")
Back to Journals » Journal of Pain Research » Volume 18
Postoperative Pain Management Strategies Following Peroral Endoscopic Myotomy (POEM): A Review
Authors Lu J, Ji W, Sang C, Wang Z, Bo L
Received 8 December 2024
Accepted for publication 27 May 2025
Published 31 May 2025 Volume 2025:18 Pages 2761—2773
DOI https://doi.org/10.2147/JPR.S511019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Jun Lu,1 Wentao Ji,1 Chao Sang,2 Zhi Wang,1 Lulong Bo1
1Department of Anesthesiology, Changhai Hospital, Naval Medical University, Shanghai, 200433, People’s Republic of China; 2Department of Anesthesiology, Yueyang Hospital of Integrated Traditional and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200437, People’s Republic of China
Correspondence: Lulong Bo, Department of Anesthesiology, Changhai Hospital, Naval Medical University, Shanghai, 200433, People’s Republic of China, Email [email protected]
Abstract: Peroral Endoscopic Myotomy (POEM) is a minimally invasive procedure for treating esophageal achalasia, but effective postoperative pain management remains a challenge. Pain following POEM is multifactorial, arising from mechanical, chemical, and thermal stimuli that activate nociceptive and neuropathic pain pathways. A multimodal analgesia approach, combining opioids, non-opioid analgesics, and regional anesthesia, is currently the most effective strategy. Opioids remain a cornerstone of pain management, but their side effects, such as nausea and constipation, highlight the need for alternatives. Non-opioid analgesics, including acetaminophen, COX-2 inhibitors, and magnesium, have shown promise in reducing pain and opioid use. Regional anesthesia techniques, such as thoracic paravertebral blocks and erector spinae plane blocks, have been explored, though their efficacy in POEM remains inconclusive. Despite advances, there are ongoing challenges in standardizing pain management protocols. Variability in clinical practices and limited high-quality research with small sample sizes complicate the development of universally applicable guidelines. Additionally, while current research primarily focuses on acute postoperative pain, long-term outcomes, such as chronic pain and quality of life, require further investigation. Addressing these gaps in knowledge will be key to improving pain management practices and optimizing recovery for POEM patients. Future studies should focus on refining multimodal analgesia strategies, exploring new analgesic agents, and evaluating long-term pain management outcomes to enhance patient care and improve clinical results.
Keywords: multimodal analgesia, non-opioid analgesics, opioid analgesics, peroral endoscopic myotomy, postoperative pain management, regional anesthesia
Introduction
Achalasia is a rare, primary esophageal motility disorder characterized by dysphagia, regurgitation, and retrosternal discomfort.1 It affects approximately 1 in 100,000 individuals annually.2,3 Despite its low incidence, achalasia significantly impacts patients’ quality of life, functional capacity, and work productivity. Furthermore, it carries a 4–6% lifetime risk of progression to esophageal cancer, highlighting the critical need for timely and effective treatments.4
Laparoscopic Heller myotomy (LHM) has long been considered the gold standard in the surgical treatment of achalasia.5 This procedure provides symptomatic relief by reducing lower esophageal sphincter (LES) pressure. However, in 2010, Inoue et al introduced peroral endoscopic myotomy (POEM), a minimally invasive endoscopic approach that has since revolutionized achalasia management.6 POEM offers outcomes comparable to LHM but with the advantage of being performed via the oral cavity, eliminating the need for external incisions. Over the past decade, POEM has gained widespread adoption, particularly for idiopathic achalasia and other motility disorders of the esophagus, owing to its lower invasiveness and similar effectiveness to LHM.7,8
Nevertheless, postoperative pain remains a significant challenge following POEM, with pain intensity ranging from mild to moderate. Up to 10% of patients experience severe postoperative pain, leading to delays in recovery and hindering rehabilitation efforts.9 The relatively short hospital stays typical for POEM, often less than 24 hours, pose further challenges to effective pain management due to the limited time for intensive postoperative care.10,11 Additionally, the lack of standardized pain management protocols complicates efforts to provide optimal pain relief.12
This narrative review aims to examine postoperative pain management strategies following POEM, focusing on the specific challenges posed by this minimally invasive procedure. By synthesizing current research and clinical practices, this review emphasizes evidence-based multimodal analgesia, tailored pharmacological interventions, and individualized care plans. Ultimately, we seek to provide actionable insights that can improve pain control and enhance outcomes for patients undergoing POEM.
Literature Search
A systematic literature search was conducted across databases including PubMed, Web of Science, and EMBASE to identify studies related to postoperative pain management in patients undergoing POEM. The search covered the period from January 2010, when POEM was first introduced,6 to May 2024. Search terms included combinations of keywords such as “peroral endoscopic myotomy”, “pyloromyotomy”, “endoscopic submucosal dissection”, “natural orifice endoscopic surgery”, “analgesia”, and “pain”. A detailed search strategy is provided in Appendix 1.
Due to the limited literature specifically addressing postoperative pain management in POEM, the search was expanded to include studies on postoperative pain management in patients undergoing upper gastrointestinal endoscopic submucosal dissection (ESD). Although both POEM and ESD are part of natural orifice transluminal endoscopic surgery (NOTES), they differ substantially: POEM involves myotomy, which causes more tissue trauma and greater postoperative pain compared to ESD. Therefore, studies on ESD were included to guide optimal pain management practices.
The literature search included prospective and retrospective studies, case reports, institutional practices, and relevant clinical guidelines published between January 2010 and May 2024. Citation tracking was employed to identify additional references. Inclusion criteria focused on studies specifically addressing postoperative pain management in POEM, supplemented by ESD-related studies that provided valuable insights into pain management practices for esophageal motility disorders.
Abstracts were initially screened for relevance, followed by full-text review to ensure the inclusion of high-quality, peer-reviewed studies. The final dataset consisted of publications from four countries and ten institutions, including five prospective studies,13–16 three retrospective studies,12,17,18 two case reports,19,20 and one letter to the editor.21 Key findings from these studies are summarized in Table 1, offering a comprehensive overview of current practices, outcomes, and emerging strategies for postoperative pain management in POEM.
