")
Back to Journals » Cancer Management and Research » Volume 17
Predictive Value of PLR, PNI, and HALP Scores in Ovarian Cancer Staging
Authors Genc SO , Gulturk EA, Kurt B
Received 6 December 2024
Accepted for publication 10 February 2025
Published 13 February 2025 Volume 2025:17 Pages 293—299
DOI https://doi.org/10.2147/CMAR.S508442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Serife Ozlem Genc,1 Esra Akaydin Gulturk,2 Begum Kurt1
1Department of Obstetrics and Gynecology, Sivas Cumhuriyet University Faculty of Medicine, Sivas, Türkiye; 2Department of Biostatistics, Sivas Cumhuriyet University Faculty of Medicine, Sivas, Türkiye
Correspondence: Serife Ozlem Genc, Department of Obstetrics and Gynecology, Sivas Cumhuriyet University Faculty of Medicine, Sivas, Türkiye, Tel +90 543 456 56 24, Email [email protected]
Purpose: Ovarian cancer (OC) is a leading cause of gynecologic cancer mortality, where accurate staging is vital for prognosis and treatment. This study aims to evaluate the prognostic potential of the Platelet-to-Lymphocyte Ratio (PLR), Prognostic Nutritional Index (PNI), and Hemoglobin, Albumin, Lymphocyte, Platelet (HALP) scores in OC staging.
Methods: The study was conducted at the Sivas Cumhuriyet University Faculty of Medicine, Department of Obstetrics and Gynecology, between January 1, 2009, and December 31, 2021. A total of 96 OC patients were retrospectively analyzed. Preoperative PLR, PNI, and HALP scores were calculated from routine laboratory parameters. Associations between these scores and clinicopathological factors, including OC stage, were evaluated. The discriminatory power of each index was assessed through ROC curve and AUC (area under the curve) analysis.
Results: The AUC for PLR was 0.689 (p < 0.05), indicating significant prognostic value, while the HALP score showed an AUC of 0.671 (p < 0.05). Both markers were significantly associated with OC stages, with higher PLR and lower HALP scores correlating with advanced stages. In contrast, PNI demonstrated a lower AUC of 0.398 (p > 0.05), indicating limited prognostic utility.
Conclusion: PLR and HALP scores are useful prognostic markers for OC staging, offering cost-effective and accessible tools in clinical practice. PNI, however, was less predictive. These findings suggest that PLR and HALP could complement existing staging methods, aiding in clinical decision-making. Future large-scale studies are warranted to validate these results.
Keywords: HALP score, PNI, ovarian cancer, prognostic markers
Introduction
Nutritional status is crucial in prognosis and diagnosis, with tools like the neutrophil-to-lymphocyte ratio, systemic inflammatory index, pan-immune inflammatory index, PLR, PNI, and HALP scores assessing it especially in ovarian cancer.1 Cancer cells evade immune detection and proliferate by exploiting adaptive immune mechanisms, contributing to tumor progression.
Platelets facilitate metastasis by shielding cancer cells from natural killer cells, and low HALP scores indicate anemia, hypoalbuminemia, and lymphopenia, which are linked to poor prognosis due to their impact on immune and nutritional status.2,3
The PNI has also gained attention for its prognostic value across cancers with higher scores indicating better nutritional and immune status, while lower scores suggest poorer prognosis.
The HALP score is a significant prognostic indicator in cancers. It includes hemoglobin, albumin, lymphocytes, and platelets, reflecting both immune and nutritional status. Each component contributes to cancer prognosis, such as platelets facilitating metastasis by shielding cancer cells from natural killer cells. Anemia, hypoalbuminemia, and lymphopenia, indicated by low HALP scores, are linked to poor prognosis due to their impact on immune and nutritional status.
This study evaluates the prognostic value of PLR, PNI, and HALP scores in ovarian cancer patients undergoing primary debulking surgery, focusing on their correlation with cancer stage.
