")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Potential Value of Plasma-Based Biomarkers for Prediction of Episodic Memory Performance and Identification of Individuals with Amnestic Mild Cognitive Impairment
Authors Wang M, Zhang Z, Shi Y, Shu H, Xie C, Ren Q, Wang Z
Received 8 January 2025
Accepted for publication 14 April 2025
Published 5 May 2025 Volume 2025:21 Pages 999—1010
DOI https://doi.org/10.2147/NDT.S516476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Mengxue Wang,1,* Zhengsheng Zhang,1,* Yachen Shi,2 Hao Shu,1 Chunming Xie,1 Qingguo Ren,1 Zan Wang1
1Department of Neurology, Zhongda Hospital, School of Medicine, Jiangsu Provincial Key Laboratory of Brain Science and Medicine, Southeast University, Nanjing, 210009, People’s Republic of China; 2Department of Neurology, Nanjing Medical University Affiliated Wuxi People’s Hospital, Wuxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zan Wang, Department of neurology, Zhongda Hospital, School of Medicine, Jiangsu Provincial Key Laboratory of Brain Science and Medicine, Southeast University, Nanjing, 210009, People’s Republic of China, Email [email protected]
Objective: Patients with amnestic mild cognitive impairment (aMCI) are thought to be highly susceptible to developing Alzheimer’s disease (AD). The study aimed to investigate the possibilities of plasma-biomarkers for individual patient identification of aMCI and prediction of episodic memory.
Methods: We recruited 87 healthy controls and 68 aMCI patients in this study; and 22/68 aMCI patients completed 3-year follow-up visits, with six aMCI patients converting to AD. An ultrasensitive quantitative method was employed to measure the levels of plasma biomarkers.
Results: Relative to healthy controls, the aMCI patients showed significantly higher levels of plasma neurofilament light (NfL) and lower levels of plasma Aβ 40, Aβ 42 and Aβ 42/Aβ 40 ratio (all P values < 0.01). Using multivariate relevance vector regression models, we further demonstrated plasma biomarkers could accurately predict baseline Rey’s Auditory Verbal Learning Test-20 min delayed recall (AVLT-DR) scores (r = 0.362, P value < 0.001) and 3-year longitudinal AVLT-DR changes (r = 0.365, P value < 0.001) for individual aMCI patients; plasma-indicators contributed most to the predictions including total-tau and NfL. Finally, by using support vector machine model, the combination of plasma Aβ 42/Aβ 40, mini-mental state examination (MMSE) score, and hippocampal/parahippocampal volume had the highest accuracy of 77.42% (sensitivity = 72.06%, specificity = 81.61%) for identifying aMCI patients.
Conclusion: We provided support to the use of plasma total-tau and NfL as simple biomarkers to predict the severity of episodic memory deficit for individual aMCI patients and aMCI progression, and further demonstrated that the combination of plasma Aβ 42/Aβ 40, hippocampal/parahippocampal volume, and MMSE score could serve as an integrated screening tool to select aMCI individuals.
Keywords: Alzheimer’s disease, amnestic mild cognitive impairment, episodic memory, machine learning, plasma-biomarkers
Introduction
Alzheimer’s disease (AD) is an irreversible neurodegenerative disease characterized by cognitive decline and memory impairment, which may be accompanied by emotional or behavioral abnormalities.1–3 Patients with amnestic mild cognitive impairment (aMCI) are thought to be highly susceptible to developing AD.4 It has been established that early aMCI therapies can prevent or postpone the onset of AD. Therefore, early identification of aMCI patients and/or prediction of the aMCI progression are critical issues for clinicians.
Blood-based biomarkers have recently emerged as a promising predictive tool for AD.5 Compared with other methods of detecting AD, such as cerebrospinal fluid (CSF) collection or brain positron emission tomography (PET) imaging,6–9 blood sampling is less invasive, more scalable, and easily accessible in primary medical settings, thereby saving time and cost.10,11 Previous autopsy studies have shown that blood biomarkers associated with amyloid,12 tau pathology,13 and neurodegeneration14 are significantly correlated with brain deposits of amyloid and tau, as well as their measurements in CSF and brain PET.15 This evidence indicated that blood-based biomarkers performed well in predicting cognitive decline, dementia, and its progression. Although several blood biomarkers that aid in the diagnosis of AD have been developed,16 the evidence regarding the accuracy of blood-based biomarkers in diagnosing patients with aMCI remains limited at present. A previous meta-analysis examined the accuracy of blood biomarkers in detecting the conversion from aMCI to AD and found that plasma total tau protein (T-tau) plays an important role in this process.17 Another meta-analysis showed that T-tau, P-tau 181, and NfL in the blood increased from controls to aMCI to AD. In addition, Aβ42, Aβ42/Aβ40 ratio, and P-tau 217, measured using ultrasensitive platforms, also demonstrated high accuracy in the diagnosis from controls to aMCI to AD.18 Chen et al demonstrated that blood biomarkers are minimally invasive and cost-effective tools for detecting AD; however, the evidence for detecting aMCI remains limited.19 Therefore, exploring the value of blood biomarkers in screening for patients with aMCI and predicting their future continuous cognitive changes is of significant importance. Thus, additional research is needed to evaluate blood biomarkers’ diagnostic utility for aMCI and their predictive value for tracking cognitive decline in these patients.
