")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Pharmacokinetics and Safety of Oxycodone/Naloxone Prolonged-Release Tablets in Chinese Patients with Chronic Pain
Authors He Y, Yang L , Mou Q, Cao X, Zhu X, Wang Y, Luo Z
Received 13 July 2024
Accepted for publication 4 April 2025
Published 7 June 2025 Volume 2025:19 Pages 4933—4944
DOI https://doi.org/10.2147/DDDT.S486714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Yongji He,1,2,* Ling Yang,1,2,* Qianqian Mou,1,2 Xiaotao Cao,1,2 Xiaohong Zhu,1,2 Ying Wang,1,2 Zhu Luo1,2
1Department of Pharmacy, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Clinical Trial Center, National Medical Products Administration Key Laboratory for Clinical Research and Evaluation of Innovative Drugs, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhu Luo, Clinical Trial Center, National Medical Products Administration Key Laboratory for Clinical Research and Evaluation of Innovative Drugs, West China Hospital, Sichuan University, No. 37 Guoxue Lane, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86 28 85422707, Email [email protected]
Purpose: The study aimed to assess pharmacokinetics and safety of two oxycodone/naloxone prolonged-release tablet formulations in the Chinese population.
Methods: The study was conducted in 36 Chinese patients with chronic pain in both fasting and fed states. Each state involved a single-dose (40 mg/20 mg), randomized, open-label, two-period crossover clinical trial.
Results: In the fasting study, the mean (± standard deviation, SD) peak concentration (Cmax), area under concentration–time curve from time 0 to the last measurable concentration (AUC0–t) and to infinite time (AUC0–∞), and elimination half-life (t1/2) of oxycodone for the brand-name and generic formulations were 50.9 ± 10.9 and 52.1 ± 9.58 ng/mL, 577 ± 148 and 554 ± 104 h*ng/mL, 579 ± 150 and 556 ± 104 h*ng/mL, and 5.17 ± 0.834 and 5.10 ± 0.877 h, respectively. Both median time to Cmax (Tmax) were 2.00 h. Parameters of naloxone and its main metabolite naloxone-3β-D-glucuronide were Cmax 89.3 ± 20.6 and 85.6 ± 23.4 ng/mL, AUC0–t 547 ± 104 and 538 ± 131 h*ng/mL, AUC0–∞ 552 ± 104 and 543 ± 133 h*ng/mL, and t1/2 6.59 ± 1.77 and 6.00 ± 1.88 h. Both Tmax were 1.00 h. In the fed study, for oxycodone, parameters were Cmax 71.2 ± 10.2 and 82.3 ± 17.1 ng/mL, AUC0–t 697 ± 171 and 696 ± 154 h*ng/mL, AUC0–∞ 699 ± 173 and 698 ± 155 h*ng/mL, and Tmax 2.50 and 3.50 h. Both t1/2 were similar to those in the fasting study. Naloxone and naloxone-3β-D-glucuronide showed similar parameters to those in the fasting study except for Tmax of 2.00 and 2.50 h. No serious adverse events were reported.
Conclusion: The study showed the pharmacokinetic profiles, as well as good safety and tolerability of 40 mg/20 mg oxycodone/naloxone prolonged-release tablets in Chinese subjects, supporting further development and application in the Chinese population.
Keywords: oxycodone, naloxone, pharmacokinetics, Chinese population
Introduction
Chronic pain is the pain lasting for more than 3 months, which is ubiquitous and the prevalence ranges from 16% to 46% across the world.1–6 In China, a study reported the chronic pain prevalence rate of 31.54%.7 Currently, formulating treatment regimens including multiple therapies, such as physical therapies, psychologically based therapies, pharmacotherapies and surgical treatments, based on the characteristics of patients, is widely emphasized in chronic pain management.8 Opioids are an important part of pharmacotherapies.9 Oxycodone, one of the most extensively used opioids, has a relatively selective agonistic effect on μ-opioid receptors, which confers on it the ability to relieve pain.10,11 However, the effect on receptors expressed in the gastrointestinal tract makes patients be faced with drug-related constipation, with the prevalence of more than 22%. One of the strategies to reverse that is to administer oxycodone in combination with the competitive opioid receptor antagonist naloxone to block the agonistic action on opioid receptors.12,13
Oral fixed-dose combination tablets containing prolonged-release oxycodone hydrochloride and naloxone hydrochloride (OXN PR), Targin®, Targinact® or Targiniq® (henceforth also referred to as the brand-name OXN PR; Mundipharma GmbH, Frankfurt, Hesse, Germany), are a good option. Oxycodone has a high oral bioavailability (up to 87%). After oral administration, it is widely distributed throughout the body, with high concentrations in the brain. Given the low concentrations of its metabolites, noroxycodone, oxymorphone and noroxymorphone in the brain, parent oxycodone is regarded as the primary contributor to the analgesic effect.14,15 For naloxone, the first-pass effect gives rise to very low oral bioavailability (<3%) so that its metabolite naloxone-3β-D-glucuronide is the majority form in vivo.16 Hence, following oral administration, naloxone primarily antagonizes the effects of oxycodone on the gastrointestinal tract rather than its analgesic action.13 In contrast, the high concentration of naloxone in the brain following parenteral administration blocks the pharmacodynamic effects of oxycodone on the nervous system, thereby deterring substance abuse.17,18 Furthermore, resistance to crushing or dissolution enhances the abuse-deterrent properties of OXN PR.19
As previously reported, after receiving a single 40 mg/20 mg oral dose of OXN PR, Caucasian populations had mean area under concentration–time curve from time 0 extrapolated to infinite time (AUC0-∞) of 491–506 h*ng/mL, mean peak concentration (Cmax) of 34.5–40.9 ng/mL, median time to peak concentration (Tmax) of 3.0–3.5 h and mean elimination half-life (t1/2) of 3.9–5.3 h for oxycodone, and AUC0-∞ of 0.833 h*ng/mL, Cmax of 0.08 ng/mL, Tmax of 2 h and t1/2 of 4.1–17.2 h for naloxone.17,20 Given the potential effect of race on pharmacokinetics (PK), exploring racial difference is warranted.21 However, no literature reported PK data of the Chinese population, according to the search results on PubMed and Embase. This study aimed to assess PK profiles and safety of the brand-name OXN PR and its generic formulation developed by Shandong Luye Pharma Co., Ltd. (Yantai, Shandong, China) in Chinese patients with chronic pain.
Materials and Methods
Ethics Statement
The study was registered on the Drug Clinical Trial Registration and Information Publicity Platform (http://www.chinadrugtrials.org.cn/index.html; CTR20212790; date of registration: November 1, 2021) and the Chinese Clinical Trial Registry (https://www.chictr.org.cn/; ChiCTR2000029198; date of registration: January 18, 2020). The study protocol, informed consent forms (ICFs) and their amendments were reviewed and approved by the Independent Ethics Committee of West China Hospital, Sichuan University (Chengdu, Sichuan, China). The study was conducted in full accordance with the Declaration of Helsinki, the International Conference on Harmonization–Good Clinical Practice Guidelines and moral, ethical and scientific principles mandated by relevant laws and regulations. Written ICFs were obtained from all subjects. Progress, safety, and endpoints of the study were reviewed by the Data and Safety Monitoring Board.