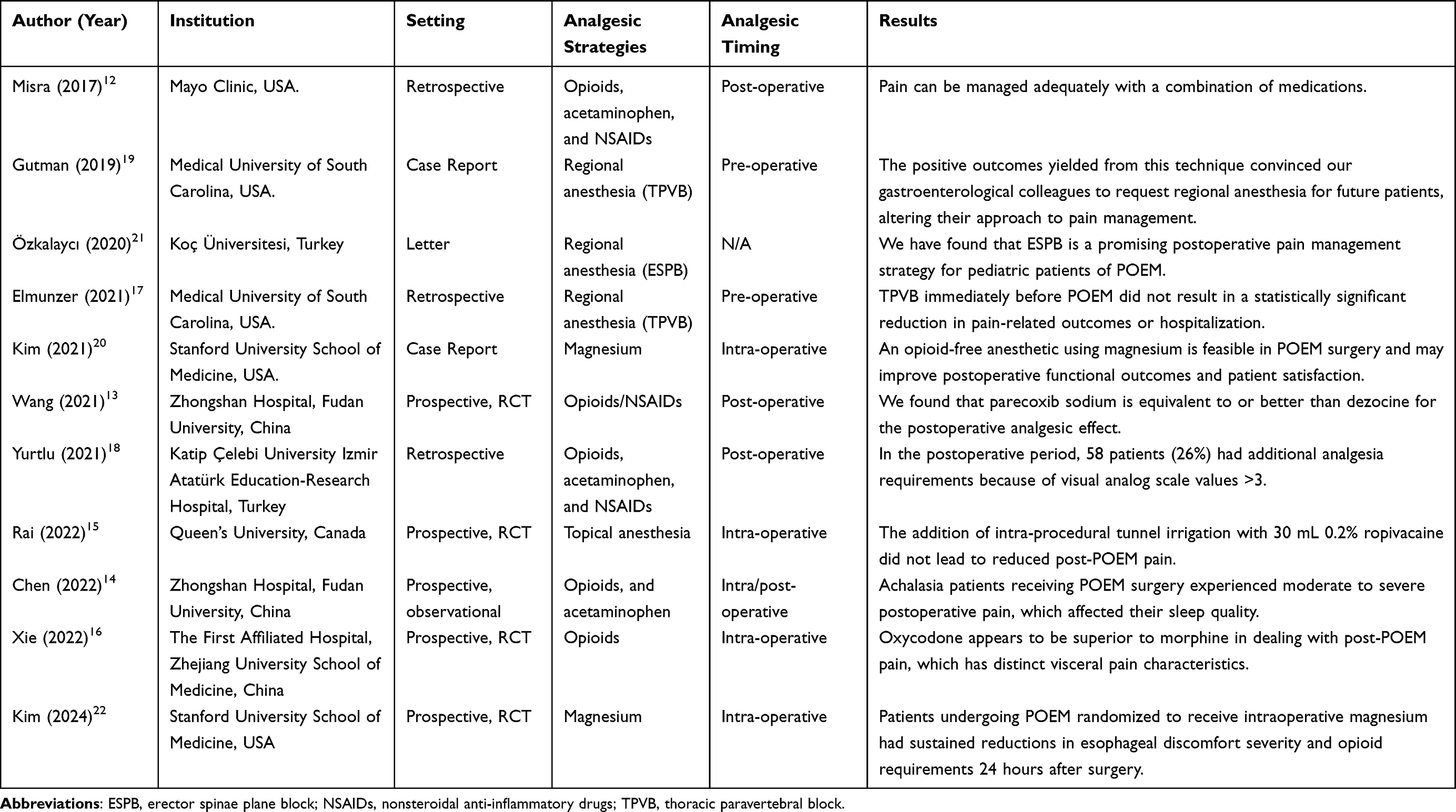 |
Table 1 Systematic Review of the Literature Regarding Pain Management After POEM |
This systematic approach provides a robust foundation for exploring and optimizing pain management protocols specifically tailored to the unique challenges of POEM.
Physiology and Pathophysiology of Pain After POEM
POEM, introduced by Inoue et al in 2010 for the treatment of esophageal achalasia, is a minimally invasive procedure that has significantly transformed the management of this motility disorder. Despite its advantages, such as faster recovery times and fewer complications compared to traditional surgical, POEM can result in postoperative pain that requires careful management.12 The procedure involves four key steps: mucosal entry, submucosal tunneling, esophageal myotomy, and closure of the entry site, as illustrated in Figure 1.23
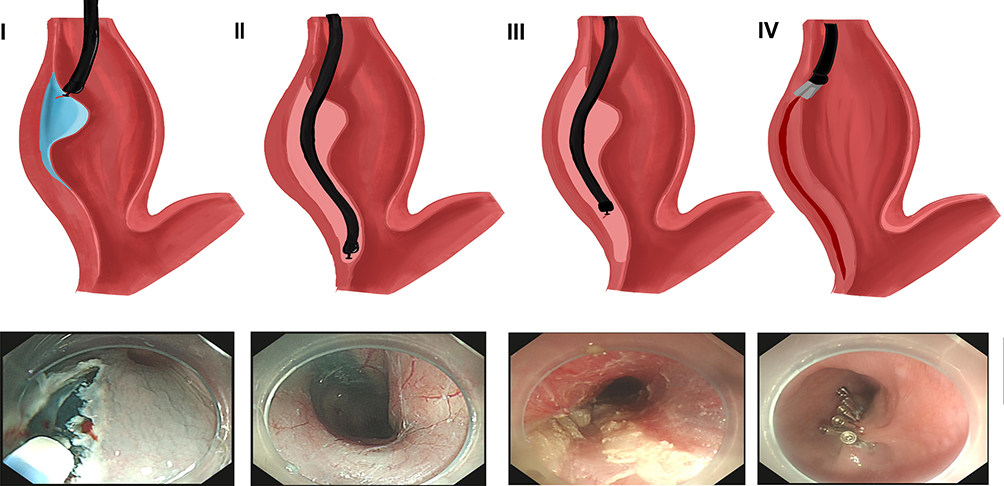 |
Figure 1 The four main steps of POEM procedure. (I) Mucosal entry, which involves the creation of a minor incision in the mid-esophagus. (II) Submucosal tunneling, which entails the performance of an endoscopic submucosal dissection from the mucosal incision to a point 2–3 cm below the gastroesophageal junction, thereby establishing a submucosal tunnel. (III) Endoscopic myotomy, a process that involves the selective myotomy of the circular muscle using electrocautery, extending a minimum of 6 cm. (IV) The closure of the mucosal entry. |
Multifactorial Nature of Postoperative Pain
Postoperative pain following POEM is multifactorial, arising from a combination of mechanical, chemical, thermal, and physiological stimuli, which interact to activate nociceptive and, in some cases, neuropathic pain pathways, resulting in a complex pain experience for patients.24
Mechanical Stimuli
Mechanical injury from esophageal tissue manipulation and incision during myotomy is a primary source of postoperative pain. The cutting of esophageal muscle fibers generates mechanical stress and trauma, activating mechanoreceptors and nociceptors. These nociceptors detect tissue deformation caused by stretching, pressure, or trauma, leading to immediate postoperative pain.25 The severity of mechanical pain varies based on the extent of the myotomy and the individual tissue response to injury.
Chemical Stimuli
Following tissue injury, chemical mediators such as prostaglandins, bradykinin, and cytokines are released during the inflammatory response. These mediators sensitize nociceptors by lowering their activation threshold, amplifying pain signals and increasing pain sensitivity in the early postoperative phase.
Thermal Stimuli
Thermal injury also contributes to postoperative pain. During POEM, electrocautery or laser devices are commonly used for tissue dissection, generating heat that can inadvertently damage surrounding esophageal tissues.26,27 This thermal injury activates thermoreceptors, adding to the intensity and duration of postoperative pain.