Materials and Methods
This observational study included ovarian cancer patients diagnosed between 2009 and 2021. The recruitment process was based on reviewing the medical records of patients treated at a tertiary care clinic. Preoperative PLR, PNI, and HALP scores were calculated using routine laboratory data. The PNI was calculated using the formula: PNI = Albumin (g/L) + 5 × Total Lymphocyte Count (cells/µL). The HALP score was calculated using the formula: HALP = Hemoglobin (g/L) × Albumin (g/L) × Lymphocyte Count (cells/µL) / Platelet Count (cells/µL). The association of these scores with age and ovarian cancer stage was evaluated using detailed data analysis procedures.
The inclusion criteria were confirmed diagnosis of ovarian cancer, undergoing primary debulking surgery, and available preoperative laboratory data. Exclusion criteria included patients under 16 years old, those with concurrent malignancies, severe infections, autoimmune disorders, prior neoadjuvant chemotherapy, or incomplete clinical/lab data. Stage IV ovarian cancer patients who did not undergo surgery due to distant metastasis were excluded.
Staging of ovarian cancer was performed according to the International Federation of Gynecology and Obstetrics classification system.4
Statistical analyses were conducted using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY), with the Kruskal–Wallis test and Spearman’s rank correlation applied for non-parametric data analysis. The classification performance of PLR, HALP and PNI indices was evaluated using ROC curve and AUC analysis, Youden Index, sensitivity and specificity calculations, and p-value and 95% confidence interval analyses. p-value of less than 0.05 was considered statistically significant.
Results
A total of 96 OC patients were included in the study, with a median age of 52 years (range 17–79 years). The patients were categorized into three OC stages: stage I, stage II, and stage III. Among them, 85.1% had epithelial tumors, 9.6% had sex cord stromal tumors, and 5.3% had germ cell tumors.
The PLR score showed significant variation across the different stages of OC. The median PLR value was 160.0 (range 96.0–378.0) for stage I, 154.0 (range 88.0–450.0) for stage II, and 215.0 (range 82.0–542.0) for stage III, with an overall median of 174.0 (range 82.0–542.0). Stage III had significantly higher PLR values compared to stages I and II (p = 0.005) (Table 1). This suggests that higher PLR values are associated with more advanced OC stages.
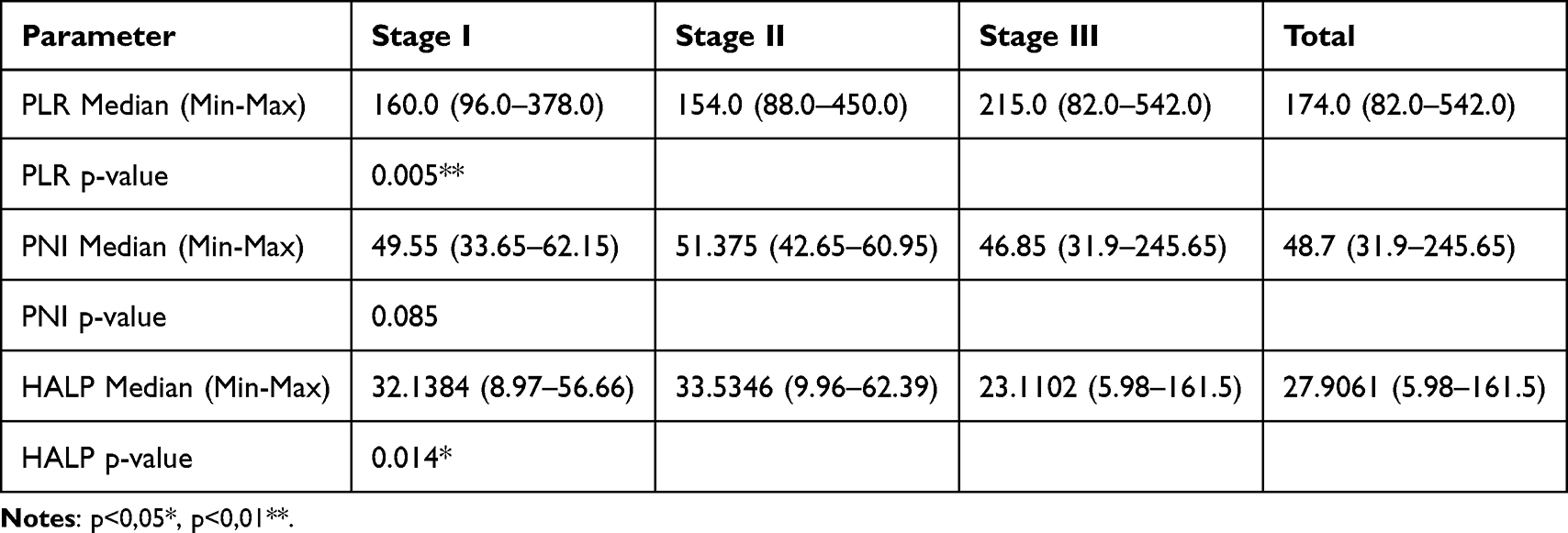 |
Table 1 PLR, PNI, and HALP Scores Across Ovarian Cancer Stages |
