the small antral stage. This phase is largely gonadotropin-independent. The bifurcation point occurs when, under the increase of FSH (and of its receptor), aromatase becomes activated. Aromatase levels increase and trigger the synthesis of estrogens, quickly followed by a parallel increase in progesterone (P4), and Activin that contributes in enhancing oocyte’s maturation. The follicle progresses until reaching the pre-ovulatory condition. This secondary phase is considered gonadotropin-dependent. |
Proper CSK configuration is needed to ensure the communication between the two functional compartments of the ovary (TCs and GCs), resulting in the reciprocal modulation of morphology, structure, growth, and function. Indeed, cellular interactions seem to be one of the major factors controlling the fate of follicular cells during follicular maturation. Conversely, when theca and granulosa cells are left to grow in isolation – with resulting disruption of the reciprocal interactions – they lose several critical features,52 meanwhile, GCs cultured alone in vitro undergo luteinization, with increased production of progesterone.53 Cytoskeleton architecture and cell–cell interactions display a critical role during the early phase of ovarian growth characterized by the primordial follicle assembly, during which a transition occurs from nests to primordial follicles. Several paracrine/autocrine factors govern this transition, including ligand (KL), leukaemia inhibitory factor (LIF), BPMs, keratinocyte growth factor (KGF) and basic fibroblast growth factor (bFGF). It is worth of note that abnormalities in the development of this very early stage of ovary specialization result in premature ovarian failure, PCOS and female infertility (reviewed in54).
The overall process proceeds through two different phases. The first – from the primordial to the secondary follicle development – is substantially independent from gonadotropin stimulation, whereas the next one is tightly dependent on gonadotropin secretion (Figure 2). On a molecular level, the phosphoinositide 3-kinase (PI3K) pathway seems to be central in regulating fate decisions in primordial follicles and activation of PI3K enable the recruitment of follicles in the maturation process.55 The PI3K-FOXO3 pathway is promoted by testosterone through a non-genomic mechanism,56 allowing primordial follicles to enter into the maturation process. This effect relies on PI3K activation and on the contemporary downregulation of GDF-9. Similarly, IGF-1 synergizes with androgens by exerting a receptor-mediated protection from apoptosis through the PI3K activation.57 During the first-phase androgens, androgen receptors (ARs) as well as AMH rise incrementally until the moment when estrogens and FSH begin to surge. The zona pellucida develops, GCs acquire a second layer thus establishing cell–cell contact with both TCs and GCs. Androgens are required for the establishment of gap junctions through which the oocyte communicates with both TCs and GCs.58 Overall, transition into the second phase is supported by androgens, given that Flutamide administration decreases connexin 43 expression and impairs connectivity among GCs. Intriguingly, this effect is strictly dependent on the phase of differentiation of granulosa, as androgen excess occurring after ovulation is associated with an opposite effect, ie with reduced connexin-43 expression.59 This example clearly shows that the degree of differentiation of GCs constraints the functional outcome downstream estrogen stimulation (context dependence). At this moment, an antrum begins to develop in the follicle and GCs differentiate leading to the appearance of mural and cumulus cells that will provide structural and nutritional support to the oocyte.
When the secondary phase begins, TCs participate in providing a vascular network to the growing follicle, while enhancing the activity of several steroidogenic enzymes (Star, CYP11A1, Cyp17A1and HSD3β), as well as the expression of LH receptor (LHr), allowing a sustained androgen synthesis.60 In this phase, TCs are extremely sensitive to the auto/paracrine control provided mainly by members of the tumor growth factor-β (TGFβ) superfamily, including GDF-9 and the bone morphogenetic proteins (BMP-4, BMP-6 and BPM-7). GDF-9 is essential for TC layer differentiation and subsequent androgen synthesis in pre-antral follicles. Noteworthy, GDF-9 contributes in inhibiting FSH-induced maturation of GCs and aromatase activity.61 Concomitantly, insulin, in synergy with LH, induces Cyp17A1 and stimulates thecal androgen production, as well as estrogens from GCs.62 On the contrary, BMP proteins attenuate androgen synthesis by downregulating Cyp17A1.63 In GCs, activin negatively modulates androgen synthesis, while, under the stimulation exerted by FSH, aromatase synthesis increases.64 Androgen surge from TCs is also needed in priming GCs receptivity to FSH stimulation, given that testosterone amplifies AR and FSHr expression, as well c-AMP signaling downstream of FSH stimulation.65
The Pivotal Role of Inositol
Androgens produced by TCs are quantitatively converted into estrogens in healthy subjects, promoting the transition from the first into the secondary phase of maturation. Aromatase (Cyp19A1) is the key enzyme that catalyzes this transition, mostly through the conversion of testosterone to 17β-Estradiol.66 Noticeably, in follicles from PCOS women, both estrogens and aromatase expression are dramatically reduced when compared to healthy control.67 Another paper evidenced that GCs from PCOS patients have little if any aromatase enzyme activity, as evidenced by their inability to convert aromatase substrate to estrogens. However, they recover their capability of aromatization when stimulated with FSH.68 Therefore, activation of aromatase identifies the critical bifurcation point that marks the transition, driving the maturation process towards the final steps. Estrogen synthesis in coordination with the activity of FSH and its receptor display a pivotal role in this process. The surge in estrogens mediated by Cyp19A1 is further followed by the increase in progesterone receptors (P4Rs) and progesterone. Although underestimated, progesterone displays a critical role in these last steps, as witnessed by the amplitude of increase in its concentrations: whereas levels of estradiol increase by 200%, progesterone concentrations vary by over 1200%.69
At this point, the participation of intra-ovarian regulatory factors – namely AMH and Inositol – becomes critical, as they orchestrate the switch of steroid synthesis, from androgens to estrogens. The Anti-Mϋllerian Hormone (AMH), a member of the TGFβ family, is exclusively synthetized by GCs and its release increases (in association with Inhibin) when the follicle progresses to the secondary phase; then AMH declines during the last steps.70 The convergence of both AMH and Inhibin B surge is consistent with the inhibitory role sustained by both on FSH activity, helping in promoting the selection of the mature follicle, leaving AMH to inhibit the transition of primordial follicles toward the primary ones. AMH antagonize also the FSH-dependent expression of Cyp19A1 and attenuates sensitivity of follicles to FSH.71 Remarkably, AMH is 75 times higher in GCs from anovulatory PCOS women, compared with normal ovaries. Moreover, this increase is insensitive to FSH downregulation, as observed in healthy controls suggesting a dramatic impairment of GCs control upon steroidogenesis.72 This combined effect increases significantly the androgen/estrogen ratio within the ovaries. A positive correlation has been recorded between testosterone and AMH circulating levels, while AMH and AR expression showed a linear correlation in GCs obtained from PCOS women.73 Interestingly, serum AMH increases in both PCOS and Type 1 diabetes mellitus patients, suggesting a link between deregulation of insulin/glucose metabolism and AMH profile.74 Ovarian sensitivity to androgen is further enhanced by insulin, even in absence of insulin resistance (IR). However, Insulin alone does not increase androgenic enzymes (CYP17A1) expression in PCOS theca cells, and other factors – including LH – are required in sustaining a «hyperandrogenic» phenotype.75 It is worth noting that insulin increases FSH synthesis without affecting estradiol secretion, given that an uncoupling mechanism leads to decrease aromatase activity.76 A lack of increase in FSHr could probably explain why FSH increase does not translate into an enhanced CYP19A1 activity.
All these factors participate in increasing androgen release. Thereby, it is mandatory to ensure an appropriate stimulation to increase both Cyp19A1 synthesis and activation in such a condition. Ovary relies on FSH (namely through the overexpression of its receptor, FSHr) for fulfilling such tasks. However, other factors demonstrated to participate in fine-tuning the process, while modulating any androgen excess that could occurs.
