")
Back to Journals » Journal of Pain Research » Volume 18
Predictors for Postoperative Nerve Recovery in Severe Carpal Tunnel Syndrome
Authors Luo Z, Ma T, Tian S, Yu K, Tian D
Received 28 January 2025
Accepted for publication 8 May 2025
Published 19 May 2025 Volume 2025:18 Pages 2559—2565
DOI https://doi.org/10.2147/JPR.S519904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Zixuan Luo,1 Tao Ma,2 Siyu Tian,3 Kunlun Yu,4 Dehu Tian4
1Department of Foot Surgery, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China; 2Department of Trauma Emergency Surgery, The First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei, 075000, People’s Republic of China; 3Department of Orthopaedic Surgery, Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China; 4Department of Hand Surgery, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China
Correspondence: Dehu Tian, Department of Hand Surgery, The Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China, Email [email protected]
Purpose: Severe carpal tunnel syndrome (CTS) is a nerve compression disease that can lead to muscle atrophy from denervation. However, research on neurological recovery after surgery in severe CTS patients is relatively limited. This study mainly explores the predictors for poor postoperative neurological recovery in severe CTS patients.
Methods: This study collected data of severe CTS patients who received surgery in our hospital from January 2022 to January 2024. According to the recovery of nerve function during follow-up, patients were divided into two groups. Clinical data of severe CTS patients were analyzed.
Results: Age (P< 0.001), disease duration (P=0.013), and 2-PD (P< 0.001) of patients were closely related to poor postoperative neurological recovery at 6-month follow-up. Logistic regression analysis showed that age (P=0.011) and 2-point discrimination (2-PD) (P=0.001) were independent risk factors for poor neurological function recovery at 6 months follow-up and the cutoff values of age and 2-PD were 53 years and 13.5 mm, respectively. Univariate analysis showed that age (P=0.044), disease duration (P=0.015), 2-PD (P< 0.001), and grip strength (P=0.005) were closely related to poor postoperative neurological recovery at 12-month follow-up. Logistic regression analysis showed that 2-PD (P=0.034) was a predictor of poor neurological function recovery at 12-month follow-up and the cutoff value of 2-PD was 13.5 mm.
Conclusion: We found that age and 2-PD were independent risk factors for poor neurological function recovery at 6-month follow-up. However, 2-PD is a predictor for poor neurological recovery at 1-year follow-up. We also identified their cutoff values. This study helps us to personalize the risk of postoperative neurological recovery in patients with severe CTS in order to provide targeted early intervention.
Keywords: carpal tunnel syndrome, 2-point discrimination, predictors, poor neurological recovery
Introduction
Carpal Tunnel Syndrome (CTS) is the most common nerve compression disease, characterized by compression of the median nerve, which provides sensation to the radial side of the thumb, index finger, middle finger, and ring finger, and controls their movements.1–4 CTS may cause various symptoms, such as pain, numbness, loss of dexterity, weakness, or even pain. Symptoms usually worsen at night and may be intermittent or continuous depending on the degree and duration of carpal tunnel compression, causing significant damage to the patient’s quality of life.
If early intervention is not carried out, hand function will deteriorate. According to the literature, the incidence rate of CTS in western countries is nearly 5%. In Sweden, 232 women and 104 men receive surgical treatment per 100000 people every year, of which women aged 50–54 and men aged 75–79 have the highest incidence rate. Similarly, in Finland, 197 women and 105 men out of 100000 people experience CTS every year.4–6 It is reported that the incidence of CTS in the UK has declined slightly.7 CTS is very common in pregnant women with an incidence rate of 31%-62%.8 In most cases, CTS can be cured postpartum without any surgery,9 but 30% of women who have not undergone surgical treatment may experience persistent symptoms up to 3 years postpartum.10
The etiology of CTS is multifactorial, including genetic and environmental factors. Research shows that obesity, rheumatoid arthritis, diabetes, acromegaly and hypothyroidism are related to CTS.11–14 Obesity may be associated with potential neurological disorders and extraneural factors. However, with the current use of effective biological treatment for rheumatoid arthritis in high-income countries, the incidence of CTS may be declining.15 Diabetes can significantly increase the risk of CTS.16 It is reported that the risk of CTS in patients with type 1 diabetes is 85% because the mechanism makes nerves more likely to be compressed.16 Type 2 diabetes, lipid metabolism and statin treatment can increase the risk of CTS, which may be related to potential neuropathy.17
There is no unified grading standard for the severity of CTS both domestically and internationally. At present, the most commonly used grading diagnosis and treatment in clinical practice is proposed by Gu,18 mainly based on the patient’s clinical symptoms, electromyography, two-point discrimination (2-PD), and other results (Table 1). The treatment methods for CTS include conservative and surgical treatment. Regarding patients with severe CTS, this surgical treatment can alleviate symptoms. However, research on neurological recovery after surgery in severe CTS patients is relatively limited. This study mainly explores the predictors for poor postoperative neurological recovery in severe CTS patients.