The PNI values demonstrated a non-significant trend towards lower scores with advancing stage (p = 0.085). The median PNI values were as follows: stage I, 49.55 (range 33.65–62.15); stage II, 51.375 (range 42.65–60.95); and stage III, 46.85 (range 31.9–245.65), with an overall median of 48.7 (range 31.9–245.65) (Table 1).
The HALP score, on the other hand, exhibited a significant decrease with advancing stages of OC (p = 0.014). The median HALP scores were: stage I, 32.1384 (range 8.97–56.66); stage II, 33.5346 (range 9.96–62.39); and stage III, 23.1102 (range 5.98–161.5), with an overall median of 27.9061 (range 5.98–161.5) (Table 1).
The AUC (area under curve) value for PLR was found to be 0.689, indicating that the classification ability of the PLR index is statistically significant (p < 0.05, 95% CI: 0.581–0.796) with a cutoff value of 175.00, sensitivity of 66.7%, and specificity of 71.1%. (Table 2, Figure 1). For HALP, the AUC value was 0.671, which is also statistically significant (p < 0.05, 95% CI: 0.561–0.780) with a cutoff value of 30.20, sensitivity of 74.5%, and specificity of 62.2%. (Table 2, Figure 2). In contrast, the AUC value for PNI was 0.398, which was not statistically significant (p > 0.05, 95% CI: 0.285–0.511) (Table 2).
 |
Table 2 Evaluation of ROC Performances for PLR, PNI and HALP Score in Ovarian Cancer |
 |
Figure 1 Receiver Operating Characteristic (ROC) curves for PLR in ovarian cancer staging. |
 |
Figure 2 Receiver Operating Characteristic (ROC) curves for HALP in ovarian cancer staging. |
The cut-off value for PLR was 183.5, with a sensitivity of 0.608, indicating that the PLR index correctly predicted 60.8% of true positive cases, and a specificity of 0.756, meaning that 75.6% of true negative cases were correctly classified (Youden Index: 0.364) (Table 2).
Logistic regression analysis showed that the PLR index was a significant predictor of advanced stage ovarian cancer (p = 0.005). An increase of 1 unit in the PLR index increased the likelihood of advanced stage by 1.007 times.
For HALP, the cut-off value was 29.7953, with a sensitivity of 0.725, demonstrating that HALP correctly identified 72.5% of positive cases, and a specificity of 0.622, indicating 62.2% of negative cases were accurately identified (Youden Index: 0.347) (Table 2).
The ROC curves for PLR, HALP, and PNI are presented in Table 2, demonstrating that both PLR and HALP had strong discriminatory abilities, with AUC values of 0.689 and 0.671, respectively, while PNI had a lower AUC of 0.398, indicating weaker classification performance.
