")
Back to Journals » Vascular Health and Risk Management » Volume 20
Perioperative Vascular Access Mapping in Patients with Hemodialysis: A Comparative Study of Access Navigation and Selection in Jordan
Authors Aljarrah Q , Al Bakkar L , Bakkar S , Abou-Foul AK, Allouh MZ
Received 31 May 2024
Accepted for publication 6 September 2024
Published 13 September 2024 Volume 2024:20 Pages 421—434
DOI https://doi.org/10.2147/VHRM.S480827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Qusai Aljarrah,1 Lujain Al Bakkar,1 Sohail Bakkar,2 Ahmad K Abou-Foul,3 Mohammed Z Allouh4,5
1Department of General Surgery & Vascular Surgery, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2Department of Surgery, Faculty of Medicine, The Hashemite University, Zarqa, 13133, Jordan; 3Institute of Cancer and Genomic Studies, University of Birmingham, Birmingham, UK; 4Department of Anatomy, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 5Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, 15551, United Arab Emirates
Correspondence: Qusai Aljarrah, Department of General Surgery & Vascular Surgery, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan, Tel +962 77 559 3131, Email [email protected] Mohammed Z Allouh, Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, 15551, United Arab Emirates, Tel +971 3 713 7551, Email [email protected]
Purpose: This study aimed to elucidate the impact of three different mapping methods on the outcomes of arteriovenous fistula (AVF), including the traditional physical examination (PE) method, color duplex ultrasonography (CDU) mapping conducted by a radiologist (CDU-R), and CDU mapping performed by the operating surgeon (CDU-S).
Patients and Methods: This retrospective study was conducted at a tertiary center in Jordan. Patients were divided into three groups based on the venous mapping method: PE, CDU-R, and CDU-S. Various outcomes were analyzed, including immediate technical success, clinical adequacy at 3 months, and 1-year patency rates. Additional demographic and clinical factors influencing access patency or contributing to early failure were also examined.
Results: The study included 303 eligible patients: 100 in the PE group, 103 in the CDU-R group, and 100 in the CDU-S group. The overall immediate technical success rate was 72%, which was highest in the CDU-S group (95%, p < 0.001). Additionally, the CDU-S group had the highest clinical access adequacy rate (78%, p < 0.01). Notably, the mapping method also influenced the anatomical location of the AVF, as none of the patients in the radiologist group had a forearm AVF. CDU-R, forearm location, intraoperative arterial calcifications, and operative duration were identified as predictors of AVF failure.
Conclusion: The results suggest that perioperative vascular mapping by the operating surgeon not only results in a higher rate of immediate success but also improves access adequacy and prevents unnecessary delays in providing an effective lifeline for hemodialysis patients. The present study highlights the burden of access failure in these patients and the evolving evidence surrounding preoperative vein mapping.
Keywords: access adequacy, access patency, arteriovenous fistula, hemodialysis, renal disease, vascular mapping
Introduction
Vascular access is a crucial lifeline for patients undergoing hemodialysis (HD).1 Among the available options, autogenous arterio-venous fistula (AVF) remains the gold standard for HD delivery in individuals with end-stage renal disease (ESRD).1 The “Fistula-First” Initiative strongly advocates for the initial prioritization of native AVF.1,2 A mature and adequately functioning AVF is associated with a reduced risk of infections and hospitalizations, and improved patient outcomes.1,3–5
However, it should be noted that the failure rates of AVF can be alarmingly high, with maturation proving to be a challenge in more than 50% of cases.1,4,6,7 This scenario poses a significant risk, potentially prolonging catheter dependence and increasing the likelihood of complications, including central venous stenosis, consequently leading to repeated hospitalizations for access-related issues.1,2 As a result, a considerable portion of the public health burden in the HD population is attributed to access delivery and maintenance, with access-related hospital admissions accounting for 25% in developed countries.1 Furthermore, there is a substantial financial aspect, with preservation of access patency constituting around 20% of healthcare spending among patients with HD.1
The global prevalence of ESRD is reported to increase significantly in the future, which is most likely due to increased population aging and the prevalence of diabetes.1 In Jordan, there are approximately 975 cases of ESRD per 1,000,000 individuals, reflecting a significant healthcare challenge.8 Given this anticipated rise and the critical nature of managing ESRD, meticulous preoperative planning is paramount.
During the preparation for access surgery, preoperative assessment of the venous system is a crucial step.6,9,10 Traditionally, physical examination has been the primary method of assessment.9,10 Physical examination attempts to identify appropriate veins for AVF creation with constraints that restrict its utility. For instance, a clinical examination does not offer sufficient data regarding the appropriate diameter of veins for AVF development. A venous and arterial diameter >2–2.5 mm is correlated with higher success rates of AVF maturation.11,12 Additionally, clinical examination alone does not typically reveal venous stenosis, thrombosis, arterial wall calcification, or unusual anatomical variations in the venous or arterial system, such as high bifurcation of the brachial artery.13–15
The Dialysis Outcomes and Practice Patterns Study (DOPPS) underscores the critical importance of thorough vascular access training, which involves meticulous preoperative planning of the access site and type.16 Successful creation of the access hinges on a blend of structural, physiological, and hemodynamic factors, in addition to technical proficiency. Real-time visualization by the operating surgeon during ultrasonographic venous mapping is deemed essential for optimal outcomes, as it enables informed decision-making based on immediate findings.9,15,17 Consequently, color duplex ultrasonography (CDU) has become a fundamental diagnostic and therapeutic tool in the care of patients with HD, helping to determine access delivery pathways and expand future access options.6,9 This approach is noninvasive, cost-effective, and readily available; therefore, it is a valuable resource for clinicians.6,10,15 Nevertheless, the success of CDU imaging largely depends on the operator’s skill and experience, which can lead to misinterpretation or delayed implementation of definitive access solutions.9,18
The ongoing debate surrounding the routine use of preoperative CDU mapping in HD access creation is reflected in the evolving international guidelines.6,9 While European societies advocate for the routine use of preoperative CDU mapping, the updated 2019 American Kidney Disease Outcomes Quality Initiative (KDOQI) and the updated 2022 United Kingdom Kidney Association (UKKA) guidelines have adopted a more selective approach.19,20 Despite these guidelines, up to a third of access procedures still fail or mature incompletely, indicating the likely influence of other yet-to-be-determined factors on AVF failure rates.6,9 Apart from CDU, venography is recognized as another valuable tool in the planning of AVF creation.6,13 Venography can aid in excluding central vein stenosis and identifying distal variants, particularly in patients with a prolonged catheter time or previous access failure.13
This study aims to provide a contemporary analysis of three prevalent preoperative methods employed for vascular access planning and creation in Jordan. The analysis includes three distinct groups of patients categorized based on the following preoperative vessel mapping methods: traditional physical examination (PE), CDU mapping conducted by a radiologist (CDU-R), and CDU mapping performed by the operating surgeon (CDU-S). The study examined the influence of these methods on key outcomes, including technical success and clinical adequacy of the AVF access. We hypothesized that ultrasound mapping performed by the operating surgeon results in increased rates of technical success and clinical adequacy of AVF access in patients with ESRD compared to the other two methods.