In the last decade, several studies evidenced that myo-Inositol (myo-Ins) and D-Chiro-Inositol (DCI) are both involved in modulating ovarian steroidogenesis.77 This role has been hypothesized long ago, when a beneficial effects upon ovary function was obtained in PCOS women treated with low doses DCI.78 This clinical result was ascribed to the improvement of the insulin resistance, given that insulin over-stimulation alters the myo-Ins/DCI ovarian ratio. Intriguingly, a previous study noticed that pharmacological reduction of insulin secretion in PCOS women (without sign of metabolic disease and normal insulin levels) induces a significant decrease in blood testosterone and LH levels, thus reinforcing the hypothesis of a pathogenetic link between insulin and PCOS.79
Indeed, a number of experimental and clinical results have suggested a tight connection between inositols and insulin. Insulin signalling depends on the faithful transduction assured by insulin receptor (IRS), which in turn enacts a number of critical biochemical cascades, including the activation of PI3K pathway.80 Transduction of IRS signal required an appropriate myo-Ins/DCI equilibrium within the cell.81 Insulin promotes the epimerase-mediated conversion of myo-Ins into DCI, which is further incorporated into glycosylphosphatidylinositol-anchored proteins (GPI), from which it is released as DCI-inositol-phosphoglycan (IPG-P), an intermediary metabolite displaying a critical role in transducing insulin effects.82 Note that myo-Ins is also found as phosphoglycan derivative (IGP-A), displaying similar effects on insulin transduction. Consequently, insulin resistance and diabetes – two conditions in which the epimerase activity is severely impaired due to the reduced effectiveness of insulin transduction – show a reduced DCI release from muscle and adipose tissues. The limited availability of DCI is in turn associated with some defects in the proper utilization of glucose.83 These findings prompted to consider the myo-Ins/DCI ratio a reliable parameter of IR.84 However, as ovaries retain their insulin sensitivity even in presence of IR, persistent increase in insulin during IR likely promotes the myo-Ins conversion into DCI, leading to a «paradoxical» DCI increase in the ovary, in contrast to what recorded in other tissues. The increased levels of both epimerase and DCI in TCs documented the «hypersensitivity» of ovarian cells to insulin, showing that the myo-Ins/DCI ratio was significantly lower than that recorded in normal women.85 Furthermore, this hypothesis received a decisive confirmation by analyses of inositol content of follicular fluid, showing that the myo-Ins/DCI ratio average 0.2:1 in PCOS patients, while in healthy control the value was around 100:1.86
The increased DCI concentration in ovarian cells could therefore amplify insulin action in PCOS theca cells, thus leading to increased intra-cellular synthesis of testosterone.87 Unexpectedly, it was ascertained that the DCI-derived phosphoglycan (IPG-P) is required for androgen synthesis downstream of insulin stimulation.88
Consequences of increased DCI are not restricted to androgen synthesis in TCs and involve GCs as well. The DCI isomer displays specific effects on estrogens availability, likely through the inhibition of aromatase activity. Indeed, in PCOS-mice administration of DCI lead to profound ovarian histologic alterations, and inhibits aromatase activity.89 Furthermore, high DCI concentrations negatively influence the quality of oocytes, therefore impairing the overall efficiency of the reproductive system.90 Yet, the increased availability of androgens promoted by DCI would favor an increased transformation into estrogens, at least in principle,91 given that androgens, insulin and IGF-1 synergize with testosterone in enhancing FSH transduction and aromatase activity.92 Therefore, it is evident that DCI not only promotes androgen release but also impairs the estrogenic response of granulosa cells to FSH and androgens.
Clinical Data
For a while, it has been supposed that inositol effects could be explained by the modulation exerted upon insulin transduction. The first study authored by Nestler et al treated with DCI (1200 mg/daily) a group of hyper-androgenic PCOS women (22% with insulin resistance). After 8 weeks of treatment, a remarkable recovery of the ovarian capability was recorded in the majority of women (86% vs 27% in the control group). These results were later confirmed by further studies performed in lean women, as well as in insulin resistant patients, in which DCI was able to reduce both testosterone and insulin.93,94 These previous findings were greeted lukewarmly, as some studies did not confirm the DCI effectiveness.95 Indeed, this result is not surprising given that DCI inhibits aromatase expression, as previously mentioned,95 thus impairing estrogen release from the ovaries. Furthermore, it was shown that DCI stimulates testosterone synthesis through its phosphoglycan (IPG-P),96 as also confirmed by the increase in testosterone levels recorded when healthy volunteers were treated with 1200 mg of DCI for a short period of time.97 Conclusively, high doses of DCI will paradoxically enhance androgen synthesis from TCs and consequently impair ovulation by decreasing aromatase activity.
Insulin overstimulation – as happens during insulin resistance – significantly impairs myo-Ins conversion into DCI in many tissues (particularly muscle and heart), with resulting low intracellular concentration of DCI.98 Conversely, the administration of DCI at pharmacological doses demonstrated to ameliorate some metabolic features related to diabetes/insulin resistance, decreasing henceforth insulin release and, consequently, the insulin-dependent stimulus on androgen synthesis.99 However, insulin resistance is not associated with impairment of the insulin transduction signal at the ovarian level, as hyperinsulinemia still stimulates ovarian androgen production in PCOS.100 Therefore, in the ovary, insulin increases «paradoxically» myo-Ins conversion into DCI. Consequently, DCI, while ameliorating the PCOS-related systemic metabolic parameters, amplifies the ovarian steroidogenic abnormalities, thus providing a mechanistic rationale explaining the «inositol paradox».101 Indeed, by raising ovarian DCI, the insulin signalling would likely be amplified, given that IPG-Ps increase mRNA and protein expression of the insulin receptor substrate (IRS1), thus improving the receptor-mediated insulin transduction, up-regulate PI3K and enhance the activation of several pathways downstream of PI3K, including the Akt-mTOR.102
Those findings also help to explain why treatment with antidiabetic drugs (metformin) improves several PCOS-associated metabolic markers,103 while being ineffective in ameliorating the ovulatory function, as demonstrated by a decrease in follicle number and quality following metformin treatment.104 By no doubt, myo-Ins can efficiently counteract some abnormalities associated with insulin resistance, as reported by studies performed in animals and humans.105,106 Investigations dealing with a rodent PCOS model showed, for example, that myo-Ins administration downregulates androgen release while increasing estrogens synthesis, ultimately leading to the recovery of the estrous cycle and ovulation function.107 The same study evidenced that insulin resistance was efficiently antagonized, as witnessed by the normalization of several metabolic parameters and the reduction of inflammatory markers (IL-6). However, insulin resistance alone cannot provide a satisfactory explanation of the complexity of PCOS. Henceforth, it is wrong to hypothesize a PCOS pathogenesis model in which the metabolic “defect” (ie, defective insulin transduction due to impaired availability of inositolphosphoglycans) plays a causative role. This model underestimates the effects directly triggered by DCI and myo-Ins upon steroidogenesis.
These findings prompted to reconsider the pivotal role played by aromatase in PCOS pathogenesis, as CYP19A1 occupies a central position in switching follicle maturation from the primary to the secondary phase by enacting the estrogen surge in thigh coordination with FSH stimulation.108 Intriguingly, myo-Ins induce very different effects upon steroidogenesis. Treatment with myo-Ins significantly decreases the LH/FSH ratio in plasma of PCOS women,109 while supplementation with myo-Ins during in vitro fertilization permits to lessen the doses of recombinant FSH administered,110 and increases CYP19A1 expression even without any previous FSH administration.111 Moreover, myo-Ins increases FSH receptor and aromatase expression in GCs, while reducing androgen synthesis in a PCOS murine model.112 In addition, myo-Ins downregulates PI3K in different cell types.113 This is an interesting finding given that PI3K activation participates in enhancing the pro-androgenic effects of LH and insulin.114 Furthermore, a new line of evidence comes from studies related to the nuclear steroidogenic factor 1 (SF-1), a critical effector involved in folliculogenesis and aromatase expression in the ovary.115 The phosphatidylinositol 4,5-bisphosphate (PIP2), a phosphoinositide that is modulated by exogenous myo-Ins, binds to SF-1 and modulates its transcription, shifting to a phosphorylate state mediated by the inositol polyphosphate multi-kinase.116 This overall evidence suggests that myo-Ins exerts direct and significant effects upon steroidogenesis.