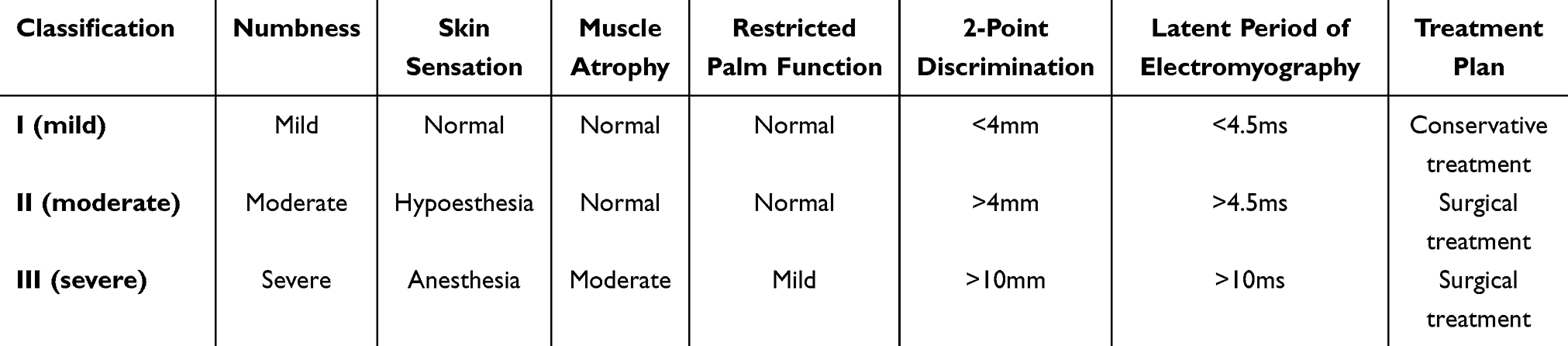 |
Table 1 Classification for Carpal Tunnel Syndrome |
Materials and Methods
Ethical Statement
The study was approved by the Institutional Review Board of Third Hospital of Hebei Medical University in compliance with the Helsinki and an exemption from the informed consent was obtained. All data were anonymized before the analysis to safeguard patient privacy (W2021-046-1).
Patients
This study retrospectively analyzed the clinical data of CTS patients treated in our hospital from January 2022 to January 2024. The diagnosis of severe CTS is based on the patient’s clinical symptoms, electromyography, 2-PD, and other results (Table 1). According to the recovery of hand nerve function at follow-up time (Table 2), excellent and good patients were divided into the excellent and good group, and average and poor patients were divided into the average and poor group. The inclusion criteria are: (1) severe CTS patients, which is based on the patient’s clinical symptoms, electromyography, 2-PD, and other results; (2) adult patients (≥18 years old); The exclusion criteria are: (1) patients with a history of multiple wrist injuries or neurovascular injuries; (2) pathological compression of the median nerve in patients; (3) cervical spondylosis patients; (4) patients with a history of surgical treatment for CTS; (5) incomplete data.
