")
Back to Journals » Journal of Pain Research » Volume 18
Posterior Percutaneous Endoscopic Cervical Discectomy for Single-Segment Cervical Spondylotic Radiculopathy: A Retrospective Study with Minimum 3-Year Follow-Up
Authors Wang X , Li T, Li Y, Long Y
Received 13 February 2025
Accepted for publication 28 May 2025
Published 9 June 2025 Volume 2025:18 Pages 2879—2888
DOI https://doi.org/10.2147/JPR.S519127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Xiangbin Wang,1,2,* Tao Li,3,* Yong Li,1 Yubin Long1
1Department of Spinal Surgery, Shaoyang Central Hospital, Shaoyang, Hunan, 422000, People’s Republic of China; 2Department of Orthopaedics, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, 830054, People’s Republic of China; 3Department of Spine Surgery and Orthopaedics, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yubin Long, Department of Spinal Surgery, Shaoyang Central Hospital, Shaoyang, Hunan, 422000, People’s Republic of China, Email [email protected] Yong Li, Department of Spinal Surgery, Shaoyang Central Hospital, Shaoyang, Hunan, 422000, People’s Republic of China, Email [email protected]
Background: Posterior percutaneous endoscopic cervical discectomy (P-PECD) has been increasingly used for cervical spondylotic radiculopathy (CSR), while few studies have reported on its medium-long-term outcomes. This study aims to investigate the medium-long-term efficacy and imaging findings of P-PECD in the treatment of single-segment CSR.
Methods: The data of 51 patients with single-segment CSR treated with P-PECD were retrospectively analyzed. Efficacy was evaluated using visual analog scale (VAS) scores of neck and arm, Japanese Orthopaedic Association (JOA) score, neck disability index (NDI), and modified Macnab criteria. Radiologic parameters were measured before and after the operation, including cervical Cobb angle, range of motion (ROM), intervertebral space height, as well as horizontal and angular displacement at the operative level.
Results: The VAS scores of neck and arm, JOA score, and NDI were significantly improved postoperatively compared with those before the operation, and the differences were statistically significant (P < 0.05). Based on the modified Macnab criteria at the final follow-up, 94.12% showed excellent to good outcomes. Postoperatively, the cervical Cobb angle was 10.63 ± 1.79°, ROM was 6.33 ± 1.11°, the intervertebral space height was 4.63 ± 0.85 mm, horizontal and angular displacement at the operative level were 0.88 ± 0.68 mm and 4.25 ± 1.04°, respectively, and there were no significantly changed at the final follow-up.
Conclusion: P-PECD for single-segment CSR has the advantages of less trauma, less bleeding, a low complication rate, faster postoperative recovery, and less impact on cervical mobility and stability, which has excellent medium-long-term efficacy.
Keywords: cervical spondylotic radiculopathy, percutaneous endoscopic, discectomy, minimally invasive
Introduction
Cervical spondylotic radiculopathy (CSR) is the most common degenerative cervical spondylosis (DCS), accounting for about 60%–70% of all DCS. It is a clinical syndrome caused by compression and inflammation of the spinal nerves or nerve roots of the cervical spine due to lateral disc herniation or foraminal stenosis, which has neck and arm pain with numbness, weakness, or altered reflexes.1,2 Cervical spondylotic radiculopathy (CSR) is a debilitating condition characterized by neck pain, radiating arm pain, and sensory/motor deficits due to compression of cervical nerve roots. The pathophysiology often involves intervertebral disc herniation or osteophyte formation, leading to mechanical and inflammatory irritation of neural structures.3
Recent studies highlight the profound impact of CSR on patients’ quality of life, with pain and disability significantly limiting daily activities and occupational function. For instance, Apaydin et al3 demonstrated that even mild to moderate nerve root compression can result in severe neuropathic pain and functional impairment, underscoring the need for timely and effective interventions. Conservative treatments, such as physical therapy and pharmacotherapy, may provide partial relief but often fail to address structural pathology in advanced cases. Surgical intervention is necessary for patients when regular conservative treatment is ineffective or neurological dysfunction progressively worsens. Anterior cervical discectomy and fusion (ACDF) are considered to be the gold standard for the treatment of CSR, while this technique can be accompanied by approach- and fusion-related complications such as dysphagia, postoperative hematoma, recurrent laryngeal nerve injury, and adjacent segment degeneration.4,5 Conventional posterior cervical discectomy does not require additional internal fixation and can maintain the motor function of the cervical spine well, but posterior open surgery requires the dissection of more paraspinal muscles and is prone to residual neck and shoulder pain after surgery.6 Since Rutten first reported posterior percutaneous endoscopic cervical discectomy (P-PECD) for cervical disc herniation or foraminal stenosis with good outcomes in 2007, this technique has gradually emerged and become widely used.4–9 Nevertheless, there are few studies on the medium-long-term outcomes of P-PECD in the treatment of CSR. Thus, we retrospectively analyzed the data of this group of patients to investigate the medium-long-term efficacy and imaging results of P-PECD for single-segment CSR, and summarized the operation points and precautions.