Based on reported data, the associated use of both isomers has been advocated by several groups. The rationale behind this strategy relies on two basic assumptions: DCI would reduce systemic insulin levels (by ameliorating glucose metabolism in tissues supposed insulin-resistant), while myo-Ins could improve FSH and aromatase activity. In turn, improvement of insulin resistance mitigates the stimulation exerted upon the ovarian epimerase that converts myo-Ins into DCI, thus facilitating the normalization of myo-Ins/DCI ratio in follicular fluid.117 To ensure that outcome it is mandatory to combine the isomers according a proper, physiological ratio.
Indeed, pre-clinical studies in PCOS mice with different myo-Ins/DCI ratio showed that only formulas with high myo-Ins concentrations and low DCI content (40:1) proven to be effective.11,25, Mice receiving myo-Ins/DCI in a 40:1 molar ratio fully recover from PCOS, while treatments with higher DCI concentrations resulted ineffective or even detrimental. Remarkably, histological findings showed that the theca layer undergoes a dramatic hyperplasia in PCOS animals treated with high doses of DCI, whereas inositols in the physiological ratio (myo-Ins/DCI 40:1) re-establish in full the normal architecture.
Several studies and meta-analyses provided a sound confirmation of pre-clinical investigations, showing that myo-Ins supplementation – associated with DCI in the 40:1 ratio – produced beneficial effects by ameliorating several endocrinological and metabolic parameters in PCOS.109,118–121
These findings indicate that the inositol isomers play a conflicting role in the ovary. Androgen release increases under DCI treatment, while aromatase is significantly downregulated. On the contrary, myo-Ins increases both aromatase and FSHr expression. Impaired availability of FSHr and CYP19A1 are specific hallmarks of PCOS.76 Indeed, it has been shown that treatment based on high DCI concentrations (either with or without myo-Ins) further deteriorate signs and symptoms of PCOS.97 Those findings has been vindicated by clinical studies using combination of myo-Ins/DCI in the ratio 40:1.122 Moreover, the fact that myo-Ins could directly modulate the estrogen/androgen balance, casts on doubt that the primary mechanism should involve insulin. Indeed, studies performed in young women with PCOS not affected by metabolic abnormalities, including insulin resistance, evidenced that myo-Ins-based treatments are in any case effective.123,124 Additionally, even women that resulted “refractory” to preliminary myo-Ins treatments, recover their sensitivity to myo-Ins when inositol was co-administered with α-lactalbumin, which favors significantly the intestinal inositol adsorption).125 In these patients, myo-Ins was able in recovering a proper reproductive function in 86% of women, while a significant improvement in endocrine profile was achieved in the majority of cases.126 Recently, Kamenov et al provided a confirmation of these findings by comparing the effects of myo-Ins versus myo-Ins plus α-Lactalbumin in a three-months trial involving 50 patients. The associated therapy improved several symptoms and endocrine features, while achieving high rates of ovulation.
An Integrated Pathogenetic Model
Cumulative evidence shows that the reproductive function is severely impaired in ovaries from PCOS women, given that androgens (and related enzymes) increase, altogether with AMH, while estrogens and CYP19A1 are significantly downregulated. Noticeably, as suggested by histologic observations from murine models, ovarian follicles develop a significantly enlarged theca cell layer, while the granulosa cell layer is reduced with the TCs/GCs thickness shows an inverted ratio.25 This finding is consistent with the characteristics of an increased TCs activity, suggesting an intra-ovarian hyperandrogenic disposition. However, hyperandrogenism by itself is untenable to account for all the fundamental characteristics of PCOS. Indeed, accumulated evidence reinforces the hypothesis of a deregulated balance in the ovary – involving both androgens and estrogens – as a fundamental pathogenetic moment for the development of PCOS.127
Histologically, PCOS ovaries are characterized by the accumulation of small antral follicles, evidencing that the physiological follicular development is impaired, with an arrest corresponding to the beginning of the secondary phase, ie from the very early, gonadotrophin-independent stage onward, finally resulting in follicular arrest without the selection of a dominant follicle.128,129 PCOS ovaries contain three to six fold the normal number of follicles, particularly at the primary follicle stage, when they reach 4–7 mm in diameter. The excessive growth of primary follicles indicates that an intra-ovarian hyperandrogenism occurs even if signs of clinical hyperandrogenism are missing. Second, the inability to select a follicle committed toward a complete maturation demonstrates that FSH and aromatase activity – required in fostering the estrogen surge – are inefficient in PCOS. These findings indicate that ovaries are partially unresponsive to the control exerted by LH and FSH. Conversely, LH suppression induced through the administration of Gn-RH analogue is unable in reducing androgen synthesis.130 Moreover, studies performed on TCs in long term cultures obtained from either PCOS women or mice models have demonstrated that TCs display a sustained activation of several androgenic enzymes (CYP17A1 and HSD3β) with resulting increased synthesis of testosterone and DHEA, even in absence of LH stimulation.127 It may be hypothesized that intra-ovarian hyperandrogenism (ie, increased ovarian availability of androgens even in absence of biochemical and clinical signs of hyperandrogenism) may indeed play a causative role in PCOS. Clinical hyperandrogenism should not be confused with ovarian hyperandrogenism. Certainly, ascertaining intra-ovarian hyperandrogenism is a difficult task, and this feature could run unnoticed. However, when appropriate chromatographic/mass-spectrometry techniques are used to investigate steroids pattern in follicular fluids, higher concentrations of individual and total androgens, lower total estrogens, and a lower total estrogen-to-androgen ratio, are identified in the majority of PCOS women compared with regularly menstruating women.122 Those results showed a lower capability of PCOS women in transforming an intra-ovarian androgen excess to estrogens via aromatase, thus leading to the arrest of follicular growth and anovulation, as already noticed by earlier findings.123 Aromatase in GCs has limited conversion capability, due to either enzymatic defects (blockade of the active site of the enzyme and decreased substrate affinity),124 or to reduced expression. Noticeably, some local factors – including myo-Ins availability – might play a significant role at that level, by either enhancing or inhibiting aromatase activity. The dynamic cross talk between systemic players and intra-ovarian factors may help explaining how the convergence of these different factors can, in turn, produce different phenotype, although impairment of reproductive function represents the outcome.
At the ovarian level, TCs show a commitment toward increased androgen synthesis, due to deregulation of LH transduction (as evidenced in presence of reduced MAP2K1 expression, high DCI content) and the contemporary overexpression of PI3K. Increased insulin stimulation – in association with LH – amplifies androgen release. In turn, decrease in FSH, eventually amplified by reduced FSHr expression and in presence of high AMH levels, reduces aromatase activity, especially in myo-Ins deficient GCs. In this context, the continuous availability of androgens reinforces the inhibition upon aromatase activity, therefore leading to a deficit in estrogens.131 Inositols participate in different steps of the process: high DCI levels (coupled with reduced myo-Ins concentrations) can worsen insulin effects upon androgen synthesis, while decreasing aromatase expression. Myo-Ins exerts opposite actions, by modulating PI3K and increasing both aromatase and FSHr expression (Figure 3). Moreover, myo-Ins displays other relevant effects upon metabolic pathways, CSK architecture, and by antagonizing inflammatory and oxidative processes, that contribute – at least in part – in the pathogenesis of PCOS.132
 |
Figure 3 Mio-Inositol effects in the ovarian cell. The picture shows schematically the principal effects related to myo-Inositol treatment. Myo-Ins modulate insulin transduction (mostly through the epimerase-dependent conversion into DCI; participate in CSK remodelling; modulate the ratio between PIP2 and PIP3; antagonize oxidative and inflammatory processes. Overall, those mechanisms contribute in modulating the ovarian steroidogenesis. Myo-Ins up-regulate CYP19A1 and FSHr expression, while inhibiting some androgenic enzymes. AT the opposite, DCI favor androgenesis and downregulates CYP19A1 expression. |
Conclusion
Conclusively, we can infer that PCOS pathogenesis should integrate both an increase in androgens as well as a reduction in estrogen availability: these two pathogenetic aspects are both required for the clinical appearance of the syndrome. Systemic factors (LH, Insulin, just to mention a few) should synergize to impair the ovarian steroidogenesis by interacting in a cooperative manner with intracellular, specific conditions, including altered BMP, activin and especially inositol concentrations. Given that LH/gonadotropin deprivation does not seem to restore a normal steroidogenesis within the ovary, it is conceivable that the systemic influence upon ovary function can predispose but not trigger the abnormalities observed in PCOS, until an intra-ovarian defect does not come into play. The selective participation of those factors can likely explain differences in the resulting clinical phenotypes. Whether PCOS could be a primary ovarian disorder or a consequence of systemic deregulation is therefore a false question, as cumulative evidence shows that systemic and intra-ovarian factors cooperatively interact in producing signs and symptoms of the disease. Myo-Ins treatments – especially when associated with low doses of DCI according to the 40:1 ratio – has proven to ameliorate some systemic effects (namely by counteracting insulin resistance) and to modulate intra-ovarian processes, leading to reactivation of aromatase and FSH sensitivity. Remarkably, following myo-Ins treatment recovery of ovulation occurs in animals and in PCOS women, with a high rate of success (63–86% of cases). It is worth noting that therapies based on inositols are usually well tolerated and can be extended over time without relevant side effects.