Carbon Dioxide Absorption
The use of carbon dioxide (CO2) during POEM—particularly in submucosal tunneling and myotomy—introduces additional pain-related factors. Rapid absorption of CO2 can lead to complications such as pneumomediastinum, subcutaneous emphysema, and pneumoperitoneum.28,29 Although these complications are not always clinically significant, they can exacerbate discomfort and contribute to postoperative pain. Addressing these effects is critical for tailoring effective pain management strategies.
Nociceptive and Neuropathic Pain Mechanisms
Postoperative pain following POEM typically involves both nociceptive and neuropathic components, which can interact to produce more complex pain profiles.
Nociceptive Pain
Nociceptive pain results directly from tissue injury during the procedure. Inflammation at the site of injury releases pain-inducing chemicals that activate nociceptors in the mucosa and muscle layers.13 These pain signals are transmitted to the CNS via the spinal cord, resulting in sharp, localized pain. Nociceptive pain is most pronounced during the early postoperative period and gradually subsides with tissue healing.
Neuropathic Pain
Neuropathic pain may arise from nerve damage or irritation during the myotomy. This includes potential injury to the vagus nerve or branches of the sympathetic nervous system.30,31 Neuropathic pain often manifests as burning or shooting sensations, which may persist beyond the normal healing period. Patients with preexisting esophageal motility disorders or higher Eckardt scores are at increased risk of developing neuropathic pain due to heightened nerve sensitivity.14
Inflammatory Response and Sensitization
Inflammation following POEM plays a pivotal role in postoperative pain pathophysiology. Pro-inflammatory cytokines, growth factors, and neurotrophic factors released during the inflammatory response can contribute to central sensitization.31 This condition arises when the CNS becomes hyper-responsive to pain signals, leading to phenomena such as hyperalgesia, which is an increased sensitivity to pain, and allodynia, a state where pain is triggered by stimuli that are typically not painful.
The degree of central sensitization is influenced by factors such as the extent of myotomy, the patient’s baseline pain threshold, and preexisting conditions. Effective management of the inflammatory response is critical to preventing persistent pain and improving recovery outcomes.
Visceral Pain Pathways
Postoperative pain after POEM is predominantly visceral in nature, originating from internal organs rather than somatic tissues. Visceral pain, transmitted primarily via the vagus nerve, is often diffuse and difficult to localize.25 This type of pain is commonly associated with sensations of fullness, pressure, or generalized discomfort.
During POEM, disruption of esophageal motility and tissue injury can result in abnormal signaling through the vagus nerve. This abnormal signaling contributes to persistent visceral pain. A thorough understanding of the visceral nociceptive pathways is essential for developing targeted therapies that address this unique aspect of POEM-related pain.
Distinction from Other Endoscopic Procedures
Unlike ESD, POEM involves smaller, higher esophageal incisions that are securely closed with hemostatic clips, significantly reducing the risk of gastric acid reflux-related discomfort. This distinction highlights the unique challenges of POEM, where pain is more likely to result from mechanical, thermal, and chemical factors than from acid exposure.
Overall, the combination of mechanical trauma resulting from submucosal tunneling and myotomy, along with thermal injury caused by electrocautery and inflammation induced by CO2, generates a unique pain profile that is distinct from both LHM and ESD.
Risk Factors for Post-POEM Pain
Several factors can increase the likelihood or severity of pain following POEM:14
- Preoperative opioid use: May result in opioid tolerance and reduced analgesic efficacy.
- High Eckardt scores: Indicate severe preoperative symptoms, which can correlate with greater postoperative discomfort.
- Previous treatments: Such as botulinum toxin injections or balloon dilation, which may alter tissue sensitivity.
- Extent of the myotomy: Greater myotomy length or proximity to the gastric cardia increases tissue trauma.
- Delayed gastric emptying: Can exacerbate pain through increased inflammation or motility disturbances.
Postoperative pain after POEM arises from a complex interplay of mechanical, chemical, thermal, and inflammatory factors, compounded by both nociceptive and neuropathic mechanisms. A comprehensive understanding of these processes, along with individual patient risk factors, is critical for developing effective pain management strategies tailored to the unique challenges of POEM.
Current Status of Postoperative Pain Management After POEM
Postoperative pain following POEM is typically transient, yet most patients require analgesic treatment to ensure adequate pain control, facilitate recovery, and improve overall outcomes. Despite its critical role in patient recovery, there is currently no universally accepted guideline for postoperative pain management after POEM. This lack of consensus arises from differences in institutional protocols, clinician preferences, and the evolving understanding of pain mechanisms. Recent studies suggest that a multimodal analgesia approach, which integrates both pharmacological and non-pharmacological methods, is optimal for minimizing opioid use while effectively managing pain and improving recovery times.32,33
Analgesics
Postoperative analgesia typically involves oral, intravenous, or intramuscular rescue medication, including acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and opioids. A combination of different analgesics optimizes pain relief while minimizing side effects, with individualized regimens enhancing recovery outcomes. Acetaminophen and NSAIDs are commonly used in combination to target both nociceptive and inflammatory pain components, while opioids are introduced for more severe pain when necessary. The goal is to reduce opioid consumption by using multimodal strategies, thus minimizing the associated risks such as respiratory depression, constipation, and addiction.12–14,16,18
The Role of Opioids in Postoperative Pain Management
Opioids remain a cornerstone of postoperative analgesia due to their potent analgesic effects, particularly for moderate to severe pain. However, the use of opioids is associated with significant side effects, such as nausea, vomiting, respiratory depression, constipation, and the potential for addiction.34 Therefore, the judicious use of opioids is essential to minimize these risks, especially in the context of POEM, where rapid recovery and minimal complications are crucial. Understanding the pharmacodynamics of different opioid receptors is essential in selecting the most suitable opioids for managing POEM-related pain.