Materials and Methods
General Information
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (approval number: 20170718–15) and performed according to the Declaration of Helsinki. A total of 51 patients (33 males and 18 females) who were diagnosed with CSR and underwent P-PECD at the First Affiliated Hospital of Xinjiang Medical University were included in the study from September 2017 to October 2019, and all patients were informed of the potential risks of the procedure and signed written consent preoperatively. Inclusion criteria: (1) patients had unilateral cervical radiculopathy with pain radiating to the arm, without relief or progressive worsening of symptoms after at least six weeks of standard conservative treatment; (2) the lesion site was lower cervical vertebra (C3-C7), and the presence of a single-segment soft cervical disc herniation or foraminal stenosis detected by magnetic resonance imaging (MRI) and computerized tomography (CT); (3) patients who underwent P-PECD; (4) the postoperative follow-up period ≥12 months. Exclusion criteria: (1) concomitant cervical spondylotic myelopathy or other cervical spine diseases (eg cervical tumor, infection, etc).; (2) imaging showed cervical instability; (3) previous surgery on the lesioned level; (4) lesion levels ≥2; (5) there were contraindications or unable to tolerate surgery.
Surgical Methods
The patients were positioned prone on a surgical bed in reverse Trendelenburg position, the head and shoulders were fixed to the bed with tape to completely straighten the neck, fluoroscopically locate the surgical segment and mark the target disc space and “V” point on the body surface (the junction of the lower edge of superior lamina, the upper edge of inferior lamina, and the medial of facet joint), and applied skin care membranes around the surgical area. The intraoperative operation was started after the surgical area skin was sterilized and waterproof sterile drapings were laid. A puncture needle was inserted through the skin entry point until the tip reached the bone surface of the lamina under radiographic guidance and injected local anesthetic along the puncture track for local anesthesia. Next, made a 7 mm longitudinal incision, a guidewire was placed, the needle was removed, the obturator was introduced along the guidewire, and fluoroscopy was performed to confirm that it was located at the “V” point. Subsequently, the oblique-type working cannula was inserted, and the obturator was removed. At this point, the endoscope irrigation system was introduced through the working cannula and opened. The soft tissue covering the bony surface was cleared with a radiofrequency coagulator, and the bone at the “V” point was ground with high-speed burr. After the outer lamina and cancellous bone were abraded, rongeur was used to remove the inner lamina to expose the outer edge of ligamentum flavum and removed, it to reveal the lateral margins of the dural and traversing nerve root. It is necessary to feel the medial wall of the pedicle with a nerve hook to avoid excessive resection of the facet joint. The herniated nucleus pulposus was explored in the axilla or shoulder of the nerve root using a nerve hook and removed with the nucleus pulposus forceps until the nerve root relaxed. A radiofrequency coagulator was used to shape the annulus fibrosus and to carefully stop the bleeding, and then the channel and endoscope were removed. The drainage catheter placement was decided based on intraoperative bleeding. Finally, the skin incision was sutured and dressed with sterile dressings. All patients reviewed imaging the next day after the procedure and ambulated with the aid of a neck brace. The drainage catheter was removed according to the drainage 24 hours postoperatively. Patients with normal incisions were discharged 2–3 days after the operation and continued to perform standardized functional exercises, which the neck brace could be removed four weeks after surgery and normal neck movement could be restored as well as returned to normal work.
Outcome Measures
General information such as gender, age, operative duration, estimated blood loss, postoperative hospital stay, and time return to work were recorded for the enrolled patients. The efficacy was evaluated using: 1) Visual Analog Scale (VAS) scores (0–10 scale where 0 = no pain and 10 = worst imaginable pain) for neck and arm pain intensity; 2) Japanese Orthopaedic Association (JOA) score (0–17 points evaluating neck function, sensory and motor deficits, with higher scores indicating better function); 3) Neck Disability Index (NDI) (0–50% disability scale derived from 10 patient-reported activity limitations); 4) Modified Macnab criteria (categorical outcomes: excellent/good/fair/poor). The type and incidence of short- and medium-long-term complications were recorded to assess the safety of the procedure. Radiologic evaluation encompassed: a) Cervical Cobb angle – measured between C2 and C7 inferior endplates on lateral radiographs to assess curvature; b) Range of motion (ROM) – angular difference between flexion and extension positions; c) Operative level intervertebral height – distance between adjacent vertebral endplates; d) Dynamic instability parameters: horizontal displacement (anteroposterior translation) and angular displacement (intersegmental angle change) measured on flexion-extension films using vertebral landmark superimposition techniques.10,11 Criteria for cervical instability: the horizontal displacement >3.5 mm and/or angular displacement >11 ° on flexion and extension radiographs.12
Statistical Analysis
The data were statistically analyzed using SPSS 26.0 software. The measurement data conformed to normal distribution were presented as mean ± standard deviation, significant differences in data (VAS, JOA, and NDI) were determined using repeated-measures analysis of variance, and the paired t-test was used to evaluate changes in radiologic parameters. P < 0.05 was considered to be statistically significant.
Results
Basic Condition
A total of 51 patients (33 males and 18 females, mean age were 50.82 ± 7.29 years) who met the criteria were included in our study. The operative levels were all lower cervical vertebra, 13 cases were C4/5, 21 cases were C5/6 and 17 cases were C6/7. All patients completed the procedure successfully, the operative duration was 65.0 ± 8.54 minutes, the estimated blood loss was 30.59 ± 6.68 mL, the postoperative hospital stay was 2.96 ± 1.15 days, and the time return to work was 32.45 ± 6.32 days (Table 1).