Expert Opinion
Cumulative evidence from both basic and clinical studies suggests that myo-Inositol (especially when associated with DCI according to the 40:1 ratio) could be as effective (and even more manageable) as Metformin, and likely better than other endocrine treatments. The 40:1 ratio allows conjugating the benefits of DCI upon insulin resistance (occurring in muscle and adipose tissues, especially in obese women) with those related to myo-Ins (enhanced FSHr and CYP19A1 expression). A critical issue is still represented by patients showing the phenotype D (anovulation and ovary cysts without clinical evidence of hyperandrogenism) in which the benefit of myo-Ins treatment is still under investigation.
The field would benefit from further, extensive research carried out at molecular and clinical level. It should be clarified how myo-Ins modulate the nuclear steroidogenic factor-1 (SF-1) and the field would benefit from further, extensive research carried out at molecular and clinical level. It should be clarified how myo-Ins modulate the nuclear steroidogenic factor-1 (SF-1) and if inositol induces epigenetic modifications on several key steroidogenic enzymes. These studies need to be complemented by investigating how myo-Ins addition modifies the overall metabolism of ovarian cells (TCs and GCs). From a clinical point of view, it is mandatory to reconsidering PCOS nosology, currently established by the Rotterdam criteria. Phenotypic differences cannot accommodate with a unified pathogenetic mechanism and likely require a differentiated treatment strategy. Recognizing the hallmarks of each phenotype will necessitate an extensive study that should encompass omics studies, including metabolomics. The identification of the specific phenotype would be followed by a «tailored» therapy, aiming to personalize the treatment. Major hurdles in adopting this new framework depend on the availability of specific diagnostic procedures and clinician’s skill. Moreover, reframing the PCOS definition according to different phenotypes would help in rationalizing the management of PCOS women. To achieve this goal, pharmacokinetic studies are urgently needed in order to establish the bioavailability of inositol(s) and the correct dosage. Indeed, a standardization of posology is urgently warranted.
Deepening of inositol studies must include the assessment of myo-Ins fate and dynamic within the cell. Inositols are metabolized into phosphoinositides, inositol phosphates and pyrophosphates, according to the context (cell type) and the specific functional/metabolic demand. This study should be prioritized in order to acquire a full understanding of this molecule. Such advancement will pave the way or future discovery regarding the potential usefulness of myo-Ins in other clinical fields, like cancer, morphogenesis-related diseases, neurological problems and metabolic disturbances, including diabetes.
Abbreviations
CYP11A1, Cholesterol side-chain cleavage enzyme P450c11a1; CYP17A1, 17α-hydroxylase P450c17; HSD3β, 3β-Hydroxysteroid dehydrogenase; GDF-9, oocyte Derived Growth factor; myo-Ins, myo-Inositol; DCI, D-Chiro-Inositol.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol. 1935;29(2):181–191. doi:10.1016/S0002-9378(15)30642-6
2. Dennett CC, Simon J. The Role of Polycystic Ovary Syndrome in Reproductive and Metabolic Health: overview and Approaches for Treatment. Diabetes Spectr. 2015;28(2):116–120. doi:10.2337/diaspect.28.2.116
3. Coyle C, Campbell RE. Pathological pulses in PCOS. Mol Cell Endocrinol. 2019;498:110561. doi:10.1016/j.mce.2019.110561
4. Yu O, Christ JP, Schulze-Rath R, et al. Incidence, prevalence, and trends in polycystic ovary syndrome diagnosis: a United States population-based study from 2006 to 2019. Am J Clin Exp Obstet Gynecol. 2023;229(1):39.e1–39.e12. doi:10.1016/j.ajog.2023.04.010
5. Miazgowski T, Martopullo I, Widecka J, Miazgowski B, Brodowska A. National and regional trends in the prevalence of polycystic ovary syndrome since 1990 within Europe: the modeled estimates from the Global Burden of Disease Study 2016. Arch Med Sci. 2021;17(2):343–351. doi:10.5114/aoms.2019.87112
6. Netter A, Lambert A, Haskeles M. [Stein-Leventhal syndrome; 4 case reports]. C R Soc Fr Gyncol. 1958;28:127–133;discussion133–135.
7. Zhang J, Zhu Y, Wang J, et al. Global burden and epidemiological prediction of polycystic ovary syndrome from 1990 to 2019: a systematic analysis from the Global Burden of Disease Study 2019. PLoS One. 2024;19(7):e0306991. doi:10.1371/journal.pone.0306991
8. The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Sterility. 2004;81(1):19–25. doi:10.1016/j.fertnstert.2003.10.004
9. Yang R, Yang S, Li R, Liu P, Qiao J, Zhang Y. Effects of hyperandrogenism on metabolic abnormalities in patients with polycystic ovary syndrome: a meta-analysis. Reprod Biol Endocrinol. 2016;14(1). doi:10.1186/s12958-016-0203-8
10. Tosi F, Bonora E, Moghetti P. Insulin resistance in a large cohort of women with polycystic ovary syndrome: a comparison between euglycaemic-hyperinsulinaemic clamp and surrogate indexes. Hum Reprod. 2017;32(12):2515–2521. doi:10.1093/humrep/dex308
11. Unfer V, Dinicola S, Russo M. A PCOS Paradox: does Inositol Therapy Find a Rationale in All the Different Phenotypes? Int J Mol Sci. 2023;24(7):6213. doi:10.3390/ijms24076213
12. Boomsma C, Fauser B, Macklon N. Pregnancy Complications in Women with Polycystic Ovary Syndrome. Semin Reprod Med. 2008;26(1):072–84. doi:10.1055/s-2007-992927
13. Gorry A, White DM, Franks S. Infertility in Polycystic Ovary Syndrome: focus on Low-Dose Gonadotropin Treatment. Endocrine. 2006;30(1):27–34. doi:10.1385/ENDO:30:1:27
14. Melo AS, Ferriani RA, Navarro PA. Treatment of infertility in women with polycystic ovary syndrome: approach to clinical practice. Clinics. 2015;70(11):765–769. doi:10.6061/clinics/2015(11)09
15. Hoffmann K. Melatonin inhibits photoperiodically induced testes development in a dwarf hamster. Die Naturwissenschaften. 1972;59(5):218–219. doi:10.1007/BF00595517
16. Yong W, Ma H, Na M, et al. Roles of melatonin in the field of reproductive medicine. Biomed Pharmacother. 2021;144:112001. doi:10.1016/j.biopha.2021.112001
17. Aasif A, Alam R, Ahsan H, Khan MM, Khan A, Khan S. The role of kisspeptin in the pathogenesis of a polycystic ovary syndrome. Endocr Regul. 2023;57(1):292–303. doi:10.2478/enr-2023-0032
18. Witchel SF, Tena-Sempere M. The Kiss1 system and polycystic ovary syndrome: lessons from physiology and putative pathophysiologic implications. Fertil Sterility. 2013;100(1):12–22. doi:10.1016/j.fertnstert.2013.05.024
19. Taylor AE, McCourt B, Martin KA, et al. Determinants of Abnormal Gonadotropin Secretion in Clinically Defined Women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 1997;82(7):2248–2256. doi:10.1210/jcem.82.7.4105
20. Gilling-Smith C, Willis DS, Beard RW, Franks S. Hypersecretion of androstenedione by isolated thecal cells from polycystic ovaries. J Clin Endocrinol Metab. 1994;79(4):1158–1165. doi:10.1210/jcem.79.4.7962289