Study Drugs
The brand-name OXN PR (specifications: 40 mg/20 mg per tablet; batch number: 10001595) was manufactured by Mundipharma GmbH (Frankfurt, Hesse, Germany). The generic OXN PR (specifications: 40 mg/20 mg per tablet; batch number: 202101164) were manufactured by Shandong Luye Pharma Co., Ltd. (Yantai, Shandong, China). The concomitant medication naltrexone hydrochloride tablets (specifications: 50 mg per tablet; batch number: 1158) were manufactured by Haupt Pharma GmbH (Wolfratshausen, Bavaria, Germany). All medications were provided by Shandong Luye Pharma Co., Ltd. (Yantai, Shandong, China).
Subjects
Eligible subjects were patients with non-cancer chronic pain, aged 18 to 55 years old, with body weights greater than 50.0 kg for males and 45.0 kg for females, and body mass index between 19.0 and 28.0 kg/m2. Subjects were required to have a mean pain score of less than 4 on the numerical rating scale within 24 hours prior to screening and not have received any medication in the 14 days before first dosing. Subjects who had received regular fixed-dose acetaminophen or ibuprofen for at least 14 days prior to first dosing were also eligible, if their chronic pain was not completely relieved, with a mean pain score of less than 4. During the study period, the dosing regimens of acetaminophen or ibuprofen remained consistent with the pre-study period. The pain symptoms of patients remained stable for at least 7 days prior to screening and were predicted to remain stable throughout the entire study period. Moreover, at screening, the results, except for symptoms and signs related to pain, of health checks (including blood pressure, heart rate, respiratory rate, body temperature, physical examination, complete blood count, routine urinalysis, comprehensive metabolic panel, 12-lead electrocardiography, and chest X-ray) of enrolled subjects were required to be either normal or, if abnormal, not affecting the study.
Main exclusion criteria included: pregnant or lactating women; allergic constitution or allergy to any ingredient in the medications used in the study or their analogue; diseases or a history of conditions that may affect the subjects’ ability to adhere to the protocol or complete the study; a history or symptoms of orthostatic hypotension; testing positive for hepatitis B surface antigen, hepatitis C virus antibody, Treponema pallidum antibody or human immunodeficiency virus antibody; the administration of any medication in the 14 days prior to the first dosing or during the study period, except for regular fixed-dose acetaminophen or ibuprofen administration for at least 14 days before the study, with dosing regimens remaining consistent throughout the study period; a history of donation or loss of a large amount of blood (more than or equal to 200 mL), or receiving blood transfusion before screening; a history of substance use disorder; tobacco use disorder; alcohol use disorder or alcohol testing positive at screening; intake of food rich in xanthine within 3 days before dosing; intake of any product containing grapefruit and/or pomelo within 7 days before dosing. Subjects had the right to withdraw from the study at any time.
Study Design
The study was divided into fasting and fed studies, both of which were single-center, single-dose, randomized, open-label, two-sequence, two-period and two-crossover clinical trials. Enrolled subjects were randomized in a ratio of 1:1 to the T–R or R–T group (R referred to the brand-name formulation and T referred to the generic formulation). Subjects received a single dose of either the brand-name or generic formulation with 240 mL water orally on Day 1, according to the randomization schedule. After a 7-day washout period, subjects received the second dose on Day 8. In the fasting trial, subjects fasted before and after the administration of OXN PR. In the fed trial, subjects consumed a high-fat meal prior to dosing. One naltrexone hydrochloride tablet was administered to each patient with 100 mL water 12–12.5 h before, 0–0.5 h before and 11.5–12 h after the administration of OXN PR on Day 1 and Day 8. The administration of naltrexone was intended to block the pharmacological action of oxycodone and reduce the incidence of adverse drug effects.22
In the light of the data from the pilot study, the study set the coefficient of intra-individual variation at 20%, T/R ratio at 0.95, two one-sided α at 0.05, β at 0.1 and the interval of bioequivalence (BE) at 80.00%–125.00%. The estimated sample size was 26 subjects for both fasting and fed trials, but accounting for a dropout rate of 25%, the sample size was adjusted to 36 for each trial.
Pharmacokinetic Evaluation and Blood Sampling
Due to the negligible oral bioavailability of naloxone, the plasma concentration of naloxone is very low. According to relevant guidance released by the National Medical Products Administration of China and the United States Food and Drug Administration, naloxone and its main metabolite naloxone-3β-D-glucuronide (henceforth also referred to as total naloxone) in plasma were detected in the study. For oxycodone, only the plasma concentration of parent oxycodone was detected.22,23
PK samples were collected within 1 h predose, at 0.17, 0.33, 0.67, 1, 1.5, 2, 2.5, 3, 3.5, 4, 5, 6, 8, 10, 12, 16, 24, 30, 36 and 48 h postdose on Day 1 and Day 8. A 4 mL blood sample was collected into the pre-cooled K2-EDTA anticoagulant tube every time. After being centrifuged, each plasma sample was separated into 3 cryovials (including two 0.7 mL samples in Cryovial 1 and Cryovial 2 for the detection of oxycodone and total naloxone, respectively, the other sample in a back-up cryovial) and stored at −80°C for further PK analysis.
Plasma concentrations of oxycodone and total naloxone were detected by high performance liquid chromatography–tandem mass spectrometry, with LC-30AD (Shimadzu Corp., Kyoto, Japan) for high performance liquid chromatography and Sciex Triple Quad 6500+ system (AB Sciex LLC, Framingham, Massachusetts, USA) for mass spectrometric detection. The chromatographic column was an Agilent Eclipse Plus C18 (3.5 µm, 4.6×50 mm; Agilent Technologies, Inc., Santa Clara, California, USA) and the mobile phase comprised A (an aqueous solution containing 0.05% formic acid and 10 mM ammonium acetate) and B (methanol) for the detection of oxycodone, whereas the chromatographic column was an Agilent Poroshell HPH C18 (2.7 µm, 2.1×50 mm; Agilent Technologies, Inc., Santa Clara, California, USA) and the mobile phase comprised A (an aqueous solution containing 0.05% ammonia) and B (a mixed solution of methanol/acetonitrile in a volume ratio of 50:50) for the detection of total naloxone. The linear ranges of oxycodone and total naloxone were 0.1–100 and 0.2–200 ng/mL, respectively. The intra-assay and inter-assay precision were less than 9.6% and 9.3%, respectively, for oxycodone, and less than 9.0% and 9.9%, respectively, for total naloxone. The intra-assay and inter-assay accuracy were −3.7% to 15.0% and −1.0% to 8.0%, respectively, for oxycodone, and −11.5% to 2.0% and −6.5% to −4.0%, respectively, for total naloxone.
Safety Assessment
All subjects who had signed ICFs were enrolled in the safety assessment, which consisted of vital signs, physical examination, complete blood count, comprehensive metabolic panel, routine urinalysis, human chorionic gonadotropin blood test, 12-lead electrocardiography, blood oxygen saturation, adverse events (AEs) and serious adverse events (SAEs). AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA, version 25.0).24 Safety assessment was conducted from subjects signing ICFs until the completion of the study, and subjects with AEs were followed up until AEs were eliminated or clinical indicators restored to baseline levels.