A new trend which is using multivariate machine learning and pattern classification techniques has been effective in increasing the applicability of plasma-based data.20,21 Considering that patients with aMCI consistently experience the development of cognitive impairment, the range of alteration in an index measuring cognitive status in those patients will be multi-valued, either ordinal or continuous, rather than dichotomous.22,23 The ability to predict future neuropsychological scores based on blood biomarkers at baseline is even more important, as it is highly valuable for tracking disease progression and treatment response. Episodic memory impairment is a primary symptom of aMCI.24,25 The Rey Auditory Verbal Learning Test (AVLT) is a widely used neuropsychological assessment of episodic memory, demonstrating clinical utility in the early detection of AD and aMCI.26 Furthermore, extensive research supports the association between AVLT performance and disease progression in individuals with aMCI.27,28 Thus, the ability to predict AVLT memory score29 or clinical changes from plasma-based measurements is even more important for aMCI patients, as it would help track aMCI progression and improve patient management.
Motivated by the aforementioned issues, we first examined the possibility of using plasma-based measurements to predict AVLT-20 min delayed recall (AVLT-DR) scores and 3-year AVLT-DR changes for individual aMCI patients using a pattern regression technique called multivariate relevance vector regression (RVR),30 which is a reliable regression method for producing robust estimates of continuous clinical variables.31,32 Furthermore, we conducted an exploratory classification analysis by using the support vector machine (SVM) method33 to investigate the viability of combining plasma-based measurements to accurately distinguish aMCI patients from healthy control (HC) subjects.
Methods and Materials
Participants
This present study recruited 68 aMCI patients and 87 hC subjects, through a normal community health screening and newspaper advertisements at the Affiliated ZhongDa Hospital of Southeast University. All of the participants were Chinese Han and right-handed, and they underwent a standardized clinical interview. The questionnaire for this study included information on education, medical history, and the use of medications. A description of the specific inclusion and exclusion criteria was contained in the Supplementary Materials. Blind methods were employed in the data collecting process to reduce potential selection bias. This study complies with the Declaration of Helsinki. The Research Ethics Committee of Affiliated ZhongDa Hospital and the Southeast University gave their approval for this work (2016ZDKYSB032). Before the trial began, informed permission forms had to be signed by each subject. Among 68 aMCI patients, 22 completed visits at 3-year follow-up, with six aMCI patients converting to AD. The follow-up study was performed at an average of 32 months (19–48 months). Notably, at follow-up, the neuropsychological assessments were identical to those conducted at baseline.
Neuropsychological Assessment
All neuropsychological tests were assessed by highly experienced professional neurologists. The AVLT is a potent neuropsychological instrument for testing episodic memory,34 by offering scores for analyzing several components of memory. In a nutshell, the AVLT comprises three successive trails that offer a list of twelve words. Following an audible reading of the list, the participant is instructed to quickly recollect as many words as they can. This process is carried out three times in a row. A further 20 minutes of interpolated testing are then given to the individual, after which time they are asked to recall the terms from the initial list (AVLT-DR).
Measurement of Plasma Aβ40, Aβ42, Total-Tau, and NfL by Simoa Assays
The concentration of plasma Aβ40, Aβ42, total-tau, and NfL were examined on the Quanterix Simoa-HD1 Platform (Supplementary Materials).35 These four plasma-based measures and the Aβ42/Aβ40 ratio were utilized as a feature vector in the ensuing analysis of RVR prediction and SVM classification.
Structural MRI Data Acquisition and Processing
A 3.0 T Siemens Verio scanner with a 12-channel head coil was used to get MRI images. The Supplementary Materials contain information about the acquisition and processing of the structural MRI data. We finally calculated the average gray-matter volume (GMV) of each hippocampal/parahippocampal subregion in the Brainnectome atlas,36 a fine-gained, cross-validated atlas that links brain architecture to cognitive and psychosocial processes. Accordingly, for all participants, the mean GMV for all 16 hippocampal and parahippocampal subregions (including four hippocampal and 12 parahippocampal subregions) was extracted (Table S1). Therefore, the feature vector for the subsequent SVM classification study was these 16 district mean GMV values.
Statistical Analysis
Neuropsychological Performance, Plasma-Based Measurement and Hippocampal/Parahippocampal GMV
Between-group differences in neuropsychological performances, plasma-based measurements, and hippocampal/parahippocampal GMV were evaluated by nonparametric permutation tests.37 Notably, multiple linear regression analyses were performed before the permutation tests to exclude the confounding impacts of age, gender, and years of education.
Multivariate RVR Analysis
For each aMCI patient, a feature vector was created by concatenating the baseline five plasma-based values. We first evaluated the correlation between baseline AVLT-DR scores and plasma-based data using multivariate RVR.38 We used leave-one-out cross-validation (LOOCV) to measure the out-of-sample generality of the model to quantify the precision of the predictions. The precision of the forecast was measured using the correlation coefficient (r) and the mean absolute error (MAE) between the real and forecasted AVLT-DR scores. The purpose of the permutation tests, which involve 1000 permutations, was to ascertain whether the coefficient r and MAE were significantly higher than would be predicted by chance. The absolute magnitude of the RVR weight of each feature quantifies its contribution to the model. Notably, as in our previous studies,38,39 a 10-fold cross-validation was further applied to validate this prediction result. The details about RVR analyses are described in the Supplementary Materials.
Furthermore, to investigate the potential of plasma-based measurements in predicting aMCI progression, we further conducted an exploratory analysis using the RVR model to predict 3-year AVLT-DR changes from baseline plasma-based measurements.