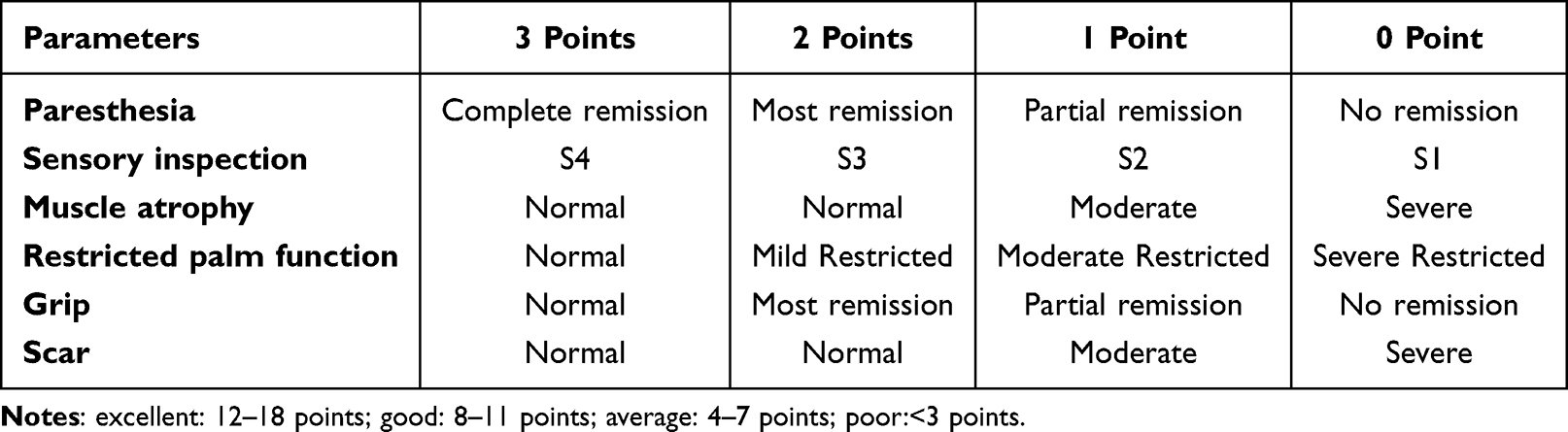 |
Table 2 Hand Function Evaluation |
This study collected clinical data and relevant examination results of patients at admission. Demographic data includes age, gender, body mass index, and disease duration; The admission examination indicators include 2-point Discriminant (2-PD), electromyography and grip strength.
Surgical Procedure
After anesthesia, we use a tourniquet on the affected upper arm. Make a 2 cm incision on the skin of the palm along the burned side of the thenar muscle line at the distal end of the wrist crease, cut open the transverse ligament of the wrist, and observe the compression of the median nerve. Thoroughly stop bleeding during surgery, and gradually engage in functional exercises after surgery, including hand grasping and fine motor exercises. And combined with oral neurotrophic drugs.
Statistics
We used SPSS (version 27.0 SPSS Inc., Chicago, IL) to analyze the data with significance levels of p<0.05. Because our data did not satisfy the criteria for normality and homogeneity of variance, we performed rank sum test. Regarding count data, we used Chi-square test. We used univariate and logistic regression analyses to analyze data. We also explore the cutoff values for continuous variables by the maximum Youden index (sensitivity+specificity-1) in the ROC curve analysis.
Results
Overall results
From January 2022 to January 2024, a total of 210 patients with CTS were screened in this study. Finally, based on the inclusion and exclusion criteria, 118 patients were included in our study. At 6-month follow-up, 63 patients received our follow-up, including 40 patients achieving excellent and good functional recovery and 23 patients achieving average and poor functional recovery (63.5%); at 12-month follow-up, 42 patients received our follow-up, including 25 patients achieving excellent and good functional recovery and 17 patients achieving average and poor functional recovery (59.5%).
Results of Univariate Analysis
As shown in Table 3, there was no statistically significant difference (P>0.05) in gender, BMI, and grip strength in the two groups at 6-month follow-up. However, we found that age (P<0.001), disease duration (P=0.013), and 2-PD (P<0.001) were closely related to postoperative neurological at 6-month follow-up (Table 3). There was no statistically significant difference in gender, and BMI at 12-month follow-up (P>0.05). However, our finding showed that age (P=0.044), disease duration (P=0.015), 2-PD (P<0.001), and grip strength (P=0.005) were closely related to postoperative neurological at 12-month follow-up (Table 3).