Statistical Analysis
PK parameters were calculated by non-compartmental analysis using Phoenix WinNonlin 8.3 (Certara, Princeton, New Jersey, USA), and the other statistical analysis was performed by SAS 9.4 (SAS Institute Inc., Cary, North Carolina, USA). After natural logarithm transformation of Cmax, area under concentration–time curve from time 0 to the time of last measurable concentration (AUC0-t) and AUC0-∞, this study evaluated BE on the basis of linear mixed effects models, with formulation, sequence and period as the fixed effects, and subjects nested in sequence as the random effect. The BE criterion was that the geometric least-squares mean (GLSM) ratios and their 90% confidence intervals (CIs) for Cmax, AUC0-t and AUC0-∞ of the generic OXN PR relative to the brand-name OXN PR should fall within 80.00%–125.00%. If the percentage of the area obtained by extrapolation in AUC0-∞ (AUC_%Extrap) was more than 20%, the corresponding AUC0-∞ was excluded from the BE analysis. The differences in Tmax of the two formulations were tested by Wilcoxon signed-rank test.
Results
Subject Demographics
As shown in Figure 1, 44 subjects were screened and 36 subjects underwent randomization for the fasting study, with 18 subjects assigned to each group. In the fed study, 45 subjects were screened and 36 subjects underwent randomization, with 18 subjects in each group. No subject received any medication other than the study medications. The demographic characteristics of the subjects at baseline are showed in Table 1. One subject in the R–T group of the fed trial dropped out 10 h after the administration of the brand-name OXN PR, due to vomiting.
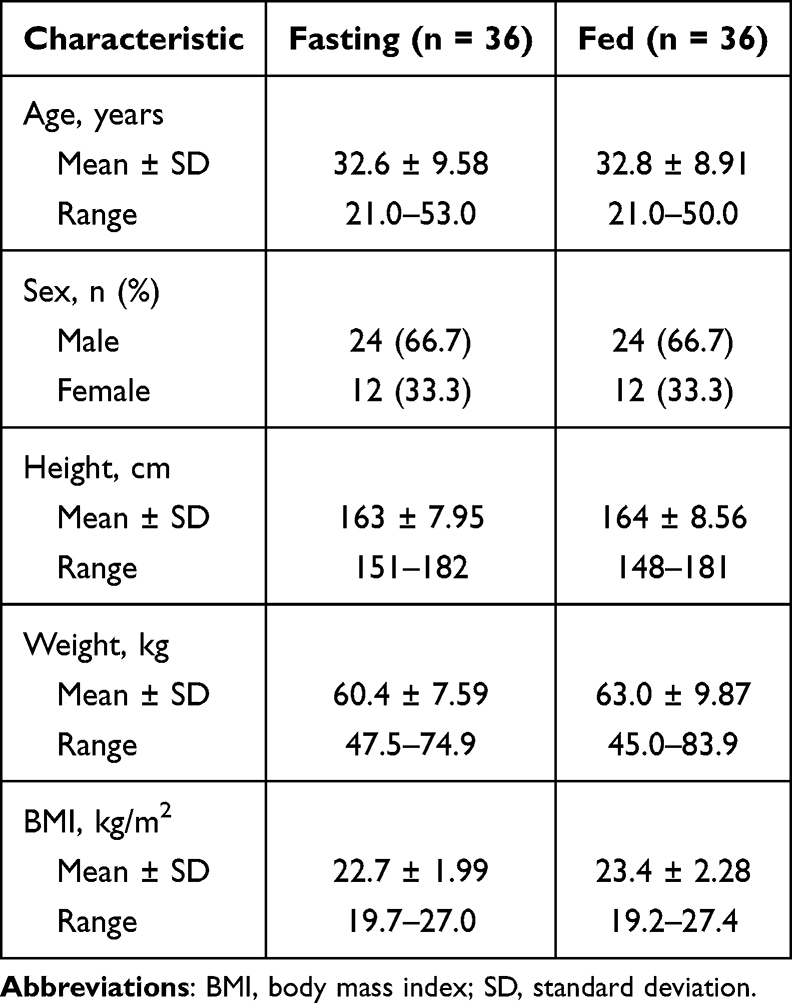 |
Table 1 Demographic Characteristics of the Subjects at Baseline |
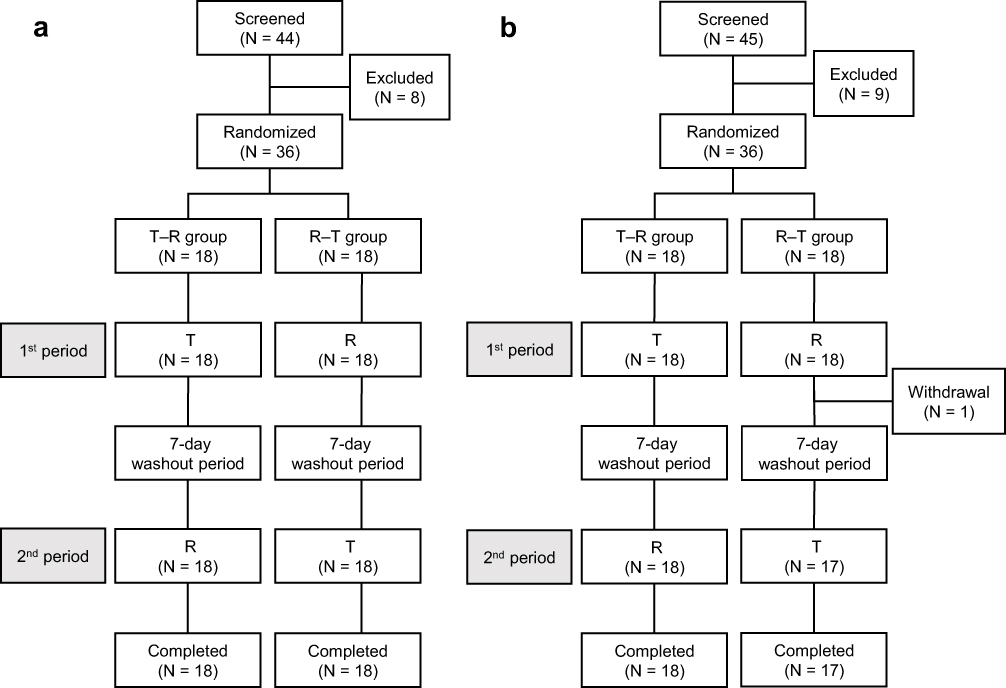 |
Figure 1 The flowchart of the study. (a) In the fasting state. (b) In the fed state. T, receiving a single dose (40 mg/20 mg) of the generic formulation; R, receiving a single dose (40 mg/20 mg) of the brand-name formulation. |
Pharmacokinetics
In the fasting trial, one subject in the T–R group vomited within 12 h following the administration of the generic formulation, and as a result, PK data of the corresponding period were not included in PK parameter analysis and BE analysis. In the fed trial, one subject in the R–T group was not included in PK parameter analysis and BE analysis on account of vomiting and dropping out at 10 h after the first administration of OXN PR. And PK data of one subject taking the generic formulation in the T–R group were excluded from PK parameter analysis and BE analysis owing to vomiting within 12 h after the administration of OXN PR.