Both PLR and HALP indices demonstrated significant results in terms of AUC values and p-values. The PLR index had the highest AUC value (0.689), indicating superior ability in distinguishing between positive and negative cases compared to the other indices. In contrast, the PNI showed poor classification performance and was not statistically significant (AUC = 0.398, p > 0.05). Significant differences were observed between the performance of the PLR and HALP indices. PLR showed higher specificity (0.756), indicating better performance in identifying true negative cases, while HALP had a higher sensitivity (0.725), reflecting better performance in identifying true positive cases. The Youden Index for both indices, with values of 0.364 for PLR and 0.347 for HALP, indicated a balanced trade-off between sensitivity and specificity.
Mann–Whitney U-test revealed significant differences in PLR and HALP scores between early and advanced stages. The median PLR was 158.00 (Q1–Q3: 131.50–195.00) in the early stage group and 215.00 (Q1–Q3: 157.00–283.00) in the advanced stage group (p = 0.001). Similarly, the median HALP was 32.77 (Q1–Q3: 20.57–42.19) in the early stage group and 23.11 (Q1–Q3: 16.89–31.29) in the advanced stage group (p = 0.004).
Discussion
Ovarian cancer is a leading cause of cancer death among women. Many oncological markers are expensive and not readily available, prompting us to develop a score accessible in any center to facilitate patient referral when needed. We focused on indices derived from hemogram and albumin parameters, which are easily obtained during routine exams. While PLR, PNI, and HALP have been explored in other cancers, their role in OC remains unclear.5–7
Recent advancements in understanding the molecular biology of ovarian cancer have identified various genetic mutations, leading to the development of molecular inhibitors. These inhibitors, which target specific pathways such as BRAF, have shown promise in preclinical studies and are currently under evaluation in clinical trials.8 Incorporating such therapies, alongside traditional prognostic indices like PLR and HALP, could further refine patient stratification and treatment approaches.
This study found that PLR and HALP scores were significant for ovarian cancer staging, but PNI was not, consistent with other studies suggesting that PNI’s prognostic value may vary by cancer type.
Our multivariate analysis confirmed that PLR and HALP scores were independent prognostic markers for ovarian cancer staging. These findings align with previous studies emphasizing the clinical utility of inflammation- and nutrition-based indices in cancer prognosis.
Growing evidence highlights the significance of tumor biomarker mutations in diagnosing and managing epithelial ovarian cancer. Recent studies have shown the correlation between specific biomarkers, such as BRCA mutations, and chemotherapy response, which has paved the way for personalized treatment strategies. For instance, the efficacy of olaparib, a PARP inhibitor, in patients with BRCA-mutated relapsed ovarian cancer underscores the importance of genetic profiling in therapeutic decision-making.9 Incorporating these targeted therapies alongside traditional prognostic indices, like PLR and HALP, could further refine patient stratification and treatment approaches.
The PLR, on the other hand, emerged as a robust prognostic factor in OC, consistent with findings from multiple studies that have shown an association between elevated PLR and poor overall and progression-free survival in OC patients.3,10,11 Previous studies report optimal PLR cutoff values ranging from 200 to 226,3,11,12 while our study identified a lower cutoff of 183.5 for stage III OC, indicating a significant difference compared to stages I and II (p=0.001, p<0.05, Table 2). This suggests that PLR can serve as an early indicator of disease progression, supporting its use as a reliable prognostic marker.