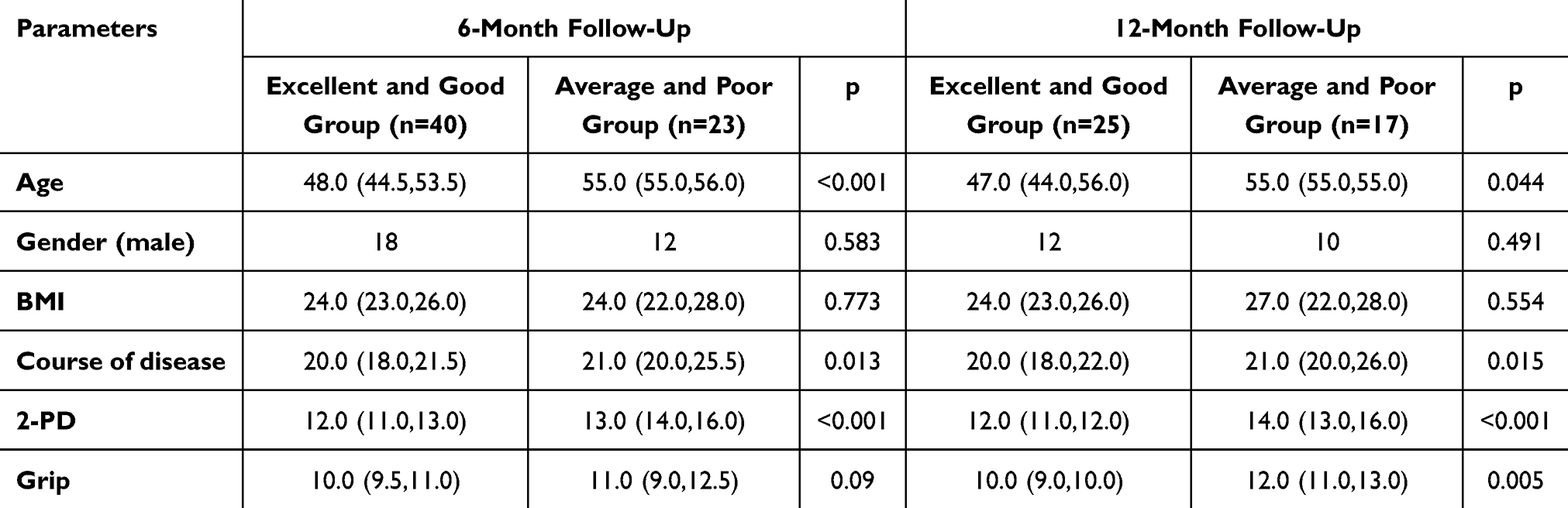 |
Table 3 Univariate Analysis of Postoperative Recovery of Carpal Tunnel Syndrome at Different Follow-Up Times |
Results of Logistic Regression Analysis
Logistic regression analysis showed that age [P=0.011, OR=1.235, 95% CI (1.050, 1.453)] and 2-PD [P=0.001, OR=2.894, 95% CI (1.530, 5.474)] were independent risk factors for poor neurological function recovery at 6-month follow-up (Table 4). However, 2-PD [P=0.034, OR=9.588, 95% CI (1.187, 77.474)] is a predictor for poor neurological function recovery at 12-month follow-up (Table 4).