The descriptive analysis of PK parameters is shown in Tables 2 and 3. In the fasting study, after oral administration of single-dose OXN PR, oxycodone of both the brand-name and generic formulations were absorbed with the median Tmax of 2.00 h, and total naloxone were absorbed with the median Tmax of 1.00 h. The two formulations showed similar Cmax, AUC0–t, AUC0–∞ and short t1/2 for both oxycodone and total naloxone. In the fed study, the median Tmax of oxycodone and total naloxone of the brand-name formulation (2.50 h and 2.00 h, respectively) were shorter than the generic (3.50 h and 2.50 h, respectively). The mean (± standard deviation, SD) Cmax of oxycodone of the brand-name OXN PR was 71.2 ± 10.2 ng/mL, lower than the generic of 82.3 ± 17.1 ng/mL, while Cmax of total naloxone were similar. There was no obvious difference in AUC0–t and AUC0–∞. The two formulations also showed similar short t1/2 for both oxycodone and total naloxone. The plasma concentration–time curves for the two formulations are showed in Figures 2 and 3.
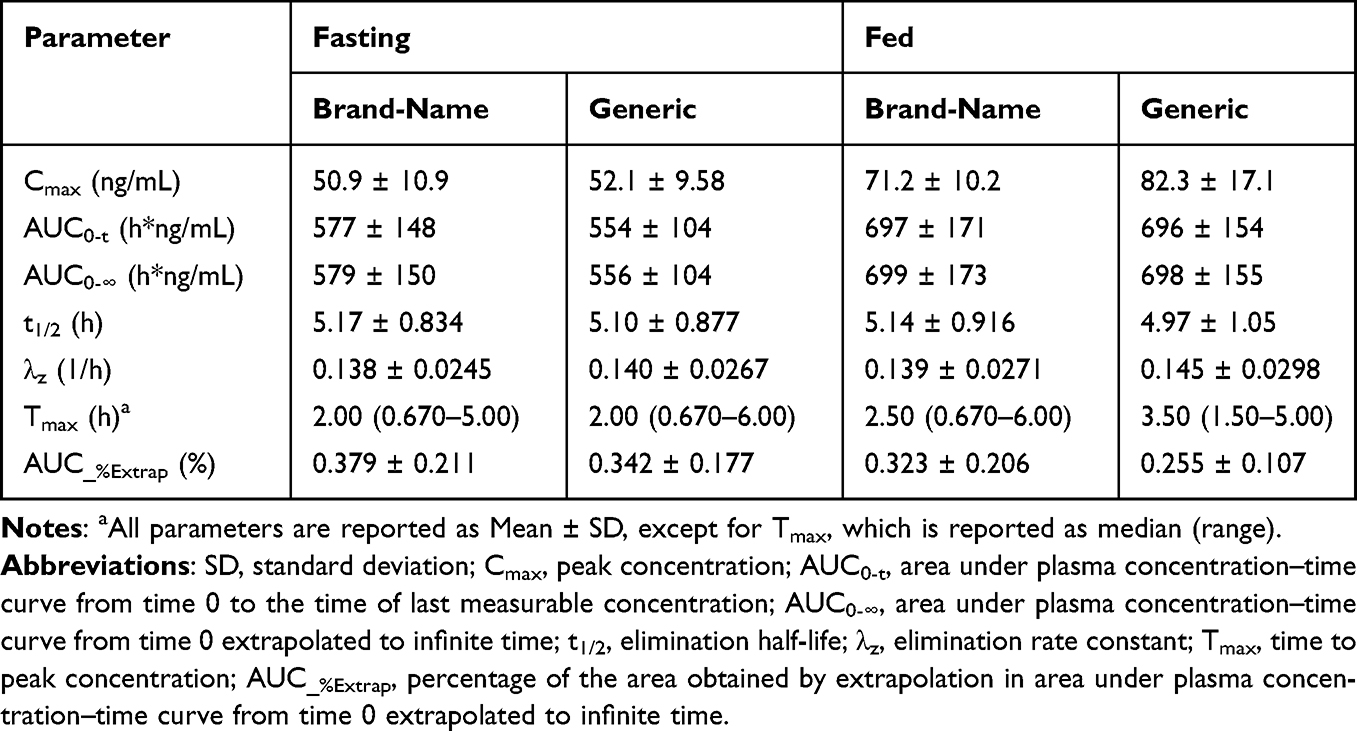 |
Table 2 Pharmacokinetic Parameters of Oxycodone |
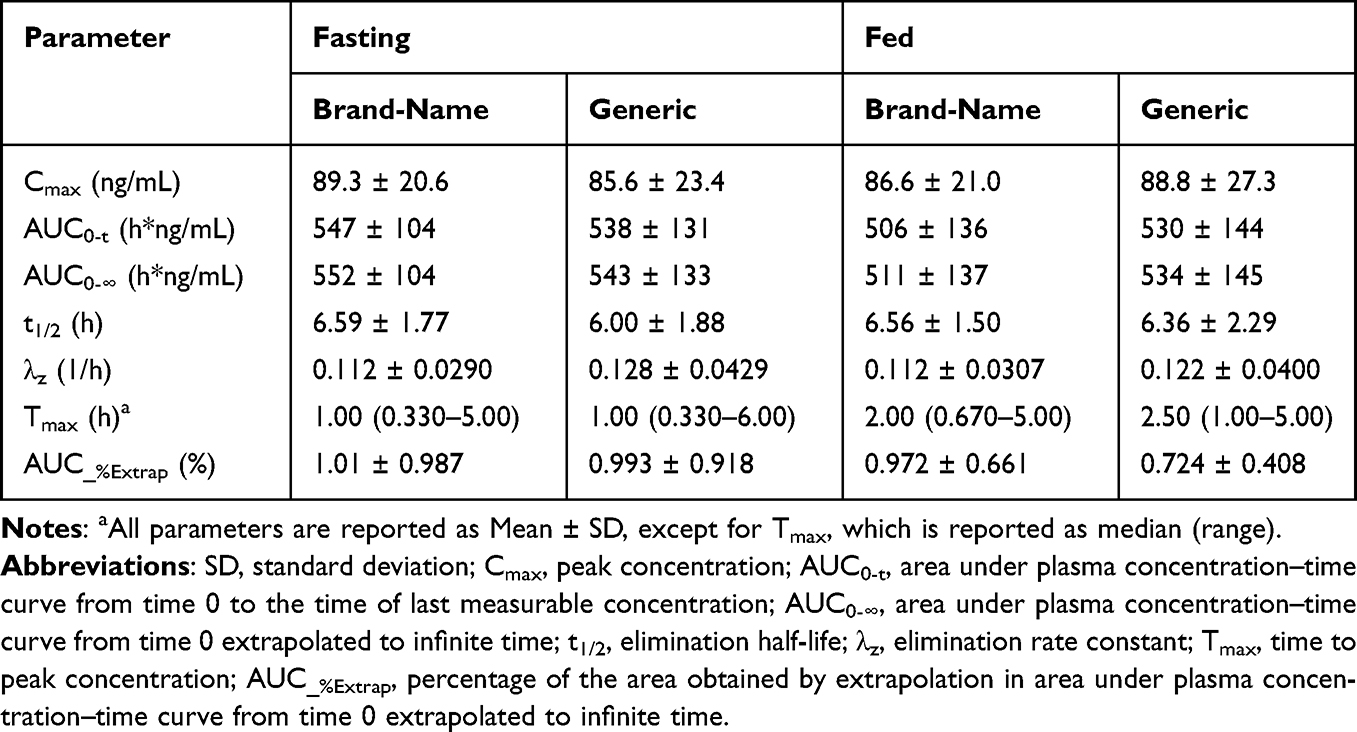 |
Table 3 Pharmacokinetic Parameters of Naloxone and Naloxone-3β-D-Glucuronide |
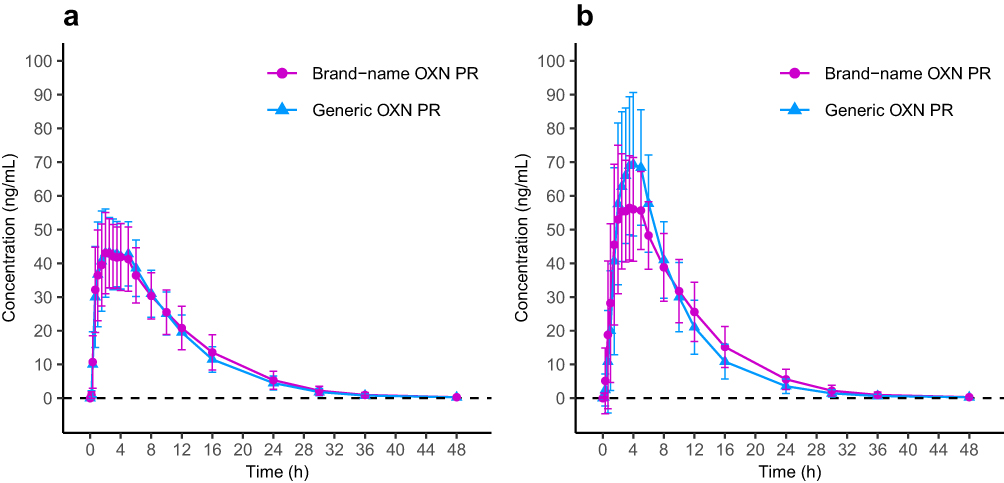 |
Figure 2 Mean (± SD) plasma concentration of oxycodone–time curves. (a) In the fasting state. (b) In the fed state. Abbreviation: OXN PR, oxycodone/naloxone prolonged-release tablets. |
 |
Figure 3 Mean (± SD) plasma concentration of naloxone and naloxone-3β-D-glucuronide–time curves. (a) In the fasting state. (b) In the fed state. Abbreviation: OXN PR, oxycodone/naloxone prolonged-release tablets. |
No formulation, sequence or period effect was found or considered clinically significant. As shown in Table 4, for oxycodone, the GLSM ratios (90% CIs) for Cmax, AUC0–t and AUC0–∞ of the generic relative to the brand-name formulation under the fasting and fed conditions fell within the acceptable BE range of 80.00% to 125.00% (P > 0.05), demonstrating the two formulations were bioequivalent in both the fasting and fed trials. As shown in Table 5, for total naloxone, the two formulations were also bioequivalent in both the fasting and fed trials.
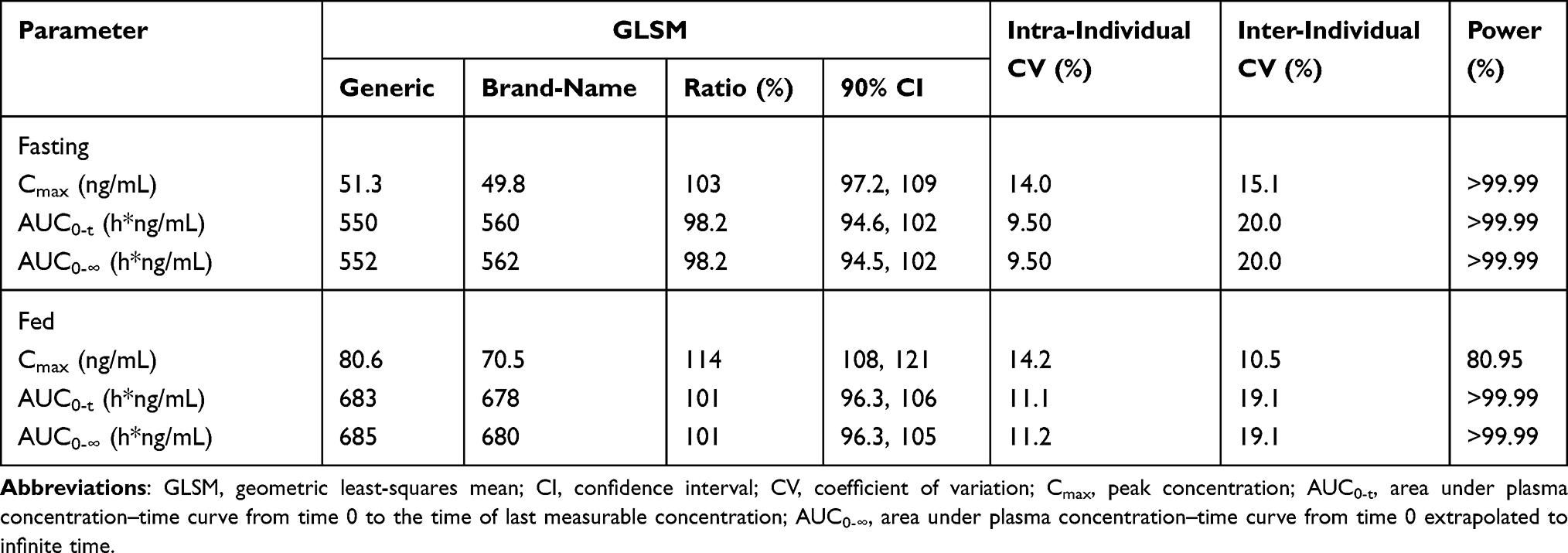 |
Table 4 Bioequivalence Analysis of Primary Pharmacokinetic Parameters of Oxycodone |
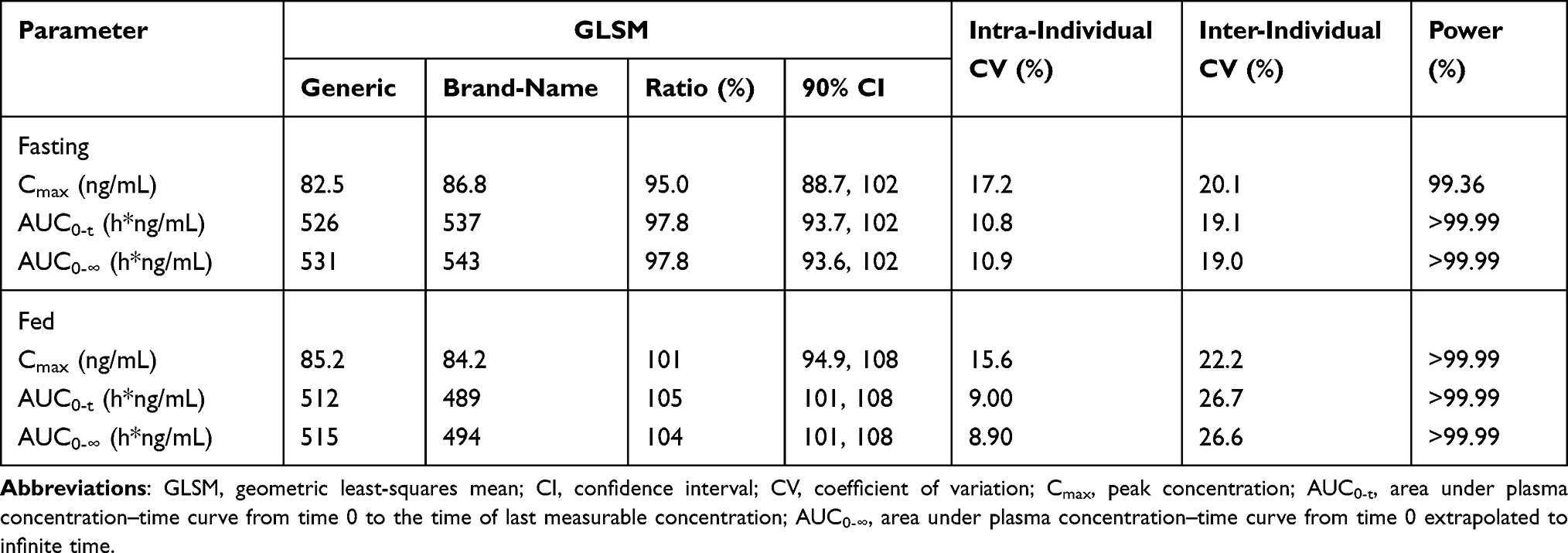 |
Table 5 Bioequivalence Analysis of Primary Pharmacokinetic Parameters of Naloxone and Naloxone-3β-D-Glucuronide |