In a study, it was found that decreased pretreatment PNI is an independent poor prognostic factor in patients with advanced-stage epithelial OC.13 In a study by Feng et al evaluating preoperative PNI in high-grade serous OC, PNI was assessed as both a predictive and prognostic factor.14 Similarly, Zhang et al conducted a study to assess the role of preoperative PNI in predicting the prognosis of stage III OC, finding that decreased preoperative PNI is a strong predictor of poor prognosis in stage III OC.15 Another study similarly found that while PNI is a significant predictor in other malignancies, it may not effectively reflect the prognostic landscape in ovarian cancer.16 This may be due to ovarian cancer’s unique inflammatory and immune characteristics, which differ from gastrointestinal cancers, where PNI has shown stronger predictive capacity. In our study, PNI did not change significantly with increasing OC stages (p=0.85, p>0.05, Table 1), corroborating Fumagalli et al’s findings that PNI has limited prognostic utility in OC.17
The HALP score has also emerged as a valuable prognostic indicator in several cancers.3,18 It has been associated with worse outcomes in locally advanced cervical cancer (HALP ≤ 22.2), advanced epithelial OC (HALP ≤ 22.6), and colon cancer (HALP ≤ 22.5).18–20 In our study, the median HALP score for stage III OC was 23.11, aligning closely with the literature. Additionally, we observed a significantly lower HALP score for stage III OC, with a cutoff value of 29.79 (p=0.002, p<0.05). This reinforces HALP’s role as an effective marker of nutritional and inflammatory status, supporting its potential as a clinical predictor of survival across various cancer types.
Limitations
There are a few limitations in the present study: The first is that it is a study with the relatively small number of patients in this single-institution retrospective study, and the second is that it did not include patients with stage IV disease.
This study was conducted using a single-institution cohort, which inherently limits the ability to validate findings in external datasets or construct advanced predictive tools such as nomograms and decision curve analysis. While we performed robust statistical analyses, including univariate and multivariate logistic regression, the development and validation of nomograms require larger, multi-cohort datasets to ensure generalizability. This was beyond the scope of our current study. Future research will focus on incorporating external cohorts and constructing nomograms to enhance the clinical utility of our findings.
Conclusions
In conclusion, the preoperative PLR, derived from serum platelet and lymphocyte counts, has shown significant potential as an independent prognostic marker in ovarian cancer patients, supplementing the International Federation of Gynecology and Obstetrics staging system. PLR may be used either as a standalone indicator or in conjunction with other clinicopathological factors to enhance the accuracy of prognosis in ovarian cancer. Similarly, the HALP score, calculated from easily accessible serum biomarkers, has proven to be a valuable prognostic tool for patients undergoing surgical staging for ovarian cancer. Its simplicity and cost-effectiveness make HALP a promising marker in clinical settings. Further large-scale, multi-center prospective studies are needed to validate the prognostic utility of both PLR and HALP in ovarian cancer management.
Abbreviations
OC, Ovarian cancer; PLR, Platelet to lymphocyte ratio; PNI, Prognostic nutritional index; HALP, Hemoglobin, Albumin, Lymphocyte, Platelet; AUC, Area under curve.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent
This study was approved by the Sivas Cumhuriyet University Clinical Research Ethics Committee (Approval Number: 2024/06-40) and in compliance with the principles outlined in the Declaration of Helsinki. All participants were informed about the purpose and procedures of the study, and written informed consent was obtained from each participant prior to their inclusion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive support from public, commercial, or non-profit groups.
Disclosure
The authors declare no conflict of interest related to this study.
References
1. Winata I, Pradnyana I, Yusrika MU, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as an early prognostic marker in patients with ovarian cancer: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2024;25:1921–1927. doi:10.31557/APJCP.2024.25.6.1921
2. Farag CM, Antar R, Akosman S, et al. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP’s prognostic ability in different cancer types. Oncotarget. 2023;14(1):153. doi:10.18632/oncotarget.28367
3. Xu H, Zheng X, Ai J, et al. Hemoglobin, albumin, lymphocyte, and platelet (HALP) score and cancer prognosis: a systematic review and meta-analysis of 13,110 patients. Int Immunopharmacol. 2023;118:110165.
4. Smith J, Brown P, Thompson L, et al. Clinical relevance of FIGO staging in ovarian cancer management: a comprehensive review. Gynecol Oncol. 2023;150(2):214–220.