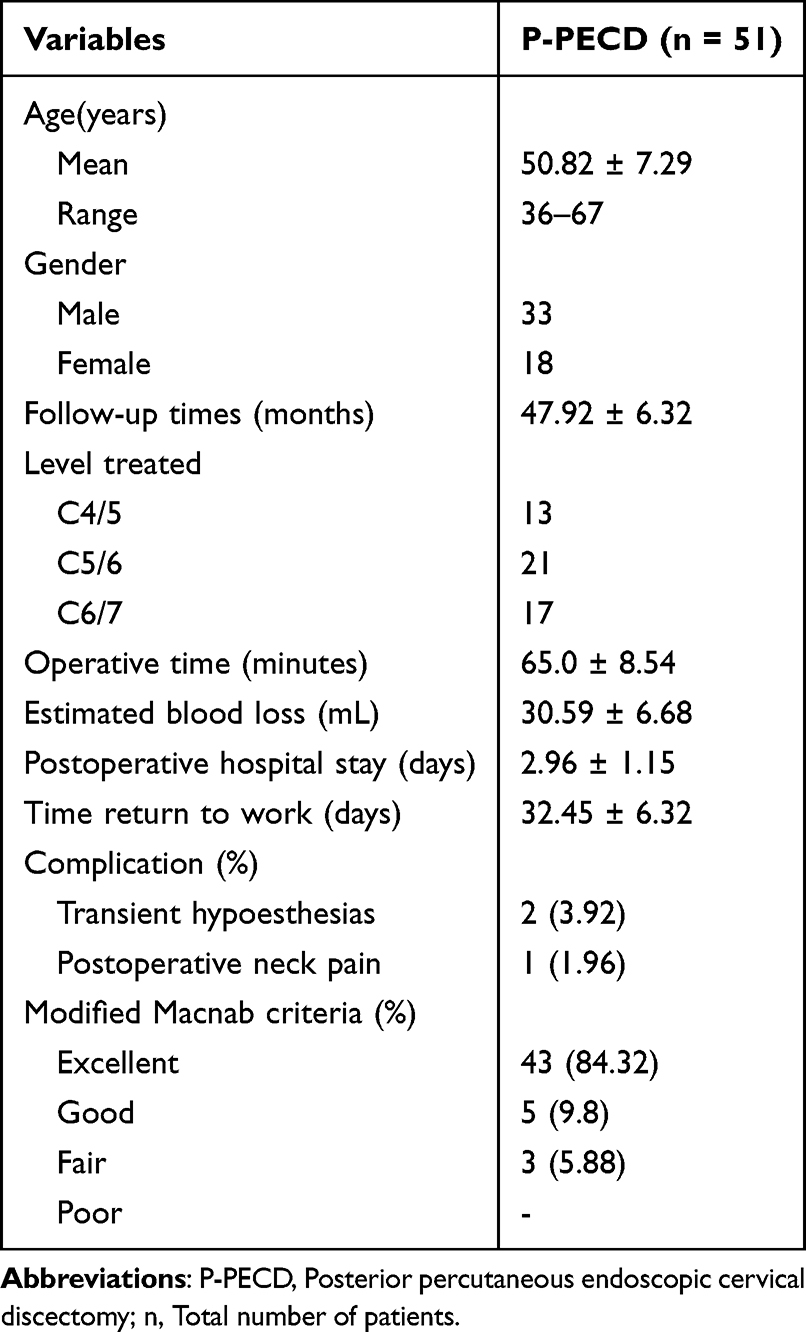 |
Table 1 Summary of the Clinical Data |
Functional Results
The VAS scores of neck and arm, JOA score, and NDI at each follow-up time point after the operation were significantly improved compared with those before the operation, and the differences were statistically significant (P < 0.05) (Table 2). Based on the modified Macnab criteria, the outcomes were excellent in 43 cases (84.32%), good in 5 cases (9.8%), fair in 3 cases (5.88%), none of the patients showed poor outcomes, and excellent and good rate was 94.12% (Table 1).