Materials and Methods
Study Design and Eligibility Criteria
This retrospective comparative single-center study included consecutive patients with ESRD at King Abdullah University Hospital (KAUH). The study was approved by the Jordan University of Science and Technology Institutional Review Board with a waiver of consent due to the retrospective nature of the study. Clinical and laboratory data were obtained from the KAUH electronic database between January 2018 and January 2020. Eligible patients were adults with ESRD who underwent first-time AVF in our center. The patients were divided into three groups based on the preoperative modality of vascular mapping: PE, CDU-R, and CDU-S.
All patients underwent clinical assessment of the arterial segment, including pulse palpation, segmental blood pressure measurement in both arms, and Allen’s test for the palmar arch. It is important to note that we did not routinely scan the arterial tree in patients with palpable distal pulses and symmetrical blood pressures. The venous assessment included a complete gross examination of the veins in the upper limb. Additionally, an inspection of the chest wall for any stigmata of central venous obstruction was conducted. In the CDU-S group, the operating surgeon employed a tourniquet if the veins were not readily apparent or appeared unintended during the ultrasound evaluation.
Mapping in the CDU-R group utilized a 7.5 MHz linear probe with the GE Logiq E9 machine (GE Healthcare, IL), while intraoperative mapping in the CDU-S group was conducted with the portable GE Venue 40 ultrasound machine (GE Healthcare, IL). All AVF procedures were completed under local anesthesia and performed by a team of three consultant vascular surgeons or an experienced transplant surgeon. The operative time was routinely measured from the instant the patient was placed on the operating table until the conclusion of skin closure. Specifically, in the CDU-S group, venous mapping was incorporated into the operative time, which was performed while the patient was still on the operative table.
Outcome Measures
The following three study outcome measures were assessed: early technical success, access clinical adequacy over three months, and access patency over 1-year. Early technical success was determined by the presence or absence of a thrill immediately after surgery, or the occurrence of AVF thrombosis within 24 h. Thrill was defined as a vibratory (buzzing) sensation in the venous outflow segment of the performed access. Access clinical adequacy was defined as successful cannulation of the access circuit and satisfactory HD over 3 months after creation of the vascular access. Access patency was ascertained by access clinical adequacy at 1 year.
Information on the type and anatomical location of AVF access was collected for all patients. Demographic data, including age, sex, race, and body mass index (BMI), in addition to comorbidities, such as diabetes mellitus (DM), hyperlipidemia, hypertension, tobacco use, and the presence or absence of prior central catheter access during AVF placement, were also collected. Furthermore, we investigated whether patients with inadequate access underwent any remedial fistulogram to promote maturation.
Surgical Procedure
The standard practice in our center is to initially create the AVF in the non-dominant arm, only moving to the contralateral arm if all access options in the non-dominant arm fail. If feasible, the preferred location for the AVF was the forearm. Tourniquets were used to assess the veins in the CDU-S group if the veins were not readily apparent or appeared unintended during the ultrasound evaluation. If there was a delay in fistula maturation after 6 weeks of the surgery, the patient was referred to the interventional radiologist to undergo a fistulogram as a remedial procedure.
Statistical Analysis
The investigated variables (factors) were described as the mean ± standard deviation (SD) for continuous variables and the frequency distribution and percentages for categorical variables. Student’s t-test and one-way ANOVA with the least significant difference post hoc were used to compare continuous variables between two and three groups, respectively. In case the assumptions of the one-way ANOVA were not met, we used the non-parametric alternative, Kruskal–Wallis H-test. Pearson’s chi-squared (χ2) test was applied to test the association between the categorical variables. A post hoc residual analysis was also conducted to determine the exact significance within the contingency tables. Additionally, a multivariate logistic regression model was performed to determine the main predictors of failure of clinical adequacy over a 3-month period. Statistical significance was set at p < 0.05. All statistical analyses were performed using IBM SPSS Statistics software (standard version 28.0.0.0, IBM, Armonk, NY, USA).
Results
Demographics and Patient Characteristics
The study comprised 303 patients who were divided into three groups based on the mapping method. The PE group consisted of 100 patients, the CDU-R group included 103 patients, and the CDU-S included 100 patients. The average age of all patients was approximately 55 years. There were no differences in age and sex distribution among the three groups (Table 1). The mean BMI was 26.3 ± 5.4 kg/m2, which was significantly higher in the CDU-S group (p < 0.001) than in the other two groups (Table 1). Regarding the fistula site, most patients had the AVF in their arm (~78%) and the remaining in their forearm (~22%). Interestingly, none of the patients in the CDU-R group had a forearm AVF. Hemodialysis was initiated via a central venous catheter (CVC) in approximately 90% of the patients and through an AVF in the remaining (~10%). All patients in the CDU-R group and 95% of patients in the CDU-S group had initiated their HD through a CVC. Most patients had one (52.5%) or two (28.7%) previous CVCs. Approximately 17% of patients (51 out of 303) started HD urgently, with most of those receiving urgent HD (39 out of 51) being assessed solely based on physical examination (PE group). Additionally, most patients (79.6%) were hospitalized once (35%) or twice (44.6%) per year for HD access (Table 1).