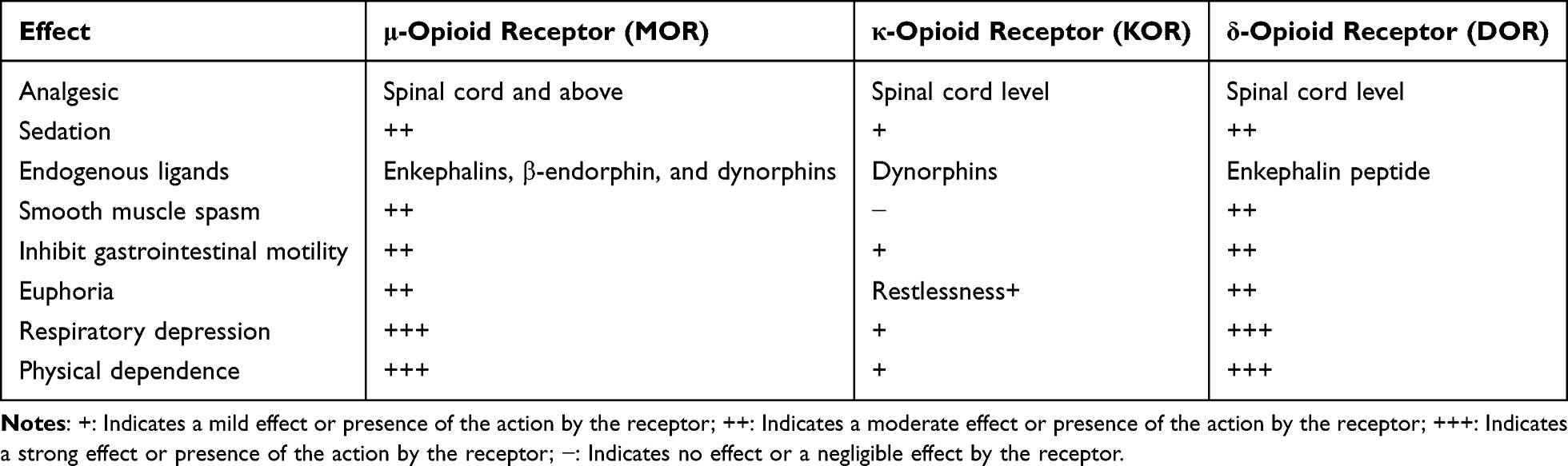
Opioids exert their analgesic effects by binding to opioid receptors in both the central and peripheral nervous systems.35 The main receptor subtypes involved in pain relief are (Table 2):
- μ-opioid receptors (MORs): These receptors are the primary target of most opioid analgesics. MOR activation results in effective pain relief but is also associated with adverse effects, including respiratory depression and gastrointestinal complications.36
- κ-opioid receptors (KORs): KORs are located mainly in the spinal cord and visceral organs, making them particularly relevant for managing visceral pain. KOR activation provides effective analgesia for deep or internal pain but also induces side effects like dysphoria and sedation.37
- δ-opioid receptors (DORs): Although less commonly targeted, DORs play a role in modulating pain and enhancing the effects of MOR activation. DOR agonists may offer effective analgesia with fewer side effects than MOR-targeted opioids.38

Table 2 Opioid Receptors and Effects Associated with Analgesia
Recommended Opioid Analgesics for POEM
Based on the pain profile and underlying pathophysiology of POEM-related pain, opioids targeting both MORs and KORs are especially effective for managing visceral and somatic pain. Below are some key opioids that have shown promise in postoperative pain management following POEM:
Oxycodone is a dual-acting opioid, targeting both MORs and KORs, making it particularly effective for managing both somatic and visceral pain post-POEM. A randomized controlled trial by Xie et al found oxycodone to be more effective than morphine in managing visceral pain in patients recovering from gastrointestinal surgeries. Additionally, oxycodone is associated with fewer side effects, including less sedation and reduced constipation rates compared to traditional opioids.16
Tramadol is a weak MOR agonist that also inhibits the reuptake of serotonin and norepinephrine, providing a multimodal approach to pain relief. Tramadol has been shown to be effective in managing postoperative pain following POEM, particularly for patients with mild to moderate pain. A study by Yurtlu et al demonstrated that tramadol as part of a multimodal analgesia regimen was associated with lower opioid consumption and faster recovery times after POEM. However, tramadol’s effects on intestinal motility may limit its use in some patients, particularly those at risk for gastrointestinal complications.18
Dezocine is a partial agonist at both MORs and KORs, providing balanced analgesia with a lower incidence of side effects compared to full opioid agonists like morphine.39 Research by Wang et al showed that dezocine was effective in managing postoperative pain following various gastrointestinal procedures, including POEM, and was well-tolerated by patients. Its lower side effect profile, including less risk of respiratory depression and gastrointestinal complications, makes it an attractive option for postoperative pain management.13,14
Transdermal fentanyl patches (TDF) provides long-lasting, stable analgesia over 72 hours, making it a viable option for managing moderate to severe postoperative pain following POEM. A study by Choi et al demonstrated that TDF significantly reduced pain scores and opioid consumption in the first 24 hours after POEM.40 Due to its prolonged-release mechanism, TDF is ideal for providing continuous pain control, particularly in patients requiring extended analgesic coverage postoperatively.
Why Discuss Different Opioids?
The discussion of different opioids is essential for several reasons:
- Pain Characteristics: POEM-related pain is often visceral in nature, which may require opioids with specific receptor activity (ie, KORs) for optimal pain management.
- Side Effect Profiles: Each opioid has a distinct side effect profile. For instance, while oxycodone and tramadol are effective for both somatic and visceral pain, tramadol’s effect on serotonin reuptake can help address neuropathic components of pain, while oxycodone’s dual receptor activity reduces the risk of opioid-related complications.
- Enhanced Recovery After Surgery (ERAS) Protocols: ERAS protocols emphasize minimizing opioid use to reduce side effects such as respiratory depression and constipation. Choosing opioids with fewer side effects supports faster recovery and aligns with ERAS principles.
Most Suitable Opioid Option
Based on the current evidence, oxycodone emerges as the most suitable opioid for managing postoperative pain following POEM due to its balanced efficacy for both somatic and visceral pain, along with a more favorable side effect profile compared to morphine. For patients with mild to moderate pain or those who require lower opioid doses, tramadol offers a reasonable alternative within a multimodal analgesia regimen. Transdermal fentanyl patches may be considered for patients requiring sustained pain control over an extended period, particularly in cases of more intense postoperative pain.
Non-Opioid Analgesics
Non-opioid analgesics are integral to multimodal pain management strategies following POEM.12,14 These agents are crucial in addressing the various aspects of postoperative pain, such as nociceptive, inflammatory, and visceral pain, and in minimizing opioid consumption, which is important for enhancing recovery outcomes and adhering to Enhanced Recovery After Surgery (ERAS) protocols.
Acetaminophen is frequently used in post-POEM pain management due to its central nervous system-mediated analgesic effects.12,14,18 Studies have demonstrated its efficacy in reducing mild to moderate pain after POEM without the side effects typically associated with opioids. For instance, one study found that acetaminophen, when administered in conjunction with other non-opioid analgesics, provided adequate pain relief while reducing opioid consumption and promoting recovery. As acetaminophen works by inhibiting cyclooxygenase enzymes in the brain, it primarily helps manage pain arising from mild tissue injury but is less effective for more intense pain, which may necessitate stronger analgesics.