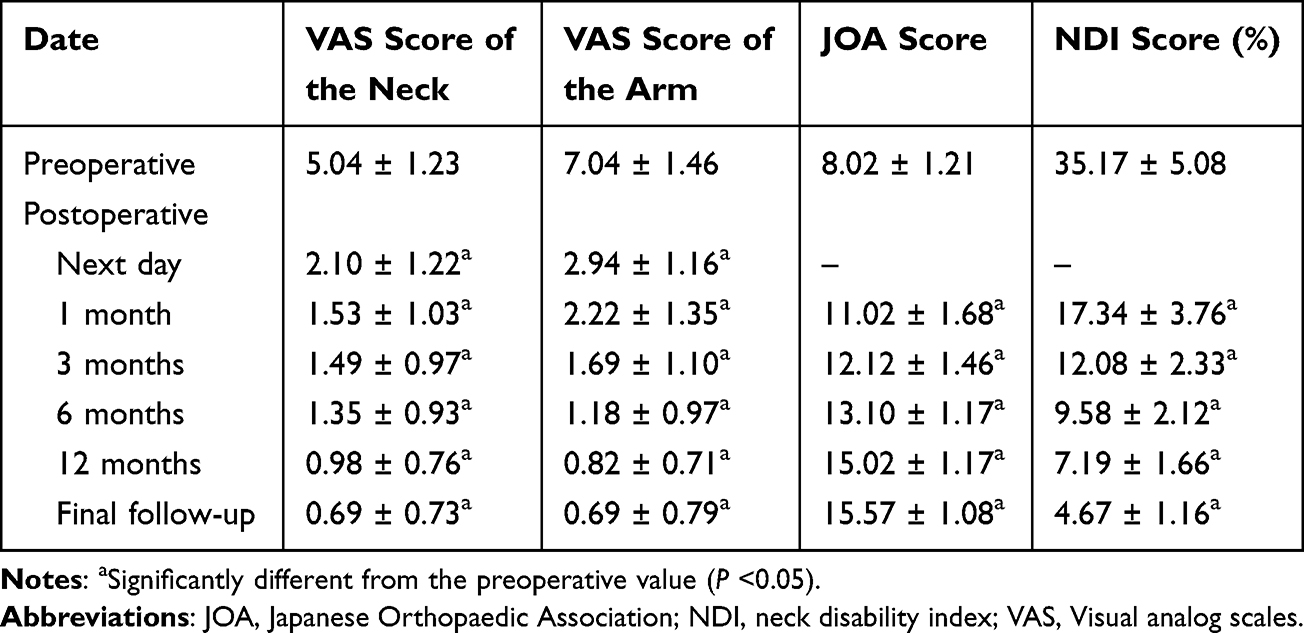 |
Table 2 Comparison of the Functional Score Between Preoperative and Postoperative |
Radiological Results
Postoperatively, the cervical Cobb angle was 10.63 ± 1.79°, ROM was 6.33 ± 1.11°, the intervertebral space height was 4.63 ± 0.85 mm, horizontal and angular displacement at the operative level were 0.88 ± 0.68 mm and 4.25 ± 1.04°, respectively, and there were no significantly changed at the final follow-up (Table 3).
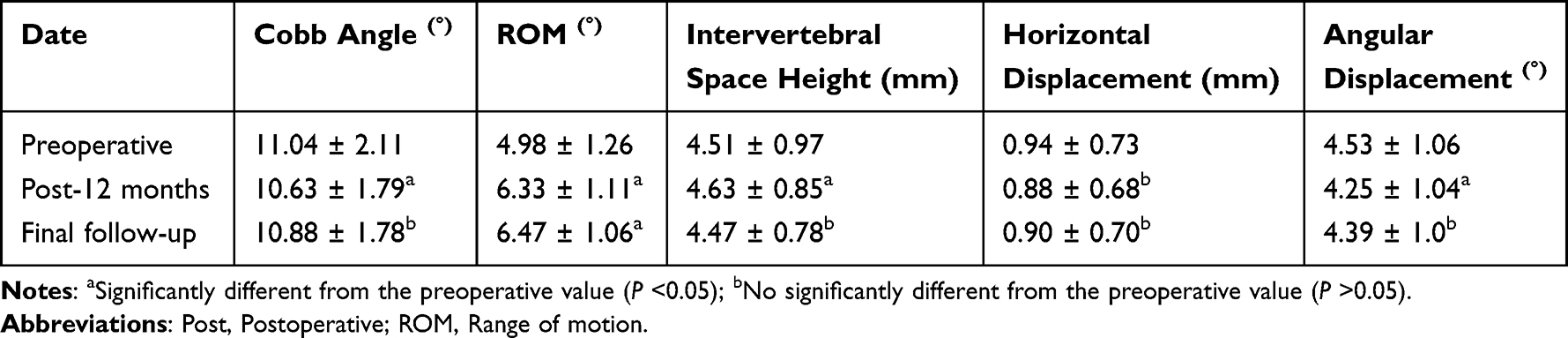 |
Table 3 Comparison of the Radiological Results Between Preoperative and Postoperative |
Complications
We observed 3 (5.88%) cases with complications (Table 1): two cases in transient hypoesthesias, one case in postoperative neck pain, and these symptoms completely disappeared after symptomatic treatment such as dehydration, detumescence, and nutritional nerve. No neurological deterioration, dural tear, cerebrospinal fluid leakage, epidural hematoma, and infections were observed in our patients. All patients had no disc herniation recurrence at each follow-up time point after the procedure, and no segmental instability 12 months postoperatively and the final follow-up (Figure 1).