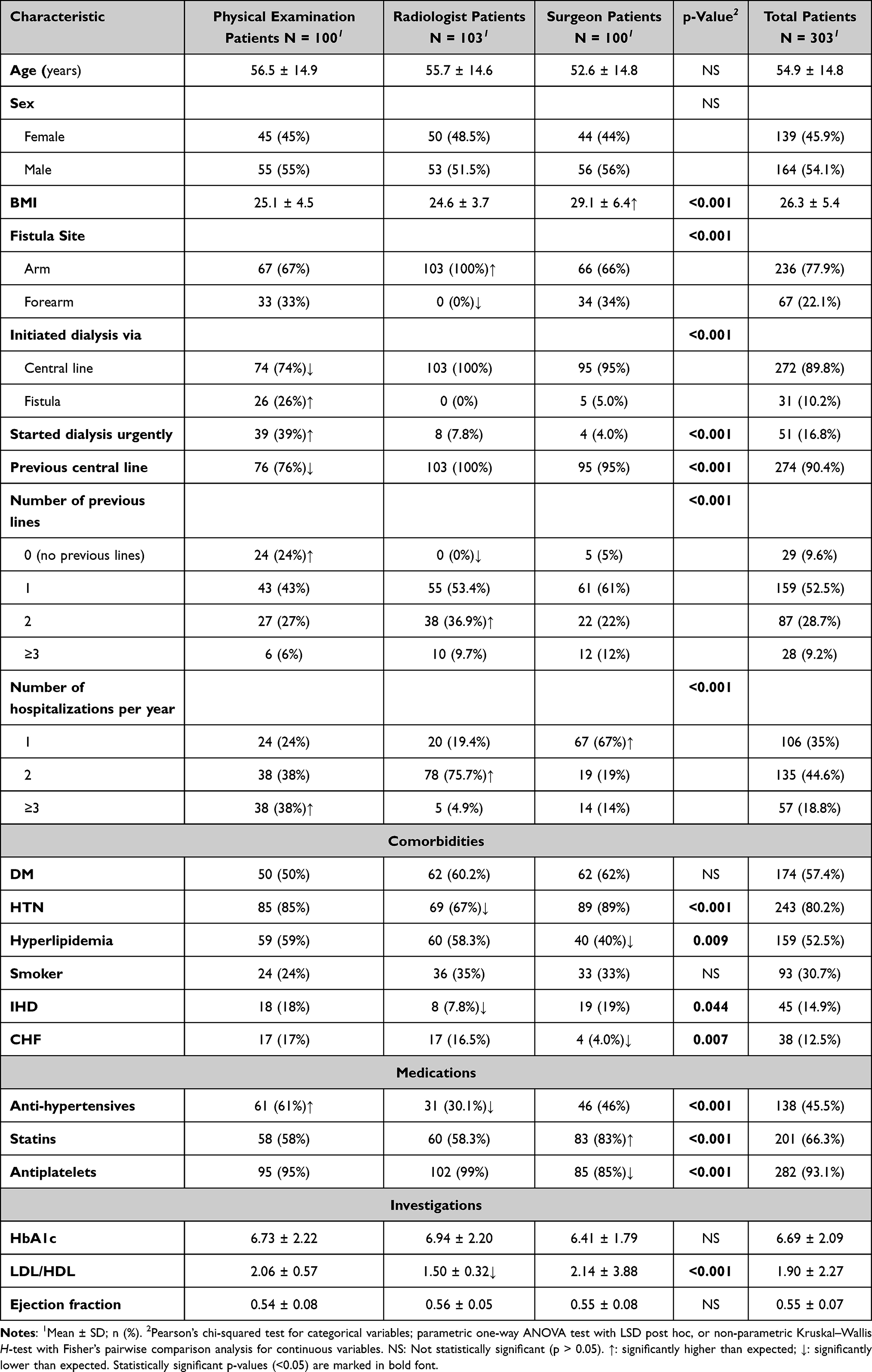 |
Table 1 Demographic and Clinical Characteristics of Patients Referred for Permanent Vascular Access Creation Based on the Mapping Method |
The patients presented with various comorbidities, including DM (57.4%), hypertension (80.2%), hyperlipidemia (52.5%), ischemic heart disease (14.9%), and congestive heart failure (CHF) (12.5%). Approximately one-third of the patients were smokers (30.7%). Furthermore, the CDU-R group exhibited significantly (p < 0.001) lower levels of low-density lipoprotein/high-density lipoprotein ratio than the PE and CDU-S groups. No significant differences were observed in HbA1c and ejection fraction among the three groups (Table 1).
Operative Parameters and Outcomes
There were 61 (20.1%) patients with intraoperative arterial calcifications. More than half of these patients were in the PE group. Thus, the PE group had a significantly (p < 0.001) higher incidence of intraoperative arterial calcifications than the other two groups (Table 2).
 |
Table 2 Perioperative Characteristics and Outcomes |
The average operation duration for all patients was approximately 70 min. The operative duration was significantly (p < 0.001) longer in the PE group than in the CDU-R and CDU-S groups (Table 2). Most patients (~72%) achieved a thrill immediately after surgery. The occurrence of a thrill was significantly (p < 0.001) higher than expected in the CDU-S group than in the other two groups, as 95% of patients in the CDU-S group had a thrill after surgery. Moreover, the CDU-S group had a significantly (p < 0.01) higher frequency of achieving clinical adequacy at 3 months compared to the PE and CDU-R groups. However, clinical adequacy at 3 months was similar between the PE and CDU-R groups (Table 2).
None of the patients in the CDU-R group required a fistulogram as a remedial procedure. Approximately 58% of all patients maintained access patency for 1 year, and the 1-year patency rate did not differ significantly among the three study groups (Table 2).
Clinical Adequacy at 3 Months
The independent factors that might be associated with the clinical adequacy of obtaining dialysis access over a 3-month period are summarized in Table 3. There were no statistical differences in terms of age, sex, and BMI on clinical adequacy. The mapping method was significantly (p < 0.01) associated with clinical adequacy, with the CDU-S group had a higher-than-expected rate (78%) of access success than the other two groups. A significantly (p < 0.001) higher percentage (76.5%) of patients who started dialysis urgently had a failure of dialysis access maturation than patients who did not start urgent dialysis. In addition, the failure to mature dialysis access was significantly (p < 0.01) associated with the presence of previous central lines. Approximately 37% of patients who had previous central lines failed to obtain access, compared to about 10% of those who did not (Table 3). The statistical analysis clearly showed a significant (p < 0.001) association between clinical adequacy and the number of previous lines. Patients who had more previous lines were more likely to have failed access at 3 months postoperative. A similar trend was observed in the hospitalization rate. Patients with a higher number of hospitalizations were more likely (p < 0.001) to have failed access maturation at 3 months postoperative (Table 3).