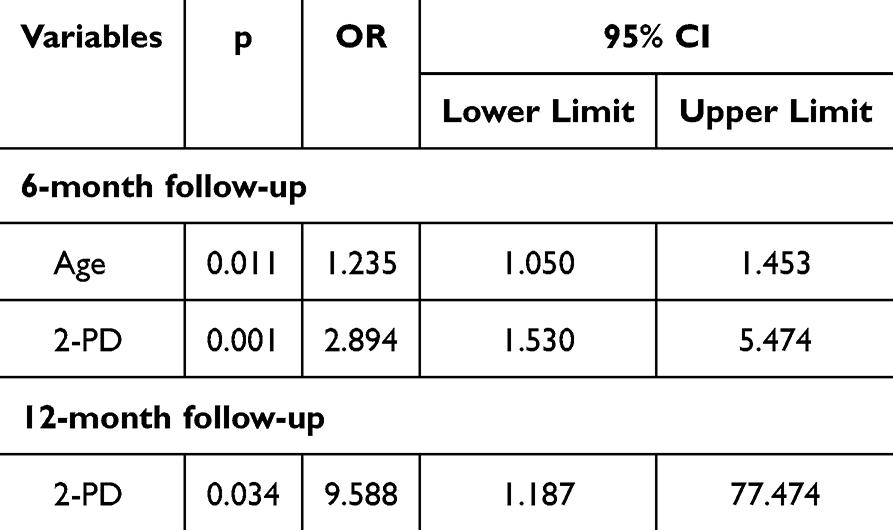 |
Table 4 Logistic Regression Analysis of Postoperative Recovery of Carpal Tunnel Syndrome at Different Follow-Up Times |
ROC curve analysis showed that age [P<0.001, AUC=0.772, 95% CI (0.653, 0.891)] and 2-PD [P<0.001, AUC=0.836, 95% CI (0.728, 0.945)] were independent risk factors for poor neurological function recovery at 6-month follow-up, with cutoff values of 53 years and 13.5 mm, respectively (Table 5). In addition, ROC curve analysis showed that 2-PD [P<0.001, AUC=0.888, 95% CI (0.774, 1.000)] was an independent risk factor for poor neurological function recovery at 12-month follow-up, with a cutoff value of 13.5 mm (Table 5).
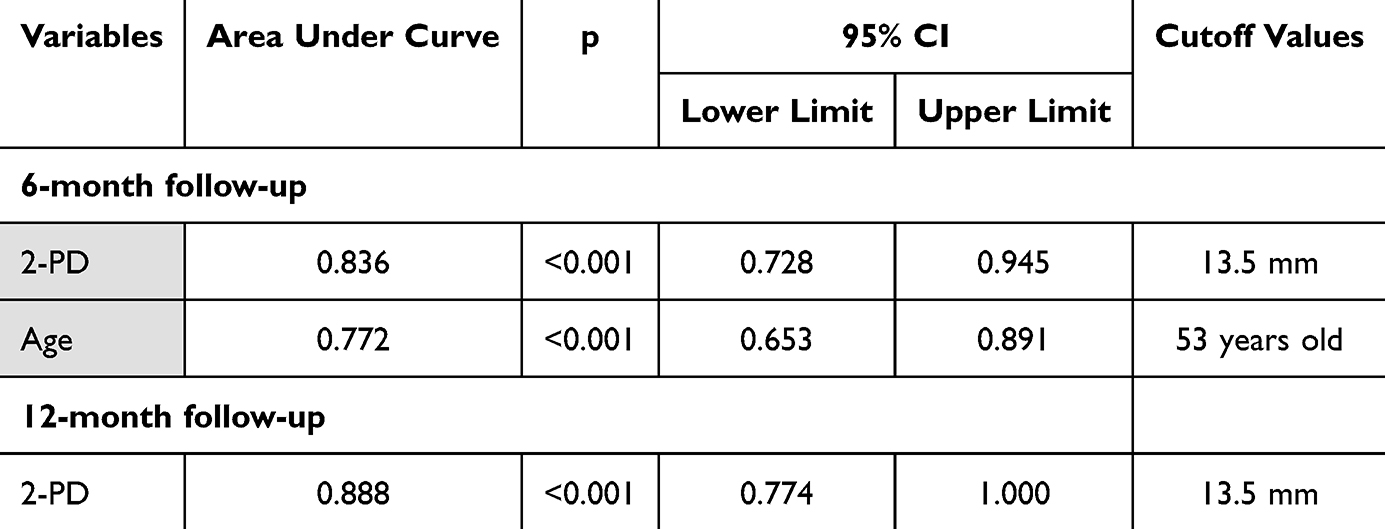 |
Table 5 ROC Curve Analysis and Cutoff Values of Postoperative Recovery of Carpal Tunnel Syndrome at Different Follow-Up Times |
Discussion
CTS is the most common compression of the median nerve, clinically manifested as numbness in the radial three and a half fingers innervated by the median nerve. Literature reports on gender, BMI, age, smoking, wrist injury, diabetes, vitamin D deficiency, hypothyroidism, high waist circumference/waist hip ratio are related to the occurrence of CTS. The treatment methods for CTS can be divided into conservative treatment and surgical treatment. Conservative treatment mainly includes fixation with braces, injection of cortisol into the carpal tunnel, drug therapy, laser therapy, or ultrasound therapy. Regarding patients with moderate to severe CTS, surgical treatment is often required.19
The latest research shows that genetic factors are the key factors leading to CTS. A genome-wide association study identified 16 gene loci associated with the development of CTS.20 In addition, factors, such as low height, may increase the risk of CTS.20 It may be speculated that this may be related to the higher incidence of women. Some psychological factors, such as stress, catastrophizing pain, and perceived illness, are associated with CTS.21–24 Compared to the general population, CTS patients who undergo surgical treatment have an increased risk of mental health impairment.25 In fact, early research on the diagnosis and treatment of CTS has emphasized the impact of occupational risk factors on the development of CTS.26,27 Occupational risk factors from different research reports worldwide include non-neutral static posture, repetitive movements, high work pressure, and exposure to arm vibration.20,28,29 However, research on neurological recovery after surgery in severe CTS patients is relatively limited. This study mainly explores the predictors for poor postoperative neurological recovery in severe CTS patients.