SVM-Based Classification
The initial step in the exploration of a time-effective and cost-effective pre-screening tool for identifying people at high risk for AD was the classification of the aMCI and HC groups using linear SVM based on plasma-based measures. Additionally, a fused classifier that integrates three classifiers (ie, the plasma-based measurements, MMSE score, and hippocampal/parahippocampal GMV) via the sum rule was employed in this study to attain improved performance in classification. In this study, LOOCV and 10-fold cross-validation were also employed to validate the effectiveness of classifiers.40 The generalizability of the classifiers was evaluated quantitatively using the metrics of accuracy, sensitivity, and specificity. A receiver operating characteristic (ROC) graph was used to assess the performance of the classifier.41 The permutation test was used to examine whether the accuracy and area under a ROC curve (AUC) of the fused classifier were considerably higher than the values expected by chance40 (Supplementary Materials). Lastly, a higher absolute weight denotes a greater contribution from the associated attribute to the classification.
Results
Demographic and Clinical Characteristics
At baseline, the scores of the aMCI patients on the MMSE, MDRS-2, and AVLT-DR tests were considerably lower than those of the HC participants (all P values <0.001) (Table 1). All neuropsychological data for the aMCI patients and healthy controls are shown in Table S2. Compared with the HC subjects, the aMCI patients showed significantly higher levels of plasma NfL and lower levels of plasma Aβ40, Aβ42 and Aβ42/Aβ40 ratio (Ps <0.01) (Table 1). The aMCI patients also indicated significantly lower GMV bilaterally in the brain subregions of hippocampus (ie, Hipp_L_2_1, Hipp_L_2_2 and Hipp_R_2_2) and parahippocampal gyrus (ie, PhG_L_6_4, PhG_R_6_4 and PhG_L_6_5) relative to the HC subjects (all P values <0.05) (Table 1). Among 68 aMCI patients, 22 completed the 3-year follow-up visit; their demographic and clinical characteristics are presented in Table S3.
 |
Table 1 Demographics, Neuropsychological Performances, Plasma-Based Measurements and Hippocampal/Parahippocampal Volumes of the aMCI Patients and Healthy Controls |
Plasma-Based Biomarkers Predicted Episodic Memory Performance (ie, AVLT-DR Score) in aMCI Patients
We first predicted the baseline AVLT-DR score by using the plasma-based measurements acquired at baseline. The personal prediction of baseline AVLT-DR scores was made possible by applying the method of RVR to the plasma-based measures (prediction r = 0.362, MAE = 0.988, Pperm value <0.001; Figure 1A, left panel; Table 2). The plasma-based measures that contributed most to the forecasting were total-tau and NfL (Figure 1A, right panel). Importantly, to confirm this outcome, we used 10-fold cross-validation as well. The primary conclusions drawn from the LOOCV method were validated by the correlation coefficient and MAE values that were obtained, which remained significant (prediction r = 0.359, MAE = 1.015, Pprediction r value = 0.001, PMAE value <0.001).
 |
Table 2 Results of RVR Prediction Using the Plasma-Based Measurements |
 |
Figure 1 Prediction of the baseline AVLT-DR scores and 3-year longitudinal AVLT-DR changes for individual aMCI patients based on plasma-based biomarkers. Using RVR model, the plasma-based measures can significantly predict the baseline AVLT-DR scores (A, left panel; r = 0.362, P < 0.001), which contributed most to the forecasting were total-tau and NfL (A, right panel). The baseline plasma-based measurements can also predict 3-year longitudinal AVLT-DR changes (B, left panel; r = 0.365, P < 0.001), and total-tau and NfL contributed the most to the prediction (B, right panel). Abbreviations: aMCI, amnestic mild cognitive impairment; AVLT-DR, Auditory Verbal Learning Test with a 20 min delayed recall; MAE, mean absolute error; NfL, neurofilament light; RVR, relevance vector regression; t-tau, total tau. |
Furthermore, we conducted an exploratory analysis using the RVR model to predict 3-year AVLT-DR changes from baseline plasma-based measurements. The actual and anticipated 3-year AVLT-DR changes in the model for aMCI patients were correlated at r = 0.365 (Pperm value <0.001) (Figure 1B, left panel). Interestingly, the plasma-based measurements that made the most contributions to the forecast also included total-tau and NfL (Figure 1B, right panel).
The Diagnostic Power of Plasma-Based Biomarkers for aMCI
The classification results of the plasma indicators-based classifier and the fused classifier are concluded in Table 3. According to the LOOCV, the plasma indicators-based classifier produced a classification accuracy of 71.61% with a significance of P value <0.001. However, the fused classifier produced a higher accuracy of identifying aMCI patients (ie, accuracy = 77.42%) with an AUC of 0.79 (Figure 2A), which had a more balanced sensitivity and specificity (ie, sensitivity = 72.06%, specificity = 81.61%) than the plasma indicators-based classifier. The 10-fold cross-validation acquired the average classification precision of the fused classifier of 76.13%. This result demonstrated the robustness of the finding, as it was comparable to those of the LOOCV. More importantly, further investigation showed that the features most useful for categorization discrimination comprised plasma Aβ42/Aβ40 ratio, MMSE score, and hippocampal/parahippocampal subregions’ GMV (ie, Hipp_R_2_2, Hipp_L_2_2, PhG_L_6_6, PhG_R_6_5, and PhG_R_6_2) (Figure 2B).