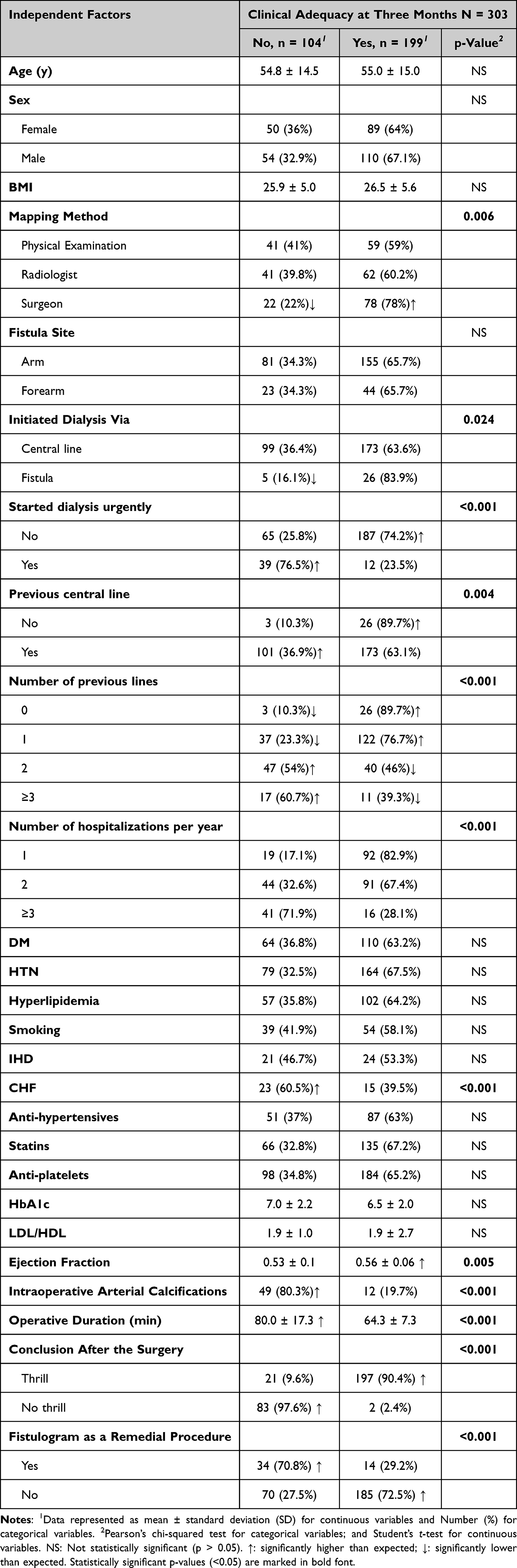 |
Table 3 Analyses of Factors Associated with Clinical Adequacy for Dialysis Access at 3 Months |
Most comorbidities were not associated with clinical adequacy at 3 months, except for CHF. A significantly (p < 0.001) high percentage (60.5%) of patients with CHF failed to develop mature dialysis access. Medications did not show any significant association. Medical investigations, including HbA1c and LDL/HDL, were not associated with access maturity; however, a higher ejection fraction was significantly (p < 0.01) associated with successful access maturity and clinical adequacy at 3 months.
Intraoperative arterial calcification was significantly (p < 0.001) associated with clinical adequacy at 3 months, as most patients with intraoperative arterial calcifications (~80%) failed to achieve mature dialysis access. Additionally, a longer operative duration was significantly (p < 0.001) associated with the failure of clinical adequacy. Patients who failed to obtain dialysis access had a mean operative duration of 80.0 ± 17.3 min compared to a mean duration of 64.3 ± 7.3 min for patients who succeeded in securing access. Most patients with skin thrill immediately after surgery (~90%) succeeded in maturing dialysis access, and most patients without thrill (~98%) failed to obtain mature access.
The requirement of a fistulogram, as a remedial procedure, was inversely/negatively associated (p < 0.001) with clinical adequacy. Approximately 71% of patients who received a fistulogram as a remedial procedure (34 out of 48) failed to develop dialysis access, while 72.5% of patients who did not receive a fistulogram (185 out of 255) succeeded in developing dialysis access over a 3-month period (Table 3).
Finally, a multivariate regression analysis model was performed to confirm the main predictors of failure to obtain dialysis access over a 3-month period (Table 4). The model included the following predictors: mapping method, fistula location, number of previous lines, hospitalization rate, intraoperative arterial calcifications, and operative duration. The model revealed that patients in the CDU-R group had about a seven-fold greater risk of failure to develop dialysis access than patients in the CDU-S group (p < 0.001). Additionally, patients who received the fistula in the forearm had about a three-fold greater risk of failure than patients who received the fistula in the arm (p < 0.05). The number of previous lines and the hospitalization rate were not predictors of access failure. Patients who developed intraoperative arterial calcifications had a significantly (p < 0.001) more than 28-fold higher risk of failure than patients without arterial calcifications. Finally, operative duration was also a significant (p < 0.001) predictor of failure; with every minute increase in the operative duration, there was a 1.145-fold greater risk of failure to secure dialysis access (Table 4).