21. Pastor CL, Griffin-Korf ML, Aloi JA, Evans WS, Marshall JC. Polycystic Ovary Syndrome: evidence for Reduced Sensitivity of the Gonadotropin-Releasing Hormone Pulse Generator to Inhibition by Estradiol and Progesterone. J Clin Endocrinol Metab. 1998;83(2):582–590. doi:10.1210/jcem.83.2.4604
22. Eagleson CA, Gingrich MB, Pastor CL, et al. Polycystic Ovarian Syndrome: evidence that Flutamide Restores Sensitivity of the Gonadotropin-Releasing Hormone Pulse Generator to Inhibition by Estradiol and Progesterone. J Clin Endocrinol Metab. 2000;85(11):4047–4052. doi:10.1210/jcem.85.11.6992
23. Bevilacqua A, Dragotto J, Giuliani A, Bizzarri M. Myo-inositol and D-chiro-inositol (40:1) reverse histological and functional features of polycystic ovary syndrome in a mouse model. J Cell Physiol. 2018;234(6):9387–9398. doi:10.1002/jcp.27623
24. Singh KB. Induction of polycystic ovarian disease in rats by continuous light. I. The reproductive cycle, organ weights, and histology of the ovaries. Am J Clin Exp Obstet Gynecol. 1969;103(8):1078–1083. doi:10.1016/0002-9378(69)90510-9
25. Trentini GP, Mess B, De Gaetani CF, Ruzsás C. Effect of melatonin on induction of ovulation in the light- induced constant estrous-anovulatory syndrome and possible role of the brain serotoninergic system. J Endocrinol Invest. 1978;1(4):305–310. doi:10.1007/BF03350974
26. Giammanco S, Ernandes M, Guardia M. Effects of Environmental Lighting and Tryptophan Devoid Diet on the Rat Vaginal Cycle. Arch Physiol Biochem. 1997;105(5):445–449. doi:10.1076/apab.105.5.445.3287
27. Reed BG, Carr BR. The normal menstrual cycle and the control of ovulation. In: Endotext. MDText.com, Inc.; 2018. PMID: 25905282.
28. McCartney CR, Campbell RE. Abnormal GnRH pulsatility in polycystic ovary syndrome: recent insights. Curr Opin Endocr Metab Res. 2020;12:78–84. doi:10.1016/j.coemr.2020.04.005
29. Lebbe M, Woodruff TK. Involvement of androgens in ovarian health and disease. Mol Hum Reprod. 2013;19(12):828–837. doi:10.1093/molehr/gat065
30. Reed BG, Carr BR. The normal menstrual cycle and the control of ovulation. In: Feingold KR, Anawalt B, Blackman MR, et al. editors. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000. PMID: 25905282.
31. Wiksten‐Almströmer M, Lindén Hirschberg A, Hagenfeldt K. Menstrual disorders and associated factors among adolescent girls visiting a youth clinic. Acta Obstetricia et Gynecologica Scandinavica. 2007;86(1):65–72. doi:10.1080/00016340601034970
32. Stewart DE. Reproductive Functions in Eating Disorders. Ann Med. 1992;24(4):287–291. doi:10.3109/07853899209149956
33. Ramos JG, Varayoud J, Kass L, et al. Bisphenol A Induces Both Transient and Permanent Histofunctional Alterations of the Hypothalamic-Pituitary-Gonadal Axis in Prenatally Exposed Male Rats. Endocrinology. 2003;144(7):3206–3215. doi:10.1210/en.2002-0198
34. Ramezani Tehrani F, Noroozzadeh M, Zahediasl S, Piryaei A, Hashemi S, Azizi F. The Time of Prenatal Androgen Exposure Affects Development of Polycystic Ovary Syndrome-Like Phenotype in Adulthood in Female Rats. Int J Endocrinol Metab. 2014;12(2). doi:10.5812/ijem.16502
35. Davoudi Z, Araghi F, Vahedi M, Mokhtari N, Gheisari M. Prolactin Level in Polycystic Ovary Syndrome (PCOS): an approach to the diagnosis and management. Acta Biomedica Atenei Parmensis. 2021;92(5):e2021291. doi:10.23750/abm.v92i5.9866
36. Li X, Lin S, Yang X, et al. When IGF-1 Meets Metabolic Inflammation and Polycystic Ovary Syndrome. Int Immunopharmacol. 2024;138:112529. doi:10.1016/j.intimp.2024.112529
37. Emanuel RHK, Roberts J, Docherty PD, Lunt H, Campbell RE, Möller K. A review of the hormones involved in the endocrine dysfunctions of polycystic ovary syndrome and their interactions. Front Endocrinol. 2022;13:1017468. doi:10.3389/fendo.2022.1017468
38. Abbott DH, Dumesic DA, Eisner JR, Colman RJ, Kemnitz JW. Insights into the Development of Polycystic Ovary Syndrome (PCOS) from Studies of Prenatally Androgenized Female Rhesus Monkeys. Trends Endocrinol Metab. 1998;9(2):62–67. doi:10.1016/s1043-2760(98)00019-8
39. Birch RA, Padmanabhan V, Foster DL, Unsworth WP, Robinson JE. Prenatal Programming of Reproductive Neuroendocrine Function: fetal Androgen Exposure Produces Progressive Disruption of Reproductive Cycles in Sheep. Endocrinology. 2003;144(4):1426–1434. doi:10.1210/en.2002-220965
40. Steckler TL, Herkimer C, Dumesic DA, Padmanabhan V. Developmental Programming: excess Weight Gain Amplifies the Effects of Prenatal Testosterone Excess On Reproductive Cyclicity—Implication for Polycystic Ovary Syndrome. Endocrinology. 2008;150(3):1456–1465. doi:10.1210/en.2008-1256
41. Manikkam M, Crespi EJ, Doop DD, et al. Fetal Programming: prenatal Testosterone Excess Leads to Fetal Growth Retardation and Postnatal Catch-Up Growth in Sheep. Endocrinology. 2004;145(2):790–798. doi:10.1210/en.2003-0478
42. Wu XY, Li Z, Wu CY, et al. Endocrine Traits of Polycystic Ovary Syndrome in Prenatally Androgenized Female Sprague-Dawley Rats. Endocr J. 2010;57(3):201–209. doi:10.1507/endocrj.k09e-205
43. Demissie M, Lazic M, Foecking EM, Aird F, Dunaif A, Levine JE. Transient prenatal androgen exposure produces metabolic syndrome in adult female rats. Am J Physiol Endocrinol Metab. 2008;295(2):E262–8. doi:10.1152/ajpendo.90208.2008
44. Roland AV, Moenter SM. Reproductive neuroendocrine dysfunction in polycystic ovary syndrome: insight from animal models. Front Neuroendocrinol. 2014;35(4):494–511. doi:10.1016/j.yfrne.2014.04.002
45. Aten S, Ramirez-Plascencia O, Blake C, et al. A time for sex: circadian regulation of mammalian sexual and reproductive function. Front Neurosci. 2025;18:1516767. doi:10.3389/fnins.2024.1516767
46. Alonge MM, Greville LJS, Ma X, Faure PA, Bentley GE. Acute restraint stress rapidly impacts reproductive neuroendocrinology and downstream gonad function in big brown bats (Eptesicus fuscus). J Exp Biol. 2023;226(19). doi:10.1242/jeb.245592
47. Noble D. A theory of biological relativity: no privileged level of causation. Interface Focus. 2011;2(1):55–64. doi:10.1098/rsfs.2011.0067
48. Hossain MA, Al Amin M, Hasan MI, et al. Bioinformatics and system biology approaches to identify molecular pathogenesis of polycystic ovarian syndrome, type 2 diabetes, obesity, and cardiovascular disease that are linked to the progression of female infertility. Inf Med Unlocked. 2022;30:100960. doi:10.1016/j.imu.2022.100960
49. Brankin V, Quinn RL, Webb R, Hunter MG. Evidence for a functional bone morphogenetic protein (BMP) system in the porcine ovary. Domest Anim Endocrinol. 2005;28(4):367–379. doi:10.1016/j.domaniend.2005.01.001
50. Sewer MB, Li D. Regulation of Steroid Hormone Biosynthesis by the Cytoskeleton. Lipids. 2008;43(12):1109–1115. doi:10.1007/s11745-008-3221-2
51. Bizzarri M, Cucina A, Dinicola S, et al. Does myo-inositol effect on PCOS follicles involve cytoskeleton regulation? Med Hypotheses. 2016;91:1–5. PMID: 27142131. doi:10.1016/j.mehy.2016.03.014
52. Tajima K, Orisaka M, Yata H, Goto K, Hosokawa K, Kotsuji F. Role of granulosa and theca cell interactions in ovarian follicular maturation. Microsc Res Tech. 2006;69(6):450–458. doi:10.1002/jemt.20304