Selective Cyclooxygenase-2 (COX-2) inhibitors, such as Parecoxib sodium, are another crucial component of postoperative pain management.32,33 These drugs are effective in controlling postoperative pain with fewer gastrointestinal side effects compared to traditional NSAIDs. For example, Parecoxib has shown non-inferiority to opioids like dezocine in controlling postoperative pain in various studies, making it an important alternative in ERAS protocols. A study conducted in Chinese tertiary care hospitals demonstrated Parecoxib’s effectiveness in minimizing opioid use while maintaining satisfactory pain control, aligning with the growing need for strategies that reduce opioid-related adverse effects.13
Dexmedetomidine (DEX), an α2-receptor agonist, provides effective sedation, analgesia, and anxiolysis,41 which can be highly beneficial in post-POEM pain management. Retrospective studies have highlighted DEX’s potential in reducing postoperative pain and opioid requirements.42 For instance, a study on gastric ESD patients found that intraoperative DEX administration led to significantly lower postoperative pain scores and reduced opioid consumption.43 In the context of POEM, this could translate into improved patient comfort, faster recovery, and reduced opioid-related side effects. Moreover, DEX has been used successfully in total intravenous anesthesia for gastrointestinal procedures, suggesting its broad applicability in gastrointestinal surgeries like POEM.42
Glucocorticoids, such as dexamethasone, have been demonstrated to provide significant analgesic effects postoperatively, in addition to their anti-inflammatory properties.44,45 Studies indicate that dexamethasone can reduce inflammation and postoperative nausea and vomiting, both of which are common after POEM. Dexamethasone has been shown to decrease opioid requirements in patients undergoing ESD procedures.46 Furthermore, its administration prior to surgery has been associated with superior analgesic effects in comparison to postoperative administration.47 While its use is well-established for reducing inflammation, care should be taken when using dexamethasone to avoid potential side effects such as delayed wound healing or immune suppression. These findings emphasize the need for careful consideration in incorporating glucocorticoids into multimodal analgesia protocols for POEM.
Intravenous lidocaine is another effective non-opioid analgesic, recognized for its analgesic, anti-hyperalgesic, and anti-inflammatory properties.48–50 Recent studies have confirmed that lidocaine reduces postoperative pain and accelerates recovery in gastrointestinal procedures, including POEM. A meta-analysis highlighted the benefits of intravenous lidocaine in reducing post-procedural pain and lowering the incidence of adverse events in gastrointestinal endoscopy patients.51 Its mechanism of action, involving sodium channel blockade, helps decrease neuronal excitability and prevent central sensitization, which is often a significant factor in postoperative pain.52,53 Lidocaine is particularly effective for managing visceral pain, a predominant type of pain following POEM, due to its action on the peripheral nerves.
Magnesium sulfate has been identified for its potential to enhance analgesia during and after surgery by inhibiting NMDA receptors and reducing central sensitization.54,55 A randomized controlled trial demonstrated that magnesium administration during POEM significantly reduced opioid requirements and esophageal discomfort in the first 24 hours post-surgery.22 These findings suggest magnesium’s role in reducing visceral hyperalgesia, which is a key component of post-POEM pain. Although magnesium shows promise in pain management, further research is needed to fully assess its therapeutic potential and optimal dosing in POEM analgesia.
Regional Anesthesia
Regional anesthesia, including techniques such as thoracic paravertebral block (TPVB) and erector spinae plane block (ESPB), has gained attention in the postoperative pain management following POEM, although its full efficacy remains unclear and warrants further investigation. Regional blocks have been well-documented in managing pain following thoracic surgeries, and they may potentially offer similar benefits in POEM patients. For example, Gutman et al successfully used TPVB in a POEM patient, which led to a shift in their postoperative pain management strategy.19 However, a retrospective cohort study of 49 POEM patients did not show significant differences in pain scores, opioid consumption, or hospital stay length between those who received TPVB and those who did not.17 Furthermore, multivariate regression analysis revealed no correlation between TPVB and reduced pain or opioid use, suggesting that TPVB may not significantly improve pain outcomes in POEM. This observation indicates the need for more research, particularly regarding the use of higher anesthetic doses or alternative formulations to enhance efficacy.
Another promising regional anesthesia technique is ESPB, which has been suggested by Özkalaycı et al as a potential strategy for postoperative pain management, especially in pediatric POEM patients.21 However, larger clinical trials are necessary to further validate its efficacy in this context.
Topical Anesthesia
In POEM procedures, the creation of a submucosal tunnel in the esophagus raises interest in the potential role of topical anesthesia for reducing postoperative pain. A prospective, double-blind, randomized controlled trial by Rai et al investigated the use of 0.2% ropivacaine irrigated into the POEM tunnel following myotomy. Their results indicated that ropivacaine irrigation did not reduce post-POEM pain.15 This finding aligns with similar inconclusive results in ESD procedures, where studies on topical anesthesia, such as bupivacaine, have yielded mixed outcomes.15 While Kim et al found that injecting bupivacaine into the cautery ulcer base before completing the ESD reduced post-procedural pain,56 Jung et al found no significant benefit of pre-emptive bupivacaine injections in managing post-ESD abdominal pain.57 The study details are presented in Table 3. These contrasting findings underscore the uncertainty surrounding the effectiveness of topical anesthesia in both POEM and ESD procedures, necessitating further studies to clarify the optimal timing, technique, and pharmacological agents for this approach.
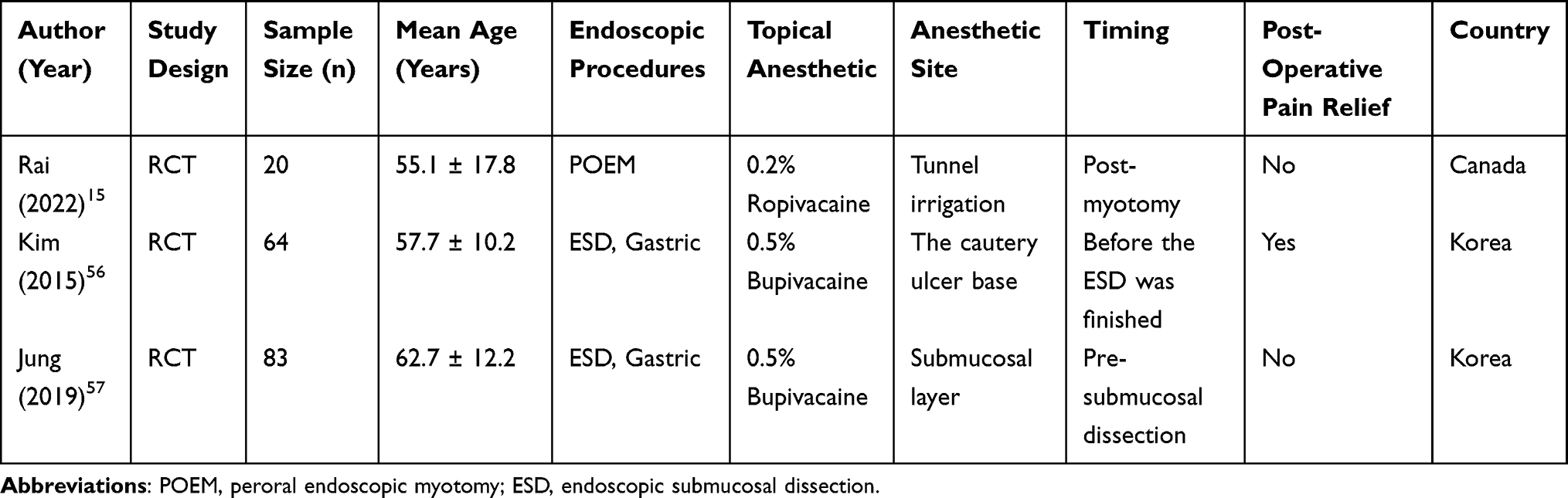 |
Table 3 Study of Topical Anesthesia for POEM and ESD Procedures |
Analgesic Strategies: Preemptive, Rescue Analgesia, or Multimodal Analgesia?