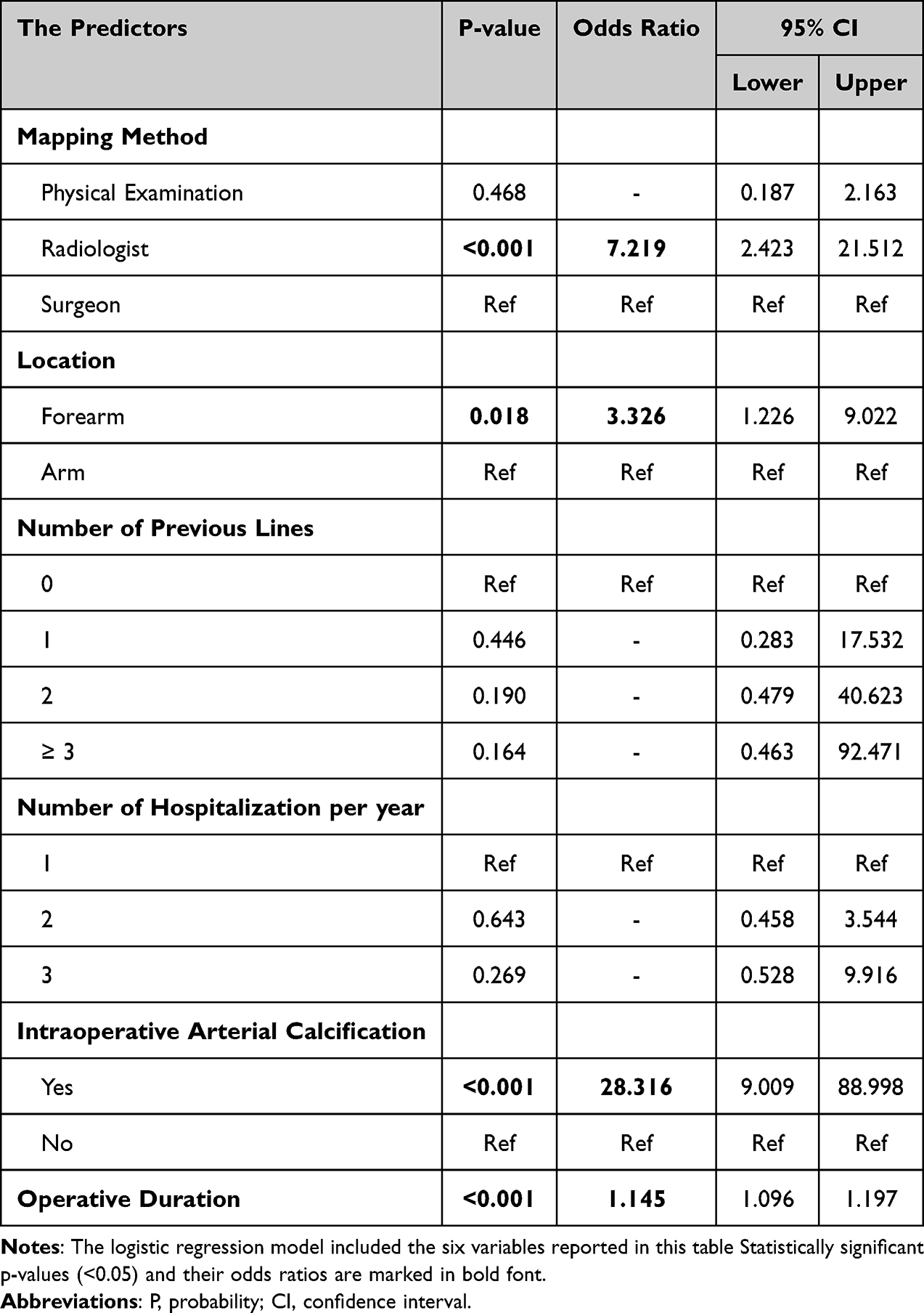 |
Table 4 Multivariate Logistic Regression Model for the Predictors of Failure of the Dialysis Access at a 3-Month Period |
Discussion
The native AVF procedure is widely recognized as the most commonly performed vascular operation.21,22 Despite its prevalence, there is ongoing debate regarding the optimal preoperative planning process.9 The KDOQI guidelines have advocated for a shift in approach, with the goal to move away from a fistula-first strategy toward a patient-centered approach, known as P-L-A-N (Patient Life Plan and their Access Needs).20 This approach emphasizes tailoring vascular access strategies to individual patient circumstances, considering factors such as patient preferences, lifestyle, and clinical considerations. The same guidelines also established three critical domains for successful renal replacement therapy: access creation, access contingency planning, and access succession planning.20 Comprehensively addressing these domains is essential to enhance the quality and longevity of vascular access for patients undergoing HD.6,9 The delineation of the access circuit anatomy is crucial for access contingency and access succession planning. Traditional PE methods miss 75% of the clinically invisible but usable target vasculature for native access formation, especially in obese patients with significant comorbidities.13 Immediate failure rates can be reduced using preoperative CDU mapping,9 with existing evidence showing the potential advantages of preoperative CDU mapping in access surgery.6,9 Additionally, access adequacy can be enhanced by remedial interventions for correctable lesions identified by postoperative ultrasound assessment of the access sites.21 However, CDU has several disadvantages, which include measurement errors due to operator skill, patient inconvenience, higher costs to the health care system, and delays in creating AVF.20
The adage “prior planning prevents poor performance” holds significant value in providing an effective lifeline for patients with HD. Currently, there is a lack of consensus and clinical equipoise in the published data from developed nations regarding the merits of CDU access mapping. Several key points have yet to be determined, including the choice between routine and selective mapping, the timing of mapping (preoperative or intraoperative), and who should be responsible for conducting the study (the operating surgeon or radiologist). The latest KDOQI guidelines recommended the selective use of preoperative ultrasonographic access mapping, as opposed to routine use in previous versions.23 Kosa et al conducted an extensive Cochrane systematic review, which included four randomized controlled trials (RCTs) comparing traditional vein mapping with routine preoperative CDU.23 They found comparable technical success and clinical adequacy, and that similar interventions were required to maintain patency. This aligns with the findings of another previous systemic review.6
It is important to note that data from developing countries is limited, and it may not be appropriate to extrapolate conclusions from existing published data to these nations, which have limited resources. For example, in Jordan, our vascular service lacks a dedicated accredited vascular laboratory, and access mapping is conducted by an overwhelmed radiology department without dedicated vascular slots. As a result, the absence of strict criteria for access mapping in the absence of a dedicated vascular lab could lead to unreliable preoperative navigation and tracking of target vessels. Therefore, access choices in Jordan are solely dependent on the preferences of the surgeons and their informed decisions.