According to the inclusion and exclusion criteria, 118 patients with severe CTS in our hospital underwent surgical treatment. At 6-month follow-up, we collected data from 63 patients with an excellent rate of 63.5% (40 patients achieving excellent and good functional recovery and 23 patients achieving average and poor functional recovery). At 12-month follow-up, we collected data from 42 patients with an excellent rate of 59.5% (25 patients achieving excellent and good functional recovery and 17 patients achieving average and poor functional recovery). Based on univariate and multivariate analysis, we found that age and 2-PD were independent risk factors for poor neurological function recovery at 6-month follow-up. However, 2-PD was found to be the only independent risk factor at 1-year follow-up.
The literature reports that the clinical and electrophysiological severity of CTS in elderly patients is increased and associated with aging, which may be secondary to chronic compression and mechanical stress-induced factors.20 Zyluk Gadowska30 found that the older patient, the worse outcome of surgery, mainly manifested as decreased hand function, which greatly affects the patient’s prognosis. Gunes31 believes that advanced age and high BMI seriously affect the surgical outcomes with 6- to 9-month follow-up. Our research confirms that age contributes to the recovery of hand function in the mid-term follow-up, but does not affect it in the long-term follow-up. The difference from previous literature may be related to the follow-up time.
Choi32 found that the disease duration also affects the surgical prognosis, implying patients with shorter disease duration recovering faster than those with longer disease duration. But at 1-year follow-up, the recovery outcomes for all groups were the same. This is partially consistent with our results that our findings showing disease duration playing a crucial role in postoperative recovery by univariate analysis. However, in multivariate analysis, the disease duration did not affect the postoperative recovery of CTS patients. We found that only 2-PD affects the postoperative prognosis of patients with severe CTS in both mid-term and long-term follow-up. Due to individual differences and variations in the causes of illness, patients with a long course of illness may not necessarily have a severe condition. Similarly, patients with a short course of illness may not necessarily have a mild condition. 2-PD can truly reflect the severity of nerve damage.
Although this article provides long-term follow-up for postoperative neurological recovery in patients with severe CTS, which is somewhat innovative, there are also some limitations. First, single center research inevitably affects the accuracy of the results. A large sample, multicenter, randomized controlled study is required. Second, retrospective studies have some inherent limitations; therefore, prospective studies are needed in the future. Third, due to the limited number of patients with severe CTS, we did not conduct subgroup analysis or establish the prediction model.