 |
Figure 1 A 44-year-old female with CSR (C5/6) underwent P-PECD. (a–e). Preoperative imaging studies. (a and b) showed cervical kyphosis, without cervical instability. (c) showed hyperostosis at the posterior margin of the vertebral body. (d and e) showed cervical disc herniation, located in the right foramen region. (f) showed intraoperative fluoroscopy. (g) endoscopic image of the dura and traversing nerve root. (h) a photo of the nucleus pulposus and bone were removed. (i) was CT image two days after the operation, and the range of fenestration was satisfactory. (j and k) showed the nucleus pulposus in the right foramen area was completely removed. (l and m) showed there was no recurrence 3 years after the operation. |
Discussion
Efficacy and Advantages of P-PECD for Single-Segment CSR
Recently, the incidence rate of cervical spondylosis has gradually increased and gotten younger. For symptomatic CSR, conservative treatment is preferred, while surgery is required for regular conservative treatment failure. A large number of studies have confirmed that the posterior cervical endoscopic technique is a safe and effective minimally invasive surgical approach.13–17 Wan et al18 adopted posterior percutaneous full-endoscopic cervical discectomy under local anesthesia for 25 patients with CSR caused by soft-disc herniation in 2018, which all had different degrees of pain relief and improvement of neck function after surgery, without serious complications. The author concluded that P-PECD under local anesthesia can achieve comparable results to surgery under general anesthesia as long as the appropriate cases are selected, the dura and nerve root are adequately decompressed intraoperatively, and the local anesthesia allows for real-time communication with the patient, which makes it a safer operation and less nerve injury. In 2020, Huang et al19 compared the clinical outcomes of P-PECD and ACDF for CSR and found that though the ACDF group had a better Cobb angle after the procedure and shorter operative time, there were no significant differences in VAS scores, NDI, and modified Macnab criteria between the two groups, and the patients treated with PECD had significantly less blood loss and hospital stay, as well as avoiding the destruction of major neck structures. Therefore, he concluded that P-PECD is safe and effective as an alternative procedure to ACDF for CSR. In 2021, Liu et al20 compared the medium and long-term outcomes of P-PECD and ACDF in the treatment of CSR, and the operative time, blood loss, and hospital stay in the P-PECD group were 75.67 ± 12.3 minutes, 13.17 ± 8.25 mL, and 3.60 ± 0.72 days, respectively, with a total of 4 complications and an incidence of 13.33% (4/30), whereas in the ACDF group were 86.72 ± 17.85 minutes, 75.31 ± 11.35 mL, and 6.22 ± 1.26 days, respectively, with a total of 4 complications and an incidence rate of 50% (16/32). The postoperative VAS and NDI scores were significantly improved between the two groups compared with before surgery, and the operative time, blood loss, hospital stay, and complications rate in the P-PECD group were lower. The ACDF group showed a significant increase in cervical curvature and lesion intervertebral space height at 6 months postoperatively and at the last follow-up compared with preoperatively, but the P-PECD group showed no significant change. Consequently, the author concluded that the medium-long-term efficacy of P-PECD for CSR was similar to ACDF and had the advantages of shorter operative time, less bleeding, shorter hospital stay, good maintenance of lesioned intervertebral space height, and no significant effect on the physiological curvature of the cervical spine. In this research, 51 patients with CSR completed the operation, postoperative neck and shoulder pain were significantly relieved, and VAS scores of neck and arm, JOA score as well as NDI were significantly improved compared with preoperatively. The modified Macnab criteria showed excellent to good outcomes of 94.12%. We consider that the reason is that, on the one hand, the compressed nerve root has been relieved. On the other hand, many patients have a long history of disease and received repeated physical therapy in the early stage, and large amounts of saline continuous flushing can wash away most of the inflammatory exudates and dilute pain factors. Also, this study was similar to the above literature in terms of operative time, estimated blood loss, and hospital stay, reflecting the advantages of this technique such as excellent efficacy, less trauma, less bleeding, fewer complications, and rapid postoperative recovery. According to the imaging findings during the follow-up in this study, the Cobb angle was decreased at 12 months postoperatively compared with before the operation, and there was no significant angle loss during the final follow-up. The ROM was increased at 12 months after the procedure and the final follow-up compared with preoperatively, and the differences were statistically significant (P < 0.05). The intervertebral space height, horizontal and angular displacement at the operative level at the final follow-up were not significantly changed compared with those before the operation, indicating that P-PECD could improve cervical mobility, maintain the intervertebral space height of the lesion well after the operation, had less effect on cervical stability, and had less possibility of adjacent spondylosis postoperatively, which were consistent with the results reported in the previous study.4,20–24 Based on the above series of literature reports and the results of this research, the authors concluded that P-PECD for CSR has the following advantages: (1) the operation can be performed under local anesthesia, and the patients remain awake throughout the operation, allowing real-time communication with the operator, which can reduce the risk of the spinal cord and nerve root injury; (2) only a 7 mm small incision was used for the operation, and the postoperative incision scar is small, in line with the concept of minimally invasive surgery and people’s pursuit of beautiful appearance; (3) no implants are required, which reduces the occurrence of implant-related complications and maintains normal motion segments and good biomechanical stability;4,25,26 (4) only the herniated nucleus pulposus tissues were removed, which causes less damage to the intervertebral space and bony structures, thereby reducing the occurrence of cervical instability after surgery; (5) water-mediated spinal endoscopic technique can control intraoperative bleeding through hydraulic pressure of flushing fluid. At the same time, it can accurately hemostasis through radiofrequency, so that the surgical field is clear, which is conducive to identifying tissue structure to reduce injury. Continuous saline flushing can wash away most of the inflammatory exudates and dilute pain factors to improve pain significantly while reducing the risk of infection.