Preemptive Analgesia
Preemptive analgesia seeks to attenuate pain by preventing central and peripheral sensitization before noxious stimuli occur. This approach is designed to reduce postoperative pain severity and minimize the need for rescue analgesics.56,58 However, its efficacy in POEM remains inconsistent. For instance, Kim et al demonstrated that the application of bupivacaine at the end of ESD reduced postoperative pain scores significantly, suggesting a potential benefit when used peri-procedurally.56 In contrast, Jung et al found no significant reduction in abdominal pain with pre-incision bupivacaine administration during ESD, especially when subsequent analgesics were not employed.57 Similarly, preemptive ropivacaine irrigation in POEM showed limited impact on postoperative pain outcomes in controlled trials.15
This variability suggests that preemptive analgesia alone may be insufficient for POEM, particularly when intraoperative opioids are minimized. It highlights the need for a balanced approach that integrates preemptive analgesia with other strategies to address pain comprehensively.
Rescue Analgesia
Rescue analgesia provides relief on demand after the onset of pain. While this approach reduces the risk of overmedication, it often allows pain to escalate before treatment, negatively affecting the patient experience. In the context of POEM, uncontrolled pain can lead to delayed recovery, reduced patient satisfaction, and increased opioid use postoperatively. Although effective in managing acute pain episodes, the reliance on rescue analgesia alone is less desirable for ERAS protocols, which prioritize proactive pain control and minimized opioid use.
For example, reliance on opioids like fentanyl or pethidine as rescue analgesics can exacerbate adverse effects such as nausea, vomiting, and respiratory depression, further complicating recovery. This underscores the importance of combining rescue analgesia with preventive strategies to mitigate the need for high-dose opioid administration.
Multimodal Analgesia
Multimodal analgesia is the cornerstone of modern pain management, particularly in procedures like POEM. By integrating pharmacological and non-pharmacological approaches, this strategy targets multiple pathways in the pain cascade, achieving superior analgesia with reduced reliance on opioids. Evidence from institutions like Zhongshan Hospital and the Mayo Clinic has demonstrated that multimodal analgesia improves pain control, shortens recovery time, and reduces complications following POEM.12,13
Typical multimodal regimens for POEM include:
- Non-opioid analgesics, such as acetaminophen, selective COX-2 inhibitors, and dexmedetomidine, to reduce inflammation and central sensitization.
- Regional anesthesia (eg, thoracic paravertebral block or erector spinae plane block) to provide localized pain relief without systemic opioid side effects.
- Magnesium sulfate, shown to reduce visceral hyperalgesia and opioid requirements during the first 24 hours post-POEM.
Considering the available evidence, multimodal analgesia emerges as the most effective strategy for POEM. However, its success depends on careful customization based on patient characteristics, procedure complexity, and institutional resources. Preemptive analgesia may complement multimodal protocols, especially when combined with regional techniques or systemic agents to preclude pain onset. Rescue analgesia, while indispensable for breakthrough pain, should be used sparingly to avoid escalating opioid dependency.
By focusing on tailored, proactive, and comprehensive pain management plans, the challenges of postoperative pain following POEM can be effectively addressed, ensuring better patient outcomes and adherence to ERAS principles.
Limitations and Future Research Directions
The current study on postoperative pain management in POEM patients reveals several limitations, primarily due to the lack of consensus on optimal analgesic strategies and the insufficient understanding of the long-term effects of perioperative analgesia on chronic pain development and quality of life. To address these gaps, future research should focus on refining multimodal analgesic regimens to enhance both immediate pain relief and long-term recovery outcomes. Additionally, there is a need to evaluate novel analgesic agents, particularly non-opioid alternatives, to decrease dependency on opioids and reduce associated side effects. Large-scale, multicenter clinical trials are essential to establish evidence-based protocols that can standardize pain management across various clinical settings and improve patient outcomes. Investigating the long-term consequences of postoperative pain management strategies will also be crucial for developing comprehensive protocols that prioritize not only immediate relief but also sustained recovery and overall well-being for POEM patients.
Conclusions
Effective postoperative pain management is crucial for optimizing recovery and improving outcomes in POEM patients. Given the multifactorial nature of pain following POEM, a multimodal analgesia approach that integrates pharmacological and non-pharmacological strategies is currently the best option for managing pain. This review highlights the need for selecting more appropriate analgesics within the multimodal framework, including optimizing the use of opioids and non-opioids such as acetaminophen, NSAIDs, and magnesium, which have shown promise in reducing pain and opioid consumption. Additionally, the role of regional/local anesthesia, such as thoracic paravertebral blocks and erector spinae plane blocks, remains to be validated through more robust evidence, as their efficacy in POEM is still inconclusive. The potential benefits of intraoperative lidocaine and magnesium also warrant further investigation. Future research must prioritize prospective trials to validate these emerging strategies and address gaps in current evidence. By focusing on these areas, we can develop more effective, tailored pain management protocols that enhance patient comfort and improve overall surgical outcomes and long-term well-being for patients undergoing POEM.
Abbreviations
COX-2, Cyclooxygenase-2; CNS, Central Nervous System; DEX, Dexmedetomidine; DORs, δ-opioid receptors; ERAS, Enhanced Recovery After Surgery; ESPB, Erector Spinae Plane Block; ESD, Endoscopic Submucosal Dissection; GPCR, G Protein-Coupled Receptor; KORs, κ-opioid receptors; MORs, μ-opioid receptors; NMDA, N-Methyl-D-Aspartate; NSAIDs, Nonsteroidal Anti-Inflammatory Drugs; POEM, Peroral Endoscopic Myotomy; TDF, Transdermal Fentanyl Patches; TPVB, Thoracic Paravertebral Block.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pandolfino JE, Gawron AJ. Achalasia: a systematic review. JAMA. 2015;313(18):1841–1852. doi:10.1001/jama.2015.2996
2. Farrukh A, DeCaestecker J, Mayberry JF. An epidemiological study of achalasia among the South Asian population of Leicester, 1986–2005. Dysphagia. 2008;23(2):161–164. doi:10.1007/s00455-007-9116-1