We found that age and 2-PD were independent risk factors for poor neurological function recovery at 6-month follow-up. However, 2-PD is an independent risk factor for poor neurological recovery at 1-year follow-up. We also identified their cutoff values. This study helps us to personalize the risk of postoperative neurological recovery in patients with severe CTS in order to provide targeted early intervention.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethical Statement
The study was approved by the Institutional Review Board of Third Hospital of Hebei Medical University in compliance with the Helsinki and an exemption from the informed consent was obtained. All data were anonymized before the analysis to safeguard patient privacy (W2021-046-1).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This article was funded by 2025 Outstanding Clinical Medicine Talent Development Initiative supported by Hebei Provincial Government (Project ID: ZF2025272).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Malakootian M, Soveizi M, Gholipour A, et al. Pathophysiology, diagnosis, treatment, and genetics of carpal tunnel syndrome: a review. Cell Mol Neurobiol. 2023;43:1817–1831. doi:10.1007/s10571-022-01297-2
2. Atroshi I, Gummesson C, Johnsson R, et al. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282:153–158. doi:10.1001/jama.282.2.153
3. Atroshi I, Englund M, Turkiewicz A, et al. Incidence of physician-diagnosed carpal tunnel syndrome in the general population. Arch Intern Med. 2011;171(10):943–944. doi:10.1001/archinternmed.2011.203
4. Tadjerbashi K, Åkesson A, Atroshi I. Incidence of referred carpal tunnel syndrome and carpal tunnel release surgery in the general population: increase over time and regional variations. J Orthop Surg. 2019;27(1):2309499019825572. doi:10.1177/2309499019825572
5. Phalen GS. The carpal-tunnel syndrome. Seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966;48(2):211–228. doi:10.2106/00004623-196648020-00001
6. Hulkkonen S, Lampainen K, Auvinen J, et al. Incidence and operations of median, ulnar and radial entrapment neuropathies in Finland: a nationwide register study. J Hand Surg Eur Vol. 2020;45(3):226–230. doi:10.1177/1753193419886741
7. Johnson NA, Darwin O, Chasiouras D, et al. The effect of social deprivation on the incidence rate of carpal and cubital tunnel syndrome surgery. J Hand Surg Eur Vol. 2021;46(3):265–269. doi:10.1177/1753193420939384
8. Daliri M, Johnston TP, Sahebkar A. Statins and peripheral neuropathy in diabetic and non-diabetic cases: a systematic review. J Pharm Pharmacol. 2023;75(5):593–611. doi:10.1093/jpp/rgac104
9. Nyrhi L, Kuitunen I, Ponkilainen V, et al. Incidence of peripheral nerve decompression surgery during pregnancy and the first year after delivery in Finland from 1999 to 2017: a retrospective register-based cohort study. J Hand Surg Am. 2023;48(5):452–459. doi:10.1016/j.jhsa.2023.01.013
10. Padua L, Di Pasquale A, Pazzaglia C, et al. Systematic review of pregnancy-related carpal tunnel syndrome. Muscle Nerve. 2010;42(5):697–702. doi:10.1002/mus.21910
11. Shiri R, Pourmemari MH, Falah-Hassani K, et al. The effect of excess body mass on the risk of carpal tunnel syndrome: a meta-analysis of 58 studies. Obes Rev. 2015;16(12):1094–1104. doi:10.1111/obr.12324
12. Wiberg A, Smillie RW, Dupré S, et al. Replication of epidemiological associations of carpal tunnel syndrome in a UK population-based cohort of over 400,000 people. J Plast Reconstr Aesthet Surg. 2022;75(3):1034–1040. doi:10.1016/j.bjps.2021.11.025
13. Hassan A, Beumer A, Kuijer PPFM, et al. Work-relatedness of carpal tunnel syndrome: systematic review including meta-analysis and GRADE. Health Sci Rep. 2022;5(6):e888. doi:10.1002/hsr2.888
14. Sandy-Hindmarch O, Bennett DL, Wiberg A, et al. Systemic inflammatory markers in neuropathic pain, nerve injury, and recovery. Pain. 2022;163(3):526–537. doi:10.1097/j.pain.0000000000002386
15. RC Vernick, CH Beckwitt, JR Fowler. Subjective and objective differences in patients with unilateral and bilateral carpal tunnel syndrome and the role of obesity in syndrome severity. Plast Reconstr Surg. 2024;153(2):423–429. doi:10.1097/PRS.0000000000010773
16. Lee KH, Lee CH, Lee BG, et al. The incidence of carpal tunnel syndrome in patients with rheumatoid arthritis. Int J Rheum Dis. 2015;18(1):52–57. doi:10.1111/1756-185X.12445
17. Pourmemari MH, Shiri R. Diabetes as a risk factor for carpal tunnel syndrome: a systematic review and meta-analysis. Diabet Med. 2016;33(1):10–16. doi:10.1111/dme.12855
18. Ming-jie Y, Qilin S, Lin Z, et al. Intraoperative distal motor latency as a predictor of carpal tunnel release. Chin J Hand Surg. 2006;22(2):92–94.