Previous research indicated that access maturation could be influenced by patient age, sex, BMI, diabetic status, and peripheral arterial disease.1,11 Our study findings are comparable with previous studies in that we observed no correlation between AVF adequacy and patient age, sex, and BMI.1,24 Furthermore, diabetic status was not associated with clinical adequacy of the AVF in this study. However, previous studies identified DM as a predictor of AVF non-maturation.25,26 This disparity may be attributed to our relatively younger patient cohort compared to data from developed nations, alongside demographic compositional differences. Notably, CHF was associated with maturation failure in this study. The functionality of an AVF depends on access circuit hemodynamics, including blood flow (ie, cardiac output/inflow) and distribution (ie, venous patency and distensibility).13 Consequently, a higher ejection fraction was associated with adequate access at 3 months. These findings align with previous studies that have associated CHF with poor clinical adequacy.27
Our data unveiled a strikingly high ratio of arm-to-forearm access (236/67). Notably, both the CDU-S and PE groups exhibited similar arm-to-forearm ratios, while surprisingly, the CDU-R group declared null forearm access. The absence of forearm access in the CDU-R group may largely stem from selection bias, where patients with more complex access anatomy or unclear physical exams underwent vein mapping by a radiologist. Moreover, the patient’s intravascular volume may affect venous diameter. Radiologist mapping occurs randomly based on available slots in the radiology department, possibly on the same day as HD when the patient is volume-depleted, whereas surgeon mapping occurs uniformly on the day following HD. Furthermore, the absence of a stringent, predefined mapping protocol and accredited vascular technologist leads to unreliable measurements and inadequate assessment of distensibility when tourniquets are denied for the CDU-R group in our analysis. In a recent analysis by Taubenfeld et al, the authors demonstrated improved vein diameter by intraoperative CDU by the surgeon, ultimately resulting in a nearly two-fold increase in forearm accesses compared to independent preoperative vein mapping by an accredited vascular lab without using a tourniquet in both scans.28 The same study concluded that the use of an intraoperative scan is associated with a 70% increase in vessel diameter compared to preoperative scans.28 Interestingly, 79% of the patients in their study had regional anesthetic blocks, which can augment vein diameter according to previously published data. Furthermore, previous studies identified that intraoperative access mapping following regional anesthesia induces more forearm AVF and improved outcomes when compared to preoperative scanning.29,30 Besides, CDU-R patients are associated with unacceptable delays between mapping and surgery, leading to target vessel consumption and perhaps a flawed interpretation due to phlebitis or thrombosis by the date of surgery. Intraoperative CDU mapping by a surgeon offers a real-time evaluation of target access options. It excludes certain impractical veins at the time of surgery that might have been deemed useful if scanned preoperatively, and avoids futile (blind) surgical explorations.9,15
It is unclear whether the impact of preparative mapping conducted by an independent imaging facility separate from the operator has the same impact as perioperative mapping conducted by the operator who will be creating the AVF. This is an area that needs to be clarified through further research. The data provided by preoperative CDU remains contingent on the expertise of the operator. Our data supports CDU by the operative surgeon as a positive predictor of clinical adequacy. Intraoperative CDU by the surgeon led to more distal access options compared to preoperative CDU by the radiologist, and resulted in a forearm access rate similar to that in the PE group, despite a significantly higher BMI in the CDU-S patient cohort. A previous study with a large patient cohort (n = 46,010) concluded that preoperative vein mapping was associated with improved incident native access placement, greater rates of forearm AVF, and favorable secondary patency.31 Intriguingly, preoperative vein mapping via CDU was employed in >85% of the cases examined in their study. However, the researchers did not investigate whether the mapping was conducted formally in a vascular lab or whether it was performed at the bedside by the surgeon in the operating room. Additionally, Asif et al suggested that vascular access surgeons should perform the CDU mapping.14 The KDOQI guidelines recognize that intraoperative CDU by the surgeon instead of preoperative mapping by a vascular technologist may lead to different AVF locations and outcomes.20 However, no studies have explored this assumption to date. We believe that surgeon judgment remains crucial, and the interpretation of access options is best when the mapping is performed by the operating surgeon, especially in cases with poorly defined vessels on PE. This approach can expedite treatment and has resource implications. Evidence supporting this includes a RCT by Nursal et al, which found no advantage of CDU mapping in patients with favorable forearm vasculature on PE.18 Additionally, this is corroborated by a meta-analysis that showed similar outcomes between different preoperative mapping methods.6 However, a recent meta-analysis revealed that implementing routine preoperative ultrasound mapping of vessels is associated with significantly better outcomes in terms of early arteriovenous fistula failure and primary patency rates at 12 months.32
This study revealed that forearm AVF was associated with a three-fold risk of failure to mature, which is in line with the published literature.24 Forearm veins are smaller in size and inherit occlusive synechiae due to frequent venous catheterization. Furthermore, existing data indicates that achieving clinical adequacy of forearm AVF may take longer than 3 months after access creation.11 As a result, remedial interventions were performed exclusively for patients who received forearm access in the current analysis, due to poor flow and delayed maturation after 6 weeks of AVF. Fistulogram remedial interventions were performed in 30% of CDU-S patients and in 18% of PE patients. Interestingly, none of the CDU-R patients received a remedial Fistulogram. This disparity could be attributed to the utilization of CDU by surgeons proficient in perioperative mapping, enabling prompt identification of correctable access circuit lesions during postoperative surveillance, thus facilitating AVF maturation. These findings are comparable with a previous multicenter research study that also noted approximately one-third of created AVFs necessitated intervention for maturation.33
In this study, the rationale for investigating clinical adequacy at 3 months was to identify parameters that influence access adequacy or are associated with prolonged AVF maturation. The goal was to reduce the duration of catheter dependency and improve HD delivery, ultimately leading to better patient outcomes. By focusing on these factors, strategies can be developed to expedite AVF maturation and decrease reliance on catheters for HD access. However, while forearm access has well-known advantages, the poor maturation rates in previous studies are of concern. Prolonged catheter dependency and frequent hospitalizations can significantly increase the financial burden of HD on healthcare providers. Therefore, addressing factors that affect AVF maturation is crucial for optimizing patient care and managing healthcare costs. Furthermore, it is important to acknowledge that accurate comparisons of published data can be deceptive due to the variation in maturation definitions, study design, predetermined access mapping parameters, and criteria.4
Our data revealed that previous CVC placement and multiple CVC catheters were associated with poor clinical adequacy at 3 months. However, the multivariate regression analysis did not reveal a negative association with the number of CVCs. This observation may raise the question of whether venography is required in patients who have had multiple CVCs or prolonged catheter time. A prospective observational study indicated that CVC use at HD initiation is linked to a higher risk of vascular access failure.34 The study involved a substantial sample of patients with HD (n = 3674) from over 300 institutions across Europe, America, and Japan. However, the authors noted that a causal link between cannulation, catheter utilization, and subsequent AVF failure could not be established due to the observational nature of the study.34
ESRD and DM are identified as predisposing factors for arterial wall calcification.35 Our current analysis revealed that intraoperative arterial calcification significantly predicts clinical adequacy at the 3-month period. Furthermore, arterial calcification is strongly associated with a 28-fold increase in the risk of access failure. These findings are consistent with the existing literature, which highlights the detrimental impact of calcification on access outcomes.10,36 Given these insights, real-time CDU by the operative surgeon is recommended during procedures to avoid calcified inflow segments that may jeopardize clinical adequacy. This may help to mitigate the risk of technical failure and ensure satisfactory inflow.
Our study demonstrated that although CDU-S resulted in improved clinical adequacy at 3 months, the access patency at 1 year was comparable among all groups with different mapping methods. Our findings indicate a 58.1% 1-year patency rate in our cohort, which is consistent with the findings of a previous meta-analysis.37 However, it is lower than the patency rate (71%) reported by another meta-analysis.38 This difference can be attributed to the higher primary failure rate of forearm AVF, which was offset by a lower rate of failures in proximal AVF.