The Wilcoxon signed-rank test demonstrated that the Tmax of the two formulations in the fasting trial were not statistically different (P = 0.1723 for oxycodone and P = 0.2637 for total naloxone), while the differences in Tmax of the two formulations in the fed trial were statistically significant (P = 0.0101 for oxycodone and P = 0.0204 for total naloxone).
Safety Assessment
All 72 subjects were included in the safety analysis. In the fasting trial, 12 subjects (33.3%) receiving the generic experienced 18 cases of treatment-emergent AEs (TEAEs) and 10 of them (27.8%) experienced 14 cases of TEAEs considered related to the study medications, whereas 11 subjects (30.6%) receiving the brand-name OXN PR experienced 22 TEAEs, 20 of which were related to the study medications. The details of TEAEs are shown in Table 6. The TEAEs considered related to the study medications consisted of dizziness, lethargy, nausea, vomiting, hyperuricaemia, hypotension, asthenia, alanine aminotransferase increased, blood uric acid increased and hyperbilirubinaemia. In the fed trial, 9 subjects (25.7%) receiving the generic experienced 14 cases of TEAEs and 7 of them (20.0%) experienced 10 cases of TEAEs considered related to the study medications, whereas 10 subjects (27.8%) receiving the brand-name OXN PR experienced 19 TEAEs, 9 of whom experienced 14 TEAEs considered related to the study medications. The TEAEs considered related to the study medications comprised dizziness, lethargy, nausea, vomiting, blood pressure decreased and palpitations. All TEAEs were mild, except for 3 moderate TEAEs of 1 subject receiving the brand-name formulation in the fed state, one of which (vomiting) caused this subject dropping out. All TEAEs were resolved without any treatment. Both formulations showed good safety and tolerability in the study.
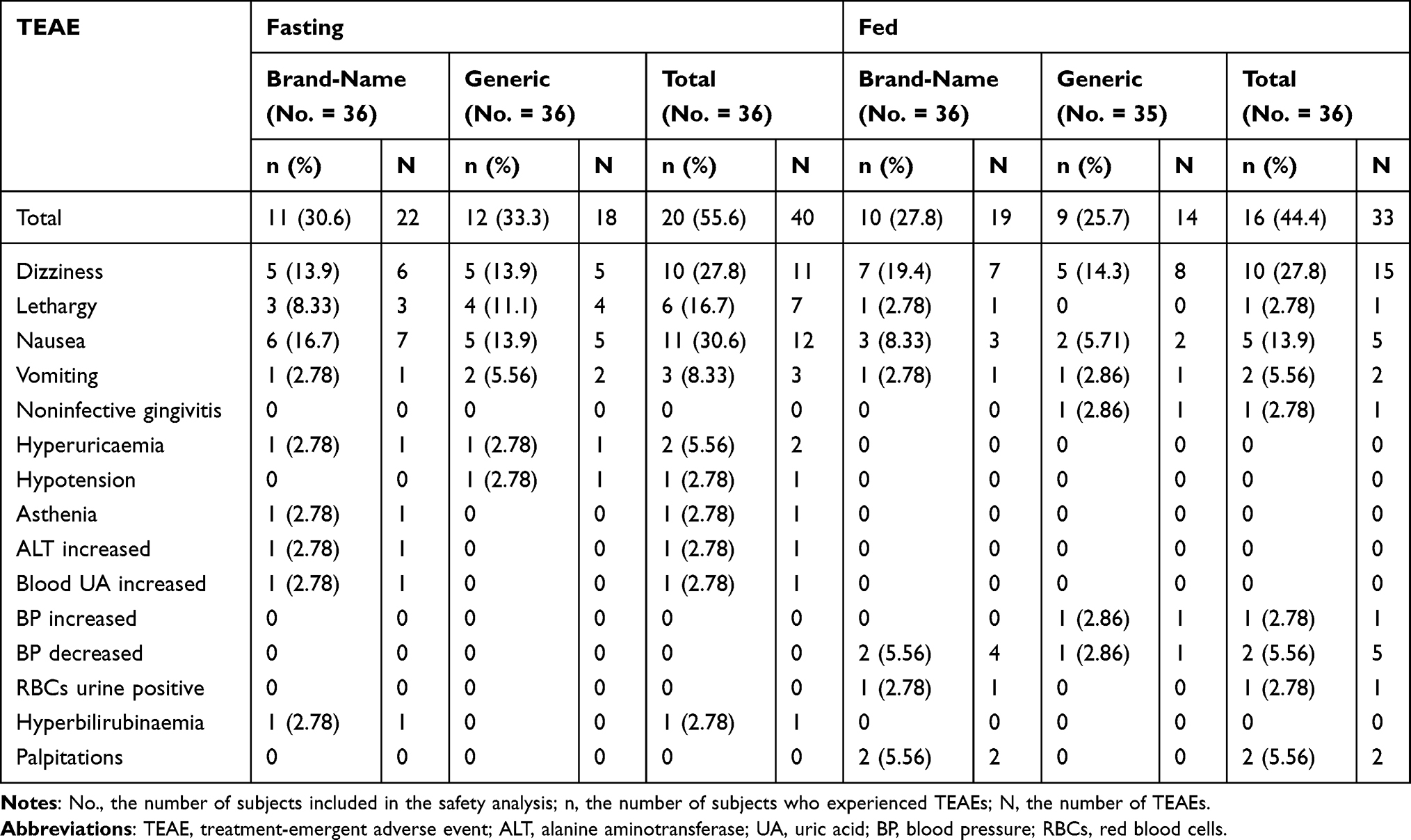 |
Table 6 Summary of Treatment-Emergent Adverse Events |
Discussion
Abuse-deterrent formulations are designed to discourage unexpected routes of abuse. The main strategies of abuse-deterrent formulations are to add excipients to form physical barriers that resist the dosage form from being crushed and chemical barriers that protect the formulation from dissolving, such as high-molecular-weight polyethylene oxide, hydrophobic fatty acid, wax, xanthan gum and hypromellose, and combine opioid agonists with opioid antagonists that exert the antagonistic effects only via unexpected routes of administration.25 The abuse-deterrent property of OXN PR is derived from the hardness and insolubility of the polyethylene oxide matrix tablet after thermal processing and antagonism of oxycodone by naloxone for parenteral use.19 It is reported that the mean oral bioavailability of oxycodone is up to 87% and that of naloxone is less than 3%. As a result, naloxone antagonizes the effect of oxycodone on the gut wall rather than the central nervous system while taking OXN PR orally, which provides pain relief with less constipation. For parenteral use, the high plasma concentration of naloxone confers the abuse-deterrent ability on OXN PR.17