With the widespread use of this technique, surgery-related complications have also been gradually exposed, and its incidence has been reported to be 3–48%,8 in which postoperative transient hypoesthesias is one of the common complications. In this group of patients, one case with transient thumb hypesthesia for 5 days, and we considered that it might be related to the thermal injury caused by the intraoperative use of radiofrequency.27,28 Another case presented with numbness in the affected arm for 3 days, which may have been caused by irritation of the nerve root during the nucleus pulposus was removed.29 Furthermore, access-related neck pain is also a common complication, and one case complained of neck pain the day after surgery in this group, which the authors considered to be caused by increased cervical epidural pressure due to continuous saline irrigation during surgery.8 These symptoms completely disappeared after symptomatic treatment such as dehydration, detumescence, and nutritional nerve. Other complications associated with this technique include dural tears, epidural hematoma, infection, and radiculitis, but the incidences are low and can be resolved with symptomatic treatment,8,30 and these complications were not observed in our study. Fewer complications occurred in this study, which further suggests that P-PECD is relatively safe in the treatment of single-segment CSR.
Our findings on cervical microendoscopic surgery align with the broader efficacy of minimally invasive spinal techniques, yet highlight region-specific challenges. Recent evidence in the lumbar spine demonstrates significant improvements in pain, disability, and quality of life post-microendoscopic discectomy, underscoring the method’s success in this region.31 However, cervical applications remain less studied, potentially due to anatomical complexities (eg, narrower operative fields and proximity to critical neurovascular structures). While our results corroborate the technique’s safety, the smaller effect size in cervical functional recovery (vs lumbar outcomes) suggests a need for protocol refinements tailored to cervical biomechanics. This gap emphasizes the novelty of our work and the urgency of cervical-specific surgical optimization research.
The Operation Points and Precautions of P-PECD for Single-Segment CSR
The goal of P-PECD for single-segment CSR is to remove the herniated nucleus pulposus and achieve adequate nerve decompression. Decompression of bony structures can be challenging for the surgeon. Kim22 suggested the “V” point at the junction of the lower edge of superior lamina, the upper edge of inferior lamina, and the medial facet joint as an anatomic landmark. In our research, the surgical approach was consistent with that, the outer lamina and cancellous bone were first abraded with a high-speed burr after cleaning the soft tissue on the surface of the bony structure, and then the inner lamina was removed with a rongeur, where reducing the use of burr could decrease the risk of dura and nerve injury. The bony drilling is usually within a 3- to 4-mm radius, and the medial wall of the pedicle can be felt with a nerve hook to avoid excessive resection of the facet joint resulting in cervical instability during the procedure. Some scholars deem that the facet joint resected should not exceed 50% as possible so that adequate decompression can be achieved while maintaining the stability of the operated segment.32,33 As early as 2015, Kim22 performed a retrospective analysis of imaging data from 32 patients with single-segment foraminal soft-disc herniation and assessed the radiological parameters, including cervical curvature (C2-7), Cobb angle as well as disc height. It was found that there was no significant change at the final follow-up compared with before surgery. Thus, he concluded that postoperative cervical sagittal curvature does not deteriorate and cervical instability does not occur as long as more than 50% of the facet joints were preserved during P-PECD. All patients had more than 50% of facet joints preserved in this study. The radiographic parameters of patients were measured before and after surgery and found that cervical Cobb angle, the intervertebral space height, as well as horizontal and angular displacement at the operative level were not significantly changed compared with those before the operation, which were consistent with the results and conclusions reported in the literature above. If there is dense adhesion between the dura and ligamentum flavum, a blunt hook can be inserted into the epidural space between them to facilitate separation and prevent dural tears. After exposing the dura and nerve root, it is recommended to explore the location of the herniated nucleus pulposus with a hook and carefully separate it. When removing the herniated nucleus pulposus, care should be taken to avoid excessive pulling and pushing the dura and nerve root to prevent injury, and when removing the nucleus pulposus ventral to the dura, the distal end of the nucleus pulposus forceps should be observed to avoid grasping the dura together and causing dural tears. The operation should be carefully hemostatic to maintain clear vision to avoid blurred surgical field due to bleeding, but it is not recommended to maintain a clear view by increasing the water pressure, as it may increase the intraspinal pressure and cause spinal cord hypertension syndrome, and it is recommended to control systolic blood pressure at 90- to 100-mmHg intraoperatively, which can effectively reduce bleeding.
Local anesthesia also has some drawbacks intraoperatively in this study. First, some patients still experience intraoperative pain to some extent, though this degree is tolerable. In addition, even without pain, patients can feel nervous and uncomfortable during the procedure when they are awake, which can not only lead to increased blood pressure and heart rate but also make the patient’s experience unpleasant as they have to remain in the prone position for a long period and hear the sounds of tools. For this reason, dexmedetomidine may be applied intraoperatively to help patients with sedation and analgesia,18 as well as to minimize stimulation of the nerve roots during the procedure to reduce pain and avoid increased bleeding due to elevated blood pressure caused by pain.
Limitations of this study are that it was a retrospective, single-center, self-controlled study with a small number of cases, selection bias when including patients, and lack of controlled and multicenter studies, and the efficacy of this procedure needs to be further confirmed by more case and multicenter follow-ups.
Conclusion
P-PECD has excellent medium-long-term efficacy in the treatment of single-segment CSR, with the advantages of less trauma, less bleeding, fewer complications, faster postoperative recovery, and less impact on cervical mobility and stability, which is worthy of clinical promotion and application. Nevertheless, this technique has a steep learning curve,34 and the operators need to strictly grasp the surgical indications and operating skills.