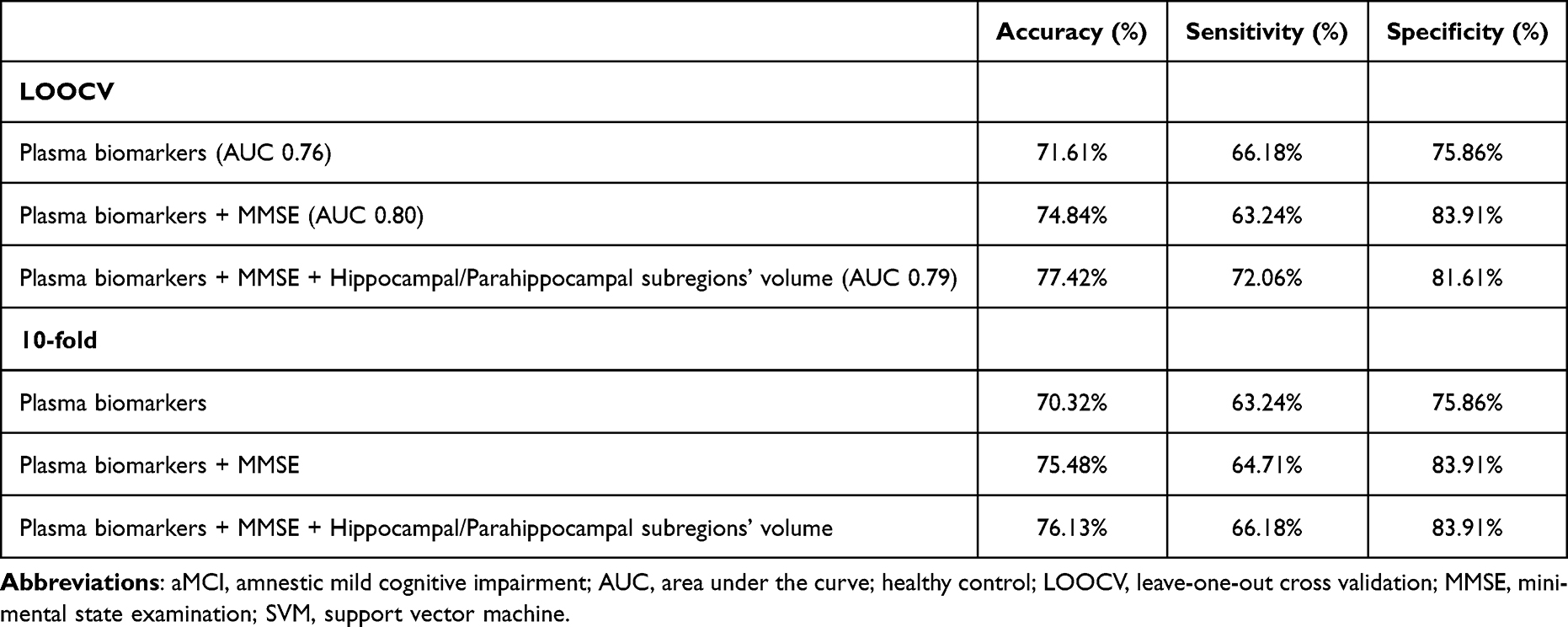 |
Table 3 Classification Performances of the SVM Models in the aMCI and HC Classification Tasks |
 |
Figure 2 Support vector machine (SVM)-based classification. The fused classifier (ie, integrating the plasma-based measurements, MMSE score and hippocampal/parahippocampal subregions’ GMV) yielded a higher accuracy of identifying aMCI patients (ie, accuracy = 77.42%, AUC = 0.79) (A). The most discriminative features for classification included plasma Aβ42/Aβ40 ratio, MMSE score and hippocampal/parahippocampal subregions’ GMV (B). Abbreviations: Aβ, amyloid-β; aMCI, amnestic mild cognitive impairment; GMV, gray-matter volume; MMSE, mini-mental state examination; NfL, neurofilament light; t-tau, total tau. |
Discussion
In this current preliminary study, our first analysis revealed that plasma Aβ40 and Aβ42 levels, and Aβ42/Aβ40 ratio were higher in the aMCI patients in contrast to HC subjects. Then, through using the machine learning framework, we further demonstrated that the plasma-based measurements could accurately predict baseline episodic performance (indicated by AVLT-DR scores) and 3-year AVLT-DR changes for individual aMCI patients; the plasma-based biomarkers that contributed the most to the predictions included the plasma total-tau and NfL levels. Finally, by using the SVM model, the combination of plasma Aβ42/Aβ40 ratio, MMSE score, and hippocampal/parahippocampal volume supported aMCI identification with an accuracy of 77.42%.
Since the neurodegeneration of AD progresses years before the disease onset and since therapy is more effective at the early stage of the disease (eg, the aMCI stage), there is a dire need to forecast the progression of aMCI as measured by cognitive scores, such as AVLT-DR, which would be more concentrated on functions linked to aMCI, and to identify a small set of biomarkers most predictive of the progression. In reality, nevertheless, the short-term (three years, for example) evolution of cognitive deterioration in aMCI patients is an ongoing occurrence. Furthermore, stable aMCI patients should only experience minor variations. Therefore, relatively objective biomarkers that are less affected by different clinical evaluators and that could accurately predict clinical scores (eg, AVLT-DR) and clinical changes are required and of great clinical significance,42 as they would help track disease progression and then improve patient management.