After being absorbed, oxycodone is widely distributed throughout the body. It can cross the blood–brain barrier and produce analgesia in the brain.26 In cerebrospinal fluid, the AUC of oxycodone is higher than that in plasma.15 In the same way, at 5 minutes after intravenous administration, the brain concentration of naloxone is 4.6 times higher than the serum concentration.18 There is evidence suggesting that the uptake of oxycodone and naloxone at the blood–brain barrier involves a pyrilamine-sensitive proton-coupled organic cation (H+/OC) antiporter, and human OATP1A2 is speculated to contribute to naloxone transport.27,28 The main metabolic conversions of oxycodone involve CYP3A4/5 responsible for N-demethylation and CYP2D6 responsible for O-demethylation, which metabolize oxycodone to noroxycodone, oxymorphone and noroxymorphone, but the concentrations of metabolites in the human brain are deemed considerably lower than oxycodone, contributing to very little analgesia.15,26 Glucuronidation via UGT1A8 and UGT2B7 plays a main role in metabolic pathways of naloxone, which converts naloxone to 6β-naloxol, naloxone-3β-glucuronide and 6β-naloxol-3β-glucuronide. Both oxycodone and naloxone are eliminated mainly by metabolism.17
In previous studies, clinical PK profiles of OXN PR were usually assessed in Caucasian populations, but the data are limited in the Chinese population.20,29,30 Our study assessed PK profiles and safety of OXN PR in the Chinese population under the fasting and fed conditions and demonstrated that the brand-name and the generic OXN PR were bioequivalent.
Compared with a study conducted in Hamburg, Germany, AUC0–∞ (579 ± 150 h*ng/mL versus 491 ± 93.5 h*ng/mL) and Cmax (50.9 ± 10.9 ng/mL versus 34.5 ± 5.02 ng/mL) of oxycodone in our Chinese subjects (versus the German subjects in the study) were higher following oral administration of a single 40 mg/20 mg dose of the brand-name OXN PR under fasting conditions, whereas the median Tmax is shorter (2.00 h versus 3.0 h). A population PK study suggested that lean body mass was a significant covariate on the clearance rate and distribution volume, so obviously different weight (60.4 ± 7.59 kg versus 75.5 ± 9.3 kg) was considered to be the cause of different PK profiles on the basis of the similar elimination parameter t1/2 (5.17 ± 0.834 h versus 4.83 ± 0.975 h), and the difference in PK profiles was not deemed clinically significant. For total naloxone, AUC0–∞ (552 ± 104 h*ng/mL versus 528 ± 135 h*ng/mL), Cmax (89.3 ± 20.6 ng/mL versus 62.0 ± 18.4 ng/mL), Tmax (1.00 h versus 1.0 h) and t1/2 (6.59 ± 1.77 h versus 7.81 ± 2.74 h) were also not clinically different between different races.20,31