53. Gier HT, Marion GB. Formation of the bovine corpus luteum. J Dairy Sci. 1961;44:1187–1192.
54. Skinner MK. Regulation of primordial follicle assembly and development. Hum Reprod Update. 2005;11(5):461–471. doi:10.1093/humupd/dmi020
55. Castrillon DH, Miao L, Kollipara R, Horner JW, DePinho RA. Suppression of Ovarian Follicle Activation in Mice by the Transcription Factor Foxo3a. Science. 2003;301(5630):215–218. doi:10.1126/science.1086336
56. Yang JL, Zhang CP, Li L, et al. Testosterone Induces Redistribution of Forkhead Box-3a and Down-Regulation of Growth and Differentiation Factor 9 Messenger Ribonucleic Acid Expression at Early Stage of Mouse Folliculogenesis. Endocrinology. 2010;151(2):774–782. doi:10.1210/en.2009-0751
57. Shelton JG, Steelman LS, White ER, McCubrey JA. Synergy between PI3K/Akt and Raf/MEK/ERK pathways in IGF-1R mediated cell cycle progression and prevention of apoptosis in hematopoietic cells. Cell Cycle. 2004;3(3):372–379. PMID: 14726697.
58. Knapczyk-Stwora K, Grzesiak M, Slomczynska M. In utero exposure to the anti-androgen flutamide influences connexin 43 and β-catenin expression in porcine fetal gonads. Domest Anim Endocrinol. 2013;44(4):185–194. doi:10.1016/j.domaniend.2013.02.001
59. Wu CH, Yang JG, Yang JJ, et al. Androgen excess down-regulates connexin43 in a human granulosa cell line. Fertil Sterility. 2010;94(7):2938–2941. doi:10.1016/j.fertnstert.2010.06.077
60. Logan KA, Juengel JL, McNatty KP. Onset of Steroidogenic Enzyme Gene Expression During Ovarian Follicular Development in Sheep. Biol Reprod. 2002;66(4):906–916. doi:10.1095/biolreprod66.4.906
61. Vitt UA, Hayashi M, Klein C, Hsueh AJW. Growth Differentiation Factor-9 Stimulates Proliferation but Suppresses the Follicle-Stimulating Hormone-Induced Differentiation of Cultured Granulosa Cells from Small Antral and Preovulatory Rat Follicles. Biol Reprod. 2000;62(2):370–377. doi:10.1095/biolreprod62.2.370
62. Franks S, Gilling-Smith C, Watson H, Willis D. Insulin action in the normal and polycystic ovary. Endocrinol Metab Clinics North Am. 1999;28(2):361–378. doi:10.1016/s0889-8529(05)70074-8
63. Glister C, Satchell L, Bathgate RAD, et al. Functional link between bone morphogenetic proteins and insulin-like peptide 3 signaling in modulating ovarian androgen production. Proc Natl Acad Sci. 2013;110(15):E1426–35. doi:10.1073/pnas.1222216110
64. Knight PG, Satchell L, Glister C. Intra-ovarian roles of activins and inhibins. Mol Cell Endocrinol. 2012;359(1–2):53–65. doi:10.1016/j.mce.2011.04.024
65. Lenie S, Smitz J. Functional AR Signaling Is Evident in an In Vitro Mouse Follicle Culture Bioassay That Encompasses Most Stages of Folliculogenesis. Biol Reprod. 2009;80(4):685–695. doi:10.1095/biolreprod.107.067280
66. Santen RJ, Brodie H, Simpson ER, Siiteri PK, Brodie A. History of Aromatase: saga of an Important Biological Mediator and Therapeutic Target. Endocr Rev. 2009;30(4):343–375. doi:10.1210/er.2008-0016
67. Jakimiuk A. Aromatase mRNA expression in individual follicles from polycystic ovaries. Mol Hum Reprod. 1998;4(1):1–8. doi:10.1093/molehr/4.1.1
68. Erickso GF, Hsueh AJW, Quigley ME, Rebar RW, Yen SSC. Functional Studies of Aromatase Activity in Human Granulosa Cells from Normal and Polycystic Ovaries*. J Clin Endocrinol Metab. 1979;49(4):514–519. doi:10.1210/jcem-49-4-514
69. Nielsen H, Brixen K, Bouillon R, Mosekilde L. Changes in Biochemical Markers of Osteoblastic Activity during the Menstrual Cycle*. J Clin Endocrinol Metab. 1990;70(5):1431–1437. doi:10.1210/jcem-70-5-1431
70. Andersen CY, Schmidt KT, Kristensen SG, Rosendahl M, Byskov AG, Ernst E. Concentrations of AMH and inhibin-B in relation to follicular diameter in normal human small antral follicles. Hum Reprod. 2010;25(5):1282–1287. doi:10.1093/humrep/deq019
71. Grossman MP, Nakajima ST, Fallat ME, Siow Y. Müllerian-inhibiting substance inhibits cytochrome P450 aromatase activity in human granulosa lutein cell culture. Fertil Steril. 2008;89(5 Suppl):1364–1370. PMID: 17517397. doi:10.1016/j.fertnstert.2007.03.066
72. Pellatt L, Hanna L, Brincat M, et al. Granulosa Cell Production of Anti-Müllerian Hormone Is Increased in Polycystic Ovaries. J Clin Endocrinol Metab. 2007;92(1):240–245. doi:10.1210/jc.2006-1582
73. Catteau-Jonard S, Jamin SP, Leclerc A, Gonzalès J, Dewailly D, Di Clemente N. Anti-Mullerian Hormone, Its Receptor, FSH Receptor, and Androgen Receptor Genes Are Overexpressed by Granulosa Cells from Stimulated Follicles in Women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2008;93(11):4456–4461. doi:10.1210/jc.2008-1231
74. Łebkowska A, Adamska A, Karczewska-Kupczewska M, et al. Serum anti-Müllerian hormone concentration in women with polycystic ovary syndrome and type 1 diabetes mellitus. Metabolism. 2016;65(5):804–811. doi:10.1016/j.metabol.2016.02.005
75. Cadagan D, Khan R, Amer S. Thecal cell sensitivity to luteinizing hormone and insulin in polycystic ovarian syndrome. Reprod Biol. 2016;16(1):53–60. doi:10.1016/j.repbio.2015.12.006
76. Bhatia B, Price CA. Insulin alters the effects of follicle stimulating hormone on aromatase in bovine granulosa cells in vitro. Steroids. 2001;66(6):511–519. doi:10.1016/s0039-128x(00)00218-x
77. Fedeli V, Catizone A, Querqui A, Unfer V, Bizzarri M. The Role of Inositols in the Hyperandrogenic Phenotypes of PCOS: a Re-Reading of Larner’s Results. Int J Mol Sci. 2023;24(7):6296. doi:10.3390/ijms24076296
78. Nestler JE, Jakubowicz DJ, Reamer P, Gunn RD, Allan G. Ovulatory and Metabolic Effects of d-Chiro-Inositol in the Polycystic Ovary Syndrome. N Engl J Med. 1999;340(17):1314–1320. doi:10.1056/NEJM199904293401703
79. Baillargeon JP, Carpentier A. Role of insulin in the hyperandrogenemia of lean women with polycystic ovary syndrome and normal insulin sensitivity. Fertil Sterility. 2007;88(4):886–893. doi:10.1016/j.fertnstert.2006.12.055
80. Hopkins BD, Goncalves MD, Cantley LC. Insulin–PI3K signalling: an evolutionarily insulated metabolic driver of cancer. Nat Rev Endocrinol. 2020;16(5):276–283. doi:10.1038/s41574-020-0329-9
81. Heimark D, McAllister J, Larner J. Decreased myo-inositol to chiro-inositol (M/C) ratios and increased M/C epimerase activity in PCOS theca cells demonstrate increased insulin sensitivity compared to controls. Endocr J. 2014;61(2):111–117. doi:10.1507/endocrj.ej13-0423