5. Jiang T, Sun H, Xue S, et al. Prognostic significance of hemoglobin, albumin, lymphocyte, and platelet (HALP) score in breast cancer: a propensity score-matching study. Cancer Cell Int. 2024;24:230. doi:10.1186/s12935-024-03419-w
6. Güç Z. HALP score: a simple and easily accessible index for predicting prognosis in colorectal cancer patients. Genel Tip Dergisi. 2022;32(5):577–582. doi:10.54005/geneltip.1179659
7. Atasever Akkas E, Erdis E, Yucel B. Prognostic value of the systemic immune-inflammation index, systemic inflammation response index, and prognostic nutritional index in head and neck cancer. Eur Arch Otorhinolaryngol. 2023;280:3821–3830. doi:10.1007/s00405-023-07954-6
8. Perrone C, Angioli R, Luvero D, et al. Targeting BRAF pathway in low-grade serous ovarian cancer. J Gynecol Oncol. 2024;35(4):e104. doi:10.3802/jgo.2024.35.e104
9. Tonti N, D’Augè G, Cuccu T, et al. The role of tumor biomarkers in tailoring the approach to advanced ovarian cancer. Int J Mol Sci. 2024;25(20):11239. doi:10.3390/ijms252011239
10. Chon S, Lee S, Jeong D, et al. Elevated platelet lymphocyte ratio is a poor prognostic factor in advanced epithelial ovarian cancer. J Gynecol Obstet Hum Reprod. 2021;50:101849. doi:10.1016/j.jogoh.2020.101849
11. Zhang WW, Liu KJ, Hu GL, et al. Preoperative platelet/lymphocyte ratio is a superior prognostic factor compared to other systemic inflammatory response markers in ovarian cancer patients. Tumor Biol. 2015;36:8831–8837. doi:10.1007/s13277-015-3533-9
12. Ma XM, Sun X, Yang GW, et al. The platelet-to-lymphocyte ratio as a predictor of patient outcomes in ovarian cancer: a meta-analysis. Climacteric. 2017;20:448–455. doi:10.1080/13697137.2017.1326894
13. Raungkaewmanee S, Tangjitgamol S, Manusirivithaya S, et al. Platelet to lymphocyte ratio as a prognostic factor for epithelial ovarian cancer. J Gynecol Oncol. 2012;23:265–273. doi:10.3802/jgo.2012.23.4.265
14. Komura N, Mabuchi S, Yokoi E, et al. Prognostic significance of the pretreatment prognostic nutritional index in patients with epithelial ovarian cancer. Oncotarget. 2019;10(38):3605. doi:10.18632/oncotarget.26914
15. Feng Z, Wen H, Ju X, et al. The preoperative prognostic nutritional index is a predictive and prognostic factor of high-grade serous ovarian cancer. BMC Cancer. 2018;18:883. doi:10.1186/s12885-018-4732-8
16. Fumagalli D, Sonik R, Luigi A, et al. Evaluating nutrition in advanced ovarian cancer: which biomarker works best? Gynecol Oncol. 2024;188:97–102. doi:10.1016/j.ygyno.2024.06.021
17. Shi Y, Zhang Y, Niu Y, et al. Prognostic role of the prognostic nutritional index (PNI) in patients with head and neck neoplasms undergoing radiotherapy: a meta-analysis. PLoS One. 2021;16(9):e0257425. doi:10.1371/journal.pone.0257425
18. Amado A, Pimenta J, Queirós T, et al. Preoperative HALP score as a predictor of survival in locally advanced colon cancer. J Surg Clin Res. 2022;13:1–9. doi:10.20398/jscr.v13i1.29546
19. Leetanaporn K, Hanprasertpong J, Vacharat N, et al. Predictive value of the hemoglobin-albumin-lymphocyte-platelet (HALP) index on the oncological outcomes of locally advanced cervical cancer patients. Cancer Manag Res. 2023;15:1961–1972.
20. Atjimakul T, Saeaib N, Tunthanathip T, et al. Significance of pretreatment hemoglobin-albumin-lymphocyte-platelet index for the prediction of suboptimal surgery in epithelial ovarian cancer. World J Oncol. 2024;15:268–274. doi:10.14740/wjon1778
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.