In this present study, we employed baseline plasma-based characteristics in a machine learning framework to generate continually valued predictions on baseline AVLT-DR scores and 3-year AVLT-DR changes for aMCI patients at each patient level. We proved that the baseline plasma-based measurements could be used to predict individual aMCI patients’ episodic memory performance (indicated by AVLT-DR scores) at baseline. The plasma total-tau and NfL were the plasma-based metrics that made the biggest contributions to the forecast. More importantly, further analysis using the longitudinal sample revealed that the plasma total-tau and NfL levels also contributed the most to the plasma-based multivariate model to predict 3-year AVLT-DR changes for individual aMCI patients. These findings demonstrated the potential of plasma total-tau and NfL in predicting baseline AVLT-DR scores and 3-year longitudinal AVLT-DR changes for individual aMCI patients. Indeed previous studies43 have demonstrated that plasma total-tau and NfL could be considered as neurodegeneration biomarkers, such as neuroaxonal damage. Previous studies also demonstrated that high plasma total-tau or NfL level is associated with both poorer global cognitive performance (eg, MMSE score) and brain atrophy in aMCI patients.44,45 A community-based cohort study analyzed the risk and predictive performance of six AD blood biomarkers for all-cause and AD dementia in a general population without dementia at baseline. The results showed that high levels of NfL were associated with an increased risk of all-cause or AD dementia over a mean follow-up period of 10 years.46 Other longitudinal studies also provide evidence that increased total-tau and NfL were related to lower MMSE scores and a faster rate of brain atrophy over time, as indicated by changes in whole-brain volume, ventricular volume, and hippocampus volume in aMCI or AD.47,48 Therefore, our findings add further support to the use of plasma total-tau and NfL as simple, accessible pre-screening tools to predict the severity of episodic memory deficit for aMCI patients and aMCI progression.
Finding accurate and stable blood biomarkers would be very helpful in daily work, as it would enable screening of a wider range of individuals at high risk for AD, hence sending fewer people for further invasive testing. Recent studies combining multiple blood biomarkers have achieved breakthroughs in the early diagnosis of AD. The superior performance of multi-analyte panels over single biomarkers. Li et al developed an integrated model to predict the conversion to dementia in patients with MCI by combining the apolipoprotein E ε4 allele status, MMSE scores, plasma p-tau181, left hippocampal and right amygdala volumes, and right inferior temporal cortical thickness. The area under the curve (AUC) reached 0.85.49 The study by Yuan et al demonstrated that the dynamic changes in plasma p-tau181 and NfL concentrations are positively correlated with the risk of conversion from MCI to AD. When plasma p-tau181 and NfL were combined to predict the progression of AD, a better predictive performance was achieved, with an AUC of 0.701.50 Additionally, a blood-based multiplex biomarker assay for AD that measures the levels of 21 proteins can accurately classify AD (AUC = 0.94 to 0.99) and MCI (AUC = 0.84 to 0.89). This demonstrated the practicality of blood-based multi-pathway biomarker detection in the early screening of AD.51 In this study, within the first diagnostic pre-screening step, the SVM model with plasma-based measurements alone identified aMCI patients with an accuracy of 71.61%. When adding a cognitive screening tool like MMSE and bilateral hippocampal/parahippocampal GMV in the SVM model, discrimination reached an accuracy of 77.42% (AUC = 0.79; sensitivity = 72.06%, specificity = 81.61%). Although the classification accuracy is moderate, this study complements the previous findings that blood-based biomarkers have potential value in screening for aMCI. Importantly, further analysis demonstrated that the most discriminative features for discrimination included plasma Aβ42/Aβ40 ratio, MMSE score, and hippocampal/parahippocampal GMV. Multiple research endeavors are examining the identification of Aβ peptides in plasma by diverse methods as a plausible indicator for AD.48,52 Patients with aMCI had reduced levels of plasma Aβ42/Aβ40 ratio, which is consistent with several studies that have also found comparable outcomes in AD.53,54 Importantly, many previous studies have found that plasma Aβ42/Aβ40 ratio can accurately predict Aβ accumulation in the brain, even using different methodological approaches.55–57 A more recent study demonstrated that the plasma Aβ42/Aβ40 ratio could discriminate dementia due to AD and dementia not due to AD.53 Additionally, our finding shows that the plasma Aβ42/Aβ40 ratio may have great value in combination with a set of simple additional variables, such as a cognitive screening tool like MMSE and hippocampal/parahippocampal GMV. Overall, the present identified features of the SVM model could be used as a preliminary instrument in the diagnostic chain. For example, in clinical practice, for large prevention studies, the initial pre-screening tool could be used to preselect individuals with high risk for AD progression into further diagnostic steps, such as lumbar puncture or PET scanning.
Several limitations should also be taken into account when summarising and extending the results of this study. First, our RVR predictions were obtained from a relatively small sample, especially from the longitudinal sample. The robustness and stability of our results were partially validated by the 10-fold cross-validation and the leave-one-out test, which were both utilized to assess the effectiveness of our methodology. Further studies using a large independent sample would be important to validate the current findings. Second, the sensitivity of SVM models may be affected by the sample sizes, future research using larger sample sizes may result in better predictive sensitivity. Third, the patients with aMCI were recruited based on the clinical criteria only but lacked amyloid-PET imaging or CSF protein examination. Consequently, there may be a significant degree of biological and clinical heterogeneity in the current sample of aMCI patients. However, aMCI patients had significantly reduced cortical thickness in the hippocampus and parahippocampal gyrus, as well as lower plasma Aβ40 and Aβ42 levels than healthy controls, as demonstrated in our earlier investigations35,58,59 using the same dataset. As a result, it is possible that the aMCI patients in this research were partially uniform. Fourth, the present study did not focus on the impact of plasma biomarkers on short-term cognitive function changes in aMCI patients. Subsequent studies should increase follow-up time points to better observe changes in cognitive function. Fifth, the medication intake of the subjects during the follow-up period may have an impact on the results, which is another limitation of the study. Finally, only 22 aMCI patients completed visits at 3-year follow-up after baseline; and six aMCI patients converted to AD. Longitudinal studies with a large sample of aMCI converters and non-converters are needed to be conducted to detect the potential value of plasma-based biomarkers for predicting AD progression. Further, in future mechanistic studies, we will further investigate the correlation between serum biomarkers and imaging parameters.