82. Shashkin PN, Shashkina EF, Fernqvist-Forbes E, Zhou YP, Grill V, Katz A. Insulin mediators in man: effects of glucose ingestion and insulin resistance. Diabetologia. 1997;40(5):557–563. doi:10.1007/s001250050715
83. Bevilacqua A, Bizzarri M. Inositols in Insulin Signaling and Glucose Metabolism. Int J Endocrinol. 2018;2018:1–8. doi:10.1155/2018/1968450
84. Larner J, Craig JW. Urinary myo-Inositol-to-chiro-Inositol Ratios and Insulin Resistance. Diabetes Care. 1996;19(1):76–78. doi:10.2337/diacare.19.1.76
85. Sun TH, Heimark DB, Nguygen T, Nadler JL, Larner J. Both myo-inositol to chiro-inositol epimerase activities and chiro-inositol to myo-inositol ratios are decreased in tissues of GK type 2 diabetic rats compared to Wistar controls. Biochem Biophys Res Commun. 2002;293(3):1092–1098. doi:10.1016/S0006-291X(02)00313-3
86. Paulick MG, Bertozzi CR. The Glycosylphosphatidylinositol Anchor: a Complex Membrane-Anchoring Structure for Proteins. Biochemistry. 2008;47(27):6991–7000. doi:10.1021/bi8006324
87. Sacchi S, Marinaro F, Tondelli D, et al. Modulation of gonadotrophin induced steroidogenic enzymes in granulosa cells by d-chiroinositol. Reprod Biol Endocrinol. 2016;14(1). doi:10.1186/s12958-016-0189-2
88. Nestler JE. Inositolphosphoglycans (IPGs) as Mediators of Insulin’s Steroidogenic Actions. J Basic Clin Physiol Pharmacol. 1998;9(2–4):197–204. doi:10.1515/jbcpp.1998.9.2-4.197
89. Bevilacqua A, Dragotto J, Lucarelli M, Di Emidio G, Monastra G, Tatone C. High Doses of D-Chiro-Inositol Alone Induce a PCO-Like Syndrome and Other Alterations in Mouse Ovaries. Int J Mol Sci. 2021;22(11):5691. doi:10.3390/ijms22115691
90. Monastra G, Vazquez-Levin M, Bezerra Espinola MS, Bilotta G, Laganà AS, Unfer V. D-chiro-inositol, an aromatase down-modulator, increases androgens and reduces estrogens in male volunteers: a pilot study. Basic Clin Androl. 2021;31(1). doi:10.1186/s12610-021-00131-x
91. Fitzpatrick S, Richards JS. Regulation of Cytochrome P450 Aromatase Messenger Ribonucleic Acid and Activity by Steroids and Gonadotropins in Rat Granulosa Cells*. Endocrinology. 1991;129(3):1452–1462. doi:10.1210/endo-129-3-1452
92. Facchinetti F, Unfer V, Dewailly D, et al. Inositols in Polycystic Ovary Syndrome: an Overview on the Advances. Trends Endocrinol Metab. 2020;31(6):435–447. doi:10.1016/j.tem.2020.02.002
93. Iuorno MJ, Jakubowicz DJ, Baillargeon JP, et al. Effects of D-Chiro-Inositol in Lean Women with the Polycystic Ovary Syndrome. Endocr Pract. 2002;8(6):417–423. doi:10.4158/EP.8.6.417
94. Genazzani AD, Santagni S, Rattighieri E, et al. Modulatory Role of D-Chiro-Inositol (DCI) on LH and Insulin Secretion in Obese PCOS Patients. Gynecol Endocrinol. 2014;30(6):438–443. doi:10.3109/09513590.2014.897321
95. Cheang KI, Baillargeon JP, Essah PA, et al. Insulin-Stimulated Release of D-Chiro-Inositol-Containing Inositolphosphoglycan Mediator Correlates with Insulin Sensitivity in Women with Polycystic Ovary Syndrome. Metabolism. 2008;57(10):1390–1397. doi:10.1016/j.metabol.2008.05.008
96. Nestler JE, Jakubowicz DJ, de Vargas AF, Brik C, Quintero N, Medina F. Insulin Stimulates Testosterone Biosynthesis by Human Thecal Cells from Women with Polycystic Ovary Syndrome by Activating Its Own Receptor and Using Inositolglycan Mediators as the Signal Transduction System. J Clin Endocrinol Metab. 1998;83(6):2001–2005. doi:10.1210/jcem.83.6.4886
97. Nordio M, Bezerra Espinola MS, Bilotta G, Capoccia E, Montanino Oliva M. Long-Lasting Therapies with High Doses of D-chiro-inositol: the Downside. J Clin Med. 2023;12(1):390. doi:10.3390/jcm12010390
98. Asplin I, Galasko G, Larner J. chiro-inositol deficiency and insulin resistance: a comparison of the chiro-inositol- and the myo-inositol-containing insulin mediators isolated from urine, hemodialysate, and muscle of control and type II diabetic subjects. Proc Natl Acad Sci. 1993;90(13):5924–5928. doi:10.1073/pnas.90.13.5924
99. Baptiste CG, Battista MC, Trottier A, Baillargeon JP. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J Steroid Biochem Mol Biol. 2010;122(1–3):42–52. doi:10.1016/j.jsbmb.2009.12.010
100. Nestler JE, Barlascini CO, Matt DW, et al. Suppression of Serum Insulin by Diazoxide Reduces Serum Testosterone Levels in Obese Women with Polycystic Ovary Syndrome*. J Clin Endocrinol Metab. 1989;68(6):1027–1032. doi:10.1210/jcem-68-6-1027
101. Carlomagno G, Unfer V, Roseff S. The D-chiro-inositol paradox in the ovary. Fertil Sterility. 2011;95(8):2515–2516. doi:10.1016/j.fertnstert.2011.05.027
102. Yap A, Nishiumi S, Yoshida K, Ashida H. Rat L6 myotubes as an in vitro model system to study GLUT4-dependent glucose uptake stimulated by inositol derivatives. Cytotechnology. 2007;55(2–3):103–108. doi:10.1007/s10616-007-9107-y
103. Hasegawa I, Murakawa H, Suzuki M, Yamamoto Y, Kurabayashi T, Tanaka K. Effect of troglitazone on endocrine and ovulatory performance in women with insulin resistance–related polycystic ovary syndrome. Fertil Sterility. 1999;71(2):323–327. doi:10.1016/s0015-0282(98)00454-3
104. Palomba S, Falbo A, Di Cello A, Cappiello F, Tolino A, Zullo F. Does metformin affect the ovarian response to gonadotropins for in vitro fertilization treatment in patients with polycystic ovary syndrome and reduced ovarian reserve? A randomized controlled trial. Fertil Sterility. 2011;96(5):1128–1133. doi:10.1016/j.fertnstert.2011.08.020
105. DiNicolantonio JJ, O’Keefe JH. Myo-inositol for insulin resistance, metabolic syndrome, polycystic ovary syndrome and gestational diabetes. Open Heart. 2022;9(1):e001989. doi:10.1136/openhrt-2022-001989
106. Watkins OC, Yong HEJ, Sharma N, Chan SY. A review of the role of inositols in conditions of insulin dysregulation and in uncomplicated and pathological pregnancy. Crit Rev Food Sci Nutr. 2020;62(6):1626–1673. doi:10.1080/10408398.2020.1845604
107. Zhang Y, Li C, Zhang W, Zheng X, Chen X. Decreased Insulin Resistance by Myo-Inositol Is Associated with Suppressed Interleukin 6/Phospho-STAT3 Signaling in a Rat Polycystic Ovary Syndrome Model. J Med Food. 2020;23(4):375–387. doi:10.1089/jmf.2019.4580
108. Agarwal SK, Judd HL, Magoffin DA. A mechanism for the suppression of estrogen production in polycystic ovary syndrome. J Clin Endocrinol Metab. 1996;81(10):3686–3691. doi:10.1210/jcem.81.10.8855823
109. Costantino D, Minozzi G, Minozzi E, Guaraldi C. Metabolic and hormonal effects of myo-inositol in women with polycystic ovary syndrome: a double-blind trial. Eur Rev Med Pharmacol Sci. 2009;13(2):105–110. PMID: 19499845.