The current study has several limitations. First, its retrospective design and single-center nature may limit the generalizability of the findings. A future RCT is essential to provide robust evidence on whether CDU conducted by the operating surgeon could lead to improved outcomes for patients with ESRD. Second, the lack of standardized ultrasonographic criteria for evaluating target vessels, coupled with variations in operator skills, introduces the potential for misinterpretations. In our study, the analysis of vessel diameter was omitted due to discrepancies in the measurements between the access surgeon and the radiologist, and the different timing at vessel measurement. For instance, the lack of tourniquet use in the CDU-R group, contrary to findings suggesting the beneficial impact of a tourniquet on AVF formation rates.39 The lack of data on vessel diameter may limit comparisons with other studies. In addition, the utilization of different ultrasound machines can alter vessel assessment. Finally, there is, unfortunately, a lack of data on AVF blood flow at the 3-month period. This data could provide valuable insights into the efficacy of each mapping method. Our study exclusively focused on initial AVF, potentially underestimating the benefits of CDU mapping, particularly for patients with a history of unsuccessful prior access surgeries. Addressing these limitations could enhance the reliability and applicability of future research in this area.
Conclusion
In conclusion, in vascular units that lack an accredited vascular laboratory, intraoperative vascular mapping conducted by the operating surgeon is significantly associated with favorable clinical outcomes. CDU by the operating surgeon can lead to improved immediate technical success and a higher chance of access clinical adequacy. On the other hand, relying on preoperative access mapping performed by a radiologist underestimates the available forearm access options, and may result in undue delays in delivering permanent access. The current clinical conundrum requires further investigations to determine whether the true value of intraoperative vascular mapping lies in the skills of the scanning surgeon or in the limitations of the preoperative scanning radiologist. The conscientious use of ultrasonography, in combination with thorough PE, is crucial for achieving positive outcomes.
Abbreviations
AVF, Arterio-venous fistula; BMI, Body mass index; CDU, Color duplex ultrasonography; CHF, Congestive heart failure; CVC, Central venous catheter; DM, Diabetes mellitus; DOPPS, Dialysis Outcomes and Practice Patterns Study; ESRD, End-stage renal disease; KAUH, King Abdullah University Hospital; KDOQI, Kidney Disease Outcomes Quality Initiative; PE, Physical examination; RCT, Randomized controlled trials; SD, Standard deviation; UKKA, United Kingdom Kidney Association.
Data Sharing Statement
The data that support the findings of this study is available from the corresponding authors upon reasonable request.
Ethics Approval and Informed Consent
This is a retrospective cohort study in which we utilized existing data from electronic medical records. Institutional Review Board approval was obtained from KAUH affiliated with Jordan University of Science and Technology. For this type of study, formal and informed consent were waived since data was used in aggregate with no personal identifiers. The study was conducted with the assurance of patient data confidentiality and in accordance with the Declaration of Helsinki and its later amendments for ethical research performance.
Consent for Publication
Not applicable. Data was used in aggregate with no personal identifiers.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allon M, Robbin ML. Increasing arteriovenous fistulas in hemodialysis patients: Problems and solutions. Kidney Int. 2002;62(4):1109–1124. doi:10.1111/j.1523-1755.2002.kid551.x
2. Lee T. Fistula first initiative: Historical impact on vascular access practice patterns and influence on future vascular access care. Cardiovas c Eng Technol. 2017;8(3):244–254. doi:10.1007/s13239-017-0319-9
3. Silva MB, Hobson RW, Pappas PJ, et al. A strategy for increasing use of autogenous hemodialysis access procedures: Impact of preoperative noninvasive evaluation. J Vasc Surg. 1998;27(2):302–307. doi:10.1016/s0741-5214(98)70360-x
4. Siddiqui MA, Ashraff S, Carline T. Maturation of arteriovenous fistula: Analysis of key factors. Kidney Res Clin Pract. 2017;36(4):318–328. doi:10.23876/j.krcp.2017.36.4.318
5. McGill RL, Ruthazer R, Lacson E, Meyer KB, Miskulin DC, Weiner DE. Vascular imaging for hemodialysis vascular access planning. Hemodial Int. 2017;21(4):490–497. doi:10.1111/hdi.12513
6. Wong CS, McNicholas N, Healy D, et al. A systematic review of preoperative duplex ultrasonography and arteriovenous fistula formation. J Vasc Surg. 2013;57(4):1129–1133. doi:10.1016/j.jvs.2012.11.094
7. Roca Tey R. Vascular access for haemodialysis: An unresolved issue. Nefrologia. 2010;30(3):280–287. doi:10.3265/Nefrologia.pre2010.Apr.10349
8. Saleh W. Jordan national registry of end stage renal disease (ESRD), 13th annual report, 2020; 2020. Available from: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://moh.gov.jo/ebv4.0/root_storage/ar/eb_list_page/kidney_report_2020_finale.pdf.
9. Georgiadis GS, Charalampidis DG, Argyriou C, Georgakarakos EI, Lazarides MK. The necessity for routine pre-operative ultrasound mapping before arteriovenous fistula creation: A meta-analysis. Eur J Vasc Endovasc Surg. 2015;49(5):600–605. doi:10.1016/j.ejvs.2015.01.012
10. Shenoy S, Darcy M. Ultrasound as a tool for preoperative planning, monitoring, and interventions in dialysis arteriovenous access. AJR Am J Roentgenol. 2013;201(4):W539–543. doi:10.2214/AJR.13.11277
11. Siddiqui MA, Ashraff S, Santos D, Rush R, Carline T, Raza Z. Predictive parameters of arteriovenous fistula maturation in patients with end-stage renal disease. Kidney Res Clin Pract. 2018;37(3):277–286. doi:10.23876/j.krcp.2018.37.3.277
12. Bashar K, Clarke-Moloney M, Burke PE, Kavanagh EG, Walsh SR. The role of venous diameter in predicting arteriovenous fistula maturation: when not to expect an AVF to mature according to pre-operative vein diameter measurements? A best evidence topic. Int J Surg. 2015;15:95–99. doi:10.1016/j.ijsu.2015.01.035
13. Vachharajani TJ. Pre-access creation evaluation--is vein mapping enough? Adv Chronic Kidney Dis. 2015;22(6):420–424. doi:10.1053/j.ackd.2015.08.002
14. Asif A, Ravani P, Roy-Chaudhury P, Spergel LM, Besarab A. Vascular mapping techniques: Advantages and disadvantages. J Nephrol. 2007;20(3):299–303.