Conclusion
In summary, our findings demonstrate that plasma biomarkers, particularly total-tau and NfL can predict episodic memory deficit and its progression for individual aMCI patients. The combination of plasma Aβ42/Aβ40, hippocampal/parahippocampal volume and MMSE score could serve as an pre-screening tool to identify people with aMCI. Based on plasma biomarkers, predicting the continuous changes in cognitive function of aMCI patients at the individual level will become a key breakthrough in personalized care and treatment.
Data Sharing Statement
The data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. The Research Ethics Committee of Affiliated ZhongDa Hospital and the Southeast University gave their approval for this work (2016ZDKYSB032). Informed consent was obtained from all individual participants included in the study.
Declaration
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Acknowledgments
We appreciate all the patients and volunteers who took part in this study. We appreciate Dr. Zaixu Cui for providing technical assistance.
Funding
This work was supported by the STI2030-Major Projects (grant number 2022ZD0211600); National Natural Science Foundation of China (grant number 81801680, 81801075, and 81870850); Health China•BuChang ZhiYuan Public welfare projects for Heart and brain health (grant number HIGHER2022130); Natural Science Foundation of Jiangsu Province (grant number BK20180379).
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Jeong HJ, Suh H, Lee YM, et al. Association of temporolimbic volumes with treatment response to antipsychotic medication for delusion in patients with Alzheimer’s disease. Alpha Psychiatry. 2021;22(5):244–249. doi:10.5152/alphapsychiatry.2021.21157
2. Menkü BE, Akın S, Tamdemir SE, Genis B, Altıparmak T, Cosar B. Diagnostic transitions from primary psychiatric disorders to underlying medical conditions: a 5-year retrospective survey from a university hospital sample. Alpha Psychiatry. 2024;25(2):226–232. doi:10.5152/alphapsychiatry.2024.231274
3. Jackson RJ, Hyman BT, Serrano-Pozo A. Multifaceted roles of APOE in Alzheimer disease. Nat Rev Neurol. 2024;20(8):457–474. doi:10.1038/s41582-024-00988-2
4. Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. 1999;56(3):303–308. doi:10.1001/archneur.56.3.303
5. Hansson O, Blennow K, Zetterberg H, Dage J. Blood biomarkers for Alzheimer’s disease in clinical practice and trials. Nat Aging. 2023;3(5):506–519. doi:10.1038/s43587-023-00403-3
6. Fandos N, Pérez-Grijalba V, Pesini P, et al. Plasma amyloid β 42/40 ratios as biomarkers for amyloid β cerebral deposition in cognitively normal individuals. Alzheimers Dement. 2017;8:179–187. doi:10.1016/j.dadm.2017.07.004
7. Dubois B, Feldman HH, Jacova C, et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 2014;13(6):614–629. doi:10.1016/S1474-4422(14)70090-0
8. Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA research framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535–562. doi:10.1016/j.jalz.2018.02.018
9. Palmqvist S, Stomrud E, Cullen N, et al. An accurate fully automated panel of plasma biomarkers for Alzheimer’s disease. Alzheimers Dement. 2023;19(4):1204–1215. doi:10.1002/alz.12751
10. Hampel H, O’Bryant SE, Molinuevo JL, et al. Blood-based biomarkers for Alzheimer disease: mapping the road to the clinic. Nat Rev Neurol. 2018;14(11):639–652. doi:10.1038/s41582-018-0079-7
11. Hampel H, Hu Y, Cummings J, et al. Blood-based biomarkers for Alzheimer’s disease: current state and future use in a transformed global healthcare landscape. Neuron. 2023;111(18):2781–2799. doi:10.1016/j.neuron.2023.05.017
12. Chatterjee P, Pedrini S, Doecke JD, et al. Plasma Aβ42/40 ratio, p-tau181, GFAP, and NfL across the Alzheimer’s disease continuum: a cross-sectional and longitudinal study in the AIBL cohort. Alzheimers Dement. 2023;19(4):1117–1134. doi:10.1002/alz.12724
13. Mielke MM, Dage JL, Frank RD, et al. Performance of plasma phosphorylated tau 181 and 217 in the community. Nat Med. 2022;28(7):1398–1405. doi:10.1038/s41591-022-01822-2
14. Janelidze S, Bali D, Ashton NJ, et al. Head-to-head comparison of 10 plasma phospho-tau assays in prodromal Alzheimer’s disease. Brain. 2023;146(4):1592–1601. doi:10.1093/brain/awac333
15. Association of CSF. Plasma, and imaging markers of neurodegeneration with clinical progression in people with subjective cognitive decline. Neurology. 2022;99(2):86. doi:10.1212/wnl.0000000000200734
16. Ashton NJ, Janelidze S, Mattsson-Carlgren N, et al. Differential roles of Aβ42/40, p-tau231 and p-tau217 for Alzheimer’s trial selection and disease monitoring. Nat Med. 2022;28(12):2555–2562. doi:10.1038/s41591-022-02074-w