List of Abbreviations
ACDF, Anterior cervical discectomy and fusion; CSR, cervical spondylotic radiculopathy; CT, computerized tomography; DCS, degenerative cervical spondylosis; JOA, Japanese Orthopaedic Association; MRI, magnetic resonance imaging; NDI, neck disability index; P-PECD, Posterior percutaneous endoscopic cervical discectomy; ROM, range of motion; VAS, visual analog scale.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All methods were carried out following the relevant guidelines and regulations. This study was approved by the Ethics Committee of The First Affiliated Hospital of Xinjiang Medical University. All surgical patients participating in the study were aware of the study and signed the informed consent forms. The whole research process follows the Declaration of Helsinki.
Acknowledgments
We are very grateful for all the subjects who participated in the study.
Author Contributions
Xiangbin Wang and Tao Li contributed equally to this work as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Hunan Provincial Natural Science Foundation of China (2024JJ7474 and 2022JJ50024) and Science and Technology Plan Project Funding Grant of Shaoyang City (2023NS2015).
Disclosure
The authors declare that they have no competing interests.
References
1. Kang K-C, Lee HS, J-H L. Cervical radiculopathy focus on characteristics and differential diagnosis. Asian Spine J. 2020;14(6):921–930. doi:10.31616/asj.2020.0647
2. Luyao H, Xiaoxiao Y, Tianxiao F, Yuandong L, Ping W. Management of cervical spondylotic radiculopathy: a systematic review. Global Spine Journal. 2022;12(8):1912–1924. doi:10.1177/21925682221075290
3. Apaydin AS, Güneş M. Relationships between stenosis severity, functional limitation, pain, and quality of life in patients with cervical spondylotic radiculopathy. Turk J Med Sci. 2024;54(4):727–734. doi:10.55730/1300-0144.5842
4. Ren J, Li R, Zhu K, et al. Biomechanical comparison of percutaneous posterior endoscopic cervical discectomy and anterior cervical decompression and fusion on the treatment of cervical spondylotic radiculopathy. J Orthopaedic Surg Res. 2019;14(1):71. doi:10.1186/s13018-019-1113-1
5. Ahn Y, Keum HJ, Shin SH. Percutaneous endoscopic cervical discectomy versus anterior cervical discectomy and fusion: a comparative cohort study with a five-year follow-up. J Clin Med. 2020;9(2):371. doi:10.3390/jcm9020371
6. Gatam AR, Gatam L, Phedy Mahadhipta H, et al. Full endoscopic posterior cervical foraminotomy in management of foraminal disc herniation and foraminal stenosis. Orthop Res Rev. 2022;14:1–7. doi:10.2147/ORR.S349701
7. Ruetten S, Komp M, Merk H, Godolias G. Godolias G: a new full-endoscopic technique for cervical posterior foraminotomy in the treatment of lateral disc herniations using 6.9-mm endoscopes: prospective 2-year results of 87 patients. Minim Invasive Neurosurg. 2007;50(4):219–226. doi:10.1055/s-2007-985860
8. Quillo-Olvera J, Lin G-X, Kim J-S. Percutaneous endoscopic cervical discectomy: a technical review. Ann Transl Med. 2018;6(6):100. doi:10.21037/atm.2018.02.09
9. Guo L, Wang J, Zhao Z, et al. Microscopic anterior cervical discectomy and fusion versus posterior percutaneous endoscopic cervical keyhole foraminotomy for single-level unilateral cervical radiculopathy: a systematic review and meta-analysis. Clin Spine Surg. 2023;36(2):59–69. doi:10.1097/BSD.0000000000001327
10. Won S, Kim CH, Chung CK, et al. Comparison of cervical sagittal alignment and kinematics after posterior full-endoscopic cervical foraminotomy and discectomy according to preoperative cervical alignment. Pain Physician. 2017;20(2):77–87.
11. Dong L, Wang D, Chen X, et al. A comprehensive meta-analysis of the adjacent segment parameters in cervical disk arthroplasty versus anterior cervical discectomy and fusion. Clin Spine Surg. 2018;31(4):162–173. doi:10.1097/BSD.0000000000000552
12. White AA, Panjabi MM. Update on the evaluation of instability of the lower cervical spine. Instruct Course Lectu. 1987;36:513–520.
13. Liu C, Liu K, Chu L, Chen L, Deng Z. Posterior percutaneous endoscopic cervical discectomy through lamina–hole approach for cervical intervertebral disc herniation. Int J Neurosci. 2019;129(7):627–634. doi:10.1080/00207454.2018.1503176
14. Liao C, Ren Q, Chu L, et al. Modified posterior percutaneous endoscopic cervical discectomy for lateral cervical disc herniation: the vertical anchoring technique. Eur Spine J. 2018;27(6):1460–1468. doi:10.1007/s00586-018-5527-y
15. Xiao C-M, Yu K-X, Deng R, et al. Modified K-hole percutaneous endoscopic surgery for cervical foraminal stenosis: partial pediculectomy approach. Pain Physician. 2019;22(5):E407–E416.