Minimum toxic concentration of oxycodone is considered to be 200 ng/mL, and the therapeutic range is 5–100 ng/mL. For naloxone, the therapeutic range is 10–30 ng/mL.32 The plasma drug concentrations of the subjects in this study were all within the safe range. One subject receiving the brand-name formulation dropped out because of vomiting, but no SAE was observed in the study. The most common AEs associated with the brand-name and generic formulations in the fasting trial were dizziness, lethargy and nausea, while AEs in the fed trial were dizziness and nausea, which was similar to previous studies.17,20 Both formulations were well safe and tolerated.
Compared with the fasting trial, exposure of oxycodone (Cmax, AUC0–t and AUC0–∞) in the fed trial increased by 40%, 21% and 21%, respectively, and exposure of total naloxone barely changed, which was similar to the previous study.16 The Tmax of oxycodone and total naloxone were delayed slightly, and the effects seemed more obvious to the generic. None of the changes were considered clinically important, and they had no impact on safety.
This study investigated PK profiles and safety of a single 40 mg/20 mg dose of OXN PR in Chinese subjects, enriching the limited PK data in the Chinese population. The results support further development and clinical application, providing a potential treatment for Chinese patients with chronic pain.
However, this study has several limitations. The enrolled subjects were patients with non-cancer chronic pain and a mean pain score of less than 4, but the conditions of patients in clinical practice are so diverse that their PK profiles might be different. The study assessed the safety of a single-dose administration of OXN PR with naltrexone, which did not reflect long-term safety. Therefore, further research is needed to address these limitations.
Conclusion
The study shed light on the pharmacokinetic profiles, as well as good safety and tolerability of both brand-name and generic 40 mg/20 mg oxycodone/naloxone prolonged-release tablets in Chinese subjects, supporting further development and application in the Chinese population.
Data Sharing Statement
Researchers can request access to detailed data by contacting the corresponding author for reasonable research purpose.
Acknowledgments
We are grateful to Shandong Luye Pharma Co., Ltd (Yantai, Shandong, China), as well as all the investigators and subjects who contributed to the study.