17. Olsson B, Lautner R, Andreasson U, et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15(7):673–684. doi:10.1016/s1474-4422(16)00070-3
18. Qu Y, Ma YH, Huang YY, et al. Blood biomarkers for the diagnosis of amnestic mild cognitive impairment and Alzheimer’s disease: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;128:479–486. doi:10.1016/j.neubiorev.2021.07.007
19. Chen YR, Liang CS, Chu H, et al. Diagnostic accuracy of blood biomarkers for Alzheimer’s disease and amnestic mild cognitive impairment: a meta-analysis. Ageing Res Rev. 2021;71:101446. doi:10.1016/j.arr.2021.101446
20. Jiao B, Ouyang Z, Xiao X, et al. Development and validation of machine learning models with blood-based digital biomarkers for Alzheimer’s disease diagnosis: a multicohort diagnostic study. EClinicalMedicine. 2025;81:103142. doi:10.1016/j.eclinm.2025.103142
21. Souchet B, Michaïl A, Heuillet M, et al. Multiomics blood-based biomarkers predict Alzheimer’s predementia with high specificity in a multicentric cohort study. J Prev Alzheimers Dis. 2024;11(3):567–581. doi:10.14283/jpad.2024.34
22. Lyu S, Tian X, Li Y, Jiang B, Chen H. Multiclass probabilistic classification vector machine. IEEE Trans Neural Netw Learn Syst. 2020;31(10):3906–3919. doi:10.1109/tnnls.2019.2947309
23. Pei H, Yang B, Liu J, Chang KC. Active surveillance via group sparse bayesian learning. IEEE Trans Pattern Anal Mach Intell. 2022;44(3):1133–1148. doi:10.1109/tpami.2020.3023092
24. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the national institute on aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–279. doi:10.1016/j.jalz.2011.03.008
25. Moreau N, Viallet F, Champagne-Lavau M. Using memories to understand others: the role of episodic memory in theory of mind impairment in Alzheimer disease. Ageing Res Rev. 2013;12(4):833–839. doi:10.1016/j.arr.2013.06.005
26. Jannati A, Toro-Serey C, Gomes-Osman J, et al. Digital clock and recall is superior to the mini-mental state examination for the detection of mild cognitive impairment and mild dementia. Alzheimers Res Ther. 2024;16(1):2. doi:10.1186/s13195-023-01367-7
27. Shahid SS, Wen Q, Risacher SL, et al. Hippocampal-subfield microstructures and their relation to plasma biomarkers in Alzheimer’s disease. Brain. 2022;145(6):2149–2160. doi:10.1093/brain/awac138
28. Yu HH, Tan CC, Huang SJ, Zhang XH, Tan L, Xu W. Predicting the reversion from mild cognitive impairment to normal cognition based on magnetic resonance imaging, clinical, and neuropsychological examinations. J Affect Disord. 2024;353:90–98. doi:10.1016/j.jad.2024.03.009
29. Alden EC, Lundt ES, Twohy EL, et al. Mayo normative studies: a conditional normative model for longitudinal change on the Auditory Verbal Learning Test and preliminary validation in preclinical Alzheimer’s disease. Alzheimers Dement. 2022;14(1):e12325. doi:10.1002/dad2.12325
30. Tipping ME. Sparse Bayesian learning and the relevance vector machine. J Mach Learn Res. 2001;1(Jun):211–244.
31. Stonnington CM, Chu C, Kloppel S, Jack CR Jr, Ashburner J, Frackowiak RS. Predicting clinical scores from magnetic resonance scans in Alzheimer’s disease. NeuroImage. 2010;51(4):1405–1413. doi:10.1016/j.neuroimage.2010.03.051
32. Cui Z, Su M, Li L, Shu H, Gong G. Individualized prediction of reading comprehension ability using gray matter volume. Cerebral Cortex. 2018;28(5):1656–1672. doi:10.1093/cercor/bhx061
33. Noble WS. What is a support vector machine? Nat Biotechnol. 2006;24(12):1565–1567. doi:10.1038/nbt1206-1565
34. Moradi E, Hallikainen I, Hanninen T, Tohka J. Rey’s auditory verbal learning test scores can be predicted from whole brain mri in Alzheimer’s disease. NeuroImage Clin. 2017;13:415–427. doi:10.1016/j.nicl.2016.12.011
35. Shi Y, Lu X, Zhang L, et al. Potential value of plasma amyloid-β, total tau, and neurofilament light for identification of early Alzheimer’s disease. ACS Chem Neurosci. 2019;10(8):3479–3485. doi:10.1021/acschemneuro.9b00095
36. Fan L, Li H, Zhuo J, et al. The human brainnetome atlas: a new brain atlas based on connectional architecture. Cerebral Cortex. 2016;26(8):3508–3526. doi:10.1093/cercor/bhw157
37. Bullmore ET, Suckling J, Overmeyer S, Rabe-Hesketh S, Taylor E, Brammer MJ. Global, voxel, and cluster tests, by theory and permutation, for a difference between two groups of structural MR images of the brain. IEEE Trans Med Imag. 1999;18(1):32–42. doi:10.1109/42.750253
38. Wang Z, Yuan Y, Jiang Y, You J, Zhang Z. Identification of specific neural circuit underlying the key cognitive deficit of remitted late-onset depression: a multi-modal MRI and machine learning study. Prog Neuropsychopharmacol Biol Psychiatry. 2021;108:110192. doi:10.1016/j.pnpbp.2020.110192