16. Haijun M, Xiaobing Z, Bin G, et al. Trans-interlamina percutaneous endoscopic cervical discectomy for symptomatic cervical spondylotic radiculopathy using the new Delta system. Sci Rep. 2020;10(1):10290. doi:10.1038/s41598-020-67381-z
17. Yu T, Wu J-P, Zhang J, Yu H-C, Liu Q-Y. Comparative evaluation of posterior percutaneous endoscopy cervical discectomy using a 3.7 mm endoscope and a 6.9 mm endoscope for cervical disc herniation: a retrospective comparative cohort study. BMC Musculoskel Disord. 2021;22(1):131. doi:10.1186/s12891-021-03980-9
18. Wan Q, Zhang D, Li S, et al. Posterior percutaneous full-endoscopic cervical discectomy under local anesthesia for cervical radiculopathy due to soft-disc herniation: a preliminary clinical study. J Neurosurg Spine. 2018;29(4):351–357. doi:10.3171/2018.1.SPINE17795
19. Ji-Jun H, Hui-Hui S, Zeng-Wu S, et al. Posterior full-endoscopic cervical discectomy in cervical radiculopathy: a prospective cohort study. Clin Neurol Neurosurg. 2020;195:105948. doi:10.1016/j.clineuro.2020.105948
20. Liu SL, Xu YS, Li XC, et al. Medium and long-term curative effect of posterior percutaneous endoscopic cervical discectomy in treatment of cervical spondylotic radiculopathy. J Pra Med. 2021;37(20):2624–2629.
21. Mintao X, Yi L, Changgui S, Jiangming Y, Xiaojian Y, Guohua X. Medium and long term efficacy of posterior percutaneous endoscopic cervical discectomy in treatment of double-segment cervical spondylotic radiculopathy. J Spin Surg. 2022;20(03):182–186.
22. Kim CH, Shin K-H, Chung CK, Park SB, Kim JH. Changes in cervical sagittal alignment after single-level posterior percutaneous endoscopic cervical diskectomy. Global Spine Journal. 2015;5(1):31–38. doi:10.1055/s-0034-1395423
23. Lv J, Mei J, Feng X, Tian X, Sun L. Clinical efficacy and safety of posterior minimally invasive surgery in cervical spondylosis: a systematic review. J Orthopaedic Surg Res. 2022;17(1):389. doi:10.1186/s13018-022-03274-3
24. Oh HS, Hwang B-W, Park S-J, Hsieh C-S, Lee S-H. Percutaneous endoscopic cervical discectomy (PECD): an analysis of outcome, causes of reoperation. World Neurosurg. 2017;102:583–592. doi:10.1016/j.wneu.2017.03.056
25. Wewel JT, Brahimaj BC, Kasliwal MK, Traynelis VC. Perioperative complications with multilevel anterior and posterior cervical decompression and fusion. J Neurosurg Spine. 2019;32(1):9–14. doi:10.3171/2019.6.SPINE198
26. Tomé-Bermejo F, JA M-V, Moreno-Pérez J, et al. Degenerative cervical disc disease: long-term changes in sagittal alignment and their clinical implications after cervical interbody fusion cage subsidence: a prospective study with standalone lordotic tantalum cages. Clin Spine Surg. 2017;30(5):E648–E655. doi:10.1097/BSD.0000000000000293
27. Kim CH, Kim K-T, Chung CK, et al. Minimally invasive cervical foraminotomy and diskectomy for laterally located soft disk herniation. Eur Spine J. 2015;24(12):3005–3012. doi:10.1007/s00586-015-4198-1
28. Zheng C, Huang X, Yu J, Ye X. Posterior percutaneous endoscopic cervical diskectomy: a single-center experience of 252 cases. World Neurosurg. 2018;120:e63–e67. doi:10.1016/j.wneu.2018.07.141
29. Liu J, Kong Q, Feng P, Zhang B, Hu Y, Ma J. Clinical effect of channel assisted cervical key hole technology combined with ultrasonic bone osteotome in the treatment of single segment cervical spondylotic radiculopathy. Front Surg. 2022;9:1029028. doi:10.3389/fsurg.2022.1029028
30. R-J L, Song Y, Z-W L, et al. Keyhole foraminotomy via a percutaneous posterior full-endoscopic approach for cervical radiculopathy: an advanced procedure and clinical study. Curr Med Sci. 2020;40(6):1170–1176. doi:10.1007/s11596-020-2299-5
31. Apaydin AS, Bozyiğit B, Koç-Apaydin Z, Güneş M, Yana M. Effects of different surgical treatments on pain, disability, anxiety and quality of life in lumbar disc herniation. Cir Cir. 2024;92(1):39–45. doi:10.24875/CIRU.23000415
32. Ahn Y. Percutaneous endoscopic cervical discectomy using working channel endoscopes. Expert Rev Med Dev. 2016;13(6):601–610. doi:10.1080/17434440.2016.1180245
33. Lee D-H, Cho JH, Hwang CJ, Lee CS, Kim C, Ha J-K. Multilevel posterior foraminotomy with laminoplasty versus laminoplasty alone for cervical spondylotic myelopathy with radiculopathy: a comparative study. Spine J. 2018;18(3):414–421. doi:10.1016/j.spinee.2017.08.222
34. Simpson AK, Lightsey HM, Xiong GX, Crawford AM, Minamide A, Schoenfeld AJ. Spinal endoscopy: evidence, techniques, global trends, and future projections. Spine J. 2022;22(1):64–74. doi:10.1016/j.spinee.2021.07.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.