Funding
The study was sponsored by Shandong Luye Pharma Co., Ltd (Yantai, Shandong, China). The funding agency had no influence on the objectivity of the study data or the conclusions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
2. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
3. Almalki MT, BinBaz SS, Alamri SS, et al. Prevalence of chronic pain and high-impact chronic pain in Saudi Arabia. Saudi Med J. 2019;40(12):1256–1266. doi:10.15537/smj.2019.12.24690
4. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):e328–e332. doi:10.1097/j.pain.0000000000002291
5. Santiago BVM, Oliveira ABG, Silva GMRD, et al. Prevalence of chronic pain in Brazil: a systematic review and meta-analysis. Clinics. 2023;78:100209. doi:10.1016/j.clinsp.2023.100209
6. Amjad MA, Siddiqui AM, Bashir K, Ghafoor AU, Durrani RS. Prevalence of chronic pain in Pakistan - a national survey. J Pak Med Assoc. 2023;73(6):1217–1220. doi:10.47391/JPMA.6671
7. Yongjun Z, Tingjie Z, Xiaoqiu Y, et al. A survey of chronic pain in China. Libyan J Med. 2020;15(1):1730550. doi:10.1080/19932820.2020.1730550
8. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
9. Scottish Intercollegiate Guidelines Network. Management of Chronic Pain. Rev ed. Edinburgh: Scottish Intercollegiate Guidelines Network; 2019. Available from: https://www.sign.ac.uk/media/2097/sign136_2019.pdf.
10. Barrett JE, Shekarabi A, Inan S. Oxycodone: a current perspective on its pharmacology, abuse, and pharmacotherapeutic developments [published correction appears in Pharmacol Rev. 2023 Dec 15;76(1):195. doi: 10.1124/pharmrev.121.000506err.]. Pharmacol Rev. 2023;75(6):1062–1118. doi:10.1124/pharmrev.121.000506
11. United Nations. Report of the International Narcotics Control Board for 2023. Vienna: United Nations; 2024. Available from: https://www.incb.org/documents/Publications/AnnualReports/AR2023/Annual_Report/E_INCB_2023_1_eng.pdf.
12. Kistemaker KRJ, Sijani F, Brinkman DJ, et al. Pharmacological prevention and treatment of opioid-induced constipation in cancer patients: a systematic review and meta-analysis [published correction appears in Cancer Treat Rev. 2024 Jun;127:102738. doi: 10.1016/j.ctrv.2024.102738.]. Cancer Treat Rev. 2024;125:102704. doi:10.1016/j.ctrv.2024.102704
13. Vijayvargiya P, Camilleri M, Vijayvargiya P, Erwin P, Murad MH. Systematic review with meta-analysis: efficacy and safety of treatments for opioid-induced constipation. Aliment Pharmacol Ther. 2020;52(1):37–53. doi:10.1111/apt.15791
14. Federal Institute for Drugs and Medical Devices. Targin 5 mg/2.5 mg, 10 mg/5 mg, 20 mg/10 mg, 40 mg/20 mg prolonged release tablets: public assessment report; 2009. Available from: https://portal.dimdi.de/amguifree/am/docoutput/additionaldocs.xhtml?mpdidentifier=2173083.
15. Kokki M, Välitalo P, Kuusisto M, et al. Central nervous system penetration of oxycodone after intravenous and epidural administration. Br J Anaesth. 2014;112(1):133–140. doi:10.1093/bja/aet337
16. U.S. Food and Drug Administration Center for Drug Evaluation and Research. Clinical pharmacology and biopharmaceutics review(s): application number: 205777Orig1s000; 2014. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/205777Orig1s000ClinPharmR.pdf.
17. Targiniq® (oxycodone hydrochloride and naloxone hydrochloride) extended-release tablets [prescribing information]. Stamford: Purdue Pharma L.P.; 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/205777s010s011lbl.pdf.
18. Ngai SH, Berkowitz BA, Yang JC, Hempstead J, Spector S. Pharmacokinetics of naloxone in rats and in man: basis for its potency and short duration of action. Anesthesiology. 1976;44(5):398–401. doi:10.1097/00000542-197605000-00008
19. Maincent J, Zhang F. Recent advances in abuse-deterrent technologies for the delivery of opioids. Int J Pharm. 2016;510(1):57–72. doi:10.1016/j.ijpharm.2016.06.012
20. Smith K, Hopp M, Mundin G, et al. Single- and multiple-dose pharmacokinetic evaluation of oxycodone and naloxone in an opioid agonist/antagonist prolonged-release combination in healthy adult volunteers. Clin Ther. 2008;30(11):2051–2068. doi:10.1016/j.clinthera.2008.11.008
21. Roden DM, McLeod HL, Relling MV, et al. Pharmacogenomics. Lancet. 2019;394(10197):521–532. doi:10.1016/S0140-6736(19)31276-0
22. U.S. Food and Drug Administration. Draft guidance on naloxone hydrochloride; oxycodone hydrochloride; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/PSG_205777.pdf.
23. National Medical Products Administration. Technical guidance for human bioequivalence study of chemical generic drugs, with pharmacokinetic parameters as endpoint evaluation indicators; 2016. Available from: https://www.cde.org.cn/zdyz/domesticinfopage?zdyzIdCODE=1e218f70d9b7c99c2663de9f6655bc5b.
24. The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. Medical dictionary for regulatory activities version 25.0; 2022. Available from: https://www.meddra.org/software-package.
25. Litman RS, Pagán OH, Cicero TJ. Abuse-deterrent opioid formulations. Anesthesiology. 2018;128(5):1015–1026. doi:10.1097/ALN.0000000000002031
26. Kinnunen M, Piirainen P, Kokki H, Lammi P, Kokki M. Updated clinical pharmacokinetics and pharmacodynamics of oxycodone. Clin Pharmacokinet. 2019;58(6):705–725. doi:10.1007/s40262-018-00731-3
27. Okura T, Hattori A, Takano Y, et al. Involvement of the pyrilamine transporter, a putative organic cation transporter, in blood-brain barrier transport of oxycodone. Drug Metab Dispos. 2008;36(10):2005–2013. doi:10.1124/dmd.108.022087
28. Suzuki T, Ohmuro A, Miyata M, et al. Involvement of an influx transporter in the blood-brain barrier transport of naloxone. Biopharm Drug Dispos. 2010;31(4):243–252. doi:10.1002/bdd.707
29. Leuppi-Taegtmeyer A, Duthaler U, Hammann F, et al. Pharmacokinetics of oxycodone/naloxone and its metabolites in patients with end-stage renal disease during and between haemodialysis sessions. Nephrol Dial Transplant. 2019;34(4):692–702. doi:10.1093/ndt/gfy285
30. Pesonen A, Hakomäki H, Kokki H, Ranta VP, Rinne V, Kokki M. Breast milk oxycodone concentrations in mothers given oxycodone for post-Caesarean delivery pain management. Br J Clin Pharmacol. 2024;90(4):1183–1192. doi:10.1111/bcp.16008
31. Saari TI, Ihmsen H, Neuvonen PJ, Olkkola KT, Schwilden H. Oxycodone clearance is markedly reduced with advancing age: a population pharmacokinetic study. Br J Anaesth. 2012;108(3):491–498. doi:10.1093/bja/aer395
32. Schulz M, Schmoldt A, Andresen-Streichert H, Iwersen-Bergmann S. Revisited: therapeutic and toxic blood concentrations of more than 1100 drugs and other xenobiotics. Crit Care. 2020;24(1):195. doi:10.1186/s13054-020-02915-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.