15. Zamboli P, Fiorini F, D’Amelio A, Fatuzzo P, Granata A. Color Doppler ultrasound and arteriovenous fistulas for hemodialysis. J Ultrasound. 2014;17(4):253–263. doi:10.1007/s40477-014-0113-6
16. Goodkin DA, Mapes DL, Held PJ. The dialysis outcomes and practice patterns study (DOPPS): How can we improve the care of hemodialysis patients? Semin Dial. 2001;14(3):157–159. doi:10.1046/j.1525-139x.2001.00043.x
17. Allon M, Lockhart ME, Lilly RZ, et al. Effect of preoperative sonographic mapping on vascular access outcomes in hemodialysis patients. Kidney Int. 2001;60(5):2013–2020. doi:10.1046/j.1523-1755.2001.00031.x
18. Nursal TZ, Oguzkurt L, Tercan F, et al. Is routine preoperative ultrasonographic mapping for arteriovenous fistula creation necessary in patients with favorable physical examination findings? Results of a randomized controlled trial. World J Surg. 2006;30(6):1100–1107. doi:10.1007/s00268-005-0586-8
19. Schmidli J, Widmer MK, Basile C, et al. Editor’s choice - vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(6):757–818. doi:10.1016/j.ejvs.2018.02.001
20. Lok CE, Huber TS, Lee T, et al. KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis. 2020;75(4 Suppl 2):S1–S164. doi:10.1053/j.ajkd.2019.12.001
21. MacRae JM, Oliver M, Clark E, et al. Arteriovenous vascular access selection and evaluation. Can J Kidney Health Dis. 2016;3:2054358116669125. doi:10.1177/2054358116669125
22. Niyyar VD, Wasse H. Vascular mapping: Does it help to maximize fistulae placement? Adv Chronic Kidney Dis. 2009;16(5):316–320. doi:10.1053/j.ackd.2009.06.007
23. Kosa SD, Al-Jaishi AA, Moist L, Lok CE. Preoperative vascular access evaluation for haemodialysis patients. Cochrane Database Syst Rev. 2015;2015(9):CD007013. doi:10.1002/14651858.CD007013.pub2
24. Lauvao LS, Ihnat DM, Goshima KR, Chavez L, Gruessner AC, Mills JL. Vein diameter is the major predictor of fistula maturation. J Vasc Surg. 2009;49(6):1499–1504. doi:10.1016/j.jvs.2009.02.018
25. Almasri J, Alsawas M, Mainou M, et al. Outcomes of vascular access for hemodialysis: A systematic review and meta-analysis. J Vasc Surg. 2016;64(1):236–243. doi:10.1016/j.jvs.2016.01.053
26. Yan Y, Ye D, Yang L, et al. A meta-analysis of the association between diabetic patients and AVF failure in dialysis. Ren Fail. 2018;40(1):379–383. doi:10.1080/0886022X.2018.1456464
27. Lok CE, Allon M, Moist L, Oliver MJ, Shah H, Zimmerman D. Risk equation determining unsuccessful cannulation events and failure to maturation in arteriovenous fistulas. J Am Soc Nephrol. 2006;17(11):3204–3212. doi:10.1681/ASN.2006030190
28. Taubenfeld E, Minjoo Kim YH, Hoffstaetter T, Silpe J, Landis G, Etkin Y. Intraoperative vascular mapping improves patient eligibility for arteriovenous fistula creation. Am J Surg. 2023;225(1):103–106. doi:10.1016/j.amjsurg.2022.09.038
29. Hui SH, Folsom R, Killewich LA, Michalek JE, Davies MG, Pounds LL. A comparison of preoperative and intraoperative vein mapping sizes for arteriovenous fistula creation. J Vasc Surg. 2018;67(6):1813–1820. doi:10.1016/j.jvs.2017.10.067
30. Aitken E, Jackson A, Kearns R, et al. Effect of regional versus local anaesthesia on outcome after arteriovenous fistula creation: A randomised controlled trial. Lancet. 2016;388(10049):1067–1074. doi:10.1016/S0140-6736(16)30948-5
31. Fedorova E, Zhang GQ, Shireman PK, Woo K, Hicks CW. Association of preoperative vein mapping with hemodialysis access characteristics and outcomes in the vascular quality initiative. J Vasc Surg. 2022;75(4):1395–1402. doi:10.1016/j.jvs.2021.10.027
32. Chlorogiannis DD, Bousi SE, Zachiotis M, Chlorogiannis A, Kyriakoulis I, Bellos I. Pre-operative ultrasound mapping before arteriovenous fistula formation: An updated systematic review and meta-analysis. J Nephrol. 2024;37(2):281–292. doi:10.1007/s40620-023-01814-6
33. Huber TS, Berceli SA, Scali ST, et al. Arteriovenous fistula maturation, functional patency, and intervention rates. JAMA Surg. 2021;156(12):1111–1118. doi:10.1001/jamasurg.2021.4527
34. Rayner HC, Pisoni RL, Gillespie BW, et al. Creation, cannulation and survival of arteriovenous fistulae: Data from the dialysis outcomes and practice patterns study. Kidney Int. 2003;63(1):323–330. doi:10.1046/j.1523-1755.2003.00724.x
35. Rocha-Singh KJ, Zeller T, Jaff MR. Peripheral arterial calcification: Prevalence, mechanism, detection, and clinical implications. Catheter Cardiovasc Interv. 2014;83(6):E212–220. doi:10.1002/ccd.25387
36. Roca-Tey R, Bordes R, Martínez-Cercós R, et al. The impact of pre-existing radial artery pathology by histological assessment on the maturation, function and patency of the radiocephalic fistula for hemodialysis. Int Angiol. 2019;38(3):239–249. doi:10.23736/S0392-9590.19.04132-4
37. Bylsma LC, Gage SM, Reichert H, Dahl SLM, Lawson JH. Arteriovenous fistulae for haemodialysis: A systematic review and meta-analysis of efficacy and safety outcomes. Eur J Vasc Endovasc Surg. 2017;54(4):513–522. doi:10.1016/j.ejvs.2017.06.024
38. Al-Jaishi AA, Oliver MJ, Thomas SM, et al. Patency rates of the arteriovenous fistula for hemodialysis: A systematic review and meta-analysis. Am J Kidney Dis. 2014;63(3):464–478. doi:10.1053/j.ajkd.2013.08.023
39. Lockhart ME, Robbin ML, Fineberg NS, Wells CG, Allon M. Cephalic vein measurement before forearm fistula creation: Does use of a tourniquet to meet the venous diameter threshold increase the number of usable fistulas? J Ultrasound Med. 2006;25(12):1541–1545. doi:10.7863/jum.2006.25.12.1541
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.