19. Macdonald K, Pearson H, Frew GH, et al. Use of a remote assessment pathway for diagnosis of carpal tunnel syndrome. J Hand Surg Eur Vol. 2025;50(3):357–361. doi:10.1177/17531934241270347
20. Padua L, Cuccagna C, Giovannini S, et al. Carpal tunnel syndrome: updated evidence and new questions. Lancet Neurol. 2023;22(3):255–267. doi:10.1016/S1474-4422(22)00432-X
21. Mondelli M, Curti S, Farioli A, et al. Anthropometric measurements as a screening test for carpal tunnel syndrome: receiver operating characteristic curves and accuracy. Arthritis Care Res. 2015;67(5):691–700. doi:10.1002/acr.22465
22. Barcenilla A, March LM, Chen JS, et al. Carpal tunnel syndrome and its relationship to occupation: a meta-analysis. Rheumatology. 2012;51(2):250–261. doi:10.1093/rheumatology/ker108
23. Harris-Adamson C, Eisen EA, Dale AM, et al. Personal and workplace psychosocial risk factors for carpal tunnel syndrome: a pooled study cohort. Occup Environ Med. 2013;70(8):529–537. doi:10.1136/oemed-2013-101365
24. Sun PO, Walbeehm ET, Selles RW, et al. Influence of illness perceptions, psychological distress and pain catastrophizing on self-reported symptom severity and functional status in patients with carpal tunnel syndrome. J Psychosom Res. 2019;126:109820. doi:10.1016/j.jpsychores.2019.109820
25. Núñez-Cortés R, Cruz-Montecinos C, Torres-Castro R, et al. Effects of cognitive and mental health factors on the outcomes following carpal tunnel release: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2022;103(8):1615–1627. doi:10.1016/j.apmr.2021.10.026
26. Eurostat. European occupational diseases statistics. European Commission. 2013. Available from: https://ec.europa.eu/eurostat/web/experimental-statistics/european-occupational-diseasesstatistics.
27. Brain WR, Wright AD, Wilkinson M. Spontaneous compression of both median nerves in the carpal tunnel; six cases treated surgically. Lancet. 1947;1(6443–6445):277–282. doi:10.1016/S0140-6736(47)90093-7
28. Tanzer RC. The carpal-tunnel syndrome; a clinical and anatomical study. J Bone Joint Surg Am. 1959;41-A(4):626–634. doi:10.2106/00004623-195941040-00007
29. Carrillo-Ruiz JD, Cortés-Contreras AP, Salazar AA, et al. Positive sensory symptoms, in surgically managed patients with carpal tunnel syndrome: a long term follow-up. Exp Ther Med. 2024;28(4):401. doi:10.3892/etm.2024.12690
30. Zyluk-Gadowska P, Zyluk A. Factors affecting the outcomes of carpal tunnel surgery: a review. Faktoren, die das Ergebnis einer Karpaltunneloperation beeinflussen - eine Literaturübersicht. Handchir Mikrochir Plast Chir. 2016;48(5):260–265. doi:10.1055/s-0042-112869
31. Gunes M, Ozeren E. Effect of age and body mass index on surgical treatment outcomes in patients with carpal tunnel syndrome. Turk Neurosurg. 2021;31(1):83–87. doi:10.5137/1019-5149.JTN.29704-20.2
32. Choi SJ, Ahn DS. Correlation of clinical history and electrodiagnostic abnormalities with outcome after surgery for carpal tunnel syndrome. Plast Reconstr Surg. 1998;102(7):2374–2380. doi:10.1097/00006534-199812000-00016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.