3. Mayberry JF. Epidemiology and demographics of achalasia. Gastrointest Endosc Clin N Am. 2001;11(2):235–48, v.
4. Gockel I, Muller M, Schumacher J. Achalasia--a disease of unknown cause that is often diagnosed too late. Dtsch Arztebl Int. 2012;109(12):209–214. doi:10.3238/arztebl.2012.0209
5. Werner YB, Hakanson B, Martinek J, et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381(23):2219–2229. doi:10.1056/NEJMoa1905380
6. Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010;42(4):265–271. doi:10.1055/s-0029-1244080
7. Han SY, Youn YH. Role of endoscopy in patients with achalasia. Clin Endosc. 2023;56(5):537–545. doi:10.5946/ce.2023.001
8. Ramchandani M, Nabi Z, Inavolu P, Reddy DN. Recent advancements and future perspectives of per oral endoscopic myotomy. Clin Gastroenterol Hepatol. 2024;22(10):1983–1996e2. doi:10.1016/j.cgh.2024.02.032
9. Li QL, Chen WF, Zhou PH, et al. Peroral endoscopic myotomy for the treatment of achalasia: a clinical comparative study of endoscopic full-thickness and circular muscle myotomy. J Am Coll Surg. 2013;217(3):442–451. doi:10.1016/j.jamcollsurg.2013.04.033
10. Moore MD, Gray KD, Panjwani S, et al. 2017 scientific session of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) Houston, Texas, USA, 22–25 March 2017: poster presentations. Surg Endosc. 2017;31(Suppl 1):137–334. doi:10.1007/s00464-017-5445-9
11. Cloutier Z, Mann A, Doumouras AG, Hong D. Same-day discharge is safe and feasible following POEM surgery for esophageal motility disorders. Surg Endosc. 2021;35(7):3398–3404. doi:10.1007/s00464-020-07781-4
12. Misra L, Fukami N, Nikolic K, Trentman TL. Peroral endoscopic myotomy: procedural complications and pain management for the perioperative clinician. Med Devices. 2017;10:53–59. doi:10.2147/MDER.S115632
13. Wang Y, Zhou D, Xiong W, Ge S. Modified protocol for enhanced recovery after surgery is beneficial for achalasia patients undergoing peroral endoscopic myotomy: a randomized prospective trial. Wideochir Inne Tech Maloinwazyjne. 2021;16(4):656–663. doi:10.5114/wiitm.2021.104013
14. Chen WN, Xu YL, Zhang XG. High Eckardt score and previous treatment were associated with poor postperoral endoscopic myotomy pain control: a retrospective study. World J Clin Cases. 2022;10(17):5655–5666. doi:10.12998/wjcc.v10.i17.5655
15. Rai M, Nazarin A, Taylor C, et al. A randomized controlled pilot study of topical ropivacaine for prevention of post-POEM pain. J Can Assoc Gastroenterol. 2022;5(5):221–225. doi:10.1093/jcag/gwac007
16. Xie G, Li S, Zeng M, et al. Oxycodone is superior to morphine for pain relief following peroral oesophageal myotomy: a prospective, randomized, controlled trial. Wideochir Inne Tech Maloinwazyjne. 2022;17(4):624–633. doi:10.5114/wiitm.2022.118544
17. Elmunzer BJ, Lewis BR, Miller KF, et al. Paravertebral anesthetic nerve block for pain control after peroral endoscopic myotomy. Tech Innov Gastrointest Endosc. 2021;23(4):297–303. doi:10.1016/j.tige.2021.06.006
18. Yurtlu DA, Aslan F. Challenges in anesthesia management for peroral endoscopic myotomy: a retrospective analysis. Surg Laparosc Endosc Percutan Tech. 2021;31(6):729–733. doi:10.1097/SLE.0000000000000978
19. Gutman DA, George R, Moore L. Paravertebral block for a patient with achalasia undergoing a peroral endoscopic myotomy procedure: a case report. A A Pract. 2019;13(11):413–414. doi:10.1213/XAA.0000000000001088
20. Kim RK, Hwang JH, Tsui BC. Utilization of magnesium in opioid-free anesthesia for peroral endoscopic myotomy: a case report. A A Pract. 2021;15(1):e01372. doi:10.1213/XAA.0000000000001372
21. Ozkalayci O, Cetin S, Yenigun Y, Karakaya MA, Gurkan Y, Ercelen O. Erector spinae plane block for peroral endoscopic myotomy analgesia in pediatric patients. Reg Anesth Pain Med. 2020;45(6):482. doi:10.1136/rapm-2019-101005
22. Kim RK, Kim JW, Angelotti T, Esquivel M, Tsui BC, Hwang JH. Magnesium and esophageal pain after peroral endoscopic myotomy of the esophagus: a randomized, double-blind, placebo-controlled trial. Anesth Analg. 2024;140(1):54–61. doi:10.1213/ANE.0000000000006990
23. Khashab MA, Kumbhari V, Kalloo AN, Saxena P. Peroral endoscopic myotomy: a 4-step approach to a challenging procedure. Gastrointest Endosc. 2014;79(6):997–998. doi:10.1016/j.gie.2013.12.004
24. Shin S, Park CH, Kim HJ, Park SH, Lee SK, Yoo YC. Patient satisfaction after endoscopic submucosal dissection under propofol-based sedation: a small premedication makes all the difference. Surg Endosc. 2017;31(6):2636–2644. doi:10.1007/s00464-016-5276-0
25. Janig W. Neurobiologie viszeraler Schmerzen [Neurobiology of visceral pain]. Schmerz. 2014;28(3):233–251. doi:10.1007/s00482-014-1402-x
26. Loser B, Werner YB, Punke MA, et al. Considerations anesthesiques pour la prise en charge des patients atteints d’achalasie de l’oesophage subissant une myotomie per-orale endoscopique: compte rendu retrospectif d’une serie de cas [Anesthetic considerations for patients with esophageal achalasia undergoing peroral endoscopic myotomy: a retrospective case series review]. Can J Anaesth. 2017;64(5):480–488. doi:10.1007/s12630-017-0820-5
27. Hanaoka N, Uedo N, Ishihara R, et al. Clinical features and outcomes of delayed perforation after endoscopic submucosal dissection for early gastric cancer. Endoscopy. 2010;42(12):1112–1115. doi:10.1055/s-0030-1255932
28. Werner YB, von Renteln D, Noder T, et al. Early adverse events of per-oral endoscopic myotomy. Gastrointest Endosc. 2017;85(4):708–718e2. doi:10.1016/j.gie.2016.08.033
29. Lee JY, Lim CH, Kim DH, et al. Adverse events associated with peroral endoscopic myotomy affecting extended hospital stay: a multi-center retrospective study in South Korea. J Neurogastroenterol Motil. 2022;28(2):247–254. doi:10.5056/jnm21081
30. Holzer P. Local effector functions of capsaicin-sensitive sensory nerve endings: involvement of tachykinins, calcitonin gene-related peptide and other neuropeptides. Neuroscience. 1988;24(3):739–768. doi:10.1016/0306-4522(88)90064-4
31. Cordero-Erausquin M, Inquimbert P, Schlichter R, Hugel S. Neuronal networks and nociceptive processing in the dorsal horn of the spinal cord. Neuroscience. 2016;338:230–247. doi:10.1016/j.neuroscience.2016.08.048