39. Wang Z, Zhang Z, Xie C, Shu H, Liu D, Zhang Z. Identification of the neural circuit underlying episodic memory deficit in amnestic mild cognitive impairment via machine learning on gray matter volume. J Alzheimers Dis. 2021;84(3):959–964. doi:10.3233/JAD-210579
40. Xie Y, Cui Z, Zhang Z, et al. Identification of amnestic mild cognitive impairment using multi-modal brain features: a combined structural MRI and diffusion tensor imaging study. J Alzheimers Dis. 2015;47(2):509–522. doi:10.3233/JAD-150184
41. Tatliparmak AC, Yilmaz S, Ak R. Importance of receiver operating characteristic curve and decision curve analysis methods in clinical studies. Am J Emerg Med. 2023;70:196–197. doi:10.1016/j.ajem.2023.06.018
42. Bruno D, Jauregi Zinkunegi A, Pomara N, et al. Cross-sectional associations of CSF tau levels with Rey’s AVLT: a recency ratio study. Neuropsychology. 2023;37(6):628–635. doi:10.1037/neu0000821
43. Simrén J, Elmgren A, Blennow K, Zetterberg H. Fluid biomarkers in Alzheimer’s disease. Adv Clin Chem. 2023;112:249–281. doi:10.1016/bs.acc.2022.09.006
44. Cavedo E, Lista S, Houot M, et al. Plasma tau correlates with basal forebrain atrophy rates in people at risk for Alzheimer disease. Neurology. 2020;94(1):e30–e41. doi:10.1212/wnl.0000000000008696
45. Preische O, Schultz SA, Apel A, et al. Serum neurofilament dynamics predicts neurodegeneration and clinical progression in presymptomatic Alzheimer’s disease. Nat Med. 2019;25(2):277–283. doi:10.1038/s41591-018-0304-3
46. Grande G, Valletta M, Rizzuto D, et al. Blood-based biomarkers of Alzheimer’s disease and incident dementia in the community. Nat Med. 2025. doi:10.1038/s41591-025-03605-x
47. Mattsson N, Cullen NC, Andreasson U, Zetterberg H, Blennow K. Association between longitudinal plasma neurofilament light and neurodegeneration in patients with Alzheimer disease. JAMA neurology. 2019;76(7):791–799. doi:10.1001/jamaneurol.2019.0765
48. Zetterberg H. Blood-based biomarkers for Alzheimer’s disease-an update. J Neurosci Meth. 2019;319:2–6. doi:10.1016/j.jneumeth.2018.10.025
49. Li TR, Li BL, Zhong J, Xu XR, Wang TS, Liu FQ. A prediction model of dementia conversion for mild cognitive impairment by combining plasma pTau181 and structural imaging features. CNS Neurosci Ther. 2024;30(9):e70051. doi:10.1111/cns.70051
50. Yuan M, Lian S, Li X, Long X, Fang Y. Blood biomarkers in dynamic prediction of conversion to Alzheimer’s disease: an application of joint modeling. Int J Geriatr Psychiatry. 2024;39(3):e6079. doi:10.1002/gps.6079
51. Jiang Y, Uhm H, Ip FC, et al. A blood-based multi-pathway biomarker assay for early detection and staging of Alzheimer’s disease across ethnic groups. Alzheimers Dement. 2024;20(3):2000–2015. doi:10.1002/alz.13676
52. Wang X, Sun Y, Li T, Cai Y, Han Y. Amyloid-β as a blood biomarker for Alzheimer’s disease: a review of recent literature. J Alzheimers Dis. 2020;73(3):819–832. doi:10.3233/JAD-190714
53. Vogelgsang J, Shahpasand-Kroner H, Vogelgsang R, Streit F, Vukovich R, Wiltfang J. Multiplex immunoassay measurement of amyloid-β(42) to amyloid-β(40) ratio in plasma discriminates between dementia due to Alzheimer’s disease and dementia not due to Alzheimer’s disease. Experiment Brain Res. 2018;236(5):1241–1250. doi:10.1007/s00221-018-5210-x
54. Shahpasand-Kroner H, Klafki HW, Bauer C, et al. A two-step immunoassay for the simultaneous assessment of Aβ38, Aβ40 and Aβ42 in human blood plasma supports the Aβ42/Aβ40 ratio as a promising biomarker candidate of Alzheimer’s disease. Alzheimer’s Res Ther. 2018;10(1):121. doi:10.1186/s13195-018-0448-x
55. Vergallo A, Mégret L, Lista S, et al. Plasma amyloid β 40/42 ratio predicts cerebral amyloidosis in cognitively normal individuals at risk for Alzheimer’s disease. Alzheimers Dement. 2019;15(6):764–775. doi:10.1016/j.jalz.2019.03.009
56. Pérez-Grijalba V, Arbizu J, Romero J, Prieto E, Pesini P. Plasma Aβ42/40 ratio alone or combined with FDG-PET can accurately predict amyloid-PET positivity: a cross-sectional analysis from the AB255 Study. Neurol Ther. 2019;11(1):96. doi:10.1007/s40120-019-00164-5
57. Risacher SL, Fandos N, Romero J, et al. Plasma amyloid beta levels are associated with cerebral amyloid and tau deposition. Alzheimers Dement. 2019;11:510–519. doi:10.1016/j.dadm.2019.05.007
58. Wang Z, Dai Z, Shu H, et al. APOE genotype effects on intrinsic brain network connectivity in patients with amnestic mild cognitive impairment. Sci Rep. 2017;7(1):397. doi:10.1038/s41598-017-00432-0
59. Wang Z, Dai Z, Shu H, et al. Cortical thickness and microstructural white matter changes detect amnestic mild cognitive impairment. J Alzheimers Dis. 2017;56(1):415–428. doi:10.3233/JAD-160724
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.