110. Emekçi Özay Ö, Özay AC, Çağlıyan E, Okyay RE, Gülekli B. Myo-inositol administration positively effects ovulation induction and intrauterine insemination in patients with polycystic ovary syndrome: a prospective, controlled, randomized trial. Gynecol Endocrinol. 2017;33(7):524–528. doi:10.1080/09513590.2017.1296127
111. Monastra G, Vucenik I, Harrath AH, et al. PCOS and Inositols: controversial Results and Necessary Clarifications. Basic Differences Between D-Chiro and Myo-Inositol. Front Endocrinol. 2021;12:660381. doi:10.3389/fendo.2021.660381
112. Fedeli V, Unfer V, Dinicola S, et al. Inositol Restores Appropriate Steroidogenesis in PCOS Ovaries Both In Vitro and In Vivo Experimental Mouse Models. Cells. 2024;13(14):1171. doi:10.3390/cells13141171
113. Dinicola S, Fabrizi G, Masiello MG, et al. Inositol induces mesenchymal-epithelial reversion in breast cancer cells through cytoskeleton rearrangement. Exp Cell Res. 2016;345(1):37–50. doi:10.1016/j.yexcr.2016.05.007
114. Munir I, Yen HW, Geller DH, et al. Insulin Augmentation of 17α-Hydroxylase Activity Is Mediated by Phosphatidyl Inositol 3-Kinase But Not Extracellular Signal-Regulated Kinase-1/2 in Human Ovarian Theca Cells. Endocrinology. 2004;145(1):175–183. doi:10.1210/en.2003-0329
115. Ikeda Y, Lala DS, Luo X, Kim E, Moisan MP, Parker KL. Characterization of the mouse FTZ-F1 gene, which encodes a key regulator of steroid hydroxylase gene expression. Mol Endocrinol. 1993;7(7):852–860. doi:10.1210/mend.7.7.8413309
116. Blind RD, Suzawa M, Ingraham HA. Direct Modification and Activation of a Nuclear Receptor–PIP2 Complex by the Inositol Lipid Kinase IPMK. Sci Signaling. 2012;5(229):ra44. doi:10.1126/scisignal.2003111
117. Nestler JE, Unfer V. Reflections on Inositol(s) for PCOS Therapy: steps Toward Success. Gynecol Endocrinol. 2015;31(7):501–505. doi:10.3109/09513590.2015.1054802
118. Pizzo A, Laganà AS, Barbaro L. Comparison between effects of myo-inositol and
119. Nordio M, Basciani S, Camajani E. The 40:1 myo-inositol/D-chiro-inositol plasma ratio is able to restore ovulation in PCOS patients: comparison with other ratios. Eur Rev Med Pharmacol Sci. 2019;23(12):5512–5521. doi:10.26355/eurrev_201906_18223
120. Pkhaladze L, Russo M, Unfer V, Nordio M, Basciani S, Khomasuridze A. Treatment of lean PCOS teenagers: a follow-up comparison between Myo-Inositol and oral contraceptives. Eur Rev Med Pharmacol Sci. 2021;25(23):7476–7485. doi:10.26355/eurrev_202112_27447
121. Unfer V, Carlomagno G, Dante G, Facchinetti F. Effects of myo-inositol in women with PCOS: a systematic review of randomized controlled trials. Gynecol Endocrinol. 2012;28(7):509–515. doi:10.3109/09513590.2011.650660
122. Naessen T, Kushnir MM, Chaika A, et al. Steroid profiles in ovarian follicular fluid in women with and without polycystic ovary syndrome, analyzed by liquid chromatography-tandem mass spectrometry. Fertil Sterility. 2010;94(6):2228–2233. doi:10.1016/j.fertnstert.2009.12.081
123. Eden JA, Jones J, Carter GD, Alaghband‐Zadeh J. Follicular fluid concentrations of insulin‐like growth factor 1, epidermal growth factor, transforming growth factor‐alpha and sex‐steroids in volume matched normal and polycystic human follicles. Clin Endocrinol. 1990;32(4):395–405. doi:10.1111/j.1365-2265.1990.tb00879.x
124. Kirilovas D, Chaika A, Bergström M, et al. Granulosa cell aromatase enzyme activity: effects of follicular fluid from patients with polycystic ovary syndrome, using aromatase conversion and [11C]vorozole-binding assays. Gynecol Endocrinol. 2006;22(12):685–691. doi:10.1080/09513590601037535
125. Monastra G, Sambuy Y, Ferruzza S, Ferrari D, Ranaldi G. Alpha-lactalbumin Effect on Myo-inositol Intestinal Absorption: in vivo and In vitro. Curr Drug Deliv. 2018;15(9):1305–1311. doi:10.2174/1567201815666180509102641
126. Montanino Oliva M, Buonomo G, Calcagno M, Unfer V. Effects of myo-inositol plus alpha-lactalbumin in myo-inositol-resistant PCOS women. Jovarian Res. 2018;11(1). doi:10.1186/s13048-018-0411-2
127. Nelson VL, Legro RS, Strauss JF, McAllister JM. Augmented Androgen Production Is a Stable Steroidogenic Phenotype of Propagated Theca Cells from Polycystic Ovaries. Mol Endocrinol. 1999;13(6):946–957. doi:10.1210/mend.13.6.0311
128. Jonard S, Robert Y, Ardaens Y, Dewailly D. Ovarian histology, morphology, and ultrasonography in the polycystic ovary syndrome. In: Azziz R, Nestler JE, Dewailly D, editors. Androgen Excess Disorders in Women: Polycystic Ovary Syndrome and Other Disorders. Totowa, NJ: Humana Press; 2007:183–193.
129. Webber L, Stubbs S, Stark J, et al. Formation and early development of follicles in the polycystic ovary. Lancet. 2003;362(9389):1017–1021. doi:10.1016/s0140-6736(03)14410-8
130. Gilling‐Smith C, Story H, Rogers V, Franks S. Evidence for a primary abnormality of thecal cell steroidogenesis in the polycystic ovary syndrome. Clin Endocrinol. 1997;47(1):93–99. doi:10.1046/j.1365-2265.1997.2321049.x
131. Diamanti-Kandarakis E. Polycystic ovarian syndrome: pathophysiology, molecular aspects and clinical implications. Expert Rev Mol Med. 2008;10:e3. doi:10.1017/S1462399408000598
132. Bizzarri M, Fuso A, Dinicola S, Cucina A, Bevilacqua A. Pharmacodynamics and pharmacokinetics of inositol(s) in health and disease. Expert Opin Drug Metab Toxicol. 2016;12(10):1181–1196. doi:10.1080/17425255.2016.1206887
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.