32. Niruthisard S, Werawataganon T, Bunburaphong P, Ussawanophakiat M, Wongsakornchaikul C, Toleb K. Improving the analgesic efficacy of intrathecal morphine with parecoxib after total abdominal hysterectomy. Anesth Analg. 2007;105(3):822–824. doi:10.1213/01.ane.0000277489.87015.1d
33. Maund E, McDaid C, Rice S, Wright K, Jenkins B, Woolacott N. Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs for the reduction in morphine-related side-effects after major surgery: a systematic review. Br J Anaesth. 2011;106(3):292–297. doi:10.1093/bja/aeq406
34. Wardhan R, Chelly J. Recent advances in acute pain management: understanding the mechanisms of acute pain, the prescription of opioids, and the role of multimodal pain therapy. F1000Res. 2017;6:2065. doi:10.12688/f1000research.12286.1
35. McRoberts JA, Coutinho SV, Marvizon JC, et al. Role of peripheral N-methyl-D-aspartate (NMDA) receptors in visceral nociception in rats. Gastroenterology. 2001;120(7):1737–1748. doi:10.1053/gast.2001.24848
36. Herman TF, Cascella M, Muzio MR. Mu Receptors. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
37. Wang A, Murphy J, Shteynman L, Daksla N, Gupta A, Bergese S. Novel opioids in the setting of acute postoperative pain: a narrative review. Pharmaceuticals. 2023;17(1):29. doi:10.3390/ph17010029
38. Feng Y, He X, Yang Y, Chao D, Lazarus LH, Xia Y. Current research on opioid receptor function. Curr Drug Targets. 2012;13(2):230–246. doi:10.2174/138945012799201612
39. Wang YH, Chai JR, Xu XJ, et al. Pharmacological characterization of dezocine, a potent analgesic acting as a kappa partial agonist and mu partial agonist. Sci Rep. 2018;8(1):14087. doi:10.1038/s41598-018-32568-y
40. Choi HS, Kim KO, Chun HJ, et al. The efficacy of transdermal fentanyl for pain relief after endoscopic submucosal dissection: a prospective, randomised controlled trial. Dig Liver Dis. 2012;44(11):925–929. doi:10.1016/j.dld.2012.06.015
41. Ramsay MA, Luterman DL. Dexmedetomidine as a total intravenous anesthetic agent. Anesthesiology. 2004;101(3):787–790. doi:10.1097/00000542-200409000-00028
42. Chang ET, Certal V, Song SA, et al. Dexmedetomidine versus propofol during drug-induced sleep endoscopy and sedation: a systematic review. Sleep Breath. 2017;21(3):727–735. doi:10.1007/s11325-017-1465-x
43. Luo X, Chen P, Chang X, et al. Intraoperative dexmedetomidine decreases postoperative pain after gastric endoscopic submucosal dissection: a prospective randomized controlled trial. J Clin Med. 2023;12(5):1816. doi:10.3390/jcm12051816
44. Laconi G, Coppens S, Roofthooft E, Van De Velde M. High dose glucocorticoids for treatment of postoperative pain: a systematic review of the literature and meta-analysis. J Clin Anesth. 2024;93:111352. doi:10.1016/j.jclinane.2023.111352
45. Corcoran TB, Martin C, O’Loughlin E, et al. Dexamethasone and clinically significant postoperative nausea and vomiting: a prespecified substudy of the randomised perioperative administration of dexamethasone and infection (PADDI) trial. Br J Anaesth. 2022;129(3):327–335. doi:10.1016/j.bja.2022.05.018
46. Lee HW, Lee H, Chung H, et al. The efficacy of single-dose postoperative intravenous dexamethasone for pain relief after endoscopic submucosal dissection for gastric neoplasm. Surg Endosc. 2014;28(8):2334–2341. doi:10.1007/s00464-014-3463-4
47. Pyo JH, Lee H, Min YW, et al. A comparative randomized trial on the optimal timing of dexamethasone for pain relief after endoscopic submucosal dissection for early gastric neoplasm. Gut Liver. 2016;10(4):549–555. doi:10.5009/gnl15302
48. Koppert W, Ostermeier N, Sittl R, Weidner C, Schmelz M. Low-dose lidocaine reduces secondary hyperalgesia by a central mode of action. Pain. 2000;85(1–2):217–224. doi:10.1016/s0304-3959(99)00268-7
49. Estebe JP. Intravenous lidocaine. Best Pract Res Clin Anaesthesiol. 2017;31(4):513–521. doi:10.1016/j.bpa.2017.05.005
50. Vigneault L, Turgeon AF, Cote D, et al. Perioperative intravenous lidocaine infusion for postoperative pain control: a meta-analysis of randomized controlled trials. Can J Anaesth. 2011;58(1):22–37. doi:10.1007/s12630-010-9407-0
51. Wu F, Zhan L, Xu W, Bian J. Effect of intravenous lidocaine on outcomes in patients receiving propofol for gastrointestinal endoscopic procedures: an updated systematic review and meta-analysis. Eur J Clin Pharmacol. 2024;80(1):39–52. doi:10.1007/s00228-023-03589-y
52. Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lidocaine infusion facilitates acute rehabilitation after laparoscopic colectomy. Anesthesiology. 2007;106(1):
53. Ness TJ. Intravenous lidocaine inhibits visceral nociceptive reflexes and spinal neurons in the rat. Anesthesiology. 2000;92(6):1685–1691. doi:10.1097/00000542-200006000-00028
54. Shin HJ, Na HS, Do SH. Magnesium and pain. Nutrients. 2020;12(8):2184. doi:10.3390/nu12082184
55. Dahake JS, Verma N, Bawiskar D. Magnesium sulfate and its versatility in anesthesia: a comprehensive review. Cureus. 2024;16(3):e56348. doi:10.7759/cureus.56348
56. Kim B, Lee H, Chung H, et al. The efficacy of topical bupivacaine and triamcinolone acetonide injection in the relief of pain after endoscopic submucosal dissection for gastric neoplasia: a randomized double-blind, placebo-controlled trial. Surg Endosc. 2015;29(3):714–722. doi:10.1007/s00464-014-3730-4
57. Jung JH, Jang HJ, Bang CS, Baik GH, Park SW. Efficacy of submucosal bupivacaine injection for pain relief after endoscopic submucosal dissection: a multicenter, prospective, randomized controlled, and double-blind trial. Medicine. 2019;98(17):e15360. doi:10.1097/MD.0000000000015360
58. Xuan C, Yan W, Wang D, et al. Efficacy of preemptive analgesia treatments for the management of postoperative pain: a network meta-analysis. Br J Anaesth. 2022;129(6):946–958. doi:10.1016/j.bja.2022.08.038
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Ultrasound-Guided Thoracic Paravertebral Block on Postoperative Quality of Recovery in Patients Undergoing Percutaneous Nephrolithotomy: A Randomized Double-Blind Placebo-Controlled Trial
Yan Z, Lin H, Yang Y, Yang J, Li X, Yao Y
Journal of Pain Research 2023, 16:1301-1310
Published Date: 19 April 2023